Riesgo Cardiaco en Cirugia No Cardiaca

of 7
-
Upload
andres-mendoza -
Category
Documents
-
view
221 -
download
0
Transcript of Riesgo Cardiaco en Cirugia No Cardiaca
-
8/3/2019 Riesgo Cardiaco en Cirugia No Cardiaca
1/7
CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 SUPPLEMENT 4 NOVEMBER 2009 S9
ABSTRACT
The American College of Cardiology and American HeartAssociation updated their joint guidelines on perioperativecardiovascular evaluation and care for noncardiac surgery in2007. The guidelines recommend preoperative cardiac testingonly when the results may influence patient management.
They specify four high-risk conditions for which evaluationand preoperative treatment are needed: unstable coronarysyndromes, decompensated heart failure, significant cardiacarrhythmias, and severe valvular disease. Patient-specificfactors and the risk of the surgery itself are considerations inthe need for an evaluation and the treatment strategy beforenoncardiac surgery. In most instances, coronary revascular-ization before noncardiac surgery has not been shown toreduce morbidity and mortality, except in patients with leftmain disease. The timing of surgery following percutaneouscoronary intervention (PCI) depends on whether a stent wasused, the type of stent, and the antiplatelet regimen.
KEY POINTSIn addition to patient-specific factors, preoperative cardiacassessment should account for the risk of cardiac morbidityrelated to the procedure itself. Vascular surgery confersthe highest risk, with reported rates of cardiac morbidityoften greater than 5%.
Continuation of chronic beta-blocker therapy is prudentduring the perioperative period.
Coronary revascularization prior to noncardiac surgeryis generally indicated only in unstable patients and inpatients with left main disease.
Nonurgent noncardiac surgery should be delayed for atleast 30 days after PCI using a bare-metal stent and forat least 365 days after PCI using a drug-eluting stent.
Discontinuing antiplatelet therapy in patients withcoronary stents may induce a hypercoagulable statewithin approximately 7 to 10 days.
In patients undergoing noncardiac surgery, pre-operative intervention or a cardiac condition israrely needed simply to reduce the risk o the surgeryunless such intervention is indicated separate rom
the preoperative context.This is the overriding message o the 2007 guidelines
on perioperative cardiovascular evaluation and care ornoncardiac surgery issued by the American College oCardiology (ACC) and American Heart Association(AHA),1 or which I was privileged to chair the writingcommittee. This article outlines current best practicesin cardiac risk stratifcation or noncardiac surgery,highlighting key recommendations rom the ACC/AHA 2007 perioperative guidelines.
PURPOSE OF THE PREOPERATIVECARDIAC EVALUATION
Provide clinical judgment, not clearance for surgeryA proper cardiac evaluation prior to noncardiac surgery
involves a comprehensive patient assessment that drawson clinical fndings, the clinical experience o the con-sulting physician (typically a cardiologist or internist),and an assessment o the literature. The purpose is notto give medical clearance or surgery but rather to pro-vide inormed clinical judgment to the anesthesiologistand the surgical team in terms o the ollowing1:
The patients current medical statusRecommendations regarding the management andrisk o cardiac problems during the perioperativeperiodThe patients clinical risk profle, to assist withtreatment decisions that may aect short- or long-
term cardiac outcomes.
Order tests only when results may change managementThe consulting physicians clinical judgment is criticalin determining the need to order any specifc tests. Ingeneral, a test to urther defne cardiac risk is valid onlywhen its results could change the planned managementand lead to a specifc intervention. Potential interven-tions that may result rom knowledge gained throughtesting include:
Delaying the operation because o unstable symptoms
LEE A. FLEISHER, MDRobert D. Dripps Professor and Chair, Department of Anesthesiology and Critical Care,
and Professor of Medicine, University of Pennsylvania School of Medicine,
Philadelphia, PA
Cardiac risk stratification for noncardiac surgery:Update from the American College of Cardiology/American Heart Association
2007 guidelines
See end of article for author disclosures. doi:10.3949/ccjm.76.s4.02
-
8/3/2019 Riesgo Cardiaco en Cirugia No Cardiaca
2/7
S10 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 SUPPLEMENT 4 NOVEMBER 2009
PREOPERATIVE CARDIAC RISK STRATIFICATION
Coronary revascularizationAttempting medical optimization beore surgeryInvolving additional specialists or providers in thepatients perioperative care
Modifcation o intraoperative monitoringModifcation o postoperative monitoringModifcation o the surgical location, particularlywhen the procedure is scheduled or an ambulatorysurgical center.
