
La terapia di resincronizzazione cardiaca nei pazienti con...
72
La terapia di resincronizzazione cardiaca nei pazienti con fibrillazione atriale Dr. Paolo Pieragnoli University of Florence
Transcript of La terapia di resincronizzazione cardiaca nei pazienti con...

La terapia di resincronizzazione cardiaca nei pazienti con fibrillazione
atriale
Dr. Paolo Pieragnoli University of Florence

“… These two motions, one of the auricles, the other of the ventricles, are consecutive, with a rhythm between them…”
William Harvey, 1628

Haemodynamic and functional effects of AF
AF
Ventricular rate
Loss of atrial systole Irregular rhythm
Loss of physiological control of heart rate

Potential Mechanisms in Atrial Fibrillation
Remodeling Increase Wall Stress Fibrosis
Age Genetics
Oxydative stress
Inflammation
Neurohormonal activation
Endothelian dysfunction

Potential Mechanisms in Heart Failure
Remodeling Increase Wall Stress Fibrosis
Age Genetics
Oxydative stress
Inflammation
Neurohormonal activation
Endothelian dysfunction

Altered atrial refractory properties
Volume and Pressure load
R-R variability (irregular ventricular response)
Cellular and extracellular remodelling
6
Interplay of AF and HF: The Vicious Cycle
Maisel WH et al. Am J Cardiol 2003;91(suppl):2D-8D.
Common risk factors (e.g. hypertension,
diabetes)
Similar findings (e.g. left atrial
enlargement, reduced LVF shortening)
Atrial Fibrillation
Heart Failure
Loss of atrioventricular node synchrony
Rapid ventricular response
Atrial chamber enlargement and hypertrophy
Interstitial fibrosis

Atrial Fibrillation and Heart Failure Heart Failure in patients with AF predicts Mortality
New Atrial Fibrillation after a prior dignosis of Heart Failure predicts Mortality
Larned JM et al. Congest Heart Fail. 2009;15:24–30

Irina Savelieva and A. John Camm. Europace 2004;5:S5-S19
Prevalence of AF in clinical studies of CHF

Haemodynamic and functional effects of AF
AF on CRT-D
Ventricular rate
Loss of atrial systole Irregular rhythm
Loss of physiological control of heart rate
Inappropriate Shocks Less Therapy

Atrial Fibrillation in ICD Patients Borleffs CJW et al. J Am Coll Cardiol 2010;55:879–85
Days
All-cause mortality
Appropriate Device Therapy
Appropriate Device Shock
Inappropriate Device Shock
Patients without a history of AF (black line), paroxysmal AF (green line), persistent AF (orange line), or permanent AF (red line).

In ICD patients with left ventricular dysfunction, persistent AF is associated with appropriate ICD shocks and deterioration of CHF.
New-onset AF is related to deterioration of CHF
Rienstra M et al. Am Heart J 2007;153:120-6
How many CRT patients develop AF?

New-onset AF in CRT patients Definitions: Patients were classified as having new-onset AF if (1) they had no history of AF at entry into the study and (2) developed AF documented on an electrocardiogram during follow-up or during an adverse event or hospitalization.
Study AF CARE-HF 16% (post-hoc analysis) COMPANION 16% (confidential) MASCOT 8%

New-onset AF/AT in CRT patients Diagnosis from the Device
Study AF
Santini M. et al. 2011 20%
Mona Lisa Study 2010 27%
Leclercq C et al. 2010 21%
Caldwell JC et al. 2009 27%
Borleffs CJW et al. 2009 25%
Puglisi A et al. 2008 42%

Kaplan-Meier estimate of time to first onset of AF. Time until first onset of AF was not different in the CRT group and medical
therapy group.
Hoppe UC et al. Circulation. 2006;114:18-25

New-Onset Atrial Fibrillation after CRT
Borleffs CJW et al. Heart Rhythm, Vol 6, No 3, March 2009

New-Onset Atrial Fibrillation after CRT NS
NS
NS
NS
Caldwell JC et al. Europace (2009) 11, 1295–1300

Aims Characterize pts’ AT/AF profiles Evaluate correlations between AT/AF and clinical outcome

Methods
A total of 1193 patients were included by 44 Italian cardiological centres. All patients received an implantable cardioverter defibrillator (ICD) able to deliver cardiac resynchronization therapy (CRT) according to ICD and CRT guidelines for • advanced heart failure • NYHA≥II • depressed LV function (LVEF<35%) • wide QRS complex (>120 ms) All patients were in sinus rhythm at implant.


