
Pie Diabetico Now-1

of 78
-
Upload
andres-estacio-yalan -
Category
Documents
-
view
233 -
download
0
Transcript of Pie Diabetico Now-1
-
8/10/2019 Pie Diabetico Now-1
1/78
TheJournal
Supplement to:of
Foot &
An k l e S
u r g e r y
DIABETIC FOOT DISORDERS:A CLINICAL PRACTICE GUIDELINE (2006 revision)
Robert G. Frykberg, DPM, MPH,1
Thomas Zgonis, DPM,2
David G. Armstrong, DPM, PhD,
!i"kie R. Driver, DPM,
M#$
%ohn M. Gi&rini, DPM,'
#teven R. (ravit), DPM,*
Adam #. +andsman, DPM, PhD,
+a-ren"e A. +avery, DPM,
MPH,
%. /hristo0her Moore, DPM,
%ohn M. #"h&berth, DPM,1
Dane (. 3&ki"h, MD,11
/har4es Andersen, MD,12
and %ohn !. !anore, DPM1
Address "orres0onden"e to5 Robert G. Frykberg, DPM, MPH, /hie6, Podiatri" #&rgery, /ar4 T. Hayden !A
Medi"a4 /enter, Phoeni7, AZ '12. 8mai45 robert.6rykberg9med.va.gov
1/hair, Diabetes Pane4, Phoeni7, AZ:
2#an Antonio, T;:
oston, MA:
Georgeto-n, T;:
Ashvi44e,
-
8/10/2019 Pie Diabetico Now-1
2/78
TheJournal
Supplement to:of
Foot &
An k l e S
u r g e r y
DIABETIC FOOT DISORDERS:A CLINICAL PRACTICE GUIDELINE (2006 revision)
ABSTRACT: The prevalence of diabetes mellitus is growing at epidemic proportions in the United States and
worldwide. Most alarming is the steady increase in type 2 diabetes, especially among young and obese people. An
estimated 7 of the US population has diabetes, and because of the increased longevity of this population, dia !
betes!associated complications are e"pected to rise in prevalence.
#oot ulcerations, infections, $harcot neuroarthropathy, and peripheral arterial disease fre%uently result in gan !
grene and lower limb amputation. $onse%uently, foot disorders are leading causes of hospitali&ation for persons
with diabetes and account for billion!dollar e"penditures annually in the US. Although not all foot complications
can be prevented, dramatic reductions in fre%uency have been achieved by ta'ing a multidisciplinary approach topatient management. Using this concept, the authors present a clinical practice guideline for diabetic foot disor !
ders based on currently available evidence, committee consensus, and current clinical practice. The pathophysiol !
ogy and treatment of diabetic foot ulcers, infections, and the diabetic $harcot foot are reviewed. (hile these guide
! lines cannot and should not dictate the care of all affected patients, they provide evidence!based guidance for gen
! eral patterns of practice. )f these concepts are embraced and incorporated into patient management protocols, a
ma*or reduction in diabetic limb amputations is certainly an attainable goal.
This "4ini"a4 0ra"ti"e g&ide4ine ?/PG@ is based on the "onsens&s o6 "&rrent "4ini"a4 0ra"ti"e and revie- o6 the "4ini"a4 4iterat&re. This g&ide4ine -as deve4o0ed by the /4ini"a4 Pra"ti"e G&ide4ine Diabetes Pane4 o6 the Ameri"an/o44ege o6 Foot and Ank4e #&rgeons.
INTRODUCTION
The 0reva4en"e o6 diabetes me44it&s is gro-ing at
e0idemi" 0ro0ortions in the Bnited #tates and -or4d-ide
?1@. Most a4arming is the steady in"rease in ty0e 2 diabetes,
es0e"ia44y among yo&ng and obese 0ersons. An estimated
C o6 Ameri"ans are a664i"ted -ith diabetes, and -ith the
4ongevity o6 this 0o0&4ation in"reasing, the 0reva4en"e o6
diabetesre4ated "om04i"ations -i44 "ontin&e to rise.
Foot disorders are a maor so&r"e o6 morbidity and a
4eading "a&se o6 hos0ita4i)ation 6or 0ersons -ith diabetes.
B4"eration, in6e"tion, gangrene, and am0&tation are signi6i"ant "om04i"ations o6 the disease, estimated to "ost bi44ions
o6 do44ars ea"h year. /har"ot 6oot, -hi"h o6 itse46 "an 4ead
to 4imbthreatening disorders, is another serio&s "om04i"a
tion o6 4ongstanding diabetes. =n addition to im0roving the
management o6 &4"ersEthe 4eading 0re"&rsor to 4o-er
e7tremity am0&tation in diabeti" 0atients ?2@E"4ini"ians
m&st determine ho- to more e66e"tive4yprevent&4"eration.
A4tho&gh not a44 diabeti" 6oot disorders "an be 0revented, it
is 0ossib4e to e66e"t dramati" red&"tions in their in"iden"e
and morbidity thro&gh a00ro0riate eviden"ebased 0reven
tion and management 0roto"o4s.
Taking a m&4tidis"i04inary a00roa"h to diabeti" 6oot dis
orders, many "enters 6rom aro&nd the -or4d have noted
"onsistent im0rovement in 4imb sa4vage rates. 3ith this
0remise as o&r "entra4 theme, the a&thors 0resent this "4ini
"a4 0ra"ti"e g&ide4ine based on "&rrent4y avai4ab4eeviden"e. Three maor 0eda4 "om04i"ations o6 diabetes are
revie-ed5 diabeti" 6oot &4"ers, diabeti" 6oot in6e"tions, and
the diabeti" /har"ot 6oot. These g&ide4ines are intended to
0rovide eviden"ebased g&idan"e 6or genera4 0atterns o6
0ra"ti"e and do not ne"essari4y di"tate the "are o6 a
0arti"&4ar 0atient.
S2 TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
3/78
-
8/10/2019 Pie Diabetico Now-1
4/78
nondiabeti" 0o0&4ations, and the rate is at 4east 'C higher
in men vers&s -omen ?, 1, 12, @. =n 22, the age
ad&sted +8A rate among men -as . 0er 1, 0ersons
-ith diabetes "om0ared -ith to the rate among -omen
re0orted at . 0er 1 0ersons -ith diabetes ?1@.
#evera4 ethni" di66eren"es o""&r in the 6reL&en"y o6 dia
betesre4ated am0&tations. Me7i"an ?His0ani"@ Ameri"ans,
-
8/10/2019 Pie Diabetico Now-1
5/78
ria ?$2, *@. A&tosym0athe"tomy -ith attendant
sym0atheti" 6ai4&re, arterioveno&s sh&nting, and
mi"rovas"&4ar thermoreg&4atory dys6&n"tion im0airs
norma4 tiss&e 0er6&sion and mi"rovas"&4ar res0onses to
in&ry. These a4terations "an s&bseL&ent4y be im04i"ated in
the 0athogenesis o6 &4"eration ?**@.
Foot de6ormities res&4ting 6rom ne&ro0athy, abnorma4
biome"hani"s, "ongenita4 disorders, or 0rior s&rgi"a4 inter
vention may res&4t in high 6o"a4 6oot 0ress&res and in"reased
risk o6 &4"eration ?2$, $, ', ', *1@. The e66e"ts o6 motor
ne&ro0athy o""&r re4ative4y ear4y and 4ead to 6oot m&s"4eatro0hy -ith "onseL&ent deve4o0ment o6 hammertoes, 6at 0ad
dis04a"ement, and asso"iated in"reases in 04antar 6ore6oot
0ress&res ?', 2'@. A4tho&gh most de6ormities "a&se high
04antar 0ress&res and 04antar 6oot &4"erations, media4 and
dorsa4 &4"erations may deve4o0 as a res&4t o6 6oot-ear
irritation. /ommon de6ormities might in"4&de 0rior 0artia4
6oot am0&tations, 0rominent metatarsa4 heads, hammertoes,
/har"ot arthro0athy, or ha44&7 va4g&s ?*, *@. A 4arge
0ros0e"tive 0o0&4ationbased st&dy 6o&nd that e4evated
04antar 6oot 0ress&res are signi6i"ant4y asso"iated -ith
ne&ro0athi" &4"eration and am0&tation ?@. The st&dy a4so
revea4ed a trend 6or in"reased 6oot 0ress&res as the n&mber o60eda4 de6ormities in"reased.
Tra&ma to the 6oot in the 0resen"e o6 sensory ne&ro0athy
is an im0ortant "om0onent "a&se o6 &4"eration ?2$@. 3hi4e
tra&ma may in"4&de 0&n"t&re -o&nds and b4&nt in&ry, a
"ommon in&ry 4eading to &4"eration is moderate re0etitive
stress asso"iated -ith -a4king or daytoday a"tivity ?*,
*, 1@. This is o6ten mani6ested by "a44&s 6ormation &nder
Fi%&r ' The ris.
fa/ors for ul/eraion
1a 3e 4isin5uishe4
3 5eneral or sse1i//onsi4eraions versus
hose lo/alie4 o he
foo an4 is 7aholo58
the metatarsa4 heads ?$, 2, @. A re"ent re0ort s&ggests
that even -ith moderate a"tivity, &4"eration may be 0re"i0
itated by a higher degree o6 variabi4ity in a"tivity or 0eriod
i" Jb&rstsK o6 a"tivity ?$@. #hoere4ated tra&ma has a4so
been identi6ied as a 6reL&ent 0re"&rsor to 6oot &4"eration
?2, '1, '$, ', *@.
Peri0hera4 arteria4 disease ?PAD@ rare4y 4eads to 6oot
&4"erations dire"t4y. Ho-ever, on"e &4"eration deve4o0s,
arteria4 ins&66i"ien"y -i44 res&4t in 0ro4onged hea4ing,
im0arting an e4evated risk o6 am0&tation ?2, , @.
Additiona44y, attem0ts to reso4ve any in6e"tion -i44 beim0aired d&e to 4a"k o6 o7ygenation and di66i"&4ty in de4iv
ering antibioti"s to the in6e"tion site. There6ore, ear4y
re"ognition and aggressive treatment o6 4o-er e7tremity
is"hemia are vita4 to 4o-er 4imb sa4vage ?, '2, 1@.
+imited oint mobi4ity has a4so been des"ribed as a
0otentia4 risk 6a"tor 6or &4"eration ?2$@. G4y"osy4ation
o6 "o44agen as a res&4t o6 4ongstanding diabetes may 4ead
to sti66ening o6 "a0s&4ar str&"t&res and 4igaments
?"heiroarthro0athy@ ?'@. The s&bseL&ent red&"tion in
ank4e, s&bta4ar, and 6irst metatarso0ha4angea4 ?MTP@ oint
mobi4ity has been sho-n to res&4t in high 6o"a4 04antar
0ress&res -ith in"reased &4"eration risk in 0atients -ithne&ro0athy ?2, *, @. #evera4 re0orts a4so attrib&te
g4y"osy4ation and a4tered arrangement o6 A"hi44es tendon
"o44agen to the 0ro0ensity 6or diabeti" 0atients to deve4o0
ank4e eL&in&s ?, @.
Ither 6a"tors 6reL&ent4y asso"iated -ith heightened&4"eration risk in"4&de ne0hro0athy, 0oor diabetes "ontro4,
d&ration o6 diabetes, vis&a4 4oss, and advan"ed age ?$, *,
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S(
-
8/10/2019 Pie Diabetico Now-1
6/78
Fi%&r 2 Dia3ees 1ellius is res7onsi3le for a varie of foo 7aholo5ies /onri3uin5 o he /o17li/aions of
ul/eraion an4 a17uaion8 uli7le 7aholo5ies 1a 3e i17li/ae4, fro1 vas/ular 4isease o neuro7ah o
1e/hani/al rau1a8
, 1@. #o6t tiss&e "hanges ?other than "heiroarthro0athy@ in
the 6eet o6 diabeti" 0atients might a4so "ontrib&te to &4"er
ation thro&gh the 0ath-ay o6 a4tered 0ress&re distrib&tions
thro&gh the so4e o6 the 6oot. #&"h a4terations in"4&de a
re0orted in"reased thi"kness o6 the 04antar 6as"ia -ith asso
"iated 4imitation o6 ha44&7 dorsi64e7ion, de"reased thi"kness o6
04antar so6t tiss&e, a""ent&ated hardnesssti66ness o6 the skin,
and a 0ro0ensity to deve4o0 "a44&ses ?2, *, 111'@. 3hi4e
these "hanges are 0res&mab4y "a&sed by g4y"osy4ation o6
"o44agen, their s&m e66e"t is to enhan"e 04antar 0ress&res in
gait. =n the 0resen"e o6 ne&ro0athy, the a""ent&ated 04antar
0ress&res "an be im04i"ated in the deve4o0ment o6 &4"eration
?, , 2, 1*@.
e/hanis1s of In9ur
The m&4ti6a"toria4 etio4ogy o6 diabeti" 6oot &4"ers is evi
den"ed by the n&mero&s 0atho0hysio4ogi" 0ath-ays that
"an 0otentia44y 4ead to this disorder ?2$, $, '$, *2, ,
1@. Among these are t-o "ommon me"hanisms by -hi"h
6oot de6ormity and ne&ro0athy may ind&"e skin breakdo-n
in 0ersons -ith diabetes ?*, 1, 1@.
