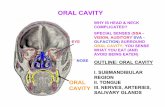
Oral Tumors,In Oral Cavity

of 33
Transcript of Oral Tumors,In Oral Cavity
-
8/9/2019 Oral Tumors,In Oral Cavity
1/33
17/5/20
Benign and malignantepithelial tumors
Localization in oral cavity
Benign and malignantmesenchymal tumors
Localization in oral cavity
Other types tumors (pigment,nervous system, odontogenic)
Synpsis
Benign tumors of mesenchymal origin. Malignant tumors of mesenchymal origin. Benign tumors of epithelial origin – adenoma, papilloma. Malignant tumors of epithelial origin – carcinoma. Localization in
oral cavity. Tumors of melanocyte origin. Tumors of the central nervous system. Tumors of the peripheral nervous system. Benign tumors of connective tissue. Benign and malignant tumors of smooth and striated muscles. Tumors from vessels’ wall – benign and malignant. Malignant tumors of connective tissue origin. Osteogenic sarcoma. Malignant synovioma. Teratogenic tumors – teratoma
-
8/9/2019 Oral Tumors,In Oral Cavity
2/33
17/5/20
CLASSIFICATION OFTUMOURS
Behavioural classification
benign or malignant
Histogenetic classification -cell of origin
Epithelial
Mesenchymal
Mixed
Teratomas
Precise classification of individual tumors isimportant for planning treatment
Principal characteristics of benign andmalignant tumours
Special features of theepithelial tumors indifferent organs
Epithelial tumors
The most often tumors
ectoderm -skin
mesoderm-kidney
endoderm - GIT
Structure the parenchyma
neoplastic epithelial cells
Benign
malignant
non-neoplastic stroma
-
8/9/2019 Oral Tumors,In Oral Cavity
3/33
17/5/20
Epithelial tumors
Benign Papilloma
from the surface epithelium
Adenoma from the glandular epithelium
Malignant carcinomas
Skin Epithelial lining of glands
and ducts Gastro-intestinal tract
Oral cavity, esophagus,stomach, intestine,hepato-biliary system,pancreas
Respiratory passages Nasal cavity, larynx,
trachea, bronchi
Urinary tract epithelium
Male and female genitalsystems
Placental epithelium
Endocrine glands
Tumors of epithelial origin
Tissue of origin Benign Malignant
Special features of epithelialtumors
Benign and malignant epithelial tumors are the mostcommon in adults.
Epithelial cells grow as cohesive groups
Malignancy can be diagnosed by invasion through tissuelayers -basement membrane, muscularis mucosae intact basement membrane in benign tumors
Carcinomas spread generally by lymphatics to lymph nodes,
later -via the blood stream (liver, pulmo, bones)
Treatment is by surgical resection In carcinomas response to radiation and chemotherapy varies
with type
Benign epithelial tumors
2 types according to the epithelium
Papilloma – from the surface epithelium
Skin, urinary tract epithelium
Adenoma – from the glandular epithelium
-
8/9/2019 Oral Tumors,In Oral Cavity
4/33
17/5/20
Papillomas
Tumors with finger-likeprojections
Macroscopic features Exophytic lesions
Rarely endophytic lesions
Histology Papillae
Epithelium lining
Squamous cell epithelium
Transitional epithelium
Preserved basement membrane
Connective tissue core
Squamous cell papilloma
Verrucae skin
viruses
Squamous cell papilloma esophagus larynx
children – juvenile papillomatosis
trachea
precancerosis
Condylomata genitals, anus
condyloma acuminatum HPV (human papilloma virus -1,
2, 4, 7 type) condyloma lata
syphilis
Urothelial papillomas
Transitional epithelium ofureter, bladder, uretra
Precancerosis
Urothelial carcinoma withlow grade malignancy