Results (1) - Profile • An history of AT/AF was present in 310/1193 (26%) patients • Median follow-up period: 13 months • AT/AF longer than 10 minutes occurred in 361/1193 (30%) patients • New-onset AT/AF occurred in 178/882 (20%) patients • Predictors of AT/AF occurrence during follow-up are shown in the following
table
Univariate analysis Multivariate analysis
Predictor OR 95%CI p-value OR 95%CI p-
value
Male sex 1.14 1.00 – 1.81 0.048 1.59 0.99 – 2.563 0.056
Age ≥ 67 years 1.55 1.20 – 1.99 0.0007 1.55 1.07 – 2.24 0.0195 Secondary prevention 1.59 1.16 – 2.17 0.0036 1.53 0.97 – 2.41 0.0697
AT/AF history 5.70 4.31 – 7.55 <.0001 5.91 4.03 – 8.67 <.0001 Ischemic cardiopathy 1.35 1.05 – 1.74 0.0182 1.19 0.82 – 1.72 0.3611 Heart valve surgery 1.78 1.21 – 2.62 0.0036 1.48 0.85 – 2.58 0.1696
ACE inhibitors 0.67 0.49 – 0.92 0.0136 0.79 0.53 – 1.17 0.2358

Kaplan-Meier curves showing freedom from the composite endpoint (death or heart transplantation or HF
hospitalization) in patients with vs without AT/AF during follow-up.
0,60
0,65
0,70
0,75
0,80
0,85
0,90
0,95
1,00
0 100 200 300 400 500 600 700 800 900 1000
Observation period (day)
Com
posi
te e
ndpo
int f
reed
om p
roba
bilit
y
Patients in sinus rhythm
Patients with AT/AF during follow--up
Log Rank test P=0.0003

Resumption of sinus rhythm in patients with heart failure and permanent atrial fibrillation undergoing cardiac
resynchronization therapy: a longitudinal observational study
Gasparini M et al.
Kaplan–Meier estimation of cumulative SR resumption. Patients at risk are reported below the curve.
European Heart Journal (2010) 31, 976–983
Conclusions: In this large cohort, one in every 10 patients with HF and permanent AF treated with CRT spontaneously reverted to SR during follow-up, usually soon after implant. Independent predictors of this phenomenon were found to be post-CRT QRS 150 ms, baseline EDD 65 mm, LA diameter 50 mm, and ablated AVJ. Additional prospective clinical studies are needed to, on one hand, substantiate these findings and, on the other hand, to improve our understanding of CRT effects on atrial structure and function

ANALYSIS OF ONSET SCENARIOS PRIOR TO AF
98 pts, 612 episodes, 1150 onset scenarios
Maas06
short run9%
multiple PACs9%
short-long 6% PAC trend
19%↑
PAC-related43%
bradycardia18%
sudden rate 3% ↓
late reinitiation
%(< 5min)
7
early reinitiation
%(< 60s)
20 sudden onset 6%
tachycardia 1%rate increase 0.3%sudden rate 2%↑
rate decay 0.2%brady-tachy 0.4%22%
27%
PAC Suppression Post-PAC Response
Pace Conditioning Rate Soothing Post-Exercise Response DDD(R) pacing
Pace Conditioning Rate Soothing
Post-AF Response Pace Conditioning Rate Soothing
Atrial Pacing Mechanisms of Prevention of AF by Algorithms

Symptomatic AF Burden
0,0%
1,0%
2,0%
3,0%
4,0%
5,0%
1-Month 3-Month 6-Month
AF
Bur
den
(%)
DAO OFF
DAO ON
Follow up
(n = 288)
*p = 0.005
ADOPT Study
*p<0.0001
% Atrial Beats Paced *
DAO OFF 67.9
DAO ON 92.9
Atrial pacing
Carlson MD et al, JACC 2003;42:627-33
*
* *

Padeletti et al. Am Heart J 2008
Pacing Prevention Therapies

Mantaining CRT therapy

CRT in HF patients with AF
A patient with AF and HF treated with CRT, spontaneous irregular intrinsic beats alternate with fusion and pseudo-fusion beats, thus markedly reducing effective CRT. As shown in the figure, this may occur even during normal rate AF.
Gasparini M et al. Europace (2009) 11, v82–v86

24-h holter data for Responders and Nonresponders
Kamath et al. JACC 2009

Atrial fibrillation (whether permanent, persistent, or paroxysmal)
poses a number of challenges for adequate CRT delivery
! Rate control strategy encompasses 3 treatment options:
1. Pharmacological
treatment
Lowering heart rate ensures CRT delivery
4 Ueng KC, et al. Acute and long-term effects of atrioventricular junction ablation and VVIR pacemaker in symptomatic patients with chronic lone atrial fibrillation and normal ventricular response. J Cardiovasc Electrophysiol 2001; 12: 303–9.

