
Diffuse Proliferative Glomerulonephritis and Acute Renal Failure Associated with Acute
7
Diffuse Proliferative Glomerulonephritis and Acute Renal Failure Associated with Acute Staphylococcal Osteomyelitis MATTHEW D. GRIFFIN,* JOHANNES BJORNSSON,t and STEPHEN B. ERICKSON* *Department of Internal Medicine, Division of Nephrology, and tDepartment of Pathology, Mayo Clinic and Mayo Foundation, Rochester, Minnesota. Abstract. A 72-year-old man developed acute renal failure after coronary bypass surgery that had been complicated by sternal osteomyelitis caused by the Staphylococcus aureus bacterium. Bacteremia and sepsis were not present. Renal biopsy demon- strated a florid, diffuse, proliferative glomerulonephritis with glomerular immune complex deposition. Management in- cluded hemodialysis, prolonged antibiotic therapy, and re- peated surgical debridement. Spontaneous recovery of renal function occurred after eradication of infection and final sur- gical wound repair. The relationship between acute bacterial infections and glomerulonephritis and, in particular, the causal role of staphylococcal antigens in the pathogenesis of such lesions is discussed. (J Am Soc Nephrol 8: 1633-1639, 1997) Coagulase-positive staphylococcus (Staphylococcus aureus) is the most common causative organism in acute osteomyelitis (1). Along with coagulase-negative staphylococcal species, it has also been implicated in the pathogenesis of immune com- plex (IC)-mediated diffuse proliferative glomerulonephritis (DPGN) in a variety of infections. These include bacterial endocarditis, ventriculoatrial shunt infections, pneumonia, and visceral abscesses with or without septicemia (2-6). No clearly documented cases of glomerulonephritis with acute renal fail- ure (ARF) in association with staphylococcal osteomyelitis have previously been reported. We describe an episode of biopsy-proven DPGN with rapidly progressive ARF occurring after postoperative wound infection and sternal osteomyelitis caused by S. aureus. Spontaneous recovery occurred after eradication of the infection through prolonged antibiotic ther- apy and multiple surgical debridements. Case Report Presentation and Management The patient, a 72-year-old white man, was transferred to our institution from another medical facility for further manage- ment of postsurgical sternal wound infection and ARF. Thirty- four days before transfer, he had undergone coronary artery bypass graft surgery (CABG) for treatment of severe three- vessel disease. Figure 1 summarizes the course of his ARF both before and after transfer and highlights important thera- peutic interventions. An increased serum creatinine concentra- tion ( 1 33 pmolIL [ 1 .5 mg/dl]) had first been noted 18 days after CABG, having been normal on day 15 (80 jtmolIL [0.9 Received July 31, 1996. Accepted January 17, 1997. Correspondence to Dr. Stephen B. Erickson, Division of Nephrology, Mayo Building, W l2B, Mayo Clinic and Foundation, 200 First St. SW, Rochester. MN 55905. 1046-6673/08010- l633$03.00/0 Journal of the American Society of Nephrology Copyright © 1997 by the American Society of Nephrology mg/dl]) and in the immediate postoperative period. Over the following days, the patient’s serum creatinine concentration increased progressively, and hemodialysis was instituted on day 23 after CABG. There was no past or family history of renal disease and no known drug allergies. Prior medical history had included degenerative disc disease, stable abdom- inal aortic aneurysm, stable benign prostatic hyperplasia, and depression. The patient had been readmitted to his home hospital with fever and purulent discharge from his wound 8 days after surgery. Blood cultures were negative at this time and on three other occasions during the illness. Wound packing and empiric antibiotic therapy with intravenous vancomycin had failed to improve his wound infection, and surgical debridement with rewiring of the sternum was first carried out 10 ten days after CABG. Staphylococcus aureus had been cultured from wound tissue and sternal bone marrow at this time, and therapy with intravenous anti-staphylococcal antibiotic therapy had been continued. At the onset of ARF, urinalysis was reported as showing microhematuria (5 to 9 cells per high-power field) with gran- ular casts. Additional pertinent studies during this period in- cluded persistently normal platelet count and negative serolo- gies for hepatitis A, B, and C; antinuclear antibody, anti- double-stranded DNA antibody, and perinuclear and cytoplasmic antineutrophil cytoplasmic antibodies. Serum C3 and C4 complement levels were documented on day 22 after CABG at 91 mg/dl (normal range, 86 to 184 mg/dl) and 23 mg/dl (normal range, 20 to 59 mg/dl), respectively. Renal ultrasound showed both kidneys to be of normal size and appearance without evidence of obstruction. Renal biopsy was carried out on day 26 and high-dose corticosteroid therapy was begun on day 28. Renal Biopsy Results Eleven glomeruli, all viable, were available for light micros- copy. Endocapillary cellular proliferation was diffuse and gen-
Transcript of Diffuse Proliferative Glomerulonephritis and Acute Renal Failure Associated with Acute

Diffuse Proliferative Glomerulonephritis and Acute Renal
Failure Associated with Acute Staphylococcal Osteomyelitis
MATTHEW D. GRIFFIN,* JOHANNES BJORNSSON,t and STEPHEN B. ERICKSON*
*Department of Internal Medicine, Division of Nephrology, and tDepartment of Pathology, Mayo Clinic and
Mayo Foundation, Rochester, Minnesota.
