Diseases of oral Pain: cavity, pharynx and oesophagus · Oral cavity ex., endoscopy , X-ray...
11
2016.12.07 1 Diseases of oral cavity, pharynx and oesophagus Prof. Vörös Károly Diff. Dx. of Dysphagia 1. Pain: Dental diseases (eg. tooth fracture, abscess, disease of periodontium, abnormal dentation) Inflammatory processes, abscess (oral, pharyngeal, tongue, lymphnodes) Foreign bodies Mandibular trauma Hyoid or temporomandibular joint disease Diff. Dx. of Dysphagia 2. Muscular: Hyperkalaemic Periodic Paralysis Nutritional myodegeneration (Se) Polysaccharide storage myopathies Masseter inflammation Hypocalcaemic tetany Megaesophagus Rupture of rectus capitis ventralis Diff. Dx. of Dysphagia 3. Obstruction: Abscessation, inflammation, neoplasia of retropharyngeal lymphonode Malformation, injury, neoplasia, oedema, cysts anywhere „on the way” Foreign body DDSP or Fourth Branchial Arch Defect (4BAD) Cleft palate Guttural pouch tympani or empyema Oesophageal obstruction Pharyngeal cicatrix Diff. Dx. of Dysphagia 4. Nervous system: V, VII, IX, X, XII cranial nerves Guttural pouch mycosis, empyema, neoplasia Broken bones, osteomyelitis Retropharyngeal abscess Neurotoxins, toxic materials Tetanus Botulism Hepatoencephalopathy Lead poisoning Generalized neurophaties Equine dysatonomia, Grass sickness Polyneuritis equi CNS disorders Intracranial edema, haemhorrhagia, neoplasia, hematome, abscess Víral encephalitis: rabies, WND, EHV-1, other tick borne encephalities (EEE, WEE, VEE) Equine protozoal myeloencephalitis (EPM) Nutritional management No long fiber Feeding foal tubes/Nasogastric tube Oesophagostomy; pellet slurries, liquid diets Electrolytes substitution (salivary loss: Na, K, Cl) Energy requirements: corn oil
Transcript of Diseases of oral Pain: cavity, pharynx and oesophagus · Oral cavity ex., endoscopy , X-ray...

2016.12.07
1
Diseases of oral cavity, pharynx and oesophagus
Prof. Vörös Károly
Diff. Dx. of Dysphagia 1.
� Pain:
� Dental diseases (eg. tooth fracture, abscess, disease of periodontium, abnormal dentation)
� Inflammatory processes, abscess (oral, pharyngeal, tongue, lymphnodes)
� Foreign bodies
� Mandibular trauma
� Hyoid or temporomandibular joint disease
Diff. Dx. of Dysphagia 2.
� Muscular:
� Hyperkalaemic Periodic Paralysis
� Nutritional myodegeneration (Se)
� Polysaccharide storage myopathies
� Masseter inflammation
� Hypocalcaemic tetany
� Megaesophagus
� Rupture of rectus capitis ventralis
Diff. Dx. of Dysphagia 3.
� Obstruction:� Abscessation, inflammation, neoplasia of retropharyngeal
lymphonode
� Malformation, injury, neoplasia, oedema, cysts anywhere „on the way”
� Foreign body
� DDSP or Fourth Branchial Arch Defect (4BAD)
� Cleft palate
� Guttural pouch tympani or empyema
� Oesophageal obstruction
� Pharyngeal cicatrix
Diff. Dx. of Dysphagia 4.� Nervous system:
� V, VII, IX, X, XII cranial nerves� Guttural pouch mycosis, empyema, neoplasia� Broken bones, osteomyelitis� Retropharyngeal abscess
� Neurotoxins, toxic materials� Tetanus� Botulism� Hepatoencephalopathy � Lead poisoning
� Generalized neurophaties� Equine dysatonomia, Grass sickness� Polyneuritis equi
� CNS disorders� Intracranial edema, haemhorrhagia, neoplasia, hematome, abscess� Víral encephalitis: rabies, WND, EHV-1,� other tick borne encephalities (EEE, WEE, VEE)� Equine protozoal myeloencephalitis (EPM)
Nutritional management
� No long fiber
� Feeding foal tubes/Nasogastric tube
Oesophagostomy; pellet slurries, liquid diets
� Electrolytes substitution
(salivary loss: Na, K, Cl)
� Energy requirements: corn oil

