29318203 Acute Glomerulonephritis
57
Acute Glomerulonephr itis
-
Upload
john-paul-agraviadorbiltz- -
Category
Documents
-
view
109 -
download
0
Transcript of 29318203 Acute Glomerulonephritis

Acute Glomerulonephri
tis

Introduction

A. Background of the studyDuring our third day of hospital duty at Amang
Rodriguez Medical Center Pedia Ward, we encountered a patient with Acute Glomerulonephritis. Mr. J VS, 4 years old, was admitted with the chief complaint of edema and swelling of the testicles on February 20, 2010.
Acute glomerulonephritis refers to a specific set of renal diseases in which an immunologic mechanism triggers inflammation and proliferation of glomerular tissue that can result in damage to the basement membrane, mesangium, or capillary endothelium. There are many diseases that cause an active inflammation within the glomeruli. Some of these diseases are systemic and some occur solely in the glomeruli. When there is active inflammation within the kidney, scar tissue may replace normal, functional kidney tissue and cause irreversible renal impairment.

Most original research focuses on the post streptococcal patient. Acute glomerulonephritis is defined as the sudden onset of hematuria, proteinuria, and red blood cell casts. This clinical picture is often accompanied by hypertension, edema, and impaired renal function.
Although this is primarily a disease of children, with ages 4-12 being at high risk, it can occur at almost any age. Males are more susceptible than females, with a ratio of 1.7-2:1. No specific race is considered at high risk of acquiring this illness, though those in lower socioeconomic brackets are more prone to this due to environmental and sanitary conditions.

B. Objectives of the Study General
The general objective of this case presentation is to foster and develop knowledge and skills in providing care and management for a patient with acute glomerulonephritis.
Specific KNOWLEDGE •To define acute glomerulonephritis•To know the clinical manifestations, nursing management and interventions for patients who have this disease.•To know the different medications that needs to be taken including its side effects which can be harmful to the patient.

SKILLS•To be able to obtain, document, and present a comprehensive medical history.•To perform initial physical examination such as general assessment of the patient’s appearance, position and degree of comfort.•To apply necessary skills in providing care for a client with acute glomerulonephritis ATTITUDES•To learn how to establish rapport with the client and significant others.•To be able to recognize the importance of patient and familial preferences when selecting among treatment options.

C. Scope and Limitation of the StudyThe scope of the study encompasses the
anatomy, physiology, and pathophysiology of the disease acute glomerulonephritis. While dealing with Mr. J VS’s case, we are subjected with the following limitations of our study:
The group only had 2 days (Feb. 24-25, 2010) of actual interaction with the patient at Amang Rodriguez Medical Memorial Center in Marikina City, Metro Manila.
The group credited the study on the references prior to books, researches in the internet and data collected from the interview with the client/family members, physical assessment and the patient’s chart.

D. Conceptual FrameworkFor this case, we used Elizabeth Ahmann’s
Concept of Family-Centered Care. This concept focuses on rendering care by involving the client’s family in the various stages of the client’s care. This focuses on the following key concepts:•The family is the most constant thing in the child’s life•Nursing strategies must encourage the family’s involvement•Parent-professional collaboration or partnership
Since parental involvement and parent-professional collaboration is vital in rendering care, it has to be achieved using the following strategies:•Establish a caring environment•Active listening; eliciting and focusing on parental goals and aspirations

• Effective communication; ascertaining the parents’ perception of the child’s condition
• Explaining and clarifying misconceptions• Acknowledgement and acceptance of differences• Recommending interventions; elicit parent’s
suggestions on plan of care• Negotiating disagreements regarding the child’s plan
of care

CLINICAL SUMMARY

A. General DataName: JVSAddress: Batasan Hills, QCAge: 4 y/oReligion: Roman CatholicCivil Status: SingleNationality: FilipinoDate of Birth: March 15, 2006Date of Admission: February 18, 2010Ward and Room: Neuro Adolescence Pedia WardAdmitting Diagnosis: AGNAttending Physician: Dr. NavarroSources of Information: Patient, Relatives and Related Medical PersonnelThe Scale of Reliability: Primary & Secondary sources were used

