Abdomen Agudo Clinics

of 19
-
Upload
victor-berrocal-arias -
Category
Documents
-
view
221 -
download
0
Transcript of Abdomen Agudo Clinics
-
8/2/2019 Abdomen Agudo Clinics
1/19
Canc er Em ergenc ies :Th e Acut e Abdom en
Jonathan S. Ilgen, MD*, Amy L. Marr, MD
The most common complaints among patients with cancer who present to the emer-gency department (ED) are related to the gastrointestinal system, and 40% of these
patients complain of abdominal pain.1 These presentations can stem from the under-
lying malignancy itself, the treatment directed toward the disease, or the full range of
pathologies present in a healthy population. Moreover, immunosuppression may blunt
many of the findings one expects in a healthy population of patients, thus rendering the
clinical examination less reliable in patients with cancer. This article focuses specifi-
cally on patients with cancer who present with an acute abdomen, and discusses
how a concurrent malignancy can shape the differential diagnosis in these cases.
To facilitate an organized approach to this article, the authors have considered
these processes within three broad categories for the acute abdomen in patientswith cancer: intestinal obstruction, intestinal perforation, or pathology unique to immu-
nosuppression and malignancy.
THE IMPACT OF IMMUNOSUPPRESSION
Clinical findings and the spectrum of infectious processes are affected by the patients
degree of immunosuppression. For simplicity, these can be classified as mild-to-
moderate or severe forms of immunosuppression (Table 1).2 Patients in group I
(mild-to-moderate) are not undergoing chemotherapy, though they have blunted
symptoms due to their lack of an appropriate inflammatory response. Because ofthis, they often seek medical attention later in the course of their disease. Other
than the direct impact of the malignancy itself, however, these patients have patholo-
gies similar to those of a healthy population.2 Patients with profound immunosuppres-
sion associated with chemotherapy (group II) are more challenging. It is in this group of
patients that classic examination findings of fever and abdominal tenderness may be
replaced by vague signs or symptoms such as tachycardia, hypotension, and confu-
sion.2 Concurrently, the differential diagnosis must be expanded to include a wide
variety of atypical opportunistic infections.2
Department of Emergency Medicine, Oregon Health & Science University, 3181 SW Sam JacksonPark Road, CDW-EM, Portland, OR 97239, USA* Corresponding author.E-mail address: [email protected] (J.S. Ilgen).
KEYWORDS
Malignancy Abdominal pain Immunosuppression Management Malignant bowel obstruction
Emerg Med Clin N Am 27 (2009) 381399doi:10.1016/j.emc.2009.04.006 emed.theclinics.com0733-8627/09/$ see front matter 2009 Elsevier Inc. All rights reserved.
mailto:[email protected]://emed.theclinics.com/http://emed.theclinics.com/mailto:[email protected] -
8/2/2019 Abdomen Agudo Clinics
2/19
MALIGNANT BOWEL OBSTRUCTION
In the United States, intestinal obstruction is a common cause of hospitalization, rep-
resenting roughly 15% of all emergency admissions for abdominal pain, or 300,000
hospitalizations per year.3 This risk increases in patients with cancerapproximately
3% per year as a groupand is substantially higher in those affected by colorectal and
ovarian cancer (10%28% and 20%50% per year, respectively).4,5 Breast cancer
and melanoma are the most common nonintra-abdominal cancers to cause bowel
obstruction, and this typically presents as diffuse peritoneal carcinomatosis.6,7
Obstruction can occur anywhere along the gastrointestinal tract. In some cases, this
represents the initial symptom of the underlying malignancy, whereas in others itdevelops during the course of disease. A recent consensus conference defined
a malignant bowel obstruction (MBO) as one of the following: clinical evidence of
bowel obstruction (by history, physical, and/or radiologic examination); bowel
obstruction beyond the ligament of Treitz, in the setting of a diagnosis of intra-abdom-
inal cancer with incurable disease; or a diagnosis of nonintra-abdominal primary
cancer with clear intraperitoneal disease.8 Many treatment options exist for these
patients, and because MBOs rarely need to be managed emergently,9 the treatment
team, patient, and family have time to discuss these decisions in the context of the
patients goals of care and underlying burden of disease.10
Obstruction is categorized as either partial or complete. In partial obstruction, gas orliquid stool can pass through the point of intestinal narrowing. With complete obstruc-
tion, no substance can pass. Such obstructions can be secondary to mechanical or
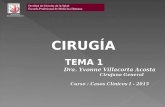
functional pathology. Mechanical obstructions are characterized as intraluminal
(enlarging primary or secondary tumor), intramural (infiltration of the bowel wall), or
extramural (extrinsic compression from masses, nodes, or adhesions) (Fig. 1). Func-
tional obstruction is characterized by an adynamic ileus. This can result from tumor
infiltration of the mesentery that affects the bowel wall muscle and nerves, or it can
be induced by the many pain medications used by this population. Ileus may also
result from a paraneoplastic neuropathy, particularly in patients with lung cancer.6
In the setting of a mechanical obstruction, distinction should be made betweensimple and closed-loop obstructions. Simple obstructions result when the intestinal
lumen is partially or completely occluded at one or more points, with resultant prox-
imal distention and distal decompression of the intestine. In contrast, closed-loop
obstructions result from two sequential occlusions. In a healthy population, this is typi-
cally a result of an incarcerated hernia or volvulus. These obstructions can rapidly
dilate and progress to strangulation and compromise the mesenteric vascular supply,
Table1
Clinical categories of immunocompromised patients
Group IMild-to-Moderate Group IISevere
Elderly
MalnourishedMalignancy
No chemotherapy
Transplant (high-dose steroids)
AIDS (CD41
-
8/2/2019 Abdomen Agudo Clinics
3/19
which results in ischemia. Strangulated closed-loop obstructions are surgical emer-
gencies. If left untreated, these types of obstructions can have mortality rates of
20% to 30%.1113
The following sections address etiologies that can precipitate malignant small- and
large-bowel obstructions. In each section, the authors have highlighted the underlying
pathophysiology, differences in patient presentations, and management options.
Small Bowel Obstruction
In Western countries, the most common causes of small-bowel obstruction (SBO) are
postsurgical adhesions (74%), Crohns disease (7%), and neoplasm (5%).14 Deter-
mining the etiology of postsurgical SBO in patients with cancer can be particularly
challenging. SBOs can be caused by intrinsic narrowing from the malignancy or
extrinsic compression of the bowel by tumor or adhesions. Once an obstruction is
present, intestinal secretions and swallowed air accumulate, resulting in dilation of
the proximal small bowel.15 This stretch stimulates additional secretory activity and
microvascular changes in the bowel wall, with resultant translocation of bacteria to
the mesenteric lymph nodes.
The most common presenting symptoms of SBO are abdominal cramps, nausea,vomiting, and abdominal distention. A source of continuous pain may point to the
location of the tumor, but patients may also have diffuse, nonlocalized signs.6 The
time course of symptoms, character of the emesis, and degree of distention also
provide helpful historical clues. For example, a rapid course, bilious emesis, and
minimal distention point toward a high-grade obstruction, whereas a more insidious
course, nonbilious emesis, and marked abdominal distension suggest a more distal
SBO or large-bowel obstruction (LBO).6,9 Passage of flatus or loose stools may
confound a history of obstruction as these can result from peristalsis above and below
the obstruction early on in the course of disease.
