hiperplasia condilar.1
9
J Oral Maxillofac Surg xx:xxx, 2010 Hyperplasia of the Mandibular Condyle: Clinical, Histopathologic, and Treatment Considerations in a Series of 36 Patients Laura Villanueva-Alcojol, MD* Florencio Monje, MD, PhD† and Raúl González-García, MD‡ Purpose: Mandibular condylar hyperplasia (CH) is a rare entity that causes overdevelopment of the mandible, creating functional and esthetic problems. The aim of this article was to describe demographic and clinical characteristics of CH, analyze histopathologic features and their association with scinti- graphic and clinical findings, and evaluate esthetic and functional results after treatment by high condylectomy during the active phase. Materials and Methods: This retrospective study included 36 patients whose condyles were removed because of excessive unilateral growth resulting in facial asymmetry and occlusal disturbance. Of the 36 patients, 13 had had symptoms related to the temporomandibular joint, such as pain or clicking. In all the cases, high condylectomy was performed, and surgical specimens were sent for histologic exami- nation and divided into 4 histologic types as described by Slootweg and Müller. Statistical analysis was performed by use of R software (version 2.10.1; R Foundation for Statistical Computing, Vienna, Austria) and SPSS software for Windows (version 15.0; SPSS, Chicago, IL) to evaluate our results. A 2 test was carried out to assess the possible association between gender and involved side. The association of histologic appearance with clinical symptoms was estimated by use of the Fisher exact test. An analysis of variance test was performed to evaluate a possible association between patient age and histologic type according to the Slootweg and Müller classification and between histologic type and uptake on bone single photon emission computed tomography (SPECT). Results: We could not find a relationship between histologic type and uptake of the affected condyle on bone SPECT or between age and histologic type. However, our statistical analysis revealed an association between histologic appearance and the presence of joint symptoms (P .0049). Clinically, occlusion and facial symmetry improved in all patients postoperatively, and no recurrence was noted in any patient. Six patients required secondary surgery. Conclusion: We could not find any significant association between age and histologic type or between bone SPECT and histologic type. However, a significant association between histologic type and temporomandibular joint symptoms was observed. High condylectomy combined with orthodontics achieved optimal esthetic and functional results and constituted the unique and definitive treatment in 30 of 36 patients. © 2010 American Association of Oral and Maxillofacial Surgeons J Oral Maxillofac Surg xx:xxx, 2010 Mandibular condylar hyperplasia (CH) is a rare entity. It was first described by Robert Adams in 1836 as a condition that causes overdevelopment of the mandi- ble, creating functional and esthetic problems. 1 Since then, there have been numerous reports in the liter- ature referring to this clinical entity. 2-4 The excessive unilateral growth of the mandibular condyle can lead to facial asymmetry, occlusal disturbance, and joint Received from the Department of Oral and Maxillofacial-Head and Neck Surgery, University Hospital Infanta Cristina, Badajoz, Spain. *Resident Surgeon. †Department Head. ‡Staff Surgeon. Address correspondence and reprint requests to Dr Villanueva- Alcojol: Department of Oral and Maxillofacial Surgery, University Hospital Infanta Cristina, Badajoz, Juan de Badajoz, 14, 2G, 06003 Badajoz, Spain; e-mail: [email protected] © 2010 American Association of Oral and Maxillofacial Surgeons 0278-2391/10/xx0x-0$36.00/0 doi:10.1016/j.joms.2010.04.025 1 ARTICLE IN PRESS
-
Upload
leonardcarreradiaz -
Category
Documents
-
view
95 -
download
1
Transcript of hiperplasia condilar.1

MIcb
R
N
A
ARTICLE IN PRESS
J Oral Maxillofac Surgxx:xxx, 2010Hyperplasia of the Mandibular Condyle:Clinical, Histopathologic, and TreatmentConsiderations in a Series of 36 Patients
Laura Villanueva-Alcojol, MD* Florencio Monje, MD, PhD† and
Raúl González-García, MD‡
Purpose: Mandibular condylar hyperplasia (CH) is a rare entity that causes overdevelopment of themandible, creating functional and esthetic problems. The aim of this article was to describe demographicand clinical characteristics of CH, analyze histopathologic features and their association with scinti-graphic and clinical findings, and evaluate esthetic and functional results after treatment by highcondylectomy during the active phase.