B. Chief ComplaintEdema and swelling of the testicles
C. History of Present Illness
2 weeks PTC – Client had an episode of sore throat; no consult done; no meds taken; only gargled with warm water and salt.
A few days PTC – Client’s mother noted tea-colored urine, along with diminished urinary frequency. Edema noted around the eyes, ankles and testicles, with testicular enlargement causing alarm for mother. Sought consult at private clinic referred to Amang ER admitted to Pedia ward

D. Past Medical HistoryCough, colds, fluSore throat (undiagnosed) – possible streptococcal infection Family History(+) Asthma- Father Side(+) Hypertension- Mother Side

SYSTEM
General “May pagkamaputla… Minsan nanghihina…”
Skin
Head
Eyes and Ears “Yung dito nya (points to area around eyes), medyo manas”
Throat and Mouth
“Naaawa ako kasi nauuhaw siya, pero di daw pwedeng painumin ng marami”
Neck
Breast
Respiratory
CVS
GIT “Minsan hirap siyang dumumi”
GUT“Hindi pa sya umiihi sa araw na ito.. parang yellow orange yung ihi nya”
Extremities “Nagmanas yung sa may bandang paa nya”
Neurologic
Hematologic
Endocrine
Psychiatric “Bugnutin… Suplado minsan…”
E. Review of System- All Subjective Complaints
Note: these statements were verbalized by the mother

FINDINGSNORMAL VALUES
ANALYSIS/ INTERPRETATION
Height
Weight 94cm
14.5kg
BMI= wt kg
Ht m²
=14.5kg
(0.94m)²
=16.4 kg/m²
73rd percentile of BMI or within normal range.
However height and weight are within the 15th percentile
Vital Signs
BP=110/80Temp=38.4 °CPR=112 bpmRR=22 cycles/min
BP: 80/50-100/70
T: 36.5 – 37.5 °C
P: 75-120
R: 15-25
Hypertensive
Febrile
F. Physical AssessmentA. General Appearance/ Survey:
The client looks weak and pale. He sleeps a lot and talks only when asked. The client experiences cold and clammy perspiration.
B. Measurement

BODY PARTS NORMAL FINDINGS ACTUAL FINGDINGS ANALYSIS/ INTERPRETATION
A. HEADSkull Rounded, (normocephalic and
symmetrical, with frontal, parietal, and occipital prominence), smooth skull contour
Smooth, uniform consistency; absence of nodules or masses
Rounded, (normocephalic and symmetrical, with frontal, parietal, and occipital prominence), smooth skull contour
Smooth, uniform consistency; absence of nodules or masses
Normal
Hair Evenly distributed hair thick hair silky, resilient hair no infection of infestation variable amount
Evenly distributed hair thick hair dry no infection of infestation variable amount
Normal
Face Symmetric or slightly asymmetric facial features; palpebral fissures equal in size, symmetric nasolabial folds
Symmetric facial movements
Symmetric or slightly asymmetric facial features; Periorbital area slightly puffy but non-tender; symmetric nasolabial folds
Symmetric facial movements
Periorbital edema, fluid volume excess
C. Head to Toe Assessment

Eye/Vision
Eyeball Movement symmetrical can move to the 6 cardinal position of gaze
Not protruding
Movement symmetrical can move to the 6 cardinal position of gaze
Not protruding
Normal
Lid margins Shiny, smooth and pink or red Slightly pale Indicates anemia
Conjunctiva Pink Pale Indicates anemia
Sclera White White Normal
Pupils PERRLA PERRLA Normal
Eyebrow, Lashes, Color, Symmetry, quality of hair, placement
Hair evenly distributed; skin intact; Eyebrows symmetrically aligned; equal movement
Lashes equally distributed; curled slightly outward
Hair evenly distributed; skin intact; Eyebrows symmetrically aligned; equal movement
Lashes equally distributed; curled slightly outward
Normal
Eye movement in all direction
Both eyes coordinated, move in unison, with parallel alignment
Both eyes coordinated, move in unison, with parallel alignment Normal