The cardiac evaluation should result in an estimationo cardiac risk. I the consulting physicians estimationo risk is not clearly above or below the threshold ora potential intervention, then urther testing may beindicated to urther defne the need or interventions(ie, reaching the threshold or action).
WHAT TO WORRY ABOUT FIRST:
HIGH-RISK CONDITIONS THAT REQUIREEVALUATION AND TREATMENT
In a recommendation categorized as a Class I, LevelB endorsement,* the ACC/AHA 2007 perioperativeguidelines speciy our active cardiac conditions orwhich an evaluation and treatment are required beorenoncardiac surgery1:
Unstable coronary syndromes , including unstableor severe angina or recent myocardial inarction (MI).These syndromes should be the frst and most importantconsideration. Unstable angina is a hypercoagulablestate, as is recent MI. The hypercoagulability o theseconditions is compounded by the hypercoagulability
induced by the perioperative setting itsel. As a result,the rate o perioperative MI or death in the setting ounstable angina is as high as 28%.2 In the case o unstablecoronary syndromes, delaying surgery is appropriatei the risks o the surgery are deemed greater than itspotential benefts.
Decompensated heart ailure , defned as NewYork Heart Association unctional class IV disease orworsening or new-onset heart ailure.
Signifcant arrhythmias , defned as high-grade orMobitz II atrioventricular block, third-degree atrioven-tricular heart block, symptomatic ventricular arrhyth-mias, supraventricular arrhythmias with uncontrolledventricular rate, symptomatic bradycardia, and newlyrecognized ventricular tachycardia.
Severe valvular disease , defned as severe aorticstenosis and symptomatic mitral stenosis.
CARDIAC RISK STRATIFICATION:INITIAL PATIENT ASSESSMENT
Clinical risk factors and functional capacity
The Revised Cardiac Risk Index o Lee et al3
remainsthe general paradigm or stratiying cardiac risk beorenoncardiac surgery. This validated index consists o sixindependent predictors o cardiac complications:
High-risk surgery (intraperitoneal, intrathoracic,or suprainguinal vascular procedures)Ischemic heart diseaseHistory o congestive heart ailureHistory o cerebrovascular diseaseInsulin therapy or diabetes mellitusPreoperative creatinine level greater than 2.0 mg/dL.
The more predictors a patient has, the greater the risko perioperative complications. Thus, the Revised Car-diac Risk Index is a good tool or establishing a baselinerisk level or use in determining whether a preoperative orperioperative intervention is likely to make a dierencein the patients surgical outcome. For the purpose o thealgorithmic approach to testing, the surgical procedure isnot considered a risk actor. Additionally, type 2 diabetesmellitus is also considered a risk actor.
Another important determinant o risk is the patientsunctional capacity. A study o 600 patients undergo-ing major noncardiac procedures ound that poor sel-reported exercise capacity, defned as an inability to walkour blocks or climb two ights o stairs, was associatedwith signifcantly more perioperative complicationsthan was good exercise capacity.4 Simple instruments
such as the Duke Activity Status Index5 can be used toestimate the patients unctional capacity.
Procedure-specific riskIn addition to patient-specifc actors, surgery-specifccardiac risk can be important, especially in patients withmore than two clinical risk actors. The ACC/AHA2007 perioperative guidelines identiy three categorieso surgery-specifc risk1:
Vascular surgery (the highest-risk category andalso the most extensively studied), which has been asso-ciated with cardiac morbidity rates o greater than 5% inmany reports. Examples include aortic and other major
vascular surgery, as well as peripheral vascular surgery.Intermediate-risk surgery , or which reportedcardiac morbidity rates range rom 1% to 5%. Examplesinclude intraperitoneal and intrathoracic procedures,carotid endarterectomy, head and neck surgery, ortho-pedic surgery, and prostate surgery.