Materials and Methods: This retrospective study included 36 patients whose condyles were removedbecause of excessive unilateral growth resulting in facial asymmetry and occlusal disturbance. Of the 36patients, 13 had had symptoms related to the temporomandibular joint, such as pain or clicking. In allthe cases, high condylectomy was performed, and surgical specimens were sent for histologic exami-nation and divided into 4 histologic types as described by Slootweg and Müller. Statistical analysis wasperformed by use of R software (version 2.10.1; R Foundation for Statistical Computing, Vienna, Austria)and SPSS software for Windows (version 15.0; SPSS, Chicago, IL) to evaluate our results. A �2 test wascarried out to assess the possible association between gender and involved side. The association ofhistologic appearance with clinical symptoms was estimated by use of the Fisher exact test. An analysisof variance test was performed to evaluate a possible association between patient age and histologic typeaccording to the Slootweg and Müller classification and between histologic type and uptake on bonesingle photon emission computed tomography (SPECT).
Results: We could not find a relationship between histologic type and uptake of the affected condyleon bone SPECT or between age and histologic type. However, our statistical analysis revealed anassociation between histologic appearance and the presence of joint symptoms (P � .0049). Clinically,occlusion and facial symmetry improved in all patients postoperatively, and no recurrence was noted inany patient. Six patients required secondary surgery.
Conclusion: We could not find any significant association between age and histologic type or betweenbone SPECT and histologic type. However, a significant association between histologic type andtemporomandibular joint symptoms was observed. High condylectomy combined with orthodonticsachieved optimal esthetic and functional results and constituted the unique and definitive treatment in30 of 36 patients.© 2010 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg xx:xxx, 2010taut
H
B
©
0
d
andibular condylar hyperplasia (CH) is a rare entity.t was first described by Robert Adams in 1836 as aondition that causes overdevelopment of the mandi-le, creating functional and esthetic problems.1 Since
eceived from the Department of Oral and Maxillofacial-Head and
eck Surgery, University Hospital Infanta Cristina, Badajoz, Spain.
*Resident Surgeon.
†Department Head.
‡Staff Surgeon.
Address correspondence and reprint requests to Dr Villanueva-
lcojol: Department of Oral and Maxillofacial Surgery, University
1
hen, there have been numerous reports in the liter-ture referring to this clinical entity.2-4 The excessivenilateral growth of the mandibular condyle can leado facial asymmetry, occlusal disturbance, and joint
ospital Infanta Cristina, Badajoz, Juan de Badajoz, 14, 2G, 06003
adajoz, Spain; e-mail: [email protected]
2010 American Association of Oral and Maxillofacial Surgeons
278-2391/10/xx0x-0$36.00/0
oi:10.1016/j.joms.2010.04.025

dmwrffpjo
aehvTctcsicco
tdgpendesist
oh
srmgrvintTbttdcfm
dchatma
tlr
oaorgcspa
V
2 HYPERPLASIA OF THE MANDIBULAR CONDYLE
ARTICLE IN PRESS
ysfunction. Prominent features include an enlargedandibular condyle, elongated condylar neck, out-ard bowing, and downward growth of the body and
amus of the mandible on the affected side, causingullness of the face on that side and flattening of theace on the contralateral side. Some patients also mayresent with symptoms from the temporomandibular
oint (TMJ) such as pain, joint sounds, and limitationf mouth opening.5
Obwegeser and Makek6 classified the asymmetryssociated with CH into 3 categories: hemimandibularlongation, with a horizontal growth vector (type 1);emimandibular hyperplasia, with a vertical growthector (type 2); and a combination of the 2 entities.ype 1 is associated with chin deviation toward theontralateral side and mandibular midline deviated tohe unaffected side. On the other hand, type 2 isharacterized by an ipsilateral open bite or compen-atory vertical overdevelopment of the maxilla on thenvolved side with canting of the occlusal plane. Mostommonly, the mandibular midline is straight and thehin is less deviated. The third type is a combinationf the other 2 types.The etiology and pathogenesis of CH remain uncer-
ain. It is not known what triggers a condyle to sud-enly start growing and become hyperplastic. Sug-ested theories include trauma followed by excessiveroliferation in repair, infection, hormonal influ-nces, arthrosis, hypervascularity, and a possible ge-etic role.7-9 Obwegeser and Makek6 suggested thatifferent growth factors individually controlling gen-ralized hypertrophy and elongation might be respon-ible for the deformities. Another possible cause be-ng taken into consideration, but thus far notubstantiated, is an increase in functional loading ofhe TMJ.10,11
The diagnosis of CH may be made by a combinationf clinical and radiologic findings. Various methodsave been used, including radiographic studies, bone
Table 1. HISTOLOGIC CLASSIFICATION OF MANDIBULAND MÜLLER12
Histologic Classification
Type I Broad proliferation zoneUnderlying thick layer of hyalinBone containing numerous car
Type II Patchy distribution (cell-rich arCartilage islands in cancellous b
Type III Great distortionIrregularly shaped masses of hy
or encroaching upward ontoType IV Continuous subchondral bone
No proliferation layer of hyalinBurned-out appearance of cond
illanueva-Alcojol, Monje, and González-García. Hyperplasia of the Ma
cintigraphy, and histopathologic assessment.5,12 TMJadiographs may show abnormalities in the size andorphology of the condylar head and/or neck re-
ions. Bone single photon emission computed tomog-aphy (SPECT) scan is an essential diagnostic tool forisualizing hyperactivity in the condyle. Various stud-es have shown the clinical significance of this tech-ique in such patients because this method identifies
hose with persistent unilateral condylar activity.5,13,14
he radioactive isotope is technetium 99 methyleneisphosphonate. Increased radionuclide uptake byhe hyperplastic condyle can be an indication of con-inued abnormal growth. It has been reported that aifference in uptake of 55%:45% or more between theondyles can be indicative of CH, because the af-ected condyles had a relative uptake of 55% orore.15-17
Slootweg and Müller12 described 4 histologicallyifferent types of mandibular CH. They proposed alassification based on histologic criteria and dividedyperplastic condyles into 4 types depending on therrangement and morphology of the various layers ofhe condyle (fibrous articular layer, undifferentiatedesenchyme proliferative layer, transitional layer,
nd hypertrophic cartilage layer)18 (Table 1).Although most reported cases are documented his-
ologically,5,12,19,20 in general, correlation of histo-ogic aspects with age, SPECT, and clinical symptomsemains unclear.