Histology Fragile papillae
Urine -cytology
Papilloma vesicae urinariae
-
8/9/2019 Oral Tumors,In Oral Cavity
5/33
17/5/20
Adenomas
Glandular epithelium Endocrine glands
functional activity – clinical syndromes Pituitary Thyroid gland Suprarenal glands Endocrine pancreas
Exocrine glands Skin - oil and sweat glands Salivary gland
Adenoma gl. Parotis
Breast Fibroadenoma
Exocrine pancreas Gastrointestinal tracts Respiratory tract Ovarium
Liver
Kidney
Adenomas
Macroscopy
nodules, capsulated
Mucosa surface – pedunculated and sessilepolyps
Single, multiple familial polyposis coli
Various size < 1 cm
> 3 cm
Adenomas
Histology
Glands
Various shape and size
Preserved basementmembrane
± dysplasia
low-grade or high-grade
high grade oftenclassified withcarcinoma-in-situ
may develop into malignancy
Uterine cervix
Colon polyps
Dysplasia
Normal gland
Mild dysplasia Severe dysplasia
Moderate dysplasia
-
8/9/2019 Oral Tumors,In Oral Cavity
6/33
17/5/20
Adenomas
Histological types acinar
Small glands lumen, endocrineglands
trabecular Tarbeculae, liver, suprarenal glands
tubular tubule, GIT
Villous Papillae, GIT
Mixed tubulovilous, GIT
Solid Nests, bronchi
Cystic Papillary cystadenoma – serous,
mucous, ovary
Adenoma рleomorphe glаndulaeparotis
Tumor mixtus
Capsulated,mucinous cut surface
Histology Gland structures
Myoepithelial cells
Mucoid substance
Basophilic
Resemblecartilagous
Fibroadenoma gl. mammae
Female, young age
Capsulated, firmnodules
Histology parenchyma
Gland structures Loose connective tissue
pericanalicular
intracanalicular
Fibrous stroma
Ovarian cystadenoma
-
8/9/2019 Oral Tumors,In Oral Cavity
7/33
17/5/20
Malignant epithelial tumors
= Carcinomas
Risk factors Preneoplastic syndromes –chronic inflammation,
hyperplasia, regeneration
Benign epithelial tumors
Macroscopy Rapid growth – necrosis, haemorrages Noncapsulated Infiltrative Exophytic and endophytic growth
Histology invasion through tissue layers -basement
membrane, muscularis mucosae differentiation
Grading - high-, moderate-, poor differentiation
Metastases Lymph nodes Distant metastases Seeding
TNM staging
Carcinomas
High morbidity andmortality
may be due to: pressure on and destruction
of adjacent tissue
metastases
blood loss from ulceratedsurfaces
obstruction of flow(intestinal obstruction)
paraneoplastic effects
weight loss, cachexia
Carcinomas
From surface epithelium Squamous cell carcinoma
Basal cell carcinoma
Transitional (urothelial)carcinoma
From glandular epithelium
Adenocarcinoma
Hepatocellular carcinoma
Renal cell carcinoma
Seminoma
Choricarcinoma
Poorly differentiated carcinoma
Malignant tumors of surfaceepithelium
Squamous cell carcinoma skin
Face
Oral cavity
leukoplakia
Metaplasia of stratifiedsquamous non-ketatinized
epithelium into keratinized Esophagus
Larynx
Bronchus
Squamous cell metaplasia
Cervix uteri, vagina
http://www.microscopyu.com/galleries/pathology/ovarianadenocarcinoma.html
-
8/9/2019 Oral Tumors,In Oral Cavity
8/33
17/5/20
Squamous cell carcinoma
Histology
atypical cells at alllevels of the epidermis,with nuclear crowdingand disorganization
invasions of basementmembrane
variable differentiation
Keratinization
perls
Squamous cell carcinoma
High differentiation With keratinization
= carcinoma planocellulare keratodes
Moderate differentiation keratinization
Low differentiation Without keratinization
= carcinoma planocellulare non-keratodes
WELL?
MODERATE?
POOR?