Low-risk surgery , or which reported cardiacmorbidity rates are generally below 1%. Examplesinclude endoscopic and superfcial procedures, cataractsurgery, breast surgery, and ambulatory surgery. Patientsundergoing these procedures do not generally require
* The ACC/AHA 2007 perioperative guidelines make recommendations byclassiying the magnitude o beneft versus risk (I = the intervention shouldbe undertaken; IIa = the intervention is reasonable to undertake; IIb = theintervention may be considered; III = the intervention should not be un-dertaken) and assigning a level o supporting evidence (A = highest levelo evidence; B = limited evidence; C = very limited evidence).
-
8/3/2019 Riesgo Cardiaco en Cirugia No Cardiaca
3/7
CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 SUPPLEMENT 4 NOVEMBER 2009 S11
FLEISHER
urther preoperative cardiac testing.1
O course, some variability exists within each risklevel as a result o institutional dierences in surgicalvolume and expertise as well as in preoperative evalu-
ation and other processes o care. Endovascular surgeryis considered intermediate risk rom a perioperativeperspective but is in the same risk category as vascularsurgery rom a 1-year perspective.
Risk stratification promotes good perioperative outcomesAppropriate risk stratifcation can make the day osurgery among the saest times or patients undergoingoutpatient procedures. A retrospective analysis o Medi-care claims rom the late 1990s or more than 500,000elderly patients undergoing low-risk procedures in vari-ous outpatient settings ound that the mortality rate wasonly 1 in 50,000 on the day o surgery but increasedsubstantially over the ollowing 7 days and 30 days.6
This was likely a reection o the diligence applied tomanaging patient-specifc risk actors beore proceedingto outpatient surgery.
HEART RATE CONTROL
Chronic beta-blockade can obviate needfor cardiac testingThe DECREASE (Dutch Echocardiographic CardiacRisk Evaluation Applying Strees Echo) II trial assessedthe value o cardiac testing beore major vascular surgeryin intermediate-risk patients (ie, with one or two car-diac risk actors) receiving chronic beta-blocker therapybegun 7 to 30 days prior to surgery.7 Among the studys770 intermediate-risk patients, the primary outcomecardiac death or MI at 30 dayswas no dierentbetween those randomized to receive stress testing orno stress testing. The investigators concluded that car-diac testing can saely be omitted in intermediate-riskpatients i beta-blockers are used with the aim o tightheart rate control.
Continue ongoing beta-blocker therapy,start in select high-risk patientsThe ACC/AHA 2007 perioperative guidelines recom-mend continuing beta-blocker therapy in patients whoare already receiving these agents (Class I, Level C). For
patients not already taking beta-blockers, their initia-tion is recommended in those undergoing vascular sur-gery who have ischemia on preoperative testing (ClassI, Level B). The guidelines designate beta-blockers asprobably recommended (Class IIa, Level B) or severalother patient subgroups with high cardiac risk, mainlyin the setting o vascular surgery.1
Notably, the guidelines were written beore publica-tion o the Perioperative Ischemic Evaluation (POISE),8which questioned the risk/beneft profle o periop-erative beta-blockade in patients with or at high risk o
atherosclerotic disease (see the PoldermansDevereauxdebate on page S84 o this supplement), and thereoremay require revision (an update is scheduled or releasein November 2009).