VISION TESTING
Visual Field When looking straight ahead, client can see objects in periphery
When looking straight ahead, client can see objects in periphery
Normal
Visual acuity Able to read newsprint Able to correctly identify distant
letters
Able to read newsprint Able to correctly identify distant
letters
Normal
EARS
Pinna Color same as facial skin Symmetrical Auricle aligned with outer
canthus of eye about 10˚ from vertical
Mobile , firm and not tender Pinna recoils after it is folded.
Color same as facial skin Symmetrical Auricle aligned with outer
canthus of eye about 10˚ from vertical
Mobile , firm and not tender Pinna recoils after it is folded.
Normal
External Canal
Distal 3rd contains hair follicles and glands
No discharges
Distal 3rd contains hair follicles and glands
No discharges noted
Normal
Hearing acuity
Assess for normal tones Normal voice tones audible Watch Tick test Able to hear tickling in both ears
Assess for normal tones Normal voice tones audible Watch Tick test Able to hear tickling in both ears
Normal

NOSE Symmetric and straight No discharge or flaring Uniform color No tender; no lesions Air moves freely as the
client breathes through the nares
Mucosa pink
Symmetric and straight No discharge or flaring Uniform color No tender; no lesions Air moves freely as the
client breathes through the nares
Mucosa pink
Normal
MOUTH/LIPS Lips and Buccal mucosa; uniform pink, soft, moist, smooth texture
Symmetry of contour Ability to purse lips
Lips and Buccal mucosa; pale and slightly dry
Symmetry of contour Ability to purse lips
Indicates anemia
Gums Pink gums; moist, firm texture to gums
No retraction of gums(pulling away from the teeth)
Slightly pale; slightly dry, firm texture to gums
No retraction of gums(pulling away from the teeth)
Indicates anemia
Teeth Smooth, white, shiny tooth enamel
Smooth, slightly yellowish, shiny tooth enamel
Normal

Tongue Tongue/floor of the mouth:
Central position
Pink color (some brown pigmentation
on tongue borders in dark-skinned
clients);moist; slightly rough; thin
whitish coating
Smooth, lateral margins; no lesions
Raised papillae (taste buds)
Tongue movement: moves freely; no
tenderness
Tongue/floor of the mouth:
Central position
Pale; slightly dry; slightly rough; thin
whitish coating
Smooth, lateral margins; no lesions
Raised papillae (taste buds)
Tongue movement: moves freely; no
tenderness
Indicates
anemia
Palate-
hard /soft
Light pink, smooth, soft palate
Lighter pink hard palate, more
irregular texture
Positioned in midline soft palate
Light pink, smooth, soft palate
Lighter pink hard palate, more
irregular texture
Positioned in midline soft palate
Normal
Orophary
nx /Tonsil
Pink and smooth posterior wall
No discharge; Of normal size
Pink and smooth posterior wall
No discharge; Of normal sizeNormal

CHEEKS Even color Pale Indicates anemia
NECK Muscles equal in size; head centered
Coordinated, smooth and movements with no discomfort
Equal strength Shoulders- equal strength Lymph nodes: Not palpable
Muscles equal in size; head centered
Coordinated, smooth and movements with no discomfort
Equal strength Shoulders- equal strength Lymph nodes: Not palpable
Normal
CHEST Absence of abnormal sounds like wheezing and crackles
Normal rate (15-25 cycles/min)
Slight crackles noted upon auscultation
RR=25 cycles/min
May indicate onset of pulmonary edema