Treatment is primarily surgical, with or withoutrthodontics, and depends on the degree of severitynd the status of condylar growth. Different surgicalptions have been proposed for treating this anomaly,anging from high condylectomy to orthognathic sur-ery or even a combination of both. There is alsoontroversy with respect to the time of surgery, withome authors preferring to perform surgery as soon asossible and others waiting for cessation of excessivectivity to perform any intervention.
NDYLAR HYPERPLASIA DESCRIBED BY SLOOTWEG
Characteristics
th cartilageslandsernating with nonproliferative, cell-poor zones)re less frequent than in type I
cartilage extending into cancellous bone of condylar neckficial articular layerovered by cell-poor fibrocartilaginous layerth cartilage
AR CO
e growtilage ieas altone a
alinesuper
plate ce growyle
ndibular Condyle. J Oral Maxillofac Surg 2010.

iChwoh
M
bfrs
wwtdS4aci
ldats
Tc1Tcrrsc
PcCegt4st
ptan
waajptsmt
aeadSssxapa
Catr
wCWotstipsceppsl
C(
R
VILLANUEVA-ALCOJOL, MONJE, AND GONZÁLEZ-GARCÍA 3ARTICLE IN PRESS
The aim of this retrospective study was to describe,n a group of 36 patients diagnosed with unilateralH, demographic and clinical characteristics; analyzeistopathologic features of CH and their associationith scintigraphic and clinical findings; and evaluateur esthetic and functional results after treatment byigh condylectomy during the active phase.
aterials and Methods
This retrospective study, which covered the periodetween 1998 and 2009, included 36 patients (25emale and 11 male patients) whose condyles wereemoved because of excessive unilateral growth re-ulting in facial asymmetry and occlusal disturbance.
The inclusion criteria for the study were 1) patientsith facial asymmetry and malocclusion, with orithout pain or clicking related to the TMJ; 2) pa-
ients who showed enlarged and/or elongated con-yles on the orthopantograph; 3) patients whosePECT scan showed a difference in uptake of 55%:5% or more between condyles or a large differencessessed subjectively by a specialist in nuclear medi-ine; and 4) patients in whom histopathologic exam-nation confirmed mandibular CH.
Exclusion criteria included patients in whom en-argement of the condyle was caused by neoplasia orysplasia, as shown by radiologic and histologic ex-mination. All patients were informed of the nature ofhis investigation and all provided their informed con-ent.
Each patient had a complete clinical examination.he presenting clinical features in these patients in-luded facial asymmetry and malocclusion. Moreover,3 of the 36 patients had had symptoms related to theMJ. In each case, these consisted of mild pain andlicking. Apart from the clinical examination, plainadiographs with orthopantographs and posteroante-ior and lateral cephalograms were obtained. Thesehowed enlarged and/or elongated condyles in mostases.In all 36 cases, bone SPECT scans were performed.
atients who had a ratio of 55%:45% or more andlinical and radiographic findings in accordance withH were operated on. A 6-month to 1-year patientvaluation period was sometimes required before sur-ery in cases in which condylar activity was uncer-ain. Exceptionally, 1 patient with an uptake of 54%:6% after several scintigraphic studies was treatedurgically because of persistent and increasing symp-oms after various evaluations.
