14 Esophagus

of 38
Transcript of 14 Esophagus
-
7/31/2019 14 Esophagus
1/38
Print | CloseW indow
Note :Largeim agesandtablesonthispagem aynecessitateprintinginlandscapem ode.
Skandalakis' Surg ica l Anatom y > Chapter 14 . Esophagus >
HI STORY
Theanatom icandsurgicalhistoryoftheesophagusisshow ninTable14-1.
Table 14-1. Anatom ic and Surg ica l His tory of th e Esophagus
Sm ithSurgicalPapyrus(3000-
2500B.C.)
Descriptionofa"gapingw oundinthethroatpenetratingthegullet"
Chinese(ca.1000B.C.) Descriptionofdysphagiasecondarytoesophagealcancer
Aristotle(384-322B.C.) Theorizedthattheesophagusgotitsnam efrom "itslengthandnarrow ness"
Galen(130-200A.D.) M entionedgrowthascauseofesophagealobstruction
Lanfranc(d.1315) Placedasilvertubeinthew indpipeofapatientw ithfalsepassagebetweentheesophagusandtracheatoassistbreathing
Vesalius 1543 Usedendotrachealtubetom aintainventilationinanim als
Durston 1670 Mayhaveseenacaseofesophagealatresia
W illis 1679 Firstdescriptionofachalasia;treatm entbydilatation
Gibson 1696 Describeda"m onstrousbirth"withtracheoesophagealfistula
M onroe(1670-1740) Repairedthetracheaandesophagusofapatientw ithseveredtracheaandpuncturedesophagus
Goursald&Roland 1750 M entionedesophagotom yandrem ovalofforeignbodies
Ludlow 1769 D escribedpharyngoesophagealdiverticulumTarenget 1786 Mentionedstrictureofthecervicalesophagus
Bell 1816 Perform edexternaldrainageofthediverticulum
Cam pbell 1848 Triedtoconvinceaprofessionalswordswallow ertoparticipateinexperim entalendoscopy;thelatterreplied,"Iknow Ican
sw allow asword,butI'llbedam nedifIcansw allow atrum pet"
Cheever 1867 Perform edsuccessfulesophagotom ies
Bevan 1868 Describedanesophagoscopew hichusedlightreflectedfrom am irror.Useddeviceforforeignbodyextractionand
exam inationofstricturesandtum ors.
Kussm aul 1868 Designedanesophagoscopeilluminatedbyagaslam p
Trendelenburg 1871 Perform edtracheostom yandinsertedanendotrachealtubew ithaninflatabletam ponw hileadm inisteringanesthesia
Billroth 1871 S tudiedstrictureoftheesophagus
Lam b 1873 Publishedfirstreportofanesophagealfistulawithoutatresia
Zenker 1877 Discussedetiology,pathology,andsym ptom atologyofthepharyngoesophagealdiverticulum (Zenker'sdiverticulum )
Czerny 1877 Perform edesophagealresectionandsuturedthelowerendoftheesophagusintotheneck.Thepatientsurvived.
Nicoladoni 1877 Perform edfirstoperationonapharyngealdiverticulum
Niehans ? Excisedanesophagealdiverticulum ;patientdiedofhem orrhagesecondarytofistula
M acewen 1880 Insertedendotrachealtubesbym outhw ithoutperform inglaryngotom yortracheostom y
M ikulicz-Radecki 1881 Developedesophagoscopeandgastroscope
G ross 1884 Treatedstrictureoftheesophagus
O'Dw yer 1885 Developedendotrachealintubationfordiphtheria,etc.
M ikulicz-Radecki 1886 Treatedcarcinom aoftheesophagusbyresectionandplasticreconstruction
W heeler 1886 Perform edfirstknownsuccessfulresectionofZenker'sdiverticulum
Fell 1887 Usedafootbellowsattachedtoatracheostom ycannulaforartificialventilation
Nassilov 1888 Suggested,butdidnotem ploy,anextrapleuralroutethroughtheposteriorm ediastinum totheesophagus
Biondi 1895 Proposedresectionbypullingthestom achupwardintothechest,followedbyesophagealanastom osis
Milton 1897 Recom m endedm idlinesternotom yforanteriorapproachtothem ediastinum
vonHacker 1899 Diagnosedesophagealcarcinom abyesophagoscopyandbiopsy
Gottstein 1901 Suggestedesophagom yotom yfortreatm entofcardiospasm
Gosset 1903 Describedtransdiaphragmaticesophagogastrostom ythroughthoracotom y
Sauerbruch 1904 Developedandusedanegative-pressuresystem cham ber
Roux 1907 Perform edasuccessfulesophagojejunostom y
Voelcker 1908 Perform edthefirstsuccessfulresectionofthelowerthoracicesophagusbytransabdom inalesophagogastrectom y
Schm id 1912 Perform e ddiverticulopexyoncadavers
Torek 1913 Successfullyrem ovedtheesophagusforcancer.Thepatientw asleftw ithcervicalesophagostom yandgastrostom y.
H eller 1913 Perform edesophagom yotom yfordysphagia
VonAch 1913 Usedbluntdissectionfromneckandabdom enforesophagectom y
Denk 1913 Usedbluntdissectionforesophagealrem oval,w ithlaterrestorationofesophagealcontinuity.Theoperationw asnot
successful.
Zaaijer 1913 Perform edfirstsuccessfultransthoracicresectionforcarcinom aofthecardia
M osher 1917 Usinganendoscope,incisedtheseptum betw eentheesophagusandaZenker'sdiverticulum
Hill 1918 Perform edfirstdiverticulopexyonalivingpatient
Knig 1922 Fixedadiverticularsactothehyoidbone
Torek 1927 Describedpharyngealsuperpressureforsurgery
GrayTurner 1931 Exploredthedistalesophagusfrom theabdom en
1. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
2/38
Historytablecom piledbyDavidA.M cCluskyIIIandJohnE.Skandalakis.
References
Elm slieRG .Perspectivesinthedevelopm entofoesophagealsurgery.In:Jam iesonGG(ed).SurgeryoftheOesophagus.New York:ChurchillLivingstone,1988,pp.
3-8.
HaegerK.TheIllustratedHistoryofSurgery.London:HaroldStarke,1988.
KittleCF.Thehistoryofesophagealsurgery.In:W astellC,NyhusLM ,DonahuePE(eds).SurgeryoftheEsophagus,Stom ach,andSm allIntestine(5thed).Boston:
Little,Brow n,1995,pp.4-29.
NaefAP.TheStoryofThoracicSurgery.Lew istonNY:HansHuber,1990.
SkandalakisJE,GraySW ,ShepardD,BourneGH.Sm oothM uscleTum orsoftheAlim entaryCanal:Leiom yom asandLeiom yosarcom as,aReview of2525Cases.
Springfield,IL:CharlesC.Thom as,1962.
SkandalakisJE,GraySW .Em bryologyforSurgeons(2nded).Baltim ore:W illiam s&W ilkins,1994.
W arrenR.Surgery.Philadelphia:W BSaunders,1963.
Ohsawa 1933 Perform edfirstintrathoracicgastroesophagealanastom osistorestoregutcontinuity
Adam s&Phem ister 1938 Reportedsuccessfulesophagealresectionsw ithesophagogastricanastom osis
Leven&Ladd 1939 Independentlyperform edsuccessfulm ultiple-stagesurgerytotreatesophagealfistulasandatresia
Haight&Towsley 1941 Perform edasingle-stageanastom osisoftheesophagusw ithinthem ediastinum
Churchill&Sw eet 1942 Perform edesophagectom yw ithend-to-sideanastom osis
Garlock 1943 Developedtechniqueforesophagealsurgery
Kaplan 1951 Reportedthefirstuseofelectivecricopharyngealm yotom y
Sw eet 1954 D evelopedsurgicaltechniqueforresection
Skandalakisetal. 1962 Collectivereview ofcasesofsm oothm uscletum orsoftheesophagusasreportedinthew orldliterature
Belsey 1966 D evelopedsurgeryforachalasia
Ellisetal. 1969 StudiedphysiologyofachalasiaandZenker'sdiverticulum
Gavriliu 1975 Reviveduseofthegastrictubeforesophagealreplacem ent
O rringer 1978 R ecom m endedesophagectom yw ithoutthoracotom y
Lieberm ann-M effert 1996 Studiedsurgery,anatom y,andem bryologyoftheesophagus
EMBRYOGENESI S
Nor m a l Dev elopm en t
Inthehum an,theprim itiveforegutform sduringthefourthw eekofgestationbyalongitudinalfoldingandincorporationofthedorsalpartoftheyolk
sacintotheem bryo.2,3,4Thetracheadevelopsfrom theforegutabout22-23daysafterfertilizationasam edianventraldiverticulum 4(Fig.14-1).
Im m ediatelyafterthisdiverticulum form s,thestom achdevelopsfurtherdistallybyanasym m etricalextension3-6(Fig.14-2).
Fig. 14-1.
Divisionoftheprim itiveforegut,w ithstippledareashow ingthefutureesophagealportion.Arrow sindicatethelocalm orphogeneticm ovem ents.Inset:Transverse
sectionthroughprim itiveforegut.Left,Trachea(ventral);Right,Esophagus(dorsal).(Modifiedfrom SkandalakisJE,GraySW .Em bryologyforSurgeons(2nded).
Baltim ore:W illiam s&W ilkins,1994;withperm ission.)
Fig. 14-2.
2. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
3/38
Foregu t
Severalphenom enatakeplaceatapproxim atelythe34thday.Thegenesisofthesubm ucosalandm uscularlayersofbothtracheaandesophagus
begins.Thedistalesophaguselongatesfirst,follow edbytheproxim al.Characteristically,theelongatedesophagealsegm entcarriesthegastric-dilated
prim ordium below theform ingdiaphragm .M ostlikely,how ever,elongationresultsfrom pharyngealascentratherthangastricdescent(Fig.14-2).
Separategrow thprocessesofthetracheaandesophagusoccurbeforethefifthweekofintrauterinelife.Theesophagusattainsitsfinaldim ensionsinthe
seventhweek.Atbirthitslengthis8-10cm ,w hichdoublesinthefirstfew yearsoflife.
Earlyinthesixthweek,them esenchym alcircularm usclecoatdevelops.Threetoninew eekslater,longitudinalm usculatureappears.4Duringthe4th
m onth,them uscularism ucosaappears.Bloodvesselsentertheesophagealw allduringtheseventhm onth,andlym phcapillariesenterthewallbetw een
thethirdandfourthm onthsoflifeafterbirth.7
Attheseventhtoeighthweektheesophageallum en(Fig.14-3)isalm ostfilledw ithcellsfrom theproliferatedesophagealepithelium .Becausethefillingisnevercom pleteandsm allvacuolesarepresent,theso-calledsolidstagedoesnotexistassuch.Aroundthe10thw eekthelum enisrestoredsincethe
vacuolescoalesce.
Theem bryonicgut,show ingtheprim itiveesophagusandthechangesinthepositionofthestom ach.A,Presum ptivestom achareaoftheundifferentiatedforegutat2.5m m (fourthweek).B,At4.2m m (fifthw eek).C,Shapeofthestom achat6.3m m (6thw eek).D, At10m m (endofsixthw eek).E,Shapeanddescentof
stom achessentiallycom pletedat17.5m m (endofsecondm onth).C7,Seventhcervicalsegm ent;T1,Firstthoracicsegm ent;T12,Tw elfththoracicsegm ent;L1,
Firstlum barsegm ent.(Modifiedfrom SkandalakisJE,GraySW .Em bryologyforSurgeons(2nded).Baltim ore:W illiam s&W ilkins,1994)Adaptedfrom
Blechschm idtE.Thestagesofhum andevelopm entbeforebirth.Philadelphia:W BSaunders,1961;w ithperm ission.)
Fig. 14-3.
3. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
4/38
Changesarealsotakingplaceintheesophagealciliatedepithelium ,w hichbecom esstratifiedsquam ousintheproxim alandm iddleesophagus.Colum nar
epithelium rem ainsunchangedinthedistalesophagus.
Theesophagealw allreceivesbothsym pathetic(thoracictrunkandceliacplexus)andparasym pathetic(vagusnerve)innervation.
R emember
Branch ia l Arch Fo rmat i on and t he Esophagus
Theem bryonicm esoderm albranchialarchesplayarolebyparticipatinginthearrangem entofvesselsandnerves.Som eoftheem bryonicm esoderm al
branchialarcheshaveadirectrelationw iththeesophagusbytheirproductionofvesselsandtheirassociationtospecificnerves.
