Oral cavity and salivary gland diseases
50
Oral Cavity Diseases Dr Nor Hidayah Abu Bakar, M.D, M.Path (Anatomic Pathologist), Medical Lecturer, FPSK, UNISZA
-
Upload
norhidayahabubakar -
Category
Health & Medicine
-
view
361 -
download
5
description
oral cavity and salivary glands diseases
Transcript of Oral cavity and salivary gland diseases

Oral Cavity Diseases
Dr Nor Hidayah Abu Bakar,M.D, M.Path (Anatomic Pathologist), Medical
Lecturer,FPSK, UNISZA

Learning objectives
• Outline vesicular (ulcerative), reactive tumour-like and pre-neoplastic lesions (leukoplakia, erythroplakia)
• Outline oral lesions in systemic diseases• Outline dental caries, gingivitis and periodontitis• Describe oral squamous cell carcinoma regarding the
etiology and pathogenesis and the pathology• Describe benign and malignant salivary gland
neoplasms regarding the pathology and the clinical manifestations

Oral cavity
• Diseases of the oral cavity divided into 2 groups, those affecting the soft tissues (include salivary glands) & those involving the teeth.

Non Neoplasia :1) Ulceration and
inflammatory lesions2) Proliferative lesions
(reactive/ tumour-like)3) Pre-neoplastic lesions
(Leukoplakia and erythroplakia)
Neoplasia:Squamous cell
carcinoma

Oral inflammatory lesions
• Aphthous ulcers (Canker sores)• Herpes Simplex Virus Infections• Oral Candidiasis (Thrush)

Aphthous Ulcers (Canker Sores)
• Common superficial mucosal ulcerations
• Up to 40% of the population.• First 2 decades of life• Extremely painful• Cause : unknown• More prevalent within some families• May be associated with celiac
disease, inflammatory bowel disease (IBD) and Behcet disease.
• Resolve spontaneously in 7 to 10 days but can recur.

• Gross: Small (<5mm)-round with superficial erosion with gray-white exudate & surrounded by erythematous rim, tender.
• Location: single or in groups on the non-keratinised oral mucosa on the soft palate, buccolabial mucosa, floor of the mouth and lateral borders of the tongue.

Herpes Simplex Virus Infections• Aetiology :
– Herpes simplex virus (HSV) type I, – HSV type II (herpes genitalis)
• Clinical features and pathogenesis:– Primary infection in children 2-4 y.o – Usually asymptomatic, dormant virus in the nerve ganglia &
can be reactivated.– Some manifests as acute herpetic gingivostomatitis –
generalised vesicles and ulcerations– Causes of reactivation: trauma, allergies, UV light exposure,
URTI, pregnancy, menstruation, immunosuppression, exposure to extreme temperature
– Self healing, resolved within 7-10 days.– antiviral agents are available.

Pathology :• Gross: Solitary or multiple
small (<5mm) vesicles containing clear fluid. Once rupture, shallow + painful ulcers.
• Location: On lips or about nasal orifices (also known as cold sores or fever blisters).

HPE: Blister in mucosa. Ballooned cells having large eosinophilic intranuclear herpes simplex inclusion bodies.

Oral Candidiasis
• Most common fungal infection of the oral cavity
• C. albicans - Normal oral flora
• Became disease when impaired protective mechanisms.
• Common in DM, anemia, on antibiotics or glucorticoid therapy, immunodeficiency.

• Gross: Adherent white, curdlike,circumscribed plaque, that can bescrapped off revealing an underlying granular erythematous inflammatory base.• HPE: fungal organisms superficiallyattached to the underlyingmucosa-pseudohyphae, ovoid yeastform

Summary: Oral inflammatory lesions
• Aphthous ulcers are painful superficial ulcers of unknown etiology that may be associated with systemic diseases.
• Herpes simplex virus causes self-limited infection that presents with vesicles (cold sores, fever blisters) that rupture and heal, without scarring, and often leave latent virus in nerve ganglia. Reativation can occur.
• Oral candidiasis may occur when the oral microbiota is altered. Invasive disease may occur in immunosuppressed individuals.