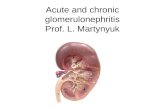
Abstract. A 72-year-old man developed acute renal failure after
coronary bypass surgery that had been complicated by sternal
osteomyelitis caused by the Staphylococcus aureus bacterium.
Bacteremia and sepsis were not present. Renal biopsy demon-
strated a florid, diffuse, proliferative glomerulonephritis with
glomerular immune complex deposition. Management in-
cluded hemodialysis, prolonged antibiotic therapy, and re-
peated surgical debridement. Spontaneous recovery of renal
function occurred after eradication of infection and final sur-
gical wound repair. The relationship between acute bacterial
infections and glomerulonephritis and, in particular, the causal
role of staphylococcal antigens in the pathogenesis of such
lesions is discussed. (J Am Soc Nephrol 8: 1633-1639, 1997)
Coagulase-positive staphylococcus (Staphylococcus aureus) is
the most common causative organism in acute osteomyelitis
(1). Along with coagulase-negative staphylococcal species, it
has also been implicated in the pathogenesis of immune com-
plex (IC)-mediated diffuse proliferative glomerulonephritis
(DPGN) in a variety of infections. These include bacterial
endocarditis, ventriculoatrial shunt infections, pneumonia, and
visceral abscesses with or without septicemia (2-6). No clearly
documented cases of glomerulonephritis with acute renal fail-
ure (ARF) in association with staphylococcal osteomyelitis
have previously been reported. We describe an episode of
biopsy-proven DPGN with rapidly progressive ARF occurring
after postoperative wound infection and sternal osteomyelitis
caused by S. aureus. Spontaneous recovery occurred after
eradication of the infection through prolonged antibiotic ther-
apy and multiple surgical debridements.
Case ReportPresentation and Management
The patient, a 72-year-old white man, was transferred to our
institution from another medical facility for further manage-
ment of postsurgical sternal wound infection and ARF. Thirty-
four days before transfer, he had undergone coronary artery
bypass graft surgery (CABG) for treatment of severe three-
vessel disease. Figure 1 summarizes the course of his ARF
both before and after transfer and highlights important thera-
peutic interventions. An increased serum creatinine concentra-
tion ( 133 p�molIL [ 1 .5 mg/dl]) had first been noted 1 8 days
after CABG, having been normal on day 15 (80 jtmolIL [0.9
Received July 31, 1996. Accepted January 17, 1997.
Correspondence to Dr. Stephen B. Erickson, Division of Nephrology, Mayo
Building, W l2B, Mayo Clinic and Foundation, 200 First St. SW, Rochester.
MN 55905.
1046-6673/08010- l633$03.00/0
Journal of the American Society of Nephrology
Copyright © 1997 by the American Society of Nephrology
mg/dl]) and in the immediate postoperative period. Over the
following days, the patient’s serum creatinine concentration
increased progressively, and hemodialysis was instituted on
day 23 after CABG. There was no past or family history of
renal disease and no known drug allergies. Prior medical
history had included degenerative disc disease, stable abdom-
inal aortic aneurysm, stable benign prostatic hyperplasia, and
depression.
