Individual Case Study Acute Glomerulonephritis
33
Christ the King College 9014 Gingoog City ACUTE GLOMERULONEPHRITIS NCM 103 Submitted to: Mrs. Vilma S. Ramoso Submitted by: Stephanie A. Reyes
-
Upload
monique-reyes -
Category
Documents
-
view
74 -
download
0
description
Case Study Individual: Acute Glumerulonephritis
Transcript of Individual Case Study Acute Glomerulonephritis

Christ the King College
9014 Gingoog City
ACUTE GLOMERULONEPHRITIS
NCM 103
Submitted to:
Mrs. Vilma S. Ramoso
Submitted by:
Stephanie A. Reyes

Acknowledgement
This dissertation would not have been possible without the guidance and the help of the people who contributed and extended their valuable assistance in the
preparation and completion of this study. Many helped shaped and completed this work and I wish to acknowledge them whose help is instrumental in the
realization of this endeavor:
To our school, Christ the King College, the source of our understanding and the residence of our learning.
To our acting dean of the Nursing Program, Mr. Tristan Jay I. Galarrita, RN, for his resilient leadership and organization for the likelihood of our hospital exposure.
To my dear beloved Clinical Instructor Mrs. Vilma S. Ramoso for extending and sharing her knowledge about nursing care and also for abiding with me during our
area work; and for your constructive insights and motivation.
To the staff of the hospital, for leading me with my performance, And to the client for allowing me to do my assessment during her Hospitalization.
To my dear mother, brother, sister, classmates, and friends, for their spirit-warming inspiration and unceasing prayers.
And above all, to our Almighty God, our creator, who gives me abundant wisdom and countless love for the strength and guidance in the preparation and
completion of this work.

Table of Contents:
I. Introduction
II. Objectives
III. Developmental Theories
IV. Client’s Profile
V. Nursing History of Illness
VI. Anatomy and Physiology
VII. Pathophysiology
VIII. Laboratory Examinations
IX. Nursing Management
X. Discharge Planning
XI. Health Teaching
XII. Nursing Care Plan
XIII. Drug Study
XIX. Bibliography

I. Introduction
Acute glomerulonephritis refers to a specific set of renal diseases in which an immunologic mechanism triggers inflammation and proliferation of glomerular tissue that can result in damage to the basement membrane, capillary endothelium. Acute nephrotic syndrome is a group of disorders that cause inflammation of the internal kidney structures (specifically, the glomeruli). In acute glomerulonephritis, the kidneys are normal in size or enlarged and edematous, and the surface of the kidney may show punctuate hemorrhages. With the development of the microscope, Langhans was later able to describe these pathophysiologic glomerular changes. Acute glomerulonephritis is defined as the sudden onset of hematuria, proteinuria, and red blood cell casts. This clinical picture is often accompanied by hypertension, edema, and impaired renal function. As will be discussed, acute glomerulonephritis can be due to a primary renal or systemic disease. Symptoms of acute glomerulonephritis include the following: Hematuria is a universal finding, even if it is microscopic. Gross hematuria is reported in 30% of pediatric patients. Edema (peripheral or periorbital) is reported in approximately 85% of pediatric patients; edema may be mild (involving only the face) to severe, bordering on a nephrotic appearance .Headache may occur secondary to hypertension; confusion secondary to malignant hypertension may be seen in as many as 5% of patients. Shortness of breath or dyspnea on exertion secondary to heart failure or pulmonary edema; usually uncommon, particularly in children. Possible flank pain secondary to stretching of the renal capsule. Hypertension is seen in as many as 80%of affected patients. Hematuria, either macroscopic (gross) or microscopic, may be noted.
Skin rashes may be observed. Abnormal neurologic examination or altered level of consciousness occurring, because of malignant hypertension or hypertensive encephalopathy. Arthritis may be noted. The most common cause is post infectious. Cases of acute nephritis often progress to a chronic form. This progression occurs in as many as 30% of adult patients and 10% of pediatric patients. Glomerulonephritis is the most common cause of chronic renal failure (25%).The mortality rate of acute glomerulonephritis in the most commonly affected age group, pediatric patients, has been
Reported at 0-7%. A male-to-female ratio of 2:1 has been reported. Most cases occur in patients aged 5-15 years. Only 10% occur inpatients older than 40 years. Acute nephritis may occur at any age, including infancy.
On the other hand, a urinary tract infection (UTI) is a bacterial infection that affects any part of the urinary tract. The main etiologic agent is Escherichia coli. Although urine contains a variety of fluids, salts, and waste products, it does not usually have bacteria in it. When bacteria gets into the bladder or kidney and multiply in the urine, they may cause a UTI. Infections of the