HEART No murmurs, crackles, gallops
noted No murmurs, crackles, gallops
noted Normal
BREAST Rounded shape, slightly unequal in size, generally symmetric.
Skin uniform in color same appearance as skin of abdomen or back.
Skin smooth and intact. Areola: round and oval and
bilaterally the same Color varies widely, from light
pink to the dark brown Irregular placement of
sebaceous glands on the surface of the areola (Montogomery’s tubercles)
Nipples: Round, everted and equal in size; similar in color soft and smooth; both nipples point in same direction
Breast No tenderness, masses,
nodules or nipples discharge
Rounded shape, slightly unequal in size, generally symmetric.
Skin uniform in color same appearance as skin of abdomen or back.
Skin smooth and intact. Areola: round and oval and
bilaterally the same Color varies widely, from light
pink to the dark brown Irregular placement of
sebaceous glands on the surface of the areola (Montogomery’s tubercles)
Nipples: Round, everted and equal in size; similar in color soft and smooth; both nipples point in same direction
Breast No tenderness, masses,
nodules or nipples discharge
Normal

ABDOMEN Unblemished skin Uniform color Flat, rounded or scaphoid No evidence of
enlargement of liver or spleen.
Symmetric contour Symmetric movements
caused by respiration Audible bowel sounds;
absence of arterial bruits No tenderness over
costovertebral angle upon palpation/percussion
Unblemished skin Uniform color Flat, rounded or
scaphoid No evidence of
enlargement of liver or spleen.
Symmetric contour Symmetric movements
caused by respiration Audible bowel sounds;
absence of arterial bruits
Tenderness noted over costovertebral angle, (+) lumbar punch
Tenderness is due to swelling or hyperplasia of renal parenchyma
UPPER EXTREMITIES
Absence of edema Even color and smooth
texture Unlimited movements
such as adduction, abduction etc.
Absence of edema Even color and smooth
texture Unlimited movements
such as adduction, abduction etc.
Normal

LOWER EXTREMITIES
Absence of edema Even color and
smooth texture Unlimited
movements such as adduction, abduction etc
Edema noted around ankles
Slightly gray in color, smooth texture
Unlimited movements such as adduction, abduction etc
Fluid volume excess

Before Hospitalization
During Hospitalization
Analysis/ Interpretation
Fluid and NutritionAt least 6 glasses, healthy appetite,
dislikes some veggies.
Restricted fluid and protein intake, slight decrease in appetite
Fluid restriction and dietary modification is indicated to minimize fluid volume excess and preserve kidney function. Decrease in appetite may be due to lesser palatability
of hospital food.
Elimination
Formed stools, adequate urine
output, yellowish urine – as verbalized
by mother
Incidence of constipation noted, decreased urinary
frequency and output, tea colored urine
Changes in elimination pattern
due to disease process and fluid
restriction.
Safety, Activity and Exercise
Energetic, “sobrang likot” as verbalized by
mother
Decreased energy, “minsan matamlay”
Excessive movement speeds up protein catabolism, and is
therefore not advised.
H. Activities of Daily Living

Hygiene and Comfort
Takes a bath regularly, somewhat
negligent about oral care and handwashing
Occasional bath, more of sponge
bathing. Oral care done when
remembered.
Alteration in hygienic practices
related to hospitalization
Rest and Sleep 6 hrs or more of sleep
Asleep most of the time
Conserving energy; following
orders to minimize activity
Substance Abuse Not applicable Not applicable The client is a child
Sexual Activity Not applicable Not applicable The client is a child

TEST RESULT REFERENCE VALUES INTERPRETATION
RBC 3.62 4.6-6.2 x 106/uLPossibly due to
hematuria
Hgb 9.20 10.0-18.0g/dLDue to increased
blood volume
Hct 26.7% 40.0-54.0%Due to increased
blood volume
Platelet 385 150-450 x 103/uL Normal
WBC 10.8 5-10 x 103/uLMay indicate
infection
I. Laboratory/ Diagnostic ExamsA. Hematology Report

