
Kardiovaskuläre Medizin – Médecine cardiovasculaire ... · Cardiovascular Medicine...
31
Cardiovascular Medicine Kardiovaskuläre Medizin – Médecine cardiovasculaire Official journal of the Swiss Society of Cardiology, the Swiss Society of Hypertension, the Swiss Society of Angiology and the Swiss Society of Paediatric Cardiology www.cardiovascmed.ch 7–8 10. 8. 2016 195 Thomas F. Lüscher The educated patient 204 Lina Melzer, Anja Faeh-Gunz, Barbara Naegeli, et al. Feasibility and limitations of 2D speckle tracking echocardiography 211 Milos Radosavac, Raphael Twerenbold, Max Wagener, et al. New quality indicator for treatment of acute myocardial infarction 197 Marco Roberto, Edoardo De Benedetti Procedural strategies for no-reflow prevention during PCI
Transcript of Kardiovaskuläre Medizin – Médecine cardiovasculaire ... · Cardiovascular Medicine...
CardiovascularMedicine
Kardiovaskuläre Medizin – Médecine cardiovasculaire
Official journal of the Swiss Society of Cardiology,
the Swiss Society of Hypertension, the Swiss Society of Angiology
and the Swiss Society of Paediatric Cardiology
www.cardiovascmed.ch
7–8
10.
8. 2
016
195 Thomas F. LüscherThe educated patient
204 Lina Melzer, Anja Faeh-Gunz, Barbara Naegeli, et al.Feasibility and limitations of 2D speckle tracking echocardiography
211 Milos Radosavac, Raphael Twerenbold, Max Wagener, et al.New quality indicator for treatment of acute myocardial infarction
197 Marco Roberto, Edoardo De BenedettiProcedural strategies for no-reflow prevention during PCI
TABLE OF CONTENTS 193
Viewpoint
Thomas F. Lüscher
195 The educated patient Wo man nicht nur Erfolg versprechen kann, muss nicht nur der Nutzen, sondern auch das Risiko
besprochen sein.
Review article
Marco Roberto, Edoardo De Benedetti
197 Procedural strategies for no-reflow prevention during PCI This revie w summarises available evidence concerning the most important nonpharmacological procedural strategies to prevent distal embolisation and, thus, no-reflow during per cutaneous coronary intervention.
Original articles
Lina Melzer, Anja Faeh-Gunz, Barbara Naegeli, Burkhardt Seifert, Monica Pfyffer,
Christine H. Attenhofer Jost
204 Feasibility and limitations of 2D speckle tracking echocardiography Two-dimensional speckle tracking echocardiography has been recommended as a helpful tool for assessing cardiac function. A mean global longitudinal strain value of >18% has been one of the recommended normal cut-off limits. Little is known about the performance of GLS and its impact in daily practice.
Editorial Board
Prof. Dr. Thomas F. Lüscher, Zürich (ed. in chief); Prof. Dr. François Mach, Genève (ed. in chief); PD Dr. Jan Steffel, Zürich (deputy editor); Dr. Philippe Meyer, Genève (deputy editor); Dr. Natalie Marty (Managing editor); Dr. Katharina Blatter (Managing editor)
Editors
Prof. Dr. Paul Erne, Luzern; Prof. Dr. Augusto Franco Gallino, Bellinzona; Prof. Dr. René Lerch, Puplinge / Genève (Senior editor); Prof. Dr. Bernhard Meier, Bern; Prof. Dr. Matthias Pfisterer, Basel; Prof. Dr. Hans Rickli, St. Gallen; Prof. Dr. Christian Seiler, Bern; Prof. Dr. Bernard Waeber, Lausanne
Section editors
The interesting ECG: Dr. Michael Kühne, Basel; Dr. Jürg Schläpfer, Lausanne. Images in cardiovascular medicine: Dr. Alain Delabays, Morges; Prof. Dr. Michel Zuber, Othmarsingen. The new device: PD Dr. Haran Burri, Genève; Prof. Dr. Stephan Windecker, Bern. The new compound: PD Dr. Georg Ehret, Genève. Evidence-based cardiology: Prof. Dr. Heiner Bucher, Basel; PD Dr. Jens Hellermann, Altstätten; PD Dr. Jörg Muntwyler, Kloten
Advisory Board
The members of the Advisory Board are listed on www.cardiovascmed.ch
compendium COMPACT – jetzt bestellen
Kurz gefasstes Fachbuch zu Arzneimitteln• Redaktionelle Zusammenfassungen aus compendium.ch• Identa-Abbildungen fester Arzneiformen• Therapeutisches Register• Stärkt Ihre Beratungskompetenz
Weitere Informationen und Bestelloptionen finden Sie auf: www.hcisolutions.ch/order
compendium COMPACT, ein Produkt der HCI Solutions AG
Ausgabe
2016 jetzt
erhältlich
Hardcover, ca. 1000 Seiten, neues, handliches Format: 15 × 21,5 cm sFr. 145.– / ¤ (D) 145.–, zzgl. Versandkosten

TABLE OF CONTENTS 194
Milos Radosavac, Raphael Twerenbold, Max Wagener, Ursina Honegger, Christian Puelacher,
Karin Wildi, Tobias Reichlin, Philipp Kreutzinger, Fabio Stallone, Petra Hillinger, Cedric Jaeger,
Maria Rubini Gimenez, Samyut Shrestha, Michael Heberer, Michael Kuehne, Stefan Osswald,
Christian Mueller
211 New quality indicator for treatment of acute myocardial infarction Crude mortality is commonly used as a quality indicator for the treatment of acute myocardial infarction, but has important limitations including its dependence on the local case-mix. The authors aimed to explore the feasibility of a novel approach using risk adjustment according to the Global Registry of Acute Coronary Events.
Case reports
Mattia Cattaneo, Daniel Sürder, Rolf Wyttenbach, Mario Alerci, Pierluigi Pedrazzi, Marcel Arnold,
Augusto Gallino
217 Dissected woman A patient with multiple spontaneous arterial dissections.
Oliver T. Reuthebuch, Christoph Kaiser, Markus Maurer, Friedrich Eckstein, Martin Grapow
220 Interventional valve-under-valve implantation A case of false deployment of a self-expandable TAVI prosthesis due to inadvertent and incorrect
release of an eyelet in the crown of the valve resulting in a tilted valve.
ww
w.v
erla
g-jo
han
nes
-pet
ri.c
h
Verlag Johannes Petri | Steinentorstrasse 11 | CH-4010 BaselTel. +41 (0)61 467 85 75 | Fax +41 (0)61 467 85 76 | [email protected]
Ver lag Johannes Pet r i
Den Toten Ruhe gebenNach einem Selbstmordversuch mit anschliessendem Psychiatrieaufenthalt beginnt die 36-jährige Emily ein Praktikum in einem Bestattungsdienst. Sie erhält Einblick in die Welt des Todes. Dabei merkt sie, wie sie an der Arbeit mit den Toten wieder lebendig wird. Doch dann passiert, was Emily sich nie hätte vorstellen können: Ihr ehemaliger Psychiater wird tot aufgefunden, die Polizei geht von einem Verbrechen aus. Nach dem ersten Schock beschleicht Emily ein ungutes Gefühl. Sie glaubt zu wissen, wer ihn umgebracht hat …
Evelyn ReimannEs muss etwas passierenRoman2016. 182 Seiten. Gebunden.sFr. 29.– / ¤ 29.– ISBN 978-3-03784-100-6Verlag Johannes Petri
ImpressumCardiovascular MedicineOfficial publication of the Swiss So-ciety of Cardiology, the Swiss Society for Angiology, the Swiss Society of Hypertension and the Swiss Paediatric Cardiology Society.Contact: Gisela Wagner, CVM Editorial office, EMH Medical Publishers Ltd., Farnsburgerstrasse 8, 4132 Muttenz, Phone +41 (0)61 467 85 52, Fax +41 (0)61 467 85 56, [email protected], www.cardiovascmed.chOnline manuscript submission: http://www.edmgr.com/cvm
Publishing company: EMH Medical Publishers Ltd., Farnsburgerstrasse 8,4132 Muttenz, Phone +41 (0)61 467 85 55,Fax +41 (0)61 467 85 56, www.emh.ch
Marketing / Advertising: Dr. phil. II Karin Würz, Head of Marketing and Communication, Phone +41 (0)61 467 85 49, Fax +41 (0)61 467 85 56, [email protected]
Subscription: EMH Medical Publish-ers Ltd., Subscriptions, Farnsburger-strasse 8, 4132 Muttenz, Tel. +41 (0)61 467 85 75, Fax +41 (0)61 467 85 76, [email protected] price (excl. postage): CHF 125.–, students CHF 63.–. Postage prices and single issues see www.sanp.ch
ISSN: print version: 1664–2031 / online version: 1662-629X
Mode of publication: 11 issues per year.
© EMH Swiss Medical Publishers Ltd. (EMH), 2016. «Cardiovascular Medicine» is an open access publication of EMH. EMH Swiss Medical Publishers Ltd. grants to all users on the basis of the Creative Commons license «Attribu-tion-NonCommercial-NoDerivatives 4.0 International» for an unlimited period the right to copy, distribute, display, and perform the work as well as to make it publicly available on condition that: (1) the work is clearly attributed to the author or licensor; (2) the work is not used for commercial purposes and (3) the work is not alte-red, transformed, or built upon. Any use of the work for commercial purpo-ses needs the explicit prior authorisa-tion of EMH on the basis of a written agreement.
Hinweis: Alle in dieser Zeitschrift publizierten Angaben wurden mit der grössten Sorgfalt überprüft. Die mit Verfassernamen gezeichneten Veröf-fentlichungen geben in erster Linie die Auffassung der Autoren und nicht zwangsläufig die Meinung der Redak-tion von «Cardiovascular Medicine» wieder. Die angegebenen Dosierun-gen, Indikationen und Applikationsfor-men, vor allem von Neuzulassungen, sollten in jedem Fall mit den Fach-informationen der verwendeten Medikamente verglichen werden.
Production: Schwabe AG, Muttenz, www.schwabe.ch

Die Zukunft der Arzt-Patienten-Beziehung
The educated patientThomas F. Lüscher
Editorial Office, Cardiovascular Medicine, Zurich Heart House, Zürich, Switzerland
Angefangen hat Medizin mit Zuwendung, als sie nur dies zu bieten hatte [1]. Mit dem Helfen und Trösten war jedoch nicht viel gewonnen, da Behandeln, und erst recht Heilen, noch in ferner Zukunft lag. Hippo-krates mahnte denn auch zur Vorsicht, als er in seinem ärzt lichen Eid primum nil nocere zu einem Grundprin-zip machte. Zu Zeiten, als die meisten Massnahmen nur Schaden brachten und sich auch der Nutzen ärztlicher Zuwen-dung im Lindern von Sorge und Schmerz erschöpfte, war eine solche Haltung ein ethisches Erfordernis. Es hat auch heute noch seine Berechtigung. Seither haben sich die Möglichkeiten der Medizin be-eindruckend entwickelt. Es gelingt uns nicht nur, Schmerz zu lindern; die Heilkunst kann ihrem Namen gemäss auch heilen, z.B. Infektionskrankheiten, oder auch wirksam behandeln, z.B. den Herzinfarkt, Herz-klappenleiden, einige Tumorleiden und vieles mehr. Mit der Wirksamkeit medizinischer Massnahmen kamen aber auch Nebenwirkungen mit ins Spiel: Was wirkt, kann auch schaden. Als Helfen nicht nur zuneh-mend half, sondern auch Unerwünschtes, ja gar Scha-den mit sich bringen konnte, musste sich das Arzt-Pati-enten-Verhältnis langsam, aber unaufhaltsam ändern. Wo man nicht nur Erfolg versprechen kann, muss
VIEWPOINT 195
Abbildung 1: Veranstaltung «Ein Herz für Zürich» der Stiftung für Herz- und Kreislauf-
forschung (Zurich Heart House) in einem Hörsaal der Universität Zürich.
nicht nur der Nutzen, sondern auch das Risiko bespro-chen sein. Auch stellt sich damit die Frage, was die beste Massnahme für den individuellen Patienten sei.Zunächst entschieden die Ärzte selbstherrlich und un-eingeschränkt – der Patient verstand ja sowieso nicht, wie die Sache sich verhielt. Noch zu Assistenzzeiten des Schreibenden wurde nicht allen Patienten die Diagno- se vermittelt, insbesondere wenn es sich um Tumoren handelte – eine heute undenkbare Haltung. Nun ist «informed consent» gefragt: Als Folge der Untaten brauner Schergen entstand die Helsinki-Deklaration und danach die Forderung des Weltärztebundes, bei je-der ärztlichen Handlung die Gesundheit der Patienten ins Zentrum aller Überlegungen zu stellen (The health of my patient will be my first consideration), ja als An-walt des Patienten uneingeschränkt seine Interessen zu vertreten (A physician should select in the patient’s best interest when providing medical care). Damals war aus der historischen Erfahrung heraus vor allem der Schutz der Patienten vor verbrecherischen Handlungen entscheidend; heute sind ökonomische Aspekte weit wichtiger [2]. Mit der Öko no mi sierung der Medizin meldete sich ein bisher unbekannter Druck auf die Entscheidungsfindung des Arztes: Das Budget des CEO (und der Versicherungen [3]) wurde plötzlich spürbar, die Unabhängigkeit ärztlichen Han-dels wahrnehmbar eingeschränkt. Dann machte die beherrschende Bedeutung des Geldes im modernen Denken auch vor Ärzten nicht halt: Die Versuchung, bei all gemeinen Patienten das Nötigste und bei Privat-versicherten möglichst viel zu tun, ist heute dokumen-tiert in Klinik und Praxis präsent [4].Mit «informed consent» kam der Bedarf nach dem «edu cated patient»: Nur ein Patient, der Grundlegen-des über seinen Körper weiss, kann den Ausführungen seines Arztes folgen. Nur eine Patientin, die Nutzen und Gefahren verschiedener Verfahren kennt, kann informiert entscheiden – und heute entscheiden letzt-lich die Pa tie n ten. Für vernünftige Entscheidungen ist Zugang zu Informationen in Laiensprache erforder-lich. Dazu braucht es eine eingehende, für den Patien-ten verständliche Aufklärung des Sachverhalts, d.h. der Krankheit sowie der Möglichkeiten ihrer Behand-lung und vor allem deren Nutzen und Risiken. Die ärzt-liche Kunst besteht hier darin, zwischen Einsicht und
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):195–196

VIEWPOINT 196
Angst den richtigen Weg für die Patientenaufklärung zu finden.Und es wurde bereits einiges erreicht: Diabetiker be-handeln sich seit langem selbständig unter Aufsicht ih-res Arztes. Viele Hypertoniker messen sich regelmäs-sig den Blutdruck selbst [5] und kennen die Zielwerte und die Wirkung ihrer Medikamente. Selbständige Pa-tienten halten sich eher an die Verordnungen [6]. Sie sind nicht nur besser eingestellt, sie brauchen auch we-niger Ressourcen. Doch nicht überall konnte sich der «edu cated patient» wirksam entwickeln. Die häufigste Informationsquelle ist Dr. Google – gewiss findet sich dort viel Gutes, aber auch viel Marketing und Junk. Vorträge werden z.B. von der Seniorenuniversität, Kli-niken und dem «Zurich Heart House» angeboten und gut besucht, was den Bedarf der Patienten unter-streicht (Abb. 1). Eine unabhängige, breit zugängliche Informationsquelle ist ein Bedürfnis. Mit dem Buch «Das gesunde und das kranke Herz» [7] (Abb. 2) haben Autoren des UniversitätsSpitals in Zürich ein Lehrbuch für Patienten geschaffen, das reich illustriert mit intu-itiv erfassbaren Abbildungen und einem allgemein verständlichen Text den Zugang zum Laien sucht. Die Devise war: «You must be able to explain it to your grandmother», wie ein amerikanischer Mentor den Schreibenden einst lehrte. Nur wer einfach zu erklären weiss, hat die Sache wirklich verstanden. Das vorlie-gende Buch des Teams des Universitären Herzzen-trums Zürich hat versucht, diesen Weg zu beschreiten.
Wir sind überzeugt, dass damit medizinische Mass-nahmen sinnvoller und nachhaltiger eingesetzt wer-den und sich damit auch der Outcome vieler Pa tienten verbessern lässt. Bei 3055 Infarktpatienten des schweizerischen SPUM-Registers zeigte sich, dass immerhin jeder 18. Patient das Statin und jeder 25. Pa tient das Aspirin nach einem Jahr auf Rat ihres Arztes – entgegen den Empfehlungen aller Richtlinien [8] – abgesetzt hatten [9]. Auch wenn nicht alle Kollegen dies gerne hören: Der «educated pa-tient» würde nachfragen – zum Nutzen seiner selbst und des Gesundheitssystems, das weniger Rehospitali-sationen und erneute Eingriffe zu verkraften hätte. Ebenso zeigte sich, dass viele Patienten mit familiärer Hypercholesterinämie und entsprechend hohem In-farktrisiko bereits in jünge rem Alter unbehandelt ein kardiales Ereignis er leiden [10] – der aufgeklärte Pati-ent hätte dies für sich und seine Familienangehörigen vermieden. Wissen und Bildung können Leben retten. Nicht nur Ärztinnen und Ärzte, auch «educated patients» können dazu beitragen.
Disclosure statementDer Autor hat zusammen mit einem Team der Zürcher Klinik für Kar-diologie ein Buch zu diesem Thema geschrieben. Es sind aber keine finanziellen Vorteile involviert.
Literatur 1 Lüscher TF. Gedankenmedizin. Heidelberg: Springer; 2009. 2 Lüscher TF. Wieviel Marketing erträgt die Medizin? Cardiovasc
Med. 2014;17:3–7. 3 Lüscher TF. Krankenversicherungsgesetz, die Versicherungen und
die ärztliche Ethik – jenseits evidenzbasierter Medizin? Cardiovasc Med. 2008;11:183–6.
4 Bisig B, Gutzwiller F, Domenighetti G. Incidence of operations in Switzerland related to insurance status. Swiss Surg. 1998;4:109–16.
5 Lüscher TF, Vetter W. Blutdruckselbstmessung. Schweiz Rund-schau Med Prax. 1982;71:1454–61.
6 Vetter W, Lüscher TF. Adherence to medication. J Human Hypert. 1990;4(Suppl. 1):S43–6.
7 Lüscher TF, Tran A-P, Meyer M, Steffel J. Das gesunde und das kranke Herz. Muttenz: EMH Schweizerischer Ärzteverlag; 2015.