urinary tract are the second most common type of infection in the body. Urinary tract infections (UTIs) account for about 8.3 million doctor visits each year. Women are especially prone to UTIs for reasons that are not yet well understood. One woman in five develops a UTI during her lifetime. UTIs in men are not as common as in women but can be very serious when they do occur. The most common type of UTI is acute cystitis often referred to as a bladder infection. An infection of the upper urinary tract or kidney is known as pyelonephritis, and is potentially more serious. Although they cause discomfort, urinary tract infections can usually be easily treated with a short course of antibiotics.
Symptoms include frequent feeling and/or need to urinate, pain during urination, and cloudy urine. The first step is to identify the infecting organism and the drugs to which it is sensitive. Usually, doctors recommend lengthier therapy in men than in women, in part to prevent infections of the prostate gland. As a group, we decided to study this kind of disease for us to know more about the complications. As a nursing students, we must not only focus to one corner or merely by just taking care of our patients but to know their underlying condition as well for the better and good nursing intervention done to promote maximum living ability. Furthermore, we have chosen this case study in order to identify and determine the general health problems and needs of the patient with an admitting diagnosis of acute glomerulonephritis. This study also intends to help patient as well as its significant others to promote health and medical understanding of such condition through the application of the nursing theories and nursing skills.

II. Objectives
General Objectives:
At the end of this case study, I will be able to gain knowledge and ideas, practice my skills and deal appropriate attitudes towards client and everyone.
Specific Objectives:
Student Centered Objectives:
At the end of the case study, I will be able to:
Affective
1. Appreciate the importance of health.
2. Appreciate the importance of significant other’s support in all aspects.
3. Give value to one’s life.
Psychomotor
1. Appreciate the importance of providing extensive care to clients with kidney disease.
2. Perform effectively the nursing procedures to clients with kidney disease.
3. Promote health teachings for betterment of the health of the client.
Cognitive
1. Identify and determine general health problems of the client.
2. Formulate care plans related to psychological and physiological aspects of the disease.
3. Analyze the effectiveness in meeting the needs of the client.
Client Centered Objectives:
At the end of the case study, the client will able to:
Affective:
1. Appreciate essence of health.
2. Appreciate the support of significant others.

3. Give value and importance to one’s health.
Psychomotor
1. Avoid things that will complicate the disease.
2. Participates with the appropriate nursing interventions.
3. Demonstrate and apply health practices concerning the disease.
Cognitive
1. Identify and determine general health problems.
2. Analyze the effectiveness in meeting the needs.
3. Verbalize understanding regarding different complications of the disease.
III. DEVELOPMENTAL THEORIES
Erik Erikson’s Psychosocial Theory
According to Erikson every stage must be complete and must be obtain by a person. Ms. X is 14 years old so she is in the stage of Adolescence, which is the identity vs. role confusion phase. Ms. X shows feelings of confusion, indecisiveness which indicates negative resolution, she is still in the role confusion phase, maybe it’s because she is still very young to make decisions.
Robert Havighurst Developmental Task Theory
Ms. X belongs to the adolescence stage. She is achieving feminine social role, accepting one’s physique and using the body effectively and achieving new and more mature realtions with age-mates of both sexes.
Sigmund Freud’s psychosexual Theory
Ms. X is in her Genital stage which means she is developing to her full sexual maturity. Her energy is directed toward full maturity and function and development of skills needed to cope with the environment. She is highly sociable and friendly because many of her friends and classmates visited her during her hospitalization.