Grading for Squamous Cell Carcinoma
Basal cell carcinoma =Ulcus rodens Tumor cells resemble the normal epidermal basal cell layer from
which they are derived
2 patterns: superficial type or nodular lesions
palisading with separation from the stroma, creating a cleft
Slow growth, local invasion, no metastases
-
8/9/2019 Oral Tumors,In Oral Cavity
9/33
17/5/20
Malignant tumors of glandularepithelium
= Adenocarcinoma Breast
Salivary glands
Gastro-intestinal tract
esopagus – Barrett esophagus
stomach – H.pylori gastritis
colon – adenomas
Pancreas
Endocrine glands
Female genital system
endometrium
ovarium
Male denital system testis - seminoma
Adenocarcinomas
Histology
Gland structures
Various shape
cellular atypia
invasion through tissuelayers
basement membranes
muscularis mucosae
Adenocarcinomas
Histological types Mucinous –
Mucin production Intra-, extracellular
"signet-ring" cells
Papillary carcinoma
Cystadenocarcinoma
Adenoacantoma
+ squamous cell metaplasia
Adenosquamous carcinoma
+ squamous cell carcinoma
Mucoepidermoid carcinoma
Mucinous adenosquamouscarcinoma
Adenocarcinoma ventriculi
Intestinal type Diffuse type
-
8/9/2019 Oral Tumors,In Oral Cavity
10/33
17/5/20
1
Adenocarcinoma uteri Seminoma Testis
Choriocarcinoma
Хепатоцелуларен карцином
Hepatocellular carcinoma
-
8/9/2019 Oral Tumors,In Oral Cavity
11/33
17/5/20
1
Renal cell carcinoma
3 types:
Clear Cell Carcinoma
the most often
Papillary Renal CellCarcinoma
Chromophobe RenalCarcinomas
Poorly differentiated carcinomas
Undifferentiatedcarcinomas
2 types
Scirousum stroma – firm
breast
medullare
stroma - soft
Special features of themesenchymal tumors indifferent organs.
Mesenchymal tumors
Soft tissue tumors
Connective/fibrous tissue
Adipose tissue
Muscle tissue
Vascular tissue
Bone tumors
Joint tumors
A broad group of non-epithelial tumors, deriving fromdifferent mesenchymal tissue types
-
8/9/2019 Oral Tumors,In Oral Cavity
12/33
17/5/20
1
SOFT TISSUE TUMORS Tumors of Adipose Tissue
Lipomas Liposarcoma
Tumors and Tumor-like Lesions ofFibrous Tissue Fibroma Nodular fasciitis Fibromatoses Fibrosarcoma
Fibrohistiocytic Tumors Fibrous histiocytoma Malignant fibrous histiocytoma
Tumors of Skeletal Muscle Rhabdomyoma Rhabdomyosarcoma
Tumors of Smooth Muscle Leiomyoma Smooth muscle tumors of uncertain
malignant potential Leiomyosarcoma
Vascular Tumors
Hemangioma
Lymphangioma
Hemangioendothelioma
Hemangiopericytoma
Angiosarcoma
Tumors of UncertainHistogenesis
Synovial sarcoma
Alveolar soft part sarcoma
Epithelioid sarcoma
Granular cell tumor
Mesenchymal tumors
Benign
by adding “-oma” to cell type, from which tumorarise
fibroma, lipoma, chondroma
Malignant
Sarcomas
Fibrosarcoma, liposarcoma, chondrosarcoma
Special features of the mesenchymaltumors
A great diversity of tumors Compared to the epithelial tumors
Appear at any age children adults
Risk factors Physical –trauma, radiation, thermal burn associations Genetic
Chromosome translocations Part of many syndromes
No clear distiction between the tumor’s parenchyma and stroma Mesenchymal origin of the components Diffuse growth
Sarcomas spread generally by via the blood stream to the pulmo, liver Diagnosis
Difficult differentiation between some benign and malignant variants Tumors of borderline malignancy
mitosis
Similar histology – spindle cell type Immunohistochemistry –histogenetic markers
Need of consultation
Chromosomal and Genetic Abnormalities in Soft Tissue Sarcomas
Tumor Cytogenetic Abnormality Genetic Abnormality
Extraosseous Ewing sarcoma andprimitive neuroectodermal tumor
t(11:22)(q24;q12) FLI-1-EWS fusion gene
t(21:22)(q22;q12) ERG-EWS fusion gene
t(7;22)(q22;q12) ETV1-EWS fusion gene
Liposarcoma —myxoid and round celltype
t(12:16)(q13;p11) CHOP/TLS fusion gene
Synovial sarcoma t(x;18)(p11;q11) SYT-SSX fusion gene
Rhabdomyosarcoma —alveolar type t(2;13)(q35;q14) PAX3-FKHR fusion gene
t(1;13)(p36;q14) PAX7-FKHR fusion gene
Extraskeletal myxoid chondrosarcoma t(9;22)(q22;q12) CHN-EWS fusion gene
Desmoplastic small round cell tumor t(11;22)(p13;q12) EWS-WT1 fusion gene
Clear cell sarcoma t(12;22)(q13;q12) EWS-ATF1 fusion gene
Dermatofibrosarcoma protuberans t(17:22)(q22;q15) COLA1-PDGFB fusiongene
Alveolar soft part sarcoma t(X;17)(p11.2;q25) TFE3-ASPL fusion gene
Congenital fibrosarcoma t(12;15)(p13;q23) ETV6-NTRK3 fusion gene
-
8/9/2019 Oral Tumors,In Oral Cavity
13/33
17/5/20
1
SOFT TISSUE TUMORS
Fat (adipose) tissue
Fibrous tissue
Fibrohistiocytic
Skeletal muscle
Smooth muscle
Vascular
Peripheral nerve
Uncertain synovial sarcoma, alveolar soft part sarcoma, epitheliod sarcoma
Tumors of Adipose Tissue
Benign
Lipomas
Malignant
Liposarcoma
Lipoma
Benign tumors of fat
The most common soft tissue tumors ofadulthood.