The 6irst me"hanism o6 in&ry re6ers to 0ro4onged 4o-
0ress&re over a bony 0rominen"e ?ie, b&nion or hammertoe
de6ormity@. This genera44y "a&ses -o&nds over the media4,
4atera4, and dorsa4 as0e"ts o6 the 6ore6oot and is asso"iated
-ith tight or i446itting shoes. #hoe tra&ma, in "on"ert -ith
4oss o6 0rote"tive sensation and "on"omitant 6oot
de6ormity, is the 4eading event 0re"i0itating 6oot &4"eration
in 0ersons -ith diabetes ?2$, 2, ', '@.
S) TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
7/78
Regions o6 high 0eda4 0ress&re are 6reL&ent4y asso"iated
-ith 6oot de6ormity ?*, , *, , 1*, 1@. 3hen an
abnorma4 6o"&s o6 0ress&re is "o&04ed -ith 4a"k o6 0rote"
tive sensation, the res&4t "an be deve4o0ment o6 a "a44&s,
b4ister, and &4"er ?11@. The other "ommon me"hanism o6
&4"eration invo4ves 0ro4onged re0etitive moderate stress
?1@. This norma44y o""&rs on the so4e o6 the 6oot and is
re4ated to 0rominent metatarsa4 heads, atro0hied oranterior4y dis04a"ed 6at 0ads, str&"t&ra4 de6ormity o6 the
4o-er e7tremity, and 0ro4onged -a4king. Rigid de6ormities
s&"h as ha44&7 va4g&s, ha44&7 rigid&s, hammertoe, /har"ot
arthro0athy, and 4imited range o6 motion o6 the ank4e
?eL&in&s@, s&bta4ar, and MTP oints have been 4inked to
the deve4o0ment o6 diabeti" 6oot &4"ers ?2, ', 1, , $,
*@.
-
8/10/2019 Pie Diabetico Now-1
8/78
Fi%&r 3 The ris.
fa/ors for a17uaion
are 1ulifa/orial an4
si1ilar o hose for
ul/eraion8
3hi4e in6e"tion is not o6ten im04i"ated in the 0ath-ay
4eading to &4"eration, it is a signi6i"ant risk 6a"tor in the "a&sa4
0ath-ay to am0&tation ?2$, 2@. +a"k o6 -o&nd hea4ing,
systemi" se0sis, or &nreso4ved in6e"tion "an 4ead to e7tensive
tiss&e ne"rosis and gangrene, reL&iring am0&tation to 0revent
more 0ro7ima4 4imb 4oss. This in"4&des so6t tiss&e in6e"tion
-ith severe tiss&e destr&"tion, dee0 s0a"e abs"ess, or
osteomye4itis. AdeL&ate debridement may reL&ire am0&tationat some 4eve4 as a means o6 removing a44 in6e"ted materia4
?, 12, 1', 1'1@.
Another 6reL&ent4y des"ribed risk 6a"tor 6or am0&tation is
"hroni" hy0erg4y"emia. Res&4ts o6 the Diabetes /ontro4 and
/om04i"ations Tria4 ?D//T@ and the Bnited (ingdom
Pros0e"tive Diabetes #t&dy ?B(PD#@ s&00ort the 4onghe4d
theory that "hroni" 0oor "ontro4 o6 diabetes is asso"iated -ith
a host o6 systemi" "om04i"ations ?1'2, 1'@. The 4ink bet-een
degree o6 g4&"ose "ontro4 and in"iden"e or 0rogression o6
n&mero&s diabeti" "om04i"ations has been -e44 estab4ished by
these and other st&dies ?1'$, 1''@. #&"h "om04i"ationsin"4&de 0eri0hera4 ne&ro0athy, mi"roangio0athy,
mi"ro"ir"&4atory dist&rban"es, im0aired 4e&ko"yte
0hago"ytosis, and g4y"osy4ation o6 tiss&e 0roteins. 8a"h has
adverse e66e"ts on the diabeti" 6oot5 They "an "ontrib&te to
the etio4ogy o6 6oot &4"eration, de4ay norma4 -o&nd hea4ing,
and s&bseL&ent4y 4ead to am0&tation ?2', , $, ', 2@.
#evera4 st&dies have re0orted a signi6i"ant "orre4ation
bet-een e4evated g4&"ose and +8A ?21, 1$1,
1'*1*1@. Am0&tation has a4so been asso"iated -ith other
diabetesre4ated "omorbidities s&"h as ne0hro0athy, r e t i n
o 0 a t h y, and "ardiovas"&4ar disease ?21, $, 1$$@.
Aggressive g4&"ose "ontro4, management o6 asso"iated
"omorbidities, and a00ro0riate 4o-er e7tremity "are
"oordinated in a team environment may indeed 4o-er
overa44 risk 6or am0&tation ?, , 1*21**@.
The best 0redi"tor o6 am0&tation is a history o6 0revio&s
am0&tation. A 0ast history o6 a 4o-er e7tremity &4"eration or
am0&tation in"reases the risk 6or 6&rther &4"eration, in6e"tion,
and s&bseL&ent am0&tation ?2, 1$2, 1', 1*@. =t may a4so be
in6erred that 0atients -ith 0revio&s &4"eration 0ossess a44 the
risk 6a"tors 6or deve4o0ing another &4"eration, having
demonstrated that they a4ready have the "om0onent e4ements
in the "a&sa4 0ath-ay ?2$, 2, 2, '@. B0 to $C o6 0atients
deve4o0 another &4"er -ithin 1 year a6ter hea4ing an inde7
-o&nd, and the 'year rate o6 deve4o0ing a ne- &4"er is C
?1*$, 1*@. The re"&rren"e rate is higher 6or 0atients -ith a
0revio&s am0&tation be"a&se o6 abnorma4 distrib&tion o604antar 0ress&res and a4tered osseo&s ar"hite"t&re. The
"&m&4ative risks o6 ne&ro0athy, de6ormity, high 04antar
0ress&re, 0oor g4&"ose "ontro4, and ma4e gender are a44
additive 6a"tors 6or 0eda4 &4"eration in these diabeti" 0atients
?2*, $*, ', ', 111@. Ream0&tation "an be attrib&ted to
disease 0rogression, nonhea4ing -o&nds, and additiona4 risk
6a"tors 6or 4imb 4oss that deve4o0 as a res&4t o6 the 6irst
am0&tation. Tragi"a44y, the 'year s&rviva4 rate
S/ TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
9/78
PAT01AY '
-
8/10/2019 Pie Diabetico Now-1
10/78
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S
-
8/10/2019 Pie Diabetico Now-1
11/78
a6ter a diabetesre4ated +8A has been re0orted to be as 4o- as
2C to 1C ?1*, 1@. Persons -ith rena4 6ai4&re or more
0ro7ima4 4eve4s o6 am0&tation have a 0oor 0rognosis and
higher morta4ity rate. Those -ho &ndergo a diabetesre4ated
am0&tation have a $C to ' C "han"e o6 &ndergoing a
"ontra4atera4 am0&tation -ithin 2 years ?*, 11, 12@.
ASSESSMENT OF T0E DIABETIC FOOT
4P!"*5!6 '7
The 0eda4 mani6estations o6 diabetes are -e44 do"&ment
ed and 0otentia44y 4imbthreatening -hen 4e6t &ntreated.
Re"ognition o6 risk 6a"tors and treatment o6 diabeti" 6oot
disorders reL&ire the ski44 o6 a s0e"ia4i)ed 0ra"titioner to
diagnose, manage, treat, and "o&nse4 the 0atient.
=ntegration o6 kno-4edge and e70erien"e thro&gh a
m&4tidis"i04inary team a00roa"h 0romotes more e66e"tive
treatment, thereby im0roving o&t"omes and 4imiting the
risk o6 4o-er e7tremity am0&tation ?, 1@.
The eva4&ation o6 the diabeti" 6oot invo4ves "are6&4
assimi4ation o6 the 0atients history and 0hysi"a4 6indings-ith the res&4ts o6 ne"essary diagnosti" 0ro"ed&res
?Path-ay 1@. #"reening too4s may be va4&ab4e in eva4&ating
the 0atient and determining risk 4eve4 ?A00endi7 1@. 8ar4y
dete"tion o6 6oot 0atho4ogy, es0e"ia44y in highrisk 0atients,
"an 4ead to ear4ier intervention and thereby red&"e the
0otentia4 6or hos0ita4i)ation and am0&tation ?1@. This is
a4so 6a"i4itated by an &nderstanding o6 the &nder4ying
0atho0hysio4ogy o6 diabeti" 6oot disorders and asso"iated
risk 6a"tors. =denti6i"ation o6 abnorma4 histori"a4 andor0hysi"a4 6indings "an there6ore im0rove the 0rognosis 6or a
6avorab4e o&t"ome thro&gh a00ro0riateEand ear4yEre6er
ra4 ?1, 1$@.
0is"or6
A thoro&gh medi"a4 and 6oot history m&st be obtained
6rom the 0atient. The history sho&4d address severa4 s0e"i6
i" diabeti" 6oot iss&es ?Tab4e 2@.
P*6sic!l E8!,i#!"io#
A44 0atients -ith diabetes reL&ire a 0eda4 ins0e"tion-henever they 0resent to any hea4th "are 0ra"titioner, and
-
8/10/2019 Pie Diabetico Now-1
12/78
S'9 TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
13/78
they sho&4d re"eive a thoro&gh 4o-er e7tremity e7amination
at 4east on"e ann&a44y ?1'@. Patients -ith "om04aints re4ating
to the diabeti" 6oot reL&ire more 6reL&ent detai4ed eva4&ations.
The e7amination sho&4d be 0er6ormed systemati"a44y so that
im0ortant as0e"ts are not over4ooked ?*2@. =t begins -ith a
gross eva4&ation o6 the 0atient and e7tremities. Any obvio&s
0rob4em "an then re"eive "4oser s"r&tiny.
(ey "om0onents o6 the 6oot e7amination are 0resentedin Tab4e . A4tho&gh not s0e"i6i"a44y mentioned in this se"
tion, it is ass&med that a genera4 medi"a4 assessment
?in"4&ding vita4 sign meas&rements@ -i44 be obtained.
Di!%#os"ic Proc&rs
Diagnosti" 0ro"ed&res may be indi"ated in the assess
ment and "are o6 the diabeti" 6oot. /onsideration sho&4d be
given to the 6o44o-ing tests in "on"ert -ith those s&ggested
by members o6 the "ons&4ting team. =t sho&4d be noted that
many o6 the 6o44o-ing tests 4a"k the abi4ity to im0art a
de6initive diagnosis, ne"essitating "4ini"a4 "orre4ation.
La3oraor Tess
/4ini"a4 4aboratory tests that may be needed in a00ro0riate
"4ini"a4 sit&ations in"4&de 6asting or random b4ood g4&"ose,
g4y"ohemog4obin ?HbA1"@, "om04ete b4ood "o&nt ?/>/@ -ith
or -itho&t di66erentia4, erythro"yte sedimentation rate ?8#R@,
ser&m "hemistries, /rea"tive 0rotein, a4ka4ine 0hos0hatase,
-o&nd and b4ood "&4t&res, and &rina4ysis. /a&tion m&st be
e7er"ised in the inter0retation o6 4aboratory tests in these
0atients, be"a&se severa4 re0orts have do"&mented the
absen"e o6 4e&ko"ytosis in the 0resen"e o6 severe 6oot
in6e"tions ?11, 122, 1'1, 1*1@. A "ommon sign o6
0ersistent in6e"tion is re"a4"itrant hy0erg4y"emia des0ite &s&a4
antihy0erg4y"emi" regimens ?1'@.
I1a5in5 %u4ies
The diabeti" 6oot may be 0redis0osed to both "ommon
and &n&s&a4 in6e"tio&s or nonin6e"tio&s 0ro"esses, 0artia44y
be"a&se o6 the "om04e7 nat&re o6 diabetes and its asso"iat
ed vas"&4ar and ne&ro0athi" "om04i"ations. As a res&4t,
imaging 0resentations -i44 vary d&e to 4a"k o6 s0e"i6i"ity
in "om04e7 "4ini"a4 "ir"&mstan"es ?111@. #&"h
variabi4ity "reates a "ha44enge in the inter0retation o6
imaging st&dies. There6ore, imaging st&dies sho&4d on4y beordered to estab4ish or "on6irm a s&s0e"ted diagnosis
andor dire"t 0atient management. Disting&ishing
osteomye4itis 6rom ase0ti" ne&ro0athi" arthro0athy is not
easy, and a44 imaging st&dies ?Fig $@ m&st be inter0reted in
"on&n"tion -ith the "4ini"a4 6indings ?12, 1'1@.