Although the history, clinical examination, and screening laboratory tests may behelpful in the management of SBO, imaging is the cornerstone of establishing the
definitive diagnosis. Imaging helps determine the level of obstruction, potential for
concurrent strangulation, and the need for immediate operative intervention.16,17
Plain radiographs using two views (flat and upright) have a sensitivity of 66% for
detecting an SBO,18 with low specificities affected by the inability of this modality
to distinguish between SBO and etiologies causing functional or mechanical
Obstruction
Mechanical Functional
-Intra-luminal
-Intra-mural
-Extra-mural
- Paraneoplastic neuropathy
Simple Closed-loop
-luminal occlusion -sequential occlusion
-incarcerated hernia
-volvulus
Fig.1.Categorizing a malignant bowel obstruction.
Cancer Emergencies: Acute Abdomen 383
-
8/2/2019 Abdomen Agudo Clinics
4/19
LBOs.16,18 Moreover, abdominal plain films, in conjunction with clinical and laboratory
findings, cannot reliably distinguish between a simple and strangulated obstruc-
tion.13,14,1922 Despite these limitations, these images can be rapidly obtained, per-
formed at the bedside, and can guide the early management and subsequent
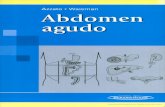
imaging. Images that show dilated gas or fluid-filled loops of small bowel with a gasless
colon are pathognomonic of SBO (Fig. 2).23 Additionally, the presence of air-fluid
differential height in the same small-bowel loop and a mean level width greater than
2.5 cm suggest a high-grade or complete SBO.14,24
Early studies of CT performed to assess for SBO found 90% to 96% sensitivity and
96% to 100% specificity.6,2527 Subsequent work questioned these results, with
substantially lower sensitivity (63%) and specificity (78%) when the study population
had a higher percentage of low-grade SBO.28 Further complicating this data, most of
these earlier studies were performed with mono-slice CT, in contrast to the multidetec-
tor machines currently in use. Despite these conflicting results, CT offers distinct advan-
tages over conventional radiography, especially in patients with underlying malignancy.
First, CT can determine the presence of a closed-loop obstruction and strangula-
tion.16,2937A negative predictive value of 89% 30,38 makes this a useful test for patients
in whom a conservative management strategy is planned.23,39 Second, multiplanar CT
can more accurately visualize adjacent anatomy, define the point of obstruction (the so-
called transition point), and identify intestinal pneumatosis. Lastly, recent evidence
suggests that a CT augmented with enteroclysisa process in which water-soluble
contrast is infused by way of a catheter into the duodenum or proximal small bowel
offers a greater sensitivity and specificity for partial obstructions (89% and 100%,
Fig. 2. Small bowel obstruction radiograph. (From MedicalFinals.co.uk. Available at: www.medicalfinals.co.uk. Accessed December 12, 2008; with permission.)
Ilgen & Marr384
http://www.medicalfinals.co.uk/http://www.medicalfinals.co.uk/http://www.medicalfinals.co.uk/http://www.medicalfinals.co.uk/http://www.medicalfinals.co.uk/http://www.medicalfinals.co.uk/http://www.medicalfinals.co.uk/ -
8/2/2019 Abdomen Agudo Clinics
5/19
respectively) and allows for greater differentiation between malignant and benign
causes of SBO.23
In past decades, amid concern for strangulation and the limited diagnostic yield of
abdominal radiographs, SBO was routinely managed operatively, following the adage
of never let the sun set or rise on an SBO.40 Management has evolved in the setting
of improved imaging modalities, and it is increasingly recognized that a conservative
approach employing fluid resuscitation and nasointestinal suction may obviate
surgery.39,41 This is encouraging for patients with MBOs, because surgical interven-
tions carry a high operative mortality (5%32%, often due to progression of disease),
involve high morbidity (42%), and are often unsuccessful, with reobstruction rates of
10% to 50%.19,4248 Conversely, among patients who develop a malignant SBO,
26% are because of underlying adhesions. In one series, this subgroup of patients
lived longer and had more effective relief when they were managed surgically.49
A conservative approach begins with nasointestinal decompression as a means to
relieve the small bowel of fluid accumulation. Typically, this is achieved by way of
a nasogastric tube. Some investigators believe that more effective decompression
can be achieved if the tube is advanced beyond the pylorus, which may result in better
outcomes.15,50 Placement of these long intestinal tubes is more challenging than the
typically used Salem sump nasogastric tube (Sherwood Medical, St Louis, MO, USA)
and requires fluoroscopy, which may limit their widespread application in the ED.51
In the context of a nonsurgical management plan, pharmacotherapy may be a useful
adjunct to bowel rest. Somatostatin analogs (octreotide) and anticholinergic agents
(scopolamine) have been employed to reduce gastrointestinal secretions and lengthen
small bowel transit time, with marked symptomatic relief and resolution of symp-
toms.5256
Because octreotide has been shown to dramatically reduce the rate ofnausea and vomiting with few side effects, and because complete relief of these
symptoms is rare with typical antiemetics, some authors advocate the early use of
this agent.10 The dose of octreotide used to manage MBO in small case series has
ranged from 0.1 to 1.2 mg/d, administered by either a continuous or bolus subcuta-
neous infusion.6 Corticosteroids have not been shown to definitely affect the relief
of MBOs, although they can act to treat obstruction-related pain.44 Corticosteroids
should thus be reserved for patients in the terminal stages of their disease and be
administered after consultation with the oncologist.10
Because of high mortality rates associated with nonsurgical care, the diagnosis of
a closed-loop obstruction or strangulation should prompt the consideration of imme-diate surgical intervention. Additionally, if conservative management of a simple SBO
fails, surgery may become a necessary next step. Laparoscopic adhesion lysis has
grown in popularity as a minimally invasive technique to relieve SBO, with success rates
of 40% to 70% in the general population.16 In patients with malignant SBO, CT imaging
may be helpful to define the etiology of obstruction (tumor vs adhesions) and to map
the location and type of adhesions.16 This may ultimately dictate whether a surgical
approach is at all possible, and if so, whether the lesions are amenable to laparoscopic
reduction. Palliative procedures such as ostomies, stenting, debulking, and intraperito-
neal chemotherapy may also be considered.10
Large Bowel Obstruction
LBOs are much less common than SBO. However, when they are encountered, their
most common cause is an underlying malignancy.57 Other etiologies include divertic-
ulitis and volvulus of the sigmoid colon or cecum. In the setting of a malignant LBO, the
cause is typically an intraluminal tumor growth, but it can also be the result of intussus-
ception (discussed in a later section). Up to 20% of patients with colorectal cancer
Cancer Emergencies: Acute Abdomen 385
-
8/2/2019 Abdomen Agudo Clinics
6/19
develop an LBO, which can have a substantial morbidity and mortality. Postopera-
tively, up to 25% of patients with a colorectal cancer resection develop an LBO.5861
Similar to SBO, mechanical obstruction of the large bowel causes bowel dilatation
above the site of obstruction. This precipitates mucosal edema, impaired vascular
flow to the bowel wall, increased mucosal permeability, and subsequent bacterial
translocation. A nonpatent ileocecal valve can create a second anatomic barrier,
thus setting the stage for a closed-loop obstruction. It is essential for the practitioner
to distinguish between LBO and non-obstructive causes of large bowel dilation, such
as a toxic megacolon. The latter refers to dilation of the colon associated with acute
colitis, either segmental or diffuse, without associated obstruction. A wide range of
etiologies can result in acute colitis: inflammation, ischemia, infection, or radiation.