The patient had been readmitted to his home hospital with
fever and purulent discharge from his wound 8 days after
surgery. Blood cultures were negative at this time and on three
other occasions during the illness. Wound packing and empiric
antibiotic therapy with intravenous vancomycin had failed to
improve his wound infection, and surgical debridement with
rewiring of the sternum was first carried out 10 ten days after
CABG. Staphylococcus aureus had been cultured from wound
tissue and sternal bone marrow at this time, and therapy with
intravenous anti-staphylococcal antibiotic therapy had been
continued.
At the onset of ARF, urinalysis was reported as showing
microhematuria (5 to 9 cells per high-power field) with gran-
ular casts. Additional pertinent studies during this period in-
cluded persistently normal platelet count and negative serolo-
gies for hepatitis A, B, and C; antinuclear antibody, anti-
double-stranded DNA antibody, and perinuclear and
cytoplasmic antineutrophil cytoplasmic antibodies. Serum C3
and C4 complement levels were documented on day 22 after
CABG at 91 mg/dl (normal range, 86 to 184 mg/dl) and 23
mg/dl (normal range, 20 to 59 mg/dl), respectively. Renal
ultrasound showed both kidneys to be of normal size and
appearance without evidence of obstruction. Renal biopsy was
carried out on day 26 and high-dose corticosteroid therapy was
begun on day 28.
Renal Biopsy Results
Eleven glomeruli, all viable, were available for light micros-
copy. Endocapillary cellular proliferation was diffuse and gen-

Renal Biopsy
*
Transfer*
1000
700
600
500
400
300
200
100
�p 0
4Rt�iQ�c T��4PY �IIemod�lysis�:prticos�erp�#{248}Th��py
IRfrctlp!! ��tt�dF’�i� j�gi#{231}���qpsure
-� 0 0 0 0 0c,� c� ‘, I0 0
*
!�ys ?�!st !�Y�?�SS S�4!��Y
*
1634 Journal of the American Society of Nephrology
C
E9�.
1.
c)EI-4?
ri�
Figure 1. Graph of serum creatinine values after coronary bypass surgery. demonstrating the course of acute renal failure episode and showing
the timing and duration of treatment modalities as well as the definitive surgical procedure.
eralized (Figure 2A). Proliferation was accounted for by rues-
angial cells and polymorphonuclear leukocytes. A few
capillary loops displayed peripheral extension of mesangial
cell cytoplasm and nuclei. Six glorneruli were examined on
irnrnunofluorescent microscopy, revealing strong granular re-
activity to inimunoglobulin G (IgG), both within glomerular
mesangiuni and along capillary walls. C3 complement had a
similar but somewhat less intense distribution. IgA. 1gM, and
kappa and lambda light chains of identical texture were like-
wise identified in a similar but significantly less intense pat-
tern.
Electron microscopy (Figure 2B confirmed the presence of
immune deposits along the internal aspect of peripheral gb-
merular basement membranes and in gbomerular mesangium,
associated with cellular proliferation and focal peripheral ex-
teflsion of mesangial cells.
Outconze
As shown in Figure 1 , corticosteroid therapy was tapered
and discontinued shortly after transfer, and vancomycin was
continued until close to discharge. Multiple surgical debride-
inents were carried out with definitive surgical wound closure
with muscle-flap transposition on day 52 after CABG. Sternal
tissue culture was negative by day 42. Urine output began to
increase shortly afterwards and hemodialysis was discontin-
ned. The patient was eventually discharged from hospital to
home with a serum creatinine concentration of 141 �.tmolIL
( I .6 mg/dl) and satisfactory wound healing.
Th4�i�1!!!This case clearly documents an IC-mediated, diffuse prolif-
erative gbomerubonephritis occurring as a result of acute osteo-
myelitis. The temporal relationship between the staphybococcal
infection and ARF in both onset and eventual resolution, along
with the unequivocal histopathobogical findings, leave no
doubt as to this association. As such it joins only a handful of
cases in which acute bone or joint infection has been clearly
linked to a gbonierulonephritis (7-9). More broadly, however,
it conforms to the well-recognized occurrence of jC-mediated
glomerulonephritis with certain infections in which the patho-
genie organism is, to some degree, sequestered from rapid
clearance by the immune system and in which progression to
chronicity may result. These include ventricuboatrial shunt
infections (3), bacterial endocarditis (2), visceral abscesses,
empyema, and others (4,6,10). Such infections may be as
clinically obvious as a septicenlia or may represent occult
infection presenting with ARF of unclear cause. They can also
be regarded as distinct from classical postinfectious gbomeru-
bonephritis in which the onset of renal disease generally fol-
lows the resolution of a self-limiting streptococcal infection.