IV. Clients Profile
A. Socio-demographic data
Patient X is a 14 year old female, Roman Catholic; a resident of Brgy. Nawasa Gingoog City. Patient X was admitted for the first time at Misamis Oriental Provincial Hospital at 5:30 pm. due to difficulty of breathing, facial and pedal edema. She arrived at the hospital awake, conscious and coherent with a chief complaint of difficulty of breathing, facial and pedal edema.
B. Vital Signs
The patient’s vital signs are essential because it provides a baseline data in determining alteration in the patient’s body that may suggest underlying disease. Any changes from the normal are considered to be an indication of the person’s state of health and provide cues to the physiological functioning of the client. The patient had the following vital signs: blood pressure: 100/70 mmHg, pulse rate: 104 bpm, respiratory rate: 32 cpm, temperature: 36.9ºC. She currently weighs 42kilograms from the previous weight of 45 kilograms and he is 5’1 tall.
C. Health Patterns Assessment
V. Nursing History of Illness
1. History of Present illness

The client was brought to the hospital due to difficulty of breathing, facial and pedal edema. Three weeks prior to admission, onset of edema with no other associated symptoms noted. One week prior to admission, persistence of facial edema associated with pallor. 3 days prior to admission, difficulty of breathing, pallor and decreased urine output was noted which prompted patient to seek medical consultation. Patient has no previous hospitalization and surgeries. Client has no family history of kidney-related diseases. Patient X was not taking any medication. She’s a non tobacco user and a non alcoholic drinker. She has no drug allergies but has a food allergy specifically “uwang”.
2. Nutrition
During pre-hospitalization, the client used to eat junk foods which are high in sodium and likes to drink soft drinks most of the time and seldom drinks water. During hospitalization, Patient X was on a low salt, low fat diet. She has a poor appetite. She was not taking in any vitamins. The client is hooked with an intravenous fluid of D5 .3% solution running at 10 gtts/min.
3. Elimination Pattern
Pre-hospitalization, Patient X defecates once to twice daily with formed, brownish stool and soft in consistency. No discomfort felt during defecation but during hospitalization, the client has difficulty in defecating, thus, making her at risk to have constipation. While confined, the client defecates after 2-3 days. Pre-hospitalization, a month before the admission to the hospital, client has difficulty urinating thus, decreasing the urinary frequency from 6-8 times to 1 time per day. It’s yellowish in color and clear.
4. Activity -Exercise Pattern (pre – hospitalization)
Patient X is incorporating her exercise when walking from her house to the highway every morning and she’s going home from the school. Playing is her leisure activity together with few of her friends but mostly, she loves to play with her other siblings.
A. Activity-Exercise Pattern (while confined)
Describe the patient’s functional abilities
a. Feeding: independent
b. Bathing: independent
c. Toileting: independent
d. Bed mobility: independent

e. Dressing: independent
f. Grooming: dependent
g. General mobility: independent
h. ROM: independent
i. Ambulation: independent
The patient can do independently all activity- exercise but then, it is limited and controlled due to disease condition and client prefer to stay in the bed than ambulating. Patient does not like to take a bath during hospitalization, her mother cleans wipe out dirt in the body which made her dependent in Grooming.
5. Cognitive-Perceptual Pattern
Patient X understands and speaks Visayan language and she didn’t have any speech deficit. Patient is a 4th year High School Student without any learning difficulties. There is pain felt in the abdominal area and patient usually guards the location of pain.
6. Sleep -Rest Pattern
Pre-hospitalization, Patient X usually sleeps for 8 hours. She doesn’t have any sleep disturbances but while confine, she verbalized problem of sleeping disturbances at night. Imagery is one of the effective tools for her in order to sleep at night.
7. Self-perception and Self-concept Pattern
Patient X says that she is good as well a responsible student because she usually gets an award after each school year. She feels that she was weak and fear to be behind in their classroom lessons and scared not to get an award this school year due to the series of absences because of her hospitalization.
8. Role-Relationship Pattern
Her family specifically her mother and grandfather who helped her during hospitalization. Her father and other members in the family also visit her in the hospital and also her classmates and friends.
9. Coping -stress Tolerance Pattern