8 Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, et al. 2015 ESC Guidelines for the management of acute coronary syn-dromes in patients presenting without persistent ST-segment ele-vation. Eur Heart J. 2016;37(3):267–315.
9 Gencer B, Rodondi N, Auer R, Räber L, Klingenberg L, Nanchen D, et al. Reasons for discontinuation of recommended therapies accor-ding to the patients after acute coronary syndromes. Eur J Intern Med. 2015;26:56–62.
10 Nanchen D, Gencer B, Auer R, Räber L, Stefanini GG, Klingenberg R, et al. Prevalence and management of familial hypercholesterola-emia in patients with acute coronary syndromes. Eur Heart J. 2015; 36(36):2438–45.
Korrespondenz: Thomas F. Lüscher, MD, FESC, FRCP Cardiovascular Medicine Editorial Office Zurich Heart House Moussonstrasse 4 CH-8091 Zürich Cardio[at]tomluescher.ch
Abbildung 2: Ein Lehrbuch für Laien und Patienten:
«Das gesunde und das kranke Herz».
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):195–196
REVIEW ARTICLE 197
Nonpharmacological strategies to prevent distal embolisation and no-reflow during percutaneous coronary intervention
Procedural strategies for no-reflow prevention during PCIMarco Robertoa, Edoardo De Benedettib
a Internal Medicine Department, La Tour Hospital, Meyrin, Switzerland; b Cardiovascular Department, La Tour Hospital, Meyrin, Switzerland
Summary
Prompt referral for myocardial reperfusion represents the gold standard
emergency treatment for patients experiencing ST-elevation myocardial
infarction (STEMI). However, in a considerable proportion of STEMI
patients, reopening of the infarct-related artery is not always followed by
myocardial reperfusion. This condition is known as no-reflow and seems
to be related to microvascular obstruction. Interestingly, no-reflow has
been observed also in NSTEMI patients and during elective percutaneous
coronary intervention, particularly when performed on saphenous vein
grafts. Distal atherothrombotic embolisation has a key role in no-reflow
physiopathology. In this revie w we will summarise available evidence con-
cerning the most important nonpharmacological procedural strategies
tested in a clinical setting to prevent distal embolisation and, thus, no-re-
flow during per cutaneous coronary intervention.
Key words: percutaneous coronary intervention; no-reflow; distal embolisation
Abbreviations and Acronyms
CMR cardiac magnetic resonance
ECG electrocardiogram
IRA infarct-related artery
IVUS intravascular ultrasound
MBG myocardial blush grade
MCE myocardial contrast echocardiography
MVO microvascular obstruction
OCT optical coherence tomography
PCI percutaneous coronary intervention
STEMI ST-segment elevation myocardial infarction
TIMI Thrombolysis in Myocardial Infarction
Introduction
Prompt referral for mechanical (primary percutane-ous coronary intervention [pPCI]) or pharmacological (fibrinolytic) reperfusion represents the gold standard emergency treatment for patients experiencing ST- elevation myocardial infarction (STEMI) [1–3]. How-ever, in a considerable proportion of STEMI patients, successful restoration of infarct-related artery (IRA) patency is not followed by adequate myocardial blood flow at a tissue level. This condition is known as no- reflow and seems to be related to microvascular ob-struction (MVO) [4]. No-reflow represents one of the most challenging conditions for interventional cardio-logists and has a strong negative impact on in-hospital and long-term clinical outcome of STEMI patients treated with pPCI or fibrinolysis, negating the benefits of prompt and effective reopening of the IRA [5–10]. In-terestingly, no-reflow has been observed also in NSTEMI patients and during elective PCI, particularly when performed on saphenous vein grafts [11].
No-reflow can be assessed with both invasive and non-invasive techniques. On the basis of coronary angio-graphy, no-reflow is usually defined as a Thrombolysis in Myocardial Infarction (TIMI) flow grade <3 or 3 in the presence of a myocardial blush grade (MBG) 0 to 1 de-spite effective mechanical or pharmacological restora-tion of IRA patency [12, 13]. In the setting of STEMI, an ST-segment elevation resolution of less than 70% 60 to 90 minutes after pPCI on the surface electrocardio-gram (ECG) is usually considered suggestive of no- reflow [14]. Myocardial contrast echocardiography (MCE) uses ultra sound to visualise contrast micro-bubbles that freely flow within patent microcircula-tion; no-reflow is detected as lack of intramyocardial contrast opacification [15]. Cardiac magnetic resonance (CMR), with gadolinium to assess regional cardiac per-fusion, diagnoses no-reflow through: (1) lack of gado-linium enhancement during first pass; and (2) lack of gadolinium enhancement within a necrotic region, identified by late gadolinium hyper-enhancement [16]. The physiopathology of no-reflow is complex, multi-factorial and still incompletely understood. In humans, no-reflow is likely to be due to a variable com-bination of four major pathogenetic components: (1) distal atherothrombotic embolisation from both cul-prit plaque and thrombus; (2) ischaemic injury; (3) rep-erfusion injury; and (4) individual susceptibility of the coronary microcirculation. Concerning distal emboli-sation, emboli of different sizes can originate from epi-cardial coronary culprit plaque and thrombus. Of note, experimental studies showed a significant and ir-
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):197–203

REVIEW ARTICLE 198
reversible reduction in myocardial blood flow when microspheres obstruct more than 50% of coronary cap-illaries [17]. Large emboli (with a diameter >200 µm) are the most likely to significantly obstruct pre-arterioles and, therefore, reduce myocardial blood flow at a tis-sue level [17, 18]. In this review we will summarise the most important predictors of no- reflow related to distal embolisation, as well as available evidence concerning the most im-portant nonpharmacological procedural strategies to preven t distal embolisation and, thus, no- reflow dur-ing PCI. As a result of the multifactorial physiopathol-ogy of no-reflow, multiple pharmaco logical agents spe-cifically targeting different physiopathological pathways, such as antiplatelet and vaso dilator drugs, have also been tested for prevention of no-reflow, espe-cially in the setting of STEMI. However, a systematic and comprehensive review of the use of pharmacologi-cal agents to prevent no-reflow is beyond the scope of the present article.
Procedural predictors of distal embolisation- related no-reflow
Several parameters have been shown to be able to pre-dict no-reflow occurrence probably owing, at least in part, to their ability to predict distal embolisation dur-ing PCI. Coronary angiography allows direct visualisation of luminal thrombus on culprit coronary stenosis. Pre-thrombectomy/pre-pPCI features of luminal thrombus as assessed with coronary angiography predict no- reflow occurrence in STEMI patients undergoing pPCI [19]. Interestingly, in STEMI patients undergoing mechanical thrombectomy as adjunct to standard pPCI, a high residual thrombus burden after thromb-ectomy has also been recently demonstrated to inde-pendently predict post-pPCI no-reflow occurrence [20]. Moreover, a reference lumen diameter bigger than 4 mm was an independent predictor of no-reflow in a study by Yip et al. [19]. In a recent large retrospective registry of acute coronary syndrome patients, PCI on bifurcation coronary lesions and PCI on complex coro-nary lesions as assessed with coronary angiography were both associated with higher no-reflow risk, prob-ably due to a high risk of distal embolisation from coro nary culprit plaque. However, both NSTEMI and STEMI patients were included in this registry [21]. Coro-nary angiography also allows prediction of distal em-bolisation and no-reflow during elective PCI per-formed on saphenous vein grafts. In a study by Liu et al., the presence of extensive graft disease, large plaque volume and presence of complicated/ulcerated plaque
were all associated with higher risk of distal embolisa-tion and periprocedural myocardial infarction in patients undergoing PCI in saphenous vein grafts [22]. A study by Sdringola et al. confirmed and further expanded these results by showing an increased risk of no-reflow/slow-flow in patients undergoing PCI in saphenous vein grafts in the presence of extensive graft disease and/or complicated/ulcerated plaque [23]. Coronary angiography represents the gold standard technique for the diagnosis of coronary stenosis. How-ever, coronary angiography does not allow direct visuali sation of coronary plaque and vessel walls. Intra vascular ultrasound (IVUS) and optical coherence tomography (OCT) are catheter-based techniques that provide high-resolution cross-sectional images of the lumen and vessel wall, thus allowing assessment of plaque burden and of plaque morphological fea-tures. A recent study by Li et al. using IVUS demon-strated, in a series of 120 STEMI patients, that plaque area, plaque volume, presence of eccentric plaque, presence of soft/lipid-rich plaque and plaque rupture were all predictors of no-reflow [24]. Moreover, pres-ence of un calcified plaques associated with backward ultrasound attenuation seems to be associated with higher risk of no- reflow in STEMI patients [25, 26]. Pre-diction of no- reflow with OCT is still controversial. In a little series from Tanaka et al. the presence of a thin-cap fibro atheroma (i.e., a plaque with lipid content in ≥2 quadrants and the thinnest part of the fibrous cap measuring <65 µm) was found to be a predictor of no-reflow in NSTEMI patients undergoing urgent PCI [27]. This association was not confirmed in a more recent study by Ikenaga et al. in 39 STEMI patients. In this study the longitudinal length of the lipid pool was found to be the only OCT predictor of no-reflow [28]. In-terestingly, IVUS and OCT data seem to be able to pre-dict no-reflow occurence mainly due to an increased risk of distal embolisation from coronary plaque. In a recent study by Carol et al. on STEMI patients, late clinical presentation (i.e., first medical contact >12 hours after symptom onset) was associated with a higher prevalence of old organised thrombus on patho logical analysis after thrombus-aspiration dur-ing pPCI [29]. Organised thrombus is known to be an independent predictor of both in-hospital and long-term mortality in STEMI patients undergoing pPCI [30–31]. Moreover, organised thrombus, as compared with fresh thrombus, was associated with a higher risk of macroscopic distal embolisation during angiogra-phy and with a lower rate of complete ST segment reso-lution after pPCI in a recent study by Verouden et al. [32]. This could explain, at least in part, the high risk of no-reflow observed in late-presenting STEMI patients.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):197–203
REVIEW ARTICLE 199
Interestingly, increased risk of severe ischaemic- and reperfusion-related injury could also contribute to the high risk of no-reflow observed in this subgroup of STEMI patients. Therefore, prompt referral for reper-fusion with reduction of ischaemia time surely repre-sents a key strategy to prevent no-reflow occurrence, reduce infarct size and allow myocardial salvage in STEMI patien ts.
Management of distal embolisation to prevent no-reflow
As seen before, distal embolisation from coronary thrombus or plaque has a key role in no-reflow physio-pathology. Multiple nonpharmacological procedural
strategies have been tested in a clinical setting in an ef-fort to prevent distal embolisation and, thus, no- reflow.
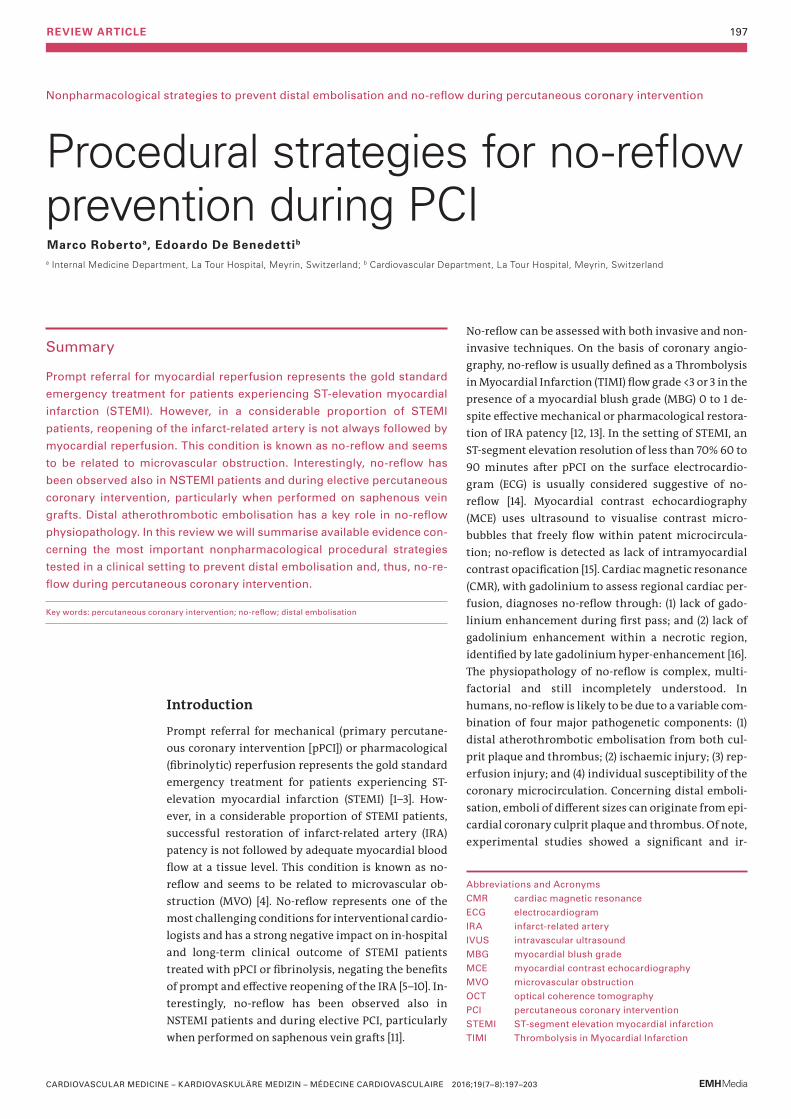
Thrombectomy devicesThe use of manual or mechanical thrombectomy de-vices to reduce the risk of distal embolisation during pPCI has been investigated in several clinical trials. Manual thrombectomy is usually performed using dedicated catheters compatible with a 6 or 7 French guiding catheter on 0.014’’ guide-wires and allows di-rect retrieval of intraluminal thrombus (fig. 1). Mechanical thrombectomy devices like Angiojet® use high-pressure backward saline jets to create a vacuum at the tip of the catheter to break up and remove thrombus.
Figure 1: Panel A. Coronary angiography of an 82-year-old smoking, hypertensive and dyslipidaemic patient presenting to the
emergency department for typical chest pain. Angio graphy shows a subocclusive thrombotic lesion of the proximal portion of
first marginal artery.
Panel B. After guidewire crossing of this thrombotic lesion, a thrombus aspiration catheter was advanced into the mid portion
of first marginal artery beyond the thrombus.
Panel C. Thrombotic material retrieved from culprit coronary plaque.
Panel D. After thrombus aspiration a percutaneous coronary intervention (PCI) was performed. The patient underwent direct
stenting with drug-eluting stent implantation. Good final angiographic result with a post-PCI TIMI flow 3.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):197–203

REVIEW ARTICLE 200
In the REMEDIA trial thrombectomy with a simple a manual aspiration catheter in a pPCI setting was asso-ciated with reduced risk of both angiographic and ECG no-reflow and better post-pPCI myocardial perfusion as assessed with MCE [33, 34]. A larger clinical trial, the TAPAS trial, randomly assigned 1071 STEMI patients to either standard PCI or PCI with manual thromb ectomy. The TAPAS trial confirmed data from the REMEDIA trial by showing a reduction in angiographic no-reflow occurrence in patients undergoing manual thromb-ectomy during pPCI. This trial further expanded REMEDIA trial results by showing a significant reduc-tion in 1-year cardiovascular mortality in patients treated by use of manual thrombus aspiration [35]. However, in a more recent clinical trial, by Lagerqvist et al., that randomised 7244 STEMI patients to manual thrombectomy followed by pPCI or pPCI alone, throm-bus aspiration was not associated with a significant reduction in overall 1-year mortality. Furthermore, thrombus aspiration did not significantly reduce the 1-year rate of a composite of death from any cause, rehospitalisation for myocardial infarction and stent thrombosis [36]. Moreover, 5-year follow-up data from a real-world, large-scale clinical registry, the KREDO-Kyoto AMI registry, were recently published and showed that thrombus aspiration was not able to significantly reduce 5-year mortality in STEMI patients undergoing pPCI [37]. The INFUSE-AMI trial is a recent 2×2 factorial design trial including 452 STEMI patients referred for pPCI who were randomly assigned to either intracoronary abciximab or no abciximab and to either manual aspiration thrombectomy as adjunct to standard pPCI or standard pPCI alone. Thrombus
aspiration was not associated with a significant reduc-tion in 30-day infarct size as assessed with CMR [38]. Of note, in more recent studies, the widespread use of bivalirudin and glycoprotein IIb/IIIa inhibitors could have diluted the beneficial effect of manual thromb-ectomy on long-term clinical outcome. At present, clinical evidence seems to support the use of manual thrombectomy to prevent no-reflow occurrence even if benefit on mortality/long-term clinical outcome remains unclear. Therefore, manual thrombectomy is still a class IIa recommendation in 2012 European Soci-ety of Cardiology (ESC) guidelines in the setting of pPCI and may be proposed to STEMI patients with a high angiographic thrombus burden [39]. Data on the use of mechanical thrombectomy devices as adjunct to standard PCI are still conflicting. In a study by Ali et al., 480 STEMI patients were randomly assigned to mechanical thrombectomy as adjunct to PCI or standard PCI alone. Despite effective thrombus removal, mechanical thrombectomy was not associ-ated with improved ECG reperfusion outcomes. More-over, no benefits on 30-day clinical outcome were observed in patients undergoing mechanical thromb-ectomy [40]. However, in the JETSTENT trial by Miglio-rini et al., rheolytic thrombectomy was associated with an increased rate of complete resolution of ST-segment elevation and better 6-month and 1-year clinical out-comes [41]. Even results of studies directly comparing manual and mechanical thrombectomy are not uni-vocal. In a study by Parodi et al., 80 STEMI patients were random ly assigned to either manual or mechani-cal throm bectomy. Mechanical thrombectomy was associated with significantly better post-pPCI reper-fusion [42]. However, in the recent COCOTH study by Giglioli et al., randomising 185 STEMI patients to either manual or mechanical thrombectomy as adjunct to standard PCI, no differences in both ECG and angio-graphic re perfusion outcomes were observed between the two study groups [43]. In summary, the inconclu-sive results of these studies do not support routine use of the more expensive mechanical thrombectomy de-vices. However, mechanical thrombectomy devices could represent a valid therapeutic option in selected cases, such as manual thrombectomy device failure or massive intracoronary thrombosis.