In relation to the scintigraphic study, we mustoint out that only 24 of the SPECT scans were quan-ified. In the earlier cases, the planar and SPECT im-ges were assessed only subjectively by a specialist in
uclear medicine. yIn all the cases in our series, high condylectomyas performed through an intra-aural or preauricular
pproach, incision on the superficial temporal fasciand periosteum of the zygomatic arch, and dissectionust above the TMJ capsule. Then, a T-incision waserformed for entry in the inferior joint space, and 4o 5 mm of the condylar head was removed, withoutmoothing of the cortical edges. Orthodontic treat-ent and mouth opening exercises were started
hereafter.All surgical specimens were sent for histologic ex-
mination. The condyles were first placed in 4% buff-red formalin and then decalcified in hydrochloriccid (Surgipath Medical, Richmond, IL) and dehy-rated sequentially in 70%, 90%, and 100% alcohol.amples were cleared with 50% and 100% methylalicylate before infiltration with paraffin. Micrometerections were prepared from blocks, deparaffinized inylene, rehydrated in descending concentrations oflcohol, and stained with hematoxylin-eosin. The sam-les were subsequently divided into 4 histologic typess described by Slootweg and Müller.12
All the cases were confirmed histopathologically asH, but only 18 were divided according to the Slootwegnd Müller classification. We compared the histology ofhe condylar specimen with preoperative bone scintig-aphy to try to find functional-morphologic correlations.
STATISTICAL ANALYSIS
Statistical analysis was performed by use of R soft-are (version 2.10.1; R Foundation for Statisticalomputing, Vienna, Austria) and SPSS software forindows (version 15.0; SPSS, Chicago, IL). The level
f statistical significance was set at .05. The descrip-ive statistical analysis was based on the mean andtandard deviation for continuous variables, whereashe frequency and percentage were used for categor-cal variables. A �2 test was carried out to assess theossible association between gender and involvedide. The association of histologic appearance withlinical symptoms was estimated by use of the Fisherxact test. An analysis of variance (ANOVA) test waserformed to evaluate a possible association betweenatient age and histologic type according to the clas-ification of Slootweg and Müller and between histo-ogic type and uptake on bone SPECT.
This study was approved by the Hospital Ethicalommittee and by the Institutional Human Studies
IRB) Committee.
esults
The mean age at surgical intervention was 22.7
ears (SD, 6.7; range, 11 to 42 years). The female-male
rwi
bspcb
mbAa(p
bAt
jiap3p
tmlba
Ad
V
4 HYPERPLASIA OF THE MANDIBULAR CONDYLE
ARTICLE IN PRESS
atio was 25:11, and the right-left affected side ratioas 11:7 (22 right and 14 left) from SPECT, histolog-
cally and clinically.It has been suggested that there is an association
etween female gender and right side, with the rightide predominating in female patients and the left sideredominating in male patients.21 In our sample, weould not find a statistically significant associationetween gender and affected side.All patients had unilateral excessive growth of theandibular condyle with concomitant occlusal distur-
ance and/or chin deviation toward the opposite side.ccording to the clinical classification of Obwegesernd Makek,6 24 patients were considered type 166.7%), 8 patients showed an asymmetry in the verticallane and were classified as type 2 (22.2%), and a com-
Table 2. CLINICAL DATA OF 36 PATIENTS WITH MAND
Patient Age (yr) Gender Side SPECT
1 27 F R —2 24 F R —3 24 M L —4 26 F L —5 26 F R —6 19 F R —7 24 F R —8 32 M R —9 11 M R —
10 18 F L —11 24 M R —12 17 F L —13 17 M R 59%:41%14 29 M R 60%:40%15 22 M R 68%:32%16 25 M L 46%:54%17 16 F R 56%:44%18 22 F R 62%:38%19 20 F L 43%:57%20 18 F L 44%:56%21 28 F R 62%:38%22 19 F L 46%:54%23 14 F R 65%:35%24 35 M L 39%:61%25 24 F R 57%:43%26 14 F R 58%:42%27 42 F L 38%:62%28 21 F L 43%:57%29 26 F L 36%:64%30 36 F R 60%:40%31 22 F R 57%:43%32 16 M R 57%:43%33 24 M L 44%:56%34 13 F L 43%:57%35 17 F R 58%:42%36 25 F R 60%:40%
bbreviations: C, combination of 2 clinical types; SPECT, siibular joint.*Clinical type according to classification of Obwegeser a
illanueva-Alcojol, Monje, and González-García. Hyperplasia of the Ma
ination of the 2 types was seen in 4 patients (11.1%).dditional symptoms, such as mild pain or clicking of
he joint, were present in 13 cases (36.1%).Bone SPECT scan had been performed on all 36 sub-
ects. On all the scans, there was appreciable asymmetryn relative condylar uptake. The maximum differencemong quantified scans was 68% to 32%. The meanercentage of the affected condyle was 59.04% (SD,.56), whereas the unaffected condyle showed a lowerercentage (40.96%; SD, 3.56) (Table 2).On examination of the histologic sections, all pa-
ients exhibited a persistent layer of undifferentiatedesenchyme cells and a layer of hypertrophic carti-
age, and evidence of cartilage rests in the cancellousone. Classification into types according to Slootwegnd Müller was only performed in 18 patients, as
R CONDYLAR HYPERPLASIA
linical Type* TMJ Symptoms Secondary Surgery
1 No No2 Yes Yes2 No No2 No NoC Yes No1 No No2 Yes No2 Yes No1 No No1 No No1 No Yes1 No No1 No No2 Yes No2 No Yes1 No No1 No Yes1 No NoC Yes Yes1 No No1 No No1 Yes No1 Yes No1 No No2 No No1 No No1 No No1 Yes No1 Yes YesC Yes NoC Yes No1 No No1 No No1 Yes No1 No No1 No No
hoton emission computed tomography; TMJ, temporoman-
kek.6
IBULA
C
ngle p
nd Ma
ndibular Condyle. J Oral Maxillofac Surg 2010.