TESTS RESULT REFERENCE VALUES INTERPRETATION
Color AmberPale yellow, straw to
amberNormal
Transparency Turbid Clear to slightly hazy Increased sediments
Reaction Acidic Acidic Normal
Specific Gravity 1.020 1.016-1.022 Normal
Glucose +1 (-) Glycosuria and
proteinuria due to
increased glomerular
permeabilityProtein +2 (-)
WBC >100/HPF Pyuria, indicatory of UTI
RBC + NTC Hematuria
A.Urinalysis

c. Ultrasound KUBResult: The right kidney measures 8.0 x 3.4 x 2.8cm and the left measures 7.2 x 2.7 x 3.9cm with cortical thickness of 10cm,both kidneys have increase parenchymal etchonegenicity.There is poor corticomedullary delineation, no evident mass, lithiasis and hydronephrosis. The urinary bladder is distended without wall thickening or intravesical echoes.Interpretation: Bilateral Renal Parenchymal Disease.Unremarkable Urinary Bladder. Final Diagnosis
Acute Glomerulonephritis

COURSE IN THE WARD

On February 18, 2010 at 9:10 am, the patient was brought to Pediatric ward from ER via wheelchair and admitted to Neuro/Adolescent Room. The patient was then placed on a low salt and low fat diet ordered by Dra. Navarro.
On February 24, 2010 at 4:10 pm, we received patient on bed, awake with IV heplock at right metacarpal vein. The I & O and vital signs are monitored, RR=22, PR=112, BP=110/80, Temp= 38.4°C. He was febrile and we gave him a Tepid Sponge Bath (TSB) to lower his temperature. After 30minutes, his temperature subsides at 37.9°C.
On February 25, 2010 at 3:50 pm, the patient was still on bed, awake and not cooperative with IV heplock. I & O was taken and recorded. The vital signs were also monitored, RR=24, PR=122, BP=100/60, Temp=37.7°C. After all intervention was done, health teaching regarding on proper personal hygiene practices, to weigh daily, reporting signs of protein deficiency, increased ICP, or DOB was told to the patient and to guardian.

ANATOMY

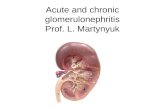
The kidneys are two, bean-shaped organs that are located in the back part of the abdomen, on either side of the spine and approximately between the twelfth thoracic and third lumbar vertebrae. Often, the left kidney is positioned up to an inch higher than the right kidney. Each kidney is about 4-5 inches long and about two inches thick, weighing 4-6 ounces in the average adult. Because of the presence of many blood vessels, the kidneys are colored a dark reddish-brown.Each kidney features a concave lateral side, where an opening, called the hilus, admits the renal artery, the renal vein, nerves, and the ureter. Within the kidney is the renal sinus, or cavity. Within the renal sinus are the functional group of the filtration called the nephrons, of which there are more than a million within each kidney. At the top of each kidney is an adrenal (also called suprarenal) gland.
The Kidneys

The Nephron
The nephron is the functional unit of the kidney, responsible for the actual purification and filtration of the blood. About one million nephrons are in thecortex of each kidney, and each one consists of a renal corpuscle and a renal tubule which carry out the functions of the nephron. The renal tubule consists of the convoluted tubule and the loop of Henle.The nephron is part of the homeostatic mechanism of the body. This system helps regulate the amount of water, salts, glucose, urea and other minerals in the body. The nephron is a filtration system located in the kidney that is responsible for the reabsorption of water, salts. This is where glucose eventually is absorbed in the body.The Loop of Henle is the part of the nephron that contains the basic pathway for liquid. The liquid begins at the Bowman's capsule (upper left) and then flows through the proximal convoluted tubule. It is here that Sodium, water, amino acids, and glucose get reabsorbed. The filtrate then flows down the descending limb and then back up. On the way it passes a major bend called the Loop Of Henle. This is located in the medulla of the kidney. As it approaches the top again, hydrogen ions (waste) flow into the tube and down the collecting duct.So, essentially, nutrients flow in through the left and exit through the right. Along the way, salts, carbohydrates, and water pass through and are reabsorbed.

The GlomerulusThe glomerulus is the main filter of the nephron and is located within the Bowman's capsule. The glomerulus resembles a twisted mass of tiny tubes through which the blood passes. The glomerulus is semipermeable, allowing water and soluble wastes to pass through and be excreted out of the Bowman's capsule as urine. The filtered blood passes out of the glomerulus into the efferent arteriole to be returned through the medullary plexus to the intralobular vein.