Patient X seldom experiences any stress during hospitalization due to difficulty of breathing, she just subject herself to sleep.
10. Value -Belief Pattern
Patient X is a Roman Catholic. To her it is important as it had helped her when she has a problem. She goes to church every Sunday together with her family. The client also prays frequently as part of her religious practices.
D. Physical Assessment
1. Neurologic Assessment
Level of consciousness ConsciousOrientation OrientedEmotional state Worried/anxious (sometimes); restless
2. Head
Head NormocephalicFacial movement SymmetricalFontanels ClosedHair FineScalp Clean
3. Eyes
Lids SymmetricalPeriorbital region EdemaConjunctiva PaleCornea & Lens Opacity R/LSclera AnictericPupils Equal in sizeReaction to light Brisk R/LReaction to accommodation Uniform to constrictionVisual acuity Grossly normal

Peripheral vision Intact/full
4. Ears
External pinnae NormosetExternal canal No dischargeTympanic membrane IntactGross hearing Normal
5. Nose
Mucosa PinkishPatency Both patentGross smell Normal/symmetricalSinuses No tenderness presence
6. Mouth
Lips PallorMucosa PinkishTongue MidlineTeeth CompleteGums Pinkish
7. Pharynx
Uvula MidlineTonsils Not inflamedPosterior pharynx No inflammation
8. Neck
Trachea MidlineThyroids Non-palpable
9. Skin
General Color PallorTexture Rough

Turgor FirmTemperature Warm
10. Abdomen
Configuration GlobularBowel sound Hypoactive (3 counts)Percussion Tympanic
11. Cardiovascular Status
Pericardial area FlatPoint of maximal impulse (PMI) 5th intercostalsApical & rhythm Normal (100bpm)Heart sound RegularPeripheral pulse Symmetrical & regular but weakCapillary refill 2 seconds
12. Respiratory Status
Breathing pattern Irregular (Tachypneic)Lung expansion SymmetricalPercussion ResonantBreath sound VesicularCough Non-productive
HOME VISIT
Post hospitalization ( August 13,2012)

VI. ANATOMY AND PHYSIOLOGY
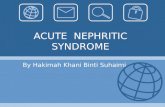
The Kidney
The main functional unit of the kidney is thenephron. There are approximately onemillion nephrons per kidney. The role of nephrons is to make urine by:
Filtering blood of small molecules and ions such as water, salt, glucose and other solutes including urea. Large “macromolecules” like proteins are untouched.
R e c y c l i n g t h e r e q u i r e d q u a n t i t i e s o f u s e f u l s o l u t e s w h i c h t h e n r e -e n t e r t h e bloodstream. (A process called reabsorption)
Allowing surplus or waste molecules/ions to flow from the tubules/ureter as urine.

Nephrons are the basic structural and functional units of the kidney. They consist of a network of tubules and canals specialized in filtration.
The kidney is responsible for maintaining fluid balance within the body. The basic structural and functional units of the kidneys are the nephrons. Each nephron is made of intricately interwoven capillaries and drainage canals to filter wastes, macromolecules, and ions from the blood to urine. The approximately 1 million nephrons in each human kidney form 10-20 cone-shaped tissue units called renal pyramids that span both the inner and outer portions of the kidney, the renal medulla and renal cortex.
A. Renal Vein
This has a large diameter and a thin wall. It carries blood away from the kidney and back to the right hand side of the heart. Blood in the kidney has had all its urea removed. Urea is produced by your liver to get rid of excess amino-acids. Blood in the