Distal protection devicesDistal protection devices used in the setting of PCI essentially consist of a filter device placed between the target lesion and the distal vasculature (fig. 2). Filter-based distal protection devices allow blood flow during PCI and prevent distal migration of microparticles whose diameter is greater than pore size (usually 100–
Figure 2: Filter distal protection device – FilterWire EX
(Copyright © by Boston Scientific – reproduced with permission).
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):197–203
REVIEW ARTICLE 201
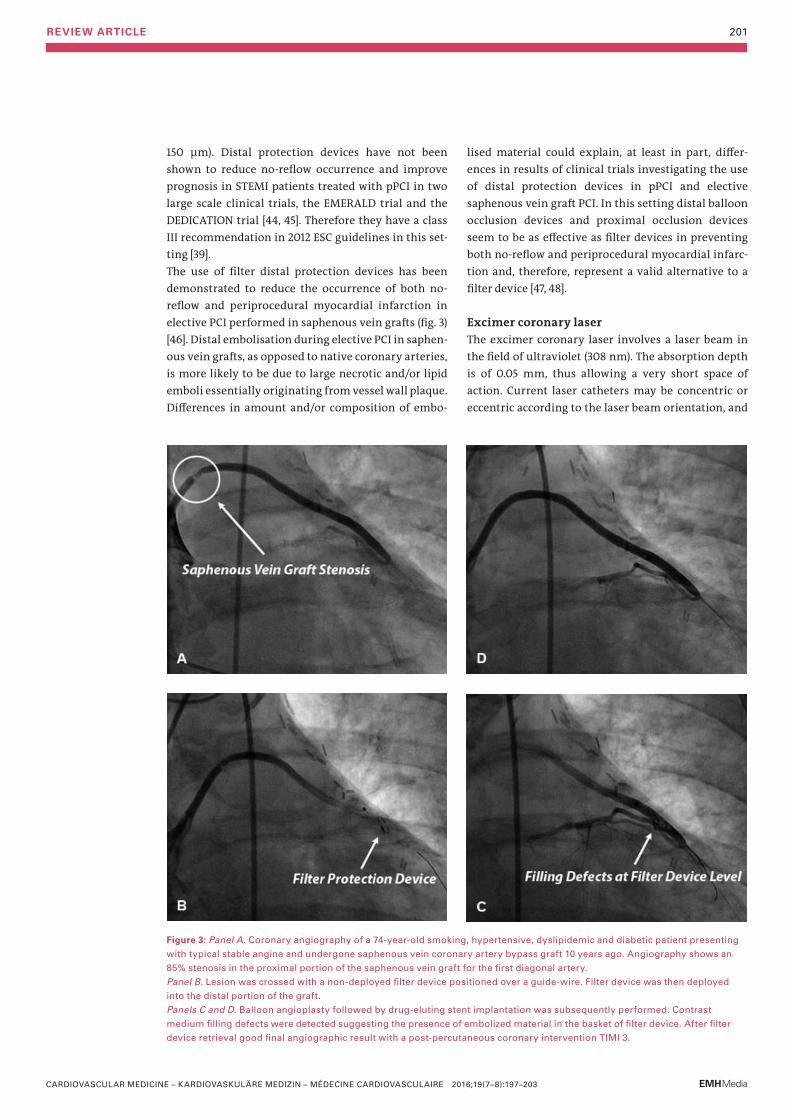
150 μm). Distal protection devices have not been shown to reduce no-reflow occurrence and improve prognosis in STEMI patients treated with pPCI in two large scale clinical trials, the EMERALD trial and the DEDICATION trial [44, 45]. Therefore they have a class III recommendation in 2012 ESC guidelines in this set-ting [39]. The use of filter distal protection devices has been demonstrated to reduce the occurrence of both no- reflow and periprocedural myocardial infarction in elective PCI performed in saphenous vein grafts (fig. 3) [46]. Distal embolisation during elective PCI in saphen-ous vein grafts, as opposed to native coronary arteries, is more likely to be due to large necrotic and/or lipid emboli essentially originating from vessel wall plaque. Differences in amount and/or composition of embo-
lised material could explain, at least in part, differ-ences in results of clinical trials investigating the use of distal protection devices in pPCI and elective saphen ous vein graft PCI. In this setting distal balloon occlusion devices and proximal occlusion devices seem to be as effective as filter devices in preventing both no-reflow and periprocedural myocardial infarc-tion and, therefore, represent a valid alternative to a filter device [47, 48].
Excimer coronary laserThe excimer coronary laser involves a laser beam in the field of ultraviolet (308 nm). The absorption depth is of 0.05 mm, thus allowing a very short space of action. Current laser catheters may be concentric or eccentric according to the laser beam orientation, and
Figure 3: Panel A. Coronary angiography of a 74-year-old smoking, hypertensive, dyslipidemic and diabetic patient presenting
with typical stable angina and undergone saphenous vein coronary artery bypass graft 10 years ago. Angiography shows an
85% stenosis in the proximal portion of the saphenous vein graft for the first diagonal artery.
Panel B. Lesion was crossed with a non-deployed filter device positioned over a guide-wire. Filter device was then deployed
into the distal portion of the graft.
Panels C and D. Balloon angioplasty followed by drug-eluting stent implantation was subsequently performed. Contrast
medium filling defects were detected suggesting the presence of embolized material in the basket of filter device. After filter
device retrieval good final angiographic result with a post-percutaneous coronary intervention TIMI 3.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):197–203

REVIEW ARTICLE 202
may vary in size: concentric catheters have a diameter of 0.9, 1.4, 1.7 or 2 mm whereas eccentric catheters have a diameter of 1.7 or 2 mm. Finally, energy production may vary as the smaller laser catheter is also the most powerful, producing a beam of 80 mJ/mm2/80 hertz. The use of excimer coronary lasers in STEMI patients undergoing pPCI could be of interest for many reasons: rapid removal of thrombus with vaporisation of pro-coagulant reactants, reduction of distal embolisation risk and debulking of underlying plaque. In the CARMEL registry 151 high-risk STEMI patients were enrolled, including patients with cardiogenic shock, rescue PCI patients and patients presenting with degenerated saphenous vein grafts and/or complex lesion morphology. The use of an excimer coronary laser was associated with high procedural and device success rates, a low complication rate and a significant increase in TIMI flow grade. Maximal laser gain was achieved in lesions with a high thrombus burden [49]. A registry by Dave et al. confirmed these positive results by showing a significant increase in MBG, and high angiographic and ECG reperfusion rates in STEMI patients treated with and excimer coronary laser [50]. Despite these encouraging results, data from large clinical trials supporting the use of excimer coronary lasers to prevent no-reflow occurrence during pPCI are still lacking. One small randomised study by Dorr et al., in a population of 27 STEMI patients, showed a shorter TIMI frame count in patients treated with an excimer coronary laser as compared with a conven-tional treatment group, treated with balloon angio-plasty and stent implantation alone [51]. The LASER-AMI trial, which is now on-going, compares use of the exci-mer coronary laser with manual thrombus aspiration in STEMI patients undergoing pPCI to prevent ECG no-reflow occurrence. Results from this trial should better clarify the role of the excimer coronary laser in this clinical setting [52].
STENTYS® Self-Apposing stentThe STENTYS® Self-Apposing stent is a self-expanding nitinol stent. STENTYS® is compatible with 6 French guiding catheters and is delivered using a rapid- exchange delivery system over a conventional 0.014” guide-wire. STENTYS® is available in a bare metal ver-sion and in a drug-eluting version eluting paclitaxel, and gradually conforms to vessel wall shape. The use of a self-expanding stent in the setting of pPCI could be of interest for many reasons. First of all, in STEMI patients, thrombus dissolution behind the stent struts and pro-gressive vessel wall relaxation after vasoconstriction which characterise the acute phase of STEMI could lead to stent undersizing and, therefore, to incomplete stent
apposition. Previous studies demonstrated that acute and late incomplete stent apposition play a key role in the pathogenesis of acute and late / very late stent thrombosis [53–55]. STENTYS® is characterised by a pro-gressive increase in stent diameter, if unconstrained. The use of STENTYS® in the pPCI setting could, there-fore, reduce the risk of both incomplete stent apposi-tion and stent thrombosis. Concerning no-reflow oc-currence, aggressive stent deployment could lead to plaque disruption and distal embolisation from culprit coronary plaques. The ability of STENTYS® to grow in volume within the first hours to days after pPCI allows more gentle stent deployment (with lower stent bal-loon inflation pressures), which could lead to a reduced risk of plaque disruption or thrombus dislodgement and, therefore, of distal embolisation related no-reflow. At present, studies specifically focusing on no-reflow occurrence following STENTYS® implantation in pPCI setting are missing. Thus, future studies comparing risk of distal embolisation and no-reflow in STEMI patients undergoing self-expanding stent implanta-tion or conventional balloon-expandable stent im-plantation during pPCI are needed. The APPOSITION V trial is now on-going and will be the first randomised trial powered on clinical endpoints and directly com-paring bare metal STENTYS® with a conventional balloon- expandable stent (MULTI-LINK®) in patients presenting with STEMI undergoing pPCI [56]. At present, STENTYS® could represent a valid therapeutic option for STEMI patients undergoing pPCI, especially in the presence of specific anatomical subsets in which good stent apposition is unlikely to be achieved with conventional balloon-expandable stents.
MGuard® and MGuard Prime® stentsMGuard® (stainless steel) and MGuard Prime® (cobalt chromium) stents are bare metal stents equipped with a bio-stable mesh woven from a single strand of 20 µm of poly ethylene terephthalate, called MicroNet®, with pore size between 150 and 180 µm. MicroNet® has been developed to trap and seal thrombus and plaque against the vessel wall, thus potentially preventing dis-tal embolisation and no-reflow. In the MASTER trial, 433 STEMI patients presenting within 12 hours from symptom onset and referred for pPCI were randomly assigned to receive a MGuard® stent or a conventional bare metal / drug-eluting stent. Patients treated with MGuard® stent experienced a higher rate of complete ST-segment elevation resolution and a lower rate of angio graphic no-reflow. However, 30-day clinical out-come did not differ between the study groups [57]. Future studies are needed to better clarify the role of MicroNet® technology in the setting of pPCI and its
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):197–203

REVIEW ARTICLE 203
eventual benefits on long-term clinical outcome. Development of drug-eluting versions of these stents is on-going.
Direct stentingSpecific stent deployment techniques could also allow reduction of no-reflow occurrence in STEMI patients throughout a reduction of distal embolisation occur-rence. Direct stenting represents the deployment of an intracoronary stent without balloon predilatation. A trial by Loubeyre et al. compared direct stenting with balloon predilatation in 206 STEMI patients treated with pPCI. Direct stenting was associated with a de-creased rate of angiographic slow-flow/no-reflow and an increased rate of complete ST-seg ment elevation resolution as compared with predilatation with an angio plasty balloon [58]. Two recent meta-analyses confirmed the benefits of direct stenting during pPCI on post-reperfusion myocardial microvascular blood flow. In these meta-analyses direct stenting was also associated with a significant reduction in short-term and 1-year mortality, although these data were mostly derived retrospectively from small clinical registries rather than randomised controlled trials [59, 60]. In conclusion, available evidence supports direct stent-ing to prevent no-reflow in STEMI patients. However, only a specific subset of patients (those with optimal distal visualisation of the IRA after guidewire passage) is suitable for this technique in order to avoid stent un-dersizing.
Deferred stentingThe DEFER-STEMI trial recently compared deferred stenting (intention-to-stent 4 to 6 hours after balloon angioplasty) with immediate stenting for no-reflow prevention in pPCI. A total of 101 STEMI patients were enrolled. Deferred stenting was significantly associ-ated with lower no-reflow/slow-reflow rates and an increased myocardial salvage index at 6 months, but also with a potentially increased risk of recurrent STEMI [61]. Results from the DEFER-STEMI trial are pro-
vocative, but clinical benefits on both no-reflow occur-rence and prognosis in STEMI patients as well as the safety of deferred stenting (risk of bail-out stenting) should be confirmed in trials on larger populations.
Conclusions
Distal atherothrombotic coronary embolisation plays a key role in no-reflow physiopathology and multiple nonpharmacological procedural strategies have been tested in clinical practice in order to prevent distal embolisation and, thus, reduce no-reflow occurrence. In the setting of pPCI direct stenting should be prefer-red when feasible and when there is confidence about the real vessel size. Manual thrombectomy represents a valid therapeutic option in STEMI patients presen-ting with a high angiographic thrombus burden, even if benefit on mortality/long-term clinical outcome re-mains unclear. Distal filter protection devices have been demonstrated to reduce both no- reflow and peri-procedural myocardial infarction occurrence in elec-tive PCI performed in saphenous vein grafts, and their use should be encouraged in this setting. Future stu-dies are needed to better clarify the role of excimer co-ronary lasers in pPCI. STENTYS® and MGuard®/McGu-ard Prime® stents could provide protection against distal embolisation and no-reflow owing to their pecu-liar mechanical properties. However, future studies are needed in order to better evaluate potential bene-fits on long-term clinical outcome and, therefore, cla-rify their role in the setting of STEMI. Finally, concer-ning deferred stenting, results of the DEFER-STEMI trial are provocative, but need to be confirmed in lar-ger clinical trials specifically addressing safety issues.
Disclosures statementNo financial support and no other potential conflict of interest relevant to this article was reported.
References – The full list of references is included in the online article at www.
cardiovascmed.ch.
Correspondence: Dr. Edoardo De Benedetti Cardiovascular Department La Tour Hospital 1bis, avenue JD Maillard CH-1217 Meyrin edb[at]latour.ch
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):197–203
ORIGINAL ARTICLE 204
A prospective study in daily clinical practice
Feasibility and limitations of 2D speckle tracking echocardiography Lina Melzer, Anja Faeh-Gunz, Barbara Naegeli, Burkhardt Seifert*, Monica Pfyffer, Christine H. Attenhofer Jost
From the Cardiovascular Centre Zürich, Klinik Im Park, Department of Biostatistics, Epidemiology, Biostatistics and Prevention Institute, University of Zurich*, Zürich, Switzerland
Abstract
Introduction: Two-dimensional speckle tracking echocardiography (2DSTE)
has been recommended as a helpful tool for assessing cardiac function. A
mean global longitudinal strain (GLS) value of >18% has been one of the
recommended normal cut-off limits. Little is known about the perfor-
mance of GLS and its impact in daily practice.
Method: Between October 2013 and January 2014, in 482 consecutive pa-
tients undergoing transthoracic echocardiography, 2DSTE was attempted
from the three apical views (resulting in mean GLS values). Diagnoses,
echocardiographic findings and image quality were collected. All studies
were done with the GE Vingmed System E9 (AFI algorithm) and analysed
during the study or offline for interobserver variability.
Results: In 447 patients (93%), 2DSTE was feasible. The most important re-
asons for inability to do 2DSTE identified were poor echocardiographic
image quality, atrial fibrillation and/or a higher body mass index (all
p <0.001). Interobserver variability was acceptable with an intraclass cor-
relation coeffici ent of 0.952 (95% confidence interval 0.919–0.972). Of
those patients in whom 2DSTE was feasible, mean ejection fraction was 58
± 10%; regional wall motion abnormalities were present in 139 patients
(31%) and left ventricular hypertrophy in 78 (17%). Mean GLS was 17.4 ±
4.6% (in excellent image quality 18.9 ± 3.2% versus 16.4 ± 4.5% in poor
image quality; p = 0.006). A GLS of less than 18% was present in 211
(47.2%) and less than 16% in 124 patients (27.7%). In 136 patients (30.4%)
GLS imaging identified abnormal left ventricular myocardial segments not
explained by scarring or left ventricular hypertrophy.
Conclusion: Assessment of GLS by 2DSTE is feasible in most and depend-
ent on image quality, body mass index and atrial fibrillation. Reproducibil-
ity is high with acceptable intra- and interobserver variability. GLS
provid es additional information, however, often showing nonspecific ab-
normalities. Using only a cut-off value of >18% may not be reasonable as
an average number does not reflect regional abnormalities. Thus for eve-
ryday practice average GLS should be provided routinely supplemented
by information on abnormal segments.
Key words: speckle tracking; echocardiography; feasibility; two-dimensional; global longitudinal strain;
introduction
Two-dimensional speckle tracking echocardiography (2DSTE) has been recommended as a helpful tool for quantifying left ventricular (LV) function and for prog-nosis [1–3]. By angle-independent tracking of small myo cardial features frame to frame within grayscale B-mo de images, local displacement is used to measure myocardial deformation (strain), strain rate and myo-cardial velocities, in any direction within the image plane [4]. This new method has been validated against sonomicrometry [4, 5], tagged magnetic resonance imaging [6] and clinically against Doppler tissue imag-ing (DTI) [7]. Using the 16- to 18-segment bullseye map, regional as well as global average strain can be evaluated [1]. Longi-tudinal strain, especially global longitudinal strain (GLS), has shown excellent reproducibility [8, 9]. GLS has been recommended for diagnosis of coronary artery disease and myocardial ischaemia, especially in combination with wall motion score index [10, 11], to evaluate prognosis in patients with heart failure [12–14], to diagnose amyloid heart disease [15] and to assess myocardial function in patients with diabetes [16], var-ious cardiomyopathies including hypertrophic cardio-myopathy, valvular heart disease [17, 18], or congenital heart disease [8, 19].Even though a GLS value of >19.7% was considered a normal value in a recent meta-analysis [20], a GLS value of >16–18% has been recommended as the cut-off limit for normal versus abnormal [21, 22]. However, there is no official cut-off recommended in the recently published guidelines [23]. Little is known about the feasi bility, impact and reproducibility of 2DSTE in daily practice [24]. The aim of this study was to evaluate feasibility and intra- and interobserver variability of 2DSTE in daily practice in consecutive patients, to analyse its clinical impact when used by experienced physicians in their daily work with patients, and to identify reasonable and advisable cutoffs of average GLS for routine prac-tice.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):204–210

ORIGINAL ARTICLE 205
Methods
Study populationAll consecutive patients undergoing standard trans-thoracic echocardiography at the Cardiovascular Cen-tre Zürich, Klinik Im Park, Zürich, Switzerland, between 1 October 2013 and 31 January 2014 were included in this study. There were 482 patients, and every patient was included only once, even if they were examined several times (in which case, only the last study was included). Demographic and clinical characteristics including age and gender, clinical parameters such as body mass in-dex (BMI), cardiovascular risk factors (arterial hyper-tension, coronary artery disease and diabetes) and additional information (rhythm, bundle-branch block, pacemaker rhythm) were acquired from the patient’s medical record. The study was approved by the local ethics committee and patient consent forms were present according to its guidelines.