2016.12.07
2
Dental diseases
� Riding difficulties, decreased appetite,
weight loss, nasal discharge, swellings etc.
� Diseases of the tooth radicals: caries, fracture,
foreign bodies
� Mandibular: fistula
� Maxillary: sinusitis
� Teeth wear problems
� Regular check
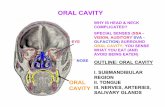
� Oral cavity exam., x-ray, endoscopy, CT, MRI
Congenital diseases(oral and pharyngeal cavity)
� Cleft Palate
� Soft or/and hard palate
� Dysphagia, regurgitation
� Aspiration pneumonia
� Weight loss
� Surgery
� Pharyngeal cysts
� Subepiglottal
� Soft palate
� Hypoplasia of upper lip, campylorhinus lateralis
Oral cavity ex.,endoscopy, X-ray
Diseases of oral cavity
� Non infectious:� Mechanical injuries (food, tooth, bite etc.)
� Chemical materials (eg. phenyl-butason)
� Toxic and metabolic diseases
� eg.: renal, liver failure
� Infectious
� viral (vesiculo, vaccinia)
� bacterial (eg.:Actinobacillosis)
� fungal (candidiosis, satratoxicosis)
� Autoimmune diseases
� Amyloidosis
Oral neoplasias
� Squamous cell carcinoma, fibrosarcoma, melanoma, haemangiosarcoma, rhabdomyoma, lymphosarcoma, osteosarcoma
� Biopsy
� Surgery (?)

2016.12.07
3
Hyoid apparatus and tongue
� Glossitis / oedema, injury of tongue
Signs: salivation, appetite loss, halitosis
� Fracture, inflammation, neoplasia of hyoid bones
� Temporohyoidal arthrosis, arthritis
Signs: bleedings, cranial nerve paralyses, decreased appetite, weight loss
DX: endoscopy, x-ray, CT, MRI, US
TX: ABs, NSAIDs, n-g feeding, surgery
Ulceration Injury
Paralysis
� N. hypoglossus
� Encephalitis, botulism, etc. (see dysphagia)
� Unilateral/bilateral
� Neonatal tongue and pharyngeal weakness
� inmature
� milk regurgitation
� 2-4 weeks
Pharyngitis
� Mechanical� Eg: nasogastric tubing, foreign bodies
� Chemical� Bacterial and viral and allergens
� Young horses (2-6 yrs), immunosuppression (Streptococci, Actinobacillus equuli, resp. viruses)
� chronic pharyngitis� lymphoid hyperplasia� Poor performance, resp. symptoms, pain,
swallowing difficulties, salivation� DX: endoscopy, swab� TX: inhalation of AB/NSAID/DMSO
Pharyngeal Paralysis
� Cranial nerves� N. glossopharyngeus (IX)
� N. vagus (X)
� CNS: mental status, other symptoms
� Usu. with oesophageal paralysis
� Sx: dysphagia, regurgitation
� Dx: nervous system ex., endoscopy
� Aspiration pneumonia (US, X-ray)
� Tx: ?, poor prognosis

