Surgery Esophagus Tg
69
Surgery Esophagus Dr. Teresa Galdona PA-C
-
Upload
miami-dade -
Category
Health & Medicine
-
view
4.342 -
download
2
description
General Surgery
Transcript of Surgery Esophagus Tg

Surgery
EsophagusDr. Teresa Galdona PA-C

Esophagus
• A) Function:• 1)passaje for ingested food• 2)emesis• 3)conduit for endoscopic evaluation• 4)evaluation of aorta and heart (TEE)• B) Anatomy:• Originates at cricoid cartilage • and pharynx in the neck

Esophagus
• B) Anatomy:
• Posterior mediastinum behind aortic
• and (L) mainstem bronchus.
• Enters abd. cavity through esophageal
• hiatus of diaphragm.
• Mucosa and 2 muscular layers
• mucosa is stratified squamous epithelium

Esophagus
• B) Anatomy(cont)• 2 muscular layers, inner layer is circular outer
layer is longitudinal. There is not serosal layer• Musculature of upper 1/3 is skeletal and
musculature of the lower 2/3 is smooth muscle.• 2 sphincters: one is physiological one in the
neck call upper esophageal sphincter, the other is located at the diaphragm called lower esophageal sphyncter

Esophagus
• C) Physiology:• food is propelled down the esophagus by
a peristaltic wave.• LES relaxes in anticipation of food, allows
food enter stomach then returns to its high resting pressure, to prevent reflux.
• Pathophysiology:• LES is to prevent reflux of gastric
content.

Esophagus
• D) Pathophysiology:
• 1) Alteration of the mechanism of LES allows reflux of acid content, on an epithelial surface that is rich in sensory innervation
• 2) Failure of LES to relax, causes proximal dilation with contractile disorders

Esophagus
• E) S/S: • 1) esophageal disorders per se• 2) other organ manifestation disorders• like angina pectoris, asthma, Pneumonia.• 3) signs of systemic Ds, like collagen Ds
or neurological Ds, like scleroderma (systemic sclerosis, LES,smooth muscle) in CREST syndrome, or in stroke and other neurologic diseases.

Esophagus
• in CREST syndrome. Also in polymyositis/dermatomyositis, where ¼ of pts have dysphagia that involves UES (striated muscle) or in stroke and other neurologic diseases.

Esophagus
• F) Clinical presentation:• Dysphagia: difficulty with transition of ingested
food • Odynophagia: painful swallowing• Globus ictericus: lump in the throat,evaluate
carefully sensation b/c it may represent a mass lesionand no a psychological symptom
• Pyrosis or water brash associated with GERD,achalasia and esophageal strictures
• Regurgitation,vomiting

Esophagus
• Pyrosis or water brash associated with GERD,achalasia and esophageal strictures
• Regurgitation: passive return of ingested food to oropharynx.
• Vomiting: active return of stomach content


Esophagus
• Recurrent episodes of bronchitis or pneumonia ( very young, elderly, may be sing of recurrent aspiration of esophageal or gastric content b/c of esophageal obstruction, congenital malformation, diverticula, or motility disorder).
•

Esophagus
• Also,
• Anemia (ulcerative esophagitis mcc of esophageal bleeding, occult blood in stools)
• Hiccups or singultus (sign of diaphragmatic irritation and early sign of
• stomach dilation, MI or diaphragmatic hernia)

Esophagus
• Esophageal diseases may mimic other process like angina pectoris. Must do cardiac and esophageal evaluation simultaneously b/c both processess are common diseases.
• G) esophagus examination:
• 1) H/P

Esophagus
• 2) stools (check for blood)• 3) xray: PA and lateral to r/o thoracic pathologies• 4) Barium swallow: esophageal anatomy and function. It
is safe and highly cost-effective. • 5) CT scan: relation to other anatomic structures and,
mediastinum, esophgeal cancer.• 6) MRI (no advantage over CT) • 7) Esophagoscopy: allows direct visualization of lumen of
esophagus, can get directed Bx and treat like esophageal varices (injecting sclerosing substances)
• 8) Manometry and fluoroscopy

Esophagus
• 7) Esophagoscopy: allows direct visualization of lumen of esophagus, can get directed Bx and treat like esophageal varices (injecting sclerosing substances)
• 8) Manometry and fluoroscopy, mostly for Dx of esophgeal motility disorders.