Thethirdbranchialarchisassociatedw iththeglossopharyngeal(IX)nerve.Itparticipatesinaverysm allw ayinthepossibleform ationofpharyngeal
m usclesandthepharyngeallining.Thethirdaorticarchliesw ithinthethirdbranchialarch.Theexternalcarotidarteryarisesdenovofrom thethird
aorticarch.Thecom m oncarotidandtheproxim alinternalcarotidarteriesarederivedfrom thethirdaorticarch.Thesuperiorthyroidarteryperhaps
participatesinthebloodsupplyaroundthepharyngoesophagealjunction.
Thefourthbranchialarchisassociatedw iththevagus(X)nerve.Therightfourthaorticarchcontributestotheform ationoftheproxim alportionofthe
rightsubclavianartery.Theleftsubclavianarterym aybederivedfrom thesixthintersegm entalartery.Thethyrocervicaltrunkarisesfrom the
subclavianarteries.Theinferiorthyroidarteryspringsdirectlyfrom thesubclavianarteryin15% ofindividuals,8andfrom thethyrocervicaltrunkin85% .Theinferiorthyroidarteryisresponsibleforthebloodsupplyoftheupperesophagus.Thearchoftheaortaandtherightdorsalaortaarealso
productsofthefourtharch.M inutevesselsfrom theaortam ayparticipateinthebloodsupplyoftheesophagus.
Thesixthaorticarch,theso-calledpulm onaryarch,m ostlikelydoesnotparticipateinthebloodsupplyoftheesophagus.
Congeni t a l Anom al ies and Surg ica l Repa i r
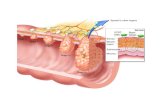
Abnorm algrow thprocessesofthetracheaandesophagusproduceagreatnum berofanom alies.Problem sinthegastroesophagealjunctionproduce
otherlessdram aticeffects(Fig.14-4A&B).
Changesintheshapeoftheesophageallum en.A,At19m m (eighthweek).B,At37m m (ninthweek).C,At42m m (lateninthweek).D,At120m m (aboutthe
fifteenthw eek).(Adaptedfrom Lew isFT.Thedevelopm entofthedigestivetractandoftheorgansofrespiration:thedevelopm entoftheoesophagus.In:KeibelF,
M allFP.Hum anEm bryology,VolII.Philadelphia:JBLippincott,1912;w ithperm ission.)
Bothendoderm andm esoderm participateintheform ationoftheesophagealw all.Theendoderm producestheesophagealepithelium andglands,andthem esoderm producestheconnectivetissue,m uscularcoat,andangioblasts.
Fig. 14-4.
4. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
5/38
Itisnotw ithinthescopeofthischaptertopresentadetaileddiscussionofem bryologyandem bryologicanom aliesoftheesophagus.Kluth9w asableto
classify10typesoftracheoesophagealdefectsand88subtypesofthisanom alyalone.Theinterestedstudentofem bryogenesisisencouragedtoread
Em bryologyforSurgeons.10Them aintypesofcongenitalesophagealanom aliesarepresentedinTable14-2.
aFrom Chittm ittrapapS,SpitzL,KielyEM ,BreretonRJ.Oesophagealatresiaandassociatedanom alies.ArchDisChild1989;64:364-368.
VACTERL,vertebral(abnorm alities),anal(atresia),cardiac(abnorm alities),tracheoesophageal(fistula)and/oresophageal(atresia),renal(agenesisanddysplasia)
lim b(defects);LES,low eresophagealsphincter.
Source:M odifiedfrom SkandalakisJE,GraySW (Eds).Em bryologyforSurgeons,2ndEd.Baltim ore:W illiam s&W ilkins,1994;withperm ission.
Jobeetal.11reportedthatCollis'gastroplastyperm itsatension-freefundoplicationforthetreatm entofshortenedesophagus,butm aintenanceofacid-
suppressiontherapyisadvised.Astosurgicalrepair,Holder12andHolderandAshcraft13advisethatligationofthefistularandprim aryanastom osis,if
possible,shouldbedoneveryearly,preferablywithin24hoursafterbirth,toavoidpneum onitis.Filsonetal.14reportedondelayedprim aryesophageal
anastom osis.Healeyetal.15statedthatdelayedrepairofbothesophagealatresiaandtracheoesophagealfistula,regardlessofgaplength,canpreserve
theesophagus.
A,Pulsiondiverticulaarelocatedm ostcom m onlyinthedistalesophagus.Heterotopicgastricm ucosam ostcom m onlyislocatedattheproxim alesophagus.B,
Usuallocationsofm alform ationsoftheesophagus.(Modifiedfrom SkandalakisJE,GraySW .Em bryologyforSurgeons(2nded).Baltim ore:W illiam s&W ilkins,
1994;w ithperm ission.)
Table 14-2. Anomal ies of the Esophagus
An om aly Pr enat al Age at
Onset
First
Appearance
Sex Chiefly
Af fec ted
R el at i ve Fr e qu e nc y Co m m e n t s
Esophagealatresia,stenosis,and
tracheoesophagealfistula
21to34days Atbirth Equal Com m on
Laryngotracheoesophagealcleft 3rdto5thw eek Atbirth Equal Rare TypeItoIV(larynxtobronchi)
VACTERLassociations Variable;3to5w k
Atbirth Equal 10to23% ofesophagealatresiaa
Esophagealwebsandrings 7thwk(?)(if
congenital)
Anyage M ale Rare M ayneverproducesym ptom s
Trueduplication 7thw k Anyage ? Veryrare M ayneverproducesym ptom s
Enterogenouscysts Endof3rdw k Brithtoanyage Fem ale(?) Rare
Diverticula(excludingtractiondiverticula) 5thm otobirth
(?)
Anyage M ale U ncom m on M uscularw eaknessm ayexistindefinitely
w ithoutherniationoccurring
H eterotopicm ucosa 5thm otobirth Anyage(ifat
all)
Equal(?) Com m on M ayneverproducesym ptom s
Congenitalshortesophagus 7thw k Birthtoanyage M ale Rare M ayneverproducesym ptom s
Achalasia Late6thw k(?) Infancy Equal Uncom m on Casesappearinginlaterlifearenotof
em bryonicorigin
Chalasia Late6thw k(?) Shortlyafter
birth
Equal Verycom m on Resolvesspontaneouslyinm ostcasesas
LESm atures
SURGI CAL ANATOMY
NO TETOTHEREAD ER:Theorganizationofthischapterdifferssom ew hatfrom thatofotherchaptersinthatthephysiology,histology,andm ostsurgical
applicationsoftheesophagushavebeenincorporatedintothepresentationofsurgicalanatom y.
Theesophagus,asoftm usculartube,allow sfoodtopassbetw eenthepharynxandthestom ach.
Aristotle(384-322BC),Greekphilosopherandphysician,suggestedthatthesourceofthewordesophagusrelatedto"itslengthanditsnarrow ness."16
Theterm 'soriginism orelikelyrelatedtotheGreekterm oisopagos,createdfrom oisein("tocarry")andphagos("toeat")orfrom phagema("food").
Theterm ,adoptedbyM edievalLatinandLateM iddleEnglish,becam eisophagusorysophagus.16-18CurrentspellinginGerm anandinBritishEnglishis
oesophagus,inFrenchesophage,andinItalianesfago.
5. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
6/38
InOldRom anLatin,thepopularnounfortheesophagusw asgula.18,19 Gulaw asdefinedasanarrow passage,them outh,orthethroat.From thisLatin
term arosetheEnglishvernacularterm gully,signifyinganarrow courseforwater,anoutlet,ortheneckofabottle.TherelatedOldLatinadjective,
gulosusorgoulu,m eantgreedy,voracious,orgluttonous.TheFrenchwordgulaiskeptaliveasgouleorgueule,m eaningsnoutorm outh.19M ore
recently,theterm gullethasreem ergedinEnglishasasynonym foresophagus.InAm ericanEnglish,esophagusrefersexclusivelyto"thetubeor
channelfrom them outhtothestom ach,byw hichfoodanddrinkpass."18,19
Posi t ion o f t he Esophagus
Theesophagusisam idlinestructureanteriortothespineandposteriortothetrachea.From itsoriginatthecricoidcartilageintheneckoppositethe
fifthtosixthcervicalvertebra,itpassesintothethoraxatthelevelofthesternalnotchandtravelscaudallyw ithinthechestintheposterior
m ediastinum .Itterm inatesintheabdom enattheesophagogastricjunctionoppositethetw elfththoracicvertebra(Fig.14-5).Theesophagealhiatusof
thediaphragm isatthelevelofthetenththoracicvertebra.
Designat ions o f t he Esophagus
Theesophagus,w hichprogressivelydescendsthroughtheneck,chest,andabdom en,hasbeenclassifiedfrom threedifferentm edicalperspectives:
classicalanatom y,function,andsurgicalunderstanding(Fig.14-5).Theseview pointsarediscussedinthefollow ingparagraphs.
Classicalanatom ydividestheesophagusintothreeparts:
Fortheclinician,thisview isunserviceableandhasledtootherperspectives.
Functiondividestheesophagusaccordingtoitsdifferingform sofm otilityintothefollow ingthreezones(Fig.14-5)20:
How ever,thisclassificationalsoem bracesthecoordinatedactionsoftheupperintestinalsystem ,includingtheoropharynx,esophagealsphinctersand
body,andstom ach.Inthiscontext,Diam ant20em phasizesthat"controlm echanism sw ithinthecentralnervoussystem aswellasperipherallywithinthe
intram uralneuralandm uscleproperties,servetointegratethesefunctionalzonesinaregionofthegutw herevoluntaryandinvoluntarycontrol
m echanism sacttogether,andw heretheactivityoftw odifferenttypesofm uscleisintim atelycoordinated."
Surgeonscanbenefitfrom view ingtheesophagusasatw o-partstructuredividedintoproxim alanddistalsegm entsborderingatthetrachealbifurcation
(Fig.14-5).Thisapproachbestm atchessurgicalneedsandtherapeuticstrategies.21Therearethreereasonsforthisapproach:
(1)Antipodallym phaticflow proceedsfrom theareaofthetrachealbifurcationcraniallyandcaudally.4,22,23Thisaffectsthedirectionofearlylym phatic
tum orspreadandtheproceduresoflym phadenectom y.24
Fig. 14-5.
Divisions,term inology,andrelationshipsoftheesophagus.UES,upperesophagealsphincter;LES,low eresophagealsphincter.(CourtesyDr.DorotheaLieberm ann-
M effert;m odified.)
Cervica
Thoracic
Abdom inal
Upperesophagealsphincter(UES)
Esophagealbody
Low eresophagealsphincter(LES)
6. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
7/38
(2)Thesurgicalview pointincorporatestheexpectedlocationsoftum orsandtheirrespectiveprognoses.Carcinom asoccurw ithgreatestfrequencyinthe
m ucosaofthedistalhalfoftheesophagus.25,26Theprognosisfordistaltum orsisfarbetterthanthatfortherarertum orslocatedintheproxim alhalfof
theesophagus.26Proxim altum orsalsorapidlyperforatetheesophagealw alltoinvadeadjacentstructuressuchasthetrachea,bronchi,andadjacent
spacessuchasthem ediastinum .26
(3)Thisclassificationconform sw iththeem bryologicdevelopm entfrom tw odifferenttissuesourcesandthespecificarrangem entofvessels,m uscle
types,andinnervation.4,22,23,27,28Furthersubdivisionofthesesegm entsintocervicalandproxim althoracicanddistalthoracicandabdom inalsections
m aybejustified.26
Conf igu ra t ion o f th e Esophagus
Theesophagusisthenarrow esttubeofthegastrointestinaltract.Itoriginatesatthedistalendofthelaryngopharynx(hypopharynx),atthelevelofthesixthcervicalvertebra.Itterm inatesbywideningtoform thestom ach,them ostvolum inouspartofthegastrointestinaltract.Theesophagusisflatinits
upperandm iddleparts(Fig.14-6A)androundedinitslow erpart(Fig.14-6B).W hendistended,thesepartspresentdiam etersof2.5cm by1.6cm and
2.5cm by2.4cm ,respectively.Theesophagealtubecollapseswhenatrestandrangesinsizefrom 0.6cm to1.5cm indiam eter.29
Ingeneral,theaxisoftheesophagusisstraightw ithonlythreem inordeviationsalongitstrajectory.Thefirstdeviationistow ardtheleftatthebaseof
theneck(seeFig.14-5,arrow 1).Thesecondisatthelevelofthesevenththoracicvertebra,w heretheesophagusturnsslightlytotherightofthespine
(seeFig.14-5,arrow 2).Thethirdandm ostprom inentdeviationislocatedjustabovetheesophagogastric(gastroesophageal)junction,w herethe
esophagusshiftsdorsallyandtotheleft(seeFig.14-5,arrow 3).Anydistortionofthisaxisrevealedbyradiologicalevaluationstronglysuggests
m ediastinalinvasionandretraction.Thecauseism ostoftenam alignantprocess.25,30
Dimens ions o f t he Esophagus
In52adultcadaversthelengthoftheesophagusbetweenthecricoidcartilageandcardiacnotchrangedfrom 21cm to34cm (27cm average).In
fem alecadaverstheaveragedistancewas23cm (standarddeviationof2),andinthem alecadaversitw as28cm (standarddeviationof3).Thelength
relateddirectlytotheheightofthebody(153cm to187cm ).Thecervicalportionw as3cm to5cm ,thethoracic18cm to22cm ,andtheabdom inal3
cm to6cm inlength(Fig.14-5).Inpractice,cliniciansm easuretheesophagusbyusingthenostrilsortheincisorsasthelandm arkform anom etricand
endoscopicprocedures.Thedistancesarefrom 13cm to16cm tothecricoidcartilage,23cm to26cm tothetrachealbifurcation,and39cm to48cm
tothegastricopening.4,23
Tissue Comp os i t ion o f t he Esophagus
Theconstructionoftheesophagusparallelsthebasicplanofthetissueorganizationofthedigestivetube,exceptforthelackofaserosalcoating.The
fourlayers(Fig.14-7)arethetunicam ucosa,telasubm ucosa,tunicam uscularis,andtunicaadventitia.