Echocardiographic image acquisitionEchocardiographic parametersStandard transthoracic echocardiography was per-formed on all patients at rest in the supine position, according to guidelines [25]. Left ventricular end-diastol ic diameter, end-diastolic volume, end-systolic diameter, shortening fraction, muscle mass index and ejection fraction, regional wall motion and diastolic function were measured and assessed as recom-mended by the European Association of Echocardio-graphy [25–27]. Pulmonary hypertension was defined as an estimated systolic right ventricular pressure of ≥36 mm Hg and measured as previously recommended [28].
Acquisition of myocardial strain imagesIn addition, 2DSTE was attempted from the three apical views, resulting in average GLS values. The frame rate was at least 50 frames per second as recommended [29]. GLS, which analyses myocardial deformation (rel-ative length change of the LV myocardium between end-diastole and end-systole), was evaluated using the three apical views (apical long axis, apical two-cham-ber and apical four-chamber view). GLS was calculated by averag ing the peak strain values of the 18 segments [30]. The semi-automatic AFI algorithm (Automated Function Imaging, GE Healthcare, Horten, Norway) was used.All diagnoses, echocardiographic parameters and image quality (excellent, average, poor) were prospec-tively collected and analysed.
If two or more of the 18 segments could not be ana-lysed, GLS was defined as not feasible. All studies were done with the GE Vingmed System E9 4D BT12 and ana-lysed during the study (or offline for inter- and intra-observer reliability on the Echopac system).
Analysis of additional information of myocardial strain imagesIn all patients, the findings of speckle tracking imaging were analysed in addition to the normal analysis of standard 2D and Doppler echocardiographic images. If speckle tracking gave possible additional diagnostic information defined as at least two myocardial seg-ments with <14% on speckle tracking and no other explanation (scar, hypertrophy), this was indicated as new diagnostic information such as described for Fabry disease by Morris [31], changes of speckle track-ing compatible with cardiac amyloidosis as described by Liu [32] and/or changes of speckle tracking indicat-ing possible dyssynchrony [33].
Reproducibility of 2D speckle tracking echocardiographic study dataIn order to assess intraobserver variability, 2DSTEs and measurements of GLS were repeated in 54 randomly selected subjects. For interobserver variability, 2D strain was analysed in 60 patients by a second experi-enced obser ver who was unaware of the results of the first observer. These 60 patients were selected to be a balanced sample representative of the three classes of image quality.
Statistical analysisContinuous data are expressed as means and standard deviations, nominal data as frequencies with percent-ages. Results are displayed in tables or as correlation plots in the figures. Student’s t test was used to com-pare continuous data. A p-values of <0.05 was consid-ered statistically significant. Inter- and intraobserver reliability was assessed using intraclass correlation coeffici ent (ICC) in a two-way mixed model (absolute agreement). The confidence interval (CI) was indicated where necessary. Categorical data are compared using the chi-square test or Fisher’s exact test as appropriate. With stepwise linear regression analysis, image qual-ity, coronary artery disease, hypertension, diabetes, presence of scar, presence of left ventricular hyper-trophy, ejection fraction, systolic blood pressure, heart rate and BMI were included in a stepwise manner, to see if the influence of these para meters on GLS re-mains an independent predictor of GLS (441 patients). The correlation of GLS with ejection fraction was calcu-lated.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):204–210
ORIGINAL ARTICLE 206
Statistical analysis was performed using IBM SPSS Statis tics, version 22 (IBM Corp., Armonk, NY, USA).
Results
It was possible to do 2DSTE in 447 cases (92.7%). The most important reasons for inability to do 2DSTE in 35 patients (7.3%) were higher BMI (17 pa tients), poor image quality (14 patients, 7 of whom were obese), and/or atrial fibrillation (11 patients). In 56% of patients with poor echoquality, GLS could not be done. In 23 of the 447 patients (5%), one or two myocardial segments could not be analysed.
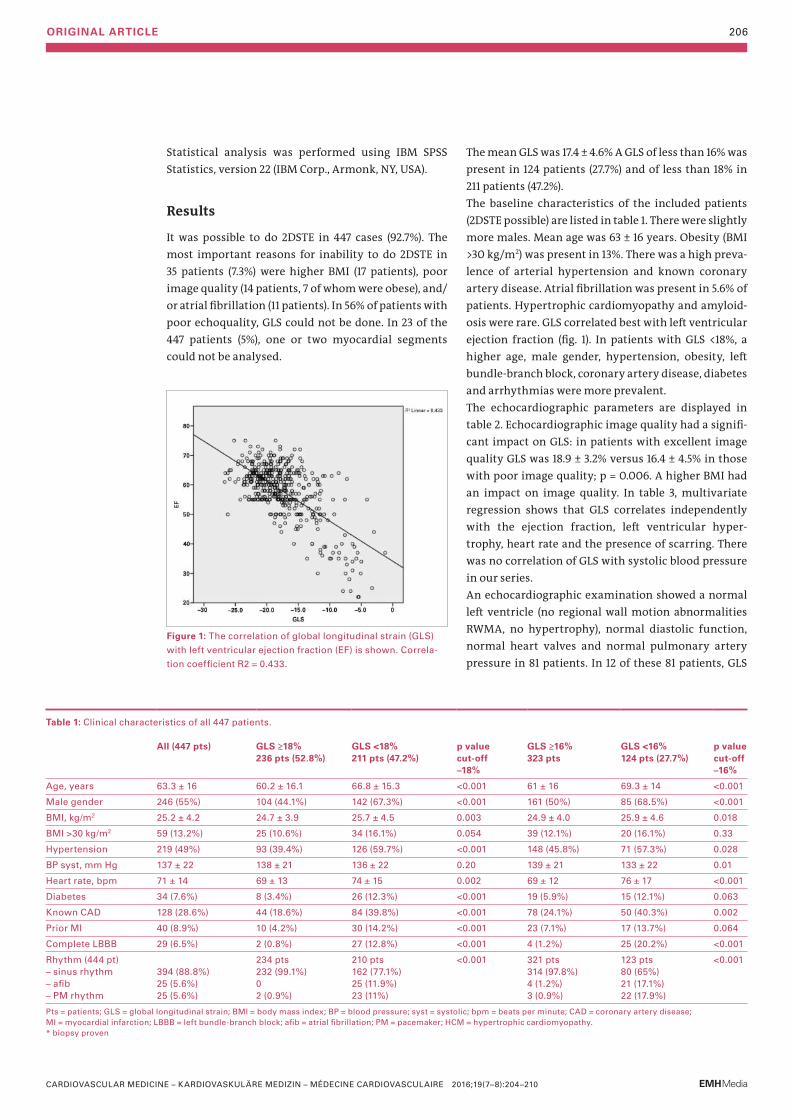
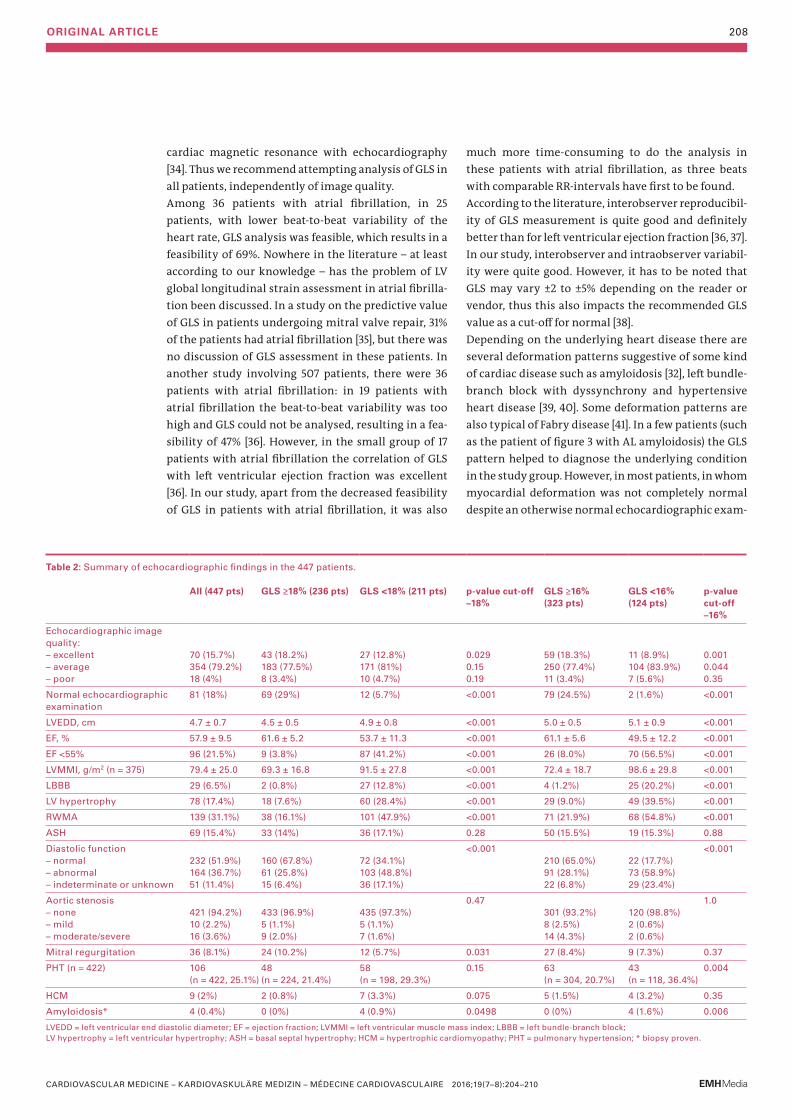
The mean GLS was 17.4 ± 4.6% A GLS of less than 16% was present in 124 patients (27.7%) and of less than 18% in 211 patients (47.2%). The baseline characteristics of the included patients (2DSTE possible) are listed in table 1. There were slightly more males. Mean age was 63 ± 16 years. Obesity (BMI >30 kg/m2) was present in 13%. There was a high preva-lence of arterial hypertension and known coronary artery disease. Atrial fibrillation was present in 5.6% of patients. Hypertrophic cardiomyopathy and amyloid-osis were rare. GLS correlated best with left ventricular ejection fraction (fig. 1). In patients with GLS <18%, a higher age, male gender, hypertension, obesity, left bundle-branch block, coronary artery disease, diabetes and arrhythmias were more prevalent.The echocardiographic parameters are displayed in tabl e 2. Echocardiographic image quality had a signifi-cant impact on GLS: in patients with excellent image quality GLS was 18.9 ± 3.2% versus 16.4 ± 4.5% in those with poor image quality; p = 0.006. A higher BMI had an impact on image quality. In table 3, multivariate regression shows that GLS correlates in dependently with the ejection fraction, left ventricular hyper-trophy, heart rate and the presence of scarring. There was no correlation of GLS with systolic blood pressure in our series.An echocardiographic examination showed a normal left ven tricle (no regional wall motion abnormalities RWMA, no hypertrophy), normal diastolic function, normal heart valves and normal pulmonary artery pressure in 81 patients. In 12 of these 81 patients, GLS
Table 1: Clinical characteristics of all 447 patients.
All (447 pts) GLS ≥18% 236 pts (52.8%)
GLS <18% 211 pts (47.2%)
p value cut-off –18%
GLS ≥16% 323 pts
GLS <16% 124 pts (27.7%)
p valuecut-off–16%
Age, years 63.3 ± 16 60.2 ± 16.1 66.8 ± 15.3 <0.001 61 ± 16 69.3 ± 14 <0.001
Male gender 246 (55%) 104 (44.1%) 142 (67.3%) <0.001 161 (50%) 85 (68.5%) <0.001
BMI, kg/m2 25.2 ± 4.2 24.7 ± 3.9 25.7 ± 4.5 0.003 24.9 ± 4.0 25.9 ± 4.6 0.018
BMI >30 kg/m2 59 (13.2%) 25 (10.6%) 34 (16.1%) 0.054 39 (12.1%) 20 (16.1%) 0.33
Hypertension 219 (49%) 93 (39.4%) 126 (59.7%) <0.001 148 (45.8%) 71 (57.3%) 0.028
BP syst, mm Hg 137 ± 22 138 ± 21 136 ± 22 0.20 139 ± 21 133 ± 22 0.01
Heart rate, bpm 71 ± 14 69 ± 13 74 ± 15 0.002 69 ± 12 76 ± 17 <0.001
Diabetes 34 (7.6%) 8 (3.4%) 26 (12.3%) <0.001 19 (5.9%) 15 (12.1%) 0.063
Known CAD 128 (28.6%) 44 (18.6%) 84 (39.8%) <0.001 78 (24.1%) 50 (40.3%) 0.002
Prior MI 40 (8.9%) 10 (4.2%) 30 (14.2%) <0.001 23 (7.1%) 17 (13.7%) 0.064
Complete LBBB 29 (6.5%) 2 (0.8%) 27 (12.8%) <0.001 4 (1.2%) 25 (20.2%) <0.001
Rhythm (444 pt) – sinus rhythm– afib– PM rhythm
394 (88.8%) 25 (5.6%) 25 (5.6%)
234 pts 232 (99.1%) 0 2 (0.9%)
210 pts 162 (77.1%) 25 (11.9%) 23 (11%)
<0.001 321 pts 314 (97.8%)4 (1.2%)3 (0.9%)
123 pts 80 (65%) 21 (17.1%) 22 (17.9%)
<0.001
Pts = patients; GLS = global longitudinal strain; BMI = body mass index; BP = blood pressure; syst = systolic; bpm = beats per minute; CAD = coronary artery disease; MI = myocardial infarction; LBBB = left bundle-branch block; afib = atrial fibrillation; PM = pacemaker; HCM = hypertrophic cardiomyopathy.* biopsy proven
Figure 1: The correlation of global longitudinal strain (GLS)
with left ventricular ejection fraction (EF) is shown. Correla-
tion coefficient R2 = 0.433.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):204–210

ORIGINAL ARTICLE 207
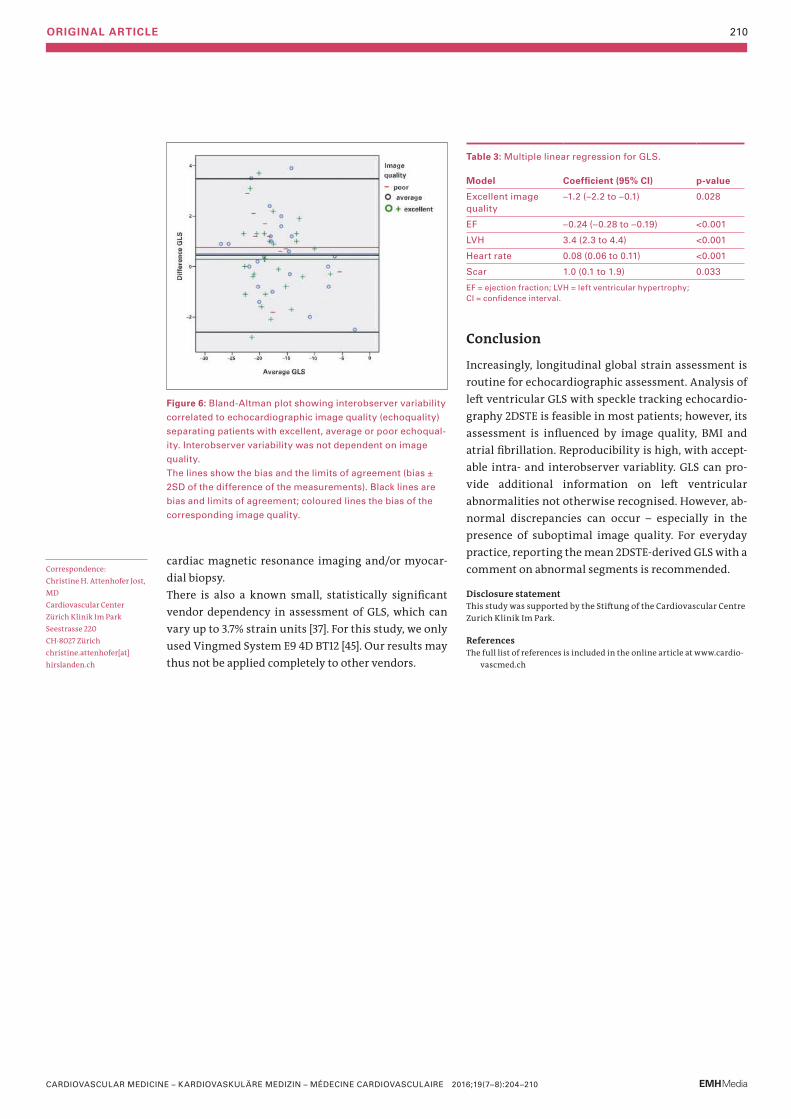
was <18% (15%); these patients were significantly older (p <0.001), they had significantly more often hyperten-sion (p = 0.0002) and coronary artery disease (p = 0.02); however, there was no correlation with obesity, gender, or diabetes in this patient group. In the whole patient group, mean ejection fraction was 58 ± 10%; regional wall motion abnormalities were present in 139 patients (31%), left ventricular hypertrophy in 78 patients (17%), hypertrophy of the basal septum in 15%, and abnormal diastolic function in 164 of 396 patients (41%). Exam-ples of individual patients are shown in figures 2 to 5.In 136 patients (30.4%), GLS provided additional infor-mation such as signs for abnormal myocardial regions (126 patients) including patients with segmental wall abnormalities of unknown aetiology and/or possible dyssynchrony, or indirect signs for possible amyloid-osis (10 patients), which so far has been confirmed by myocardial biopsy in four of these patients.Interobserver variability was 0.952 (95% CI 0.919–0.972) and no correlation with echocardiographic quality could be seen (fig. 6). Intraobserver variability for GLS was 0.92 (95% CI 0.861–0.952).
Discussion
Assessment of GLS with 2DSTE is feasible in most patients. Feasibility is critically dependent on image quality, BMI and the presence of atrial fibrillation. Re-producibility is good, with acceptable intra- and inter-observer variablity, and not dependent on image qual-ity. To use any cut-off may not be reasonable as decreased values can be observed in normal hearts due to diminished image quality and abnormal segments can be present even in hearts with a rather high and thus “normal” GLS. In some patients with otherwise normal echocardiographic findings, GLS may identify subtle myocardial changes not identifiable otherwise. We are convinced that GLS provides useful additional information and should be integrated into routine practice.
