Ca esophagus
41
Esophageal Cancer Dr Pavan kumar L 15 th July 2013
-
Upload
lachi-pavan -
Category
Education
-
view
744 -
download
2
Transcript of Ca esophagus

Esophageal Cancer
Dr Pavan kumar L15th July 2013

Anatomy
• The esophagus is a thin-walled, hollow tube approximately 25 cm in length.

• The lower third (5 to 10 cm) of the esophagus may contain glandular elements.
• Replacement of the stratified squamous epithelium with columnar epithelium is referred to as Barrett's esophagus, often occurring in the lower third.


Esophageal wall layers
• Innermost mucosa • Sub mucosa• Muscular propria• Adventitia.
• No serosal layer in esophagus, facilitating extra esophageal spread of disease.

Lymphatic Drainage

Lymphatic drainage

• Lymphatics of the esophagus drain into nodes that usually follow arteries
1. Inferior thyroid artery 2. Bronchial and esophageal arteries3. Left gastric artery (celiac axis)

Epidemiology - esophageal cancer

Epidemiology - esophageal cancer• Incidence rates of squamous cell esophageal
cancer can vary 100- to 200-fold among different populations living in geographic adjacency.
• Squamous cell esophageal cancer is the foremost malignancy in the Bantu of Africa.
• South Africa, Japan, China, Russia, Scotland, and the Caspian region of Iran also have relatively high incidence rates.

• In many Western countries the incidence of adenocarcinoma of the esophagus (distal esophagus and gastroesophageal junction) is rapidly rising and the incidence of squamous cell cancers is declining.

Relative change in incidence of esophageal adenocarcinoma and other malignancies

Etiology
• Carcinogens– Tobacco and alcohol– Human papillomavirus (HPV) infection– Dietary carcinogens• Plants growing in soil deficient in molybdenum have
reduced vitamin C content • Elevated nitrates in the drinking water• Food containing fungi: Geotrichum candidum (pickles,
air-dried corn), Fusarium sp., and Aspergillus sp. (corn)

Predisposing factors for squamous cell esophageal cancer
– Lye stricture (up to 30%)– Esophageal achalasia (30%)– Esophageal web (20%)– Plummer-Vinson syndrome (iron-deficiency
anemia, dysphagia from an esophageal web, and glossitis, 10%)

– Short esophagus (5%)– Peptic esophagitis (1%)– Patients with head and neck cancer (Field's
cancerization theory)– Patients with celiac disease– Chronic esophagitis without Barrett's esophagus– Thermal injury to the esophagus because of
drinking boiling hot tea or coffee (Russia, China, and Middle East)
Predisposing factors for squamous cell esophageal cancer

Predisposing factors for adenocarcinoma of the esophagus
– Barrett's esophagus is metaplastic replacement of squamous with intestinalized columnar epithelium.
– Obesity– Reflux esophagitis

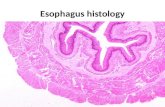
Pathology - Histology
• Upper and middle esophagus - Squamous cell tumors constitute 98%
• Lower esophagus - adenocarcinoma is becoming more common.
1. Barrett's esophagus2. Extension of a gastric adenocarcinoma.

SCC Location of cancer in the esophagus• Upper – 15%• Middle – 50%• Lower – 35%Adenocarcinoma is most common in thelower third of the esophagus, accounting for
over 65% of cases.

Clinical course
• Esophageal cancer is highly lethal • More than 90% of affected patients die from the
disease. • About 75% present initially with mediastinal nodal
involvement or distant metastasis.
• Death is usually caused by local disease that results in malnutrition or aspiration pneumonia.

Patterns of Spread
• Lesions in the upper esophagus can impinge on or invade the recurrent laryngeal nerves, carotid arteries, and trachea.
• Tumors in the lower third of the esophagus can invade the aorta or pericardium, resulting in mediastinitis, massive hemorrhage, or empyema.

• T1 lesions -incidence of nodal spread is 14% to 21%
• T2 lesions, this rises to 38% to 60%.• The location of involved lymph nodes is
influenced by the origin of the primary tumor.

• The primary direction for lymphatic flow for the lower esophagus is toward the abdomen.
• According to the classification by Siewert

• Type I tumors-nodal metastases are often seen in the mediastinum and abdomen ,
• Type II tumors are intermediate, preferentially spreading inferiorly and less frequently into the mediastinum.
• Type III tumors metastasize almost exclusively inferiorly, toward the celiac axis.

• The primary value in the Siewert classification is to the guidance of appropriate type surgery
• Type I tumors are generally treated with esophagectomy and mediastinal lymph node resection, with types II and III approached through the abdomen.

Clinical Presentation
• Location of the primary tumor in the esophagus may influence presenting symptoms.
• Dysphagia • Odynophagia• Weight loss - extent of weight loss has been
associated with a worse prognosis.

• Hoarseness • Cough• Glossopharyngeal
neuralgia• Hematemesis
• Hemoptysis, • Melena, • Dyspnea, • Persistent cough -
tracheoesophageal or bronchoesophageal fistula

Proposed algorithm for diagnosis and staging of esophageal cancer

Barium swallow 1. visualize areas of obstruction and assess stricture. 2. Extravasation of contrast may indicate a fistulaEsophagogastroduodenoscopy (EGD)3. Direct visualization and relative location &size of the
primary tumor. 4. Cold-forceps biopsies are obtained for pathologic diagnosisEndoscopic ultrasound (EUS) 5. Assesses depth of invasion 6. Involvement of adjacent lymph nodes essential for clinical
staging.

Bronchoscopy 1. Upper and middle thoracic esophageal lesions
to exclude invasion of trachea or bronchi.
Laparoscopy for GEJ/proximal stomach tumors 2. To exclude possible
intra-abdominal/peritoneal metastasis3. Could also be used to place G- or J-tube for
patients with complete obstruction

Contrast computer tomography (CT) of chest and abdomen 1. to exclude presence of metastasis to the lung and liver and
locoregional spread
Bone scan2. indicated in patients with complaints suggestive of bone
metastasis or with elevated serum alkaline phosphatase
Fluorodeoxyglucose (FDG)-PET/CT 3. initial staging workup4. monitor response to chemoradiation treatment.
5. Detects occult metastasis in 15% of cases

Role of PET CT in Ca Esophagus

Illustration of management impactof PET/CT.

Management impactof PET/CT.

Role of PET CT in Ca Esophagus

Staging





Prognostic factors of esophageal cancer
Disease related1. Stage at diagnosis2. Depth of invasion 3. Tumor volume4. Lymphovascular invasion Patient related• Age• Performance status
Treatment related• Incomplete
pathologic response to preoperative therapy (chemotherapy or chemoradiotherapy) is a poor prognostic factor.

Treatment related• Incomplete pathologic response to
preoperative therapy (chemotherapy or chemoradiotherapy) is a poor prognostic factor.