Fig. 14-6.
Transversesectionthroughtheneckandupperchestofahum anautopsyspecim en.A,Thehistologicalsectionshow stheesophagusstillinm idlineposterior
position.B,Inthem oredistallevelofthem acroscopiccutsurface,theesophagushasshiftedtow ardtheleft(rightinphotograph).Notetheintim atelocalrelationshipbetweenesophagusandtrachea.1,Esophagus;2,Trachea;3,Thyroidgland;4,Vessels;5,Pleura.(CourtesyDr.DorotheaLieberm ann-M effert;
m odified.)
7. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
8/38
Tunica Mucosa
EPI THELI UM I NCLUDI NG GLANDS
Them ucosallayerconfinestheesophageallum en.Itconsistsofthefollow ingthreeparts.
POI NTS OF CLI NI CAL AND SURGI CAL RELEVANCE
Thetransitionbetw eenthem ucosaofthelaryngopharynxandesophagusisinconspicuous.31M acroscopically,theendoscopistseestheesophageal
m ucosaasareddishcolorinitscranialportion.Itturnspalertow ardthelow erthirdoftheesophagus.Thesm oothsurfaceoftheesophagealm ucosacan
bereadilydistinguishedfrom thedark,m am illatedgastricm ucosa.
Thetransitionbetw eenthesquam ousesophagealandcolum nargastricepithelium isanobjectivelyrecognizablereferencepoint.Thisabrupt,serrated
line,know nastheZ-line(Fig.14-8),has"fourtosixsm all,longorshorttongues."32Itisnorm allylocatednearthegastricorifice33,34orjustaboveit.
Endoscopiststhusbasetheirdeterm inationondifferencesincolor,thedegreeoftransparencyoftheepithelium ,m ucosalstructure,andepithelial
thickness.32
Fig. 14-7.
Schem aticillustrationofthetissueorganizationoftheesophagus(E) ,theesophagogastricjunction(EGJ),andthestom ach(S).Theobliquenarrow nessattheentry
intothestom achisshow nintheleftuppercorner.LC,lessercurvature;GC,greatercurvature.1,Tunicaadventitia;2,Tunicam uscularisw ith(a)longitudinaland
(b)circularlayersincludingthem yenteric(Auerbach)nerveplexus;3,Telasubm ucosaincludingthesubm ucous(M eissner)nerveplexusandbloodandlym phatic
vessels;4,Tunicam ucosaw ith(a )m uscularism ucosa,(b )lam inapropriam ucosa,and(c )epithelium includingglands.Arrowindicatesthetransition(Z-line)
betw eenesophagealandgastricepithelium .(Modifiedfrom Lieberm ann-M effertD,DuranceauA.Anatom yandem bryology.In:OrringerM B,Zuidem aGD (eds).
Shackelford'sSurgeryoftheAlim entaryTract(4thed).VolITheEsophagus.Philadelphia:W BSaunders,1996,pp.3-38;reprintedbyperm ission.)
Squamous epitheliumisofthestratified,nonkeratinizingtype.Itnorm allycoverstheinnersurfaceofthelaryngopharynxandthetubularesophagus
Esophagealm ucosacontainsexclusivelyalveolarserousglands.Esophagealcardiacglands,closelyresem blingthecardiacglandsofthestom ach,arepresent
betw eenthecricoidcartilageandthefifthtrachealring.
Esophagealglandsaresm all,tubular,m ucoustypeglandslodgedoutsidethem uscularism ucosa(Fig.14-7).31
Fig. 14-8.
8. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
9/38
Anyproxim alshiftofgastric-orintestinal-typecolum narepithelium intotheesophagusisconsideredpathological.Thechangeresultsfrom long-lasting
gastroesophagealrefluxthatcauseschronicdam agetotheesophagealm ucosa.35,36Theultim ateresultm aybethat"thedistalesophagustoagreater
orlesserextentiscircum ferentiallylinedbycolum narepithelium "32transform edtothegastricorintestinaltype.Thispathology,calledBarrett's
esophagus,isregardedasaprecancerouscondition.26,32,34,36
Katadaetal.37andW etscheretal.38reportedthatincreasedapoptosisintheesophagealepithelium w henBarrett'sesophagusispresentm aybea
protectivem echanism counteractingincreasedproliferation.InhibitionofapoptosisinBarrett'sesophagusisinterpretedbytheseinvestigatorsas
possiblyprom otingneoplasticprogressivediseases.W hatisapoptosis?Inbrief,itisprogram m edcelldeath,theintricaciesofw hicharereview edina
paperbyKuanandPassaro.39AccordingtoCarlson(personalcom m unicationtoW oodandSkandalakis,Feb.19,1998)thefibroblasts"com m itsuicide"
attheendofhealing.Thephenom enonofapoptosisneedsm orestudy.
Theauthorsofthischapterrecom m endbiopsyinallBarrett'spatients.Collardetal.40
believethatearlydetectionofhigh-gradedysplasiainBarrett'sesophagusandradicalesophagealresectionw ithradicallym phnoderesectiongivesthebestchanceofcure.Farrelletal.41reportedthatfundoplication
w illprovideequivalentreliefofsym ptom sforGER D(gastroesophagealrefluxdisease)patientsw ithandwithoutBarrett'sesophagus.
LAMI NA PROPRI A MUCOSA
Sim ilartothelam inapropriaofthestom ach,thelam inapropriam ucosaoftheesophagusconsistsofconnectivetissuebuiltupofareolar,elastic,and
collagenousfibernetworks(seealsoFig.14-24).Inthepharynx,thislayeristhin.Intheesophagus,thelayerism orevolum inousandcontainssm all
bloodvessels,presum ablyterm inallym phatics,follicles,esophagealglandsofm ucoustype,and,intheterm inalesophagus,glandsthatresem ble
cardiacglands.Projectingintotheepithelium ,thelayerform sthepapillae.
LAMI NA MUSCULARI S MUCOSA
Thelam inam uscularism ucosaisathinlayerofshortsm oothm usclebundles.Itbegins6m m to8m m caudaltothepharyngoesophagealjunction.
Thesem usclebundlesarearrangedtransverselythroughouttheesophagealw all.
Inthelaryngopharynx,them ucosalfoldsareratherobliquelyoriented.Achangeoccursjustcaudaltothepharyngoesophagealjunctionw herethe
lam inam uscularism ucosadraw sthelum enintothreeorfourlargelongitudinalesophagealfolds(Fig.14-8).
Structuralchangesoccuratthelow erendoftheesophagus.Herethelam inam uscularism ucosaattainsitsgreatestsizeintheesophagus,42
exhibitsagreaternum berofsm alltransversefolds(Fig.14-8),andtakesarippledshapew hencontracted.33,42,43Thecauseoftheseripplesm aybethelocal
increaseofm uscularm assandthefan-shapedinsertionofitsfibersintothelam inapropriam ucosa.44W hentheendoscopistinflatestheesophageal
lum en,thewallextendsw idelyandthefoldsdisappear.
Atthepointofentryintothestom achtheorientationofthem ucosalfoldsabruptlychangesfrom longitudinalesophagealfoldstotransversegastricfolds
(Fig.14-8).
Tela Subm ucosa
Thetelasubm ucosalayerliesbetw eenthem ucosaandthem uscularcoat.Thetelasubm ucosaofthepharynxisafirm sheaththatfunctionsasan
aponeurosis(pharyngealaponeurosis)45,46anddiffersfrom thelooselyseparatinglayerpresentinthew alloftheesophagusandstom ach(Fig.14-7).At
thislocationthetelasubm ucosaconsistsof:
Esophagealglandsaresm allbranchingglandsofm ixedtypewithductspenetratingthelam inam uscularism ucosa.Thesubm ucosaincreasesinthickness
Schem aticdiagram ofthetissuestructuresattheesophagogastricjunctionasseenfrom thelum inalaspect.Esophagusandstom achhavebeenopenedalongside
thegreatergastriccurvature.Thesidew allsareevertedandshow theintersectingline( i).Thelessercurvatureisinthecenter.Thesubperitonealconnectivetissue
spaceextendsfrom theinsertionofthe(a )uppertothe(b )low erleafletofthephrenoesophagealm em brane.(Modifiedfrom Lieberm ann-M effertD,DuranceauA.
Anatom yandem bryology.In:OrringerM B,Zuidem aGD(eds).Shackelford'sSurgeryoftheAlim entaryTract(4thed).VolITheEsophagus.Philadelphia:W B
Saunders,1996,pp.3-38,reprintedbyperm ission.)
Looseareolarconnectivetissuecontainingelasticandcollagenfibers
Num erousfinebloodvessels(Fig.14-7)
Anetw orkoflym phaticchannels(Fig.14-7;seealsoFigs.14-24and14-27)
Nerves,includingthesubm ucousnerveplexus(Meissner'splexus)
Thedeepm ucousglands(Fig.14-7)
9. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
10/38
acrosstheesophagogastricjunction.
Tunica Muscular i s
Sim ilartoFigures14-9and14-10,thepharyngealm usculatureism ainlyobliquelyarranged.Thetransitionfrom theobliquem uscularfiberstothe
transversecricopharyngealm uscleproducesatriangularareaofsparsem usclecover(Figs.14-9,14-10)cranialtotheupperesophagealsphincter,as
hasbeendescribedanddepictedbyKillian.47Asinglem uscularlayercoatsthelum enofthepharynx,w hereastw odifferentm uscularlayerscoatthatof
theesophagus(Fig.14-10).Them uscleoftheesophagusconsistsofalongitudinallyarrangedouterlayerandatransverseinnerlayer(Fig.14-11).
Fig. 14-9.
Dispositionofthem usclebundlesatthepharynx(P),pharyngoesophagealjunction(PEJ),andesophagus(E) view edfrom posterior.Hum anunopeneddryfiber
specim enfrom autopsyw ithconnectivetissuesrem oved.1, M iddlepharyngealconstrictorm uscle;2,Parsthyropharyngeal;3,Parscricopharyngealoftheinferior
pharyngealconstrictorm usclethatcorrespondswiththeupperesophagealsphincter(UES).Killian'striangleliescranialtotheUES.4,Circularm usclelayerofthe
esophagus.Longitudinalm usclelayerrem ovedw ithonlyresidualbundlespreservedatthelateralaspect.5,Residualsofthethyroidglands;6,Trachea.(Courtesy
Dr.DorotheaLieberm ann-M effert.)
Fig. 14-10.