renal vein also has exactly the right amount of water and salts. This is because the kidney gets rid of excess water and salts. The kidney is controlled by the brain. A hormone in our blood called Anti-Diuretic Hormone (ADH for short) is used to control exactly how much water is excreted. This blood vessel supplies blood to the kidney from the left hand side of the heart. This blood must contain glucose and oxygen because the kidney has to work hard producing urine. Blood in the renal artery must have sufficient pressure or the kidney will not be able to filter the blood. Blood supplied to the kidney contains a toxic product called urea which must be removed from the blood. It may have too much salt and too much water. The kidney removes this excess material that is its function.
B. Renal Artery
This blood vessel supplies blood to the kidney from the left hand side of the heart. This blood must contain glucose and oxygen because the kidney has to work hard producing urine. Blood in the renal artery must have sufficient pressure or the kidney will not be able to filter the blood. Blood supplied to the kidney contains a toxic product called urea which must be removed from the blood. It may have too much salt and too much water. The kidney removes these excess materials; that are its function.
C. Pelvis
This is the region of the kidney where urine collects. If you are very unlucky, you may develop kidney stones. Sometimes the salts in the urine crystallize in the pelvis and form a solid mass which prevents urine from draining out of the medulla of the kidney. You will need treatment: see your doctor.
D. Ureter
This one is easy peasy: the ureter carries the urine down to the bladder. It does this 24 hours per day, but fortunately the urine can be stored in a bladder so that it is not necessary to wear a nappy!
E. Medulla
The medulla is the inside part of the kidney. It is shown in green in the diagram, but in real life it is a very dark red color. This is where the amount of salt and water in your urine is controlled. It consists of billions of loops of Henlé. These work very hard pumping sodium ions. ADH makes the loops work harder to pump more sodium ions. The result of this is that very concentrated urine is produced. The opposite of an anti-diuretic is a "diuretic". Alcohol and tea are diuretics

F. Cortex
The cortex is the outer part of the kidney. This is where blood is filtered. We call this process "ultra-filtration" or "high pressure filtration" because it only works if the blood entering the kidney in the renal artery is at high pressure. Billions of glomeruli are found in the cortex. A glomerulus is a tiny ball of capillaries. Each glomerulus is surrounded by a "Bowman's Capsule". Glomeruli leak. Things like red blood cells, white blood cells, platelets and fibrinogen stay in the blood vessels. Most of the plasma leaks out into the Bowman's capsules. This is about 160 liters of liquid every 24 hours. Most of this liquid, which we call "ultra-filtrate" is re-absorbed in the medulla and put back into the blood.
G. Glomerulus and Bowman's Capsule
This is where ultra-filtration takes place. Blood from the renal artery is forced into the glomerulus under high pressure. Most of the liquid is forced out of the glomerulus into the Bowman's capsule which surrounds it. This does not work properly in people who have very low blood pressure. Proximal Convoluted Tubules Proximal means "near to" and convoluted means "coiled up" so this is the coiled up tube near to the Bowman's capsule. This is the place where all that useful glucose is re-absorbed from the ultra-filtrate and put back into the blood. If the glucose was not absorbed it would end up in your urine. This happens in people who are suffering from diabetes.
H. Loop of Henlé
This part of the nephron is where water is reabsorbed. Kidney cells in this region spend all their time pumping sodium ions. This makes the medulla very salty; you could say that this is a region of very low water concentration. If you remember the definition of osmosis, you will realize that water will pass from a region of high water concentration (the ultra-filtrate and urine) into a region of low water concentration (the medulla) through cell membranes which are semi-permeable.
I. Distal Convoluted Tubules
Distal means "distant" so it is at the other end of the nephron from the Bowman's capsule. This is where most of the salts in the ultra-filtrate are re-absorbed.
J. Collecting Duct
Collecting ducts run through the medulla and are surrounded by loops of Henlé. The liquid in the collecting ducts (ultra-filtrate) is turned into urine as water and salts are removed from it. Although our kidneys make about 160 liters of urine every 24 hours, we only produce about ½