The clear clinical and histological documentation in this case,as well as the lack of confounding coexisting or preexisting
disease, make it an ideal platform for the discussion of what

Glomerulonephntis in Acute Osteomyelitis 1635
common histological lesion described in all of the above cases
is diffuse endocapillary proliferation, sometimes with mem-
branoproliferative features. Extracapillary proliferation and in-
terstitial infiltrates may occur. Immune-type deposits have
been demonstrated in subendothelial, intramembranous, and
subepithelial locations (the latter often as typical “humps”)
(3,5,7-10,1 1-13). As regards clinical course and prognosis, in
general these cases have in common a lag time of 5 days to 4
weeks between onset of infection and renal disease, as well as
a strong dependence of renal recovery on successful treatment
of the underlying infection. Chronic renal impairment, varying
from mild to severe, usually occurs in the setting of a pro-
longed active infection. One series, which also included cases
of typical poststreptococcal glomerulonephritis, found that
older age, higher serum creatinine concentration, and crescen-
tic features on biopsy were predictive of poorer overall and
renal survival (5).
Figure 2. (A) Diffuse proliferative glomerulonephritis. Glomerularlobularity is enhanced because of endocapillary cellular proliferation
and inflammatory infiltrates (examples indicated by arrowheads).(Periodic acid-Schiff stain, X400). (B) Endocapillary cellular prolif-
eration with extension of mesangial and inflammatory cells into
peripheral capillary loops (closed arrowhead). Subendothelial im-
mune-complex deposition (open arrowheads). (Electron micrograph,X1200).
might best be classified as “infective glomerulonephritis.” It
also serves to highlight the potentially important role of staph-
ylococcal antigens in the pathogenesis of IC-mediated glomer-
ular disease.
Infective Glomerulonephritis
Table 1 lists sites of bacterial infection that have been
reported to be associated with DPGN, excluding the better-
recognized associations with bacterial endocarditis and yen-
triculoatrial shunt infections. It is clear that a variety of Gram-
positive and Gram-negative organisms have been isolated
under these circumstances. Table 2 summarizes the accompa-
flying clinical, laboratory, and histopathological features that
have been described. The reduction in serum levels of com-
plement components, which may be a valuable clue in classical
postinfectious GN, “shunt nephritis,” and the GN of endocar-
ditis, is often not present (4,6,10). An accompanying purpuric
rash may be noted in up to 20% of cases (5, 10). The most
Glomerulonephritis and Staphylococcal Infections
The predominance of staphylococcal infections, regardless
of the site of infection, is clear from Table 1 . A recent review
of infection-related glomerulonephritis at one institution found
that of 3 1 cases in which a causative organism had been
identified, 13 were associated with staphylococcal species (5).
Well-documented cases exist involving septicemic and non-
septicemic infections and both coagulase-positive and coagu-
lase-negative staphybococcal species. Septicemic cases most
commonly represent acute bacterial endocarditis due to S.
aureus, although well-documented cases of DPGN with septi-
cemic S. aureus pneumonia, empyema, and arthritis exist
(2,4,6,9, 1 1). Nonsepticemic cases predominantly represent in-
fection of ventriculoatrial shunts by coagulase-negative staph-
ylococcus (3). In addition, however, DPGN has been described
with impetigo and abscesses of lung and skin due to S. aureus
in the absence of bacteremia (12,14,15). Our case best repre-
sents an example of the latter, uncommon group. Only one
report of an association between gbomerulonephritis and staph-
ybococcal osteomyelitis exists and, in fact, this describes ne-
phrosis rather than ARF in three patients with chronic osteo-
myelitis without evidence of amyloidosis (7). An additional
case of osteomyelitis with DPGN is included among a series
reported by Beaufils and colleagues, but the causative organ-
ism and the degree of renal impairment are not specified (10).