Proliferative lesions of the oral cavity (reactive/tumour-like)
• Fibrous proliferative lesions :– fibromas, – pyogenic granuloma

Fibromas
• Submucosal nodular fibrous tissue masses • Chronic irritation causes reactive connective
tissue hyperplasia• Site : buccal mucosa along the bite line• Tx : – complete surgical excision– Removal of the source of
irritation

Pyogenic granulomas• Pedunculated mass,• Location : gingiva of children, young adults
and pregnant women• Richly vascular, ulcerated, red to purple
colour• Growth can be rapid – simulate malignant
neoplasm• HPE : dense proliferation of immature
vessels.• Can regress, mature into dense fibrous
masses or develop into a peripheral ossifiying fibroma
• Tx : complete surgical excision

Pre-neoplastic lesions
• Leukoplakia• Erythroplakia

Leukoplakia
• Leukoplakia=whitish, well-defined mucosal patch or plaque caused by epidermal thickening or hyperkeratosis.
• Cannot be scraped off.• Unknown cause.• In older men (40-70 y.o), • Site: vermilion border of the lower lip, buccal
mucosa, hard & soft palates, floor of the mouth and others intraoral sites.

• Localised or multifocal/diffuse, smooth or rough, leathery, white, discrete areas of mucosal thickening.
• HPE: Variable - hyperkeratosis without epithelial dysplasia to mild to severe dysplasia that merges with carcinoma in situ.
• 3-25% undergo transformation to SCC.
• Must be considered precancerous until proven histologically.

Erythroplakia
• Erythroplakia= red, velvety, granular, flat or slightly depressed mucosa, poorly defined irregular boundaries.
• Much greater risk of malignant transformation• HPE: Marked epithelial dysplasia• Etiology : multifactorial, tobacco use is the
most common risk factor for leukoplakia and erythroplakia.


Oral lesions in systemic diseases
Hairy Leukoplakia• White confluent fluffy patches on lateral boarder of
the tongue that CANNOT BE SCRAPED OFF• Immunocompromised patients (80% HAVE HIV, 20%
in others eg. Cancer therapy, transplant immunosuppression)
• CAUSED BY EBV • Not a pre malignant condition
Hairy Leukoplakia histology:• Hyperkeratosis (thickening of the stratum corneum)• Acanthosis (increased thickness of stratum
spinosum)• +/- koilocytosis (clear area around the nucleus,
known as a perinuclear halo)• No dysplasia

Oral lesions in systemic diseases

Dental caries
• Due to food degradation of the tooth structure• Most common cause of tooth loss before age 35• Pathogenesis : bacteria ferments sugar from
carbohydrate →acid metabolic end products → mineral dissolution of tooth structure
• Prevention : – Good oral hygiene– Increase flouride intake. Mech :flourides incorporates into
crystalline structure of the enamel→forms flouroapatite ( resistance to degradation by bacterial acids)

Gingivitis
• Gingiva : squamous mucosa in between the teeth and around them.
• Gingivitis : inflammation of the mucosa and associated soft tissues.
• Due to lack of proper oral hygiene→accumulation of dental plaque and calculus
• Dental plaque is a sticky, colourless biofilm that builds in between and on the surface of the teeth,
• Components of dental plaque: – oral bacteria, – proteins from oral saliva – desquamated epithelial cells

• Plaque become mineralized to form calculus.• Bacteria in the plaque release acids from sugar
rich foods → erode enamel surface→dental caries
• Plaque build-up beneath the gumline cause gingivitis (gingival erythema, edema, bleeding, changes in contour, loss of tissue adaptation to the teeth.
• Reversible disease• Tx: reduce accumulation of plaque and calculus
via brushing, flossing and regular dental visits.

Periodontitis
• Inflammatory process affecting the supporting structures of the teeth : periodontal ligaments, alveolar bone and cementum
• May cause complete destruction of periodontal ligament and alveolar bone →loss of attachment → loosening and loss of teeth.

• Pathogenesis : – shift in the types and proportion of bacteria along
the gingiva ( from facultative gram-positive organisms to anaerobic and microaerophilic gram-negative flora)
– poor oral hygiene

• Can be associated with several systemic
diseases : AIDS, leukemia, Crohn’s disease, diabetes mellitus, Down Syndrome, sarcoidosis and syndrome associated with polymorphonuclear defects (Chediak-Higashi syndrome, agranulocytosis and cyclic neutropenia)
• Can also be etiologic factor for systemic diseases : infective endocarditis, pulmonary and brain abscess and adverse pregnancy outcome.

Neoplastic lesion of the oral cavity
• Oral squamous cell carcinoma

Oral squamous cell carcinoma
• Most common cancer of the oral cavity and tongue
• >40 years old• Risk factors: – tobacco use, alcohol abuse, Human papillomavirus
types 16 and 18 (oncogenic types) infection

• Pathogenesis :
1 - chronic alcohol and tobacco users : exposure to carcinogens →gene mutation (p53 and gene regulating maturation of squamous cells)
2 – infection by oncogenic variants of HPV→ overexpress p16 (a-cyclin-dependent kinase inhibitor), occurs in tonsillar crypts/ base of tongue.