liter of urine. It is called a collecting duct because it collects the liquid produced by lots of nephrons.
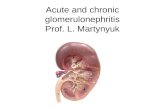
Nephron Function
The blood is filtered and urine formed by the actions of the nephrons. In each nephron, high pressure in the glomerulus pushes water and small dissolved materials into the extra vascular space of the Bowman’s capsule and into the tubule. The proximal tubule reabsorbs water, salts, glucose, and amino acids to maintain electrolyte levels in the body. The interstitial of, that is the tissue space surrounding, the loop of Henle concentrates salts that will be excreted in the urine, creating a concentration gradient in the medulla. The limbs of Henle’s loop are permeable to particular ions (descending, water and some urea; thin ascending, general ions; medullary thick ascending –sodium, potassium, chloride), with the cortical thick ascending limb draining into the distal convoluted tubule. The distal tubule contains cells specialized in active transport and maintains urine and blood pH levels, particularly through the regulation of sodium and potassium. Fluid then passes from the distal tubule to the collecting ducts, a tubule system that can become permeable or impermeable to water depending on the body’s needs. Ultra filtration also occurs in the cortex in the cortical collecting ducts, which is regarded by some anatomy references as not being a portion of the nephron, and by others as being the final portion of the nephron. The urine then passes from the collecting ducts through the drainage system of the kidney to the ureters and bladder for urination.
Tubular Secretion in the Kidneys
Another, less familiar, mechanism for urine production in the kidneys is tubular secretion. Specialized cells move solutes directly from the blood into the tubular fluid. For example, hydrogen and potassium ions are secreted directly into the tubular fluid. This process is “coupled” or balanced by the re-uptake of sodium ions back into the blood. Tubular secretion of hydrogen ions, augmented by control of bicarbonate levels is important in maintaining correct blood pH. When the blood is too acidic (acidosis) more hydrogen ions are secreted. If the blood becomes too alkaline (alkalosis), hydrogen secretion is reduced. In maintaining blood pH within normal limits (about7.35–7.45) the kidney can produce urine with pH as low as that of acid rain or as alkaline as baking soda!
The Kidney as an Endocrine Gland
In addition to its excretory and homeostatic roles, the kidneys also release two important hormones into the blood. These are:
• Erythropoietin which acts on bone marrow to increase the production of red blood cells

• Calciterol which promotes the absorption of calcium from food in the intestine and acts directly on bones to shift calcium into the blood stream. Finally the kidney produces the enzyme renin, an important regulator of blood pressure.
THE RENIN ±ANGIOTENSIN MECHANISM
Decreased blood pressure stimulates the kidney to secrete renin. Renin splits the plasma protein angiotensinogen (synthesized by the liver) to
angiotensin I Angiotensin I is converted to angiotensin II by an enzyme (called converting enzyme) Secreted by the lung tissue and vascular endothelium.
Angiotensin II:
-causes vasoconstriction- stimulates the adrenal cortex to secrete aldosterone which maintains normal blood levels of sodium and potassium and contributes to the maintenance of normal blood pH, blood volume, and blood pressure.
VIII. Laboratory Examinations
Complete Blood Count

PARAMETERS NORMAL VALUES ACTUAL VALUES ANALYSISWBC 4.5-11.0 x 10mm 11.1 Increase indicates
infection, leukemia, tissue
necrosis.Hemoglobin Female: 11.7 –
14.5 g/dl 10.9 Inadequate
production of RBCs, which may
result to anemia,fluid
overload, recent hemorrhage.
Hematocrit Female: 34.1 – 44.3 vol%
33.0 Decrease may result
hemodilation, anemia, acute massive blood
loss.Platelet 175,000 –
350,000/mm256,000 NORMAL
PARAMETERS NORMAL VALUES ACTUAL VALUES ANALYSISSegmenters 45-70% 67 Increased;
Indicates high glucose level in the blood.
Lymphocytes 18-45% 24 Increased; Indicates infection
Monocytes 4-8% 7 NORMALEosinophils 2-3% 2 NORMAL
Blood Chemistry Report
PARAMETER NORMAL VALUES ACTUAL VALUES ANALYSIS

BUN/ Urea 1.7-8.3 Mmol/L 10.10
Increased BUN levels suggest
impaired kidney function. This may be due to acute or
chronic kidney disease, damage,
or failure.
Urinalysis Report
PARAMETER NORMAL VALUES ACTUAL VALUES ANALYSISColor Yellow/Amber Light yellow Normal
Transparency Clear to slightly turbid
cloudy
Reaction 4.5-8 6.0 NormalSpecific Gravity 1.005-1.030 1.025 Normal
Sugar Negative Trace Indicative of glucosuria
Protein Negative Positive (+1) Indicative of proteinuria
Squamous Epithelial Cells
Few Few Normal
Red Blood Cells Few 7.50 Hematuria, indicative of
possible glomerular
damagePus Cells Few 3-5 Indicative of
bacterial infectionMucous Few Few NormalBacteria Few Many Indicative of
presence of bacteria.
Amorp. Urates/Phosphate
Few Moderate Indicative of bacterial infection