Thedispositionofthem usclefasciclesatthepharyngoesophagealjunctionfrom theposterioraspect.Thereisonesinglelayerinthepharynxwiththeupperpartof
theconstrictorm uscleobliquelyarranged(m .thyreopharyngeus)andthelow erparttransverse(m .cricopharyngeus).Thisdirectionchangeproducestriangle
cranialtocricopharyngealm uscle.Thecricopharyngeusiscontinuedbytheesophagealm usculature,w ithitstwolayersinoppositeorientation:longitudinaland
transverse.(From Lieberm ann-M effertD.Thepharyngoesophagealsegm ent:anatom yandinnervation.DisEsoph1995;8:242-251;reprintedbyperm ission.)
Fig. 14-11.
10. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
11/38
Functionally,thepharynxandesophaguspresentacontinuum ofsequentialcontractions.Incontrast,histologicallythem uscletypesinthesetw oareas
arecom pletelydifferent.Them uscleofthepharynxisstriated,w hilethelow ertubularesophagusissm ooth.Directlybelow thepharyngoesophageal
junction,isolatedsm oothm usclebundles28,48appearinterm ingledw iththestriatedm uscles.Thenum berofsm oothm usclebundlesincreasesw ithinthe
firstcentim eteroftheesophagealtunicam uscularis.Thisoccurssom ew hathigherintheinner,anteriorm usclelayerthanintheouter,longitudinal
layer.4,23,28Nosharptransitionlinesoccur.Insteadbothm uscletypesrem aininterw ovenw ithoutanyapparentanatom icboundary.Astheydescend,
thesm oothm usclecom ponentssim plybecom em orenum erousandreplace inthesam eproportion thestriatedm uscle(Fig.14-12).Finally,only
isolatedfibersorstrandsofthestriatedtypelodgewithinthesm oothm uscles.4,23,28Caudaltothetrachealbifurcation,thefibersofbothlayersare
exclusivelyofsm oothm uscletype.28,48M easurem entsshow ednoessentialindividualvariation.28
Thearrangem entanddispositionofthem usculatureofthepharynx,esophagus,andstom achview edfrom theleftlateralaspect.UES,Upperesophagealsphincter;
LES,Low eresophagealsphincter.(Modifiedfrom Lieberm ann-M effertD,DuranceauA.Anatom yandem bryology.In:OrringerM B,Zuidem aGD(eds).Shackelford's
SurgeryoftheAlim entaryTract(4thed).VolITheEsophagus.Philadelphia:W BSaunders,1996,pp.3-38,reprintedbyperm ission.)
Fig. 14-12.
Distributionandtransitionofstriatedandsm oothm usculatureinthehum anadultesophagus.Nostriatedm uscleexistscaudaltothetrachealbifurcation.(Modified
from Lieberm ann-M effertD.Anatom y,em bryology,andhistology.In:PearsonFG ,DeslauriersJ,GinsbergRJ,HiebertCA,M cKneallyMF,UrschelHC(eds).
EsophagealSurgery.New York:ChurchillLivingstone,1996,pp.1-25,reprintedbyperm ission.)
11. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
12/38
Tun i ca Adven t i t i a
Tunicaadventitiaispresentedlaterinthechapter.
Pecu l ia r i t ies o f t he Tubu lar Esophagus
Theprim aryorientationsoftheesophagusm usclelayersarelongitudinalandcircular(Fig.14-9andFig.14-10)andthethicknessofbothlayersofthe
esophagealtubeissim ilar,only1m m to1.5m m foreachlayer.Thereisnodifferenceattributabletoage.33,42
Longi tud ina l Musc le Layer
Thelongitudinallayeroriginatesatthecranialm arginofthecricoidcartilageandatthefirm subm ucosaltissuecoveringthearytenoidm usclesthrough
thecricoesophagealtendon(Fig.14-13).Thelongitudinalm usculaturerepresentsonesheathofm ultiple,flat,delicatem usclebundlesthatw rapthe
esophagealw allinacom pletelayer.Adjacentbundlesrarelyconverge,butconnectw itheachotherandwiththecircularm usclebundlesbyseptaof
looseconnectivetissue(perim ysium ).Finevesselsandnervesirregularlyperforatethem usclelayersandcreatelocalovalorlongitudinalslits.The
m usclebundlestraveldirectlylongitudinallydow ntheesophagusforaconsiderabledistance(Fig.14-11)beforetheycrossthegastricorifice.Herethey
becom eorganizedpartlytransverselyalongsidetheanteriorandposteriorgastricw all(Fig.14-11).Beyondtheesophagogastricjunction,the
longitudinalm usclescontinueintothosecoveringthestom ach.
Ci rcu lar Musc le Layer
Thecircularlayerisacontinuationofthecricopharyngeusm uscle,them ostcaudalpartofthem usculatureofthepharynx(Fig.14-11)andthelow est
pointofvoluntarycontrolofsw allow ing.Itbeginsatthelevelofthecricoidcartilageanddescendsalongtheesophagusbyw rappingitcom pletely.Atno
placedothem usclesform closedrings,butpresentim perfectcircleswithsuperim posedends.33
Additionaldistinctivethreadlikem usclestrandsfacetheinnersurfaceofthecircularlayertow ardtheendoftheesophagusandcanbeseenbeneaththe
m ucosaandsubm ucosaaftertheyarerem oved.Theyareshort,thin,sparse,irregularlydistributed,andstraightw ithX-orY-shapedendings.They
correspondtoLaim er's49descriptionandillustrationof"bracketfibers."How ever,theyneverform acontinuouslayerorafascicularnetwork.
Sphinc ters
Sphinctersdividethealim entarycanalintofunctionalsegm ents.Theyarecharacterizedbyarestingtonethatishigherthaninthetwoadjacent
segm ents.Sphinctersareanatom icallyill-defined.
Thewordsphincterisderivedfrom theGreekterm forstring,cord,orlaceandhaslongbeenusedtodesignateacircularm uscle.50Galenem ployedthe
nam eform usculararrangem entsthatw ereabletotieup,tostrangleorthrottle,buthealsoterm edsom eofthem constrictoresoradstrictores
accordingtotheirpropertytoconstrict,draw togetherorcontract.Becauseoftheircircularshape,suchm usclesw erealsoterm edm usculiorbiculares.
Fig. 14-13.
Thishum anautopsyspecim en,fixedw ithalcohol,show sview intothelaryngopharynx,pharyngoesophagealjunction,andcervicalesophagus(1 )from theposterior
aspect.Thesoftpharyngealw all(2 )isshow n,w iththeconstrictorm usculaturedividedandthelineofintersection(3 )reflectedlaterally(arrows).Thetunica
m ucosacoveringtheconstrictorm usclesandthecricoesophagealtendon(4)hasbeenpreserved,butrem ovedabovebothpiriform fossae,lateraltothecricoesophagealtendon(4 )andtheposteriorcricoarytenoidm uscle(5 )toexposethelaryngealpartoftheinferiorlaryngealnerve(recurrentlaryngealnerve[RLN ])
andsuperiorlaryngealnerve(6, 7).CervicalbranchoftheRLN(8 )anditsentryintothelarynxisshow nbetweentwoarrow s.Subclavianarteryisindicatedby(9 ).
Longitudinalm uscleoftheesophagus(1 )insertsatthecranialm arginofthecricoidcartilageandinthefirm connectivetissuecaudaltothecuneiform and
corniculatetubercles(10)oppositetheepiglottis(11)usingthecricoesophagealtendon.(CourtesyDr.DorotheaLieberm ann-Meffert;m odified.)
12. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
13/38
M orerecently,intheanatom icdefinition,sphincterdesignatesacircularoranularm usclesurroundinganopening,51 oraringlikebandofm usclefibers
thatconstrictapassage.17
Theterm cardia,alternativelyusedfortheareaoftheesophagogastricjunction,hastwom eanings:oneistheheart;theother,thegastric
orifice.52,53,54Thenounw asfirstrecordedintheHippocraticw ritingsandreferredtoasthecardiacendofthestom ach.52
Upper Esophageal Sphinc ter ( UES)
Thecom plexm echanism softhepharyngoesophagealfunctions20,55,56thatinvolvesw allow ing,breathing,andspeecharepossiblebecauseofvarious
tissuem aterialssuchasbonyandcartilaginousstructures,andsoftstructuressuchasthepalate,pharynx,andesophagealm usclesincludingthe
supplyingvesselsandnerves.
Thepharynxincludesthenasopharynx,oropharynx,andlaryngopharynx(hypopharynx).Thelaryngopharynxdividesintotw otubes,thelarynxw iththe
trachea,andtheesophagus(Fig.14-14).Thelarynxisform edbyafram ew orkofcartilagesconnectedbym em branesandligam ents;theyarem ovedby
thelaryngealm uscles.Thesestructuresareresponsibleforthem echanism sofairpassage,epiglotticm ovem ent,phonation,and,togetherw iththe
inferiorlaryngealconstrictorm uscles,sphincteractionatthepharyngoesophagealjunction.
Theupperesophagealsphincter(UES )liesattheendofthepharynxandcontrolstheentryintotheesophagusandlarynx.Itisconstructedoftwo
anatom icelem ents.Theanteriorwallisrigid,correspondingtotheposteriorsurfaceofthecricoidcartilagethatalsoform stheposteriorwallofthe
larynx(Fig.14-13).TheposteriorwalloftheUESissoftandform edbyonecontinuousm usclesling,thetransverse,horseshoelikeloopofthelow erpart
oftheinferiorpharyngealconstrictorm uscle(Figs.14-9and14-10).Thiscricopharyngeusm uscleinsertsatthelateralprocessofthecricoidcartilage.
M easurem entsofthem uscularthicknessacrossthepharynxandupperesophagusshow edthatthecricopharyngeus(sphincter)m uscleissm allerbyfar
thanthem oreproxim alpartsofthebilateral,obliquelyarrangedinferiorandm iddlepharyngealconstrictorm uscle.57
Thesphincterservesprim arilytopreventdistensionoftheesophagusduringrespirationandtoprotectthetracheaandlungsagainsttheuptakeofreflux
m aterialorrefluxaspiration.Norm allythesphincterrem ainsinastateofstrong,nerve-controlledtoniccontractionbetw eenepisodesofsw allow ing.
O nm anom etry,theUEShasalengthof2cm to4.5cm andcanbeidentifiedradiologicallybyaposteriorindentation.Theupperesophagealsphincter's
asym m etricalpressurem easurem ents58clearlyequatewithitsanatom icconstruction.
Low er Esophag eal Sphin c ter ( LES)
Thelow eresophagealsphincter(LES)beginsapproxim ately3cm cranialtothejunctionw iththestom ach.Herethenum berofm usclefibersofthe
circularlayerofthetubularesophagusincreaseandsuperim poseoneachother,producingaprogressivem uscularthickening(Fig.14-15).Thisis
consistentw iththerearrangem entofthem usclebundlesacrossthejunctiontothestom ach(Fig.14-16left).Them usclebundlesatthesideofthe
greatergastriccurvaturechangedirectiontoform theobliquegastricslingfibers.Thoseatthesideofthelessercurvatureretaintheirprevioushorizontalorientationtobecom etheshortm uscleclasps33show ninFigures14-11,14-16left,and14-17.
Fig. 14-14.
Positionalrelationshipsofanatom icstructuresinvolvedinswallow ing,breathing,andspeech.Show ninsagittalsection.(CourtesyDr.DorotheaLieberm ann-M effert;
m odified.)
Fig. 14-15.
13. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
14/38
M easurem entsofthicknessoftunicam uscularisbetw eenesophagusandstom ach.Averagethicknessm easuredin32form aldehyde-fixedhum anspecim ensat4
pointsofcircum ferenceandat5m m steps,usingthem axim um thicknessaslandm ark.Num bersclearlydem onstrateasym m etryofLES (low eresophageal
sphincter).EGJ,Esophagogastricjunction.(Modifiedfrom SteinHJ,Lieberm ann-M effertD,DeM eesterTR,Siew ertJR.Threedim ensionalpressureim ageand
m uscularstructureofthehum anlow eresophagealsphincter.Surgery1995;117:692-698,reprintedbyperm ission.)
Fig. 14-16.
Correlationbetw eenradialandaxialm usclethickness(inm m )andm usculararrangem ent(left),andthreedim ensionalm anom etricpressureim age(right)acrossthehum anesophagogastricjunction(EGJ),i.e.low eresophagealsphincter.RadialpressuresattheEG J(inm m ofm ercury)wereplottedaroundaxisrepresenting
atm osphericpressure.PW,Posteriorw all;GC,Greatercurvature;AW,Anteriorw all;LC,Lessercurvature;SM -M,Subm ucosa-M ucosa;M P,M uscularispropria
(sm oothm uscle).(Modifiedfrom SteinHJ,Lieberm ann-M effertD,DeM eesterTR,Siew ertJR.Threedim ensionalpressureim ageandm uscularstructureofthe
hum anlow eresophagealsphincter.Surgery1995;117:692-698,reprintedbyperm ission.)