Symptoms of LBO typically follow an indolent course, with progression over several
days. Initially, lower abdominal or diffuse colicky pain is accompanied by abdominal
distention and changes in bowel habits (stool caliber changes or obstipation). De-
pending on the patency of the ileocecal valve, these symptoms can eventually prog-
ress to nausea and vomiting.62 Rarely, this emesis is feculent, a result of bacterial
overgrowth in the stagnant fluid proximal to the obstruction.62 Evidence of systemic
symptoms, such as fever or tachycardia, and laboratory abnormalities, such as a white
blood cell count over 20,000/mm3, may suggest the presence of a gangrenous bowel
or perforation.57 However, immunocompromised patients may continue to have unim-
pressive abdominal examinations, even in the presence of these abdominal
catastrophes.
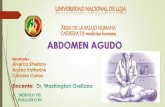
Abdominal radiographs, when performed for evaluation of LBO, have a sensitivity
and specificity of 84% and 72%, respectively (Fig. 3).63 In patients who are mobile,
the addition of a contrast enema plain radiograph improves the sensitivity (96%)and specificity (98%) of this study to detect a mechanical obstruction.63 These studies
do not, however, evaluate the viability of the proximal bowel, determine the extent of
the primary malignancy or distant metastases, or significantly affect subsequent
procedural planning.58
Fig. 3. Large bowel obstruction radiograph. (From Ho V, Lee YC. Acute colonic pseudo-obstruction in an elderly alcoholic man. Internet J Gastroenterol 2007;5(2); with permission.)
Ilgen & Marr386
-
8/2/2019 Abdomen Agudo Clinics
7/19
Early studies using CT to detect LBO found that it was able to confirm the diagnosis
in over 90% of cases, with one study citing a sensitivity of 96% and specificity of
93%.64,65 This same study found an improved diagnostic accuracy, sensitivity, and
negative predictive value of CT when compared to the contrast enema outlined
earlier.64 The use of multidetector CT, with improved spatial resolution and multiplanar
images, likely improves its diagnostic accuracy for LBO, although evidence to support
this is scarce.58,66 CT also enables the clinician to accurately exclude closed-loop
obstructions or strangulation, evaluate for the nonobstructive causes of colonic dila-
tion outlined earlier, and assess for nonmalignant causes of LBO such as volvulus
and diverticulitis.
Once identified, malignant LBOs necessitate prompt intervention. Historically, this
has involved operative management, with approximately 85% of emergency large
bowel surgery performed to relieve malignant LBO.67 These obstructions can be
addressed by either a palliative stoma or a rectosigmoid resection with accompanying
colostomy, although these operations portend frequent complications and high
mortality rates (8.8%27%).59,61,6871 Recent advances in endoscopy have estab-
lished a role for colonic stenting in the management of malignant LBO, either as a palli-
ative measure or as a bridge toward definitive operative management in patients with
resectable disease.68,72 Stenting carries the risk of perforation (3%4%), migration
(10%11%), and reobstruction (7%10%).58,73 A meta-analysis that compared oper-
ative versus endoscopic management of malignant LBO found that colonic stents
were associated with significant reductions in length of hospital stay, mortality rate,
eventual need for a palliative stoma, and medical complications.68 Moreover, mortality
rates were similar between patients who underwent emergency surgery and those
who were stented in anticipation of an elective bowel resection, although there wassubstantial heterogeneity among the two groups.68 A prospective trial that compares
these two interventions is ongoing (http://www.crstrial.com).
Gastric Outlet Obstruction
Gastric outlet obstruction (GOO) results from an underlying malignancy in 63% of
cases.4,74 Typically, cancer involving organs of the lesser sac results in intrinsic or
extrinsic obstruction of the adjacent pyloric channel or duodenum. This obstruction
may result from a combination of local infiltration, edema, and adhesions. The symp-
toms of GOO may be intermittent until occlusion is complete. Pancreatic cancer is the
most common malignancy to cause GOO (10%20%). Other etiologies that causeGOO include ampullary cancer, duodenal cancer, cholangiocarcinoma, gastric
cancer, and metastases to the gastric outlet from lung and breast cancer.6,75
Early symptoms of GOO may include gastroesophageal reflux, early satiety, and
weight loss. Eventually, patients progress to nausea and vomiting, usually nonbilious
with undigested food particles, along with abdominal pain and distention. Although
nausea and vomiting are frequent complaints in patients with any underlying malig-
nancy, especially in the context of ongoing chemotherapy, this sequence of symp-
toms should also prompt consideration of GOO.
Although it is difficult to definitively establish the diagnosis of GOO in the ED,
patients can be managed symptomatically with fluid resuscitation and gastric decom-pression. Gastrojejunostomy remains the definitive surgical treatment of choice,
although self-expandable metallic stents have become a viable nonsurgical alterna-
tive, with relief of obstruction in more than 90% of cases.7679 Studies that compare
these two interventions have shown equivalent survival rates, although patients who
received endoscopic stents had shorter hospital stays, lower costs, and an improved
ability to consume food orally.6,80 Patients managed surgically, however, had
Cancer Emergencies: Acute Abdomen 387
http://www.crstrial.com/http://www.crstrial.com/http://www.crstrial.com/ -
8/2/2019 Abdomen Agudo Clinics
8/19
a reduced need for reintervention, a result attributed to delayed stent occlusion.81,82
As an additional option, gastric venting can be achieved by way of a percutaneously
placed gastrostomy tube.6
Malignant IntussusceptionIntussusception occurs in all age groups, but is primarily a disease of infancy and early
childhood. Overall, only 5% of intussusceptions occur in adults, and intussusceptions
account for approximately1% to 5% of adult SBOs.83,84 Childhood causes tend to be
idiopathic, whereas a mechanical cause is present in more than 90% of adult cases.
Solid tumors, benign and malignant, act as the lead point in over 65% of adult
cases.83,85 Intussusception results when a segment of bowel lumen that either
contains a mass lesion or has altered peristaltic activity telescopes into an adjacent
segment. This results in obstruction and ischemic injury to the intussuscepting
segment.84 A neoplastic mass must be strongly considered in children older than
4 years and adults who present with intussusception.
Patients with intussusception have acute, subacute, or chronic nonspecific symp-
toms. In small studies, the most common complaint reported is intermittent abdominal
cramping (79%), followed by obstructive signs, such as nausea, vomiting, and
abdominal distention.83,84 Plain radiographic evaluation of the abdomen is similarly
nonspecific. The abdominal radiograph may suggest partial or complete bowel
obstruction, although occasionally a soft-tissue density outlined by two strips of air
may be seen.83,84,86 The use of CT in adults has been recently advocated to better
differentiate an associated mass and rule out other etiologies. Characteristic imaging
findings include the target sign or sausage-shaped appearance.83,85 Manage-
ment of adult intussusceptions is dictated by their location. Pure colonic intussuscep-
tions are typically resected because of their high malignant potential, whereas ileocolic
lesions may be approached with intraoperative colonoscopy to identify the lesion
before intervention and potentially avoid resection.84,86
PERFORATION
MBOs, transmural erosion of primary gastrointestinal cancers, metastatic lesions to
the gut, and atypical infections have the potential to cause bowel perforation and peri-
tonitis. The clinical severity of these perforations and therapeutic options for treatmentare affected by the location, involvement of adjacent structures, and the time to
patient presentation. Intra-abdominal perforations are categorized as either free,
when bowel contents are spilled into the abdominal cavity, or contained, if contiguous
organs wall off the area. In an immunocompromised population, over 90% of colonic
perforations result in pneumoperitoneum because of these patients inability to
localize infection and the late onset of presentation.2
The differential for peritonitis in this population is shaped by the patients underlying
malignancy and degree of immunosuppression. Common causes of colonic perfora-
tions in immunocompromised patients include diverticular disease, ischemic colitis,
fecal impaction, neutropenic enterocolitis, and opportunistic infections such as cyto-megalovirus (CMV) andCandida.2,87,88 Perforations secondary to CMV have also been
found in the ileum and jejunum among patients undergoing chemotherapy.8992
CT has the ability to demonstrate small amounts of free air, pneumatosis intestinalis,
portal venous air, and the site of intestinal obstruction.2,93 Once perforation is estab-
lished, broad-spectrum antibiotics along with rapid surgical consultation should be
initiated with likely operative management.
