Learning from Failure: Quality Lessons from 2014- the Year of the Recall Michael Brajac Michael...
21
Learning from Failure: Quality Lessons from 2014- the Year of the Recall Michael Brajac Michael Brajac Consulting Presentation to Toronto Section ASQ February 2015
-
Upload
ophelia-dickerson -
Category
Documents
-
view
214 -
download
0
Transcript of Learning from Failure: Quality Lessons from 2014- the Year of the Recall Michael Brajac Michael...

Learning from Failure: Quality Lessons from 2014-
the Year of the RecallMichael Brajac
Michael Brajac ConsultingPresentation to Toronto Section ASQ February 2015

Learning From Failure!

Learning From Failure
• Creates psychological anchors that reinforce learning• Asking “What went wrong?” is more insightful than “What went
right?”• Need a “clinically detached” approach--admit the failure, learn from
the failure, don’t repeat the failure• We need more of this kind of discussion in the Quality Profession

The GM Ignition Switch Is the Automotive Equivalent of the Space Shuttle Disasters
GM Recalls• 52 confirmed deaths GM ignition switch • No understanding of the risk or
sequence of events that can lead to loss of power—customer convenience issue• House and Senate Investigations• Numerous lawsuits• Little understanding of the “systems
aspect” of the ignition/air bag interface2
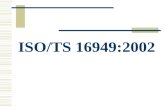
Challenger Disaster• 7 Astronauts killed• Risk greatly underestimated• Extensive cross functional
investigation• Rogers Commission• Neither NASA nor Thiokol
understand mechanism of joint sealing action1
1. The Presidential Commission on the Space Shuttle Challenger Accident Report, June 6, 1986, p. 120, p. 1482. Valukas Report, pp. 33, 44

Space Shuttle Challenger Data “O-ring Failure”
Source: Datavis.ca


Rogers Commission (sample of members)
• William P. Rogers, (Chairman), former secretary of state• Neil A. Armstrong (Vice Chairman) Retired Astronaut• Richard P. Feynman, 1965 Nobel Prize in Physics• Robert B. Hotz, Editor Aviation Week and Space Technology• Donald J. Kutyna, Air Force General, ICBM Background• Sally K. Ride, astronaut, first American woman in space• Charles E. Yeager, retired Air Force general,
Source: Wikipedia

Source: GMIgnitionCompensation.com

GM Ignition Switch
Picture credit: JonesWard.com

Understanding Your Customer

Is There Only One Way to Solve a Problem?• Red X1 Team engaged Sept 6, 20122
• Key component of Red X—BOBs and WOWs looking at the extremes• Team tasked with “What Changed from 2007 to 2008• Crashed vehicles are supposedly “quarantined” as evidence• Red X Engineer assigned to project essentially walks away from the
project when he is denied access to the crashed vehicles• Project declared “stuck”—outside experts retained—reach the same
conclusion in 2013 that Trooper Young and Indiana University reached in 2007Valukas Report, p. 186-188Red X is a Service Mark registered to the Shainin Consultants

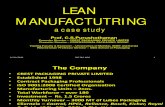
The Changed Detent Plunger
Photo credit: McSwain Engineering, GM’s Hit and Run: How a lawyer, mechanic and engineer blew open the worst auto scandal in history. www.pando.com/2014/10/18

Lessons Learned
• There was ample opportunity for other leverage—all non deployments were prior to 2008. • Don’t assume anything! Simple contrast—model year to model year—
utilizing a group comparison would have shown right away the switch was different• Admit when you are “lost in the data” and ask for help• A fresh outside look can help return the proper focus • If you don’t do your own due diligence, someone else will do it for
you

ISO 9001:2000
• Fundamental error made—part change no part number change• No oversight system for Documentation—a well implemented and
managed quality system could have been that system1
• Organization wide adherence to these standards could have created a a more compliant culture with respect to documentation requirements• Quality standards not discussed in any detail in Valukas Report
1. Page 33 Valukas Report

Leadership Is Crucial in Establishing Culture
Ignition Switch Issue• Not seen as customer safety
issue—you can still steer and brake• No one is sure what their role is • Senior engineering leadership
transition—championenergize the team
Issue X (Old GM)• Team formed— “you guys are
together until this is solved”• Team experienced issue first hand
on a highway• Ten customer vehicles bought
back on the spot• Everyone knows their role—cross-
functional team approach critical in resolving the issue
Valukas Report p. 178

Robust Design Failure Example 1—Heat in Electrical Modules
• NHTS Campaign Number 14V26100• Models Under Recall• Certain MY 2004-2008 Chevrolet Aveo vehicles with daytime running lights
(DRL) equipped
• Problem:• In the affected vehicles, there may be heat generated within the DRL module
located in the center console in the instrument panel, which could melt the DRL module.
• Consequence:• If the DRL module melts due to the heat generation, it could cause a vehicle
fire
Source: Autoblog.com

Robust Design Failure Example 2
Source: Autoblog.com Picture Credit: Frugalityisfree.com
Certain model year 2014 CTS vehicles manufactured June 2013 to February 2014.
If vehicle is turned off, with wiper functionality left on, and battery dies, when vehicle is jump started, wipers will not work

Robust Design
• First introduced to North American manufacturing in the mid 80’s• When done right, it is very effective “building in” quality to a product• Training trends--brief web based courses and tutorials• Tendency to design to a test• Clean sheet Robust Design techniques could have prevented at least
some of the recalls• Understanding customer usage is key

Supplier Interaction and Management
• Supplier’s actions can impact business further up the chain•Not enough to have culture of safety only at the OEM•Document Management—PPAP package never
located•Design responsibility

A “Fundamental Failure”
• Engineering leadership—missing in action• Failure to recognize systems aspects of the vehicle• Chief Counsel—lack of oversight • Quality Organization—no escalation—where was the cross-
functional approach with Engineering?

Concluding Remarks
• One cannot hide anything• Initial sample sizes may have been small—impact was huge• Circumstances of crashes added a degree of confounding• Clinical look-- solely at the vehicle—did it perform as expected?• “5 whys” could have provided insight• Information Silos--No one person seemed to understand how the
whole system worked, information not shared cross-functionally• “Says Who?” -- “tribal knowledge and practices”-- nothing
documented