Feasibility and reproducibilityFeasibility of GLS in our patient group was excellent, at 92.7%. We could also confirm the fair correlation of GLS with left ventricular ejection fraction as previously reported. However, in patients with increased body weight, diminished echocardiographic image quality and atrial fibrillation with a high beat-to-beat heart rate variability, feasibility was diminished. Surpris-ingly, in patients with a limited acoustic window, assessment of longitudinal strain by speckle tracking may be more accurate than assessment of left ventric-ular ejection fraction, as seen in a study comparing
Figure 2: A 60-year-old patient with a previous large anterior myocardial infarction. She
has no left bundle-branch block. Her left ventricular ejection fraction was 43%, the left
ventricular volume index 83 ml/m2 body surface area, but her GLS was severely dimin-
ished at –7.3%, better reflecting more left ventricular impairment than the ejection frac-
tion suggests. Because of apical aneurysm and thus diminished echoquality, two
segments could not be assessed (x).
Figure 3: A 54-year-old patient who presented with dyspnoea on exertion. Biplane left
ventricular ejection fraction was 63%, and he had diastolic dysfunction and increased
left ventricular wall thickness up to 13 mm. His GLS was –9.7% with a pattern sugges-
tive of amyloid heart disease. Further evaluation was performed and revealed AL amy-
loidosis.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):204–210
ORIGINAL ARTICLE 208
much more time-consuming to do the analysis in these patients with atrial fibrillation, as three beats with comparable RR-intervals have first to be found.According to the literature, interobserver reproducibil-ity of GLS measurement is quite good and definitely better than for left ventricular ejection fraction [36, 37]. In our study, interobserver and intraobserver variabil-ity were quite good. However, it has to be noted that GLS may vary ±2 to ±5% depending on the reader or vendor, thus this also impacts the recommended GLS value as a cut-off for normal [38].Depending on the underlying heart disease there are several deformation patterns suggestive of some kind of cardiac disease such as amyloidosis [32], left bundle-branch block with dyssynchrony and hypertensive heart disease [39, 40]. Some deformation patterns are also typical of Fabry disease [41]. In a few patients (such as the patient of figure 3 with AL amyloidosis) the GLS pattern helped to diagnose the underlying condition in the study group. However, in most patients, in whom myocardial deformation was not completely normal despite an otherwise normal echocardiographic exam-
Table 2: Summary of echocardiographic findings in the 447 patients.
All (447 pts) GLS ≥18% (236 pts) GLS <18% (211 pts) p-value cut-off–18%
GLS ≥16%(323 pts)
GLS <16% (124 pts)
p-value cut-off–16%
Echocardiographic image quali ty: – excellent – average – poor
70 (15.7%) 354 (79.2%) 18 (4%)
43 (18.2%)183 (77.5%)8 (3.4%)
27 (12.8%) 171 (81%) 10 (4.7%)
0.0290.150.19
59 (18.3%)250 (77.4%)11 (3.4%)
11 (8.9%) 104 (83.9%) 7 (5.6%)
0.0010.0440.35
Normal echocardiographic examination
81 (18%) 69 (29%) 12 (5.7%) <0.001 79 (24.5%) 2 (1.6%) <0.001
LVEDD, cm 4.7 ± 0.7 4.5 ± 0.5 4.9 ± 0.8 <0.001 5.0 ± 0.5 5.1 ± 0.9 <0.001
EF, % 57.9 ± 9.5 61.6 ± 5.2 53.7 ± 11.3 <0.001 61.1 ± 5.6 49.5 ± 12.2 <0.001
EF <55% 96 (21.5%) 9 (3.8%) 87 (41.2%) <0.001 26 (8.0%) 70 (56.5%) <0.001
LVMMI, g/m2 (n = 375) 79.4 ± 25.0 69.3 ± 16.8 91.5 ± 27.8 <0.001 72.4 ± 18.7 98.6 ± 29.8 <0.001
LBBB 29 (6.5%) 2 (0.8%) 27 (12.8%) <0.001 4 (1.2%) 25 (20.2%) <0.001
LV hypertrophy 78 (17.4%) 18 (7.6%) 60 (28.4%) <0.001 29 (9.0%) 49 (39.5%) <0.001
RWMA 139 (31.1%) 38 (16.1%) 101 (47.9%) <0.001 71 (21.9%) 68 (54.8%) <0.001
ASH 69 (15.4%) 33 (14%) 36 (17.1%) 0.28 50 (15.5%) 19 (15.3%) 0.88
Diastolic function – normal – abnormal – indeterminate or unknown
232 (51.9%)164 (36.7%)51 (11.4%)
160 (67.8%)61 (25.8%)15 (6.4%)
72 (34.1%)103 (48.8%)36 (17.1%)
<0.001210 (65.0%)91 (28.1%)22 (6.8%)
22 (17.7%)73 (58.9%)29 (23.4%)
<0.001
Aortic stenosis – none – mild – moderate/severe
421 (94.2%) 10 (2.2%) 16 (3.6%)
433 (96.9%) 5 (1.1%) 9 (2.0%)
435 (97.3%) 5 (1.1%) 7 (1.6%)
0.47301 (93.2%)8 (2.5%)14 (4.3%)
120 (98.8%) 2 (0.6%) 2 (0.6%)
1.0
Mitral regurgitation 36 (8.1%) 24 (10.2%) 12 (5.7%) 0.031 27 (8.4%) 9 (7.3%) 0.37
PHT (n = 422) 106 (n = 422, 25.1%)
48 (n = 224, 21.4%)
58 (n = 198, 29.3%)
0.15 63 (n = 304, 20.7%)
43 (n = 118, 36.4%)
0.004
HCM 9 (2%) 2 (0.8%) 7 (3.3%) 0.075 5 (1.5%) 4 (3.2%) 0.35
Amyloidosis* 4 (0.4%) 0 (0%) 4 (0.9%) 0.0498 0 (0%) 4 (1.6%) 0.006
LVEDD = left ventricular end diastolic diameter; EF = ejection fraction; LVMMI = left ventricular muscle mass index; LBBB = left bundle-branch block; LV hypertrophy = left ventricular hypertrophy; ASH = basal septal hypertrophy; HCM = hypertrophic cardiomyopathy; PHT = pulmonary hypertension; * biopsy proven.
cardiac magnetic resonance with echocardiography [34]. Thus we recommend attempting analysis of GLS in all patients, independently of image quality.Among 36 patients with atrial fibrillation, in 25 pa tients, with lower beat-to-beat variability of the heart rate, GLS analysis was feasible, which results in a feasibility of 69%. Nowhere in the literature – at least according to our knowledge – has the problem of LV global longitudinal strain assessment in atrial fibrilla-tion been discussed. In a study on the predictive value of GLS in patients undergoing mitral valve repair, 31% of the patients had atrial fibrillation [35], but there was no discussion of GLS assessment in these patients. In another study involving 507 patients, there were 36 patients with atrial fibrillation: in 19 patients with atrial fibrillation the beat-to-beat variability was too high and GLS could not be analysed, resulting in a fea-sibility of 47% [36]. However, in the small group of 17 patients with atrial fibrillation the correlation of GLS with left ventricular ejection fraction was excellent [36]. In our study, apart from the decreased feasibility of GLS in patients with atrial fibrillation, it was also
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):204–210

ORIGINAL ARTICLE 209
ination, it remained unclear what cardiac disease could cause the abnormality. Arterial hypertension was common in our study group, and in mild hyper-tensive heart disease abnormal speckle tracking with reduced myocardial velocities can occur early in the disease prior to other visible changes [42]. We have no correlation with findings of gadolinium enhancement of cardiac magnetic resonance imaging in this study group to prove or exclude, for example, underlying myocardial fibrosis. We also did not have any genetic testing performed in these patien ts to rule out,for ex-ample, occult hypertrophic cardio myopathy, neuro-muscular disease or Fabry disease. It is known that strain patterns in genotype-positive patients with hyper trophic cardiomyopathy can be abnormal [43] prior to echocardiographic changes. In the 81 patients with a completely normal echocardiographic exami-nation, 5.7% had a GLS value of less than 18% and 1.6% a GLS value of less than 16%. So cut-off values might not be reasonable for every-day practice. Fourteen patients with a seemingly normal echocardiographic examina-tion had a history of hypertension, coronary artery disease and/or diabetes; only two of these had a GLS of less than 18%, at 17.7% and 16.8%.
LimitationsDuring the study period, we did not routinely perform three-dimensional strain imaging in our routine prac-tice, therefore these data apply only for two-dimen-sional strain imaging. Two-dimensional speckle track-ing echocardiography (2DSTE) is limited as it does not track tissue motion in three dimensions; however, feasi bility may be higher in two-dimensional speckle tracking than three-dimensional speckle tracking althou gh three-dimensional speckle tracking might be less time-consuming and more exact [44]. Our data do not apply for three-dimensional strain imaging.Image quality was graded prospectively during the echocardiographic examination as excellent, average or poor. Most examinations were classified at that time as “average”, therefore the range of “average” is wider as the goal was not to make three groups of compara-ble size. This may have an impact on the results as the influence of diminished image quality might be under-estimated.Currently, there are no clear guidelines how to further evaluate patients in whom speckle tracking imaging identifies abnormal myocardial segments not explain ed by the conventional echocardiographic fin-dings, with the exception of patients in whom a pat-tern typical for cardiac amyloidosis is found where we usually recommend further evaluation including
Figure 4: A14-year-old patient with severe hypertrophic cardiomyopathy and dyspnoea
NYHA II. The boy has a history of previous septal myectomy. His left ventricular ejection
fraction was preserved (55%), there was relaxation abnormality, his wall thickness mea-
sured up to 22 mm and his GLS-9.5%, with myocardial deformation being worst in the
whole septum and preserved in the anterolateral basal and middle wall segments.
Figure 5: A 43-year-old female patient with dilated cardiomyopathy, normal coronary
arteries and severely diminished left ventricular ejection fraction (22%). There is an al-
most diffusely abnormal myocardial deformation pattern apart from mid-anterior and
lateral segments. Mean GLS in this patient was –5.3%.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):204–210
ORIGINAL ARTICLE 210
Table 3: Multiple linear regression for GLS.
Model Coefficient (95% CI) p-value
Excellent image quality
–1.2 (–2.2 to –0.1) 0.028
EF –0.24 (–0.28 to –0.19) <0.001
LVH 3.4 (2.3 to 4.4) <0.001
Heart rate 0.08 (0.06 to 0.11) <0.001
Scar 1.0 (0.1 to 1.9) 0.033
EF = ejection fraction; LVH = left ventricular hypertrophy; CI = confidence interval.
Figure 6: Bland-Altman plot showing interobserver variability
correlated to echocardiographic image quality (echoquality)
separating patients with excellent, average or poor echoqual-
ity. Interobserver variability was not dependent on image
quality.
The lines show the bias and the limits of agreement (bias ±
2SD of the difference of the measurements). Black lines are
bias and limits of agreement; coloured lines the bias of the
corresponding image quality.
cardiac magnetic resonance imaging and/or myocar-dial biopsy.There is also a known small, statistically significant vendor dependency in assessment of GLS, which can vary up to 3.7% strain units [37]. For this study, we only used Vingmed System E9 4D BT12 [45]. Our results may thus not be applied completely to other vendors.
Conclusion
Increasingly, longitudinal global strain assessment is routine for echocardiographic assessment. Analysis of left ventricular GLS with speckle tracking echocardio-graphy 2DSTE is feasible in most patients; however, its assessment is influenced by image quality, BMI and atrial fibrillation. Reproducibility is high, with accept-able intra- and interobserver variablity. GLS can pro-vide additional information on left ventricular abnorm alities not otherwise recognised. However, ab-normal discrepancies can occur – especially in the presence of suboptimal image quality. For everyday practice, reporting the mean 2DSTE-derived GLS with a comment on abnormal segments is recommended.
Disclosure statement This study was supported by the Stiftung of the Cardiovascular Centre Zurich Klinik Im Park.
ReferencesThe full list of references is included in the online article at www.cardio-
vascmed.ch
Correspondence: Christine H. Attenhofer Jost, MD Cardiovascular Center Zürich Klinik Im Park Seestrasse 220 CH-8027 Zürich christine.attenhofer[at]hirslanden.ch
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):204–210
ORIGINAL ARTICLE 211
Feasibility and first results with a novel quality indicator for AMI mortality
New quality indicator for treatment of acute myocardial infarctionMilos Radosavaca, b, Raphael Twerenbolda, b, Max Wagenera, b, Ursina Honeggerb, Christian Puelachera, b, Karin Wildia, b, Tobias Reichlina, b, Philipp Kreutzingera, b, Fabio Stallonea, b, Petra Hillingera, b, Cedric Jaegera, b, Maria Rubini Gimeneza, b, Samyut Shresthaa, b, Michael Hebererc, Michael Kuehnea, b, Stefan Osswalda, b, Christian Muellera, b
University Hospital Basel, Switzerlanda Department of Cardiology; b Cardiovascular Research Institute Basel (CRIB); c Department for Quality Management
Introduction
Quality indicators (QIs) play a central role in the evalu-ation of healthcare provided in hospitals [1]. Since the introduction of the diagnosis-related group (DRG) class ification system (SwissDRG in Switzerland), gov-ernmental agencies and health insurers, as well as the press, increasingly focus on QIs in order to assess, com-pare and comment on the cost-effectiveness and stand-ard of care provided by healthcare providers. In Switzerland, the performance of care providers is assessed and compared using a catalogue called Swiss Inpatient Quality Indicators (CH-IQI) [2]. In most cen-tres of care, these data are acquired routinely and on an automated basis in order to maintain a cost-effec-tive way of evaluation. The results are published every year for the public. Crude in-hospital mortality, adjusted by age and gen-der, and in certain cases the Charlson comorbidity index are currently used to assess quality of care in acute myocardial infarction (AMI) [3–5]. Unfortunately, this approach has multiple shortcomings: for example, the local case mix for certain diseases can vary widely between centres of care, either because of their regional status as a central hub for interventional and intensive care, or because of the quality of life in a cer-tain region [6]. Therefore, for acute diseases including AMI, risk adjustment solely based on gender and age seems incomplete, as variables including vital signs at presen tation outperform by far age and gender in the predic tion of in-hospital death [7–9]. Appropriate risk adjust ment for these variables would seem mandatory, but has until now not been implemented.Our aim was to explore the feasibility of a novel approach that uses the Global Registry of Acute Coro-nary Events (GRACE) risk score, an internationally vali-dated [10–12] and accepted [13, 14] tool for risk adjust-ment and estimation of in-hospital mortality, as a QI for treatment of AMI.
Summary
Introduction: Crude mortality is commonly used as a quality indicator (QI)
for the treatment of acute myocardial infarction (AMI), but has important
limitations including its dependence on the local case-mix. We aimed to
explore the feasibility of a novel approach using risk adjustment according
to the Global Registry of Acute Coronary Events (GRACE).
Methods: In 1471 consecutive patients admitted with AMI to a Swiss uni-
versity hospital in 2012 and 2013, we quantified working hours needed by
a trained healthcare professional to complement the available administra-
tive dataset by detailed medical review of all available medical records to:
1) differentiate the subtypes of AMI in order to separate type 1 (including
type 4) AMIs from type 2 and postoperative AMIs (GRACE is only validated
for type 1 AMI); 2) add all medical variables required to calculate the
GRACE score.
Results: Detailed medical review identified 93 additional patients (6.7%)
with AMI as the main diagnosis, who were missed in the administrative
dataset. Complete data for the calculation of the GRACE score could be
obtained for 1233 patients (93.8%). In both years, observed crude mortal-
ity was significantly lower than the expected in-hospital mortality using
the GRACE model (2012 [n = 613]: crude mortality 6.0%, mean GRACE mor-
tality 8.3% [95% CI 7.2–9.4%]; 2013 [n = 620]: crude mortality 5.8%, mean
GRACE mortality 9.4% [95%CI 8.3–10.6%]). Overall, the number of working
hours required to retrospectively complement the administrative dataset
was 1150 hours (575 h per year).
Conclusion: Assessment of risk-adjusted in-hospital mortality in AMI is
feasible, provides important insights regarding treatment results while
improving comparability between hospitals, but is very time-consuming
if done retrospectively. Prospective documentation of the GRACE score
within the electronic medical records would help to reduce the effort
needed to obtain this novel QI. Further multicentre studies are warranted.
Key words: quality indicators; outcome; mortality; myocardial infarction
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):211–216
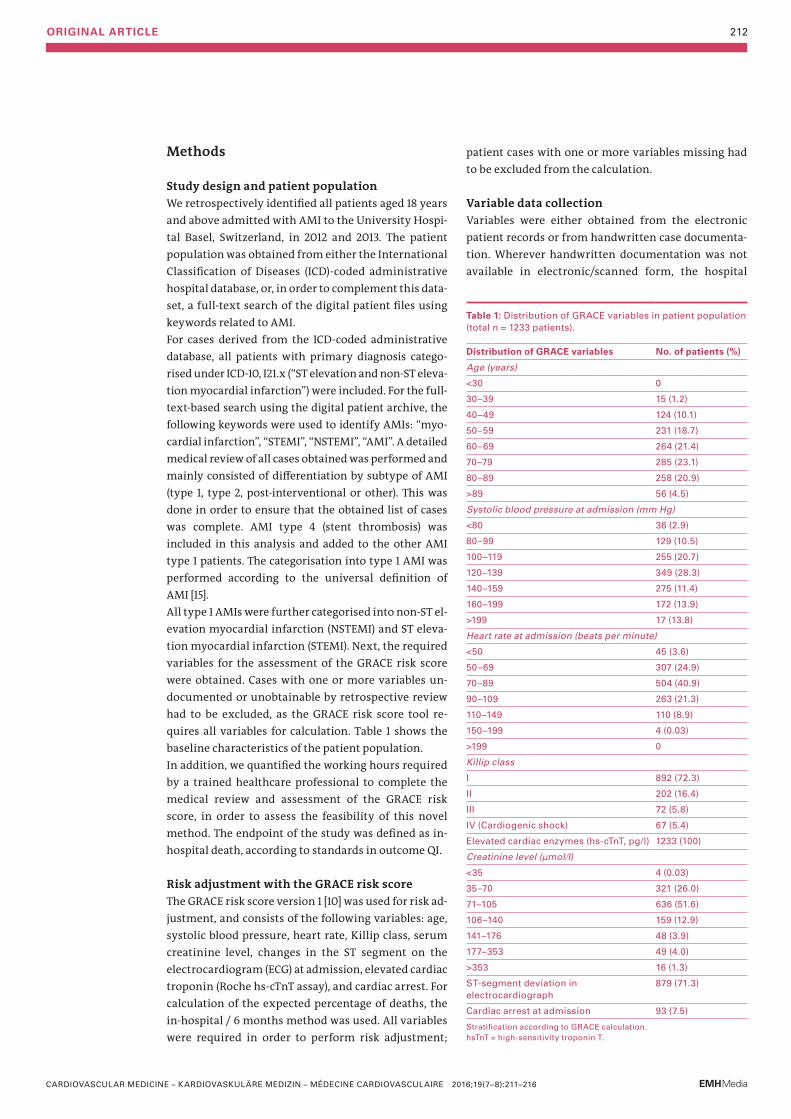
ORIGINAL ARTICLE 212
Methods
Study design and patient populationWe retrospectively identified all patients aged 18 years and above admitted with AMI to the University Hospi-tal Basel, Switzerland, in 2012 and 2013. The patient population was obtained from either the International Classification of Diseases (ICD)-coded administrative hospital database, or, in order to complement this data-set, a full-text search of the digital patient files using keywords related to AMI.For cases derived from the ICD-coded administrative database, all patients with primary diagnosis catego-rised under ICD-10, I21.x (“ST elevation and non-ST eleva-tion myocardial infarction”) were included. For the full- text-based search using the digital patient archive, the following keywords were used to identify AMIs: “myo-cardial infarction”, “STEMI”, “NSTEMI”, “AMI”. A detailed medical review of all cases obtained was performed and mainly consisted of differentiation by subtype of AMI (type 1, type 2, post-interventional or other). This was done in order to ensure that the obtained list of cases was complete. AMI type 4 (stent thrombosis) was included in this analysis and added to the other AMI type 1 patients. The categorisation into type 1 AMI was performed according to the universal definition of AMI [15]. All type 1 AMIs were further categorised into non-ST el-evation myocardial infarction (NSTEMI) and ST eleva-tion myocardial infarction (STEMI). Next, the required variables for the assessment of the GRACE risk score were obtained. Cases with one or more variables un-documented or unobtainable by retrospective review had to be excluded, as the GRACE risk score tool re-quires all variables for calculation. Table 1 shows the baseline characteristics of the patient population.In addition, we quantified the working hours required by a trained healthcare professional to complete the medical review and assessment of the GRACE risk score, in order to assess the feasibility of this novel method. The endpoint of the study was defined as in-hospital death, according to standards in outcome QI.