Pathogenesis
Although conventional histology and immunofluorescence
microscopy allow classification of the renal lesion, in this case
they provide little useful information regarding pathogenesis.
The previously reported demonstration of staphylococcal pro-
teins within gbomerular immune deposits in similar cases of
DPGN supports a direct role for bacterial antigens in the
disease process ( 16, 17). To formulate a hypothesis on how
foreign antigens might generate such a process, however, it is
necessary to look to data from in vivo models of IC-mediated
glomerulonephritis (1 8). Table 3 categorizes the important
major steps in the pathogenic process in experimental models
and lists some of the variables that have been shown to be of

1636 Journal of the American Society of Nephrology
Table 1. Bacterial infections that have been reported to be associated with immune complex-mediated glomerulonephritis
(excluding bacterial endocarditis and ventriculoatrial shunt infections)
Site of Infection Type of Infection Organisms Reference
Lung Pneumonia, lung abscess,
empyema
S. aureus, Klebsiella pneumonia,
Pseudomonas aeruginosa,
Proteus mirabilis,
Pneumococcus, Moraxella
alcaligenes
4, 5, 6, 10, 14, 26, 27
Skin Wound infection, impetigo, skin
abscesses
S. Aureus 5, 6, 10, 12, 15
Abdomen Appendiceal abscess, subphrenic
abscess, septic abortion,
infected ascites
Escherichia coli, P. mirabilis,
Clostridium petfringens,
S. aureus
2, 4, 5, 10
Spine/CSF Meningitis, vertebral abscess,
postsurgical infection
S. aureus S
Bone and joint Septic arthritis, infected hip
prosthesis, osteomyelitis
S. aureus 5, 8, 9, 10
Paranasal sinuses/teeth Sinus abscess, dental abscess S. aureus 4, 5Unidentified sepsis N/A E. coli, S. aureus 5, 11, 28
Vascular Infected vascular graft Not reported 4, 10
Table 2. Reported clinical and histopathological features of immune-complex-mediated glomerulonephritis associated with
bacterial infections (excluding bacterial endocarditis and ventriculoatnal shunt infections)
Clinical Features
Frequent (>50%)
Oliguria
Hypertension
Documented bacterial infection within days to weeks
Raised serum creatinine
Microhematuria/red cell casts
Moderate proteinuria (0.5 to 3.0 g/d)
Normal serum complement components
Cryogbobulinemia
Frequent
Histological Features
Diffuse glomerular proliferation and exudation
Mesangial proliferation
Mild to moderate interstitial cellular infiltrate
Immunoglobulin chain and complement component deposition
Infrequent (<50%)
Anuria
Purpuric skin rash
Arthralgias
Nephrotic syndrome
Gross hematuria
Circulating immune complexes
Reduced serum complement components
Infrequent
Crescent formation
Membranoproliferative features
Severe interstitial cellular infiltrate
potential importance in initiating or maintaining gbomerular
injury under these circumstances.
Although it remains possible that the some deposits ob-
served within the gbomerular wall represent circulating IC that
have been “trapped” during filtration, it has been well-estab-
lished that ionic charge, as well as specific binding properties,
may mediate the direct adhesion of foreign antigens to com-
ponents of the glomerular basement membrane (1 8, 19). Sub-
sequent events include binding of specific antibodies to the
foreign antigen, as well as secondary humoral and cellular
responses to this primary complex. The resulting lesion can
then be viewed as a dynamic structure composed of self and
foreign material, which may be processed uneventfully or may
set in motion an array of pathways capable of causing tissue
injury. The factors that determine which course will ensue are
likely to include the type, dose, route of presentation, and
persistence of foreign antigen, as well as individual, genetically
based variations in primary and secondary inflammatory re-
sponses (18,20,21). The role of the complement system in
these early events merits particular comment. It has been
shown that the normal processing of circulating IC is depen-
dent on an interaction between complement components con-

Table 3. Likely sequence of pathogenic events in immune complex-mediated glomerulonephritis secondary to bacterial
antigens; variables that may play an important role in disease onset and severity based on data from experimental
models, are included�’
Infiltration of glomerulus by inflammatory cells
Clinical expression of glomerulonephritis
Disease progression or resolution
a GBM, glomerular basement membrane; IC, immune complex.
