Gynaecology Emergencies in Primary Care€¦ · PPT file · Web view · 2015-10-01So – if not...
15
Gynaecology Emergencies in Primary Care Mr Philip Kaloo Consultant Gynaecologist and Laparoscopic Surgeon
Transcript of Gynaecology Emergencies in Primary Care€¦ · PPT file · Web view · 2015-10-01So – if not...

Gynaecology Emergencies in Primary Care
Mr Philip KalooConsultant Gynaecologist and
Laparoscopic Surgeon
Symptoms
Bleeding
InfectionPain

Until proven otherwise -
• All vaginal bleeding is due to pregnancy• All pelvic pain is due to ectopic pregnancy• All pelvic pain + pyrexia = PID

Bleeding
28 year old comes into your practice complaining of heavy bleeding
ABCHistory – How much?
Menstrual, LMPMedical hx, Drug hx
Examination – ObservationsAbdominal Vaginal
Investigations – pregnancy test

Scenario
7/40 pregnant, heavy bleeding. Soaked 4 pads at home.
BP 90/40, pulse 50Looks pale, not happy
Diagnosis?What do you do?
Speculum and remove products, refer.

So – if Pregnant + bleeding
Ectopic – unlikelyThreatened miscarriageInevitable miscarriageComplete miscarriage

So – if not pregnant + bleeding
Uterine pathologyFibroids, adenomyosis, endometrial pathology (e.g. polyp)
Anovulatory bleeds PCO, perimenopause, perimenarche
Systemic diseaseThyroid disorders, hepatic diseases, renal diseases, adrenal hyperplasia and Cushing's disease
CoagulopathyVon Willebrands disease, thrombocytopenia
IatrogenicIUCD in situ, Anticoagulants, antipsychotics, corticosteroids, pop, SSRI’s, tamoxifen, thyroxine, herbal and other supplements such as ginseng, ginkgo and soy
Dysfunctional uterine bleedingDiagnosis of exclusion
Pain
33 year old, G3P0, IVF 6 weeks ago, PMH – Endometriosis, CIN 3Sx - pelvic pain, no pv bleeding.Hx and examination
What is your differential?1. Ectopic until proven otherwise2. Ovarian cyst incident / torsion3. OHSS4. ?Endometriosis
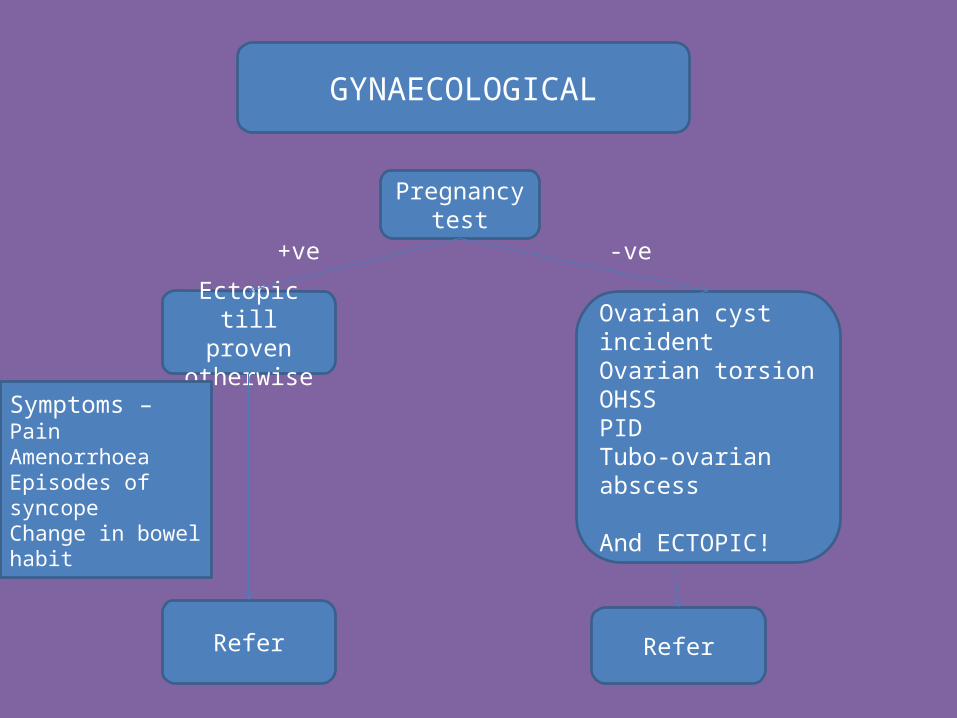
Pregnancy test
Ectopic till proven
otherwise
GYNAECOLOGICAL
Symptoms – PainAmenorrhoeaEpisodes of syncopeChange in bowel habit
Ovarian cyst incidentOvarian torsionOHSSPIDTubo-ovarian abscess
And ECTOPIC!
+ve -ve
Refer Refer

Ovarian torsion
Uncommon cause of gynae emergencies <4%. 80% in reproductive ageIncreased with pregnancy (14%), ovarian cysts,
previous abdominal surgery, right sided.
Presentation •Systemically unwell (↑ Temp,↑ Pulse, ↑ Resp rate)•Unilateral lumbar or abdominal pain•Pain duration >8 hours•Nausea / Vomiting

Infectiona) PIDb) Tubo-ovarian abscessc) Bartholins cyst/abscessd) Toxic-shock syndrome
PID Presentation:● bilateral lower abdominal tenderness (sometimes radiating to the legs)● abnormal vaginal or cervical discharge● fever (greater than 38°C)● abnormal vaginal bleeding (intermenstrual, postcoital or ‘breakthrough’)● deep dyspareunia● cervical motion tenderness on bimanual vaginal examination● adnexal tenderness on bimanual vaginal examination (with or without a palpable mass).

PID – when to refer in
• Surgical emergency cannot be excluded• Clinically severe disease• Tubo-ovarian abscess• PID in pregnancy• Lack of response to oral therapy• Intolerance to oral therapy.

Toxic Shock SyndromeRare 18 cases per year in UK. ½ related to menstruationAcute, noncontagious, toxin-mediated febrile illness caused by staphylococcal
infection
Presentation•pyrexia (>39°C)•hypotension•diarrhoea and vomiting•headache •muscle cramps and myalgias•rash (diffuse macular erythroderma or 'sunburn')•multi-organ dysfunction•shock, adult respiratory distress syndrome, disseminated intravascular coagulation and renal failure

Gynae scanning

Take home messages
Bleeding – Assume pregnantDon’t underestimate
Pain – Ectopic till proven otherwise A negative pregnancy test does not
exclude an ectopic Ovarian torsion if treated <48 hours =
viable ovaryInfection – Treat early , refer early








![Effects of Ovarian Pathologies and Uterine Inflammations on Adenomyosis … · 2018-08-14 · the course of histopathologic examination of uteri [25]. However, adenomyosis can be](https://static.fdocuments.in/doc/165x107/5c9ca8f088c9938d348b62dd/effects-of-ovarian-pathologies-and-uterine-inflammations-on-adenomyosis-2018-08-14.jpg)