LIMITED ROLE FOR CORONARY REVASCULARIZATION
Until recently, no randomized trials had assessed thebeneft o prophylactic coronary revascularization toreduce the perioperative risk o noncardiac surgery.The frst large such trial was the Coronary ArteryRevascularization Prophylaxis (CARP) study, whichrandomized 510 patients scheduled or major electivevascular surgery to undergo or not undergo coronaryartery revascularization beore the procedure.9 Thestudy ound that revascularization ailed to aect anyoutcome measure, including mortality or the develop-ment o MI, out to 6 years o ollow-up. Notably, theCARP population consisted mostly o patients withsingle-, double-, or mild triple-vessel coronary arterydisease, so the study was limited in that it did notinclude patients with strong indications or coronaryartery bypass grat surgery (CABG).7
A reanalysis o the CARP results by the type orevascularization procedureCABG or percutaneouscoronary intervention (PCI)revealed that patientsundergoing CABG had lower rates o death, MI, andadditional revascularization procedures compared withthose undergoing PCI, despite the presumably moreextensive disease o the CABG recipients.10
Benefit apparently limited to left main diseaseFurther analysis o patients in the CARP trial whounderwent coronary angiography ound that one sub-grouppatients with let main diseasedid experiencean improvement in survival with preoperative coronaryrevascularization.11
In a subsequent randomized pilot study, Poldermanset al ound no advantage to preoperative coronary revas-cularization among patients with extensive ischemiawho underwent major vascular surgery.12 While thisstudy was not adequately sized to defnitively addressthe value o preoperative revascularization in thesehigh-risk patients, its results are consistent with those
o the CARP trial.In a retrospective cohort study o patients whounderwent noncardiac surgery, Posner and colleaguesound that rates o adverse cardiac outcomes amongpatients who had recent PCI ( 90 days beore surgery)were similar to rates among matched controls withnonrevascularized coronary disease.13 Patients who hadhad remote PCI (> 90 days beore surgery) had a lowerrisk o poor outcomes than did matched controls withnonrevascularized disease, but had a higher risk than didcontrols without coronary disease.13
-
8/3/2019 Riesgo Cardiaco en Cirugia No Cardiaca
4/7
S12 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 SUPPLEMENT 4 NOVEMBER 2009
PREOPERATIVE CARDIAC RISK STRATIFICATION
PATIENTS WITH CORONARY STENTS:STENT TYPE AND TIME SINCE PLACEMENT ARE KEY
The lack o beneft rom prophylactic PCI prior tononcardiac surgery also applies to PCI procedures thatinvolve coronary stent placement. For instance, apropensity-score analysis ound no beneft rom prophy-lactic PCI (using stents in the vast majority o cases) inpatients with coronary artery disease in terms o adversecoronary events or death ollowing aortic surgery.14
In patients who have undergone prior PCI, non-
cardiac surgery poses special challenges, especially inrelation to stents. Restenosis is a particular concernwith the use o bare-metal stents, and development ostent thrombosis is a particular risk with the use o drug-eluting stents.15 The use o drug-eluting stents requiresintensive antiplatelet therapy or at least 1 year ollow-ing stent implantation to prevent stent thrombosis.16
Time interval to surgery after bare-metal stent placementThe eect o prior PCI with bare-metal stents on out-comes ollowing noncardiac surgery was examined in arecent large retrospective study by Nuttall et al.17 Theincidence o major cardiac events was ound to be lowest
when noncardiac surgery was perormed more than 90days ater PCI with bare-metal stents. Using patientswho had a greater than 90-day interval beore surgeryas the reerence group, propensity analysis showed thatperorming surgery within 30 days o PCI was associatedwith an odds ratio o 3.6 or major cardiac events. Theodds ratio was reduced to 1.6 when surgery was per-ormed 31 to 90 days ater PCI. These fndings suggestthat 30 days may be an ideal minimum time interval,rom a risk/beneft standpoint, between PCI with bare-metal stents and noncardiac surgery.
Time interval to surgery after drug-eluting stent placementA recent retrospective study by Rabbitts et al examinedpatients who had noncardiac surgery ater prior PCIwith drug-eluting stents, ocusing on the relationshipbetween the timing o the procedures and major cardiacevents during hospitalization or the surgery.18 Althoughthe requency o major cardiac events was not statisti-cally signifcantly associated with the time betweenstent placement and surgery, the requency was low-est3.3%when surgery ollowed drug-eluting stent
placement by more than 365 days (versus rates o 5.7%to 6.4% or various intervals o less than 365 days).