Esophagus
• H) Pathologies:• 1) Hiatal Hernia:• MCC in women who have been pregnant, and in
both women and men when there is increased intraabdominal pressure, for example obesity, it predisposes to reflux of gastric acid into distal esophagus. It is important to know that GERD and HH are separated conditions. Although, 80% of pts with reflux have demostrable HH.

Esophagus
• type I: sliding hernia
• Allows the GEJ and a portion of the stomach to slide into the mediastinum.
• Only important when there is association with reflux of gastric acid into the lower esophagus.

• Sliding Hiatal Hernia

Esophagus
• Type II: paraesophageal hernia.
• GEJ is normal in position, reflux is uncommon.
• Portion of the gastric fundus that herniates alonside esophagus is prone to herniation and incarceration.
• Surgical repair is necessary to avoid strangulation or incarceration.

Esophagus
• Sliding and paraesophageal Hiatal hernia

Hiatal Hernia
• Figure 1 shows a normal connection between the esophagus in the chest cavity and the stomach in the abdomen. Figure 2 shows a small portion of the stomach pushing upward into the chest cavity from the abdomen, causing a hiatal hernia.

Esophagus
• Type III: combination of I and II.• It is a very large defect at esophageal
hiatus.• Other abdominal organs may be found in
the mediastinum like stomach.• Surgical repair is necessary.• I) Pathophysiology:• Loss of anatomic relationship between the
diaphragmatic hiatus and esophagus


Esophagus
• Reflux of gastric acid causes burn of esophageal mucosa.
• Very important the degree of mucosal injury is due to duration of acid contact and not to excessive gastric acidity (normal acid in the wrong place).
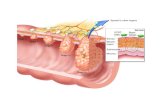
• Continue inflammation of distal esophagus may cause mucosal erosion, ulceration, scarring, stricture, chronic reflux, transformation of epithelium to columnar ( Barret’s esophagus), to Ca (adenocarcinoma)

Esophagus

Esophagus
• J) Most commonly presentation is: • Reflux,(GERD) a burning epigastric or
substernal pain or tightness. 10% of pts can be confused with MI.Becomes worse when supine or leaning over.
• GERD symptoms are non specific and can mimic other processes for example:
• a) angina of cardiac origin must be evaluated if pt has a sensation of substernal pressure that is not relieved by belching or antiacids.

Esophagus
• b) Occult blood in stools due to erosive esophagitis.
• c) Schatzki ring is a variant of GERD, it is a muscular constriction of distal esophagus due to irritaton of circular muscle by refluxed acid. 10% becomes fibrotic and requires dilation and or excision.
• d) Dysphagia is a symptom of oropharyngeal Ca or altered esophagial motility 2nd to achalasia or stroke.


Esophagus
• f) DGER is bile and pancreatic enzimes reflux, this process can complicate GERD when both processes coexist.
• Recurrent pneumonia may indicate advance GERD and distal esophageal stricture

Esophagus
• Immunocompromised pts with GERD may present with candida esophagitis, CMV or Herpes virus infection.
• Gastric irritants and stimulants like chocolate, caffeine, alcohol, tobacco, ASA,
• NSAID’s,can increase symptoms.

Esophagus
• Other way of presentation can be chronic aspiration pneumonitis, asthma or chronic laryngitis.
• Other presentation can be a complain of a “lump or food stuck” below xiphoid process due to muscular spasm of esophagus.
• Many pts with type I have no sympyoms.

Esophagus
• Other forms of presentations are vomiting and dysphagia (suggest stricture).
• Type II HH give symptoms mostly when incarcerated and isquemic, and presents with dysphagia, bleeding and respiratory distress.
• K) Dx:• Barium swallow (mostly for Dx. of HH type
I and II)

Esophagus
• EGD (esophagogastroduodenoscopy) and
• Bx (mostly for reflux esophagitis).
• L) Tx: medical, 80% respond to medical treatment and only 20% do not respond to it and ½ of this (10%) require surgery.
• Medical treatment:
• No gastric irritants like
• Alcohol, chocolate, caffeine, tobacco

Esophagus
• Avoid tight gardments that rise intraabdominal pressure
• Avoid drinking or eating within several hours of sleeping
• Regular use of: antiacids, H2 blokers, PPI’s.
• Elevation of head’s bed at least 6 inches• to avoid nocturnal reflux.

