Acute Glomerulonephritis - e-learning.kku.ac.th
28
Acute Glomerulonephritis Assoc. Prof. Suwannee Wisanuyotin Department of Pediatrics , K K U
Transcript of Acute Glomerulonephritis - e-learning.kku.ac.th
Acute Glomerulonephritis
Assoc. Prof. Suwannee Wisanuyotin
Department of Pediatrics, KKU
Objectives
◼ Etiology of AGN in children
◼ APSGN
➢ Etiology
➢ Epidemiology
➢ Pathogenesis
➢ Clinical manifestations
➢ Investigatios
➢ Treatment
➢ Prognosis
AGN
Acute inflammation of glomeruli
(mostly immunologic process)
Edema, oliguria, HTN, hematuria, proteinuria, azotemia
Etiology
Common
-Post infectious GN
APSGN
Other systemic infections
Etiology (cont.)
Less common
-HSP
-MPGN
-IgA nephropathy
-SLE
-Familial nephritis
-IE-related
-Shunt nephritis
Etiology (cont.)
Uncommon
-Wegener’s granumatosus
-Polyarteritis nodosa
Acute Post-streptococcal Glomerulonephritis
(APSGN)
Etiology
-Gr A β-hemolytic streptococcus
(nephritogenic strain)
-Pharyngitis, pyoderma
Epidemiology
-Age 2-12 yr (esp. 5-6 yr)
-M : F = 1.7-2:1
-Sporadic, epidemic
-Crowd, poor hygiene, malnutrition,
anemia, parasitic infestation
Pathogenesis
Streptococcal infectionLatent period
Immune-mediated process
Complement activation