Ilgen & Marr388
-
8/2/2019 Abdomen Agudo Clinics
9/19
PATHOLOGY UNIQUE TO PROFOUND IMMUNOSUPPRESSION
All patients with an underlying malignancy who present to the ED should be consid-
ered immunosuppressed. The degree to which this immunosuppression affects their
clinical presentation is dependent upon whether they recently received chemo-
therapy, their current absolute neutrophil count, and associated medical problems.Patients that are categorized as severely immunosuppressed (see group II in Table 1)
require a special consideration of unique diagnoses. The most common cause of an
acute abdomen in neutropenic patients, neutropenic enterocolitis, is discussed in
detail elsewhere in this issue. Additional pathologies are outlined in Table 2.
Neutropenic Enterocolitis
Neutropenic enterocolitis, or typhlitis, is a necrotizing inflammation of the cecum that
is found almost exclusively in patients who are immunocompromised. This entity hasreceived a multitude of names: neutropenic colitis, necrotizing enterocolitis, ileocecal
syndrome, and cecitis.9496 The incidence of this disease among adults varies widely
in the literature (0.8%26%), likely due to the heterogeneity of the diagnostic criteria.97
When identified, this diagnosis carries a mortality rate of 50% and higher.97103Among
patients with solid or hematologic malignancies, typhlitis typically manifests in the
setting of chemotherapy-induced neutropenia or bone-marrow transplantation, and
it has emerged as the most common cause of the acute abdomen in the neutropenic
cancer patient.2 Case reports also cite neutropenic enterocolitis as a presenting
symptom in patients with acute myelogenous and acute lymphoblastic leukemia,
before the onset of chemotherapy.104109 Moreover, it has also been described inpatients with AIDS, as well as patients who require immunosuppression after organ
transplantation.110,111 Despite its name, patients can develop neutropenic enteroco-
litis in the absence of neutropenia.112114
The etiology and pathogenesis of this syndrome remain poorly understood. It has
been postulated that the disease is caused by the inability to maintain an intact intes-
tinal mucosa. This lack of mucosal integrity likely results from a combination of neutro-
penia, impaired host defenses, and direct injury from chemotherapeutic agents.111
Table 2
Additional presentations unique to underlying malignancy or immunocompromise
Disease State Manifestations
CMV GI tract mucosal ulcers (mouth to rectum),commonly with secondary bleeding thatcan progress to perforation.
Varicella (diffuse & primary) Acute abdomen can occur withoutcutaneous findings. Typically in stem-celltransplant patient, associated withhyponatremia secondary to SIADH. Treated
with acyclovir and IVIG.GVHD Skin (rash/dermatitis), liver (hepatitis/
jaundice), GI tract (abdominal pain/diarrhea). Findings can occur together orin isolation.
Abbreviations: GI, gastrointestinal; GVHD, graft-versus-host disease; IVIG, intravenous immuneglobulin; SIADH, syndrome of inappropriate antidiuretic hormone.
Cancer Emergencies: Acute Abdomen 389
-
8/2/2019 Abdomen Agudo Clinics
10/19
Transmucosal migration of bacteria causes systemic bacteremia, endotoxin
production, mucosal or transmural necrosis, and focal hemorrhage.94,110
There is considerable variation in presentation among patients with neutropenic
enterocolitis. The most common symptoms are fever, right lower quadrant abdominal
pain, nausea, and vomiting. Computed tomography is the imaging modality of choice
because this constellation of complaints poses a fairly wide differential. Ultrasound
and abdominal plain films may provide clues to this diagnosis, but have higher false
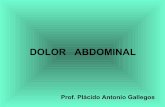
negative rates.115 Typical CT findings (Fig. 4) include circumferential cecal wall thick-
ening; dilated, fluid-filled cecum; and adjacent mesenteric fat stranding.94 The degree
of bowel-wall thickening may correlate with prognosis, with one retrospective study
showing a mortality of 60% if the bowel wall was 10 mm or more by ultrasound,
and only 4.2% if 10 mm or less.116 Focal findings of high attenuation in the cecal
wall may represent hemorrhage.
Neutropenic enterocolitis is an uncommon diagnosis, and there are no randomized
prospective trials to guide management. Most authors advocate broad-spectrum
antibiotics, bowel rest, aggressive nutritional supplementation, and correction of
underlying cytopenias and coagulopathies.94,104 If the patient is neutropenic, admin-
istration of granulocyte colony-stimulating factor may provide benefit. A more detailed
review of neutropenic enterocolitis is presented elsewhere in this issue.
ETIOLOGIES UNIQUE TO PATIENTS WITH CANCER
Malignant Ascites
Malignant ascites is defined as the collection of fluid containing cancerous cells in the
abdomen. Malignant ascites can occur from direct invasion of the peritoneum (perito-
neal carcinomatosis), or as a result of venous or lymphatic obstruction.117 Ovariancancer is the most common malignancy to cause ascites, occurring in 37% of all re-
ported cases. Because of this, malignant ascites is twice as likely in females as males
(67% vs 33%).118,119 Additional malignancies complicated by ascites include, but are
not limited to, pancreaticobiliary, gastric, esophageal, and colorectal cancers. The
pathophysiology of ascitic fluid accumulation is multifactorial and may result from
venous and lymphatic obstruction, oncotic shifts, or enhanced vascular permeability
as a result of diffuse cytokine release.120
Patients with malignant ascites can present with abdominal distention, pain, dysp-
nea, nausea, anorexia, and vomiting. In more than 50% of patients ultimately
Fig. 4. Computed tomography image of neutropenic enterocolitis. (From Lodhawala T,Shaikh A, Carmosino L. Gastroenterology photo quiz. Resid Staff Physician 2007;53(1),with permission.)