P4ain radiogra0hs sho&4d be the initia4 imaging st&dy indiabeti" 0atients -ith signs and sym0toms o6 a diabeti" 6oot
disorder ?1, 12@. Radiogra0hs "an dete"t osteomye4itis,
osteo4ysis, 6ra"t&res, dis4o"ations seen in ne&ro0athi"
arthro0athy, media4 arteria4 "a4"i6i"ation, so6t tiss&e gas, and
6oreign bodies as -e44 as str&"t&ra4 6oot de6ormities, 0resen"e
o6 arthritis, and biome"hani"a4 a4terations ?1@. A"&te
osteomye4itis might not demonstrate osseo&s "hanges 6or &0 to
1$ days. #eria4 radiogra0hs sho&4d be obtained in the 6a"e o6
an initia4 negative radiogra0hi" image and a high "4ini"a4s&s0i"ion o6 osseo&s disease ?11, 12@.
Te"hneti&m methy4ene di0hos0honate ?T" MDP@
bone s"ans are o6ten &sed in diabeti" 6oot in6e"tion to deter
mine the 0resen"e o6 osteomye4itis. A4tho&gh high4y sensi
tive, this moda4ity 4a"ks s0e"i6i"ity in the ne&ro0athi" 6oot
?1$, 1'@. Isteomye4itis, 6ra"t&res, arthritis, and ne&ro0athi"
arthro0athy -i44 a44 demonstrate in"reased radiotra"er &0take.
Ho-ever, a negative bone s"an is strong eviden"e against the
0resen"e o6 in6e"tion. To im0rove the s0e"i6i"ity o6 n&"4ear
imaging, -hite b4ood "e44s "an be 4abe4ed -ith T"
he7amethy40ro0y4eneamineo7ime ?T" HMPAI@, indi&m
111 o7ime, or ga44i&m* "itrate ?1, 1*1@.
=ndi&m111 se4e"tive4y 4abe4s 0o4ymor0hon&"4ear 4e&ko
"ytes and is more s0e"i6i" 6or a"&te in6e"tions than T"
MDP s"anning. /hroni" in6e"tions and in64ammation are not
-e44 imaged -ith indi&m111, be"a&se "hroni" in64ammatory
"e44s ?ie, 4ym0ho"ytes@ 0redominate and are not -e44 4abe4ed
-ith indi&m. /ombining T" MDP and indi&m111
in"reases the s0e"i6i"ity o6 diagnosing osteomye4itis ?1@.
This "ombined te"hniL&e is &se6&4, be"a&se the T" MDP
s"an 4o"a4i)es the anatomi" site o6 in64ammation and the
indi&m111 4abe4s the in6e"ted bone ?1, 11@. The indi&m
111 s"an is not ty0i"a44y 0ositive in ase0ti" ne&ro0athi"
arthro0athy, a4tho&gh 6a4se0ositive indi&m s"ans "an o""&r
?121$@. A 1C sensitivity and C s0e"i6i"ity have been
re0orted -ith the "ombined te"hniL&e in eva4&ating diabeti"
in6e"tions ?1, 11, 1'@.
=n T" HMPAI s"anning, -hite b4ood "e44s are 4abe4ed in
a simi4ar manner as in indi&m s"anning. Ho-ever, -ith T"
MHPAI s"ans, imaging o""&rs $ ho&rs 6o44o-ing
administration vers&s 2$ ho&rs 0ostadministration -ith indi&m
s"anning. T" HMPAI &ses a sma44er radiation dose, is 4ess
e70ensive, and o66ers im0roved reso4&tion "om0ared -ith
indi&m s"anning. The sensitivity and s0e"i6i"ity o6 both
te"hniL&es are "om0arab4e ?1*, 1*@. T" HMPAI s"ans
"annot be "ombined -ith T" MDP s"ans be"a&se o6 simi4ar
4abe4ing "hara"teristi"s.
T" s&46&r "o44oid is &se6&4 in disting&ishing
osteomye4itis 6rom ne&ro0athi" arthro0athy ?1@. This
tra"er is 0i"ked &0 by the bone marro- and any hema0oet
i"a44ya"tive marro- -i44 be 0ositive. =n6e"ted bone
re04a"es norma4 bone marro-, so it sho-s &0 as a re4ative
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S''
-
8/10/2019 Pie Diabetico Now-1
14/78
S'2 TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
15/78
Fi%&r $ Dia5nosi/ i1a5in5 7las an i17oran role in he evaluaion of 4ia3ei/ foo infe/:
ions8 (A)This 7aien 7resene4 ;ih a 4ee7 foul:s1ellin5 ne/roi/ ul/er of he heel ha ha4
3een 7resen for 1ore han < 1onh8 (B)In he 7as, a e/hneiu1 3one s/an 7i/all ;oul4 3e
7erfor1e4, 3u he i1a5in5 is nons7e/ifi/ an4 1an false 7osiive resuls iner7reaive as
oseo1eliis ;ere seen8 (C)=hie 3loo4 /ell a55e4 i1a5in5 ;ih in4iu1 or e/hneiu1 is a
1ore relia3le e/hni>ue for 4ee/in5 he 7resen/e of infe/ion8
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S'3
-
8/10/2019 Pie Diabetico Now-1
16/78
J"o4d s0ot.K This te"hniL&e is best "ombined -ith indi&ms"anning, and osteomye4itis -o&4d a00ear as a JhotKindi&m s"an and a J"o4dK s&46&r "o44oid s"an ?1, 1@.
/om0&ted tomogra0hy ?/T@ s"ans may be indi"ated in
the assessment o6 s&s0e"ted bone and oint 0atho4ogy not
evident on 04ain radiogra0hs ?1, 1@. /T o66ers high
anatomi" detai4 and reso4&tion o6 bone -ith osseo&s 6rag
mentation and oint s&b4&7ation ?1@. #&b4&7ation o6 thetransverse tarsa4 or tarsometatarsa4 oints "an be seen 0rior
to being vis&a4i)ed on radiogra0hs.
Magneti" resonan"e imaging ?MR=@ is &s&a44y 0re6erred
over /T 6or the investigation o6 osteomye4itis, be"a&se o6
its enhan"ed reso4&tion and abi4ity to vis&a4i)e the e7tent o6
any in6e"tio&s 0ro"ess ?1, 1@. MR= is o6ten &sed in
eva4&ating so6t tiss&e and bone 0atho4ogy. This s"an may
be indi"ated to aid in the diagnosis o6 osteomye4itis, dee0
abs"ess, se0ti" oint, and tendon r&0t&re. =t is a readi4y
avai4ab4e moda4ity that has a very high sensitivity 6or bone
in6e"tion and "an a4so be &sed 6or s&rgi"a4 04anning ?12,
22@. Des0ite its high "ost, MR= has gained -idea""e0tan"e in the management o6 diabeti" 6oot in6e"tions.
3hen ne&ro0athi" arthro0athy is 0resent, the T1 and T2
bone images are hy0ointense ?ie, de"reased signa4@ and the
so6t tiss&es sho- edema. =n"reased signa4 on T2 bone
images is seen in osteomye4itis: ho-ever, t&mors and avas
"&4ar ne"rosis "an a4so be hy0erintense on T2 ?2$@. MR=
is an e7"e44ent moda4ity 6or assessing the 0resen"e o6 a so6t
tiss&e abs"ess, es0e"ia44y i6 gado4ini&m administration is
&ti4i)ed ?2', 2*@. Post"ontrast 6at s&00ression images
sho&4d be obtained, i6 avai4ab4e ?2@.
Positive emission tomogra0hy ?P8T@ s"anning is a
0romising ne- te"hniL&e 6or disting&ishing osteomye4itis
6rom ne&ro0athi" arthro0athy, b&t it "&rrent4y is not -ide4y
avai4ab4e ?1, 2, 2@. A re"ent metaana4ysis
"om0aring the diagnosti" a""&ra"y o6 P8T s"anning -ith
bone and 4e&ko"yte s"anning 6o&nd that P8T s"ans -ere
the most a""&rate moda4ity 6or diagnosing osteomye4itis,
0roviding a sensitivity o6 *C and s0e"i6i"ity o6 1C
?1@. 3hen P8T s"anning -as &navai4ab4e, an indi&m
4abe4ed 4e&ko"yte s"an -as 6o&nd to be an a""e0tab4e
a4ternative, o66ering a sensitivity o6 $C and s0e"i6i"ity o6
C in the 0eri0hera4 ske4eton ?1@.
The &se o6 &4traso&nd 6or dete"ting "hroni" osteomye4itis
has been sho-n to be s&0erior to 04ain radiogra0hs, 0rovid
ing sensitivity "om0arab4e to T" MDP bone s"anning
?21@. A4tho&gh &4traso&nd is a -ide4y avai4ab4e, "oste66e"
tive imaging moda4ity, MR= is more a""&rate and is the
imaging st&dy o6 "hoi"e i6 radiogra0hs are norma4 and "4in
i"a4 s&s0i"ion is high 6or bone or so6t tiss&e in6e"tion ?211@.
as/ular Evaluaion
The 4o-er e7tremity m&st be assessed 6or vas"&4ar andne&ro0athi" risk 6a"tors. A4tho&gh 0ositive 6indings in thene&ro4ogi" e7amination rare4y reL&ire 6&rther eva4&ation,0ositive 6indings o6 vas"&4ar ins&66i"ien"y may reL&ire 6&rther "ons&4tation. The indi"ations 6or vas"&4ar "ons&4tationin"4&de an ank4e bra"hia4 inde7 o6 4ess than ., toe b4ood0ress&res 4ess than $ mmHg, or trans"&taneo&s o7ygen
tension ?T"PI2@ 4eve4s 4ess than mmHg, sin"e these
meas&res o6 arteria4 0er6&sion are asso"iated -ith im0aired-o&nd hea4ing ?2, $, , , 212, 21@.
=6 the history and 0hysi"a4 e7amination s&ggest is"hemia
?ie, absent 0eda4 0&4ses@ or i6 a nonhea4ing &4"er is 0resent,
6&rther eva4&ation in the 6orm o6 noninvasive testing is -ar
ranted ?Path-ay 2@.
=@, toe b4ood 0ress&res,
and T"PI2?, 21$, 21'@. Ank4ebra"hia4 indi"es may be
mis4eading, be"a&se ank4e 0ress&res "an be 6a4se4y e4evatedd&e to media4 arteria4 "a4"inosis and non"om0ressibi4ity o6a66e"ted arteries ?'2, 21*, 21@. A gro-ing body eviden"es&ggests that toe b4ood 0ress&res in diabeti" 0atients mayhave a ro4e in 0redi"ting 6oot &4"eration risk as -e44 as 0re
di"ting s&""ess6&4 -o&nd hea4ing ?21, 21, 21@. T"PI2meas&rements have re"eived simi4ar s&00ort in the 4iterat&re ?$, , 212@. A4tho&gh not "onsistent4y 0redi"tive o6-o&nd hea4ing o&t"omes, these 0hysio4ogi" meas&res o6tiss&e o7ygenation are high4y 0redi"tive o6 -o&nd hea4ing
6ai4&re at 4eve4s be4o- 2' mmHg ?, 212, 22@. >oth tests"an be 0er6ormed dista44y on the 6oot regard4ess o6 arteria4"a4"i6i"ation in the maor 0eda4 arteries, and they are both6avorab4e at 0ress&res in the range o6 $ mmHg ?, 212,
21@.
+aser Do004er ve4o"imetry and meas&rement o6 skin 0er
6&sion 0ress&re ?#PP@ have 0rimari4y been &sed in resear"h
settings, b&t "an a""&rate4y assess b4ood 64o- and o7ygen
tension in the s&0er6i"ia4 arterio4es and "a0i44aries o6 the
skin ?2222'@. #evera4 re"ent re0orts indi"ate that 4aser
Do004er meas&rement o6 #PP "an be high4y 0redi"tive o6
"riti"a4 4imb is"hemia and -o&nd hea4ing 6ai4&re at 4eve4s
4ess than mmHg ?22, 22$@.
!as"&4ar "ons&4tation sho&4d be "onsidered in the 0res
en"e o6 abnorma4 noninvasive arteria4 st&dies or a nonhea4
ing &4"eration ?, '$, 1, 21', 22*@. Arteriogra0hy -ith
"4ear4y vis&a4i)ed dista4 r&no66 a44o-s a00ro0riate assess
ment 6or 0otentia4 revas"&4ari)ation ?2222@. Magneti"
resonan"e angiogra0hy ?2@ or /T angiogram are a4terna
tives 6or eva4&ation o6 dista4 arteria4 0er6&sion ?22, 21@.
S'$ TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
17/78
PAT01AY 2
-
8/10/2019 Pie Diabetico Now-1
18/78
-
8/10/2019 Pie Diabetico Now-1
19/78
Neurolo5i/ Evaluaion
Peri0hera4 sensory ne&ro0athy is the maor risk 6a"tor 6or
diabeti" 6oot &4"eration ?2$, 2*, 2, $*, '@. The 0atient his
tory and 0hysi"a4 e7amination &ti4i)ing the '. #emmes
3einstein mono6i4ament ?1g@ -ire are s&66i"ient to identi6y
individ&a4s at risk 6or &4"eration ?2*, 222'@.
