Pediatric Surgery - semcme.org · – C = atresia with TEF between distal esophagus and trachea –...
39
Pediatric Surgery
Transcript of Pediatric Surgery - semcme.org · – C = atresia with TEF between distal esophagus and trachea –...

Pediatric Surgery
ddx of double bubble sign
• ddx of double bubble sign:
• duodenal atresia
• malrotation
• annular pancreas
• MUST DO UGI (or LGI) contrast study to
R/O malrotation (surgical emergency)

gastroschisis Omphalocele

General considerations
• Daily maintenance fluids: 100ml/kg/d 0 – 10 kg 4ml/kg/h first 10 kg
50ml/kg/d 10 – 20 kg 2ml/kg/h second 10 kg
25ml/kg/d >20kg 1ml/kg/h each add. kg
• Central venous access
– External jugular, facial, saphenous veins
• Blood volume / replacement
– Total blood volume = 85ml/kg
– Transfusion = 10ml/kg (similar to 500ml in adult)
Pyloric stenosis
• Most common cause of vomiting in infancy
• Typically 4-6 weeks old, male, first born
• Projectile, nonbilious emesis with near complete obstruction
• Metabolic alkalosis, ↓K+, Cl-
• Urine pH ↑ initially, then ↓ as H+ ions excreted for Na in distal tubule
• PE – classic “olive” in RUQ, visible gastric waves
• US can make diagnosis in 95% of cases when PE unclear
• Must first fluid resuscitate (D5W, 0.45NS, +2-4meq/kg K+ at a rate of 150-175ml/h over 24hrs)
• Freder- Ramstedt pyloromyotomy = seromuscular layers of the pylorus excised down to submucosal layer allowing mucosa to herniate through incision
• Oral feedings resumed post-op, gradually increasing strength and volume, usually discharge in 48 hours
Lesions of the NeckThyroglossal duct cyst
• Thyroid develops at base of tongue (foreamen caecum), migrates
anterior and caudal
• Remnants of the thyroid migration may persist in midline of neck
• Usually apparent in children age 2-4yo when baby fat subsides
• Moves up and down with swallowing and tongue protrusion
• May become infected, needs I&D, then resection
• May be ectopic thyroid tissue, must feel normal thyroid first or do scan
• Resection (Sistrunk operation) involves removal of tissue, tract up to
base of tongue, midportion of hyoid bone, ligation of foramen cecum

Lesions of the NeckBrachial cleft anomalies
• Usually remnant of second brachial cleft
• Presents as fistula tract form pharynx to anterior border of SCM
• Typically drains clear fluid
• Tract extends superiorly from skin through carotid bifurcation to posterior
lateral pharynx at base of tonsillar fossa
• Surgical treatment only cure, must excise entire tract
• Step ladder incisions better cosmetically, use probe or dye to follow


Lesions of the NeckCystic hygroma
• Results from sequestration or obstruction of development of lymph channels
• Most common sites are posterior triangle of neck, axilla, groin, mediastinum
• Usually multiple cysts containing lymph fluid, cause local distortion
• May be present at birth, usually appear in first two years of life
• Can become infected with Staph or Strep → percutaneous drain
• Radical excision not advised in this benign lesion
• Conservative resection with unroofing of cysts indicated, may go back and
do re-excision to preserve vital structures


Congenital Diaphragmatic Hernia
(Bochdalek)
• Occurs when pleuroperitoneal canal does not close resulting in posteriolateral defect, commonly on left side (Morgagni - anterolateral)
• Abdominal cavity small, poorly developed, scaphoid
• Lungs hypoplastic bilaterally, decreased weight, volume and vasculature
• Can be detected by US as early as 15 weeks gestation
• Infants born hypoxic, hypercarbic, acidotic, persistent pulmonary HTN
• Immediate surgery usually not performed, placed on ventilator
• ECMO (extracorporeal membrane oxygenation) often needed to support infant 1-3 weeks
• Surgical approach through abdomen, 3/4 require synthetic patch
• May need to make abdominal wall defect or silo temporarily


Congenital Lobar Emphysema
• Results from intrinsic poor bronchial cartilage development
• Causes trapping of air and hyperexpansion of affected lung tissue
• Occurs in upper lobes the most, then middle, then lower lobes
– LUL (40%) > RML (35%) > RUL (20%) > lower lobes (<1%)
• Affected lobe over inflates and compresses normal lung
• Symptoms range from mild respiratory distress to complete failure
• CXR diagnostic showing hyperlucent affected side, compressed
adjacent lobes and shifted mediastinum to unaffected side
• 14% of children have associated cardiac defects
• Treatment is resection of affected lobe