dfis(t
hwc
ttsniae
bc
ft(oimwtfmbnbo
D
pfn
mtcpnc27tp
doaaTNhinf
t1oovitafa
oIbamhitiBs
imp
Vt
VILLANUEVA-ALCOJOL, MONJE, AND GONZÁLEZ-GARCÍA 5ARTICLE IN PRESS
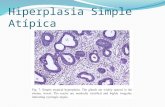
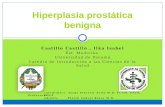
epicted in Figure 1. None of the samples was classi-ed as type IV. We only found types I, II, and III in oureries. Type I was the most frequently observed44.4%), followed by type III (38.9%). Only 16.7% ofhe patients showed type II CH (Fig 2).
A possible association between patient age andistologic type, as suggested by Slootweg and Müller,as evaluated, without a statistically significant asso-
iation.When analyzing our results, we observed that all
he patients with type II CH presented with symp-oms, such as pain and clicking. In type III patients,ome had symptoms and some did not. Conversely,one of the patients with type I CH had any problems
n relation to the TMJ. Our statistical analysis showedn association between histologic type and the pres-nce of joint symptoms (P � .0049).On the other hand, we could not find a relationship
etween histologic type and uptake of the affectedondyle on bone SPECT.The mean follow-up was 4.3 years. Occlusion and
acial symmetry improved in all patients postopera-ively, and no recurrence was noted in any patientFigs 3, 4). Six patients required orthognathic surgeryr esthetic surgery to correct residual deformity dur-
ng the follow-up period (4 bimaxillary surgeries, 2entoplasties, and an angle prosthesis). Furthermore,e observed, in accordance with other authors, that
he function of the joint was unimpaired and painree.22 The clinical examination showed a normalaximum interincisal opening and lateral excursions
efore and after surgery. High condylectomy left aormally functioning joint. No long-term joint mor-idity in patients treated in this way has yet been
0%5%
10%15%20%25%30%35%40%45%50%
CH I CH II CH III
Histologic types
FIGURE 1. Distribution of histologic types.
illanueva-Alcojol, Monje, and González-García. Hyperplasia ofhe Mandibular Condyle. J Oral Maxillofac Surg 2010.
bserved. e
iscussion
Rowe2 defined mandibular CH as an entity thatroduces an asymmetry of the mandible resulting
rom an enlargement of one side that is not due toeoplasia or dysplasia.Traditionally, it has been reported that CH afflictsale patients and female patients in equal propor-
ions.23,24 Moreover, some authors have even indi-ated that this condition is more common in maleatients.25 However, a female predisposition has beenoted in other studies,20 and, indeed, our group in-luded more female patients than male patients (ratio,5:11), in agreement with other reports of ratios of:27 and 3:1.5,21 In light of our results, we can statehat treatment was more commonly sought by femaleatients than by male patients.With regard to preferential laterality, an equal side
istribution has been found by some authors, whereasthers have found that the left side is more frequentlyffected.26 In our study, the right side was moreffected, with a ratio of 11:7 (22 right and 14 left).his result is consistent with other reports.21,27
itzan et al21 found that this preferential laterality wasighly gender dependent, with the right side predom-
nating in female patients and the left side predomi-ating in male patients. Nevertheless, we have notound this association in our series.
With respect to clinical classification depending onhe growth vector, a prevalence ratio between typesand 2 of approximately 15:1 has been reported.28 Inur group of patients, this ratio was 3:1, and more-ver, we found 4 patients with a combination of bothertical and horizontal asymmetry. Our results (type 1n 66.7% of patients, type 2 in 22.2%, and a combina-ion of transverse and vertical asymmetry in 11.1%)re similar to those of Nitzan et al,21 who reportedrequencies of 53%, 31%, and 16% for type 1, type 2,nd a combination of the 2 entities, respectively.