2016.12.07
4
Diseases of salivary glands
� 12 l saliva daily
� Parotis: electrolytes, (sialoliths: calcium)
� Submandibular, sublingual glands less important
� Inflammation� Acute, chronic
� Ascending through Stenon-duct
� Haematogenous
� Traumatic
� Signs:� Pain symptoms
� Unilateral swelling
� Purulent - putrid (US: gas, Ca deposits)
� Fistula formation – saliva drains
� Chronic: fibrosis
� Tx: AB, NSAID, formalin inj.,
surgery
� Neoplasia� Adenocarcinoma, melanoma
Diseases of oesophagus
� Congenital� Intramural cysts
� Endoscopy, contrast x-ray, biopsy
� Surgery
� Megaoesophagus � Primer: muscular hypoplasia, dysplasia
� Secunder: stricture, strangulation (Botallo-duct)
� Oesophagus duplex
� Oesophageal spasm
� Cold water, fast eating
� Young, nervous, hungry horses
� Inflammatory processes, nasogastric tubing
� Cardiospasm
� Transient or followed by obstruction

2016.12.07
5
� Oesophageal obstruction/Choke� Primer: food parts, foreign bodies,
poor dentation,
after narcosis or exhausting work
� Secunder: as a consequence of
other (oesophageal) diseases
� Behind pharynx, thoracic inlet, front of diaphragm
� Signs: Discomfort, regurgitation
� Dx: palpable?, n-g tubing, X-ray, endoscopy
� Complications:� Aspiration pneumonia
� Oesophageal ulceration, mucosal necrosis, perforation
� Chronic: dehydration, hyponatraemia, hypochloraemia, hypokalaemia, metabolic acidosis
� Tx:
� Massage
� Spasmolytic (butil-scopolamin, oxytocin), painkillers (NSAID), sedatives (acepromazine, xylazine, detomidine)
� Infusion therapy
� Lavage through nasogastric tube (standing, gen. anaesthesia.)
� Surgery
� Endoscopic control after
� Diet, feeding tube
� Stricture formation!
� Oesophageal inflammation, ulceration
� Swallowing irrigative materials
� Gastric and duodenal ulcers, delayed gastric emptying: reflux oesophagitis
� Loss of appetite, teeth-grinding, dysphagia
� Dx: endoscopy, contrast x-ray
� Tx: sucralfate, ranitidine, omeprazole, metoclopramide
� Oesophageal perforation, rupture
� Nasogastric tubing, strange bodies, trauma from outside
� Chronic inflammation, obstruction
� Cervical region: putrid perioesophagitis (nerves, vessels)
� Thoracic region: mediastinitis, pleuritis – poor prognosis
� Dx: signs, endoscopy, x-ray
� Tx: surgery, NSAID, AB

2016.12.07
6
� Esophageal stricture, compression, dilatation� Stricture: secondary
� Compression: neoplasia, abscess (lymphnodes!!!)
� Dilatation: front of stricture or compression
� Diverticulum (pulsion, traction)
� Tx: surgery, balloon catether
General features ofcolic diseases
The „COLIC”:
� In most cases: symptoms of gastrointestinal pain
� Other possible causes
e.g..: urinary system,
spleen rupture, uterine torsion,
liver diseases etc.
� Colic like behaviour
e.g. nervous system diseases
Common features of the pathogenesis
of colic diseases
Non-strangulating Strangulating disorders Enteritis
• Muscle spasm
•Intestinal damage
• Tense mesenterium
Pain, exhaustion
•Local circulatorydisorder
•Fluid sequestration
Hypovolaemia
•Wall permeability
•Dysbacteriosis
Endotoxinemiavasoconstrictionsplenic contractionsweating
inflamm. mediatorsDIC, organ dysfunctionvessel dilatationSIRS MODS
Peripherial circulatory failure
[--] tissue perfusion, haemoconcentration, metabolic acidosis, uremia