• Clinical: Asymptomatic; local pain or difficulty in chewing
• Common sites : ventral surface of the tongue, floor of the mouth, lower lip, soft palate, gingiva

Pathology :Gross : raised, firm, pearly plaque or irregular, rough or verrucous mucosal thickening.Background of leukoplakia/erythroplakiaLater may ulcerate and protrude out with irregular and indurated or rolled border.

• Micro : dysplastic squamous cells infiltrating the underlying connective tissue stroma

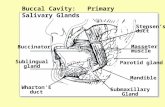
Salivary Gland Diseases
Non-neoplasia1. Xerostomia2. Sialadenitis
Neoplasia1. Benign
2. Malignant

Xerostomia• Dry mouth due to decrease production of saliva• Causes : autoimmune syndrome (Sjogren
Syndrome), radiation therapy, tx with anticholinergic, antidepressant/ antipsychotic, diuretic, antihypertensive, sedative, muscle relaxant, antihistamine
• Pathology : dry oral mucosa, atrophy of tongue papillae, fissure, ulcer, enlarge salivary glands
• Complications : dental caries, candidiasis, difficulty in swallowing and speaking.

Sialadenitis
• Caused by trauma, viral, bacterial or autoimmune.
• Trauma: Mucocele - caused by blockage or rupture of salivary gland duct with consequent leakage of saliva into the surrounding tissue. Fluctuant swelling of lower lip.

• Viral: Mump, paramyxovirus, influenza, parainfluenza viruses. Diffuse interstitial inflammation with oedema & mononuclear cell infiltration ± focal necrosis.
• Bacterial: Staphylococcus aureus, Streptococcus viridans. Often secondary to ductal obstruction resulting from stone formation.
• Autoimmune disease eg Sjören syndrome cause chronic sialadenitis- due to decreased production of saliva with subsequent inflammation.



Summary : Lesions of the oral cavity
• Fibromas and pyogenic granulomas are common reactive lesions of the oral mucosa
• Leukoplakias are mucosal plaques that may undergo malignant transformation
• The risk of malignant transformation is greater in erythroplakia (relative to leukoplakia)
• A majority of oral cavity cancers are squamous cell carcinomas
• Oral squamous cell carcinomas are classically linked tobacco and alcohol use, but the incidence of HPV associated lesions is raising.

Salivary Glands Neoplasia
• Often affected parotid glands• Most are benign; but as size of gland decreases, the
risk of malignancy increase (parotid>submaxillary>sublingual>minor salivary glands)
• Most common: Pleomorphic adenoma (mixed tumour of salivary glands); may recur; 2-3% transform into carcinoma ex pleomorphic adenoma
• Most common malignant tumour: Mucoepidermoid carcinoma.

• Usually occurs in adult• Female predominance• Swelling, 4-6 cm• Mobile on palpation• Not able to differentiate benign or malignant
lesions on clinical ground.

Salivary Gland Tumours
Benign
• Pleomorphic adenoma (50%)
• Warthin tumour (5%)• Oncocytoma (2%)• Cystadenoma (2%)• Basal cell adenoma (2%)
Malignant
• Mucoepidermoid carcinoma (15%)
• Acinic cell carcinoma (6%) • Adenocarcinoma, NOS (6%)• Adenoid cystic carcinoma
(4%)• Malignant mixed tumour
(3%)

Pleomorphic adenoma
• Common in parotid• Painless, slow growing, mobile mass• Pathology : – Gross : rounded, well demarcated mass, encapsulated– Gray white cut surface– Microscopic : mixture of both epithelial and mesenchymal components in the tumour.
• Tx : complete excision• Malignant transformation.

Mucoepidermoid carcinoma
• Common in parotid• Most common form of malignant
tumour of salivary glands• Gross : circumscribed, lack capsule, infiltrative
border• Pale gray to white cut surface, with small cysts• Microscopic : Mixture of squamous cells, mucus
secreting cells and intermediate cells.• Subclassified as low-, intermediate-, or high-
grade.

Acinic cell carcinoma
Warthin Tumour (benign)
Adenoid cystic carcinoma
Other tumours:

Summary:
• Sialadenitis can be caused by trauma, infection or an autoimmune reaction
• Pleomorphic adenoma is a slow-growing neoplasm composed of a heterogenous mixture of epithelial and mesenchymal cells.
• Mucoepidermoid carcinoma is a malignant neoplasm of variable biologic aggressiveness that is composed of a mixture of squamous and mucous cells.

Thank you