!ibration 0er"e0tion thresho4d assessment -ith the
biothesiometer is a4so &se6&4 in identi6ying 0atients at highrisk 6or &4"eration ?$$, ', 2*@. More so0histi"ated st&dies
s&"h as nerve "ond&"tion st&dies are rare4y ne"essary to
diagnose 0eri0hera4 sensory ne&ro0athy. Patients -ith ne&
ro0athi" &4"erations &s&a44y have s&"h 0ro6o&nd sensory
ne&ro0athy that these st&dies add 4itt4e to their "4ini"a4
management ?$@.
Planar "oo Pressure Assess1en
High 04antar 6oot 0ress&re is a signi6i"ant risk 6a"tor 6or
&4"eration ?2*, $', ', , *, , 2@. Meas&rement o6
high 04antar 6oot 0ress&re is 0ossib4e &ti4i)ing a variety o6
moda4ities. #evera4 "om0&teri)ed systems "an 0rovide
L&antitative meas&rement o6 04antar 6oot 0ress&re ?*, 1,
22$1@. 3hi4e these meas&rements may be im0ortant in
identi6ying areas o6 the 6oot at risk 6or &4"eration and 0ossi
b4y in eva4&ating orthoti" ad&stments ?', '@, they are
0rimari4y &sed in diabeti" 6oot resear"h. The Harris mat,
-hi4e not as so0histi"ated, "an 0rovide a L&a4itative
meas&rement o6 04antar 6oot 0ress&res and "an identi6y
0otentia44y v&4nerab4e areas 6or &4"eration.?2$2@. A ne-er
non"om0&teri)ed devi"e ?Press&re#tat, Foot+ogi",
-
8/10/2019 Pie Diabetico Now-1
20/78
Fi%&r (A 4ia3ei/ foo servi/e is /o17ose4 of a varie of s7e/ialiss 5enerall
nee4e4 o evaluae an4 rea he 7aholo5 seen in he 7aien ;ih 4ia3ees8Effe/ive 1ana5e1en 1us in/lu4e a77ro7riae /onsulaion for rea1en of .no;n
/o1or3i4iies8
tion o6 the disease. A re"ent Markov ana4ysis o6 the "ost
e66e"tiveness o6 6oot "are a""ording to 0&b4ished g&ide4ines
6o&nd that s&"h 0reventive "are "an im0rove s&rviva4,
red&"e &4"eration and am0&tation rates, is "oste66e"tive,
and "an even save on 4ongterm "osts -hen "om0ared -ith
standard "are ?2'$@.
Risk strati6i"ation based on the 0resen"e o6 0redis0osing
"a&sa4 risk 6a"tors, in"4&ding 0rior history o6 &4"eration,
a4so serves as a g&ide to the 6reL&en"y o6 6oot "are visits.>y identi6ying highrisk 0atient and tai4oring a tota4 6oot
"are 0revention 0rogram a""ording4y, the in"iden"es o6
&4"eration and 4o-er e7tremity am0&tations "an be
red&"ed ?2', 2''2'@.
Thera0e&ti" shoes -ith 0ress&rere4ieving inso4es and
high toe bo7es are im0ortant ad&n"tive treatments that "an
red&"e the o""&rren"e o6 &4"eration and res&4tant am0&ta
tion in highrisk 0atients ?'1, *, 2'2*2@. 3hi4e most
st&dies s&00ort the e66i"a"y o6 0rote"tive 6oot-ear in this
regard, t-o re0orts s&ggest that shoes in the absen"e o6 a
"om0rehensive 0revention 0rogram might not be s&66i"ient
to 0revent ne- 4esions ?2*, 2*$@.
-
8/10/2019 Pie Diabetico Now-1
21/78
"overed 4esions. Home tem0erat&re assessment o6 the 6oot
has been sho-n to red&"e the in"iden"e o6 6oot &4"ers 1
6o4d "om0ared -ith standard 0reventive "are ?2@.
Patients -ith vis&a4 or 0hysi"a4 im0airments that 0re"4&de
their o-n "are sho&4d engage the assistan"e o6 6ami4y or
6riends to aid in this regard ?2'@. 3hen "ombined -ith a
"om0rehensive a00roa"h to 0reventive 6oot "are, 0atient
ed&"ation "an red&"e the 6reL&en"y and morbidity o6 4imbthreatening diabeti" 6oot 4esions ?2$, 2, 2@.
Provider ed&"ation is eL&a44y im0ortant in 0revention,
sin"e not a44 "4ini"ians are "ogni)ant o6 im0ortant signs and
risk 6a"tors 6or 0eda4 "om04i"ations ?1*, 1$, 2*@.
F&rthermore, 0rovider ed&"ation is e66e"tive in rein6or"ing
0ro0er diabetes management and 6oot "are 0ra"ti"es,
res&4ting in red&"tions in &4"eration and adverse 4o-er
e7tremity o&t"omes ?$, 2*, 222@.
PAT0OLOGIC ENTITIES OF T0E DIABETIC FOOT
4Foo" Ulcr< I#fc"io#< C*!rco" Foo"7
866e"tive management o6 diabeti" 6oot disorders reL&ires
kno-4edge o6 the 0otentia4 0atho4ogies, the asso"iated "4as
si6i"ation systems, and the 0rin"i04e tenets o6 intervention.
B4"eration, in6e"tion, and /har"ot arthro0athy are the most
signi6i"ant o6 these 0atho4ogies and "4assi6i"ation systems
have been deve4o0ed 6or ea"h entity. 3hi4e the "onditions
may be seen either as an iso4ated event or "oe7isting in the
same e7tremity, ea"h entity is e7amined inde0endent4y in
this "4ini"a4 0ra"ti"e g&ide4ine.
DIABETIC FOOT ULCERS (Pathway 3)
Evaluation of Ulcers
The initia4 eva4&ation o6 the diabeti" 6oot &4"er m&st be
"om0rehensive and systemati" to as"ertain the 0arameters that
might have 4ed to its onset as -e44 as determine the 0resen"e
o6 6a"tors that "an im0air -o&nd hea4ing ?2', '2, '$@. /riti"a4
in this regard are assessments 6or vas"&4ar 0er6&sion
?is"hemia@, in6e"tionosteomye4itis, and ne&ro0athy. As
0revio&s4y dis"&ssed, a thoro&gh vas"&4ar eva4&ation m&st be
0er6ormed: this in"4&des 0a40ation o6 0&4ses, "4ini"a4
eva4&ation o6 "a0i44ary 6i44ing time, veno&s 6i44ing time, 0a44or
on e4evation, and de0endent r&bor ?2@. =6 0&4ses are not
0a40ab4e or i6 "4ini"a4 6indings s&ggest is"hemia, noninvasive
arteria4 eva4&ation ?eg, segmenta4 Do004er 0ress&res -ith
-ave6orms, ank4e bra"hia4 indi"es, toe 0ress&res, T"PI2meas&rements@ and vas"&4ar s&rgi"a4 "ons&4tation are
-arranted. 3hen reL&ired, these 0hysio4ogi" and anatomi"
data "an be s&004emented -ith the &se o6 magneti" resonan"e
angiogra0hy ?2@ or /T angiogra0hy ?/TA@ and s&bseL&ent
&se o6 arteriogra0hy -ith digita4 s&btra"tion angiogra0hy
?D#A@ as ne"essary ?, , 2$@.
Des"ri0tion o6 the &4"er "hara"teristi"s on 0resentation is
essentia4 6or the ma00ing o6 the &4"ers 0rogress d&ring
treatment ?, $@. 3hi4e some "hara"teristi"s are more
im0ortant than others, they a44 have 0rognosti" va4&e
d&ring management. The 0res&med etio4ogy o6 the &4"er
?ie, "hemi"a4 vs me"hani"a4@ and "hara"ter o6 the 4esion
?ne&ro0athi", is"hemi", or ne&rois"hemi"@ sho&4d be
determined ?@. The eva4&ation sho&4d a4so des"ribe thesi)e and de0th o6 the &4"er as -e44 as the margins, base, and
geogra0hi" 4o"ation on the e7tremity or 6oot. A44 b&t the
most s&0er6i"ia4 &4"ers sho&4d be e7amined -ith a b4&nt,
steri4e 0robe. The des"ri0tion sho&4d note -hether the
steri4e 0robe dete"ts sin&s tra"t 6ormation, &ndermining o6
the &4"er margins, or disse"tion o6 the &4"er into tendon
sheaths, bone, or oints. A 0ositive 0robe to bone ?PT>@
6inding is high4y 0redi"tive o6 osteomye4itis, a4tho&gh the
6reL&en"y o6 6a4senegative tests red&"es its sensitivity
?11, 12, 2'@. Perha0s most im0ortant4y, the 0ositive
0redi"tive va4&e 6or PT> 6a44s o66 signi6i"ant4y -hen the
0reva4en"e o6 osteomye4itis de"reases ?2*@.
The e7isten"e and "hara"ter o6 odor or e7&date sho&4d be
noted. /&4t&res may be ne"essary -hen signs o6 in64amma
tion are 0resent. Genera44y, "4ini"a44y &nin6e"ted &4"ers
-itho&t in64ammation sho&4d not be "&4t&red ?, 12@.
/&rrent re"ommendations 6or "&4t&re and sensitivity
in"4&de thoro&gh s&rgi"a4 0re0aration o6 the -o&nd site
-ith "&rettage o6 the -o&nd base 6or s0e"imen or -ith
as0iration o6 abs"ess materia4 ?, 2@.
Cl!ssific!"io# of Ulcrs
A00ro0riate "4assi6i"ation o6 the 6oot -o&nd is based on a
thoro&gh assessment. /4assi6i"ation sho&4d 6a"i4itate treat
ment and be genera44y 0redi"tive o6 e70e"ted o&t"omes.
#evera4 systems o6 &4"er "4assi6i"ation are "&rrent4y in &se in
the B# and abroad to des"ribe these 4esions and "omm&ni"ate
severity ?*2, , 222@. Perha0s the easiest system is to
"4assi6y 4esions as ne&ro0athi", is"hemi", or ne&rois"hemi",
-ith des"ri0tors o6 -o&nd si)e, de0th, and in6e"tion ?@.
Regard4ess o6 -hi"h system is &sed, the "4ini"ian m&st be ab4e
to easi4y "ategori)e the -o&nd and, on"e "4assi6ied, the
ens&ing treatment sho&4d be dire"ted by the &nder4ying
severity o6 0atho4ogy.
A4tho&gh no sing4e system has been &niversa44y ado0ted,the "4assi6i"ation system most o6ten &sed -as des"ribed and
0o0&4ari)ed by 3agner ?22@. =n the 3agner system ?Tab4e '@,
6oot 4esions are divided into si7 grades based on the de0th o6
the -o&nd and e7tent o6 tiss&e ne"rosis. #in"e these grades
6ai4 to "onsider the im0ortant ro4es o6 in6e"tion, is"hemia, and
other "omorbid 6a"tors, s&bseL&ent a&thors have modi6ied the
"4assi6i"ation system by in"4&ding
S'/ TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
22/78
PAT01AY 3
-
8/10/2019 Pie Diabetico Now-1
23/78
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S'
-
8/10/2019 Pie Diabetico Now-1
24/78
des"ri0tors 6or these "onsiderations ?*2, 2, 21@. For
e7am04e, the Bniversity o6 Te7as #an Antonio ?BT#A@ sys
tem ?Tab4e *@ asso"iates 4esion de0th -ith both is"hemia and
in6e"tion ?2@. This system has been va4idated and is
genera44y 0redi"tive o6 o&t"ome, sin"e in"reasing grade and
stage o6 -o&nds are 4ess 4ike4y to hea4 -itho&t revas"&4ar
i)ation or am0&tation ?2, 2@. The BT#A system is no-
-ide4y &sed in many "4ini"a4 tria4s and diabeti" 6oot "enters.
Another hybrid system, the P8D=# system, eva4&ates 6ive
basi" "hara"teristi"s5 0er6&sion, e7tentsi)e, de0thtiss&e 4oss,
in6e"tion and sensation ?2$@ ?Tab4e @. 3hi4e this system
has yet to be va4idated, it 0rovides the bene6it o6 having been
deve4o0ed by a "onsens&s body.
=maging st&dies 04ay an im0ortant ro4e in the assessment
and eva4&ation o6 the diabeti" 6oot &4"er ?1, 1, 1,
1@. P4ain 7rays are indi"ated based on the e7tent and
nat&re o6 the &4"er. /4ini"a4 "hange in the a00earan"e o6 the
&4"er or 6ai4&re to hea4 -ith a00ro0riate treatment may di"
tate re0eating the radiogra0h 0eriodi"a44y to monitor 6or
osseo&s invo4vement ?@. Additiona4 imaging moda4ities
s&"h as n&"4ear medi"ine s"ans, &4trasonogra0hy, MR=, and
/T may be indi"ated, de0ending on the "4ini"a4 0i"t&re.
These moda4ities have been 0revio&s4y dis"&ssed in this
do"&ment.
Fig&re * s&mmari)es the im0ortant e4ements o6 the over
a44 assessment o6 the 0atient -ith a diabeti" 6oot &4"er. The
assessment addresses &nder4ying 0atho0hysio4ogy, 0ossib4e
"a&sa4 6a"tors, and signi6i"ant 0redi"tors o6 o&t"ome ?2',
$, '$, 1, 22@.