Risk adjustment with the GRACE risk scoreThe GRACE risk score version 1 [10] was used for risk ad-justment, and consists of the following variables: age, systolic blood pressure, heart rate, Killip class, serum creatinine level, changes in the ST segment on the electro cardiogram (ECG) at admission, elevated cardiac troponin (Roche hs-cTnT assay), and cardiac arrest. For calculation of the expected percentage of deaths, the in-hospital / 6 months method was used. All variables were required in order to perform risk adjustment;
patien t cases with one or more variables missing had to be excluded from the calculation.
Variable data collection Variables were either obtained from the electronic patien t records or from handwritten case documenta-tion. Wherever handwritten documentation was not available in electronic/scanned form, the hospital
Table 1: Distribution of GRACE variables in patient population (total n = 1233 patients).
Distribution of GRACE variables No. of patients (%)
Age (years)
<30 0
30–39 15 (1.2)
40–49 124 (10.1)
50–59 231 (18.7)
60–69 264 (21.4)
70–79 285 (23.1)
80–89 258 (20.9)
>89 56 (4.5)
Systolic blood pressure at admission (mm Hg)
<80 36 (2.9)
80–99 129 (10.5)
100–119 255 (20.7)
120–139 349 (28.3)
140–159 275 (11.4)
160–199 172 (13.9)
>199 17 (13.8)
Heart rate at admission (beats per minute)
<50 45 (3.6)
50–69 307 (24.9)
70–89 504 (40.9)
90–109 263 (21.3)
110–149 110 (8.9)
150–199 4 (0.03)
>199 0
Killip class
I 892 (72.3)
II 202 (16.4)
III 72 (5.8)
IV (Cardiogenic shock) 67 (5.4)
Elevated cardiac enzymes (hs-cTnT, pg/l) 1233 (100)
Creatinine level (µmol/l)
<35 4 (0.03)
35–70 321 (26.0)
71–105 636 (51.6)
106–140 159 (12.9)
141–176 48 (3.9)
177–353 49 (4.0)
>353 16 (1.3)
ST-segment deviation in electrocardiograph
879 (71.3)
Cardiac arrest at admission 93 (7.5)
Stratification according to GRACE calculation. hsTnT = high-sensitivity troponin T.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):211–216
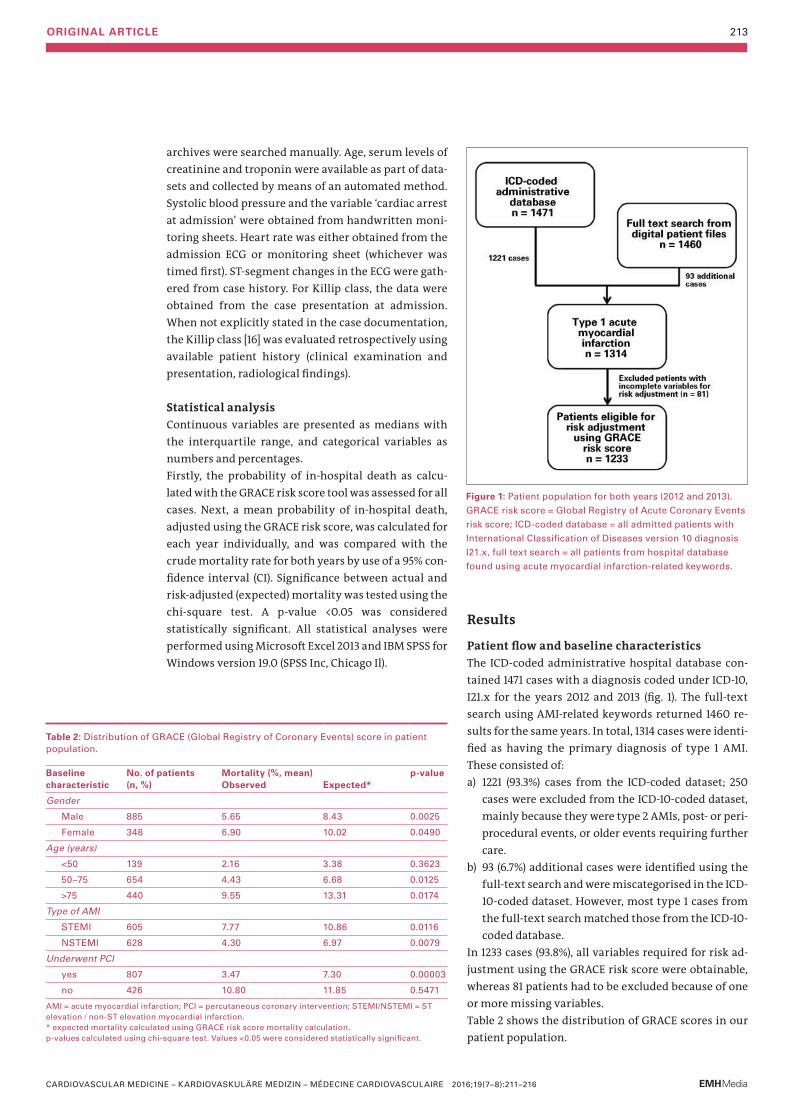
ORIGINAL ARTICLE 213
archives were searched manually. Age, serum levels of creatinine and troponin were available as part of data-sets and collected by means of an automated method. Systolic blood pressure and the variable ‘cardiac arrest at admission’ were obtained from handwritten moni-toring sheets. Heart rate was either obtained from the admission ECG or monitoring sheet (whichever was timed first). ST-segment changes in the ECG were gath-ered from case history. For Killip class, the data were obtained from the case presentation at admission. When not explicitly stated in the case documentation, the Killip class [16] was evaluated retrospectively using available patient history (clinical examination and presentation, radiological findings).
Statistical analysis Continuous variables are presented as medians with the interquartile range, and categorical variables as numbers and percentages.Firstly, the probability of in-hospital death as calcu-lated with the GRACE risk score tool was assessed for all cases. Next, a mean probability of in-hospital death, adjusted using the GRACE risk score, was calculated for each year individually, and was compared with the crude mortality rate for both years by use of a 95% con-fidence interval (CI). Significance between actual and risk-adjusted (expected) mortality was tested using the chi-square test. A p-value <0.05 was considered statistic ally significant. All statistical analyses were performed using Microsoft Excel 2013 and IBM SPSS for Windows version 19.0 (SPSS Inc, Chicago Il).
Results
Patient flow and baseline characteristics The ICD-coded administrative hospital database con-tained 1471 cases with a diagnosis coded under ICD-10, I21.x for the years 2012 and 2013 (fig. 1). The full-text search using AMI-related keywords returned 1460 re-sults for the same years. In total, 1314 cases were identi-fied as having the primary diagnosis of type 1 AMI. These consisted of:a) 1221 (93.3%) cases from the ICD-coded dataset; 250
cases were excluded from the ICD-10-coded dataset, mainly because they were type 2 AMIs, post- or peri-procedural events, or older events requiring further care.
b) 93 (6.7%) additional cases were identified using the full-text search and were miscategorised in the ICD-10-coded dataset. However, most type 1 cases from the full-text search matched those from the ICD-10-coded database.
In 1233 cases (93.8%), all variables required for risk ad-justment using the GRACE risk score were obtainable, whereas 81 patients had to be excluded because of one or more missing variables.Table 2 shows the distribution of GRACE scores in our patient population.
Figure 1: Patient population for both years (2012 and 2013).
GRACE risk score = Global Registry of Acute Coronary Events
risk score; ICD-coded database = all admitted patients with
International Classification of Diseases version 10 diagnosis
I21.x, full text search = all patients from hospital database
found using acute myocardial infarction-related keywords.
Table 2: Distribution of GRACE (Global Registry of Coronary Events) score in patient population.
Baseline characteristic
No. of patients (n, %)
Mortality (%, mean) Observed
Expected*
p-value
Gender
Male 885 5.65 8.43 0.0025
Female 348 6.90 10.02 0.0490
Age (years)
<50 139 2.16 3.38 0.3623
50–75 654 4.43 6.68 0.0125
>75 440 9.55 13.31 0.0174
Type of AMI
STEMI 605 7.77 10.86 0.0116
NSTEMI 628 4.30 6.97 0.0079
Underwent PCI
yes 807 3.47 7.30 0.00003
no 426 10.80 11.85 0.5471
AMI = acute myocardial infarction; PCI = percutaneous coronary intervention; STEMI/NSTEMI = ST elevation / non-ST elevation myocardial infarction. * expected mortality calculated using GRACE risk score mortality calculation. p-values calculated using chi-square test. Values <0.05 were considered statistically significant.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):211–216
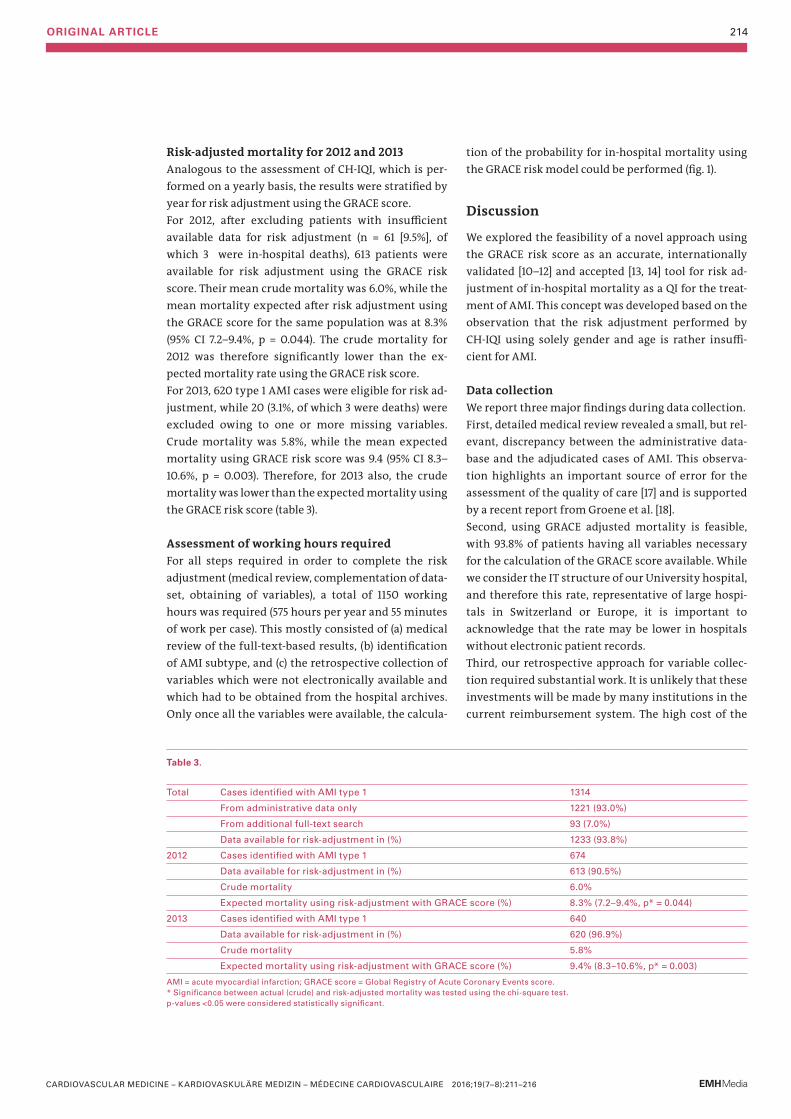
ORIGINAL ARTICLE 214
Risk-adjusted mortality for 2012 and 2013Analogous to the assessment of CH-IQI, which is per-formed on a yearly basis, the results were stratified by year for risk adjustment using the GRACE score. For 2012, after excluding patients with insufficient available data for risk adjustment (n = 61 [9.5%], of which 3 were in-hospital deaths), 613 patients were available for risk adjustment using the GRACE risk score. Their mean crude mortality was 6.0%, while the mean mortality expected after risk adjustment using the GRACE score for the same population was at 8.3% (95% CI 7.2–9.4%, p = 0.044). The crude mortality for 2012 was therefore significantly lower than the ex-pected mortality rate using the GRACE risk score.For 2013, 620 type 1 AMI cases were eligible for risk ad-justment, while 20 (3.1%, of which 3 were deaths) were excluded owing to one or more missing variables. Crude mortality was 5.8%, while the mean expected mortality using GRACE risk score was 9.4 (95% CI 8.3–10.6%, p = 0.003). Therefore, for 2013 also, the crude mortality was lower than the expected mortality using the GRACE risk score (table 3).
Assessment of working hours requiredFor all steps required in order to complete the risk adjustment (medical review, complementation of data-set, obtaining of variables), a total of 1150 working hours was required (575 hours per year and 55 minutes of work per case). This mostly consisted of (a) medical review of the full-text-based results, (b) identification of AMI subtype, and (c) the retrospective collection of variables which were not electronically available and which had to be obtained from the hospital archives. Only once all the variables were available, the calcula-
tion of the probability for in-hospital mortality using the GRACE risk model could be performed (fig. 1).
Discussion
We explored the feasibility of a novel approach using the GRACE risk score as an accurate, internationally validated [10–12] and accepted [13, 14] tool for risk ad-justment of in-hospital mortality as a QI for the treat-ment of AMI. This concept was developed based on the observation that the risk adjustment performed by CH-IQI using solely gender and age is rather insuffi-cient for AMI.
Data collection We report three major findings during data collection.First, detailed medical review revealed a small, but rel-evant, discrepancy between the administrative data-base and the adjudicated cases of AMI. This observa-tion highlights an important source of error for the assessment of the quality of care [17] and is supported by a recent report from Groene et al. [18]. Second, using GRACE adjusted mortality is feasible, with 93.8% of patients having all variables necessary for the calculation of the GRACE score available. While we consider the IT structure of our University hospital, and therefore this rate, representative of large hospi-tals in Switzerland or Europe, it is important to acknowledge that the rate may be lower in hospitals without electronic patient records. Third, our retrospective approach for variable collec-tion required substantial work. It is unlikely that these investments will be made by many institutions in the current reimbursement system. The high cost of the
Table 3.
Total Cases identified with AMI type 1 1314
From administrative data only 1221 (93.0%)
From additional full-text search 93 (7.0%)
Data available for risk-adjustment in (%) 1233 (93.8%)
2012 Cases identified with AMI type 1 674
Data available for risk-adjustment in (%) 613 (90.5%)
Crude mortality 6.0%
Expected mortality using risk-adjustment with GRACE score (%) 8.3% (7.2–9.4%, p* = 0.044)
2013 Cases identified with AMI type 1 640
Data available for risk-adjustment in (%) 620 (96.9%)
Crude mortality 5.8%
Expected mortality using risk-adjustment with GRACE score (%) 9.4% (8.3–10.6%, p* = 0.003)
AMI = acute myocardial infarction; GRACE score = Global Registry of Acute Coronary Events score.* Significance between actual (crude) and risk-adjusted mortality was tested using the chi-square test. p-values <0.05 were considered statistically significant.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):211–216
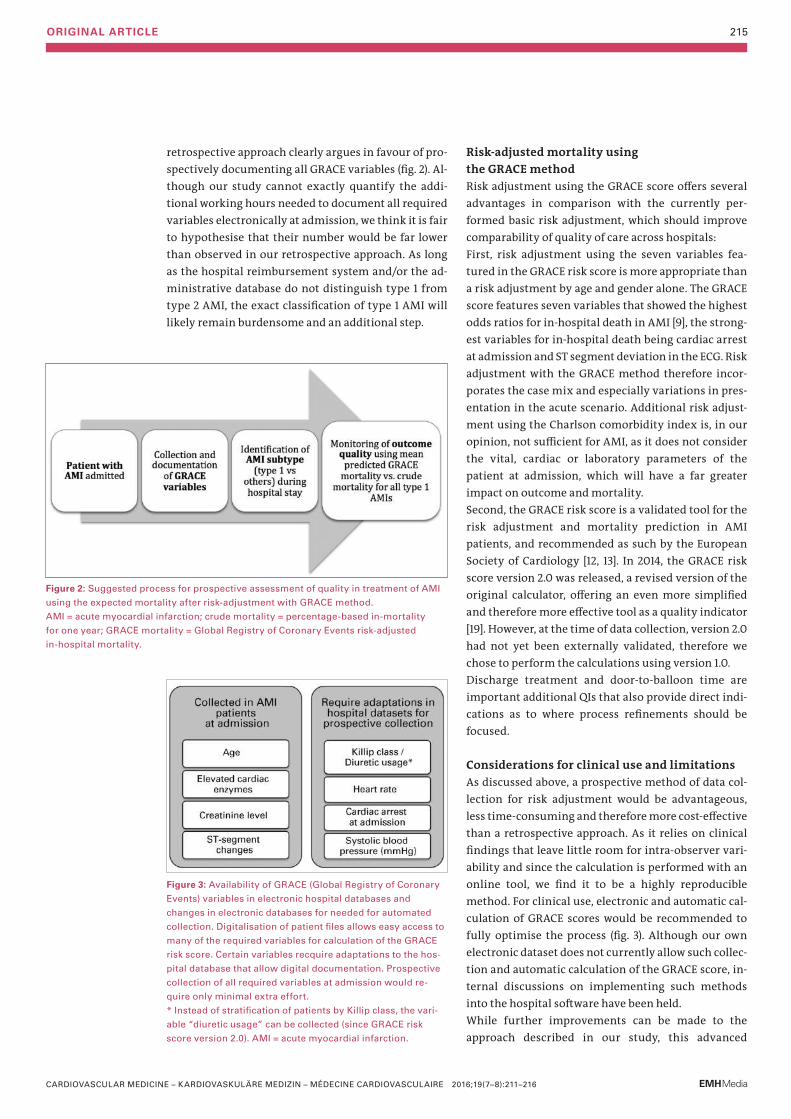
ORIGINAL ARTICLE 215
retrospective approach clearly argues in favour of pro-spectively documenting all GRACE variables (fig. 2). Al-though our study cannot exactly quantify the addi-tional working hours needed to document all required variables electronically at admission, we think it is fair to hypothesise that their number would be far lower than observed in our retrospective approach. As long as the hospital reimbursement system and/or the ad-ministrative database do not distinguish type 1 from type 2 AMI, the exact classification of type 1 AMI will likely remain burdensome and an additional step.