Fig. 14-17.
14. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
15/38
Thegastricslingfibersbeginattheterm inalesophagus(Fig.14-11),hookaroundtheesophagogastricjunction,andform theangleofHis.Theythen
rundow nattheanteriorandposterioraspectofthestom achandfanoutwardinthedirectionofthegreatergastriccurvature.Theretheyform slings
(Fig.14-11)andendbetw eenthefibersoftheinnerm usclelayerofthegastricantrum .33
TheshortbundlesonthelessercurvesidethatLieberm ann-Meffertcallsclasps33anchorfirm lyintheconnectivetissuealongtheinnerm arginofthe
sheathofthegastricslingfibers(Fig.14-11).Tosom eextent,theseclaspsaresuspendedfrom orpartlysupportedbyfibersofthegastricsling(Fig.14-
17).DiDioandAnderson51show Curti's59originalphotographoftheclaspsintheirpublicationonsphincters,buttheydonotm entionthem .
Them axim um m uscularthicknessoccursatthejunctionbetw eentheesophagusandstom achandtapersoffw ithinthestom ach(Fig.14-15).
M acroscopicexam inationofthefreshspecim enorofthelivingindividualdoesnotrevealm arkedthickening.Thissoft,oftenstretchedm uscletissue
readilyescapespalpationduetoitsconcealedpositionnearthespine,coveredbythefilm yconnectivetissueandfatunderthephrenoesophageal
m em brane.Theanatom icspecim en,how ever,show sthem usculatureinthecontractedstage.Them axim um m uscularthicknessof4m m atthe
esophagogastricjunctionistw icethatoftheesophagusandthestom ach.
Itm ustbestressedinthiscontextthatthenorm alpressuresoftheLESarem uchlow erthanthoseofothersphincters.Theyrangeonlyfrom 14.5m m
Hgto34m m Hg58,60w hile,forexam ple,thepressureoftheupperesophagealsphincterrangesfrom 30m m Hgto142m m Hg.58
POI NTS OF CLI NI CAL AND SURGI CAL RELEVANCE
Therearrangem entofthepharyngealm uscleintotheUES m usculatureleavesanareaofpotentialtissuew eakness(Killian'striangle).Itm aybe
predisposedtotheform ationofaprotrusionofthepharyngealw allcranialtotheUES.47Suchadiverticulum m aycontainthefullthicknessofthew allor
onlym ucosaandsubm ucosa,54butbecauseitoriginatesinthepharynx,itnevercontainsm uscularism ucosa.Zenker'sdiverticulum is,bydefinition,the
m idlineprotrusion.47Laterallaryngopharyngealdiverticuladevelopattheentryofvessels,asdescribedatlengthbyothers.45,46Theyseem toberareinhum ans.Them echanism sleadingtotheform ationofadiverticulum arenotyetclear,andanatom icandpathophysiologiccausesarestilldebated.For
surgicaltreatm entofZenker'sdiverticulum Peracchiaetal.61advisedm inim allyinvasivesurgeryusingalinearendostaplerintroducedthroughaW eerda
endoscope.
Theliteratureincludesabundantclaim sthatthediaphragm aticcrurarepresentthem echanicalequivalentoftheLES.How ever,dissectionofthe
diaphragm and/ordisruptionofthephrenoesophagealm em branealteredneithertheLESpressurenorthepressurecharacteristics.62Regardingthe
norm alanatom iclocationoftheLES ,m uscularrearrangem entandm axim um thicknessarem ostprom inentpreciselyattheesophagogastricjunction,at
thetransitionofesophagealintogastricfolds.33
Thefollow ingpointssupporttheargum entthattheuniquem uscularstructuresattheendoftheesophagusconstitutethephysiologicLES:
M usclestructuresatesophagogastricjunction(atlow eresophagealsphincter)(view from lum inalaspect).Esophagusandstom achopenedalongsidegreatergastric
curvature,thesidew allseverted,andm ucosaandsubm ucosastrippedoff.M usclefasciclesofthegastricsling(1)andclasps(2) exposedandshow ingthefascicular
relationship.Hum anautopsyspecim en.(CourtesyofDr.Nakam uraandProf.M inoriOi,Tokyo.)
Sim ultaneousradiom orphologicalm otilitystudiesusingw allm arkersidentifiedthelocationofm axim um m uscularthickeningatthesiteoftheLEShighpressure
zone.62
W henm usclestripsoftheesophagogastricjunctionareplacedinvitrointoabathoflow dosepentagastrin,theym aintain,orevenincrease,toniccontractions.
M usclestripstakenfrom levelsaboveorbelow donot.63
Theextentofthespecializedm usclestructureisidenticalw iththelengthofthefunctionalsphincter.58,60Theasym m etricm usclebundlearrangem entoftheinnerlayerm atchestheasym m etricthickeningoftheesophagogastricjunctionalm usculature(Fig.14-11bandFig.14-16).Theestablishedaxialandradialasym m etryof
thefunctionalsphincterreflectstheasym m etryofthem uscularstructures.Thisisshow nbydifferentm anom etrytechniques58,64includingthenew technique65-67ofthree-dim ensionalim aging(Fig.14-16right).Inaddition,theirregulardistributionofforceswithintheLESclearlydem onstratestheabsenceofam uscular"ring."
Thespecialm usculature,m usculararrangem ent,andcorrespondingthickeningextendupw ardfor3cm to4cm throughthediaphragm andpassbeyondthedistal
15. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
16/38
Advent i t ia and Stab i l i z ing S t ruc tur es
Tun i ca Adven t i t i a
Incontrasttothebuccopharyngealfasciaintheneck,theperiesophagealtissue,oradventitia,iscom posedoflooseconnectivetissuethatenvelopsthe
esophagusandconnectsitw iththem ediastinum andtheneighboringstructures.Itcontainssm allvessels,lym phaticchannels,andnervefibers.
Tissue Mant le
Theesophaguslieslooselytiedthroughtheadventitiainitsbedofareolarconnectivetissue.Nom esenteryorserosacoatsitw ithinthem ediastinum .
Thispropertyallow stheesophagusgreatm obilitybothintransverseandlongitudinaldirections.Asaconsequence,respirationinducesanesophageal
m ovem entoversom em illim eters,andswallow ingresultsindisplacem entoverafew centim eters.79
Theuniquelocationoftheesophagussubjectsittobluntstrippingfrom them ediastinum w henperform edbythesurgeoninpull-through
esophagectom y.25,27,80,81Bluntdissectionm ayoccasionallybehazardous,how ever,andisstronglycontraindicatedinthepresenceofperiesophageal
tum orinvasion,particularlyifitoccursclosetotheazygosveinorifinflam m atoryadhesionsarepresent.
Theintim ateproxim ityofesophagus,trachea,andpleura(seeFig.14-6)allthew aydow ntothetrachealbifurcation,inconjunctionw iththelackofany
interveningpartitionsorconnectivetissuesheaths,pavesthew ayforreadyandrapidlocalspreadofm alignancyandfistulaform ation.
Tissues Anchor in g and Stab i l i z ing th e Esophagu s
Afram ew orkofbony,cartilaginous,andm em branousstructuresstabilizethepharynxandesophagus(Fig.14-18).Thebuccopharyngealm em brane
attachesthenasopharynxandlaryngopharynxtotheircartilagesandtothecranium and,byw ayoftheprevertebralfascia,tothevertebralcolum n.The
attachm entsoftheesophagusarefarm oreflexiblethanthoseofthepharynx.
endoftheesophagusintothestom achw allforanother1cm to2cm .Theareaofthegreatestfiberconcentrationandm usclethicknessisattheangleofHis.33
Therefore,onem aysuggestthatthegastricslingfibersexerttheantirefluxeffectofthesphincter.53,68,69
Surgicaldisruptionofthejunctionalm usculaturebypartialortotalm yotom yorm yectom ysignificantlyreducesorevenabolishesLESpressurevalues.68,69Forsurgicalm anagem entofpatientsw ithachalasia,them ainprincipleisdivisionoftheLESm usculature.Recently,am odifiedHeller'soperationw ithm yotom yofthe
anteriorw alloftheesophagogastricjunctionhasbeenperform ed.How ever,theproperlengthofthem yotom yisstilldebated.68,70,71Theincisionhasbeencom m onlyrecom m endedtobeginatleast10cm proxim allyontheesophagusandtoextendthem yotom yatleast3cm intothebodyofthestom ach.Thisis
considerablylongerthantheanatom icsphincter.Bom beckandassociates68andEllisandothers72lim itedthelengthofthegastricm yotom yto0.5cm and1cm ,respectively,inordertopreservethefunctionofthesphincter,toavoidrefluxbyitsdisruption,andtoavoiddisruptionofthem uscularslingoftheobliquegastric
fibers.Gozzettiandcow orkers70questionthebenefitofthisfunction-preservingprocedure.How ever,althoughstillextendingthem yotom yfarintothestom ach,theytakegreatcarenottodam agethesphinctericfunctionofthegastricfiberslinganddivideonlythe"m uscularclasps"atthelessercurvature.
Cosentinietal.73reportedexcellenttofairresultsw ithm yotom yandantirefluxsurgeryin23patientsinwhom previousdilatationshadnotyieldedsatisfactory
results.Holzm anetal.74reportedthatlaparoscopicm yotom yisasim pleandeffectivetreatm entforachalasia.SpiessandKahrilas75reportedthatlaparoscopicHeller'sm yotom yisem ergingastheoptim alsurgicaltherapyforachalasia.SincelaparoscopicHellerm yotom yissuperiorinrelievingdysphagiaandpreventing
heartburnforsom e patients,Stewartetal.76preferittothorascopicHellerm yotom y.
KoshyandNostrant77reportedgoodresultsusingbotulinum toxininpatientsw ithesophagealm otordisorders.Endoscopicandballoontreatm entforvariousdysm otilitydisordersarealsoadvised.
Gow enetal.78identifiedfiveriskfactorsforgastroesophagealintussusceptioninpatientsw ithnoncardiacchestpain:
Eatingdisordersoralchoholabuse
Suddensustainedexertion
Sm allbow elobstruction
Acidbilepepticdisease
Pregnancy
Fig. 14-18.
16. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
17/38
ATTACHMENT OF THE CRANI AL END OF THE ESOPHAGUS
Atthecranialendoftheesophagusthecricoesophagealtendon,w hichisastrongtendon2cm to3cm longand1cm w ide,attachesthelongitudinal
esophagealm uscleontotheposteriorplaneofthelam inaofthecricoidcartilage(Fig.14-13,Fig.14-18).
ATTACHMENT OF THE TUBULAR ESOPHAGUS
Betweentheoriginoftheesophagusandthebifurcationofthetrachea,severaldelicatefiberstrands or,m oreprecisely,m em branes anchorthe
esophagealw allelasticallytothetrachea,thepleura,anddorsallytow ardtheprevertebralfascia(Fig.14-18).4,23,82
Research Resul ts
LargefieldhistologicaltransversesectionsintwostudiesbyLieberm ann-M effertetal.4,82show edthatthefiberstrands,orm em branes,thatanchorthe
esophagealw allvaryinnum ber,size,andextensionbutw erepresentinalltheirspecim ens.Theyarecom posedm ainlyofelasticandcollagenfibers
(Fig.14-19).O ccasionallytheycontainstriatedorsm oothm usclebundles.
Atthetrachea,thefiberstrandsinsertm ostoftenm ediolaterallyintothedenseconnectivetissuethatform sthetrachealm em braneorinthe
perichondrium ofthecartilages.Theythenturntow ardthelateralaspectoftheesophagealw all,expandneartheesophagealm uscle,andbecom e
continuouswiththeperim ysium (Fig.14-19).
InhistologicalcrosssectionsbyLieberm ann-M effertetal.,4,82thecoiledstrandspresenteddefinitivelengthsfrom 1m m to17m m andthicknessesof30
to300m icrons(1000m icronsinonesingularcase).W henanalyzedinconsecutiveserialsections,thestrandsactuallyform edlam inatedm em branesof
1.5m m to3cm incraniocaudalextent.Thesam estudiesfoundalargernum berofsim ilarfiberstrandsoriginatinginallspecim ensdorsalto,andlateral
from theesophagus,andradiatingintothem eshesoftheperiesophagealconnectivetissuespaceorinsertingintothetissueofthepleura.