Solitary lesions Multiple – in rare autosomal dominant
syndromes.
Localization Back, shoulders, thigh
Submucosa of GIT
Macroscopy soft, yellow, well-encapsulated masses
Histology Conventional - mature adipocytes
Varied in size Clear empty cytoplasm Peripheral nucleus
Angiolipoma Numerous capillaries
Treatment com lete excision is usuall curative
Lipoma
-
8/9/2019 Oral Tumors,In Oral Cavity
14/33
17/5/20
1
Liposarcoma Malignant neoplasm of adipocytes
Rare tumors,
Adults, 60-70 y - f > m chromosomal translocation - myxoid liposarcomas
Localization deep soft tissues, retroperitoneum
in visceral sites
Macroscopy relatively well-circumscribed lesions , large size
polylobulated
± myxoid cut surface
Histology Lipoblasts
fetal fat cells with cytoplasmic lipid vacuoles
myxoid liposarcoma Mucoid stroma
Pleomorphic variant Atypical cells, inc. multinuclated cells mitoses
Liposarcoma
Tumors and Tumor-like Lesionsof Fibrous Tissue
Benign
Fibroma
Malignant
Fibrosarcoma
Fibroma
Benign tumor of fibrousconnective tissue
A common tumor of the skin
Macroscopy Capsulated nodule
Histology Fibrocytes
Spindle cells with sharp edgesnuclei
storiform pattern of growth
+ collagen fibers
hard fibroma -fibroma durum
Soft fibroma -fibroma molle
-
8/9/2019 Oral Tumors,In Oral Cavity
15/33
17/5/20
1
Fibroma cutis Fibrosarcomas
Malignant neoplasms composed offibroblasts tend to grow slowly
often recur locally after excision (>50% ofcases)
can metastasize hematogenously (>25% ofcases) - lungs
Adults Localization
deep tissues of the thigh, knee, andretroperitoneal area
Macroscopy soft unencapsulated, infiltrative masses
± areas of hemorrhage and necrosis
Histology all degrees of differentiation spindled cells growing in a herring bone
fashion pleomorphism, mitoses necrosis
Fbrosarcoma Tumors of Smooth Muscle
Leiomyoma
Smooth muscle tumors of uncertainmalignant potential (atypical leiomyomas)
DD leiomyoma/leiomyosarcoma Leiomyosarcoma - > 10/10 HPF mitoses
Leiomyosarcoma
-
8/9/2019 Oral Tumors,In Oral Cavity
16/33
17/5/20
1
Leiomyoma
Benign tumor of smooth muscle cells
Low malignant potential
Localization
Myometrium – multiple nodules
Submucosa, intramural, subserosal
Age – female
estrogen-dependent
Macroscopy
Well circumscribed, grey-white firmnodules, up to 20 cm
Fascicled cut surface
Histology
Spindle cells (smooth muscle), fascicles
Round edges of the nuclei
± fibrosis, calcifications, necrosis, cysts
Leiomyoma (HE)
Leiomyosarcoma
Malignant tumor of smooth musclecells 10% - 20% of sarcomas
Adult, f> m Localization
skin,
Deep tissues of extremities
Retroperitoneum, uterus Local invasion, metastasis
метастази
Macroscopy Large, firm tumor mass
Histology spindle cells with cigar-shaped
nuclei
arranged in interweaving fascicles
Leiomyosarcoma
-
8/9/2019 Oral Tumors,In Oral Cavity
17/33
17/5/20
1
Tumors of Skeletal Muscle
Rhabdomyoma
Rhabdomyosarcoma
More common
Rhabdomyoma
Benign tumor of striated muslecells
Very rare
malformation
Age
Adult type
Fetal type
Localization
Skeletal muscles
Heart
Sclerosis tuberans
Histology
Large round cells with
eozinophilic granular cytoplasm
Rhabdomyosarcoma
Malignant tumor of striated muscle cells > 50% of sarcomas in children
Localization head, neck, face extremties genitourinary tract
sarcoma botryoides -soft, gelatinous, grapelike masses
Macroscopy poorly defined, infiltrating masses
Histology Rhabdomyoblast - round or elongated cells
granular eosinophilic cytoplasm, filaments