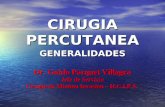
ACC/AHA recommendationsRecommendations on the timing o noncardiac surgeryin patients with prior PCI rom the ACC/AHA 2007perioperative guidelines (Figure 1) are consistent withthe fndings o the above two retrospective studies,17,18although the guideline writers concede that these recom-mendations are based on expert opinion and lack high-quality supportive evidence.1 Indeed, stent thrombosishas been known to occur during operations perormed18 months or more ater drug-eluting stent placement,so vigilance is always in order.
Timing of antiplatelet interruptionResults rom a prospectively maintained Dutch regis-try19 are consistent with the fndings reviewed above:patients who underwent noncardiac surgery less than30 days ater bare-metal stent implantation or less than6 months ater drug-eluting stent implantation (earlysurgery group) had a signifcantly elevated rate o majorcardiac events compared with patients in whom theinterval between stenting and noncardiac surgery waslonger (late surgery group). Notably, this report also
FIGURE 1. Recommendedtiming of noncardiac surgeryfollowing percutaneouscoronary intervention (PCI)depends on whether a stentwas placed and the type ofstent used.1
Reprinted fromJournal of theAmerican College of Cardiology(Fleisher LA, et al. ACC/AHA 2007
Guidelines on PerioperativeCardiovascular Evaluation and
Care for Noncardiac Surgery. J AmColl Cardiol 2007; 50:17071732),
Copyright 2007, withpermission from Elsevier.www.sciencedirect.com/
science/journal/07351097
Delay for elective ornonurgent surgery
Proceed to theoperating room
with aspirin
Delay for elective ornonurgent surgery
Time since PCI< 14days
> 14days
< 365days
Proceed to theoperating room
with aspirin
< 3045days
> 3045days
> 365days
Balloonangioplasty
Bare-metalstent
Drug-elutingstent
Previous PCI
Proposed approach to management of patients with prior PCI
-
8/3/2019 Riesgo Cardiaco en Cirugia No Cardiaca
5/7
CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 SUPPLEMENT 4 NOVEMBER 2009 S13
FLEISHER
ound that the rate o major cardiac events within theearly surgery group was signifcantly higher in patientswhose antiplatelet therapy was discontinued during thepreoperative period than in those whose antiplatelet
therapy was not stopped.19A hypercoagulable state develops within 7 to 10 days
ater interruption o antiplatelet therapy, at which timethe patient is vulnerable to thrombosis. In general, sur-gery should not proceed during this time without anti-platelet coverage.
From my perspective, giving ketorolac or aspirin themorning o surgery may be benefcial or patients whoseantiplatelet therapy has been stopped 7 to 10 days pre-viously, although no data rom randomized trials existto support this practice. Theoretically, it is reasonableto stop antiplatelet therapy 4 to 5 days beore surgeryin patients with an increased risk o bleeding without
exposing them to the hypercoagulability that would setin i therapy were stopped earlier.
A FRAMEWORK FOR CARDIAC EVALUATION
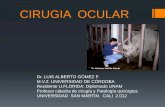
The ACC/AHA 2007 perioperative guidelines includean evidence-based algorithm or determining whichpatients are candidates or cardiac testing as part o pre-operative cardiac assessment.1 As presented inFigure 2,this stepwise approach takes into account the urgencyo the surgery, the presence or absence o active cardiacconditions, the type o surgery and its risk level, and thepatients unctional capacity and cardiac risk actors.1,20
The ollowing are among the algorithms key
recommendations:Patients requiring urgent noncardiac surgery
should proceed to the operating room with periopera-tive surveillance (Class I, Level C).
Patients with active cardiac conditions who areundergoing nonurgent surgery should be evaluated andtreated per ACC/AHA guidelines beore proceeding tothe operating room is considered (Class I, Level B).
Patients scheduled or a low-risk procedure canproceed to surgery without testing (Class I, Level B).
Patients scheduled or intermediate-risk surgery orvascular surgery are to be assessed by unctional capacityand clinical risk actors. Proceeding with planned surgery
is appropriate in patients with good unctional capacity(Class IIa, Level B). In patients with poor or unknownunctional capacity undergoing vascular surgery whohave three or more clinical risk actors, testing shouldbe considered i the results would change management(Class IIa, Level B).