Atrial fibrillation (whether permanent, persistent, or paroxysmal)
poses a number of challenges for adequate CRT delivery
! Rate control strategy encompasses 3 treatment options:
2. Device algorithm
options
Special pacing algorithms track / overdrive spontaneous ventricular beats. Reasonable as first-line approach when AF burden is low/intermediate.

The device provides these features for ensuring CRT delivery during events that potentially would interrupt it, as, for
example, PVC or atrial arrhythmias.
– Ventricular Sense Response (VSR) Allows the device to maintain the CRT when ventricular sensed event is detected.
– Atrial Tracking Recovery (ATR)
It is designed to restore A-V synchrony and CRT if they are lost due to PVC or a quick sinus rhythm 1:1
– Conducted AF Response (CAFR) Enables the delivery of CRT during AT or AF episodes
Features functioning

Conducted AF Response (CAFR)
Comparison: Conducted AF Response
Paroxymal AF Permanent AF

Atrial fibrillation (whether permanent, persistent, or paroxysmal)
poses a number of challenges for adequate CRT delivery
! Rate control strategy encompasses 3 treatment options:
3. Ablate and (CRT)-pace
for selected patients in whom high-rate AF may jeopardizes satisfactory biventricular stimulation, and in CRT-D recipients determines inappropriate ICD interventions


ABLATE AND PACE: EF

Wood, M. A. et al. Circulation 2000;101:1138-1144
Clinical Improvement Using AVN Ablation for Refractory
AF

Wood, M. A. et al. Circulation 2000;101:1138-1144
Clinical Improvement Using AVN Ablation for Refractory
AF

Wood, M. A. et al. Circulation 2000;101:1138-1144
Clinical Improvement Using AVN Ablation for Refractory
AF



PAVE
• Left Ventricular-Based Cardiac Stimulation Post AV Nodal Ablation Evaluation
• 184 patients with chronic atrial fibrillation • Randomized after AV nodal Ablation
– RV-VVIR pacing – BiV VVIR pacing
• Followed for 6 months

PAVE Trial: Improvement of 6-minute walk score for AVN ablation with biventricular
pacemaker

PAVE Trial: Improvement of ejection fraction for AVN ablation with
biventricular pacemaker

Temporal changes in the 6-minute hallway walk test stratified by left ventricular ejection
fraction
100
80
60
40
20
0
Improvement (m)
6-weeks 3-months 6-months Time Frame
Baseline
BV ≤ 45% BV > 45% RV ≤ 45% RV > 45%
PAVE study J Cardiovasc Electrophysiol 2005:16;1160

Conclusions • In patients undergoing AV nodal ablation and
pacing AND – LVEF <45% – NYHA FC II or III CHF
• BiV pacing improved – 6 minute walk – Exercise Duration – VO2 max – Symptoms of CHF
• No Benefit was demonstrated for patients with preserved LV function

Brignole et all.; European Heart Journal (2011) 32, 2420–2429

Brignole et all.; European Heart Journal (2011) 32, 2420–2429

Conclusioni
In patients undergoing Ablate and Pace therapy for severely
symptomatic permanent atrial fibrillation, CRT is superior to RV
apical pacing in reducing the clinical manifestation of HF.
Brignole et all.; European Heart Journal (2011) 32, 2420–2429

M Brignole et all. Heart 2012;98:297e302.

M Brignole et all. Heart 2012;98:297e302.

Reduce Inappropriate Shocks

ICD Shocks in Atrial Fibrillation
Van Rees et al., JACC Vol. 57, No. 5, 2011

Improved SVT Discrimination • The most frequent cause of inappropriate shock is the incorrect
classification of SVT arrhythmias as VT by the device.1
• 8% to 40% of patients receive inappropriate shocks due to incorrect SVT classification2-7
• SVT discriminators optimized programming has shown a 25% reduction of inappropriate shock for SVT.8
1. Klein, JCE, 2003 2. Kuhlkamp V, JCE, 1999. 3. Deisenhofer I, JCE, 2001. 4. Theuns DA, JACC, 2004. 5. Grimm W, PACE, 1992. 6. Schmitt C, PACE, 1994. 7. Theuns DA, JACC, 2005. 8. Swerdlow, PACE, 2006
Friedman et al, Circulation, 2006
400 pts 27 centri
Theuns DA, JACC, 2005
60 pts single center