Other Respiratory Disorders
• Pulmonary sequestration– Extralobar = Nonaerated, systemic blood supply, above left
diaphragm, usually asymptomatic, no tx necessary
– Intralobar = Within lung parenchyma, usually left side, also nonaerated, arterial supply from aorta below diaphragm, often causes infection, venous drainage to pulmonary vein, may need resection of entire L lower lobe to cure
• Bronchogenic cyst– Hamartomas, occur anywhere in respiratory tract, usually simple
cysts with respiratory epithelium, cartilage, smooth muscle
– May be asymptomatic, cause infection or airway compression
– CXR or CT shows dense mass; tx is simple cyst resection
Foreign Bodies
• Respiratory
– Usually toddler age, peanut most common object, hyperlucency
of affected lobe seen
– Most often ends up in R main stem bronchus or R lower lobe
– Mild respiratory distress or unilateral wheezing seen
– Remove with bronchoscopy
• Esophagus
– Toddlers, most commonly coins, may require contrast swallow
– Lodges in one of three places where the esophagus narrows –
cricipharyngeus, aortic arch, GE junction
– May cause drooling (inability to swallow), often asymptomatic
– Usually requires UGI endoscopy for removal

Esophageal atresia
Tracheoesophageal fistula
• Occurs when esophagus and tracheal fail to divide into
separate tubes at around 5 weeks gestation
• Catagorized by Gross-Vogt into five types
– A = atresia without fistula
– B = atresia with TEF between proximal esophagus and trachea
– C = atresia with TEF between distal esophagus and trachea
– D = atresia with TEF between both proximal & distal esophagus
– E = TEF without atresia (H type)
• 85% are type C, allows air in stomach and aspiration
• Congenital anomalies common (VATER)
Vertebral Anorectal TracheoEsophageal Renal


Esophageal atresia
Tracheoesophageal fistula cont.
• Clinical manifestations → regurgitation and drooling,
feedings followed by choking or coughing, abdomen
either distended (TEF present) or scaphoid (no TEF)
• Diagnosis may be made with prenetal US, or by a tube
coiled in the upper pouch
• Contrast media may be given to determine the type of
atresia/TEF
• Need to evaluate the condition of the lungs for
pneumonia/atelectasis, also echo heart for defects

Esophageal atresia
Tracheoesophageal fistula cont.
• Initial tx consists of: 1)warmer, 2) 30° head elevated,
3) IV access. 4)AB, 5)sump drainage proximal pouch
• Primary surgical correction
– Performed if baby stable, R retroperitoneal approach
– Divide TEF, close tracheal opening, mobilize esophageal ends
– Single layer primary anastomosis, drain, no gastrostomy
• Delayed surgical repair
– If baby unstable, premature, multiple anomalies
– First place gastrostomy until baby mature, stable
– Do standard primary repair

Esophageal atresia
Tracheoesophageal fistula cont.
• Post-operative course
– Parenteral nutrition for one week
– Contrast swallowing study to check for leak
– Continue drainage if leak present (will heal especially if done retropleural)
• Prognosis – 90% survive if stable, >60% if not
• Strictures develop in 10-20% of cases (especially if a leak)
– May occur months to years later
– Usually treatable with multiple dilatations
• “Recurrent” TEF
– Usually due to missed TEF or leak
• Reflux
– May develop clinical symptoms as child
– Tx with anti-reflux procedure (Nissen) but dysmotility may persist
Duodenal malformations
• Incomplete obstruction – web,anular pancreas, midgut volvulus
• Complete obstruction – atresia
– Polyhydramnios usually 3rd trimester
– Bilious vomiting (85%)
– No abdominal distention
– Classic “double bubble” seen
– One third have Down’s syndrome (trisomy 21)
– Tx = NG/OG tube, IVF, doudenoduodenostomy after evaluating for other abnormalities
• Tx anular pancreas = do not divide, duodenojejunostomy
• Tx web = excise through vertical incision, close horizontally
Midgut volvulus
• Midgut in umbilical cord 6-12 weeks
• Normally rotates 270° around SMA when returning into abdominal cavity
• If incomplete, cecum stays in epigastrum, but Ladd’s bands still form between the cecum and lateral abdominal wall crossing duodenum
• SMA is in a narrow pedicle and a volvulus may occur around the mesentery with jejunal obstruction and ischemia (clockwise)
• Must be ruled out in infant with bilious vomiting → UGI series
– Shows displacement of duodenal-jejunal junction to right
– May show corkscrew pattern of duodenum or complete obstruction
• Early surgical intervention mandatory due to risk of entire midgut necrosis
– Bowel untwisted counter-clockwise
– Ladd’s bands lysed
– Appendectomy (cecum usually ends up in LLQ)
– Frankly necrotic bowel resected or second-look operation done

Meconium ileus
• Occurs from meconium impaction in distal ileum
• Etiology usually cystic fibrosis causing a lack of
pancreatic enzymes
• Presents with bilious vomiting late, failure to pass
meconium
• Films show dilated loops of SB, no air/fluid levels
• Classic sign is “ground glass” appearance in terminal
ileum
• Tx non-operatively with dilute Gastrografin enema
• May need to repeat every 12 hours for several days