Ilgen & Marr390
-
8/2/2019 Abdomen Agudo Clinics
11/19
diagnosed with malignant ascites, this fluid accumulation caused the first presenting
signs and symptoms of their underlying malignancy.118 Because of the many potential
etiologies that can cause ascites, paracentesis is necessary to establish a malignant
source. In these cases, cytology is diagnostic in 50% to 60% of cases, with sensitiv-
ities of 58% to 75%.117,118
Management strategies for malignant ascites are directed toward symptomatic
relief, similar to the treatment of patients with nonmalignant ascites. Initial interven-
tions include diuretics and therapeutic paracentesis.118 When these measures are
unsuccessful, a peritoneal drain can be placed, with relief in 83% to 100% of
cases.120,121 A peritoneovenous shunt (PVS) incorporates 1-way valves allowing
flow from the peritoneum to the vena cava and is a more invasive alternative to the ex-
traperitoneal drain. Although there is little data to compare these two interventions,
PVS has been shown to have a higher rate of patency at 72 days.118 There is a theo-
retical risk of disseminated intravascular coagulation in patients with PVS, because of
shunting of cancerous cells into the vena cava.118
Patients with malignant ascites are at risk for spontaneous bacterial peritonitis,
although this risk is believed to be lower than in patients with nephrotic or cirrhotic
ascites.122 That said, because of the concurrent immunosuppression, physicians
should have a low threshold to perform diagnostic paracenteses as part of their infec-
tious work-up. To address the malignant ascites itself, palliative intraperitoneal
chemotherapy can be considered.121,123
Radiation Enteritis
Radiation enteritis occurs in patients receiving irradiation of the abdomen or pelvis
during the course of their cancer treatment. The disease is characterized by diffusecollagen deposition and progressive occlusive vasculitis that results in local narrowing
of the intestinal lumen.124 These microvascular changes result in bowel dilation prox-
imal to affected segments and mucosal damage, with secondary effects of bowel
ulceration, perforation, and massive gastrointestinal bleeding.125,126 Pelvic irradiation,
where the greatest volume of bowel is affected, is predominantly used in the treatment
of gynecologic and urologic cancers. A recent United Kingdom study cited a 50% inci-
dence of radiation-induced bowel damage among their cohort of 12,000 patients with
pelvic cancer. Although only 4% to 8% of these patients had life-threatening compli-
cations, as many as 80% were chronically affected by malnutrition, fistula formation,
and strictures.126,127
The small bowel is particularly susceptible to radiation enteritis, especially at doses
greater than 45 Gy.124 The most important factors to prevent both acute and chronic
radiation-induced injury are the reduction of dose and field size.125,128 Once radiation
enteritis is diagnosed, medical therapy can include 5-aminosalicylate, octreotide, and
the administration of probiotics. These measures have been shown to be most effec-
tive in the acute phase. Unfortunately, few pharmacologic choices for chronic radia-
tion enteritis have shown an established benefit.126,128 Ongoing research is
evaluating cytokine levels as a means to predict which patients are most susceptible
to radiation enteritis, manipulation of growth factors in formation of fibrotic tissue, and
dietary supplementation.124,126,128
Budd-Chiari Syndrome
The Budd-Chiari syndrome (BCS) describes the clinical manifestations of hepatic
venous outflow obstruction at the level of the hepatic venules, large hepatic veins,
inferior vena cava, or right atrium.129131 These obstructive thromboses occur most
frequently in the setting of an underlying hypercoagulable state and in rare cases
Cancer Emergencies: Acute Abdomen 391
-
8/2/2019 Abdomen Agudo Clinics
12/19
can result from tumor invasion. The malignancies that most frequently precipitate BCS
are hepatocellular, renal-cell, and adrenal carcinoma.130 The resultant venous stasis
and hepatic congestion cause hypoxic parenchymal cell injury, centrilobular necrosis,
and eventual cirrhosis.130 Unless hepatic congestion is relieved, obstruction prog-
resses to liver failure and death.132
Typical symptoms of the Budd-Chiari syndrome include ascites, hepatomegaly, and
abdominal pain, with some cases progressing to jaundice, portal hypertension, and
variceal bleeding.131 Coagulopathy, encephalopathy, and development of the hepa-
torenal syndrome all indicate a poor prognosis.130 The diagnosis can be established
using ultrasound, CT, or MRI. If advanced imaging is inconclusive, a liver biopsy
may be necessary.133,134 The sensitivity of Doppler ultrasonography for diagnosing
BCS is 85% to 90%, and this should be the initial imaging technique performed
when this diagnosis is entertained.135,136 Ultrasonography findings in BCS include
nonvisualization of hepatic veins, absence of flow in the hepatic vein, stenosis of
or thrombosis within the hepatic veins, intrahepatic collaterals, and obstruction of
the infrahepatic inferior vena cava.135 CT and MRI offer the advantages of better
identification of necrotic areas of the liver and improved detail of liver perfusion.135
For relatively asymptomatic patients with BCS who have normal liver function tests,
medical therapy with sodium restriction, diuretics, anticoagulation, and intermittent
paracenteses can constitute the initial management strategy. In the setting of hepato-
cellular necrosis, however, patients need either surgical or percutaneous portosyste-
mic shunting (mesoatrial, mesocaval, transjugular intrahepatic portosystemic shunting
or hepatic vein angioplasty).132,137 Both treatments are typically followed by lifelong
systemic anticoagulation.132 Fulminant or refractory cases of Budd-Chiari syndrome
may require liver transplantation.
SUMMARY
Gastrointestinal complaints among patients with cancer can pose a diagnostic
dilemma with significant rates of morbidity and mortality. Mass lesions or adhesions
related to intra-abdominal malignancies place these patients at higher risk for bowel
obstruction or perforation, while ongoing chemotherapy or functional immunosup-
pression can mask many of the findings among healthy patients. This affects the
timing of patients presentation and their clinical examination in the ED. Moreover,
in the setting of profound immunosuppression, a wide range of atypical infections
and pathologies must be considered. Clinical vigilance by the practitioner is thus
essential, with a low threshold to use advanced imaging modalities and careful
consideration of this expanded differential.
REFERENCES
1. Swenson KK, Rose MA, Ritz L, et al. Recognition and evaluation of oncology-
related symptoms in the emergency department. Ann Emerg Med 1995;26(1):
127.
2. Scott-Conner CE, Fabrega AJ. Gastrointestinal problems in the immunocompro-
mised host. A review for surgeons. Surg Endosc 1996;10(10):95964.3. Cappell MS, Batke M. Mechanical obstruction of the small bowel and colon. Med
Clin North Am 2008;92(3):57597, viii.
4. Hirst B, Regnard C. Management of intestinal obstruction in malignant disease.
Clin Med 2003;3(4):3114.
5. Ripamonti C, Bruera E. Palliative management of malignant bowel obstruction.
Int J Gynecol Cancer 2002;12(2):13543.
Ilgen & Marr392
-
8/2/2019 Abdomen Agudo Clinics
13/19
6. Ripamonti CI, Easson AM, Gerdes H. Management of malignant bowel obstruc-
tion. Eur J Cancer 2008;44(8):110515.
7. Krouse RS. The international conference on malignant bowel obstruction:
a meeting of the minds to advance palliative care research. J Pain Symptom
Manage 2007;34(Suppl 1):S16.
8. Anthony T, Baron T, Mercadante S, et al. Report of the clinical protocol
committee: development of randomized trials for malignant bowel obstruction.
J Pain Symptom Manage 2007;34(Suppl 1):S4959.
9. Rubin SC. Intestinal obstruction in advanced ovarian cancer: what does the
patient want? Gynecol Oncol 1999;75(3):3112.
10. Krouse RS, McCahill LE, Easson AM, et al. When the sun can set on an unoper-
ated bowel obstruction: management of malignant bowel obstruction. J Am Coll
Surg 2002;195(1):11728.
11. Dixon JA, Nichols RL, Hunter DC Jr. Strangulation obstruction of the intestine.
early detection. Arch Surg 1964;88:52732.
12. Saltzstein EC, Marshall WJ, Freeark RJ. Gangrenous intestinal obstruction. Surg
Gynecol Obstet 1962;114:694700.
13. Leffall LD, Syphax B. Clinical aids in strangulation intestinal obstruction. Am
J Surg 1970;120(6):7569.
14. Miller G, Boman J, Shrier I, et al. Etiology of small bowel obstruction. Am J Surg
2000;180(1):336.
15. Paine JR. The hydro-dynamics of the relief of distention in the gastrointestinal
tract by suction applied to inlaying catheters. Arch Surg 1936;33:9951020.