Patients with one or more clinical risk actorsundergoing intermediate-risk surgery and those withewer than three clinical risk actors undergoing vascularsurgery may proceed to planned surgery with control oheart rate to diminish the stress response perioperatively
(Class IIa, Level B), or they may undergo noninvasivetesting, but only i the results would change manage-ment (Class IIb, Level B).
Patients undergoing intermediate-risk or vascular
surgery who have poor or unknown unctional capacitybut no clinical risk actors may proceed to surgery with-out testing (Class I, Level B).
DISCUSSION
Question rom the audience: The POISE study showeda 30% reduction in nonatal MI with routine periopera-tive beta-blockade but an overall increase in mortality.Since most MIs occur immediately postoperatively andsepsis occurs a bit later, would you consider continuingbeta-blocker therapy or a ew days to prevent an MI butthen stopping it beore sepsis develops?
Dr. Fleisher: Ive had discussions with sepsis expertsabout the link between beta-blocker therapy and sepsisand death in POISE, and the belie is that beta-blockersdo not cause sepsis. I think that a septic patient on acutehigh-dose beta-blocker therapy cant respond appropri-ately because o an inability to increase cardiac output.I believe we should titrate beta-blockers more closely.Inormation on preoperative dose titration in POISE isnot available because o the way the trial was designed.Sepsis developed in only 53 o the 8,351 patients ran-domized in the study.
I would not start an acute beta-blocker protocol justto get a patient through surgery. I would start a periop-erative hemodynamic protocol with the goal o main-taining the patients heart rate at lower than 80 beatsper minute. Because I dont believe that beta-blockerscause sepsis, i I initiated a beta-blocker preoperatively,I would not stop it at 2 days.
Question rom the audience: Is there a time period dur-ing which a patient with a bare-metal stent could haveback surgery or knee replacement surgery while not onaspirin?
Dr. Fleisher: The guidelines say that i a patient is onaspirin, it should be continued indefnitely. The issue isone o risk versus beneft. For back surgery, i bleedingis a concern, stopping aspirin or 6 or 7 days ater the
30-day period ollowing PCI is not unreasonable, but Iwould not stop it during the frst 30 days ollowing PCI.
Question rom the audience: I dont assess or vascularsurgery but rather or the Whipple procedure [radicalpancreatoduodenectomy], and I use the Revised CardiacRisk Index to assess the number o risk actors. I believethe Whipple procedure is a high-risk operation, but itappears to be considered an intermediate-risk operationby the ACC/AHA guidelines. Is my approach to riskassessment appropriate?
-
8/3/2019 Riesgo Cardiaco en Cirugia No Cardiaca
6/7
S14 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 SUPPLEMENT 4 NOVEMBER 2009
PREOPERATIVE CARDIAC RISK STRATIFICATION
Dr. Fleisher: I the rates o morbidity and mortalitywith the Whipple procedure are low at your institution,you might risk worsening your outcomes by applyingsomeone elses paradigms to your institution. Theresa big dierence in risk between a surgeon who does aWhipple in 5 hours with 0.5 to 1.0 U o blood loss and asurgeon who does a 12-hour Whipple with 20 U o bloodloss, necessitating a stay in the intensive care unit ormultiple days. You need to consider the risk associated
with your institution and specifcally with the surgeon.
Question rom the audience: Peripheral vascular diseaseis considered a coronary heart disease risk equivalent, sowhy is it not one o the criteria in the Revised CardiacRisk Index?
Dr. Fleisher: The criteria are not hard and ast. The indexwas devised at one institution, Brigham and WomensHospital, in about 4,000 patients, and it has been used
Consider testing if it willchange management
* Noninvasive testing may be considered before surgery in specific patients with risk factors if it will change management. Clinical risk factors include ischemic heart disease, compensated or prior heart failure, diabetes mell itus, renal insufficiency, and cerebrovascular disease. Consider perioperative beta-blockade for populations in which this has been shown to reduce cardiac morbidity/mortality.