Bowman's Capsule The Bowman's capsule contains the
primary filtering device of the nephron, the glomerulus. Blood is transported into the Bowman's capsule from the afferent arteriole (branching off of the interlobular artery). Within the capsule, the blood is filtered through the glomerulus and then passes out via the efferent arteriole. Meanwhile, the filtered water and aqueous wastes are passed out of the Bowman's capsule into the proximal convoluted tubule.

PATHOPHYSIOLOGY

Most forms of acute poststreptococcal glomerulonephritis are mediated by an immunologic process. Both cellular and humoral immunity is important in the pathogenesis of acute poststreptococcal glomerulonephritis. Humoral immunity in acute poststreptococcal glomerulonephritis is presumed to be mediated by the in situ formation of nephritogenic streptococcal antigen-antibody complexes and circulating immune complexes. The most widely proposed mechanism for the development of acute poststreptococcal glomerulonephritis is that nephritogenic streptococci produce proteins with unique antigenic determinants. These antigenic determinants have a particular affinity for sites within the normal glomerulus.
Following release into the circulation, these antigens bind to these sites within the glomerulus. Once bound to the glomerulus, they activate complement directly by interaction with properdin. Glomerular-bound streptococcal antibodies also serve as fixed antigens and bind to circulating antistreptococcal antibodies forming immune complexes. Complement fixation via the classical pathway leads to generation of additional inflammatory mediators and recruitment of inflammatory cells.

Polymorphonuclear leukocytes are also often observed as part of the inflammatory process. In persons with the most severe disease, the glomeruli appear bloodless because of the associated edema of the capillary walls, which impedes glomerular perfusion. A direct correlation exists between the severity of the histologic process and the clinical manifestations of the disease during the acute phase and possibly the prognosis.
In most patients with moderate-to-severe AGN, a measurable reduction in volume of glomerular filtrate (GF) is present, and the capacity to excrete salt and water is usually diminished, leading to expansion of the extracellular fluid (ECF) volume. The expanded ECF volume is responsible for edema and, in part, for hypertension, anemia, circulatory congestion, and encephalopathy.

CLINICAL MANIFESTATIONS•Oliguria/anuria, due to decreased glomerular filtration rate (GFR)•Elevated BUN and serum creatinine, due to decreased urine output•Hematuria (microscopic or gross), occurs in approximately 30% of cases; urine may appear dark, cola-colored or tea-like•Proteinuria, primarily albumin, due to increased permeability of glomerular membrane•Edema (facial, periorbital and/or pedal), hypertension, anemia, increased ICP, pulmonary edema, all related to increased circulating blood volume/excess extra-cellular fluid (ECF)•Tenderness over the costo-vertebral angle ( + kidney punch), due to swelling of kidneys

ASSESSMENT AND DIAGNOSTICS•History taking; 1-3 weeks post-streptococcal infection (1-2 weeks post-pharyngitis)•Urinalysis; dark urine, (+) RBC, albumin, casts; specific gravity > 1.020•CBC; decreased Hgb, Hct•Blood chemistry; elevated BUN and serum creatinine •Kidney biopsy, electron microscopy and immunofluorescent analysis•Antistreptolysin O; increased in 60-80% of patients•KUB; enlarged kidneys
COMPLICATIONS•Hypertensive encephalopathy•Heart failure•Pulmonary edema•Rapidly progressive glomerulonephritis end-stage renal disease (ESRD)

MEDICAL MANAGEMENTAcute glomerulonephritis is usually self-limiting, so
management is aimed at treating symptoms, preserving kidney function and treating complications promptly. Pharmacologic treatment depends on a case-to-case basis. If there is residual streptococcal infection, then penicillin is the drug of choice; however, other antibiotics can also be given. Loop diuretics and antihypertensives are used to control hypertension. Sodium is restricted, as is fluid intake because of fluid volume excess.
Carbohydrates are given liberally to provide energy and to reduce catabolism of proteins. As for proteins, there are two schools of thought: dietary restriction or increased intake. Dietary restriction is merited only when there is nitrogen retention (elevated BUN) and/or renal insufficiency. However, due to albuminuria, the client loses more proteins than can be replaced. Hence, most diets would include foods high in albumin and other complete proteins, such as egg whites and dairy products.