16. Maglinte DD, Kelvin FM, Sandrasegaran K, et al. Radiology of small bowel
obstruction: contemporary approach and controversies. Abdom Imaging2005;30(2):16078.
17. Herlinger H, Maglinte DDT. Small bowel obstruction. Philadelphia: W.B. Sauders;
1989.
18. Shrake PD, Rex DK, Lappas JC, et al. Radiographic evaluation of suspected
small bowel obstruction. Am J Gastroenterol 1991;86(2):1758.
19. Sarr MG, Bulkley GB, Zuidema GD. Preoperative recognition of intestinal stran-
gulation obstruction. Prospective evaluation of diagnostic capability. Am J Surg
1983;145(1):17682.
20. Hofstetter SR. Acute adhesive obstruction of the small intestine. Surg Gynecol
Obstet 1981;152(2):1414.21. Barnett WO, Petro AB, Williamson JW. A current appraisal of problems with
gangrenous bowel. Ann Surg 1976;183(6):6539.
22. Laws HL, Aldrete JS. Small-bowel obstruction: a review of 465 cases. Southampt
Med J 1976;69(6):7334.
23. Maglinte DD, Heitkamp DE, Howard TJ, et al. Current concepts in imaging of
small bowel obstruction. Radiol Clin North Am 2003;41(2):26383, vi.
24. Langell JT, Mulvihill SJ. Gastrointestinal perforation and the acute abdomen.
Med Clin North Am 2008;92(3):599625, viiiix.
25. Megibow AJ, Balthazar EJ, Cho KC, et al. Bowel obstruction: evaluation with CT.
Radiology 1991;180(2):3138.26. Fukuya T, Hawes DR, Lu CC, et al. CT diagnosis of small-bowel obstruction: effi-
cacy in 60 patients. AJR Am J Roentgenol 1992;158(4):7659 [discussion: 7712].
27. Balthazar EJ. George W. Holmes Lecture. CT of small-bowel obstruction. AJR
Am J Roentgenol 1994;162(2):25561.
28. Maglinte DD, Gage SN, Harmon BH, et al. Obstruction of the small intestine:
accuracy and role of CT in diagnosis. Radiology 1993;188(1):614.
Cancer Emergencies: Acute Abdomen 393
-
8/2/2019 Abdomen Agudo Clinics
14/19
29. Taourel PG, Fabre JM, Pradel JA, et al. Value of CT in the diagnosis and
management of patients with suspected acute small-bowel obstruction. AJR
Am J Roentgenol 1995;165(5):118792.
30. Balthazar EJ, Birnbaum BA, Megibow AJ, et al. Closed-loop and strangulating
intestinal obstruction: CT signs. Radiology 1992;185(3):76975.
31. Balthazar EJ, Bauman JS, Megibow AJ. CT diagnosis of closed loop obstruction.
J Comput Assist Tomogr 1985;9(5):9535.
32. Cho KC, Hoffman-Tretin JC, Alterman DD. Closed-loop obstruction of the small
bowel: CT and sonographic appearance. J Comput Assist Tomogr 1989;13(2):
2568.
33. Fisher JK. Computed tomographic diagnosis of volvulus in intestinal malrotation.
Radiology 1981;140(1):1456.
34. Frager D, Baer JW, Medwid SW, et al. Detection of intestinal ischemia in patients
with acute small-bowel obstruction due to adhesions or hernia: efficacy of CT.
AJR Am J Roentgenol 1996;166(1):6771.
35. Ha HK, Park CH, Kim SK, et al. CT analysis of intestinal obstruction due to adhe-
sions: early detection of strangulation. J Comput Assist Tomogr 1993;17(3):
3869.
36. Jaramillo D, Raval B. CT diagnosis of primary small-bowel volvulus. AJR Am
J Roentgenol 1986;147(5):9412.
37. Shaff MI, Himmelfarb E, Sacks GA, et al. The whirl sign: a CT finding in volvulus
of the large bowel. J Comput Assist Tomogr 1985;9(2):410.
38. Gazelle GS, Goldberg MA, Wittenberg J, et al. Efficacy of CT in distinguishing
small-bowel obstruction from other causes of small-bowel dilatation. AJR Am
J Roentgenol 1994;162(1):437.39. Seror D, Feigin E, Szold A, et al. How conservatively can postoperative small
bowel obstruction be treated? Am J Surg 1993;165(1):1215 [discussion:
1256].
40. Miller G, Boman J, Shrier I, et al. Natural history of patients with adhesive small
bowel obstruction. Br J Surg 2000;87(9):12407.
41. Brolin RE, Krasna MJ, Mast BA. Use of tubes and radiographs in the manage-
ment of small bowel obstruction. Ann Surg 1987;206(2):12633.
42. Legendre H, Vanhuyse F, Caroli-Bosc FX, et al. Survival and quality of life after
palliative surgery for neoplastic gastrointestinal obstruction. Eur J Surg Oncol
2001;27(4):3647.43. Makela J, Kiviniemi H, Laitinen S, et al. Surgical management of intestinal
obstruction after treatment for cancer. Case reports. Eur J Surg 1991;157(1):
737.
44. Feuer DJ, Broadley KE, Shepherd JH, et al. Systematic review of surgery in
malignant bowel obstruction in advanced gynecological and gastrointestinal
cancer. The Systematic Review Steering Committee. Gynecol Oncol 1999;
75(3):31322.
45. Turner DM, Croom RD III. Acute adhesive obstruction of the small intestine. Am
Surg 1983;49(3):12630.
46. Stewart RM, Page CP, Brender J, et al. The incidence and risk of early postop-erative small bowel obstruction. A cohort study. Am J Surg 1987;154(6):6437.
47. Ellis CN, Boggs HW Jr, Slagle GW, et al. Small bowel obstruction after colon
resection for benign and malignant diseases. Dis Colon Rectum 1991;34(5):
36771.
48. van Ooijen B, van der Burg ME, Planting AS, et al. Surgical treatment or gastric
drainage only for intestinal obstruction in patients with carcinoma of the ovary or
Ilgen & Marr394
-
8/2/2019 Abdomen Agudo Clinics
15/19
peritoneal carcinomatosis of other origin. Surg Gynecol Obstet 1993;176(5):
46974.
49. Gallick HL, Weaver DW, Sachs RJ, et al. Intestinal obstruction in cancer patients.
An assessment of risk factors and outcome. Am Surg 1986;52(8):4347.
50. Pickleman J, Lee RM. The management of patients with suspected early post-
operative small bowel obstruction. Ann Surg 1989;210(2):2169.
51. Maglinte DD, Stevens LH, Hall RC, et al. Dual-purpose tube for enteroclysis and
nasogastric-nasoenteric decompression. Radiology 1992;185(1):2812.
52. Pandha HS, Waxman J. Octreotide in malignant intestinal obstruction. Anti-
cancer Drugs 1996;1(Suppl 7):510.
53. Ripamonti C, Mercadante S, Groff L, et al. Role of octreotide, scopolamine bu-
tylbromide, and hydration in symptom control of patients with inoperable bowel
obstruction and nasogastric tubes: a prospective randomized trial. J Pain
Symptom Manage 2000;19(1):2334.
54. Khoo D, Hall E, Motson R, et al. Palliation of malignant intestinal obstruction
using octreotide. Eur J Cancer 1994;30A(1):2830.
55. Mangili G, Franchi M, Mariani A, et al. Octreotide in the management of bowel
obstruction in terminal ovarian cancer. Gynecol Oncol 1996;61(3):3458.