The scintigraphic results showed hyperactivity ofne of the condyles consistent with clinical findings.t is important to emphasize that SPECT results shoulde interpreted in light of a full clinical, radiographic,nd cephalometric evaluation. It should be borne inind that this method of bone scanning, thoughighly sensitive, is nonspecific and does not necessar-
ly correlate with active growth because it can also behe result of inflammatory conditions, infection, heal-ng after traumatic injuries, and neoplastic lesions.one SPECT scintigraphy should not be used as theole determinant of the need for condylar resection.
In describing the histologic characteristics of spec-mens of hyperplastic condyles that were surgically re-
oved, similar to other authors,5,12 we have observed theresence of an interrupted layer of undifferentiated mes-
nchymal cells and a hypertrophic cartilage layer. Another
sccs
tca
tCbsoar
ddtsaHh
sewapb
FpbIo
V the Ma
6 HYPERPLASIA OF THE MANDIBULAR CONDYLE
ARTICLE IN PRESS
tructural feature observed consistently in hyperplasticondyles is the distribution of cartilage rests in the sub-hondral spongiosa, which is histologic proof of progres-ive lengthening of the condyle.
Given the retrospective character of the study, al-hough all the cases were confirmed histopathologi-ally to have mandibular CH, only 18 were dividedccording to the classification of Slootweg and Müller.
In all the patients with increased radionuclide up-ake, we observed the histologic characteristics ofH. However, when analyzing a possible associationetween the activity level of the affected condyle oncintigraphic examination and the histologic featuresf a determined type of CH according to the Slootwegnd Müller classification, we could not find consistent
IGURE 2. Histopathologic examination. A, Type I CH. The phoresent within the bony trabeculae (hematoxylin-eosin stain, originone (4.6 mm deep from surface) of a hyperplastic condyle. C, Typ(hematoxylin-eosin stain, original magnification �10). D, Type Iriginal magnification �10).
illanueva-Alcojol, Monje, and González-García. Hyperplasia of
esults in our series. T
Gray et al5 reported that the increase in uptake wasirectly related to the frequency and penetrationepth of the cartilage islands. They also reported thathose patients who had marked uptake on the scinti-can also had a higher frequency of cartilage islands,nd the depth at which they were found was greater.owever, they did not correlate these findings withistologic types.Slootweg and Müller12 found that the results of
cintigraphy did not correlate with histologic growthvidence. On the other hand, they assumed that thereas a correlation between histologic growth activity
nd age, with type I being more frequently found inatients younger than 20 years of age and type IIeing more common in patients over 20 years of age.
ograph shows a broad proliferation area. Cartilage islands arenification �20). B, Cartilage island in deep layers of trabecular. Cartilage rests are less frequent in the spongy bone than in type
showing more distorted layered pattern (hematoxylin-eosin stain,
ndibular Condyle. J Oral Maxillofac Surg 2010.
tomicral mage II CH
II CH,
hey indicated that type III would be more frequently

fths
bottInCatadodTpTpahbgtt
stMttpaopasdatldeh
mibcsdcg
Focns
Villanueva-Alcojol, Monje, and González-García. Hyperplasia of theMandibular Condyle. J Oral Maxillofac Surg 2010.
VILLANUEVA-ALCOJOL, MONJE, AND GONZÁLEZ-GARCÍA 7ARTICLE IN PRESS
ound in older patients. In our group, when we triedo find an association between age and the variousistologic appearances of the condyle, a statisticallyignificant relationship was not encountered.
Nevertheless, we found a significant correlationetween histologic type and the presence or absencef symptoms (P � .0049). Particularly, we observedhat all patients with type II CH had clinical manifes-ations such as pain and joint sounds. Among the typeII patients, some were symptomatic and the rest didot report any disturbance in relation to the TMJ.onversely, none of the patients with type I CH hadny joint symptoms. To our knowledge, this associa-ion has not been reported in the literature until now,nd it could suggest that histologic types representifferent stages of the pathologic entity, with thenset of symptoms as the illness becomes more evi-ent and their disappearance as the fibrosis develops.ype I CH could be considered as a first phase ofroliferation in which there are no symptoms yet.hese would start in a latter phase (type II CH) ofatchy activity, and patients would probably becomesymptomatic again as the fibrosis generalizes andyaline cartilage disappears (type III CH). However,ecause this study was conducted in a relatively smallroup of patients, the results cannot be generalized tohe whole population of CH patients. They first needo be confirmed in further studies in larger series.