Thetiny,delicate,lam inatedm em branes,individuallyvaryinginnum berandsize,arefarsm allerandshorterthanthelong,coarsefibroelasticcordsthat
Laim er49depictedin1883andNetter83lateradoptedintohisillustrations.Norwastheirorientationfoundtobelongitudinaltotheesophagotracheal
axis,82butinsteadw asregularlytransverse.Oneotherfactorusefulforthestabilizationoftheesophagusnotyetdiscussedisprovidedbythenum erous
finem em branesthatanchoritlaterallyintheconnectivetissuenetw orkofthem ediastinum andtothepleura,andalsom em branesthatextenddorsally,
presum ablytotheprevertebralfascia.
Clinical Considerations and Relevance.O nem ayagreethattheshortanchoringm em branesrestrictthem obilityoftheesophagus.Yet,thecapacityof
thecollagenm em branestoextendandoftheelasticcom ponentstorecoilyieldsadequatem obilitywhentheyarestretchedundernorm altension.W hen
thetinym em branesaretorn,theym aybreakeasilywithoutdam agetoeitherthetrachealorpleuralw all.
Theunpredictablepresenceofindividuallydevelopedcoarserm em branesm aycausedam agew hentheesophagusisstrippedduringesophagectom y.
Therefore,transdiaphragm aticesophagectom ym aybenefitfrom m ediastinoscopicdissectiontoreducetheincidenceoftearsincaseunusuallystrong
m em branesarepresent.Thedistalhalfoftheesophagusw ithinthem ediastinum ism orelooselyadherent.
Anchoringandstabilizingstructuresofesophagusandstom ach.Gastroretroperitonealattachm entsandreflectionsincludegastrophrenic,gastrosplenic,and
splenorenalligam ents,lesserom entum .UES,Upperesophagealsphincter;LES,Low eresophagealsphincter.(Modifiedfrom Lieberm ann-M effertD,DuranceauA.
Anatom yandem bryology.In:OrringerM B,Zuidem aGD(eds).Shackelford'sSurgeryoftheAlim entaryTract(4thed).VolITheEsophagus.Philadelphia:W B
Saunders,1996,pp.3-38,reprintedbyperm ission).
Fig. 14-19.
Oneoftinyfiberm em branes(single arrow)connectingesophagus(1 )w ithtrachea(2) ;5 thicktransversehistologicalsection.M em branem im icsslightlycoiledbandintransversesection,250 m thickand14m m long,and90% elasticfiberelem ents.Typicalfan-shapedinsertionofbandintoperim ysium oflongitudinal,outerlayerofesophagealm usculature(double arrow).Hum anautopsyspecim en,4cm caudaltothelow erm arginofthecricoidcartilage.(Modifiedfrom
Lieberm ann-M effertD,HuberW ,HberleB,W urzingerLJ,Siew ertJR.Relationshipbetweenesophagus,tracheaandpleura.In:NabeyaK,HanaokaT,Nogam iH
(eds).RecentAdvancesinDiseasesoftheEsophagus.New York:Springer,1993,pp.1045-1049,reprintedbyperm ission).
17. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
18/38
ATTACHMENT AT THE DI STAL END
Initspassagethroughtheesophagealhiatus,theesophagusisboundedbythetw odiaphragm aticcruraandthephrenoesophagealm em brane(Fig.14-
18).
Thesubdiaphragm aticandtheendothoracicconnectivetissuesofthediaphragm blendtocreatethephrenoesophagealm em brane(Fig.14-18).This
tissuesheathhasalsobeencalledLaim er'sfasciaorAllison'sm em brane.Becauseitoriginatesfrom afascia,thephrenoesophagealm em braneis
relativelystrong.Them em branesplitsintoparts,describedinthefollow ingparagraphs.
Theuppersheathofthem em braneextendsupw ardfor2cm to4cm throughthehiatus(seeFig.14-8).Hereitsfiberstraversetheesophagealm uscle
andinsertintothetunicam uscularisandthesubm ucosa.84Thisresem blestheinsertionofthetinym em branesthatattachtheesophagealm uscletothe
m em branouspartofthetrachea(Fig.14-19).
Thelow ersheathpassesdow nalongsidethecardiatothelevelofthetopofthegastricfundus.Hereitblendsintothegastricserosa(seeFig.14-8),the
hepatogastricligam ent,andthedorsalgastricm esentery(Fig.14-18).
Thelow ersheathofthephrenoesophagealm em branecanberecognizedduringsurgeryandlaparoscopybyitsw ell-definedlow eredgeandslightly
yellow tissuecolor,evenifsevereperiesophagitisispresent.Them em braneiscom posedofequalportionsofelasticandcollagenousfiberelem ents,
guaranteeingsufficientplasticity.Itw rapstheesophagogastricjunctionlikeawidecollar(Fig.14-18).Despiteasom ew hatloosefibrousconnectionw ith
thewalloftheesophagogastricjunctionthroughtheunderlyingareolarconnectivetissue,theentirephrenoesophagealm em braneclearlyseparatesfrom
theesophagealm uscleacrossthejunction.4,23
Cl in ica l Considerat ions and Relevance
Thestructuralarrangem entofthephrenoesophagealm em braneallow sfreeverticalm ovem entoftheterm inalesophagusandofthejunctionofthe
stom achinrelationtothediaphragm .Itisableto"slipthroughthehiatusasinatendonsheath."85
W ithadvancingage,thetissueproportionsofthephrenoesophagealm em branechange.Collagenousfibersprogressivelyreplacetheelasticfibers,84
looseningtheattachm ents.Them em branebecom esslackandinelastic,andfattissueusuallygathersw ithintheareolarconnectivetissuebetweenthe
m em braneandthem uscularw all.Theresultisalossofpliability.Theseevents,w hencom binedw ithawidehiatus,m aycontributetothedevelopm entofthediaphragm atichernia.84Abnorm allylooseanchorageofthephrenoesophagealm em braneinyouth,togetherw ithanextraordinarilylarge
accum ulationofadiposetissueintheconnectivetissuespacebetweenthephrenoesophagealm em braneandthecardiam usclem aycausesim ilar
problem s.84
Innorm alindividuals,variousfirm ligam entsandm em branesattachthecardiaandgastricfundusposteriorlytothefascialretroperitonealplanes,
providingadequatestabilitytotheesophagogastricjunction.
Inslidinghiatalhernia,boththeterm inalesophagusandgastricfundusprotrudeintothethorax.Inthelesscom m onparaesophagealhernia,the
term inalesophagusispositionednorm ally,butthegastricfundusandbodyadvancebesidetheesophagusintothem ediastinum throughthe
diaphragm atichiatus.86
Inthediscussionofthedifferentetiologicalfactorsleadingtohiatalhernia,onepotentiallyim portantanatom icaspecthasbeenconsistentlyignored.This
isthecloseproxim ityofthegastricfundustothehiatus.Inconjunctionw ithweakeningandslackeningofthegastricattachm entsbyaging,thism ay
producethepreconditionforherniation.4,23Thisconditionw ouldbeconsistentw ithwhatEliska84hassuggestedforslidingherniasandwiththe
observationofEllis,86w hofoundthatthe"sym ptom susuallydeveloponlyinadultsorintheelderly."
Comp ar tm ents and Spaces
Thelooseconnectivetissueinw hichboththeesophagusandtracheaareem beddedisboundedbyfascialplanesanteriorlyandposteriorly,form ingtw o
potentialspacesbetweenneckandchest.Theanteriororpretracheal(previsceral)spaceislim iteddistallybythefibroustissueofthepericardium .The
posteriororprevertebralspacem ay,how ever,extendfrom thebaseoftheskulldow ntothediaphragm .
Theposteriorspaceisofclinicalim portancebecausem ostinstrum entalperforationsoccurinthelaryngopharynxabovethecricopharyngealsphincter.
Subsequentoutflow oftheheavilycontam inatedesophagealcontentspreadsrapidlydow nthefascialspace.Rupturesoftheesophagus(Boerhaave's
syndrom e)andleakageofanesophagealanastom osisoccurringw ithinthechestusuallycauseasim ilareffectbyspreadingupordow nthroughthese
planes.Earlydiagnosisisvitalforthepatient,becausetheprognosisforesophagealperforationisstillpooranddependsentirelyuponsw iftsurgical
treatm ent.
Cons t r ic t ions
Som estructurescom pressthelum enofthetubeandcauseclinicallyidentifiablenarrow ings.Thefirstconstrictioniscausedbythetonusofthe
cricopharyngeusm usclesandisidentifiedabout15cm caudaltotheincisors.Thesecond,theaorticcom pression,iscausedbythecrossingoftheaortic
archandtheleftm ainbronchusat22cm from theincisors.Thethirdnarrow ingisinconstant.Ifprom inent,itislocatedabout44cm from theincisors
andm aybecausedbythetoniceffectofthelow eresophagealsphincter.Thetw om uscularconstrictionscorrespondw iththeupperandthelow er
esophagealsphinctersandcanbeidentifiedm anom etricallyateitherendoftheesophagus.
Vesse ls and Nerves : S t ruc tur es o f Suppor t
Vesselsandnervesaresupportingstructuresoftheesophagus.4,22Theydonotproperlybelongtotheesophagealtissue,butthechannellikevascularor
solidnervecordsfeed,drain,andprovidem otilityandsensoryim pulsestothetissuecom ponentsoftheesophagealw all.Inshort,thesestructures
m aintainesophagealfunction.
Forthepurposeofdifferentiatingthepartsofthesystem locatedexternaltotheesophagusfrom thosew ithinthew all,thestructureshavebeen
classifiedasextrinsicorintrinsic.Botharediscussedbelow .
Ar te r i a l Supp l y
O nem ightbeconcernedaboutfatalm ediastinalbleedingfrom esophagealvessels;how ever,"bluntstripping"oftheesophagusw ithoutthoracotom yfor
carcinom ahasbeenshow ntoberelativelysafe.25,27,80,81Therem arkablylow bloodlossduringtheprocedureandthelow susceptibilityto
postoperativeanastom oticleakssuggestaprim arilypooresophagealvascularsupply.Nevertheless,thesurgicallym obilizedesophagusretainsviability
"overalongdistance,"inthewordsofW illiam sandSpencerPayne,w henhandledcarefully.87
EXTRAMURAL, EXTRI NSI C ARTERIES
ThepharynxandtheUES aresuppliedbysm allarteriesoriginatingfrom thesuperiorthyroidarteries.
I n fer ior Thyr o id Ar ter ies: Cerv ica l Esophagus
Thecervicalesophagusissuppliedbythepairedinferiorthyroidarteries(Fig.14-20).Theyarisefrom thethyrocervicaltrunkofthesubclavianartery.
Theinferiorthyroidarteriesgiveoffbranches2cm to3cm longcalledtracheoesophagealarteries.Thesetravelcaudalandm edialoneachsidetow ard
18. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
19/38
thetracheoesophagealgroove.Thevesselsofbothsidesare"joinedbyanastom otictw igsalongthetrachea"88 anddivideintothreetofourtrachealbranchesw ithtwotothreebranchestotheesophagus.These,inturn,subdividew ithintheperiesophagealtissueintovesselsoflessthan500 m
lum inaldiam eterbeforetheyentertheesophagealw all.Variants,suchasdirectesophagealbranchesfrom thesubclavianartery,thesuperiorthyroid
artery,thethyroideaim aartery,andthecom m oncarotidarteryareinfrequentandratherinsignificant.27,89
Tracheobronchia l and Bronchoesophageal Ar ter ies: I n t r a thor ac ic Esophagus
Theintrathoracicesophagusreceivesbloodfrom tw osources(Fig.14-20):theunpairedtracheobronchialarteries,27,89w hichariseasagroupfrom the
concavityoftheaorticarch27andcannum berbetw eenoneandfour;andthebronchoesophagealartery.Thetracheobronchialarteriesgiveoffseveralsm allbranchestotheesophagusw hichsubdividewithintheperiesophagealtissueintovesselsof350 m to500 m indiam eter.Frequently,one
bronchoesophagealarteryoriginates1cm to3cm caudaltothevascularbundlefrom theanterolateralaspectofthedescendingaorta.27Inthisarea,
w hichrelatestothetrachealbifurcation,allthevesselsarestraightandshort(lessthan1.5cm )andform afirm connectionbetw eentheaorta,trachea,
andesophagus.Variants,ifany,suchasbranchesfrom intercostalarteries,89seem tobeinsignificantforthebloodsupplyofthehum anesophagus.