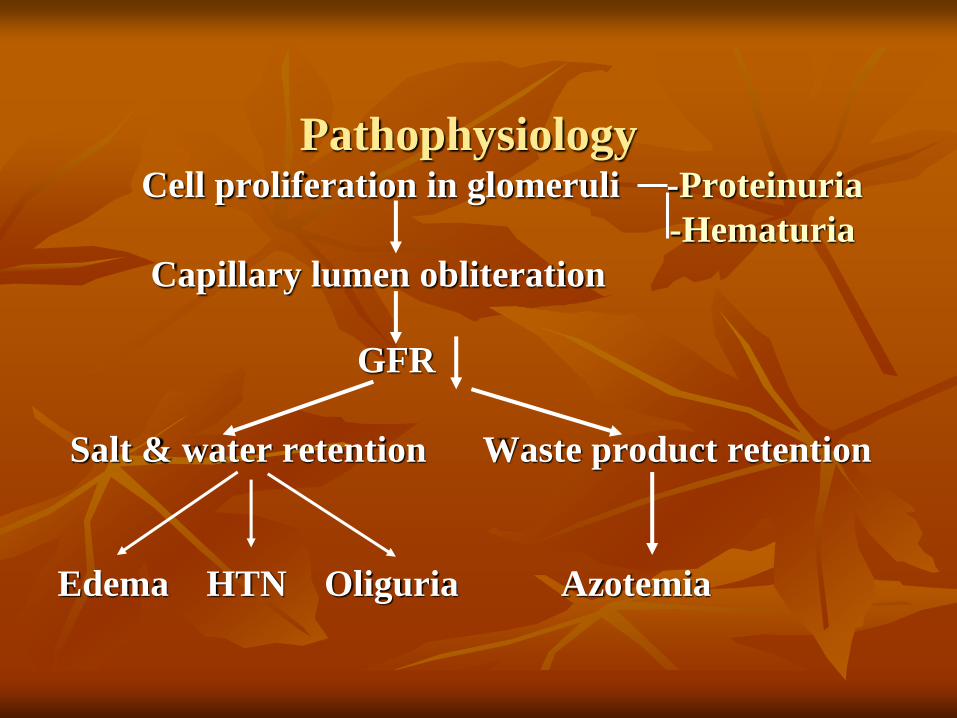
PathophysiologyCell proliferation in glomeruli -Proteinuria
-Hematuria
Capillary lumen obliteration
GFR
Salt & water retention Waste product retention
Edema HTN Oliguria Azotemia
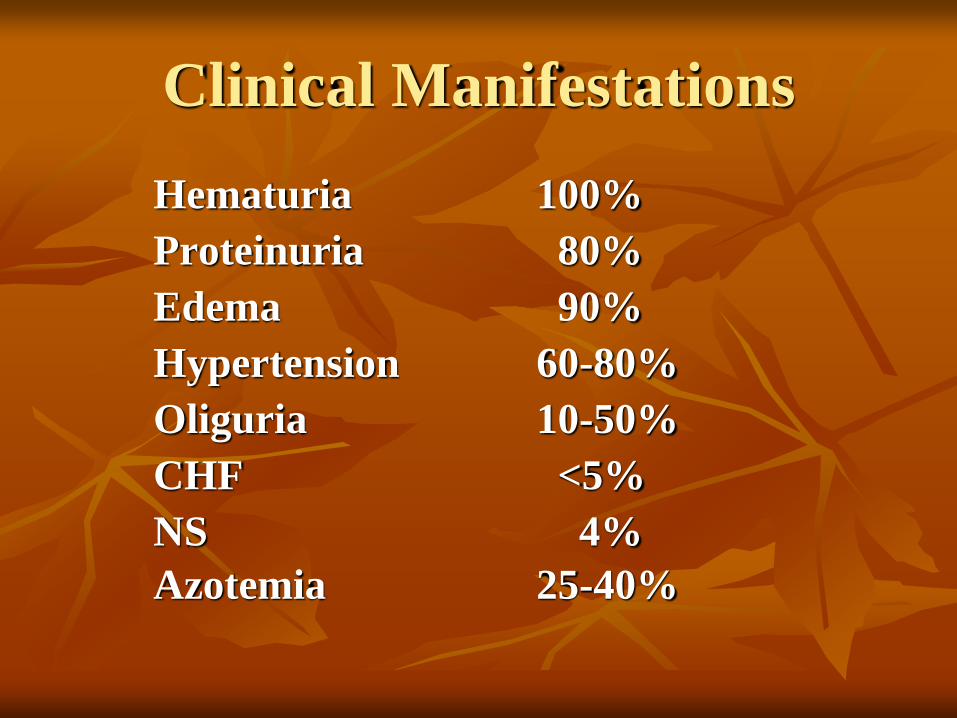
Clinical Manifestations
Hematuria 100%
Proteinuria 80%
Edema 90%
Hypertension 60-80%
Oliguria 10-50%
CHF <5%
NS 4%
Azotemia 25-40%
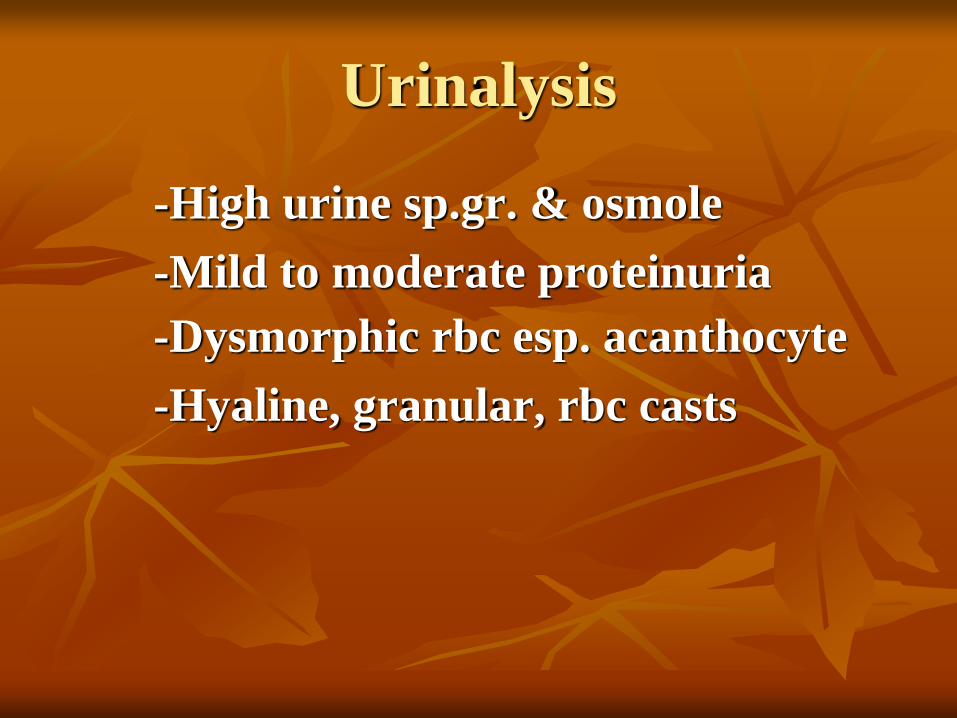
Urinalysis
-High urine sp.gr. & osmole
-Mild to moderate proteinuria
-Dysmorphic rbc esp. acanthocyte
-Hyaline, granular, rbc casts
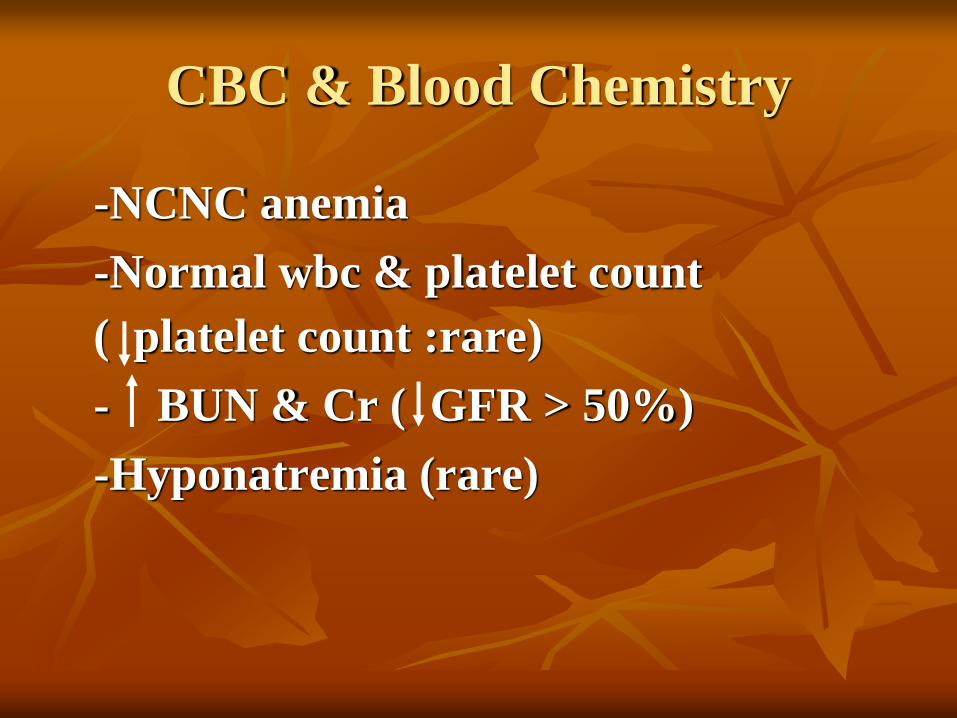
CBC & Blood Chemistry
-NCNC anemia
-Normal wbc & platelet count
( platelet count :rare)
- BUN & Cr ( GFR > 50%)
-Hyponatremia (rare)
Evidence of Streptococcal Infection
-Antibody : ASO, antiDNase B, AHT,
anti NADase, antistreptolysin
-Culture : TSC, pus C/S
Complement
- CH50, C3 (6-8 wks)
- Normal C4
AGN : Low C3
- Acute postinfectious GN
- LN
- MPGN
- SBE
- Shunt nephritis
AGN : Normal C3
- HSP
- IgA nephropathy
- Idiopathic RPGN
- Wegener’s granulomatosis
Differential Diagnosis
- LN
- MPGN
- HSP
- IgA nephropathy
- RPGN
Indication for admission
- Severe hypertension
- Severe edema