LOE = level of evidence; MET = metabolic equivalent
Proceed with planned surgery with heart rate control (Class IIa, LOE B) orconsider noninvasive testing (Class IIb, LOE B) if it will change management
Proceed withplanned surgery
Vascular surgery
Vascular surgery
Intermediate-risk surgery Intermediate-
risk surgeryClass IIa,LOE B
No clinicalrisk factors
Class I,LOE B
12 clinicalrisk factors3 or more clinical
risk factors
Step 1
Step 2
Step 3
Step 4
Step 5 No or unknown
Functional capacityl to 4 METswithout symptoms
Yes(Class IIa, LOE B)
Proceed withplanned surgery*
No
Low-risk surgeryYes
(Class I, LOE B)Proceed with
planned surgery
No
Active cardiacconditions
Consideroperating room
Evaluate and treat perACC/AHA guidelines
Yes(Class I, LOE B)
No
Need for emergency
noncardiac surgery?
Yes
(Class I, LOE C)
Operating roomPerioperative surveillance
and postoperative riskstratification and risk factormanagement
Recommended approach to cardiac evaluation and care prior to noncardiac surgery
FIGURE 2. Algorithm for preoperative cardiac evaluation and care.1,20Reprinted fromJournal of the American College of Cardiology (Fleisher LA, et al. Correction. J Am Coll Cardiol 2008;
52:794797), Copyright 2008, with permission from Elsevier. www.sciencedirect.com/science/journal/07351097
-
8/3/2019 Riesgo Cardiaco en Cirugia No Cardiaca
7/7
CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 76 SUPPLEMENT 4 NOVEMBER 2009 S15
FLEISHER
dierently. It assigns 1 point to ischemic heart disease.It would not be inappropriate to assume that any athero-sclerotic class o disease is equivalent to ischemic heartdisease or risk purposes.
Question rom the audience: You mentioned a 4-daywindow or withholding clopidogrel. Do you actor intothe decision the duration o therapy? Some cardiolo-gists go beyond the 1-year recommendation to continueclopidogrel ater stenting because they believe there isstill beneft.
Dr. Fleisher: The key is to coner with the cardiologistwho implanted the stent, who knows the stenosis orwhich the stent was implanted. A problem weve hador years is that a practitioner will stop the antiplateletagent without having spoken to the surgeon or the anes-thesiologist. As an anesthesiologist, I need to know that
someone has done a risk/beneft assessment o whetherto continue antiplatelet agents in a given patient.
Question rom the audience: The Revised Cardiac RiskIndex o Lee et al3 includes the type o surgery in its totalpoint system while the ACC/AHA guidelines do not.Can you explain the discrepancy?
Dr. Fleisher: We on the writing committee or theACC/AHA 2007 perioperative guidelines made a deci-sion to pull out the type o surgery and use the other fverisk actors o Lee et al. It was a consensus o the com-mittee because we believed that the complexity o thesurgery itsel is a separate consideration or risk. Thatswhy we included the medical risk actors and consideredthe surgical actors separately.
DISCLOSURESDr. Fleisher has indicated that he has no financial relationships with commercialinterests that have a direct bearing on the subject matter of this article.
This article was developed from an audio transcript of Dr. Fleishers lecture atthe 4th Annual Perioperative Medicine Summit. The transcript was edited bythe Cleveland Clinic Journal of Medicine staff for clarity and conciseness, andwas then reviewed, revised, and approved by Dr. Fleisher.
REFERENCES1. Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007
guidelines on perioperative cardiovascular evaluation and care ornoncardiac surgery: a report o the American College o Cardiol-
ogy/American Heart Association Task Force on Practice Guidelines[published correction appears in J Am Coll Cardiol 2008; 52:794797]. J Am Coll Cardiol 2007; 50:17071732.
2. Shah KB, Kleinman BS, Rao TLK, Jacobs HK, Mestan K,Schaasma M. Angina and other risk actors in patients with cardiacdiseases undergoing noncardiac operations. Anesth Analg 1990;70:240247.