56. Mercadante S, Spoldi E, Caraceni A, et al. Octreotide in relieving gastrointestinal
symptoms due to bowel obstruction. Palliat Med 1993;7(4):2959.
57. Peterson MA. Large intestine. In: Marx JA, Hockberger RS, Walls RM, et al,
editors. Rosens emergency medicine: concepts and clinical practice. 5th
edition. Mosby/Elsevier; Philadelphia: 2006. p. 13324.
58. Finan PJ, Campbell S, Verma R, et al. The management of malignant large
bowel obstruction: ACPGBI position statement. Colorectal Dis 2007;4(Suppl9):117.
59. Phillips RK, Hittinger R, Fry JS, et al. Malignant large bowel obstruction.
Br J Surg 1985;72(4):296302.
60. Carraro PG, Segala M, Cesana BM, et al. Obstructing colonic cancer: failure and
survival patterns over a ten-year follow-up after one-stage curative surgery. Dis
Colon Rectum 2001;44(2):24350.
61. Tekkis PP, Kinsman R, Thompson MR, et al. The Association of Coloproctology of
Great Britain and Ireland study of large bowel obstruction caused by colorectal
cancer. Ann Surg 2004;240(1):7681.
62. Lopez-Kostner F, Hool GR, Lavery IC. Management and causes of acute large-bowel obstruction. Surg Clin North Am 1997;77(6):126590.
63. Chapman AH, McNamara M, Porter G. The acute contrast enema in suspected
large bowel obstruction: value and technique. Clin Radiol 1992;46(4):2738.
64. Frager D, Rovno HD, Baer JW, et al. Prospective evaluation of colonic obstruc-
tion with computed tomography. Abdom Imaging 1998;23(2):1416.
65. Megibow AJ. Bowel obstruction. Evaluation with CT. Radiol Clin North Am 1994;
32(5):86170.
66. Sinha R, Verma R. Multidetector row computed tomography in bowel obstruc-
tion. Part 1. Small bowel obstruction. Clin Radiol 2005;60(10):105867.
67. Baron TH, Kozarek RA. Endoscopic stenting of colonic tumours. Best Pract ResClin Gastroenterol 2004;18(1):20929.
68. Tilney HS, Lovegrove RE, Purkayastha S, et al. Comparison of colonic stenting
and open surgery for malignant large bowel obstruction. Surg Endosc 2007;
21(2):22533.
69. Valerio D, Jones PF. Immediate resection in the treatment of large bowel emer-
gencies. Br J Surg 1978;65(10):7126.
Cancer Emergencies: Acute Abdomen 395
-
8/2/2019 Abdomen Agudo Clinics
16/19
70. Serpell JW, McDermott FT, Katrivessis H, et al. Obstructing carcinomas of the
colon. Br J Surg 1989;76(9):9659.
71. Buechter KJ, Boustany C, Caillouette R, et al. Surgical management of the
acutely obstructed colon. A review of 127 cases. Am J Surg 1988;156(3 Pt 1):
1638.
72. Harris GJ, Senagore AJ, Lavery IC, et al. The management of neoplastic colo-
rectal obstruction with colonic endolumenal stenting devices. Am J Surg 2001;
181(6):499506.
73. Khot UP, Lang AW, Murali K, et al. Systematic review of the efficacy and safety of
colorectal stents. Br J Surg 2002;89(9):1096102.
74. Tintinalli JE, Kelen GD, Stapczynski JS, et al. Emergency medicine: a compre-
hensive study guide. 5th edition. New York: McGraw-Hill, Health Professions
Division; 2000.
75. Hassan C, Zullo A, Risio M, et al. Histologic risk factors and clinical outcome in
colorectal malignant polyp: a pooled-data analysis. Dis Colon Rectum 2005;
48(8):158896.
76. Lowe AS, Beckett CG, Jowett S, et al. Self-expandable metal stent placement for
the palliation of malignant gastroduodenal obstruction: experience in a large,
single, UK centre. Clin Radiol 2007;62(8):73844.
77. Telford JJ, Carr-Locke DL, Baron TH, et al. Palliation of patients with malignant
gastric outlet obstruction with the enteral Wallstent: outcomes from a multicenter
study. Gastrointest Endosc 2004;60(6):91620.
78. Dormann A, Meisner S, Verin N, et al. Self-expanding metal stents for gastrodu-
odenal malignancies: systematic review of their clinical effectiveness. Endos-
copy 2004;36(6):54350.79. Nassif T, Prat F, Meduri B, et al. Endoscopic palliation of malignant gastric outlet
obstruction using self-expandable metallic stents: results of a multicenter study.
Endoscopy 2003;35(6):4839.
80. Espinel J, Sanz O, Vivas S, et al. Malignant gastrointestinal obstruction: endo-
scopic stenting versus surgical palliation. Surg Endosc 2006;20(7):10837.
81. Jeurnink SM, Steyerberg EW, Hof G, et al. Gastrojejunostomy versus stent place-
ment in patients with malignant gastric outlet obstruction: a comparison in 95
patients. J Surg Oncol 2007;96(5):38996.
82. Wong YT, Brams DM, Munson L, et al. Gastric outlet obstruction secondary to
pancreatic cancer: surgical versus endoscopic palliation. Surg Endosc 2002;16(2):3102.
83. Takeuchi K, Tsuzuki Y, Ando T, et al. The diagnosis and treatment of adult intus-
susception. J Clin Gastroenterol 2003;36(1):1821.
84. Wang LT, Wu CC, Yu JC, et al. Clinical entity and treatment strategies for
adult intussusceptions: 20 years experience. Dis Colon Rectum 2007;
50(11):19419.
85. Rea JD, Lockhart ME, Yarbrough DE, et al. Approach to management of intus-
susception in adults: a new paradigm in the computed tomography era. Am
Surg 2007;73(11):1098105.
86. Azar T, Berger DL. Adult intussusception. Ann Surg 1997;226(2):1348.87. Fernandez Sola A, Valles Callol JA, Capdevila Morell JA, et al. [Acute abdomen
secondary to cytomegalovirus infection]. An Med Interna 1992;9(1):335
[in Spanish].
88. Glenn J, Funkhouser WK, Schneider PS. Acute illnesses necessitating urgent
abdominal surgery in neutropenic cancer patients: description of 14 cases
and review of the literature. Surgery 1989;105(6):77889.
Ilgen & Marr396
-
8/2/2019 Abdomen Agudo Clinics
17/19
89. Kawate S, Ohwada S, Sano T, et al. Ileal perforation caused by cytomegalovirus
infection in a patient with recurrent gastric cancer: report of a case. Surg Today
2002;32(12):108890.
90. Nabeshima K, Sakaguchi E, Inoue S, et al. Jejunal perforation associated with
cytomegalovirus infection in a patient with adult T-cell leukemia-lymphoma.
Acta Pathol Jpn 1992;42(4):26771.
91. Nishii T, Rino Y, Ando K, et al. Successful treatment of multiple small-bowel
perforations caused by cytomegalovirus in a patient with malignant lymphoma:
report of a case. Surg Today 2006;36(10):9303.
92. Yasunaga M, Hodohara K, Uda K, et al. Small intestinal perforation due to cyto-
megalovirus infection in patients with non-Hodgkins lymphoma. Acta Haematol
1995;93(24):98100.
93. Wyatt SH, Fishman EK. The acute abdomen in individuals with AIDS. Radiol Clin
North Am 1994;32(5):102343.
94. Davila ML. Neutropenic enterocolitis. Curr Treat Options Gastroenterol 2006;
9(3):24955.