Tr!",#" of Di!="ic Ulcrs: G&ii#% Pri#ci-ls
The 0rimary treatment goa4 6or diabeti" 6oot &4"ers is to
obtain -o&nd "4os&re as e70editio&s4y as 0ossib4e. Reso4ving
6oot &4"ers and de"reasing the re"&rren"e rate "an
4o-er the 0robabi4ity o6 4o-er e7tremity am0&tation in the
diabeti" 0atient ?, $, 1*2, 1*, 2'2@. The 3o&nd
Hea4ing #o"iety de6ines a "hroni" -o&nd as one that has
6ai4ed to 0ro"eed thro&gh an order4y and time4y re0air 0ro"ess
to 0rod&"e anatomi" and 6&n"tiona4 integrity ?2@. A "hroni"
-o&nd is 6&rther de6ined as one in -hi"h the hea4ing "as"ade
has been disr&0ted at some 0oint, 4eading to 0ro4onged
in64ammation and 6ai4&re to ree0ithe4ia4i)e and a44o-ing 6or6&rther breakdo-n and in6e"tion. 8ar4y advan"ed or
a00ro0riate -o&nd "are 0ra"ti"es may be more "oste66e"tive
than standard "are 0ra"ti"es 6or de"reasing the in"iden"e o6
4o-er e7tremity am0&tations ?$, 2@.
The essentia4 thera0e&ti" areas o6 diabeti" &4"er manage
ment are as 6o44o-s5 management o6 "omorbidities: eva4&a
tion o6 vas"&4ar stat&s and a00ro0riate treatment: assess
ment o6 4i6esty4e0sy"hoso"ia4 6a"tors: &4"er assessment
and eva4&ation: tiss&e management-o&nd bed 0re0aration:
and 0ress&re re4ie6.
ana5e1en of Co1or3i4iies
>e"a&se diabetes is a m&4tiorgan systemi" disease, a44
"omorbidities that a66e"t -o&nd hea4ing m&st be assessed and
managed by a m&4tidis"i04inary team 6or o0tima4 o&t"omes in
the diabeti" 6oot &4"er ?1*1*', 1, 2, 21@. Many
systemi" mani6estations a66e"t -o&nd hea4ing. Among the
most "ommon "omorbidities are hy0erg4y"emia and vas"&4ar
diseases s&"h as "erebra4 vas"&4ar a""idents, transient
is"hemi" atta"ks, myo"ardia4 in6ar"tions, angina, va4v&4ar
heart disease, atria4 6ibri44ation, ane&rysms, rena4 dys6&n"tion,
hy0ertension, hy0er"ho4estero4emia, and hy0er4i0idemia ?$,
2', 2$@.
Evaluaion of as/ular %aus
Arteria4 0er6&sion is a vita4 "om0onent 6or hea4ing and
m&st be assessed in the &4"erated 0atient, sin"e im0aired
"ir"&4ation "ontrib&tes signi6i"ant4y to nonhea4ing o6
&4"ers and s&bseL&ent risk 6or am0&tation ?'2, , , 21$,
'@. 8ar4y eva4&ation and re6erra4 are im0ortant ?1@.
#ym0toms o6 vas"&4ar ins&66i"ien"y may in"4&de edema,
a4tered skin "hara"teristi"s ?4a"k o6 hair, diseased nai4s,
a4tered moist&re@, s4o- hea4ing, "oo4 or "o4d e7tremities,
and im0aired arteria4 0&4sation. !as"&4ar re"onstr&"tive
s&rgery o6 the o""4&ded 4imb im0roves 0rognosis and may
be reL&ired 0rior to debridement, 6oot s0aring s&rgery, and
0artia4 am0&tation ?, 22, *, @.
Assess1en of Lifesle-Ps/hoso/ial "a/ors
+i6esty4e and 0sy"hoso"ia4 6a"tors may in64&en"e -o&ndhea4ing. For e7am04e, smoking has a 0ro6o&nd e66e"t on
S29 TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
25/78
-o&nd hea4ing d&e to its asso"iated vaso"onstri"tion and
4o- o7ygen"arrying "a0a"ity o6 b4ood ?, @. Ither
6a"tors ?eg, a4"oho4 and dr&g ab&se, eating habits, obesity,ma4n&trition, and mobi4ity and a"tivity 4eve4s@ sho&4d a4so
be noted. =n addition, de0ression and menta4 i44ness may
im0a"t the o&t"ome o6 treatment, sin"e these "onditions
"an dire"t4y a66e"t the 0atients adheren"e to
re"ommendations and attit&de to-ards hea4ing ?1, 11@.
Ul/er Assess1en an4 Evaluaion
The im0ortan"e o6 a thoro&gh and systemati" eva4&ation o6
any &4"eration "annot be overem0hasi)ed: indeed, the 6indings
o6 an &4"ers0e"i6i" e7amination -i44 dire"t4y g&ide
s&bseL&ent treatment ?2', 1@. =nitia4 eva4&ation and
detai4ed des"ri0tion o6 any &4"er sho&4d en"om0asses 4o"a
tion, si)e, de0th, sha0e, in64ammation, edema, e7&date?L&a4ity and L&antity@, 0ast treatment, and d&ration ?12,
22@. The margins o6 the &4"er sho&4d be assessed 6or "a44&s
6ormation, ma"eration, and erythema. The 0resen"e o6 ery
thema a4ong -ith other signs s&"h as tenderness and
-armth might s&ggest in6e"tion ?12@. The L&a4ity o6 the
tiss&e ?ie, moist, gran&4ar, desi""ated, ne"roti", &ndermin
ing, s4o&gh, es"har, or 4iL&e6ied@ sho&4d be noted ?1@.
Thoro&gh eva4&ation is &sed to determine the 0resen"e o6
sin&s tra"k or dee0 abs"ess.
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S2'
-
8/10/2019 Pie Diabetico Now-1
26/78
FreL&ent reeva4&ation -ith res0onsedire"ted treatment
is essentia4. In"e the &4"er is hea4ed, management "onsistso6 de"reasing the 0robabi4ity o6 re"&rren"e.
Tissue ana5e1en - =oun4 'e4 Pre7araion
Debridement. Debridement o6 ne"roti" tiss&e is an inte
gra4 "om0onent in the treatment o6 "hroni" -o&nds sin"e they
-i44 not hea4 in the 0resen"e o6 &nviab4e tiss&e, debris, or
"riti"a4 "o4oni)ation ?1$, 1'@. Bndermined tiss&e or "4osed
-o&nd s0a"es -i44 other-ise harbor ba"teria4 gro-th ?12,1*, 1@. Debridement serves vario&s 6&n"tions5 remova4 o6
ne"roti" tiss&e and "a44&s: red&"tion o6 0ress&re: eva4&ation o6
the -o&nd bed: eva4&ation o6 tra"king and t&nne4ing: and
red&"tion o6 ba"teria4 b&rden ?1, 1@. Debridement
6a"i4itates drainage and stim&4ates hea4ing ?2@. Ho-ever,
debridement may be "ontraindi"ated in arteria4 &4"ers ?21@.
Additiona44y, e7"e0t in avas"&4ar "ases, adeL&ate debridement
m&st a4-ays 0re"ede the a004i"ation o6 to0i"a4 -o&nd hea4ing
agents, dressings, or -o&nd "4os&re 0ro"ed&res ?, 2, 22,
2@. I6 the 6ive ty0es o6 debridement ?s&rgi"a4, en)ymati",
a&to4yti", me"hani"a4, bio4ogi"a4@, on4y s&rgi"a4 debridement
has been 0roven to be e66i"a"io&s in "4ini"a4 tria4s ?2@.
Surgical debridement. #&rgi"a4 debridement is the "or
nerstone o6 management o6 diabeti" 6oot &4"ers. Thoro&gh
shar0 debridement o6 a44 nonviab4e so6t tiss&e and bone
6rom the o0en -o&nd is a""om04ished 0rimari4y -ith a
s"a40e4, tiss&e ni00ers, "&rettes, and "&rved s"issors ?2$@.
87"ision o6 ne"roti" tiss&e e7tends as dee04y and 0ro7ima4
Fi%&r )Assess1enofa 4ia3ei/ foo ul/er
in/lu4es no onl a
4es/ri7ion of he s.in
lesion 3u also he fin4:
in5s ne/essar for a//u:rae assess1en of he
/onri3uin5 fa/ors an4
eiolo58
4y as ne"essary &nti4 hea4thy, b4eeding so6t tiss&e and bone
are en"o&ntered. Any "a44&s tiss&e s&rro&nding the &4"er
m&st a4so be removed. The main 0&r0ose o6 s&rgi"a4
debridement is to t&rn a "hroni" &4"er into an a"&te, hea4ing
-o&nd ?2'@. A diabeti" &4"er asso"iated -ith a dee0
abs"ess reL&ires hos0ita4 admission and immediate in"ision
and drainage ?1@. %oint rese"tion or 0artia4 am0&tation o6
the 6oot is ne"essary i6 osteomye4itis, oint in6e"tion, or
gangrene are 0resent ?$1, 1, 12, 1'1, 1, 21@. The
0rin"i04es g&iding the s&rgi"a4 management o6 diabeti"
6oot &4"ers are dis"&ssed &nder J#&rgi"a4 Management o6
the Diabeti" Foot.K
-
8/10/2019 Pie Diabetico Now-1
27/78
?2, @. Among its 0ro0erties are 0re"ision, se4e"tive"&tting, and minima4 therma4 damage to the tiss&es ?1@.
3hen s&rgi"a4 or shar0 debridement is not indi"ated,
other ty0es o6 debridement "an be &sed. For e7am04e, vas
"&4ar -o&nds may bene6it 6rom en)ymati" debridement,
-hi4e an e7treme4y 0ain6&4 -o&nd may bene6it 6rom
a&to4yti" debridement. Me"hani"a4 debridement is o6ten
&sed to "4eanse -o&nds 0rior to s&rgi"a4 or shar0 debridement. =n areas -here the medi"a4 sta66 is not trained in s&r
gi"a4 or shar0 debridement, these other 6orms o6 debride
ment may be &se6&4 ?2'@.
+n&ymatic debridement. A high4y se4e"tive method, en)y
mati" debridement "onsists o6 the a004i"ation o6 e7ogeno&s
0roteo4yti" en)ymes man&6a"t&red s0e"i6i"a44y 6or -o&nd
debridement. !ario&s en)ymes have been deve4o0ed,
in"4&ding ba"teria4 "o44agenase, 04ant derived 0a0ain&rea,
6ibrino4ysinD
-
8/10/2019 Pie Diabetico Now-1
28/78
S2$ TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
29/78
Advanced !ound "are Modalities. 3o&nd bed 0re0a
ration o66ers "4ini"ians a "om0rehensive a00roa"h to remov
ing barriers to hea4ing and stim&4ating the hea4ing 0ro"ess so
that the bene6its o6 advan"ed -o&nd "are "an be ma7imi)ed
?1$, '@. Advan"ed "are may sometimes be the on4y means
o6 ra0id4y and e66e"tive4y attaining -o&nd "4os&re ?*@. The
advent o6 thera0e&ti" gro-th 6a"tors, gene thera0y, tiss&e
engineered "onstr&"ts, stem "e44 thera0y, and other dr&gs anddevi"es that a"t thro&gh "e44&4ar and mo4e"&4arbased
me"hanisms is enab4ing the modern s&rgeon and -o&nd"are
0rovider to a"tive4y 0romote -o&nd angiogenesis to
a""e4erate hea4ing ?*1*@.
0rowth factor therapy. /hroni" &4"ers have demonstrated
bene6it 6rom a&to4ogo&s 04ate4et re4easates or geneti"a44y
engineered 0rod&"ts s&"h as re"ombinant D
-
8/10/2019 Pie Diabetico Now-1
30/78
>i4ayered skin s&bstit&tes ?4iving "e44s@ in"4&de bi4ayered skin
eL&iva4ent ?A04igra6
@ and "&4t&red "om0osite skin ?Ir/e4
bi4ayered "e44&4ar matri7, Irte"h =nternationa4, =n"., I@ has sho-n 0romise in
the treatment o6 diabeti" 6oot -o&nds -ith hy0o7ia severe
eno&gh to inter6ere -ith hea4ing ?2@. Ho-ever, most o6
the H>I st&dies -ere ham0ered by methodo4ogi"a4 errors that0re"4&de any de6inite ro4e 6or this moda4ity in the ro&tine
treatment o6 diabeti" 6oot &4"ers ?2, , @.