Embryonal variant Small round cells
Alveolar variant Alveoli, fibrous septa
Pleomorphic variant
Immunohistochemistry Desmin, myoglobin, actin, myosin
Vascular tumorsTumors of blood vessels and lymphatics
Benign hamartomas, not even true
neoplasms
Intermediate Locally aggressive, rarely metastasize
Malignant
Frequent and early metastases – lungs
Diagnosis “endothelium” lined blood filled
spaces immunohistochemistry - factor VIII
mitosis
Hemangioma
Lymphangioma
Hemangioendothelioma
Angiosarcoma
-
8/9/2019 Oral Tumors,In Oral Cavity
18/33
17/5/20
1
Vascular tumors
Benign
Rare mitosis
Mild, rare atypia
No metastases
Malignant
Common mitosis
Frequent, severeatypia
Early, frequentmetastases
via bloodstream
Hemangioma
= a generic term for any benign blood vesseltumor
Capillary (small vascular spaces) Also called “juvenile”, often called “birth marks”
Usually regress with age
Cavernous (large vascular spaces) Also called “adult”
Usually do not regress
Smooth-muscle hemangioma
Pyogenic hemangioma
Hemangioma
Hаemangioma cavernosum hepatis
-
8/9/2019 Oral Tumors,In Oral Cavity
19/33
17/5/20
1
Pyogenic granuloma
Oral cavity most common
Regress
Histology
like capillary hemangioma
Indistinguishable from normalgranulation tissue
Glomus tumor
Most commonlyunder nail
Small tumor, 1 cm
Painful
Lymphangiomas
Benign lymphatic analogue ofhemangiomas.
Generally rare
Simple (Capillary) Lymphangioma
small lymphatic channels
absence of blood cells
head, neck, axillary subcutaneous tissues
flat lesions - 1 to 2 cm
Cavernous Lymphangioma (Cystic Hygroma) typically found in the neck or axilla of
children
common in Turner syndrome
can be enormous (≤15 cm in diameter), not
encapsulated
Producing gross deformities - neck
composed of dilated lymphatic spaces andconnective tissue stroma, Ly aggregates
Malignant vascular tumors
Angiosarcoma
± vessels lumens
Factor VIII
atypical endothelial cells
Cellular pleomorphism
Mitoses, atypical
Lymphangiosarcoma
After mastectomy
Papillary projections ofatypical endothelial cells
-
8/9/2019 Oral Tumors,In Oral Cavity
20/33
17/5/20
2
Tumors of UncertainHistogenesis
Synovial sarcoma
Alveolar soft part sarcoma
Epithelioid sarcoma
Synovial sarcoma
Uncertain cellular origin, agressive,malignant The cells are not synoviocytes
metastases –lung, bones, LN
Localization Joints - 10%, knee
extrajoints
Young adults Chromosomal translocations t(X;18)
SYT gene (transcription factor)
Histology Biphasic variant
Epithelial-like cells, glands Spindle cells
Monophasic variant Spindle cells – fascicles
DD fibrosarcoma – keratin, EMA
Bone tumors
Bone
Cartilage
Fibrous
Other
Ewing’s “sarcoma”
Giant cell tumor Metastases
Benign
Malignant
Classification of Primary Tumors Involving Bones
Histologic Type Benign Malignant Hematopoietic (40%) Myeloma
Malignant lymphoma
Chondrogenic (22%) Osteochondroma Chondrosarcoma
Chondroma Dedifferentiated chondrosarcoma
Chondroblastoma Mesenchymal chondrosarcoma
Chondromyxoid fibroma
Osteogenic (19%) Osteoid osteoma Osteosarcoma
Osteoblastoma
Unknown origin (10%) Giant cell tumor Ewing’s sarcoma
Giant cell tumor
AdamantinomaHistiocytic origin Fibrous histiocytoma Malignant fibrous histiocytoma
Fibrogenic Metaphyseal fibrous defect(fibroma)
Desmoplastic fibroma
Fibrosarcoma
Notochordal Chordoma
Vascular Hemangioma Hemangioendothelioma
Hemangiopericytoma
Lipogenic Lipoma Liposarcoma
Neurogenic Neurilemmoma
-
8/9/2019 Oral Tumors,In Oral Cavity
21/33
17/5/20
2
Benignosteogenic bone tumors