Glomerulonephritis in Acute Osteomyelitis 1637
Major Pathogenic Event
Exposure to bacterial antigen (±binding to
GBM components)Production of primary antibody to circulating or
bound antigen
In-situ formation or trapping of IC in GBM and
secondary modifications to IC
Early injury to glomerular structures
Disease-Modifying Variables
Charge and binding properties of antigen, individual
variation in GBM components.
Route of exposure, dose of antigen, persistence of infection.
Site of antigen binding, secondary humoral and/or cellular
immune responses
Complement activation, complement receptor expression,
local production of ROMs, cytokines and other
inflammatory mediators; structural alterations to GBM
Glomerular expression of chemoattractants, adhesion
molecules, activating factors; GBM exposure with
platelet adhesion and activation
Pattern of release of inflammatory mediators and cytokines
from neutrophils, monocytes, and platelets; variations in
activity of protective pathways and feedback mechanisms
Duration of bacterial infection
tamed within these complexes and a group of receptors ex-
pressed primarily by erythrocytes. These complement
receptors (E-CR) may also play a role in preventing the gen-
eration by tissue-bound IC of the complement products C3b
and C5b-9, which directly injure gbomerular cells and lead to
the local production of a variety of cytokines. Individual dif-
ferences in the level of E-CR or depletion by prolonged IC
formation may be an important factor in disease pathogenesis
(18,20,22). Administration of a soluble form of CR-i has been
shown to reduce the severity of certain animal models of
IC-mediated glomerulonephritis (22).
The type and severity of initial cellular damage within the
glomerulus may dictate subsequent patterns of recruitment and
activation of neutrophils, platelets, and monocytes. Many sub-
stances, produced both by native and infiltrating cells, may
then contribute to progressive injury. Although the list of such
mediators continues to grow and includes reactive oxygen
metabolites (ROM), proteases, eicosanoids, kinins, coagulation
components, chemoattractants, adhesion molecules, cytokines,
and growth factors, the precise role of each in various glomer-
ular diseases remains to be defined. The value of in vivo
models lies in the opportunity they present for the selective
alteration of single elements of this network and observation of
the effects on a defined disease process. In animal models of
IC-mediated glomeruionephritis, central pathogenic roles have
been predicted for neutrophil and platelet-derived products,
platelet-activating factor, ROM, and specific cytokines such as
interleukin 1 and transforming growth factor /3 (18,23,24). A
more recent development has been the recognition that the
expression of certain groups of cytokines and other inflamma-
tory mediators may share a dependence on single gene tran-
scription factors (for example, NF-KB) (25). These transcrip-
tion factors may be induced during the early events of a disease
process and may represent important targets for the treatment
of many immune-mediated diseases in the future.
In the case of infective glomerulonephritis, it is clear that
persistence of bacterial antigen is the primary determinant of
ongoing disease activity and only rarely have cases of active
nephritis been reported after eradication of the causative infec-
tion. This emphasizes the role of the many inhibitors and
feedback mechanisms involved in modulating the inflamma-
tory response to antigen-antibody complexes. Depletion or
genetically based variation in protective pathways, such as
free-radical scavenging, may also represent a central issue in
the correlation between the underlying pathogenesis and the
clinical course of individual cases (24).
Treatment
The primary consideration in the management of ARF in the
setting of active bacterial infection is the close prognostic
relationship between renal recovery and successful eradication
of the causative infection. This point is highlighted by our
patient’s clinical course, with resolution of his ARF commenc-
ing only after complete clearance of the infection. In many
settings, this necessitates a multidisciplinary approach to rapid
and accurate diagnostic and therapeutic planning. Of particular
value is a clear microbiological diagnosis from the outset, with
frequent surveillance cultures when possible. Renal biopsy, in
addition to demonstrating the severity of the glomerular lesion,
may be most important as a means of eliminating other diag-
noses that might impact strongly on management decisions.