Areas of consensus on ablation techniques that were identified by the Task Force.
The Task Force recommends that:

AF ablation in CHF
Study Study population Results
Hsu et al. 2004 Prospective study
58 consecutive patients with HF and LVEF < 45% vs. 58 matched patients without HF
78% of the patients with CHF and 84% of controls were free of AF Significant improvement in LVEF of 21 ± 13%, exercise capacity, symptoms scores, and QoL scores
Tondo et al. 2006 Prospective study
40 patients with LVEF < 40% vs. 65 patients with normal ventricular function
87% of patients with decreased EF and 92% of patients with normal EF were free of AF Improvement in LVEF from 33% to 47%
Gentlesk et al. 2007 Prospective study
67 patients with reduced LVEF (≤50%) vs. 366 patients with normal LVEF
86% of patients in decreased LVEF and 87% of patients in normal EF were free of AF LVEF increased from 42% to 56% after ablation
Khan et al. 2008 Prospective study
41 patients who underwent PVI vs. 40 patients who underwent Avj-Abl+CRT
Significant improvement in LVEF of 35 ± 9%, exercise capacity, symptoms scores, and QoL scores

PVI in AF-HF patients
1. No clinically relevant endpoints 2. Inadequate sample sizes 3. Younger patients (mean age range: 54-64 yrs)
4. Short term follow-up: long term effects of the therapy and of new scar formation remained uninvestigated

PABA-CHF Pulmonary Vein Antrum Isolation vs AV
Node Ablation and Biventricular Pacing In Heart Failure Patients with Atrial
Fibrillation
Kahn M, Natale A et al NEJM 2008
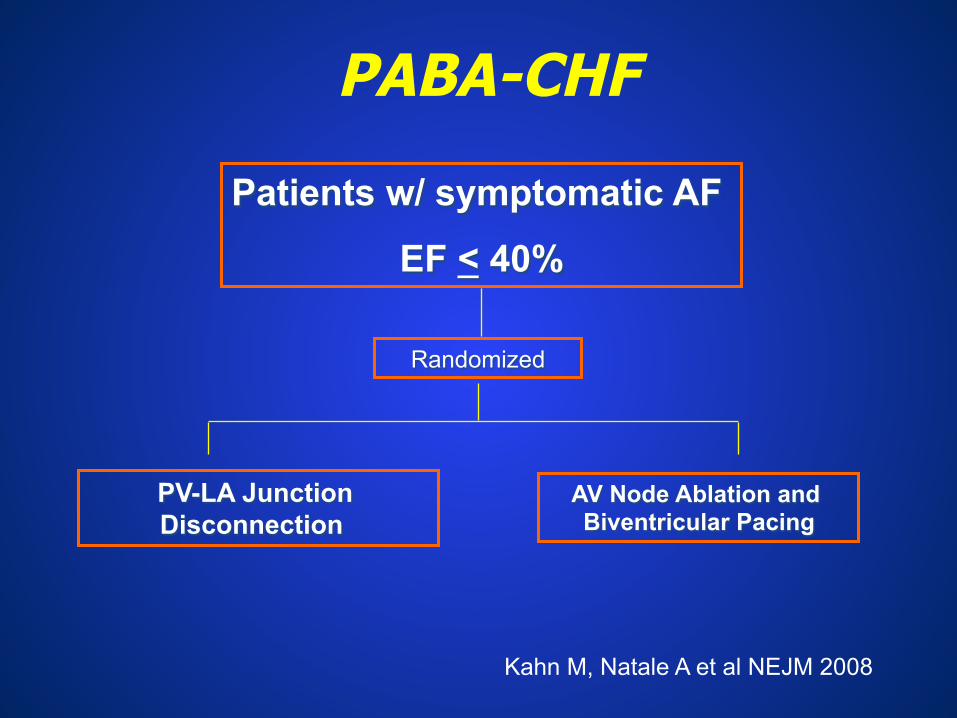
Patients w/ symptomatic AF
EF < 40%
PV-LA Junction Disconnection
Randomized
AV Node Ablation and Biventricular Pacing
PABA-CHF
Kahn M, Natale A et al NEJM 2008

Flow diagram of trial
81 patients qualified
41 randomized to PVI 40 randomized to AVN ablation with BIV
39 with follow-up at 3 months
38 with follow-up at 3 months
39 with follow-up at 6 months
38 with follow-up at 6 months