2016.12.07
7
Drugs
� Non-strangulating, enteritis, colitis: conservative
� Strangulating: surgery
Pain, exhaustion, motility� Spasmolytic (butil-
scopolamin)� Analgesics (NSAIDs,
lidocaine)� Sedatives
(alpha2agonists)� Prokinetics
(neostigmine, metoclopramide, etc)
Hypovolaemia
•Infusions (saline, ringer, ringer-lactate, hetastarch, colloids, plasma)
Laxatives
•Mineral oil
•Na/MgSO4
Endotoxinemia
/DIC
•Hyperimmune plasma
•PolimixinB
•Corticosteroids
•Pentoxifilin
•DMSO
•Heparine, aspirine
Steps of establishing Dx and Tx
� Define cardiovascular and metabolic status
� Define exact diagnosis and causative agents (if possible)
� Decide about hospitalisation
� Decide about surgery
� Define measures of conservative tx and monitoring techniques
� If surgery, prepare to minimalize risk and time for general anaesthesia, define type of general anaesthesia
� When not sure, do not hesitate rather operate!
History
� Season, weather
� Sex, age, breed, use
� Previous treatments (NSAID, anthelmintics) and diseases, abdominal surgery
� Feeding and stabling technology, pasture (eg: grass sickness, atropine toxicities)
� Duration of colic (level of intestinal injury), how serious, reaction for treatments
sex
„management” age
breed
sport
Physical examination 1: General impression
� Facial expression
� Sweating
� Signs of colic injuries
� Abdominal distension
� Muscle tremor (electrolyte disturbances, pain)
� Body position
� Behaviour (colic, apatic)
Physical examination 2.: Pain
� One of the most important „parameters”
� Age, temperament, surroundings
� Level� Serious: not reacting to outside stimuli, no effect
of painkillers (max. 3-5 mins.), usu. surgery
� Medium: calms down when walking or transport, effect of painkillers 2-4 hours
� Mild: outside stimuli draws attention easily, effect of painkillers 8-12 hours

2016.12.07
8
Colic pain
Physical examination 3.: Definition of basic clinical values and cardiovascular status
� Body temperature: 39°C< no surgery, acute infectious or other inflammatory process (endotoxaemia)
� Respiratory rate: endotoxaemia, increased diaphragmatic pressure, hypovolaemia, diaphragmatic hernia
� Pulse rate: not correlates with pain but cardiovascular system (eg.: endotoxin shock)
� CRT, mucus membrane, venous refill, arrhythmias, skin temperature
� Rapid worsening of cardiovascular parameters= indication for surgery (after stabilization)
Color of mucus membrane Physical examination 4.: Gastrointestinal organs
� Shape of abdomen: determine site of gas (fluid or content) accumulation
� Abdominal stretch
� Auscultation: min. 5 mins., type and strength of borborygmi (eg.: fluid/gas-steel band effect, sand-10-25 cm behind xyphoideus scratch-like), how it reacts for treatment (prokinetics), no borborygmi surgery
� Percussion, auscultation with simultaneous percussion: gas in caecum or large colon
� Palpation, ballotation: in foals less then 4 weeks
Additional diagnostic methods: Rectal examination
� Systematic examination:
� urinary and reproductive organs, inguinal rings, pelvic flexure, (ventral ?) and dorsal part of colon, taenias, spleen, left kidney, nephrosplenic space, mesentery, aorta, small intestine (?), small colon, head of caecum, ventral and medial taenia, peritoneum
� Exact diagnosis not always possible/ necessary
� Indications for surgery: gas distended small intestines, displaced and gas distended large colon, enteroliths
� Euthanasia: rupture of intestines or stomach, rectal tear-GI content in abdominal cavity
Additional diagnostic methods: Nasogastric tubing
� Life-saving, always wash till empty, abnormal fermentation, gastroesophageal reflux at surgery, pressure on diaphragm
� Quantity: 4 l > (10 l< proximal enteritis!)
� Quality: colour, odour, consistency, pH� Food particles
� Greenish-brown, fluid, bad smell
� Orange, fluid (culture)
� Bloody, reddish, or blood only with test paper