-
8/10/2019 Pie Diabetico Now-1
31/78
Fi%&r / Dia3ei/ foo ul/ers are 1os ofen lo/ae4 un4er ;ei5h3earin5 areas of he foo8 Essenials of
1ana5e1en in/lu4e @off:loa4in5 of he foo or area of ul/eraion8 eale4 ul/ers 1a 3e 1ana5e4 ;ih shoes
an4 variaions of 1ol4e4 or 1uli7le 4ensi insoles, ;hile he oal /ona/ /as re1ains he san4ar4
a77roa/h o off:loa4in5 areas of ul/eraion8
ments based on the "4ini"a4 0rogress o6 the -o&nd. 8ven as
sim04e a method as a 6e4ted 6oam a0ert&re 0ad has been 6o&nd
to be e66e"tive in removing 0ress&re and 0romoting hea4ing o6
6oot &4"ers ?$1$21@. A st&dy 0&b4ished in 21 noted that
&se o6 a tota4 "onta"t "ast ?T//@ hea4ed a higher 0ortion o6
-o&nds in a shorter time than a ha46 shoe or removab4e "ast
-a4ker ?R/3@ ?$1$@. More re"ent4y, investigators "om0ared
T// &se -ith that o6 a removab4e "ast -a4ker that -as
rendered irremovab4e ?iT//@ by "ir"&m6erentia4 -ra00ing o6
an R/3 -ith a sing4e stri0 o6 6iberg4ass "asting materia4.
They "on"4&ded that the 4atter may be eL&a44y e66i"a"io&s,
6aster to 04a"e, easier to &se, and 4ess e70ensive than T// in
the treatment o6 diabeti" ne&ro0athi" 04antar 6oot &4"ers
?$22@. The 6indings o6 this st&dy and another st&dy a4so
s&ggest that modi6i"ation o6 the R/3 into an irremovab4e
devi"e may im0rove 0atient "om04ian"e, thereby in"reasing
the 0ro0ortion o6 hea4ed &4"ers and
the rate o6 hea4ing o6 diabeti" ne&ro0athi" -o&nds [email protected] o6 the moda4ity se4e"ted, no 0atient sho&4d
ret&rn to an &nmodi6ied shoe &nti4 "om04ete hea4ing o6 the
&4"er has o""&rred ?, , , 2''@. F&rthermore, any shoe
that res&4ted in the 6ormation o6 an &4"er sho&4d never
again be -orn by the 0atient.
1os T*!" F!il "o 0!l
3o&nds that do not res0ond to a00ro0riate "are,
in"4&ding debridement, o664oading, and to0i"a4 -o&nd
thera0ies, m&st be reassessed. =n6e"tion and is"hemia are
es0e"ia44y im0ortant "onsiderations and "ommon reasons
6or 6ai4&re to hea4.
The 0resen"e o6 in6e"tion m&st be determined and identi
6ied as either so6t tiss&e, osseo&s, or both. 87"essive
biob&rden "an be indi"ated by 0a4e or 6riab4e gran&4ation
tiss&e, 0ersistent drainage, or 6ibrino&s s&r6a"e 4ayer ?1$@.
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S2.
-
8/10/2019 Pie Diabetico Now-1
32/78
=ndi"ators 6or 6rank in6e"tion -i44 a4so in"4&de 0ain ?es0e
"ia44y in the ne&ro0athi" 0atient@, erythema, and ind&ration.
3hen bone or oint is visib4e or 0a40ab4e at the de0th o6 the&4"er, osseo&s in6e"tion be"omes more 4ike4y ?2', $2@. A
thoro&gh dis"&ssion o6 the management o6 in6e"ted
-o&nds is 0resented 4ater in this do"&ment and
s&mmari)ed in Path-ay $.
Bnre"ogni)ed is"hemia -i44 a4so im0air -o&nd hea4ing and
m&st be diagnosed 0rior to deve4o0ment o6 in6e"tion or
is"hemi" ne"rosis o6 the &4"er. 3hen no 0rogress or en4arge
ment o6 the -o&nd has taken 04a"e, ree7amination o6 the
vas"&4ar stat&s o6 the e7tremity is -arranted ?Path-ay 2@. This
sho&4d in"4&de arteria4 Do004er segmenta4 0ress&res -ith
-ave6orms, digita4 arteria4 0ress&res, or meas&rement o6
trans"&taneo&s o7ygen 0artia4 0ress&res ?T"PI2@ ?'2, 212@.!as"&4ar s&rgi"a4 "ons&4tation sho&4d a4so be "onsidered 6or
6&rther eva4&ation and treatment.
Ither 0arameters "riti"a4 to -o&nd hea4ing sho&4d a4so be
addressed, in"4&ding the need 6or 6&rther debridement or a
"hange in o664oading moda4ity.
-
8/10/2019 Pie Diabetico Now-1
33/78
PAT01AY $
-
8/10/2019 Pie Diabetico Now-1
34/78
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S2
-
8/10/2019 Pie Diabetico Now-1
35/78
be 0resent. Hos0ita4i)ation is reL&ired to treat the in6e"tion
as -e44 as systemi" seL&e4ae. Patients -ith 0oor vas"&4ar
stat&s and is"hemia have an in"reased 0otentia4 6or
am0&tation and reL&ire 0rom0t "ons&4tation 6or 0otentia4
revas"&4ari)ation ?, , 2@.
=n 2$, the =n6e"tio&s Disease #o"iety o6 Ameri"a?=D#A@ deve4o0ed ne- g&ide4ines 6or the diagnosis and
treatment o6 diabeti" 6oot in6e"tions ?12@. The g&ide4ines
in"or0orate the in6e"tion 0ortion o6 the P8D=# system into
=D#As 0re6erred "4ini"a4 "4assi6i"ation 6or in6e"tions in the
diabeti" 6oot ?Tab4e 1@.
Assss,#" of Di!="ic Foo" I#fc"io#s
3hen eva4&ating the 0atient -ith a diabeti" 6oot in6e"tion,
a 0rob4emdire"ted history and 0hysi"a4 e7amination sho&4d
be obtained. A systemati" a00roa"h to the "om04ete
assessment o6 these 0atients is reL&ired, sin"e there is evi
den"e that they are o6ten inadeL&ate4y eva4&ated, even -hen
hos0ita4i)ed ?$1@. The 0ast medi"a4 history sho&4d assess the
0atients ne&ro4ogi", "ardiovas"&4ar, rena4, and dermato4ogi"
stat&s. Bse o6 "&rrent medi"ations as -e44 as 0revio&s
antibioti"s may inter6ere -ith 04anned treatments or indi"ate
that standard treatments -i44 4ike4y be ine66e"tive. Pain sho&4d
be "onsidered an &nre4iab4e sym0tom in ttindivid&a4s -ith
0eri0hera4 ne&ro0athy. The 0atient sho&4d be L&es
tioned regarding 0revio&s &4"erations, in6e"tions, tra&ma,and s&rgeries at the 0resent site or at any other 0ast 4o"ationo6 in6e"tion.
/onstit&tiona4 sym0toms ?eg, na&sea, ma4aise, 6atig&e,
vomiting, 6ever, "hi44s@ are im0ortant "4ini"a4 "4&es -hen
0resented -ith an in6e"ted diabeti" 6oot. #evere in6e"tionor se0sis m&st be "onsidered -hen these sym0toms are
0resent. Ho-ever, in abo&t 'C o6 diabeti" 0atients
0resenting -ith signi6i"ant in6e"tion, systemi" signs ?6ever
and 4e&ko"ytosis@ are absent ?1@. FreL&ent4y, the on4y
indi"ation o6 in6e"tion is &ne704ained or re"a4"itrant hy0erg
4 y " e m i a . +aboratory testing might in"4&de a />/ -ith
or -itho&t di66erentia4, b4ood "&4t&res, g4y"osy4ated
hemog4obin, 6asting b4ood s&gar, sedimentation rate, and
&rina4ysis. Ither tests sho&4d be 0er6ormed as indi"ated by
the 0atients "ondition or "omorbidities.
The history o6 the -o&nd or in6e"tion sho&4d in"4&de the
onset, d&ration, and a00earan"e be6ore in6e"tion o6 the area.
De0th or si)e o6 the &4"er, amo&nt o6 drainage, s-e44ing, "o4or,
odor, and e7tent o6 in6e"tion sho&4d be eva4&ated. The
in6e"tion or &4"er sho&4d be 0robed to determine the 0resen"e
o6 bone or oint invo4vement, sin&s tra"ts, or e7tension into
tendon sheaths. The 4atter are "ommon ro&tes 6or the s0read o6
in6e"tion both dista44y and 0ro7ima44y. Re4iab4e aerobi" and
anaerobi" "&4t&res sho&4d be obtained 6rom
S39 TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
36/78
Fi%&r Dia3ei/ foo infe/ions are 5enerall /onsi4ere4 7ol1i/ro3ial, 3e/ause 1uli7le or5anis1s are
fre>uenl foun4 in a ;oun4 1ilieu8 Staphylococcusan4 Streptococcusre1ain he 1os i17oran or5anis1s
/ausin5 infe/ion8
0&r&4ent drainage or "&rettage o6 the &4"er base, sin"e st&d
ies have sho-n good "on"ordan"e -ith the tr&e 0athogen
?11*, $2, $2@. #im04e s-ab "&4t&res o6 an &4"er s&r6a"eare genera44y not advisab4e be"a&se they tend to be &nre4i
ab4e, es0e"ia44y in the 0resen"e o6 osteomye4itis or sin&s
tra"ts ?12, $, $$@.
For 0atients -ith "4ini"a44y &nin6e"ted or nonin64amed
ne&ro0athi" &4"ers, the ro4e o6 antibioti" thera0y is sti44 in
L&estion ?@. There6ore, in these instan"es, -o&nd "&4t&re
is 0robab4y &nne"essary ?12@. =6 osteomye4itis is
s&s0e"ted, bone "&4t&res are ne"essary to make the
de6initive diagnosis and iso4ate the tr&e 0athogen ?1,
$', $*@. Ho-ever, this m&st be ba4an"ed against the
0otentia4 6or "ontaminating nonin6e"ted bone in the
0resen"e o6 an a"tive so6t tiss&e in6e"tion. =ntrao0erative6ro)en se"tion is a4so &se6&4 in assessing 6or dee0 in6e"tion.
The 0resen"e o6 more than ' to 1 ne&tro0hi4s 0er high
0o-er 6ie4d is s&ggestive o6 a"&te in6e"tion ?$@.
The maority o6 -o&nds are "a&sed by Staphylococcus
aureus, betahemo4yti" stre0to"o""i, and other gram 0osi
tive "o""i ?Fig @ ?1'1, $, $@. A4tho&gh "omm&nity
a"L&ired "ases o6 resistant ba"teria4 in6e"tions have been
re0orted, 0atients -ho have been 0revio&s4y hos0ita4i)ed -ith
an o0en -o&nd are more 4ike4y to deve4o0 an in6e"tion 6rom
resistant ba"teria s&"h as methi"i44inresistant S aureus?MR#A@ and van"omy"inresistant entero"o""i ?!R8@ ?$$@.
/hroni" -o&nds may deve4o0 a more "om04e7 assortment o6
ba"teria, in"4&ding gram negative rods, ob4igate anaerobes,
1seudomonas aeruginosa, and entero"o""i.
=maging st&dies are a4so im0ortant in the overa44 assess
ment o6 diabeti" 6oot in6e"tions, not-ithstanding their
short"omings. P4ain 6i4m 7rays may indi"ate the 0resen"e o6
bony erosions andor gas in the so6t tiss&es. =t sho&4d be noted
that the demonstration o6 osteomye4itis by 04ain radiogra0hs
4ags the onset o6 bone invo4vement by 1 to 1$ days ?1,
1@. Radion&"4eotide bone s"ans s&"h as T" may
demonstrate abnorma4 &0take o6 the radion&"4eotide be6ore"hanges are visib4e on radiogra0hs ?1@. This may be 4ess
s0e"i6i" in 0atients -ith 0eri0hera4 ne&ro0athy or -ith any
0ree7isting osseo&s "ondition that "a&ses in"reased bone
t&rnover ?eg, s&rgery, 6ra"t&re, ne&ro0athi" arthro0athy@ ?$$1@.
A "ombination o6 s"ans s&"h as the T"m and an indi&m
4abe4ed 4e&ko"yte s"an or the T"m HMPAI4abe4ed
4e&ko"yte s"an may aid the "4ini"ian in di66erentiat
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S3'
-
8/10/2019 Pie Diabetico Now-1
37/78
ing /har"ot arthro0athy and osteomye4itis -ith greater
a""&ra"y ?1', 1*, 2@. MR= has genera44y s&004anted
the /T s"an in the ear4y diagnosis o6 osteomye4itis ?Fig
1@, d&e to its higher tiss&e "ontrast and abi4ity to dete"t
both so6t tiss&e and marro- in64ammation ?1, 2, 22,
$$2@. Additiona44y, MR= "an be &sed to 6o44o- the
reso4&tion o6 in6e"tion or as an aid in s&rgi"a4 04anning
?21, $$@. Ho-ever, none o6 these imaging moda4ities are
1C sensitive and s0e"i6i" 6or diagnosing or r&4ing o&t
bone in6e"tion. F&rthermore, these tests are e70ensive and
may not be readi4y avai4ab4e. A00ro0riate "4ini"a4
assessment and diagnosti" a"&men sho&4d there6ore
remain the g&iding 0rin"i04es to management.