= Bone Forming, 19% Osteoma
face, skull; 40-50yrs Histology - similar to normal bone
Osteoid Osteoma metaphysis femur, tibia 10-20yrs Histology – similar to woven bone
Osteoblastoma vertebral column 10-20yrs Histology -similar to osteoid osteoma
Osteoma
Solitary tumor
Mean age
Face, skull
Exophytic growth,attached to the bone
Histology similar to normal bone
Frontal sinus
Malignantosteogenic bone tumors
Osteosarcoma (osteogenic sarcoma) Primary
Metaphysis of distal femur, proximal; 10-20 yrs
secondary - associated with pre-existing disorders suchas benign tumors, Paget disease
Femur, humerus, pelvis, > 40 yrs
Histologic variants osteoblastic, chondroblastic, fibroblastic, telangiectatic,
small cell, and giant cell
Different degree of differentiation
The most common subtype is osteosarcoma that arises in the
metaphysis of long bones; solitary, intramedullary, and poorly
differentiated; produces a predominantly bony matrix
Osteosarcoma
-
8/9/2019 Oral Tumors,In Oral Cavity
22/33
17/5/20
2
Sarcoma osteogenes Benign cartilagenous bone tumors
= Cartilage forming, 22%
Osteochondroma (exostosis) Metaphysis of long bones; 10-30 yrs;
Histology - cartilage and bone tissue
Chondroma Small bones of hands and feet; 30-50 yrs; medullary cavity
Histology – hyaline cartilage
Chondroblastoma Knees, epiphyses, teenagers, m>>f, Histology - much less matrix than a chondroma
Chondromyxoid fibroma
Myxoid, atypia
Osteochondroma (exostosis)
Common
Often multiple as ahereditary syndrome
m>>>f
Pelvis, scapulae, ribs
Metaphysis Cartilage and bone
present
Chondroma
Hyaline cartilage
Multiple enchondromas Ollier’s disease
Maffucci syndrome - if hemangiomas present
-
8/9/2019 Oral Tumors,In Oral Cavity
23/33
-
8/9/2019 Oral Tumors,In Oral Cavity
24/33
17/5/20
2
Giant cell tumor of bone
Localization
epiphysis of long bones
cortical lesions
Young adults -20-40 yrs
Histology Macrophages
Giant cells
Ewing sarcoma (tumor)
PNET (primitiveneuroectodermal tumor)
Localization Diaphysis and metaphysis
medullary lesions
Age -10-20 yrs Chromosomal translocation
-t(11;22)
FLI-EWS gene fusion
Histology - small roundcells Resemble lymphoma
Tumors of the central nervous system
General features of the CNS tumors
85 % - intracranial, 15% - intraspinal tumors primary tumors and metastatic
20% of all - tumors of childhood. differ from those in adults both in histologic subtype and location
arise in the posterior fossa ( in adults -mostly supratentorial)
Tumors of the nervous system have unique characteristics Histologic distinction between benign/malignant lesions – not clear
low-grade lesions (low mitotic rate, cellular uniformity, and slowgrowth) may infiltrate large regions of the brain
The anatomic site of the neoplasm - lethal consequencesirrespective of histologic classification
A benign meningioma in the medulla cardiorespiratory arrest
The ability to resect a lesion may be limited
The pattern of spread of primary CNS neoplasms differs from thatof other tumors -rarely metastasize outside the CNS
the subarachnoid space - a seeding along the brain and spinal cord
-
8/9/2019 Oral Tumors,In Oral Cavity
25/33
17/5/20
2
CNS TUMORS
GLIOMAS
Astrocytoma (I, II, III, IV) Oligodendroglioma
Ependymoma
MENINGIOMAS
NEURONAL
POORLY DIFFERENTIATED (medulloblastoma)
LYMPHOMAS
METASTATIC
CNS TUMORS
Symptoms? Headache Vomiting
Mental Changes
Motor Problems Seizures Increased Intracranial Pressure
any localizing CNS abnormality
CNS TUMORS
History