2016.12.07
9
Nasogastric tubingAdditional diagnostic methods: Abdominocentesis� Not better for routine treatments� General site or ultrasound guide, serial sampling� Quality, quantity (colour, turbidity, cells: Ht, sediment,
etc.)� Protein: 2,5 g/dl>� Cell count 5000-10,000/µl (foal 1500),
2:1=neutrophyl: mononuclear� Protein RBC+fibrinogen WBC
(transudate→exudate)� Cytology: wbc, rbc, bacteria, neoplastic cells, food
particles� Culture� Biochemistry: pH (7,3>), glucose (30 mg/dl>), fibrinogen
� GGT, lipase, amylase� LDH, CK, ALKP
Abdominocentesis Hematology
� PCV: � Hypovolaemia (intestinal wall injury,
endotoxaemia)
� Spleen contraction (30%)
� Nephrosplenic entrapment
� Increasing even with therapy – surgery
� Decreasing: intraabdominal bleeding
� TPP:� Reflects more reliably the hypovolaemia
� Serious permeability disorders: increases then falls
� Primary decrease: peritonitis, severe, acute enteritis
Hematology
� CBC:
� Endotoxaemia, Gr- sepsis, Salmonellosis: neutropenia (toxic)
� Stress-leukogram: low wbc, relativ neutrophilia, lymphopenia
� Neutrophilia: e.g..:mesenterial abscess, subacute or chronic processes
� Thrombocytopenia: DIC
� Negative
Acid-base parameters and ionogram
� Na +↓ ,K+↓:small intestinal ileus, diarrhoea
� Cl-↓: not absorbed gastric content, reflux, sweating (metabolic alkalosis?)
� Ca++↓:no absorption from gut, sweating, abnormal sensitivity to PTH, intracellular sequestration, Ca-bind to albumin, ionised
� Metabolic acidosis: peripheral shock, loss of bicarbonates in intestinal fluids, ischemic intestinal wall lactacidosis

2016.12.07
10
Biochemistry
� Protein: albumin↓, globulin↑
� Glucose: increase then decrease - stress, endotoxaemia
� Creatinine: hypovolaemia and kidney
� Liver enzymes: general anaesthesia, in large colon displacement and in enteritis (pancreas enzymes also)� Alterations usu. after surgery
Additional diagnostic methods:X-ray
� Foals, ponies (140 kg>): site and degree of gas distension, necrosis of intestinal wall
� Contrast material: po., per rectum barium-sulfate 5ml/ttkg (30%)� Po: gastric emptying, invagination, ileus
� Per rectum: small colon and colon transverse obstipation, obturation
� Adult horses: limited� Sand, enteroliths, diaphragmatic hernia
X-ray Additional diagnostic methods: ultrasonography
� Foals: umbilical remnants, bladder, invaginations, necrotizing enteritis, hernias
� Adults: limited� Intraabdominal abscesses, neoplasia
� Invaginations
� Intestinal strangulation: motility, wall thickness
� Nephrosplenic entrapment
� Hernias (diaphragmatic, inguinal, scrotal)
� Peritonitis
� Peritoneal fluid: quality, quantity
� Enteroliths
� Spleen rupture
Ultrasonography Additional diagnostic methods: CT?
� Ponies and foals
� Genera anaesthesia

2016.12.07
11
Additional diagnostic methods: endoscopy
� 3 m long flexible endoscope
� oesophagus, stomach, small intestine
� Rectum, ampulla
� Biopsy
� Rather in chronic cases
Endoscopy
Additional diagnostic methods: laparoscopy
� Chronic cases or for diagnostics
� Standing or general anaesthesia
� Adhesions, neoplasias, biopsies, etc.
Additional diagnostic methods: scintigraphy
� Gamma-camera images increased density of radioactive material (iv.)
� Increased uptake on inflammatory areas (20 hrs later)� Right dorsal colitis
� Abscesse
� Neoplasias
� Gastric emptying
� Bile flow