Tr!",#" of Di!="ic Foo" I#fc"io#s
Diabeti" 6oot in6e"tions sho&4d be managed thro&gh am&4tidis"i04inary team a00roa"h &ti4i)ing a00ro0riate "on
Fi%&r '9 (A)This 4ia3ei/ foo infe/ion is >uie
severe, ;ih ne/roi/ s.in 4efe/s an4 sof issue
sinus for1aion8 (B)An RI reveale4 1arro;
e4e1a an4 a49a/en flui4 a//u1ulaion o he firs
1eaarsal in4i/aive of oseo1eliis an4 a3s/ess8
(C)A17uaion of he 5rea oe an4 4isal firs
1eaarsal ;as 7erfor1e4, 3u (D)re/urren infe/:ion o//urre4 an4 follo;:u7 ra4io5ra7hs reveale4
a/ive 7roliferaive /han5es of he re1ainin5 firs1eaarsal8 (E)This 7aien ;as 3rou5h 3a/. o
sur5er for a44iional 3one rese/ion8
s&4tations ?1, 1, @. Hos0ita4i)ation o6 0atients -ith
4imbthreatening in6e"tions is mandatory. A44 diabeti" 6oot
in6e"tions m&st be monitored "4ose4y. 8L&a44y im0ortant 6or
the best 0ossib4e o&t"ome are 0atient "om04ian"e and ed&
"ation, es0e"ia44y in o&t0atient management.
Trea1en of Non:Li13:Threaenin5 Infe/ions
Treatment o6 diabeti" 6oot in6e"tions is g&ided by the
severity o6 the in6e"tion. As 0revio&s4y dis"&ssed, non4imb
threatening in6e"tions invo4ve s&0er6i"ia4 &4"erations -itho&t
signi6i"ant is"hemia and they do not invo4ve bone or oint
?$@. Ty0i"a44y, "e44&4itis does not e7tend 2 "m beyond the
&4"er margins and there is an absen"e o6 systemi" sym0toms
?e.g. 6ever, "hi44s, na&sea, vomiting@. These 4ess severe
in6e"tions that 6reL&ent4y "om04i"ate diabeti" 6oot &4"ers, may
be initia44y treated in an o&t0atient setting ?$1, $, $$$@.
Many mi4d or moderate in6e"tions are
S32 TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
38/78
monomi"robia4, -ith S aureus, S epidermidis, and stre0to
"o""i the most "ommon 0athogens ?11, 121, $@. Re4iab4e
s0e"imens 6or "&4t&res may be obtained thro&gh "&rettage o6
the in6e"ted &4"er ?12, 12, $$', $$*@. =n addition to the
standard treatment 6or &4"erations ?ie, non-eightbearing and
dressing "hanges@, ora4 antibioti" thera0y is &s&a44y s&66i"ient
as initia4 thera0y ?Tab4e 11@. Antimi"robia4 treatment sho&4d
be started as soon as 0ossib4e -ith an agent 0rovidingadeL&ate gram 0ositive "overage, re"ogni)ing that gram
negative organisms might a4so be invo4ved ?2, $, $@.
A4tho&gh the in"iden"e o6 MR#A in6e"tions has in"reased
dramati"a44y in the 0ast severa4 years, methi"i44insensitive S
aureus ?M##A@ remains the most 4ike4y 0athogen in "om
m&nitya"L&ired diabeti" 6oot in6e"tions ?12, $$@.
There6ore, initia4 antibioti" "overage m&st be tai4ored to "over
M##A, &n4ess a re4iab4e "&4t&re and sensitivity is avai4ab4e or
there is a history o6 other 0athogens ?eg, MR#A,
1seudomonas, entero"o""&s@ that reL&ire s0e"i6i"
"overage. Antibioti"s sho&4d be ad&sted a""ording to "&4t&re res&4ts and the 0atients res0onse to treatment.
3hi4e many &se6&4 ora4 antimi"robia4 agents ?eg,
"e0ha4e7in, "4indamy"in, amo7i"i44in"4av&4anate, 4ev
o64o7a"in@ are avai4ab4e 6or managing mi4d to moderate dia
beti" 6oot in6e"tions, re4ative4y 6e- have been st&died or have
demonstrated s&0eriority in 0ros0e"tive randomi)ed "4ini"a4
tria4s ?12@. There6ore, =D#A g&ide4ines "ontain no s0e"i6i"re"ommendations 6or antimi"robia4 regimens in the
management o6 diabeti" 6oot in6e"tions.
A44 antibioti" treatments sho&4d be monitored 6or deve4
o0ment o6 resistan"e. Most "ases o6 "e44&4itis res0ond -ith
in to ' days o6 initiation o6 a00ro0riate antibioti"s. =6 "e4
4&4itis is s4o- to res0ond, -orsens, or re"&rs 6o44o-ing sev
era4 days o6 treatment, the &4"eration sho&4d be reassessed
and 0ossib4y re"&4t&red. >a"teria 6reL&ent4y deve4o0 resist
an"e to an antimi"robia4 agent, es0e"ia44y -ith 0ro4onged t
h e r a 0 y. This is not &n"ommon -ith the L&ino4ones.
-
8/10/2019 Pie Diabetico Now-1
39/78
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S33
-
8/10/2019 Pie Diabetico Now-1
40/78
#&0erin6e"tion "an a4so deve4o0 -hen antibioti"s se4e"t o&t
o00ort&nisti" organisms, as in the "ase o6 1seudomonasor
yeast ?$andida s0@. >e"a&se MR#A in6e"tions have
be"ome in"reasing4y more "ommon 0athogens and are
asso"iated -ith 0rior antimi"robia4 e70os&re ?$$, $$@,
0atients -ith "4ini"a4 in6e"tion and a 0rior history o6
MR#A sho&4d be "onsidered to have the same 0athogen
&nti4 0roven other-ise and treated a""ording4y.Antimi"robia4 thera0y a4one is not s&66i"ient 6or treating
in6e"tions asso"iated -ith 6oot &4"ers ?22, $$, $'@. The
-o&nd sho&4d be assessed and "4eansed thoro&gh4y, &sing
0ro0er debridement as indi"ated. 3hi4e there are severa4
to0i"a4 antimi"robia4 agents that "an be &sed on the in6e"t
ed -o&nd, there is 4itt4e data on to0i"a4 treatment ?2@.
There6ore, s&"h thera0y at 0resent "an on4y be "onsidered
ad&n"tive to systemi" antimi"robia4 thera0y.
The -o&nd sho&4d be managed a""ording to the 0rin"i
04es dis"&ssed 0revio&s4y. Most im0ortant4y, the 0atient
sho&4d be reassessed -ithin $ to 2 ho&rs. =6 no im0rove
ment is noted, hos0ita4i)ation -ith intraveno&s antibioti"s
sho&4d be "onsidered. Management o6 this ty0e o6
in6e"tion sho&4d a4so in"4&de "4ose monitoring o6 the
0atients hy0erg4y"emia and genera4 hea4th stat&s. Patient
"om04ian"e as -e44 as a red&"tion in the 0ress&re o6 the
in6e"ted 4imb m&st be "onsidered ear4y on in the treatment
o6 any diabeti" 6oot in6e"tion ?, $'1@.
Trea1en of Li13:Threaenin5 Infe/ions
>y de6inition, 4imbthreatening in6e"tions are m&"h more
serio&s and more o6ten a"&te "om0ared -ith the mi4der non
4imbthreatening in6e"tions. =n the P8D=# system ?Tab4e 1@,
4imbthreatening in6e"tions are "4assi6ied as grade or $,
de0ending on severity and the 0resen"e o6 systemi" man
i6estations ?122, 12, $'2@.
-
8/10/2019 Pie Diabetico Now-1
41/78
a4, or genera4 anestheti"s. Ho-ever, s0ina4 b4o"ks are ty0i"a44y avoided in 0atients -ho may be se0ti".
8ven the si"kest o6 0atients sho&4d be "onsidered 6or
emergent in"ision, drainage, and debridement 0ro"ed&res,
be"a&se their i44ness in this regard is dire"t4y attrib&tab4e to
the in6e"tion severity. #&"h 4i6ethreatening in6e"tions
ne"essitate immediate s&rgi"a4 attention, -itho&t de4ay in
obtaining radio4ogi" or medi"a4 -ork&0 o6 other "omorbid"onditions ?$1, , $*2, $*@. Po4ymi"robia4 in6e"tion sho&4d
be anti"i0ated in these 0atients ?Fig @, -ith a variety o6 gram
0ositive "o""i, gram negative rods, and anaerobi" organisms
0redominating ?2, $*', $**@. A""ording4y, em0iri"a4
antibioti" thera0y ty0i"a44y in"4&des broads0e"tr&m
"overage 6or more "ommon iso4ates 6rom ea"h o6 these three
"ategories ?Tab4e 11@. F&44y "om0rehensive em0iri" "overage
is &s&a44y &nne"essary &n4ess the in6e"tion is 4i6ethreatening
?11, 12@.
Hos0ita4 thera0ies are &s&a44y initiated -ith intraveno&s
medi"ations, a4tho&gh most ora4 64&oroL&ino4ones and ora4
4ine)o4id have the same bioavai4abi4ity as 0arentera4 thera0y
?11, $, $*@. In"e -o&nd "&4t&re res&4ts be"ome
avai4ab4e, the initia4 antimi"robia4 thera0y may reL&ire
ad&stment to 0rovide more s0e"i6i" "overage or 0rovide
thera0y against resistant organisms "a&sing 0ersisting in6e"
tion. Re"ent eviden"e a4so s&00orts the e66i"a"y o6 initia4
0arentera4 thera0y 6o44o-ed by the a00ro0riate ora4 agent in
the management o6 these 0atients ?$, $**, $*@. =6 the
0atient deve4o0s eviden"e o6 re"&rrent in6e"tion -hi4e
re"eiving antibioti" thera0y, re0eat "&4t&res sho&4d be
obtained to assess 6or s&0erin6e"tion. Methi"i44inresistant
sta0hy4o"o""i, -hi"h have emerged as im0ortant 0athogens
in "hroni"a44ytreated diabeti" 6oot &4"er 0atients ?$$,
$$@, m&st be dete"ted ear4y and treated a00ro0riate4y to
avoid 6&rther tiss&e 4oss or e7tension o6 in6e"tion.
The s&rgi"a4 -o&nd may reL&ire re0eated s&rg i " a 4debridement to "om04ete4y eradi"ate in6e"tion and so6t tis
s&e ne"rosis ?$'1, $*, $*@. 3o&nd "are is initiated onday 1 or day 2 0osts&rgery and may initia44y invo4ve sa4inega&)e dressing "hanges. Ither dressings may be &sed to aid
in hea4ing.
-
8/10/2019 Pie Diabetico Now-1
42/78
i" thera0y 2$ to $ ho&rs 0res&rgery to im0rove "&4t&re
a""&ra"y. A diagnosis o6 osteomye4itis reL&ires that both
"&4t&re and bio0sy st&dies revea4 0ositive 6indings, in"4&d
ing ne"rosis, "hroni" in64ammatory in6i4trates, and 0ositive
iso4ation o6 ba"teria ?1@. Rese"tion o6 in6e"ted bone -ith
or -itho&t 4o"a4 am0&tation and "on"&rrent antimi"robia4
thera0y is the most o0tima4 management 6or osteomye4itis
?12$, $@. Ho-ever, the ro&tine need 6or s&rgery in this"ondition has re"ent4y been L&estioned ?$'@. =n some
"ases, based on 0atient morbidity or 0re6eren"es, medi"a4
thera0y a4one 6or osteomye4itis might be -arranted ?12@.
=6 the a66e"ted bone has been "om04ete4y rese"ted or
am0&tated, the in6e"tion may be treated as a so6t tiss&e
in6e"tion. Ho-ever, i6 resid&a4 bone is 0resent in the
-o&nd, the 0atient -i44 4ike4y reL&ire $ to -eeks o6
antibioti" thera0y based on the "&4t&re res&4ts ?11, 2@.
=ntraveno&s or ora4 agents may be &sed, de0ending on the
mi"robia4 iso4ates and in6e"tion severity ?12@. Antibioti"
im0regnated bone "ement has been advo"ated 6or treatment o6
osteomye4itis, b&t it sho&4d on4y be &sed i6 the bone has been
thoro&gh4y debrided and the so6t tiss&e enve4o0e is adeL&ate
6or -o&nd "4os&re 6o44o-ing antibioti"im0regnated bead
04a"ement ?$1, $2@. Gentami"in, tobramy"in, or
van"omy"in are ty0i"a44y &sed in the beads. =t is genera44y
re"ommended that antibioti" beads be removed 2 -eeks or so
a6ter 04a"ement. An a4ternative to bone "ement is absorbab4e
bone gra6t s&bstit&tes mi7ed -ith antibioti" 0o-der ?$@.
The 0e44ets are grad&a44y resorbed as the antibioti" is e4&ted,
th&s o66ering the advantage o6 avoiding a se"ond o0eration 6or
remova4. 3hi4e -ide4y &sed in this regard, st&dies are 4a"king
as to the e66i"a"y o6 either moda4ity "om0ared -ith systemi"
antimi"robia4 thera0y a4one. =6 the in6e"tion 6ai4s to res0ond to
thera0y, the 0atient sho&4d be 6&44y reassessed as 0revio&s4y
dis"&ssed.