Esophagus
• Weight loss in obese pts.
• Surgical Tx is to correct or repair the anatomic defect and prevent reflux,
• 2) Achalasia is the MC motility disorder of esophagus and it means “failure to relax”. The affected area is distal esophageal circular muscle.

Esophagus
• It is caused by failure of relaxation of high pressure zone sphincter, the proximal esophagus dilates resulting in a painless dysphagia.
• Symptoms are dysphagia, regurgitation of indigested food, some weight loss, pain is not a hallmark.
• Drinking large amounts of liquid necessary to push down food.

Esophagus
• Aspiration pneumonia is common. • Very common complain of spitting up foul
smelling secretions when lean forward.• Dx is made by Barium swallow, by dilation of
proximal esophagus, “bird-beak” deformity.• Tx : is surgical, 95% pts have complete relief.
Procedure is known as esophageal myotomy (Heller myotomy). Medical Tx can use CCBlokers, and dilation at the esphagogastric junction

• Achalasia • Bird-beak

Esophagus
• 3) Diverticula.• 2nd MC motility disorder. It is an out-pouching of
all or part of the wall of the esophagus. May ocurred at any level in esophagus. Can be classified as pulsion (as cervical Zenker’s diverticula) and traction.
• Symptoms same as achalasia like regurgitation, choking, or putrid breath odor.
• Pts with traction diverticula are asymptomatic, which is the contrary for pulsion diverticula

Diverticula
• Mid-esophageal diverticulum

Diverticula
• Epiphrenic diverticulum

Esophagus
• Tx is mostly excision of diverticula.• Other disorders of esophagus:• Scleroderma: 70% of pts have esophageal
abnormalities with progressive decline in muscular contractility towards LES.
• Dx is made by Barium swallow xrays.• MC GI symptom is dysphagia.• Progressive reflux, ulceration of distal
esophagus, strictures.

Esophagus
• Nutcracker esophagus:
• Painful diffuse esophageal spasm of circular muscle through the length of esophagus that can be confused with angina pectoris.
• Dysphagia:
• associated with stress, or psychological factors.

Esophagus
• 4)Esophagus tumors:• Benign tumor: leiomyoma• Most common in middle and distal thirds,
usualy asymptomatic.• Malignant tumors:• Most common are:• Squamous Ca ---- 85%• Adenocarcinoma ----10%

Esophagus
• Sarcomas ----0.8%• Primary esophgeal lymphoma ----very rare• APUDomas (tumors of amine precursor
uptake and decarboxilation system) 0.8%,• very malignant (already met when initial
presentation).• Epidemiology:• Environmental factors are involved as
etiology.

Esophagus
• Low dietary levels of ascorbic acid, alphatocoferol, retinol, riboflavine, high levels of nitrosamines in fungus infected food are associated with Esophageal cancer in China.
• In Western hemisphere (USA and other countries) alcohol, tobacco, achalasia, Barret’s esophagus and caustic injuries play as etiologies for esophageal cancer.

• Squamous cell Ca




Esophagus
Also, poor oral hygiene, surgical procedures and pre-malignant conditions besides Barret’s esophagus, like radiation, or Plummer-Vinson syndrome (iron anemia, esophageal webs).
Great risk factor is consumption of alcohol of more or equal to 9 g of ethanol and same if person smokes more than 20 cig per day.

Esophagus
• 10% of pts with Barret’s will develop adenocarcinoma.
• Tylosis (hyperkeratosis of palms and soles) is the only genetic disorder associated to esophageal cancer, 95% chance of esophageal cancer if live long.