The possibility of drug-related interstitial nephritis is a com-
mon consideration in the context of active infection and may
restrict the use of optimal antibiotic regimens if not ruled out

I 638 Journal of the American Society of Nephrology
histologically. When clinical evidence of nephritis occurs with
cavitating lung lesions, it is important to distinguish between
infection-related glomerulonephritis and Wegener’ s granulo-
matosis. In this setting, renal biopsy may be the most definitive
test. In a variety of situations (e.g. , “shunt nephritis,” empy-
ema, intraabdominal abscess, infected prosthetic material, and
bone orjoint infections), the need for early or repeated surgical
intervention will be heightened by the additional goal of pro-
moting renal recovery. The failure of ARF to respond to
corticosteroid therapy in our patient argues against the use of
immunosuppressive therapy for acute glomerulonephritis that
occurs in the face of active bacterial infection, even with rapid
progression of ARF. Occasional reports suggest that the un-
common situation of persistent active renal disease despite
clearly successful treatment of infection may merit a trial of
corticosteroid therapy if no other contraindication exists
(11,13).
ConclusionsThis case documents an unusual association between staph-
ylococcal osteomyelitis and ARF secondary to immune corn-
plex-mediated DPGN. It serves to illustrate the range of bac-
terial infections that have been reported to cause
gbomerulonephritis in the presence or absence of bacteremia, as
well as the frequent implication of staphylococcal antigens in
the pathogenesis of such lesions. The importance of early
microbiological and histological diagnosis and a multidisci-
plinary approach to eradication of infection for both patient and
renal survival are stressed. The role of corticosteroids or other
immunosuppressives should be confined to the rare circurn-
stance in which renal disease remains active despite complete
elimination of the underlying infection. Although infrequently
reported, it is possible that milder forms of infective gbomer-
ulonephritis or episodes occurring in the setting of sepsis often
go unrecognized. With the continuing emergence of antibiotic-
resistant staphybococcal species, the association of immune
complex-mediated glomerulonephritis with infections by this
organism is likely to remain an important consideration for the
clinical nephrologist.
References1 . Madler JT, Calhoun J: Osteomyelitis. In: Principles and Practice
ofinfectious Diseases, edited by Mandell GF, Bennett JE, Dolin
R, New York, Churchill Livingstone, 19952. Tu WH, Shearn MA, Lee JC: Acute diffuse glomerulonephritis
in acute Staphylococcal endocarditis. Ann Intern Med 7 1 : 335-
341, 1969
3. Stickler GB, Shin MH, Burke EC, Holley KE, Miler RH, Segar
WE: Diffuse glomerulonephritis associated with infected yen-triculoatrial shunt. N Eng! J Med 279: 1077-1082, 1968
4. Beaufils M, Moel-Maroger L, Sraer J-D, Kanfer A, Kourilsky 0,Richet G: Acute renal failure of glomerular origin during visceral
abscesses. N Eng! J Med 295: 185-189, 1976
5. Montseny ii, Meyrier AA, Kleinknecht D, Callard P: The current
spectrum of infectious glomerulonephritis- experience with 76
patients and review of the literature. Medicine (Baltimore) 74:
63-73, 1995
6. Spector DA, Milla J, Zauber N, Burton J: Glomerulonephritis
and Staphvlococcal aureus infections. C/in Nephrol 14: 256-
261, 1980
7. Boonshaft B, Maher iF, Schreiner GE: Nephrotic syndrome
associated with osteomyelitis without secondary amyloidosis.
Arc/i Intern Med 125: 322-327, 1970
8. Maher ER, Thiru 5, Hamilton DV, Wheatly T: Acute renal
failure due to glomerulonephritis associated with Staphylococcalinfection. Postgrad Med 60: 433-434, 1984
9. Connolly CE, Gallagher B: Acute crescentic glomerulonephritis
as a complication of a Stapkv!ococcus aureus abscess of hip joint
prosthesis [Letter]. J C/in Pathol 40: 1486, 1987
10. Beaufils M, Gibert C, Morel-Maroger L, Sraer JD, Kanfer A,Meyrier A, Kounlsky 0, Vachon F, Richet G: Glomerulonephri-
tis in severe bacterial infections with and without endocarditis.