Physical Neurologic exam
LP (including cytology)
CT MRI
Brain angiography
Biopsy
Gliomas
Tumors of the brain parenchyma thathistologically resemble different types
of glial cells
astrocytomas,
oligodendrogliomas ependymomas
-
8/9/2019 Oral Tumors,In Oral Cavity
26/33
17/5/20
2
Astrocytomas
Different categories of astrocytictumors
characteristic histologic features
distribution within the brain
age groups
Fibrillary
Pilocytic astrocytomas
Fibrillary astrocytomas
80% of adult primarybrain tumors
Age – 40 -60 y Localization
cerebral hemispheres seizures, headaches, and
focal neurologic deficits
Macroscopy a poorly defined, gray,
infiltrative tumor
cut surface - firm, or soft orgelatinous
± cystic degeneration andhemorrhage
Fibrillary astrocytomas
Microscopy I –IV grades
cellularity
nuclear pleomorphism
necrosis
mitoses
Astrocytoma (I, II gr. Anaplastic astrocytoma (III
gr.)
Glioblastoma- IV grade vascular or endothelial cell
proliferation and pseudo-palisading nuclei
Astrocytoma
-
8/9/2019 Oral Tumors,In Oral Cavity
27/33
17/5/20
2
Glioblastoma MultiformePilocytic Astrocytoma
Relatively benign tumors
Age - children and young adults
Localization
Cerebellum,
in the floor and walls of the thirdventricle
the optic nerves
Macroscopy
well circumscribed, often cystic
with a mural nodule in the wall of thecyst
Microscopy
areas with bipolar cells with long, thin"hairlike" processes, GFAP (+)
Rosenthal fibers (eosinophilic granularbodies)
Necrosis and mitoses are rare.
Oligodendrogliomas
Frequency -5-15% Age – 40-50 y Localization
cerebral hemispheres
Macroscopy infiltrative tumors - gelatinous, gray ± cysts, focal hemorrhage, and calcifications
Microscopy sheets of regular cells with spherical nuclei
containing finely granular chromatin (similarto normal oligodendrocytes) surrounded by aclear halo of cytoplasm
a delicate network of anastomosingcapillaries.
Calcifications
Mitoses -rare Except in anaplastic oligodendroglioma
Oligodendrogliomas
-
8/9/2019 Oral Tumors,In Oral Cavity
28/33
17/5/20
2
Ependymoma
Frequency -5-10%
Age – 10-20 y
Localization
IV –th ventricle hydrocephalus
Macroscopy
solid or papillary masses
Microscopy
cells with regular, round to ovalnuclei with abundant granularchromatin
perivascular pseudo-rosettes
Variants
Anaplastic increased cell density, high
mitotic rates, necrosis
Ependymoma
Poorly Differentiated NeoplasmsMedulloblastoma
Neuroectodermal cells Age - children Localization
cerebellum (vermis)
Макроскопски well circumscribed, gray,
friable
Histology with sheets of anaplastic
("small blue") cells with little cytoplasm and
hyperchromatic nuclei Rossetes of Homer-Wright
mitoses – abundant
Medulloblastoma
-
8/9/2019 Oral Tumors,In Oral Cavity
29/33
17/5/20
2
Meningiomas
Benign tumors of adults
from the meningothelial cell of thearachnoid
Localization any of the external surfaces of the
brain
ventricular system
from the arachnoid cells of the
choroid plexus
Macroscopy well-defined dural-based masses
compress underlying brain
Meningiomas
Microscopy -variants
Fibroblastic - with elongated cells andabundant collagen deposition
Psammomatous - with numerouspsammoma bodies
Secretory - with PAS-positiveintracytoplasmic droplets
Microcystic - with a loose, spongyappearance
Atypical meningiomas – mitosis
Anaplastic (malignant) meningiomas resemble a high-grade sarcoma
MeningeomaMetastatic brain tumors
Most common brain tumor inadults.
Common primary sites:melanoma, lung, breast, GItract, kidney.