s
IX. Nursing Management
According to book
•Review fluid and diet restrictions measure and record intake and output.
•Instruct patient to schedule follow up evaluations of blood pressure, urinalysis for protein and BUN and creatinine studies to determine if disease has worsened.
•Instruct patient to notify physician if infection or symptoms of renal failure occur: fatigue, nausea, and vomiting, diminishing urinary output.
•Refer to home care nurse as indicated for assessment and detection of early symptoms and follow-up evaluations.
According to patient
•Vital sign was monitored timely and was recorded in TPP chart.
•An electrolyte value was monitored.
•Renal function was assessed
•Intake and output chart was strictly maintained.
•Acute renal failure was monitored.
•Oliguria
•Azotaemia (Increased blood urea)

•Acidosis and hyperkalemia (K+increased)
•Health education was provided about the nature of illness, diet, and medicines
IX. Discharge Planning
D– iscipline regarding the diet
I – nstruct to avoid excessive use of salt
S– eek for medical assistance for further complications
C- ontinue to take medication for maintenance
H– ealth teaching regarding the importance of restricting diet
A– ssess for any adverse effect of the medication
R- egular check-up
G – ive the importance in taking the medication
E – ncourage to follow the prescribed medication at home
Explain to the patient and family members the importance of taking medicines. Discuss to the patient and family the dosage, frequency and adverse effects of the
drugs. Encourage to follow the dosages and proper timing of her meds. Such as the
Furosemide 40mg once a day x 3 doses, Prednisone 20mg tab 1 tab Twice a day oral, Ranitidine 50mg x 6 doses. As prescribed by her physician.
Economic status
Explain to significant others that the rehabilitation may be prolonged to be able for the family to prepare financial needs
Have occupational therapist to help re- learn everyday activities or ADL Inform the patient to avail to some government programs such as Philhealth.

Treatment
Tell the patient that she should have self-monitoring by checking his vital signs and weighing regularly.
Encourage/instruct to keep the edematous extremities to elevate as often Limit of water intake; monitor intake and output Provide warm environment Provide egg white a day Weight the pt. daily, at the same time. Avoid eating foods high in sodium and drinking soft drinks.
X. HEALTH TEACHINGS
Instruct the patient to take medications religiously. Improve nutritional status. Importance of proper hygiene for comfort.
OUT-PATIENT
The patient could avail her medication from government hospitals that she could get some benefits.
She will also be able to avail the services offered by the Barangay health center and at the “Botika ng barangay”.
Instruct patient to seek regular medical check-up
DIET
Eat five or more servings of vegetables and fruit daily. Intake of fluids 8-10 glasses a day to avoid constipation and to maintain skin turgor. Instruct patient to eat low fat and low sodium foods that will help and will not
complicate her condition that is ordered by the physician.

XIX. Bibliography
WEB:
http://generalmedicine.suite101.com/article.cfm/the_human_kidney_structure_and_function#ixzz0wIXUzTtr
http://cellstissuesmembranes.suite101.com/article.cfm/nephron_structure_and_function
http://emedicine.medscape.com/article/777272-overview;http://www.total-health-care.com/illness/acute-glomerulonephritis.htm)
BOOKS:
Nurse’s Pocket Guide 11th edition (Diagnoses, Prioritized interventions, and Rationales) By:Marilyn E. DoengesMary Frances Moorhouse Alice C. Murr
Nursing 2003 Drug Handbook 23rd edition By: Springhouse Lippincott Williams and Wilkins
Medical Surgical Nursing 8th Edition, (Clinical Management for Positive Outcomes) by: Joyce M. Black, Jane Hokanson Hawks
Kozier & Erb’s Fundamentals of Nursing 8th Edition (Concepts, Process and Practice) by: Berman, Synder, Kozier, Erb