DIABETIC CHARCOT FOOT (NEUROPATHIC
OSTEOARTHROPATHY) (Pathway 5)
/har"ot 6oot ?ne&ro0athi" osteoarthro0athy@ is a 0rogres
sive "ondition "hara"teri)ed by oint dis4o"ation, 0atho4ogi"
6ra"t&res, and severe destr&"tion o6 the 0eda4 ar"hite"t&re.
This "ondition "an there6ore res&4t in debi4itating de6ormity or
even am0&tation ?12, 11, 11', $$@.
E"iolo%6 of N&ro-!"*ic Os"o!r"*ro-!"*6
The etio4ogy o6 /har"ot ne&roarthro0athy is most 4ike4y
a "ombination o6 the e66e"ts invo4ved in the ne&rovas"&4ar
and ne&rotra&mati" theories ?, 12, 1, 1', 1, 1$,
$'$@. Tra&ma s&0erim0osed on a severe4y ne&ro0athi"
e7tremity is the most -ide4y a""e0ted theory regarding the
deve4o0ment o6 an a"&te /har"ot 6oot ?$@. As a res&4t o6
asso"iated a&tonomi" ne&ro0athy, b4ood 64o- to the 6oot
in"reases, res&4ting in osteo0enia and attendant -eakness
o6 the bone ?1, 1, $*, $, $@. >e"a&se o6 the 4oss
o6 0rote"tive sensation that a""om0anies 0eri0hera4 sensory
ne&ro0athy, the 0atient is &na-are o6 the initiating tra&ma
and the 0ro6o&nd osseo&s destr&"tion that o6ten o""&rs d&r
ing amb&4ation. A vi"io&s "y"4e ens&es in -hi"h the 0atient"ontin&es to -a4k on the in&red 6oot, a44o-ing 6&rther
damage to o""&r ?12, 1$, $, $1@ ?Fig 12@.
There is good eviden"e s&ggesting that the e66e"ts o6
ne&ro0athy "ombined -ith asso"iated vas"&4ar res0onse
are invo4ved in the deve4o0ment o6 /har"ot arthro0athy
?$, $2@. Additiona44y, re"ent 6indings s&ggest that ty0e 1
diabetes may have a greater 0re0onderan"e o6 de"reased
bone density than ty0e 2 diabetes ?1, $@. F&rthermore,
the age o6 onset 6or a"&te /har"ot arthro0athy a00ears to be
4o-er 6or ty0e 1 than ty0e 2 diabetes. +arge "ohorts o6
0atients or 0atients -ith ty0e 2 diabetes a4one tend to be in
their si7th to seventh de"ades at 0resentation, -hi4e
0atients -ith ty0e 1 diabetes genera44y deve4o0
ne&roarthro0athy in the 6o&rth to 6i6th de"ades ?$, $,
$$@. !ario&s metabo4i" 6a"tors have a4so been im04i"ated
as 0otentia44y etio4ogi". Ine re"ent theory re"eiving m&"h
interest is the ro4e o6 0roin64ammatory "ytokines and the
RA
-
8/10/2019 Pie Diabetico Now-1
43/78
PAT01AY (
-
8/10/2019 Pie Diabetico Now-1
44/78
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S3.
-
8/10/2019 Pie Diabetico Now-1
45/78
Fi%&r '2 Dia3ei/ neuroarhro7ah, or Char/o foo, is 3elieve4 o 3e a neurolo5i/all:1e4iae4 /o1:
7li/aion of 4ia3ees, ;ih he 4evelo71en 1o4ifie4 3 1us/ulos.eleal sress8 The resul is osseous fra5:
1enaion an4 9oin su3luBaion ;ih ofen si5nifi/an 1or7holo5i/ /han5es in he ar/hie/ure of he foo8
Co17li/aions of he Char/o foo in/lu4e ul/eraion un4er areas of 3on 7ro1inen/e an4 7oenial a17u:
aion ofen relae4 o infe/ion-oseo1eliis ha 4evelo7s a49a/en o he area of ul/eraion8
S3/ TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
46/78
=6 the 0atient 0resents -ith a -arm, edemato&s, erythema
to&s, insensate 6oot, 04ain radiogra0hs are inva4&ab4e in
as"ertaining 0resen"e o6 osteoarthro0athy ?$, $$@. =n most
"ases, no 6&rther imaging st&dies are reL&ired to make the
"orre"t diagnosis. 3ith a "on"omitant -o&nd, it may be
di66i"&4t to di66erentiate a"&te /har"ot arthro0athy 6rom
osteomye4itis &sing 04ain radiogra0hs a4one ?1, 1@.
Additiona4 4aboratory st&dies may 0rove &se6&4 in arriving at a"orre"t diagnosis. The -hite b4ood "e44 "o&nt ?3>/@ -ith a
4e6t shi6t -i44 o6ten be e4evated in a"&te osteomye4itis,
a4tho&gh this "an be b4&nted in diabeti" 0atients ?$'@. 3hi4e
the erythro"yte sedimentation rate and /rea"tive 0rotein 4eve4
may a4so be e4evated in a"&te in6e"tion, they o6ten res0ond
simi4ar4y to any in64ammatory 0ro"ess and are there6ore
nons0e"i6i". >one bio0sy, -hen indi"ated, is the most s0e"i6i"
method 6or disting&ishing osteomye4itis 6rom
osteoarthro0athy in these "ir"&mstan"es. A bio0sy "onsisting
o6 m&4ti04e shards o6 bone and so6t tiss&e embedded in the
dee0 4ayers o6 synovi&m is 0athognomoni" 6or ne&ro0athi"
osteoarthro0athy ?$'@.
Te"hneti&m bone s"ans are genera44y nons0e"i6i" in
assisting in the di66erentiation bet-een osteomye4itis and
a"&te /har"ot arthro0athy ?1, 1'@. =ndi&m s"anning,
-hi4e more e70ensive, has been sho-n to be more s0e"i6i"
?1, 1, $*@. Additiona4 st&dies to aid in di66erentiating
osteoarthro0athy 6rom osteomye4itis in"4&de bone s"ans
&ti4i)ing T" HMPAI4abe4ed -hite b4ood "e44s, MR=, and
P8T s"anning ?1, 1*, 1, 2@.
Ither sero4ogi" markers "an be he406&4 6or the diagnosis
o6 a"&te /har"ot osteoarthro0athy. A marker 6or in"reased
osteo"4asti" a"tivity, 1/PT ?"arbo7ytermina4 te4o0e0tide o6
ty0e 1 "o44agen@, has been sho-n to be e4evated b&t o""&rs
-itho&t in"reased 4eve4s o6 0ro"o44agen "arbo7ytermina4
0ro0e0tide ?P1/P@, a marker 6or osteob4asti" a"tivity ?$
$@.
-
8/10/2019 Pie Diabetico Now-1
47/78
Fi%&r '3 Dia3ei/ neuroarhro7ah 1a 3e /lassifie4 a//or4in5 o he anao1i/ lo/aion of 9oin
involve1en8 The relaive 7er/ena5e of fre>uen/ of involve1en is 5iven8 (A4a7e4 fro1 %an4ers LJ
an4 "r.3er5 RG8 The High Risk Foot in Diabetes Mellitus, 7@ bra"e in"or0orated into a "&stom shoe ?$, '1,
'1@. The PT> bra"e has re0orted4y de"reased mean rear
6oot 0eak 6or"es by at 4east 2C ?'1@.
There is re"ent interest in the ad&n"tive &se o6 bis0hos
0honate thera0y in a"&te /har"ot arthro0athy to he40 e70edite
"onversion o6 the a"&te 0ro"ess to the L&ies"ent, re0arative
stage ?'1'21@. These 0yro0hos0hate ana4ogs are 0otent
inhibitors o6 osteo"4asti" bone resor0tion and are -ide4y &sed
in the treatment o6 osteo0orosis, Pagets disease, and re64e7
sym0atheti" dystro0hy syndrome ?', 1@. Ine randomi)ed
tria4 in the B( "om0ared the &se o6 a sin
S$9 TE J!URNAL !" "!!T # AN$LE %URGER&
-
8/10/2019 Pie Diabetico Now-1
48/78
g4e intraveno&s in6&sion o6 0amidronate -ith the &se o6
sa4ine in6&sion ?$@. The treatment gro&0 had signi6i"ant
de"4ines in tem0erat&re and bone t&rnover markers
?deo7y0yridino4ine "ross4inks and bone s0e"i6i" a4ka4ine
0hos0hatase@ in s&bseL&ent -eeks "om0ared -ith the "on
tro4 gro&0, b&t no di66eren"es in "4ini"a4 or radiogra0hi"
o&t"omes -ere re0orted. A sma44 tria4 "om0aring *
months o6 ora4 a4endronate 04&s o664oading -ith standardo664oading a4one in a"&te /har"ot 0atients 6o&nd that the
st&dy gro&0 had signi6i"ant red&"tions in 1/TP and
hydro7y0ro4in, both o6 -hi"h are markers o6 bone
resor0tion and in"reased 6oot bone density ?$@: no
di66eren"es in "4ini"a4 o&t"omes -ere noted.
#imi4ar4y, e4e"tri"a4 bone gro-th stim&4ation has been
a004ied to the management o6 a"&te ne&roarthro0athy to
0romote ra0id "onso4idation o6 6ra"t&res ?'22'2$@. +o-
intensity 0&4sed &4traso&nd ?+=PB#@ has a4so been s&ggest
ed as a &se6&4 ad&n"t in 0romoting hea4ing o6 /har"ot
6ra"t&res ?'2'@. A4tho&gh 0romising in theory, none o6
these ad&n"tive treatments have yet been "on"4&sive4y
0roven e66e"tive thro&gh 4arge 0ros0e"tive m&4ti"enter,
randomi)ed tria4s.
S&r%ic!l M!#!%,#" of C*!rco"
Os"o!r"*ro-!"*6
Re"onstr&"tive s&rgery in a"&te /har"ot may be "onsid
ered i6 a de6ormity or instabi4ity e7ists that "annot e66e"
tive4y be "ontro44ed or a""ommodated by immobi4i)ation
and o664oading ?1*, 1$, $, ', '1, '11, '2*@. =6 the
ne&roarthro0athy is identi6ied in its ear4y stages and non-eightbearing is instit&ted, s&rgery is &s&a44y &nne"essary.
A""ording to "onsens&s o0inion, s&rgery in the a"&te stage
is genera44y nonadvisab4e d&e to the e7treme hy0eremia,
osteo0enia, and edema 0resent ?11, 12, 1$, 1', $,
'11, '2, '2@. Ho-ever, s&rgi"a4 intervention d&ring the
a"&te 0hase may be "onsidered in the 0resen"e o6 a"&te
s&b4&7ation -itho&t osteo"hondra4 6ragmentation ?',
'2@. Ine sma44 series re0orted s&""ess6&4 arthrodeses
rates -ith 0reserved 6oot 6&n"tion in 0atients -ith a"&te
arthro0athy o6 the mid6oot ?'@.
-
8/10/2019 Pie Diabetico Now-1
49/78
DIA'ETIC "!!T DI%!RDER% !LUE *+, NU'ER +, %EPTE'ER-!CT!'ER 2006 S$'
-
8/10/2019 Pie Diabetico Now-1
50/78
so&r"es and -ith vario&s degrees o6 de6ormity 0resent:
there6ore, their rate o6 o0eration on these 0atients does not
re64e"t the tr&e in"iden"e or need 6or s&"h treatment in the
"omm&nity. A re"ent revie- o6 one "enters e70erien"e
-ith mid6oot ne&roarthro0athy in 1 0atients ?21 6eet@
indi"ated that more than ha46 o6 these 0atients "o&4d be
s&""ess6&44y managed -itho&t s&rgery ?'1@. Hen"e, 4arge
0o0&4ationbased st&dies are needed to assess the need 6ors&rgi"a4 intervention and "om0are the e66i"a"y o6 vario&s
"onservative thera0ies ?$$, $, '2@.
The goa4 o6 any s&rgery on the a"&te or "hroni" /har"ot
6oot is to "reate a stab4e, 04antigrade 6oot that may be a00ro
0riate4y a""ommodated ?1$, $, '1, ', '1@. Most
o0erations on "hroni" /har"ot 6eet "onsist o6 e7oste"tomies
6or 0rominent 04antar ?Qro"kerbottomK@ de6ormities "a&s
ing &4"eration -hen the remainder o6 the 6oot is stab4e
?1', '', '11, '2@ ?Fig 1$@.








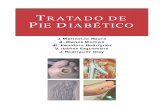
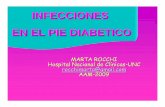
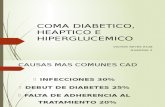


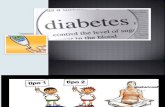
![Pie Diabetico IDSA 2012[1]](https://static.fdocuments.in/doc/165x107/577cdb0b1a28ab9e78a739aa/pie-diabetico-idsa-20121.jpg)