Most are in cerebrum in gray-white junctions due to
rich capillarity
Single or multiple.
Discrete, globoid, sharplydemarcated tumors
amenable to surgical resection.
-
8/9/2019 Oral Tumors,In Oral Cavity
30/33
17/5/20
3
Tumors of the peripheralnervous system
Tumors of the peripheralnervous system
Arise from cells of the peripheral nerve
Schwann cells,
perineurial cells
Fibroblasts
Schwannoma
Neurofibroma
Malignant Peripheral Nerve Sheath Tumor
Schwannoma
From Schwann cells
Symptoms – due to local compression
Localization
in the cerebellopontine angle -attached tothe vestibular branch of the 8 th nerve(vestibular schwannoma)
sensory nerves, large nerve trunks
Macroscopy
well-circumscribed encapsulated massesthat are attached to the nerve
Morphology – 2 growth patterns
Schwannoma Antoni A - Antoni B
Antoni A pattern of growth
elongated cells with cytoplasmicprocesses - fascicles
Verocay bodies
the "nuclear-free zones" ofprocesses that lie between the
regions of nuclear palisading
Antoni B pattern of growth less densely cellular areas
microcysts and myxoid changes
Immuhistochemistry
S-100 protein
-
8/9/2019 Oral Tumors,In Oral Cavity
31/33
17/5/20
3
Neurofibroma
Well differentiated, benign
Form whorls of fibroblasts
Two types:
Classic form
Cutaneous / nerves – solitary
collagen matrix, spindle cells,
Plexiform
Neurofibromatosis type 1
Multiple, infiltrative
Myxoid stroma
Malignant Peripheral NerveSheath Tumor
Sarcoma Highly malignant
multiple recurrence
metastases
Origin De novo plexiform neurofibroma
Macroscopy poorly defined tumor masses
±infiltration along the axis of nerve
± invasion of adjacent soft tissues
Histology the tumor cells resemble Schwann cells - elongated nucleiand prominent bipolar processes, fascicle formation
Mitoses, necrosis, nuclear anaplasia
Tumors and Tumor-LikeLesions of Melanocytes
Benign – melanocytic nevusMalignant - melanoma
Melanocytic nevus
Benign congenital or acquiredneoplasm of melanocytes
Numerous types, with varied clinicalappearance
Macroscopy relatively small,
symmetric,
and uniformly pigmented
Morphology Junctional
more pigmented,
more closely associated withmelanoma)
Intradermal
Compound (both)
-
8/9/2019 Oral Tumors,In Oral Cavity
32/33
17/5/20
3
Melanocytic nevus
Junctional nevus
Dermal nevus
MALIGNANT MELANOMA
Malignant proliferations of melanocytes.
Incidence rising, Related to sun like all other skin cancers
The only primary skin cancer that canquickly metastasizes
Sporadic
Hereditary -5-10% Germ-line mutations in the CDKN2A gene
(9p21)
MALIGNANT MELANOMA
Difficult to differentiate fromnevus clinically often microscopically
Clinical features Skin
a change in the color or size of apigmented lesion
less common sites - oral andanogenital mucosal surfaces, theesophagus, the meninges, eye.
Morphology Vertical growth phase
Horizontal growth phase Related with prognosis
Breslow, Clark’s staging
MALIGNANT MELANOMA
Morphology
Malignant cells with largenuclei with irregularcontours
chromatin characteristicallyclumped at the periphery ofthe nuclear membrane
prominent eosinophilicnucleoli -"cherry red"
nests or individual cells atall levels of the epidermis
-
8/9/2019 Oral Tumors,In Oral Cavity
33/33
17/5/20
MALIGNANT MELANOMA Teratomas
=mixed tumors originate from totipotential stem cells
the capacity to differentiate into any of the celltypes found in the adult body
Ovary, testis
3 variants Mature teratomas
contain fully differentiated tissues from one ormore germ cell layers
neural tissue, cartilage, adipose tissue, bone,epithelium in a haphazard array
Immature teratomas contain immature somatic elements reminiscent
of those in developing fetal tissue mediastinum
Teratomas with malignancies malignancy in preexisting teratomatous elements
squamous cell carcinoma or adenocarcinoma Mixed germ cell tumors of testis, 40%
combination of teratoma, embryonalcarcinoma, and yolk sac tumors.
Cystic teratoma of ovary