Adt’ Nephrol 7: 217-234, 1978
1 1 . McKinsey DS, McMurray TI, Flynn IM: Immune complex gb-
merulonephritis associated with Staphylococcus aureus bactere-
mia: Response to corticosteroid therapy. Rev Infect Dis 12:
125-127, 1990
12. Takaue Y, Tokumaru M: Staphybococcal skin lesions and acute
glomerubonephritis [Letterl. N Engl J Med 307: 1 2 1 3-12 14, 1982
13. Keller CK, Andrassy K, Waldherr R, Ritz E: Postinfectious
glomerubonephritis-Is there a link to alcoholism? Q J Med 87:
97-102, 1994
14. Danovitch GM, Nord EP, Barki Y, Krugliak L: Staphylococcal
lung abscess and acute gbomerubonephritis. Isr J Med Sci 15:
840-843, 1979
15. Rosenberg HG, Donoso PL, Vial SU, Carranza C, Romero P:
Clinical and morphological recovery between two episodes of
acute gbomerulonephritis: A light and electron microscopic study
with immunofluorescence. C/in Nephro/ 21: 350-354, 1984
16. Pertschuk LP, Woda BA, Vuletin JC, Brigti Di, Soriano CB,Nicastri AD: Glomerubonephritis due to Staphylococcus aureus
antigen. Am J C/in Patho! 65: 301-307, 1976
17. Yum MN, Wheat Li, Maxwell D, Edwards JL: Immunofluores-
cent localization of Staphylococcus aureus antigen in acute bac-
terial endocarditis nephritis. Am J C/in Patho! 70: 832- 835, 1978
18. Eddy AA, Michael AF: Immunopathogenic mechanisms of gb-merular injury. In: Rena! Pathology, 4th Ed., edited by Brenner
BM, Tisher CC, Philadelphia, JP Lippincott Co., 1994, pp 162-221
19. Cosi FG, Mahan JD, Sedmak DD: Experimental glomerulone-
phritis induced by antigen that binds to gbomerular fibronectin.
Am J Kidney Dis 15: 160-168, 1990
20. Hebert LA, Cosio FG, Birmingham Di, Mahan JD, Sharma HM,
Smead WL, Goel R: Experimental immune complex-mediated
glomerulonephritis in nonhuman primates. 39: 44-56, 1991
21. Rees AJ: The immunogenetics of glomerulonephritis. Kidney mt45: 377-383, 1994
22. Couser WG, Johnson RJ, Young BA, Yeh CG, Toth CA, Ru-
dolph AR: The effects of soluble recombinant complement re-ceptor 1 on complement-mediated experimental gbomerubone-
phritis.J Am Soc Nephro/ 5: 1888-1894, 1995
23. iohnson RJ, Alpers CE, Pritzi P, Schulze M, Baker P, Pruchno C,
Couser WG: Platelets mediate neutrophil-dependent immune
complex nephritis in the rat. J C/in m,it’82: 1225-1235, 1988
24. Shah SV: The role of reactive oxygen metabolites in gbomerular
disease. Annu Rev Phvsio/ 57: 245-262, 1995
25. Sakurai H, Hisada Y, Ueno M, Sugiura M, Kawashima K, Sugita
T: Activation of transcription factor NF-KB in experimentalgbomerubonephritis in rats. Biochim Biophys Acta 13 16: 132-
138, 1996

Glomerubonephritis in Acute Osteomyelitis 1639
26. Forrest JW ir, John F, Mills LR, Buxton TB, Moore WL ir,
Hudson JB, Ozawa T: Immune complex gbomerulonephritis as-
sociated with Kiebsiella pneumoniae infection. C/in Nephro! 7:
76-80, 197727. Hyman LR, ienis EH, Hill GS, Zimmerman SW, Burkholder
PM: Alternate C3 pathway activation in pneumococcal glomer-ulonephritis. Am J Med 58: 810-814, 1974
28. Zappacosta AR, Ashby BL: Gram-negative sepsis with acute
renal failure: Occurrence from acute glomerulonephritis. JAMA
238: 1389-1390, 1977














![Acute glomerulonephritis 1[autosaved]](https://static.fdocuments.in/doc/165x107/558406c7d8b42a126e8b4928/acute-glomerulonephritis-1autosaved.jpg)