Esophagus
• Squamous cell Carcinoma of esophagus arises from squamous epithelium,from the upper part of esophagus
• Adenocarcinoma of esophagus arises from transformation of columnar epithelium that replaces normal squamous epithelium of distal esophagus as a result of chronic acid reflux. Metaplasia like this is known as Barret’s esophagus

Esophagus
• S/S of esophgeal malignancy:
• Slow onset
• Dysphagia (MC symptom)
• Starts with solids to liquids
• 2nd MC symptom is odinophagia (retrosternal pain with swallowing)
• Rare symptom is constant mid-back or midchest pain

Esophagus
• Hoarseness (when Tumor invade locally)• Can have episodes of aspiration
pneumonia.• When Ds is too advance pts can’t swallow • their own saliva.• Very important is that no serosa layer in
esophagus it allows tumors spread early to adjacent structures like aorta, lymph nodes.

Esophagus
• Dx:
• Barium contrast studies, “apple core” image.
• Endoscopy
• Bx
• Ct scan used to stage esophageal Ca.
• PET (positron emission tomography) for staging mediastinal and distant mts.

Esophagus
• Tx: • When possible, depending of stage, surgical
approach is definitely the treatment. It may depend of level of the lesion and if pt has a curable lesion. Taking this in consideration upper esophagus lesions require surgical removal of esophagus en bloc with larynx, permanent tracheostomy and restoration of swallowing

Esophagus
• In lesions that involve middle third of esophagus are treated by stage procedure, total thoracic esophagectomy and bypass.
• Lower third of esophagus is treated by esophagogastric resection and end to end anastomosis in the mid-chest.
• When prognosis is not good then radiation and /or intubation are the Tx

Esophagus
SCC and ADC have per se bad prognosis. Cure rate for a favorable case is only 20%,
but in general cure rate for esophageal cancer is about 5%
• Because SCC and ADC of esophagus have a very poor prognosis treatment is directed to restore swallowing.
• Radiation and/or intubation are more used Tx for advanced cases.

Esophagus Strictures
• MCC = sequelae of GERD –induced esophagitis • Causes:
– Diffuse esophageal spasm (DES)– Scleroderma– Rings & Webs– Hiatal Hernia– Dysfunctional LES– Motility Disorders– Cancer
• Dx:– Manometry (records pressures)
• Tx:– Pneumatic (balloon dilation)

EsophagusMallory-Weiss Tear
• Repeated strenuous retching or vomiting may be responsible for the tears in the mucosa – results from prolonged and forceful vomiting,
coughing or convulsions
• Significant hemorrhage can occur• It may occur as a result of excessive alcohol
ingestion. • This is an acute condition which usually resolves
within 10 days without special treatment.

Esophagus
• Esophageal perforation:• Instrumentation 1st cause: endoscopy,
biopsy, nasogastric tube, dilation procedures, inflation of devices to tamponade esophageal varices (Seng-staken- Blakemore tube), balloon dilation for achalasia, or spontaneous perforation due to forcefull vomiting or retching that increases intraesophageal pressure (Boerhaave’s syndrome)

Esophagus
• In esophageal perforation you will find a pt that after few hours of perforated presents with deep shock due to mediastinal sepsis,
and death.
• Other presentation is almost immediately the pt goes with severe pain chest, hypotension, diaphoresis, nausea and vomiting then collapse and death.

Esophagus
• Tx is aggressive surgical intervention.• Mortality is directly directed to time
between perforation and intervention.
• Foreign body: • Toddlers, mentally ill adults.• Dx. is confirm based on imaging studies
(plain films, detect radio opaque object, and/or barium swallow)

Esophagus
• Tx: • Endoscopic removal.
• Ingestion of caustic material:• Accidental• Intentional• Most damaging are alkaline containing products
(Drano, Liquid Plumr). Alkalinity above pH12.0 very corrosive

Esophagus
• They destroy from lips to small intestine. Acidic material are a bit less damaging.
1st )identification (early) of product.• each product has different approach.• 2nd) Thorough H/P to stimate damage.• Pt presents with burning pain in upper
GI tract, nausea, vomit, difficulty swallowing and breathing.
• 3rd )Xrays, emergency endoscopy.

Esophagus
• TX:• A glass of water in case of caustic and mlik
and/or water for acids• No induced vomit (aspiration and/or further
damage).• Airway and • esophagus patency• Steroids to avoid strictures if no perforation• Use of ANTB controversial• Long term dilation in case of strictures.

Esophagus
• Very important:
• caustic or alkaline substances cause liquefaction necrosis
• Acidic substances cause coagulation necrosis