Aor t ic Proper Esophageal Ar tery : I n t r a thor ac ic Esophagus
O ne(orrarely,tw o)unpairedproperesophagealarterywithalum inaldiam eterof1m m to2m m m ayarisem orecaudallyfrom theanterioraspectof
thedescendingaortaasanexclusivesourcefortheesophagus.27,89Ifpresent,thisvesseltravelsobliquelydow ntow ardtheesophaguswithinthem ediastinum todivideintorecurrentascendinganddescendingbranches.Bothsubdivideintoseveralperiesophagealvesselsoflessthan500 m in
diam eter.
Lef t Gast r ic and Splen ic Ar ter ies: Abdom inal Esophagus and Gast r ic Card ia
Theabdom inalesophagusandgastriccardiaaresuppliedbytheunpairedleftgastric27,89andsplenicarteries.27Thesederivefrom theceliacaxis(Fig.
14-20).W ithasm anyas11arterialbranches,theleftgastricarterym ainlysuppliestheanteriorandrightlateralaspectsoftheesophagealw all.Thesplenicarteryprim arilysupportstheposteriorandleftlateralaspects(cardiacnotch)byeitheroneortwodirectbranchesorbyvesselsofthegastric
fundus,includingconnectionsw iththeshortgastrics.Thebranchesfrom bothstem vesselsthatsupplytheesophagusextendstraightupw ard4cm to6cm w ithintheperiesophagealtissueacrossthediaphragm atichiatus.Atvariabledistancessm alltributariesoflessthan500 m internaldiam eterem erge
beforethem ainvesselspiercetheesophagealw all.27Theleftinferiorphrenicarteryaffordsadditionalarterialsupply.
I NTRAMURAL, INTRI NSIC ARTERIES
Havingpenetratedbothlayersofthem uscularw all,thesm allvesselsform thesubm ucosalplexus.M anyofthefinevesselsinthesubm ucosaparallel
eachotherinlongitudinalorientation.Lessfrequently,othersform circum ferentialvessels.90Num erousarteriolesandvenulesarepresentbeneaththe
epithelium .
POI NTS OF CLI NI CAL AND SURGI CAL RELEVANCE
O neim portantpointisthatafterenteringtheesophagustheperiesophagealbranchesextendtoform adenseandcom pleteintrinsicsubm ucosalnetwork
thatcancom pensateintheeventthatanarteryissevered.Thecontinuityoftheintram uralvascularityretainsviabilityandagoodcirculationovera
longdistancew ithinthesurgicallym obilizedesophagus.27,87Thisalsoexplainsw hycarefullyhandledligationofextram uralvesselsdoesnotcom prom ise
theunderlyingtissueandw hythelineofdissectionm aintainsadequatecirculation.
W iththeexceptionofonevesselofdirectaorticorigin,thevascularpatternderivesfrom thelargerstem vesselsneededforthesupplyofdifferentorgans(Table14-3).Thisdem onstratesthattheesophagusdependson"asharedvasculature."89
Fig. 14-20.
M ostcom m onpatternofarterialsupplyofesophagus.Dotted linesshow largerintram uralanastom oses.Dashed linesbehindstom achshow splenicarteryandits
esophagealbranches.Dim ensionsnotproportional.(Modifiedfrom Lieberm ann-M effertD,DuranceauA.Anatom yandem bryology.In:OrringerM B,Zuidem aGD
(eds).Shackelford'sSurgeryoftheAlim entaryTract(4thed).VolITheEsophagus.Philadelphia:W BSaunders,1996,pp.3-38;reprintedbyperm ission.)
Table 14-3. Commo n Ext r ins ic B lood Sources of the Esophagu s
Sect ion * Sour ces Sh ar in g Or gan s
19. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
20/38
*Inneck,chest,andabdom en,theesophagussharesbloodsupplywithotherorgansbyusingsam evascularsources.
Source:CourtesyofDr.DorotheaLieberm ann-M effert.
Repetitivebranchingofthealreadysm allesophagealvesselsresultsintheform ationofverysm allvesselsintheperiesophagealtissuebeforetheirentry
intothew alloftheesophagus.Thesevessels,therefore,m ayundergocontractilehem ostasisw hentorn.
Acontinuousregularnetw orklocatedinthesubm ucosaconnectsalltheextram uralvessels.Thereisnopoorlysuppliedoravascularzone.Further,
surgicalexperienceclearlyshow sthatproblem sduetocirculatorydisturbancesaregreatlyoverestim ated.Anastom oticfailuresalm ostalw aysarisefrom
thevisceralsubstitute.91
Itiscrucialthattheesophagusreceivesanexcellentbloodsupplythroughlongitudinallyorientedintram uralvesselsthatperm ittheplacem entof
anastom osesatanylevel.Theintram uralnetw orkthusprovidesaluxurious,albeitfine,vascularityfortheesophagusbyasystem ofsm allarteries,
arterioles,andcapillaries.Nevertheless,thisareaneedscarefulsurgicalhandling.
Venous Dra i nage
Theintram ural,intrinsicveinscom m enceasfinevenulestoform thesubepithelialplexuswithinthelam inapropriaofthetunicam ucosa(Fig.14-21).
Theyreceivebloodfrom theadjacentcapillariesanddrainintothesubm ucosalplexus.92,93
Aharinejadetal.90recentlystudiedthehum anm icrovasculaturesystem indetail.Theyobservedthattw osm allveinsusuallyaccom panythe
circum ferentialarteriesinthelam inasubm ucosa.Perforatingveinsoriginatingfrom thesm allcom m unicatingveinsofthesubm ucousplexuspiercethe
m uscularw alloftheesophagustogetherw iththeperforatingarteries.Theyreceivetributariesfrom them usclecoatsandform theextram ural,extrinsic
veinsatthesurfaceoftheesophagus.90-93Novalvesw erefoundintheesophagealvenouscirculatorysystem .
Theextrinsicveinsdrainintothelocallycorrespondinglargevessels.Thesuperiorvesselsdraintothejugularveinsortheazygosandhem iazygosveins.
Theinferiorveinsterm inateintheleftgastricandsplenicveins.
Asw elldescribedin1918byElzeandBeck,94therearetw oclearlydelineatedvenousplexusesinthelaryngopharynxwithintheextrem elythin
subm ucosabeneaththem ucosa(Fig.14-22).Theseareexactlyatthelevelofthepharyngoesophagealjunction.O neplexusliesonthedorsalaspectof
theinferiorconstrictorm uscle;theotherinthem idlineposteriortothecricoidcartilage.
Cervical Twopairedstemvessels +Thyroidgland
+ Trachea
Thoracic Severalunpairedstem vessels + Trachea
+ Bronchi
Properunpairedvessel N one
Abdom inal Twopairedstem vessels +Stom ach
+ Spleen
Fig. 14-21.
Diagram ofvenousdrainageofesophagusinnorm alhum an.(Modifiedfrom KitanoS,TerblancheJ,KahnD,Bornm anPC.Venousanatom yofthelow eresophagus
inportalhypertension:practicalim plications.BrJSurg1986;73:525-531,reprintedbyperm ission.)
Fig. 14-22.
20. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
21/38
Tenspecim ens(unpublisheddatabyLieberm ann-Meffert,publicationinpreparation)show edbothplexusestobesim ilarinsize,approxim ately2cm to3
cm w ide,andconsistingofseveralthickveinswitham axim um w idthof4m m .Thesew ereprim arilylongitudinalinorientationandwerejoinedby
severaltransverseanastom oses.Theseveinsreceivebloodfrom them ucosaofthelaryngopharynx,larynx,andesophagusanddrainintothethyroid
andjugularveins.94Thesevenousplexusesm aycausearecognizablepostcricoidim pressionontheesophagus95,96andm aybeinvolvedinthe"globus
sensation"inpatientsw ithvenousstasisandtissuesw elling.47,94Theseplexusesm ayalsocontributetothecom petenceandactionoftheupper
esophagealsphincter.
Viannaetal.97clearlydocum entedaspecializedvenousarrangem entattheterm inalesophagus(Fig.14-23).Thesevenousanastom oseshavebeen
suggestedtopossiblysupplycom m unicationbetweentheazygosandtheportalsystem .Theinterm ediate"palisadezone"(Fig.14-23)m ayactasa
high-resistancewatershedbetweenbothsystem s,providingbidirectionalflow .97
Laryngopharyngealvenousplexusesview edfrom posterioraspectasdepictedbyElzeandBeck.94Thefirstdeepplexus(depictedontheleftsideofthedraw ing)liesm edialontheanteriorsideofthepharynxcoveringtheposterior,transverse,andobliquearyepiglotticm usclesandthehardposteriorsurfaceofthecricoid
cartilage(seenfrom thelum inalaspectofthepharynx).Aseconddeepplexus(shiftedaftercuttingofthew alltotherightsideofthedraw ing)liesexactlyonthe
oppositesideofthelum enofthepharynx,posteriorlyunderneaththeinferiorconstrictorm usclesandthecricopharyngealm uscles(UES ).(Modifiedfrom ElzeC,
BeckK.DievensenW undernetzedesHypopharynx.ZOhrenhk1918;77:185-194.)
Fig. 14-23.
21. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
22/38
Inapaperaboutprogressandchangesinsurgery,Idezuki98statedthatoverthelastfivedecades,theacceptedtreatm entofesophagealvariceswith
portalhypertensionhasm ovedfrom decom pressionshuntstoselectiveshuntsanddirectoperation,andnow toendoscopicsclerotherapy,som etim es
com binedw ithvaricealligation,ortotransjugularintrahepaticportosystem icshunt.Hashizum eetal.99reportedthatlaparoscopicgastric
devascularizationandsplenectom yforsclerotherapy-resistantesophagogastricvaricesinpatientsw ithhypersplenism isafeasibleandrelativelysafe
procedure.
Jenkinsetal.100statedthatdistalsplenorenalshuntisasafe,durable,andeffectiveprocedureforthetreatm entofrecurrentbleedingsecondaryto
gastroesophagealvaricesandportalhypertensioninpatientsw ithacceptableoperativeriskandgoodliverfunction.
Lympha t i c Dra i nage
Presum ablyduetotheconsiderabletechnicaldifficultyofidentifyingthem inutechannelsbothinvivoandpostm ortem ,anatom icknow ledgeofthe
lym phaticsystem oftheesophagusisextrem elylim ited.Accountsofpreviousinvestigationshavesofarnotbeensubstantiated.4,23Neverthelessone
m ayacceptthatthelym phaticsystem oftheesophagusincludesthelym phductsandlym phnodesasdescribedforotherpartsofthegut.
Lym phcapillariesm aycom m enceinthetissuespacesasanetw orkofendothelialchannels(Fig.14-24)orasblindendothelialsacculations(Fig.14-25)
sim ilartothosefoundinm esenterictissues.101,102
Radiographicillustrationofvenouscirculationinm iddleandlow eresophagus,esophagogastricjunction,andstom achafterinjectionw ithbarium gelatin.Various
zonespresentdifferentvenousarchitecture.Afew longitudinallyarrangedveinsintruncalzone(TZ),additionaltransverseveinsinperforatingzone(PfZ),unique
arrangem entofveinsinpalisadezone(PZ)thatseem stocorrespondtoareaofam pullaofradiologists,andgastriczone(GZ)w ithnetlikerearrangem entofveins.
(From ViannaA,HayesPC,M oscosoG,DriverM ,Portm annB,W estabyD,W illiam sR.Norm alvenouscirculationofthegastroesophagealjunction.Arouteofunderstandingvarices.Gastroenterology1987;93:876-889,reprintedbyperm ission.)
Fig. 14-24.
22. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
23/38
Initiallym phatics(arrows)betw eenlow erborderoftunicam ucosaandtelasubm ucosainthehistological( A) andelectronm icroscopic( B) display.Takenfrom
gastricwall,butisrelevantalsoforesophagus.MM,m uscularism ucosae.(A,from LehnertT,ErlandsonA,DecosseJJ.Lym phandbloodcapillariesofthehum an
gastricm ucosa.Am orphologicbasisform etastasisinearlygastriccarcinom a.Gastroenterology1985;89:939-950,reprintedbyperm ission.B,CourtesyDr.
DorotheaLieberm ann-M effert.)
Fig. 14-25.
23. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
24/38
Thesubm ucosaofthehum anstom achhasrecentlybeenshow ntocontainanetw orkofnum erouslym phvessels.Theseshow parallelorientationalong
thelongitudinalaxisoftheorgan(Fig.14-26).Theysendoccasionalbranchestothecollectingsubadventitialandsurfacetrunks.97Allthesechannels
possessvalves(Fig.14-25).StudiesbyM ayrandLieberm ann-M effert103usingautopsyspecim ensandelectronm icroscopictechniquesim plythata
sim ilarpatternispresentintheesophagus.Initiallym phaticsseem tooriginateexclusivelyintheregionbetw eenthem ucosaandsubm ucosaandtoform longitudinallyarrangedcollectingchannelsinthesubm ucosa.
Initiallym phaticnetworkinm esenteryoriginatesinblindendothelialsacculationsandsm allchannels.M easurem entsrefertothediam eterofthelym phaticvessels.
(Reconstructionfrom apreparationafterdirectinvivoinjectionofdyeintolym phaticchannelsofgreaterom entum .)(ModifiedafterZw eifachBW ,PratherJW .
M anipulationofpressureinterm inallym phaticsinthem esentery.Am erJPhysiol1975;228:1326-1335;w ithperm ission.)
Fig. 14-26.
24. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
25/38
Thelym phatictrunksatthesurfaceoftheesophagusm aydrainintotheregionallym phnodes.Lym phfrom theesophagusm ostlikelydrainsintothe
follow inglym phnodes
104,105,106
:
Thelym phoftheabdom inalesophagusem ptiesintothefollow inglym phnodes:
Innoncancerousautopsyspecim ens,Lieberm ann-M effertetal.andMayrandLieberm ann-M effert4,103,107foundonlyafew sm alllym phnodesinthe
m ediastinum .Thelym phnodeswerelargerandm orenum erousaroundthetrachealbifurcation.M ostofthesecontainedblackcoal-likeparticles.The
authorscouldnotdeterm inewhetherthesenodesdrainedtheesophagusand/orthelungsoriftheytransportedproxim allyordistally.Thisobservation
coincidesw iththereportofW irthandFrom m hold108
w hofoundm ediastinallym phnodesinonly5percentof500norm allym phogram s.Theclassicalchainoflym phnodessurroundingtheesophagusasdescribedintextbooksandillustratedbyNetter83couldnotbesubstantiatedatthistim e.
POI NTS OF CLI NI CAL AND SURGI CAL RELEVANCE
Theclinicalobservationthatinitialtum orspreadfollow sthelongitudinalaxisoftheesophagusw ithinthesubm ucosaratherthanextendinginacircular
m annersupportsthefollow ingconcepts:
Thepaucityoflym phaticsw ithinthelam inam ucosaandtheabundanceofsubm ucosallym phaticchannels101,109(Fig.14-26)m ayexplainwhy
intram uralcancerspreadspredom inantlyw ithinthislayer.Undetectedm alignantm ucosallesionsm aybeaccom paniedbyextensivetum orspread
underneathanintactm ucosa.Tum orcellsm ayfollow thelym phaticchannelsforaconsiderabledistancebeforetheypassthem uscularcoattoem pty
intotheregionallym phnodes.
Tum or-freem arginattheresectionline,asconfirm edbytheanatom icpointofview (histologic),doesnotguaranteeradicaltum orrem oval.Thisfeature
m aybeconsistentw iththerelativelyhighpostoperativerecurrencerateattheresectionline,includingsatellitetum orsandm etastasisinthesubm ucosafardistantfrom theprim arytum or,25evenifthem arginsattheresectionlinehadbeenpreviouslytum or-free.
Law etal.110reportedthathistologictum orinfiltrationattheesophagealresectionm arginsonpatientsw ithesophagealcarcinom am ostlikelyisnot
responsibleforleakage.Theanastom oticrecurrencewasrelatedtothelengthofesophagealresectionm argin.
Locallym phaticdrainagewithinesophagealw all.A,Lym phaticflow asexpectedundernorm alhealthyconditionsandinearlym alignancy.Valves,presentevenin
sm allchannels,determ inetheflow direction(seeFig.14-27).B,Flow m ayreversew hentum orm assesblocklym phaticpathw ays;resultingelevated,reversed
pressurem ayinterferewithfunctionoflym phaticvalves.(A,M odifiedfrom Lieberm ann-M effertD,DuranceauA.Anatom yandem bryology.In:OrringerM B,
Zuidem aGD(eds).Shackelford'sSurgeryoftheAlim entaryTract(4thed).VolITheEsophagus.Philadelphia:W BSaunders,1996,pp.3-38;reprintedby
perm ission.B,CourtesyDr.DorotheaLieberm ann-M effert,m odified.)
Fig. 14-27.
Lym phaticpathw aysofesophagus.Alsoshow show ,undernorm alconditions,lym phfrom areasabovetrachealbifurcationem ptiescranially,andlym phfrom below
thatpointpreferentiallyem ptiescaudallytopassthroughceliaclym phnodes.Flow attrachealbifurcationseem stobeorientedbidirectionally.Thisfeatureis
essentialtounderstandingofpotentialspreadofm alignancies.(Modifiedfrom Lieberm ann-M effertD.Anatom y,em bryology,andhistology.In:PearsonFG ,
DeslauriersJ,GinsbergRJ,HiebertCA,M cKneallyMF,UrschelHC(eds).EsophagealSurgery.New York:ChurchillLivingstone,1996,pp1-25,reprintedby
perm ission.)
Paratrachea
Tracheobronchialbifurcation
Juxtaesophageal
Intraaorticoesophageal
Superiorgastric
Pericardiac
Inferiordiaphragm atic
Lym phflow sm orereadilylongitudinallyinthesubm ucosalchannelsthanthroughthefew transverseconnectionsinthem uscle(Fig.14-26)
Lym phflow sonlyfinallythroughthesubadventitiallym phaticsandsm alltrunksintothem ediastinallym phnodes4,23
Asaconsequence,esophagealtum orsm ayspreadfarcraniallyorcaudallywithintheesophagealsubm ucosalchannelsbeforeobstructingthelum en
25. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
26/38
From clinicalobservationsincancerpatients,23,25,26thefollow ingpatternsm aybededuced(Fig.14-27):
Nakagaw aetal.112reportedthattum orangiogenesisexpressedasm icrovesseldensitycorrelatesw ithclinicopathologicparam etersfortum or
progression.Theyconsiderthisanindependentprognosticindicatorforpatientsundergoingextendedradicalesophagectom yforinvasive[squam ous
cell]esophagealcancer.
Cooperetal.113reportedthatcom binedchem oradiotherapyincreasesthesurvivalrateofpatientsw ithsquam ouscellcarcinom aoradenocarcinom aof
theesophagusoverradiotherapyalone.
I n n e r v a t i o n
Thepharynx,larynx,andesophagusareinnervatedbybothvisceralcom ponentsoftheautonom icnervoussystem ,thesym patheticandthe
parasym patheticsystem s,w hichexertm utuallyantagonisticinfluencesontheviscera.20,31,114,115Thesym patheticefferentpathw ays,com m oninthe
gut,areconcernedw ithvasoconstriction,contractionofsphincters,andrelaxationofthem uscularwall.Theparasym patheticefferentfibersincreasethe
glandularandperistalticactivityofthegut.20
SYMPATHETI C N ERVES
Thesym patheticnervessupplythepharynx,larynx,andproxim alesophagusthroughthecervicalandthoracicsym patheticchains(Fig.14-28).These
chainstraveldow nw ardlateraltothespineandfrom thecardiobronchialandtheperiesophagealsplanchnicnervesthatarisefrom theceliacplexus.
Interlacedwithfibersoftheparasym patheticcervicalandthoracicplexuses,thesym patheticnervoussystem usesthevagusnerveasacarrierforsom e
ofitsfibers.31
PARASYMPATHETI C NERVES
Theparasym patheticnervesupplyisthroughthevagus,thetenthcranialnerve.Thevaguscarriesgeneralsom aticandvisceralsensory,skeletalm otor,
andparasym patheticfiberstotheesophagus.Thelaryngopharynxreceivesgeneralsom aticsensoryandskeletalm otorinnervationviathevagusnerve.
Thesensoryneuroncellbodiescontributetoform ingtheganglionnodosum (Fig.14-28).
Therightandleftvagipassasthicktrunksthroughtherespectivejugularforam ina.Theinnervationofthem usculatureandm ucosaofthepharynx,
larynx,UES,andupperhalfoftheesophagusisbythebilateralsuperiorlaryngealnerves(SLN )and/orinferiorlaryngeal(recurrent)nerves(RLN ).The
SLN issaidtobem ainlysensoryandsecretory,althoughitsexternallaryngealbranchism otortothelarynxandthecricopharyngeus.TheRLNislargely
m otorandsuppliesm ostofthelaryngealm usclesandtheUES.
Thesuperiorlaryngealnerveoriginatesfrom thevagaltrunknearthenodoseganglion,travelsdow nalongsidethecarotidarteries,anddividesintothe
internallaryngealbranchandtheexternallaryngealnerve.Thislatternervesuppliesthecricothyroidm uscleandthecricopharyngeusportionofthe
inferiorpharyngealconstrictor,w hichservesastheupperesophagealsphincter.Theinternallaryngealnerve,containingparasym patheticandsensory
fibers,suppliesthelaryngealm ucosaabovethevocalfoldsandtheregionofthepiriform fossae.31,116-118
TheRLNarisesontherightsidefrom thevagusnerveinfrontofthesubclavianartery,turnsbackw ardaroundtheartery(Fig.14-28),andascends
obliquelytotherightlateralaspectofthetracheaandposteriortothecom m oncarotidartery.31,116,117
O ntheleftsidetheRLNarisesfrom thevagusnerveinfrontoftheaorticarch,turnsbackw ardaroundtheaortabehindtheligam entum arteriosum ,and
ascendsobliquelytotheleftofthetrachea.
Lym phfrom abovethecarinaflow scraniallytow ardthethoracicductorthesubclavianlym phtrunks31
Lym phfrom below thecarinaflow sm ainlytowardthecisternachyliviathelow erm ediastinal,leftgastric,andceliaclym phnodes31
Flow m aychangeunderpathologicalconditions.111W henlym phvesselsbecom eblockedanddilatedduetotum orinvasion,thevalvesbecom eineffectualandtheflow reverses(Fig.14-26).Thisphenom enonexplainstheretrograde,unexpectedspreadofsom eofthem alignanttum ors,butlim itsthevalueofestablishing
pathw aysofnorm alflow .
Fig. 14-28.
Innervationofesophagus.(Modifiedfrom Lieberm ann-M effertD,DuranceauA.Anatom yandem bryology.In:OrringerM B,Zuidem aGD (eds).Shackelford's
SurgeryoftheAlim entaryTract(4thed).VolITheEsophagus.Philadelphia:W BSaunders,1996,pp.3-38,reprintedbyperm ission.)
26. oldal, sszesen: 38 oldalPrint: Chapter 14. Esophagus
2012.03.20.mk:@MSITStore:D:\Sebszet\Surgical%20Anatomy%20The%20Embryologic%20A...
-
7/31/2019 14 Esophagus
27/38
AsbothRLNstravelcranially,theyapproachtheesophagusandtrachea,oftenpositioninginthetracheoesophagealgroove,117 andtheydistributean
equalnum berofnervefiberstobothstructures(Fig.14-29).Reachingthepharyngoesophagealjunction,bothRLNsgaincloseproxim itytothe
esophagus,theleftsideusuallycloserthantheright.Nearthelow erpoleofthethyroidgland,bothnervesarealwaysintim atelyrelatedtotheglandand
oftenpassbetw eenbranchesoftheinferiorthyroidvessels(Fig.14-29).Som eofthenervebranchesdipintotheparenchym aofthegland.
O nbothsides,asinglethickterm inalbranchoftheRLNentersthelarynxjustbelow thecricopharyngealm uscleband(Fig.14-29).Herebothdivideinto
severalbranchestosupplyalltheintrinsiclaryngealm uscles(exceptthecricothyroid),includingthearytenoid(vocal)andepiglotticm uscles.
O ccasionallythem ajorterm inalbranchcom m unicatesw iththesuperiorlaryngealnerve107(seeFig.14-13).
Posteriortothelunghilum atthelevelofthetrachealbifurcation,thevagalnervesform anetworkoffascicles,thepulm onaryandesophagealplexus.
Theleftvaguscontributesprim arilytotheanterior,andtherightvagustotheposterioresophagealplexus.
Atthelow erendoftheesophagus,thefibersreorganizeintotw otrunksthatpassdow nontheanteriorandposterioresophagealw all.118Togetherw ith