3. Lee TH, Marcantonio ER, Mangione CM, et al. Derivation andprospective validation o a simple index or prediction o cardiac risk
o major noncardiac surgery. Circulation 1999; 100:10431049.4. Reilly DF, McNeely MJ, Doerner D, et al. Sel-reported exercise
tolerance and the risk o serious perioperative complications. ArchIntern Med 1999; 159:21852192.
5. Nelson CL, Herndon JE, Mark DB, et al. Relation o clinical and
angiographic actors to unctional capacity as measured by the DukeActivity Status Index. Am J Cardiol 1991; 68:973975.6. Fleisher LA, Pasternak LR, Herbert R, Anderson GF. Inpatient
hospital admission and death ater outpatient surgery in elderlypatients: importance o patient and system characteristics and loca-tion o care. Arch Surg 2004; 139:6772.
7. Poldermans D, Bax JJ, Schouten O, et al. Should major vascu-lar surgery be delayed because o preoperative cardiac testing inintermediate-risk patients receiving beta-blocker therapy with tightheart rate control? J Am Coll Cardiol 2006; 48:964969.
8. POISE Study Group, Devereaux PJ, Yang H, Yusu S, et al. Eectso extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomized controlled trial. Lancet2008; 371:18391847.
9. McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascu-larization beore elective major vascular surgery. N Engl J Med 2004;351:27952804.
10. Ward HB, Kelly RF, Thottapurathu L, et al. Coronary arterybypass grating is superior to percutaneous coronary interventionin prevention o perioperative myocardial inarctions during subse-quent vascular surgery. Ann Thorac Surg 2006; 82:795801.
11. Garcia S, Moritz TE, Ward HB, et al. Useulness o revasculariza-tion o patients with multivessel coronary artery disease beore elec-tive vascular surgery or abdominal aortic and peripheral occlusivedisease. Am J Cardiol 2008; 102:809813.
12. Poldermans D, Schouten O, Vidakovic R, et al. A clinical random-ized trial to evaluate the saety o a noninvasive approach in high-risk patients undergoing major vascular surgery: the DECREASE-VPilot Study. J Am Coll Cardiol 2007; 49:17631769.
13. Posner KL, Van Norman GA, Chan V. Adverse cardiac outcomesater noncardiac surgery in patients with prior percutaneous translu-minal coronary angioplasty. Anesth Analg 1999; 89:553560.
14. Godet G, Riou B, Bertrand M, et al. Does preoperative coronaryangioplasty improve perioperative cardiac outcome? Anesthesiology
2005; 102:739746.15. Shuchman M. Debating the risks o drug-eluting stents. N Engl JMed 2007; 356:325328.
16. King SB III, Smith SC Jr, Hirsheld JW Jr, et al. ACC/AHA/SCAI. 2007 ocused update o the ACC/AHA/SCAI 2005 guide-line update or percutaneous coronary intervention: a report o theAmerican College o Cardiology/American Heart Association TaskForce on Practice guidelines. J Am Coll Cardiol 2008; 51:172209.
17. Nuttall GA, Brown MJ, Stombaugh JW, et al. Time and cardiacrisk o surgery ater bare-metal stent percutaneous coronary inter-vention. Anesthesiology 2008; 109:588595.
18. Rabbitts JA, Nuttall GA, Brown MJ, et al. Cardiac risk o non-cardiac surgery ater percutaneous coronary intervention with drug-eluting stents. Anesthesiology 2008; 109:596604.
19. Schouten O, van Domburg RT, Bax JJ, et al. Noncardiac surgeryater coronary stenting: early surgery and interruption o antiplate-let therapy are associated with an increase in major adverse cardiac
events. J Am Coll Cardiol 2007; 49:122124.20. Correction to Fleisher et al, J Am Coll Cardiol 2007; 50:17071732.J Am Coll Cardiol 2008; 52:794797.
Correspondence: Lee A. Fleisher, MD, Department of Anes-thesiology and Critical Care, University of Pennsylvania Health
System, 3400 Spruce Street, 6 Dulles Building, Philadelphia, PA
19104; [email protected]