- Dyspnea, orthopnea
- Renal failure
- Anuria
Treatment
- Bed rest : esp. in HTN, dyspnea, gross
hematuria
- Water : IL + UO
Treatment (cont.)
- Diet
Energy : RDA
Salt : < 1/3 – 1/2 of maintenance
Na+
Protein : restriction if renal failure
Potassium : restriction if renal failure
or severe oliguria
Treatment (cont.)
- Drugs
Diuretics : Furosemide
X Mannitol
Antihypertensive drugs :
hydralazine, CCB
hypertensive encephalopathy →
Nicardipine, labetalol,
sodium nitroprusside
Treatment (cont.)
◼ Drugs
Antibiotics : Pen V, amoxycillin,
erythromycin if TSC or pus C/S +
X Prednisolone
Clinical Course
- Recovery in 7-10 d ( urine, edema,
HTN, BUN & Cr)
- Gross hematuria 2-3 wks
- Normalized C3 in 6-8 wks
- Proteinuria 3-6 mo
- Microscopic hematuria 1-2 yr
Kidney biopsy
X Typical APSGN
Severe disease (NS, RPGN)
Atypical APSGN
Prognosis
- CRF < 2%
- Recurrence < 0.7-7%
- Poor prognostic factors
Adult onset
RPGN
NS
Avoid vigorous exercise 1 yr
References
◼ Pediatric Nephrology. 7th ed.
◼ ต ำรำวชิำกมุำรเวชศำสตร์ คณะแพทยศำสตร์ มหำวทิยำลยัขอนแก่น 2556, 2564
◼ ปัญหำสำรน ำ้ อเิลก็โทรไลต์ และโรคไตในเดก็ ของชมรมโรคไตเดก็แห่งประเทศไทย ฉบับเรียบเรียงคร้ังที่ 5
◼ โรคไตที่พบบ่อยในเดก็. สุวรรณ ีวษิณุโยธิน. 2557