Traditionally, the surgical methods used have con-isted primarily of orthognathic surgery for correction ofhe asymmetry when further growth is not anticipated.otamedi27 performs unilateral or bilateral ramus os-
eotomy when growth is complete. Macintosh29 leaveshe articulation surgically undisturbed, allows the hyper-lasia to run its course, and then treats its sequelae withppropriate osteotomies. In our opinion, this optionften means waiting a long time, and consequently, theatient may have functional and esthetic disturbances,ssociated with psychosocial problems derived from aevere facial deformity. Moreover, the magnitude of theeformity and its compensatory changes in the maxilland dentoalveolar structures could compromise clinicalreatment outcomes. Some authors perform a bimaxil-ary operation including resection of the involved con-yle in the same procedure. Wolford et al28 and Sheffert al30 propose orthognathic surgery and simultaneousigh condylectomy to correct the asymmetry.In our opinion, basic considerations in the manage-ent of facial asymmetry caused by active CH must
nclude control of the growth process to allow morealanced facial development. If evidence of abnormalondylar growth is present, then condylar surgeryhould be undertaken before a severe facial deformityevelops.31 It is expected that the removal of theondyle will arrest the excessive and disproportionate
IGURE 3. A, B, and C, Unilateral mandibular type II CH in a 24-year-ld patient. The elongation of the left side of the face, chin deviation, andanting of the occlusal plane should be noted. The mandibular midline isot deviated. D, E, and F, Patient at 2 years after high condylectomy,howing significantly improved facial harmony and good occlusal result.
rowth of the mandible in the diseased region and

caOc
dstrtas
c3pslibts
sbcsbad
A
a
R
1
1
1
1
Fpplyi
Vt
8 HYPERPLASIA OF THE MANDIBULAR CONDYLE
ARTICLE IN PRESS
an therefore limit progressive asymmetry during thective phase and provide stable long-term results.rthodontic treatment after surgery can correct oc-
IGURE 4. Unilateral mandibular type I CH in a 14-year-oldatient. A, B, and C, Preoperative frontal, lateral, and intraoralictures. The deviation of the chin and the interincisal mandibular
ine toward the left side should be noted. D, E, and F, Patient at 2.5ears after high condylectomy. The deviation of the chin andnterincisal mandibular line has been corrected.
illanueva-Alcojol, Monje, and González-García. Hyperplasia ofhe Mandibular Condyle. J Oral Maxillofac Surg 2010.
lusal and esthetic deformity definitively without ad-
itional surgical interventions in most cases. If not,econdary correction by mandibular or maxillary os-eotomies or both can be appropriate to correct anyesidual occlusal and facial asymmetry. In generalerms, if a high condylectomy has been performednd posterior orthognathic surgery is necessary, thisecond operation will be easier.
High condylectomy (removal of 4 to 5 mm of theondyle) instead of condylar shaving (removal of 2 tomm of the condyle) is our preferred method. The
resence of cartilage islands in the cancellous bonehows that the pathology is not limited to the carti-age surface. Masses of hyaline cartilage extendingnto the cancellous bone of the condylar neck haveeen identified in our samples. Therefore, not onlyhe cartilage surface but also the subchondral bonehould be removed to eliminate the growth center.
In summary, we could not find any significant as-ociation between age and histologic type or betweenone SPECT and histologic type. However, a signifi-ant association between histologic type and TMJymptoms was observed. High condylectomy com-ined with orthodontics achieved optimal estheticnd functional results and constituted the unique andefinitive treatment in 30 of 36 patients.
cknowledgments
The authors thank Dr Fernandez de Mera for the histologicnalysis.