95. Alt B, Glass NR, Sollinger H. Neutropenic enterocolitis in adults. Review of the liter-
ature and assessment of surgical intervention. Am J Surg 1985;149(3):4058.
96. Williams N, Scott AD. Neutropenic colitis: a continuing surgical challenge.
Br J Surg 1997;84(9):12005.
97. Gorschluter M, Mey U, Strehl J, et al. Neutropenic enterocolitis in adults: system-
atic analysis of evidence quality. Eur J Haematol 2005;75(1):113.
98. Buyukasik Y, Ozcebe OI, Haznedaroglu IC, et al. Neutropenic enterocolitis in
adult leukemias. Int J Hematol 1997;66(1):4755.
99. Gorschluter M, Glasmacher A, Hahn C, et al. Severe abdominal infections inneutropenic patients. Cancer Invest 2001;19(7):66977.
100. Gorschluter M, Marklein G, Hofling K, et al. Abdominal infections in patients with
acute leukaemia: a prospective study applying ultrasonography and microbi-
ology. Br J Haematol 2002;117(2):3518.
101. Jones GT, Abramson N. Gastrointestinal necrosis in acute leukemia: a complica-
tion of induction therapy. Cancer Invest 1983;1(4):31520.
102. Salazar R, Sola C, Maroto P, et al. Infectious complications in 126 patients
treated with high-dose chemotherapy and autologous peripheral blood stem
cell transplantation. Bone Marrow Transplant 1999;23(1):2733.
103. Wade DS, Nava HR, Douglass HO Jr. Neutropenic enterocolitis. Clinical diag-nosis and treatment. Cancer 1992;69(1):1723.
104. Schlatter M, Snyder K, Freyer D. Successful nonoperative management of
typhlitis in pediatric oncology patients. J Pediatr Surg 2002;37(8):11515.
105. Nagler A, Pavel L, Naparstek E, et al. Typhlitis occurring in autologous bone
marrow transplantation. Bone Marrow Transplant 1992;9(1):634.
106. Song HK, Kreisel D, Canter R, et al. Changing presentation and management of
neutropenic enterocolitis. Arch Surg 1998;133(9):97982.
107. DSouza S, Lindberg M. Typhlitis as a presenting manifestation of acute myelog-
enous leukemia. Southampt Med J 2000;93(2):21820.
108. Kaste SC, Flynn PM, Furman WL. Acute lymphoblastic leukemia presenting withtyphlitis. Med Pediatr Oncol 1997;28(3):20912.
109. Paulino AF, Kenney R, Forman EN, et al. Typhlitis in a patient with acute lympho-
blastic leukemia prior to the administration of chemotherapy. Am J Pediatr Hem-
atol Oncol 1994;16(4):34851.
110. Katz JA, Wagner ML, Gresik MV, et al. Typhlitis. An 18-year experience and
postmortem review. Cancer 1990;65(4):10417.
Cancer Emergencies: Acute Abdomen 397
-
8/2/2019 Abdomen Agudo Clinics
18/19
111. Urbach DR, Rotstein OD. Typhlitis. Can J Surg 1999;42(6):4159.
112. Abu-Hilal MA, Jones JM. Typhlitis; is it just in immunocompromised patients?
Med Sci Monit 2008;14(8):CS6770.
113. Cunningham SC, Fakhry K, Bass BL, et al. Neutropenic enterocolitis in adults:
case series and review of the literature. Dig Dis Sci 2005;50(2):21520.
114. Martin SI, Mueller PS. 39-Year-old man with human immunodeficiency virus
infection and abdominal pain. Mayo Clin Proc 2003;78(10):12858.
115. Sloas MM, Flynn PM, Kaste SC, et al. Typhlitis in children with cancer: a 30-year
experience. Clin Infect Dis 1993;17(3):48490.
116. Cartoni C, Dragoni F, Micozzi A, et al. Neutropenic enterocolitis in patients with
acute leukemia: prognostic significance of bowel wall thickening detected by
ultrasonography. J Clin Oncol 2001;19(3):75661.
117. Enck RE. Malignant ascites. Am J Hosp Palliat Care 2002;19(1):78.
118. Chung M, Kozuch P. Treatment of malignant ascites. Curr Treat Options Oncol
2008;9(2-3):21533.
119. Runyon BA. Care of patients with ascites. N Engl J Med 1994;330(5):33742.
120. Smith EM, Jayson GC. The current and future management of malignant ascites.
Clin Oncol (R Coll Radiol) 2003;15(2):5972.
121. Adam RA, Adam YG. Malignant ascites: past, present, and future. J Am Coll
Surg 2004;198(6):9991011.
122. Makharia GK, Sharma BC, Bhasin DK, et al. Spontaneous bacterial peritonitis in
a patient with gastric carcinoma. J Clin Gastroenterol 1998;27(3):26970.
123. Patriti A, Cavazzoni E, Graziosi L, et al. Successful palliation of malignant ascites
from peritoneal mesothelioma by laparoscopic intraperitoneal hyperthermic
chemotherapy. Surg Laparosc Endosc Percutan Tech 2008;18(4):4268.124. Rodier JF. Radiation enteropathyincidence, aetiology, risk factors, pathology
and symptoms. Tumori 1995;81(Suppl 3):1225.
125. Bismar MM, Sinicrope FA. Radiation enteritis. Curr Gastroenterol Rep 2002;4(5):
3615.
126. Yeoh E. Radiotherapy: long-term effects on gastrointestinal function. Curr Opin
Support Palliat Care 2008;2(1):404.
127. Andreyev J. Gastrointestinal complications of pelvic radiotherapy: are they of
any importance? Gut 2005;54(8):10514.
128. Zimmerer T, Bocker U, Wenz F, et al. Medical prevention and treatment of acute
and chronic radiation induced enteritisis there any proven therapy? A shortreview. Z Gastroenterol 2008;46(5):4418.
129. Ludwig J, Hashimoto E, McGill DB, et al. Classification of hepatic venous outflow
obstruction: ambiguous terminology of the Budd-Chiari syndrome. Mayo Clin
Proc 1990;65(1):515.
130. Menon KV, Shah V, Kamath PS. The Budd-Chiari syndrome. N Engl J Med 2004;
350(6):57885.
131. Murphy FB, Steinberg HV, Shires GT III, et al. The Budd-Chiari syndrome:
a review. AJR Am J Roentgenol 1986;147(1):915.
132. Slakey DP, Klein AS, Venbrux AC, et al. Budd-Chiari syndrome: current manage-
ment options. Ann Surg 2001;233(4):5227.133. Valla DC. Prognosis in Budd Chiari syndrome after re-establishing hepatic
venous drainage. Gut 2006;55(6):7613.
134. Valla DC. Budd-Chiari syndrome and veno-occlusive disease/sinusoidal
obstruction syndrome. Gut 2008;57(10):146978.
135. Kamath PS. Budd-Chiari syndrome: radiologic findings. Liver Transpl 2006;
12(11 Suppl 2):S212.
Ilgen & Marr398
-
8/2/2019 Abdomen Agudo Clinics
19/19
136. Bolondi L, Gaiani S, Li Bassi S, et al. Diagnosis of Budd-Chiari syndrome by
pulsed Doppler ultrasound. Gastroenterology 1991;100(5 Pt 1):132431.
137. Fisher NC, McCafferty I, Dolapci M, et al. Managing Budd-Chiari syndrome:
a retrospective review of percutaneous hepatic vein angioplasty and surgical
shunting. Gut 1999;44(4):56874.
Cancer Emergencies: Acute Abdomen 399