Risk-adjusted mortality using the GRACE methodRisk adjustment using the GRACE score offers several advantages in comparison with the currently per-formed basic risk adjustment, which should improve comparability of quality of care across hospitals:First, risk adjustment using the seven variables fea-tured in the GRACE risk score is more appropriate than a risk adjustment by age and gender alone. The GRACE score features seven variables that showed the highest odds ratios for in-hospital death in AMI [9], the strong-est variables for in-hospital death being cardiac arrest at admission and ST segment deviation in the ECG. Risk adjustment with the GRACE method therefore incor-porates the case mix and especially varia tions in pres-entation in the acute scenario. Additional risk adjust-ment using the Charlson comorbidity index is, in our opinion, not sufficient for AMI, as it does not consider the vital, cardiac or laboratory para meters of the patient at admission, which will have a far greater impact on outcome and mortality. Second, the GRACE risk score is a validated tool for the risk adjustment and mortality prediction in AMI patients, and recommended as such by the European Society of Cardiology [12, 13]. In 2014, the GRACE risk score version 2.0 was released, a revised version of the original calculator, offering an even more simplified and therefore more effective tool as a quality indicator [19]. However, at the time of data collection, version 2.0 had not yet been externally validated, therefore we chose to perform the calculations using version 1.0. Discharge treatment and door-to-balloon time are impor tant additional QIs that also provide direct indi-cations as to where process refinements should be focus ed.
Considerations for clinical use and limitationsAs discussed above, a prospective method of data col-lection for risk adjustment would be advantageous, less time-consuming and therefore more cost-effective than a retrospective approach. As it relies on clinical findings that leave little room for intra-observer vari-ability and since the calculation is performed with an online tool, we find it to be a highly reproducible method. For clinical use, electronic and automatic cal-culation of GRACE scores would be recommended to fully optimise the process (fig. 3). Although our own electronic datase t does not currently allow such collec-tion and automat ic calculation of the GRACE score, in-ternal discussions on implementing such methods into the hospital software have been held. While further improvements can be made to the approach described in our study, this advanced
Figure 2: Suggested process for prospective assessment of quality in treatment of AMI
using the expected mortality after risk-adjustment with GRACE method.
AMI = acute myocardial infarction; crude mortality = percentage-based in-mortality
for one year; GRACE mortality = Global Registry of Coronary Events risk-adjusted
in-hospital mortality.
Figure 3: Availability of GRACE (Global Registry of Coronary
Events) variables in electronic hospital databases and
changes in electronic databases for needed for automated
collection. Digitalisation of patient files allows easy access to
many of the required variables for calculation of the GRACE
risk score. Certain variables recquire adaptations to the hos-
pital database that allow digital documentation. Prospective
collection of all required variables at admission would re-
quire only minimal extra effort.
* Instead of stratification of patients by Killip class, the vari-
able “diuretic usage” can be collected (since GRACE risk
score version 2.0). AMI = acute myocardial infarction.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):211–216

ORIGINAL ARTICLE 216
method will still require additional efforts compared with the simplified method used by CH-IQI. Performance was better than predicted by the GRACE model for both years, as well as all patient groups, and percutaneous coronary intervention seemed to be the most influential variable. The comparison of predicted versus crude mortality allows review of the perform-ance of a hospital. It is conceivable that, due to the high standard of patient care in Switzerland, a small degree of overestimation of mortality with the GRACE score may occur. The GRACE risk score was developed using a multicentre, multinational cohort, and outcomes in-cluding mortality may vary with the geographical location, especially with differences in clinical practice [20, 21]. In our university hospital, the standard cardiac troponin assay is the hs-cTnT assay. The GRACE risk score was derived and validated using less sensitive assays, which may have further influenced the results. As the prognostic accuracy of hs-cTnT is even higher as that of less sensitive assays, it seems fair to assume that this effect might have been small [13].In conclusion, assessment of risk-adjusted in-hospital mortality in AMI is feasible, provides important in-sights regarding treatment results and could improve comparability between healthcare centres. If done retro spectively, it is very time-consuming, relying heavily on the quality and availability of the requir ed data. Prospective documentation of the GRACE score within the electronic medical records would help to reduce substantially the effort needed to obtain this novel QI and improve reliability of data. Further studies in a multicentre setting are required in order to con-firm the advantages of using the GRACE score as a qual-ity indicator and tool for comparison of perform ance.
Disclosure statement No financial support and no other potential conflict of interest relevant to this article was reported.
References 1 Palmer RH. Using health outcomes data to compare plans , net-
works and providers. Int J Qual Health Care. 1998;10(6):477–83. 2 BAG (Bundesamt für Gesundheit). CH-IQI - Swiss Inpatient Quality
Indicators. http://www.bag-anw.admin.ch/kuv/spitalstatistik/data/download/qip12_spezifikationen_31.pdf. Published 2012. Ac-cessed February 18, 2016.
3 Tu J, Khalid L, Donovan L, Ko D. Indicators of quality of care for patients with acute myocardial infarction. CMAJ. 2008;179(9): 909–15.
4 D’Hoore W, Sicotte C, Tilquin C. Risk adjustment in outcome assessment: The Charlson comorbidity index. Methods Inf Med. 1993;32:382–7.
5 Iezzoni LI. 100 Apples Divided by 15 Red Herrings: A Cautionary Tale from the Mid-19th Century on Comparing Hospital Mortality Rates. Ann Intern Med. 1996:1079–85.
6 Rashid S, Simms A, Batin P, Kurian J, Gale CP. Inequalities in care in patients with acute myocardial infarction. World J Cardiol. 2015;7(12):895–901.
7 Canto J, Rogers W, Goldberg R. Association of age and sex with my-ocardial infarction symptom presentation and in-hospital mortal-ity. JAMA. 2012;307(8):813–22.
8 Champney KP, Frederick PD, Bueno H, et al. The joint contribution of sex, age and type of myocardial infarction on hospital mortality following acute myocardial infarction. Heart. 2009;95(11):895–9.
9 Granger CB, Goldberg RJ, Dabbous O, et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch In-tern Med. 2003;163:2345–53.
10 Bradshaw PJ, Ko DT, Newman AM, Donovan LR, Tu J V. Validity of the GRACE (Global Registry of Acute Coronary Events) acute coro-nary syndrome prediction model for six month post-discharge death in an independent data set. Heart. 2006;92:905–9.
11 Eagle KA, Lim MJ, Dabbous OH, et al. A validated prediction model for all forms of acute coronary syndrome: Estimating the risk of 6-month postdischarge death in an international registry. JAMA. 2004;291(22):2727–33.
12 Pieper KS, Gore JM, FitzGerald G, et al. Validity of a risk-prediction tool for hospital mortality: the Global Registry of Acute Coronary Events. Am Heart J. 2009;157(6):1097–1105.
13 Roffi M, Patrono C, Collet J-P, et al. ESC Guidelines for the manage-ment of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Per-sistent ST-Segment Elevation. Eur Heart J. 2016;37(3):267–315.
14 Steg PG, James SK, Atar D, et al. ESC Guidelines for the manage-ment of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012;33(20):2569–619.
15 Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Eur Heart J. 2012;33:2551–67.
16 Killip T, Kimball JT. Treatment of myocardial infarction in a coro-nary care unit. Am J Cardiol. 1967;20:457–64.
17 Maass C, Kuske S, Lessing C, Schrappe M. Are administrative data valid when measuring patient safety in hospitals? A comparison of data collection methods using a chart review and administrative data. Int J Qual Health Care. 2015;27(4):305–13.
18 Groene O, Kristensen S, Arah O a, et al. Feasibility of using admin-istrative data to compare hospital performance in the EU. Int J Qual Health Care. 2014;26 Suppl 1:108–15.
19 Fox KA, Fitzgerald G, Puymirat E, et al. Should patients with acute coronary disease be stratified for management according to their risk? Derivation, external validation and outcomes using the up-dated GRACE risk score. BMJ Open. 2014;4(2):e004425.
20 Elbarouni B, Goodman SG, Yan RT, et al. Validation of the Global Registry of Acute Coronary Event (GRACE) risk score for in-hospital mortality in patients with acute coronary syndrome in Canada. Am Heart J. 2009;158(3):392–9.
21 Insam C, Paccaud F, Marques-Vidal P. Trends in hospital discharges, management and in-hospital mortality from acute myocardial infarction in Switzerland between 1998 and 2008. BMC Public Health. 2013;13(1):270.
Correspondence: Prof. Dr. Christian Müller Department of Cardiology University Hospital Basel Petersgraben 4 CH-4031 Basel christian.mueller[at]usb.ch
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):211–216

CASE REPORT 217
A patient with multiple spontaneous arterial dissections
Dissected womanMattia Cattaneoa*, Daniel Sürderb, Rolf Wyttenbachc, Mario Alercic, Pierluigi Pedrazzid, Marcel Arnolde, Augusto Gallinoa
a Department of Cardiology, Ospedale Regionale di Bellinzona e Valli – San Giovanni, Bellinzona, Switzerland; b Department of Cardiology, Fondazione Cardiocentro Ticino, Lugano, Switzerland; c Department of Radiology, Ospedale Regionale di Bellinzona e Valli – San Giovanni, Bellinzona, Switzerland; d Department of Neurology, Neurocentre of Southern Switzerland, Lugano, Switzerland; e Department of Neurology, Inselspital Universitätsspital Bern, Switzerland
Case report
A 45-year-old woman was admitted to our stroke unit because of acute right hemiparesis, aphasia and mod-erate frontal headache while running on a treadmill. She had no cardiovascular risk factors apart from pre-vious smoking. Furthermore, no recent infections, blunt neck trauma, medical or surgical procedures or risk factors for bleeding were identified. Brain multi-detector computed tomography (MDCT) showed neither acute ischaemic nor haemorrhagic lesions, while MDCT angiography and magnetic resonance imaging angiography (MRA) revealed a 1-cm long sub-occlusive dissection of the left internal carotid artery (LICA) at the level of the cervical-petrous segment junc-tion (figs 1A–B). Aortic MDCT angiography excluded the presence of Stanford type A aortic dissection. Treat-ment with aspirin and neurological follow-up were implemented for the LICA spontaneous dissection [1]. Ten days later the patient was admitted because of acute chest pain at rest later diagnosed as ST-segment elevation acute myocardial infarction. Primary selec-
tive angiography of the right coronary artery, via the radial approach, disclosed distal posterior descending artery (PD) occlusion (fig. 1C; online-only Data Supple-ment Video 1). The lesion was carefully crossed with a guidewire, revealing a subocclusive stenosis along the entire distal PD (fig. 1D; online-only Data Supplement Video 2). On the basis of the characteristics of the lesion and the absence of any additional coronary atheroma-tosis, the diagnosis of spontaneous coronary artery dissection was retained [2]. Due to the small diameter of the vessel lumen, no intravascular imaging was per-formed and a conservative approach was chosen. Four days later, the patient reported acute right back pain. Abdominal aorta MDCT angiography revealed spontaneous right renal artery dissection. It was con-firmed by nonselective renal artery angiography, which also suggested fibromuscular dysplasia (FMD) because of the presence of a possible “string of beads” lesion, but only in a side branch of the renal artery (fig. 1E). A conservative approach was preferred [2, 3]. Since the arterial lesion was not pathognomonic for FMD, genetic testing for vascular Ehlers-Danlos syn-drome (COL3A1 mutation) was also performed, but the results were negative. The patient underwent cautious cardiac rehabilitation, avoiding strong isometric efforts, and implemented measures for secondary prevention of cardiovascular disease. A 6-month follow-up encompassed cardio-vascular imaging such as carotid and cerebral MRA, as well as cardiac and abdominal MDCT angiography. This showed complete spontaneous recanalisation of the affected arteries, with the exception of the distal PD. This is a rare case of three consecutive spontane-ous arterial dissections affecting three different vascu-lar beds and occurring within only 14 days. Despite its exceptionality, this case underscores the need for com-prehensive vascular evaluation and the usefulness of multiple imaging modalities in young and mid-dle-aged patients presenting with spontaneous cervi-cal artery dissection and clinical symptoms suggesting other organ involvement.
Summary
A 45-year-old woman was admitted to our stroke unit because of acute
focal neurological symptoms. A spontaneous left internal carotid artery
dissection was later diagnosed. In the following 14 days the patient was
affected by ST-segment elevation acute myocardial infarction due to distal
posterior descending artery (PD) occlusion and acute right back pain due
to spontaneous right renal artery dissection. A 6-month follow-up showed
complete spontaneous recanalisation of the affected arteries, with the ex-
ception of the distal PD. Despite its exceptionality, this case underscores
the need for comprehensive vascular evaluation in young and middle-aged
patients presenting with spontaneous cervical artery dissection and clini-
cal symptoms suggesting other organ involvement.
Key words: spontaneous arterial dissection; stroke; acute coronary syndrome; vascular imaging
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):217–219
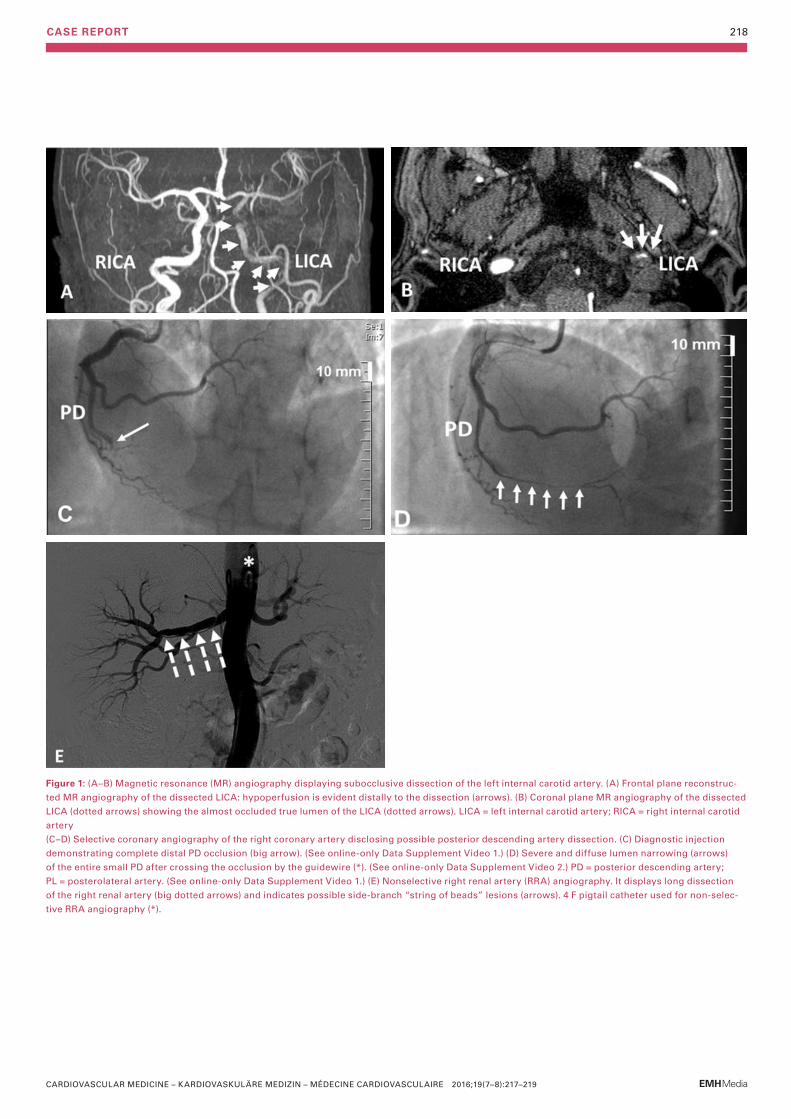
CASE REPORT 218
Figure 1: (A–B) Magnetic resonance (MR) angiography displaying subocclusive dissection of the left internal carotid artery. (A) Frontal plane reconstruc-
ted MR angiography of the dissected LICA: hypo per fu sion is evident distally to the dissection (arrows). (B) Coronal plane MR angiography of the dissected
LICA (dotted arrows) showing the almost occluded true lumen of the LICA (dotted arrows). LICA = left internal carotid artery; RICA = right internal carotid
artery
(C–D) Selective coronary angiography of the right coronary artery disclosing possible posterior descending artery dis section. (C) Diagnostic injection
demonstrating complete distal PD occlusion (big arrow). (See online-only Data Supplement Video 1.) (D) Severe and diffuse lumen narrowing (arrows)
of the entire small PD after crossing the occlusion by the guidewire (*). (See online-only Data Supplement Video 2.) PD = posterior descending artery;
PL = posterolateral artery. (See online-only Data Supplement Video 1.) (E) Nonselective right renal artery (RRA) angiography. It displays long dissection
of the right renal artery (big dotted arrows) and indicates possible side-branch “string of beads” lesions (arrows). 4 F pigtail catheter used for non-selec-
tive RRA angiography (*).