eferences1. Adams R: Case history of Mary Keefe, in Medical Section of the
British Association, Bristol Meeting, 18362. Rowe NL: Aetiology, clinical features and treatment of mandib-
ular deformity. Br Dent J 108:41, 19603. Norman JE, Painter DM: Hyperplasia of the mandibular condyle. A
historical review of important early cases with a presentation andanalysis of twelve patients. J Maxillofac Surg 8:161, 1980
4. Papavasiliou A, Sawyer R, Lund V, et al: Benign conditions ofthe temporomandibular joint: A diagnostic dilemma. Br J OralSurg 21:222, 1983
5. Gray RJ, Sloan P, Quayle AA, et al: Histopathological and scin-tigraphic features of condylar hyperplasia. Int J Oral MaxillofacSurg 19:65, 1990
6. Obwegeser H, Makek M: Hemimandibular hyperplasia—Hemi-mandibular elongation. J Maxillofac Surg 14:183, 1986
7. Egyedi P: Aetiology of condylar hyperplasia. Aust Dent J 14:12, 19698. Yang J, Lignelli JL, Ruprecht A: Mirror image condylar hyper-
plasia in two siblings. Oral Surg Oral Med Oral Pathol OralRadiol Endod 97:281, 2004
9. Oberg T: Unilateral hyperplasia of the mandibular condylar process:A histological, microradiographic and autoradiographic examinationof one case. Acta Odontol Scand 20:485, 1962
0. Hansson T, Solberg WK, Penn MK, et al: Anatomic study of the TMJsof young adults. A pilot investigation. J Prosthet Dent 41:556, 1979
1. Scapino RP: Histopathology associated with malposition of the hu-man temporomandibular joint disc. J Prosthet Dent 55:382, 1983
2. Slootweg PJ, Müller H: Condylar hyperplasia. A clinico-patho-logical analysis of 22 cases. J Maxillofac Surg 14:209, 1986
3. Saridin CP, Raijmakers P, Becking AG: Quantitative analysis of planar
bone scintigraphy in patients with unilateral condylar hyperplasia.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 104:259, 2007
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
VILLANUEVA-ALCOJOL, MONJE, AND GONZÁLEZ-GARCÍA 9ARTICLE IN PRESS
4. Hodder SC, Rees JIS, Oliver TB, et al: SPECT bone scintigraphyin the diagnosis and management of mandibular condylar hy-perplasia. Br J Oral Maxillofac Surg 38:87, 2000
5. Bohuslavizki KH, Brenner W, Kerscher A, et al: The value of bonescanning in the pre-operative decision-making in patients with pro-gressive facial asymmetry. Nucl Med Commun 17:562, 1996
6. Cisneros GJ, Kaban LB: Computerized skeletal scintigraphy for theassessment of mandibular asymmetry. J Oral Maxillofac Surg 42:513,1984
7. Pogrel MA: Quantitative assessment of isotope activity in the tem-poromandibular joint region as a means of assessing unilateral con-dylar hypertrophy. Oral Surg Oral Med Oral Pathol 60:15, 1985
8. Hansson T, Oberg T, Carlsson GE, et al: Thickness of the softtissue layers and the articular disk in the temporomandibularjoint. Acta Odontol Scand 35:77, 1977
9. Eslami B, Behnia H, Javadi H, et al: Histopathologic comparisonof normal and hyperplastic condyles. Oral Surg Oral Med OralPathol Oral Radiol Endod 96:711, 2003
0. Angiero F, Farronato G, Benedicenti S, et al: Mandibular con-dylar hyperplasia. Clinical, histopathological and treatmentconsiderations. Cranio 27:24, 2009
1. Nitzan D, Katsnelson A, Bermanis I, et al: The clinical charac-teristics of condylar hyperplasia: Experience with 61 patients.J Oral Maxillofac Surg 66:312, 2008
2. Lippold C, Kruse-Losler B, Danesh G, et al: Treatment of hemi-mandibular hyperplasia: The biological basis of condylectomy.
Br J Oral Maxillofac Surg 45:353, 20073. Henderson MJ, Wastie ML, Bromige L, et al: Technetium-99mbone scintigraphy and mandibular condylar hyperplasia. ClinRadiol 41:411, 1990
4. Matteson SR, Proffit WR, Terry BC, et al: Bone scanning with99m technetium phosphate to assess condylar hyperplasia.Oral Surg Oral Med Oral Pathol 60:356, 1985
5. Worth HM: Radiology of the temporomandibular joint, in ZarbGA, Carlsson GE (eds): Temporomandibular Joint Function andDysfunction. Copenhagen, Munksgaard, 1979, p 334
6. Iannetti G, Cascone P, Belli E, et al: Condylar hyperplasia:Cephalometric study, treatment planning and surgical correc-tion (our experience). Oral Surg Oral Med Oral Pathol 68:673,1989
7. Motamedi MH: Treatment of condylar hyperplasia of the man-dible using unilateral ramus osteotomies. J Oral Maxillofac Surg54:1161, 1996
8. Wolford LM, Mehra P, Reiche-Fischel, et al: Efficacy of highcondylectomy for management of condylar hyperplasia. Am JOrthod Dentofac Orthop 121:136, 2002
9. Macintosh RB: Treatment of condylar hyperplasia of the man-dible using unilateral ramus osteotomies. J Oral Maxillofac Surg54:1169, 1996
0. Sheffer MA, Corso A, Tomazi M, et al: Condylar hyperplasiatreated by simultaneous orthognathic surgery and high condy-lectomy. A case report. Rev Odont Cienc 23:407, 2008
1. Chen YR, Bendor-Samuel R, Huang CS: Hemimandibular hyper-
plasia. Plast Reconstr Surg 97:730, 1996



![Hiperplasia y Cancer Prostatico[1]](https://static.fdocuments.in/doc/165x107/55cf9bb4550346d033a71157/hiperplasia-y-cancer-prostatico1.jpg)