Necrotizing enterocolitis (NEC)
• Disease found mostly in stressed premature infants
• Common factors include intestinal ischemia, bacterial colonization of the gut, enteric feedings of synthetic formula, hypoalbuninemia
• First sign usually feeding intolerance (vomiting, large residuals)
• Invasion of the mucosa by gas-forming organisms causes “pneumatosis intestinalis” or hepato/portal gas
• Initial treatment = NPO, NG, IVAB
• Indications for surgery 1) free air 2) diffuse peritonitis 3) refractory acidosis, especially with hepato/portal air
• Resection of gangrenous bowel done with stomas, may need second looks
• If infant (<1500 grams) desperately ill → consider local drainage at bedside
• TPN continued for 2 weeks minimum
• 20% develop strictures (need to evaluate before restoring continuity of bowel), up to 80% survival now


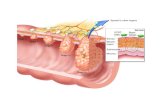
Intussusception
• Usually in infants 8-12 weeks old, male
• Commonly occurs after viral illness 2 hypertrophy of Peyer’s
patches in terminal ileum
• May occur due to tumors, polyps, Meckel’s diverticulum
• Symptoms include cramping abdominal pain, vomiting, lethargy
• May pass bloody mucous “currant jelly”
• Classic finding is elongated mass in RUQ
• Tx is air enema using pressure less than 120 mmHG (60-90%
successful)
• If unsuccessful→ surgery and manual reduction, appy
• Occasionally need to resect gangrenous bowel, or cause of leading
point

Meckel’s diverticulum
• Remnant of ophalomesenteric (vitelline) duct
• On antimesenteric border 2 feet from ileocecal valve
• May mimic appendicitis; bleed if gastric mucosa present;
cause intussusception
• Can use technetium scan to diagnosis if gastric mucosa
present
• Tx is wedge resection if base is narrow, sleeve resection
for larger base

Imperforate anus
• Results from failure of decent of the urorectal septum
• “High” ends above levator ani muscle, “low” descends
partially through it
• Low lesions have fistula to perineum; midline of
scrotum/penis in males, posterior forchette in females
• Low lesions (40% in males, 70% in females) approached
through perineal incision, usually pts continent
• High lesions require colostomy, then pull-through
procedure at 2 months
• Tx : posterior lateral anorectoplasty

Hirshsprung’s disease
• Absence of ganglion cells in myenteric plexus of intestine, usually rectum or rectosigmoid
• Cause functional obstruction, variable degree
• Often failure to pass meconium in first 24 hours
• Barium enema shows transition zone (lg to sm), unreliable in infants
• Suction biopsy usually adequate to demonstrate lack of ganglion cells (may need full thickness)
• Also shows increase cholinesterase staining, hypertrophied nerve bundles
• Three pull-through procedures used with similar results
1) Swenson – rectum resected, colo-anal anatomosis
2) Duhamel – colon anastomosed to posterior rectum above anus
3) Soave – rectal mucosa resected and colon brought through sleeve
Omphalocele
• Abdominal wall defect at umbilicus
• Herniated bowel covered with peritoneum
• Frequently (60-70%) associated with other anomalies
• Tx: primary closure of abdominal wall, mechanical
stretching, may need silo
• Silo used to steadily apply pressure over 7 days to
reduce hernia contents
• 20-30% mortality due to associated cardiac and
chromosomal abnormalities


Gastroschisis
• Full thickness abdominal wall defect just right of
umbilicus
• Results form intrauterine rupture of umbilical cord
• Herniated bowel not covered with peritoneum
• Rarely associated with other anomalies
• Intestine usually thickened, edematous, discolored,
covered with exudate
• Transport in bowel bag to keep moist & normothermic
• Tx: emergent primary closure of abdominal wall,
mechanical stretching, may need silo
• Survival rate 90%


Wilm’s tumor (nephroblastoma)
• Most common renal malignancy of childhood
• Peak incidence between 1-5 years
• Typical X-ray finding: linear calcifications
• Tx: resection, chemo, radiation
• Clamp renal vein prior to mobilization to prevent spread
• May do resection of adjacent organ if needed
• Actinomycin D and vincristine useful
• 80-97% cure rate, depending on stage
• Long term follow-up required due to ↑ second
malignancies

Neuroblastoma
• Arises from sympathetic nervous tissue (neural crest cells)
• 3rd most common malignancy in children (#1 brain, #2 leukemia)
• Most common tumor in children < 1 yr
• Originates in adrenals, posterior mediastinum, pelvis, neck, etc.
• X-ray finding: fine-stippled calcification
• Best localizing test: MIBG scan
• Usually elevated catacholamines, VMA and HVMA in urine
• Tx: Resection, chemo, radiation
• Best chance of cure is complete surgical resection
• Better prognosis the younger the patient (85% if < 1 yr)
• Spontaneous regression can occur

Biliary tract abnormalities
• Choledochal cysts
– 5 types, type 1 most common, fusiform common duct dilation
– Classic triad includes pain, RUQ mass, jaundice
– Untreated leads to cirrhosis, portal htn, cholangitis, cancer
– Tx: resection of cyst, choledocho – jejunostomy or duodenostomy
• Biliary atresia
– May involve common duct, hepatic ducts, GB, cystic duct, etc.
– Causes jaundice, growth retardation, portal htn
– Kasai procedure (hepatoportoenterostomy) best tx

Kasai procedure