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):217–219

CASE REPORT 219
Discussion
Spontaneous arterial dissection (SAD) is defined as a nontraumatic and noniatrogenic separation of the arterial walls, creating a false lumen. This separation can occur between the intima and media or between the media and adventitia [1, 2]. Spontaneous artery dis-sections are infrequent and underdiagnosed events affecting predominantly young and middle-aged patients and women [1–6]. The spontaneous dissection of a cervical artery accounts for only about 2% of all ischaemic strokes, but the proportion is much higher in young and middle-aged patients [1, 2]. It is difficult to determine the prevalence of coronary SAD ranging from 0.3 to 8% according to clinical setting, age and diagnostic method [2]. Renal SAD is an infrequent dis-ease and epidemiology is based largely on case reports and series [1–6]. Peripartum and underlying heritable arteriopathies or FMD represent the major risk factors for SAD occurrence and recurrence [1–6]. The overall prognosis of cervical SAD is good, with a low mortality rate, good morbidity, and a low rate of recurrent dissection and of ischaemic and bleeding complications. Anticoagulant or antiplatelet treatment strat egies have been implemented in its management. However, no large randomised trial has specifically addressed the management of cervical SAD [1]. Anti-platelet therapy is still considered the first choice, par-ticularly for intracranial extension. Nonetheless, anti-coagulation has also been used in the presence of floating thrombus, occlusion or progression on anti-platelet therapy [1]. Similarly, there are no prospective randomised data specifically addressing the manage-ment of coronary SAD by hard clinical endpoints [2, 3]. Therefore, uncertainty exists on whether the standard management of acute coronary syndrome may be
beneficial for coronary SAD. Revascularisation proce-dures depend on the patient’s performance status and affected coronary anatomy, but often conservative treatment is preferred for stable patients. The progno-sis may be underestimated, since it relies mainly on post-mortem reporting, but female patients poten-tially have a poorer prognosis [2, 3]. The natural history of renal SAD is poorly understood owing to the infre-quency of reporting and the lack of prospective data. Most renal dissections seem to be self-limiting, but malignant hypertension or renal failure secondary to ischaemia may occur [5–6]. Various individualised treatment options have been suggested for renal SAD based on lesion stability, renal function and the pa-tient’s performance status. These options include the conservative approach, medical therapy (such as anti-coagulation), endovascular procedures such as arterial stenting or coiling, and surgical therapy such as vascu-lar reconstruction or nephrectomy [5–6].
Disclosure statementNo financial support and no other potential conflict of interest relevant to this article was reported.
References1 Yang-Ki K, Schulman S. Cervical artery dissection: Pathology,
epidemiology and management. Thromb Res. 2009;123:810–21.2 Yip A, Saw J. Spontaneous coronary artery dissection – A review.
Cardiovasc Diagn Ther. 2015;5(1):37–48.3 Giacoppo D, Capodanno D, Dangas G, Tamburino C. Spontaneous
coronary artery dissection. Int J Cardiol. 2014;175(1):8–20.4 Olin JW, Gornik HL, Bacharach JM, Biller J, Fine LJ, Gray BH, et al.
Fibromuscular dysplasia: state of the science and critical unan-swered questions: a scientific statement from the American Heart Association. Circulation. 2014;129:1048–78.
5 Edwards BS, Stanson AW, Holley KE, Sheps SG Isolated renal artery dissection: presentation, evaluation, management and pathology Mayo Clin Proc. 1982;57:564–71.
6 Lee SH, Lee HC, Oh SJ, Park MC, Park KJ, Moon YS, et al. Percutane-ous intervention of spontaneous renal artery dissection compli-cated with renal infarction: a case report and literature review.Catheter Cardiovasc Interv. 2003;60(3):335–8.
Correspondence: Dr. Mattia Cattaneo, MD Clinical and Research fellow Department of Cardio-vascular Medicine Ospedale Regionale di Bellinzona e Valli San Giovanni CH-6500 Bellinzona mattia.cattaneo[at]eoc.ch
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):217–219
CASE REPORT 220
Bailout procedure after inadvertent false release of a self-expandable TAVI prosthesis
Interventional valve-under-valve implantationOliver T. Reuthebucha, Christoph Kaiserb, Markus Maurerc, Friedrich Ecksteina, Martin Grapowa
a Clinic for Cardiac Surgery, University Hospital Basel, Switzerland b Department of Cardiology, University Hospital Basel, Switzerland c Department of Anaesthesiology, University Hospital Basel, Switzerland
SummaryWe present a case of false deployment of a self-expandable transcatheter aortic valve
implantation (TAVI) prosthesis due to inadvertent and incorrect release of an eyelet in the
crown of the valve resulting in a tilted valve. Hence the prosthesis had to be deployed in
an anatomically and functionally inappropriate position above the coronary ostia at the
level of the sinotubular junction. Because of previous coronary artery bypass grafting
with patent grafts, conventional re-do surgery as bailout was rejected and implantation
of a second, balloon-expandable TAVI prostheses favoured instead. This caused a valve-
under-valve situation. Because of the patent bypass grafts, myocardial ischa emia could
be prevented, although diastolic myocardial perfusion via native coronaries was
restrict ed in this unique setting. The postoperative course was uneventful. The gradient
over the valves was 12 mm Hg with minimal paravalvular leakage. At 1-year follow-up, the
patient was in good clinical condition. Transthoracic echocardiography revealed a peak/
mean gradient of 16/8 mm Hg with grade 1 paravalvular leakage.
Key words: TAVI, misplacement, bail out, myocardial perfusion
Case description
An 83-year-old male patient (73 kg, 170 cm, body mass index 25 kg/m2, EuroSCORE II 4.2%, Society of Thoracic Surgeons score 14.27%) was scheduled for transapical transcatheter aortic valve implantation (TAVI) because of moderate to severe aortic stenosis (mean pressure gradient: 29 mm Hg, effective orifice area: 0.9 cm2).Preoperative work-up revealed massive kinking as well as distinct atherosclerosis of the abdominal aorta. Be-sides that, the patient was suffering from coronary heart disease, with a triple bypass revascularisation in 2005. Recent angiography revealed patent grafts: left internal mammary artery to left anterior descend ing artery (LAD), and single vein grafts to the right poste-rior descending artery as well as to the circumflex ar-tery. However, native coronaries were either 95% stenotic (left main, proximal LAD, circumflex artery) or even occluded (middle LAD, right coronary artery). As a result of the uncompromised graft flow, left ejec-tion fraction was preserved at 55%. Because of brady-cardic atrial fibrillation, a pacemaker was implanted in 2010.
Data derived from a preoperative computed tomogra-phy (CT) scan and analysed with 3mensio planning software (3mensio Medical Imaging BV, Bilthoven, Netherlands) revealed a valve annulus diameter of 26.1 mm according to perimeter and of 25.8 mm accord-ing to area, moderate calcifications of the leaflets and a distance of 67 mm between the annulus and the curv-ature of the ascending aorta. In accordance with the heart team decision and with our clinical algorithm, we suggested implanting a 27 mm JenaValveTM (Jena-Valve Technology GmbH, Munich, Germany). At a pre-operative consultation, the patient chose the inter-ventional approach.Under general anaesthesia the apex was accessed in the fifth intercostal space. Pericardial adhesions were de tached and purse-string sutures applied. Under rapid pacing, straight valvuloplasty was performed and the JenaValveTM subsequently introduced. After re-lease of the positioning feelers they were placed in the sinuses of the native valve. Because of imperfect pos-itioning, the feelers of the JenaValveTM were repos-itioned. Simultaneously, one of the three eyelets of the crown inadvertently popped out of the catheter tip (fig. 1). Thus the valve became immobile and could no lon-ger be replaced or removed. It had to be finally released at the level of the sinotubular junction. Severe para-valvular leakage could be determined angiographi-cally and echocardiographically. Fortunately the pati-ent was haemodynamically stable and no signs of myocardial ischaemia were detected. Because of the severe atherosclerosis of the native coronaries, as well as the sufficient myocardial perfusion via bypass grafts, conventional reoperation with sternotomy as bailout was rejected and implantation of a second TAVI prosthesis favoured instead. Therefore, a 26-mm Sapien S3 valve (Edwards, Irvine, USA) was chosen and uneventfully implanted transapically. The prosthesis was posi tioned directly beneath the JenaValveTM resul-ting in a valve-under-valve situation (fig. 2). Angio-graphy and echocardiography revealed overall mini-mal paravalvular leakage at the level of the right
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):220–222
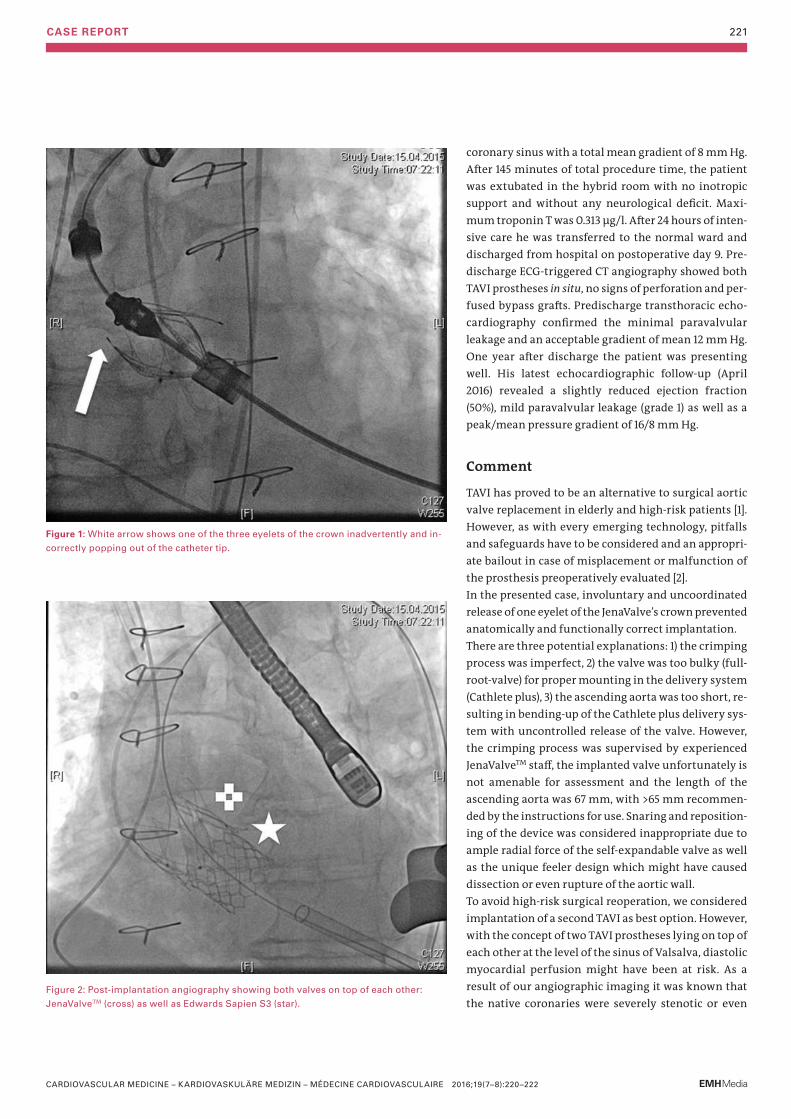
CASE REPORT 221
coronary sinus with a total mean gradient of 8 mm Hg. After 145 minutes of total procedure time, the patient was extubated in the hybrid room with no inotropic support and with out any neurological deficit. Maxi-mum troponin T was 0.313 μg/l. After 24 hours of inten-sive care he was transferred to the normal ward and dis charged from hospital on postoperative day 9. Pre-discharge ECG-triggered CT angiography showed both TAVI prostheses in situ, no signs of perforation and per-fused bypass grafts. Predischarge transthoracic echo-cardiography confirmed the minimal paravalvular leakage and an acceptable gradient of mean 12 mm Hg. One year after discharge the patient was presenting well. His latest echocardiographic follow-up (April 2016) revealed a slightly reduced ejection fraction (50%), mild paravalvular leakage (grade 1) as well as a peak/mean pressure gradient of 16/8 mm Hg.
Comment
TAVI has proved to be an alternative to surgical aortic valve replacement in elderly and high-risk pa tients [1]. However, as with every emerging technology, pitfalls and safeguards have to be considered and an appropri-ate bailout in case of misplacement or malfunction of the prosthesis preoperatively evaluated [2]. In the presented case, involuntary and uncoordinated release of one eyelet of the JenaValve’s crown prevent ed anatomically and functionally correct implantation. There are three potential explanations: 1) the crimping process was imperfect, 2) the valve was too bulky (full-root-valve) for proper mounting in the delivery system (Cathlete plus), 3) the ascending aorta was too short, re-sulting in bending-up of the Cathlete plus delivery sys-tem with uncontrolled release of the valve. However, the crimping process was supervised by experienced JenaValveTM staff, the implanted valve unfortunately is not amenable for assessment and the length of the ascend ing aorta was 67 mm, with >65 mm recommen-ded by the instructions for use. Snaring and reposition-ing of the device was considered inappropriate due to ample radial force of the self-expandable valve as well as the unique feeler design which might have caused dissection or even rupture of the aortic wall.To avoid high-risk surgical reoperation, we considered implantation of a second TAVI as best option. However, with the concept of two TAVI prostheses lying on top of each other at the level of the sinus of Valsalva, diastolic myocardial perfusion might have been at risk. As a result of our angiographic imaging it was known that the native coronaries were severely stenotic or even
Figure 2: Post-implantation angiography showing both valves on top of each other:
JenaValveTM (cross) as well as Edwards Sapien S3 (star).
Figure 1: White arrow shows one of the three eyelets of the crown inadvertently and in-
correctly popping out of the catheter tip.
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):220–222
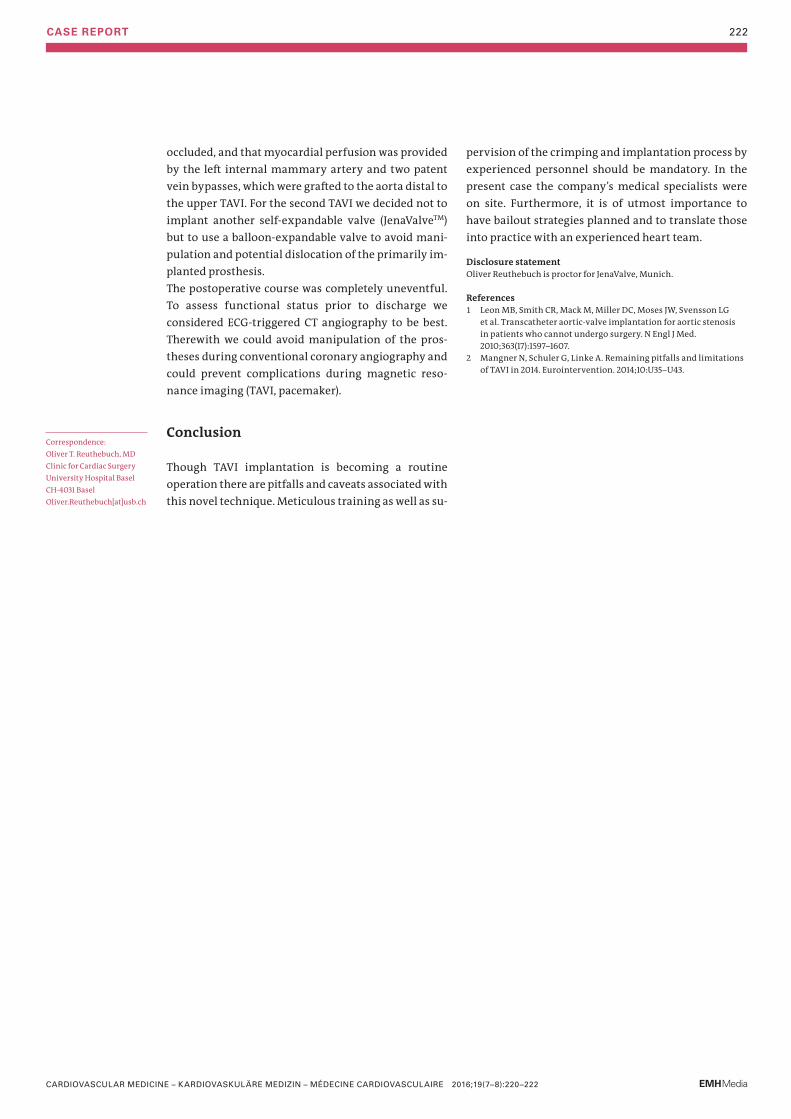
CASE REPORT 222
occluded, and that myocardial perfusion was provided by the left internal mammary artery and two patent vein bypasses, which were grafted to the aorta distal to the upper TAVI. For the second TAVI we decided not to implant another self-expandable valve (JenaValveTM) but to use a balloon-expandable valve to avoid mani-pulation and potential dislocation of the primarily im-planted prosthesis. The postoperative course was completely uneventful. To assess functional status prior to discharge we consid ered ECG-triggered CT angiography to be best. Therewith we could avoid manipulation of the pros-theses during conventional coronary angiography and could prevent complications during magnetic reso-nance imaging (TAVI, pace maker).
Conclusion
Though TAVI implantation is becoming a routine operation there are pitfalls and caveats associated with this novel technique. Meticulous training as well as su-
pervision of the crimping and implantation process by experienced personnel should be mandatory. In the present case the company’s medical specialists were on site. Furthermore, it is of utmost importance to have bailout strategies planned and to translate those into practice with an experienced heart team.
Disclosure statement Oliver Reuthebuch is proctor for JenaValve, Munich.
References1 Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG
et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597–1607.
2 Mangner N, Schuler G, Linke A. Remaining pitfalls and limitations of TAVI in 2014. Eurointervention. 2014;10:U35–U43.
Correspondence: Oliver T. Reuthebuch, MD Clinic for Cardiac Surgery University Hospital Basel CH-4031 Basel Oliver.Reuthebuch[at]usb.ch
CARDIOVASCULAR MEDICINE – KARDIOVASKULÄRE MEDIZIN – MÉDECINE CARDIOVASCULAIRE 2016;19(7–8):220–222


