Baseline Characteristics Pulmonary
vein isolation (n=41)
AVN ablation-Biv
(n=40) Age ± SD (years) 60 ± 8 61 ± 8 Sex (% male) 95 88 CAD (%) 73 68 Type of AF
Paroxysmal (%) 49 54 Persistent/chronic (%) 51 46
Duration of AF ± SD (years) 4.0 ± 2.4 3.9 ± 2.8 Ejection Fraction ± SD (%) 27 ± 8 29 ± 7 Left atrial size ± SD (cm) 4.9 ± 0.5 4.7 ± 0.6 6-min walk distance ± SD (m) 267 ± 54 281 ± 44 MLWHF QOL scor ± SD 89 ± 12 89 ± 11
P is non-significant for all variables MLWHF: Minnesota Living with Heart Failure questionnaire

020406080
100
Free from AF (%)
0 6
Month
Freedom from Atrial Fibrillation With Anti-Arrhythmic Medications and More
Than One Procedure
PVI
AVN ablation-PVI
86%

020406080
Free from AF (%)
0 6
Month
Freedom from Atrial Fibrillation Without Anti-Arrhythmic
Medications and More Than One
PVI
AVN ablation-PVI
67%

PABA-CHF
37 35 33 31 29 27 25
0 3 6 0 3 6
100 80 60 40 20 0
360 340 320 300 280 260
P=0.003
P=0.0001
P=0.01
P=0.0004
Eje
ctio
n Fr
actio
n
Sco
re
Minnesota Living with Heart Failure Questionnaire
0 6
PVI AVN ablation-BIV
Dis
tanc
e (m
) PVI AVN ablation-BIV P<0.0001
Month Month
Month
Ejection Fraction 6-Minute Walk

Primary Endpoint Met in PVI Arm
• All three primary endpoints with P<0.05, at least 2 endpoints with P<0.025 and 1 endpoint with P<0.017 – QOL score (60 vs. 80, P<0.0001) – EF (35 vs. 28%, P=0.0004) – 6-minute walk distance (338 vs. 297 m,
P=0.0001) • Endpoints include parameters of
morphology, QOL and functional capacity

4
4,2
4,4
4,6
4,8
5
LA size (cm)
0 6
Month
Left Atrial Size
PVI
AVN ablation-BIV
P=0.0005

0
20
40
60
80
100
AAD Use (%)
0 6
Month
Anti-arrhythmic Medication Use
PVI
AVN ablation-BIV
P=0.12

Paroxysmal vs. Non-Paroxysmal AF in PVI Arm: Change over 6 Months
4,1
4,2
4,3
4,4
4,5
4,6
4,7
4,8
4,9
5
5,1
Paroxysmal Non-Paroxysmal
Change in LA Size
0
50
100
150
200
250
300
350
Paroxysmal Non-Paroxysmal
Change in 6-Minute Walk
P=0.06 P<0.0001

Paroxysmal vs. Non-Paroxysmal AF in PVI Arm: Change over 6 Months
0
5
10
15
20
25
30
35
40
Paroxysmal Non-Paroxysmal
Change in EF
0
10
20
30
40
50
60
70
80
90
100
Paroxysmal Non-Paroxysmal
Change in QOL
P=0.05 P=0.001

Conclusioni 1 La terapia di risincronizzazione elettrica nei
pazienti con scompenso cardiaco e FA cronica • È efficace purchè siano soddisfatti i criteri di
desincronizzazione ventricolare • Può essere eseguita anche con comuni
apparecchi DDD se il minimo AV delay lo consente
• Necessita spesso della contemporanea ablazione del nodo AV per ottenere il 100% di cattura ventricolare

Conclusioni 2 La terapia di risincronizzazione elettrica nei pazienti
con scompenso cardiaco e FA parossistica può efficacemente prevenire l’aritmia per:
• Miglioramento del quadro emodinamico • Impiego degli algoritmi di prevenzione delle
tachiaritmie atriali • Impiego delle terapie ATP • Impiego di tecniche alternative di pacing atriale

Conclusioni 3 • La FA in pazienti con scompenso cardiaco può avere un rilevante impatto negativo sul beneficio clinico dato dalla CRT, se questi non sono gestiti in modo appropriato. • E’ necessaria un’ attenta valutazione globale per definire con precisione il burden di FA al fine di impostare adeguate strategie diagnostiche e terapeutiche. • Alcuni sofisticati algoritmi di stimolazione presenti nei dispositivi di ultima generazione permettono di mantenere alto il livello di stimolazione della CRT. • Il beneficio clinico di tali algoritmi non sono stati ancora valutati da trial clinici randomizzati.


