NURSING MANAGEMENT•Intake and output are measured carefully and recorded. •Patient’s daily weight is also recorded using the same scale at the same time of the day as previous weighing sessions.• Assess also for signs of increased ICP, such as headaches or blurring of vision.• Client is also advised to report immediately should any sign or symptom of renal failure occur (fatigue, nauseas, vomiting, diminishing urine output).• Maintain dietary and fluid restrictions to avoid worsening edema and hypertension.•Stress the importance of follow-up check-ups to monitor BP, urinalysis, blood chemistry and CBC, to determine whether there is progress in the management of the disease.•Educate client and significant others on proper administration of medications, especially those taken orally; include adverse effects, dosage, time, frequency, and the desired actions of the medications taken and the precautions to be followed.

PROBLEM LISTS

• Fluid volume excess related to decreased glomerular filtration rate as evidenced by decreased urine output, edema and hypertension
• Imbalanced body temperature related to unknown etiology (possible infection) as evidenced by Temp=38.4 °C
• Imbalanced nutrition: less than body requirements related to increased glomerular permeability as evidenced by proteinuria
• Knowledge deficit related to medical management of the disease as evidenced by questioning attitude by the mother
• Anxiety related to outcome of treatment• Impaired parent-child interaction related to irritability of
child• Risk for impaired skin integrity related to edema/altered
skin turgor• Risk for infection related ongoing disease process
(immunocompromised)• Note: Underlined diagnoses are considered priority
problems which the group will address, and upon which we will formulate plans of care.

NURSING CARE PLAN

FLUID VOLUME EXCESSASSESSMENT DIAGNOSIS PLANNING INTERVENTION
Subjective: “Hindi pa siya umiihi sa araw na ito.” – as verbalized by the mother Objective:Periorbital and pedal edema notedIrritable when awakeLOC: lethargicUA: SG= 1.020CBC: Hct =26.7% Hgb = 9.2VS: BP = 110/80
Fluid volume excess related to decreased glomerular filtration rate as evidenced by decreased urine output, decreased Hgb & Hct and Hypertension
Short Term: After 8 hours of intervention, the client will: Maintain fluid volume at a functional level as evidenced by stable vital signs, ideal body weight, and reduction of edema.
IndependentEvaluate extent of fluid excess:Assess vital signs: BP, PR, RR, quality of pulse, respiratory effort.Note complaints associated with fluid excess: edema, poor skin turgor, distention of neck veins, sudden increase in weightObtain and evaluate lab results (Hct, Hgb, Serum electrolytes, BUN/Creatinine, total protein/albumin)Limit sodium and fluid intake to prescribed value:Advise family members to remove water, food or drinks from bedside.Identify potential sources of fluid (IV and oral meds, food, etc), and factor them in when determining fluid intake. Assist client and family to cope with the discomfort caused by fluid restrictions:Explain the rationale behind fluid restriction.Encourage the family to provide a supportive and caring atmosphereProvide and/or encourage frequent oral hygieneDependentAdminister IV fluids and meds as prescribed.

RATIONALE EVALUATION Obtain baseline for comparison. Objective and subjective data help identify underlying cause and monitor progress. Fluid restriction is based on urine output, weight and response to therapy.To monitor other sources of excess fluid Understanding and comfort promotes compliance. Oral hygiene minimizes dryness of oral mucosa.
Prevent fluid overload and address causative factors.
After performing interventions for 8 hours, the client: Had vitals near normal levels, no longer complains of headaches, and has visibly reduced periorbital edema.Complied and actively participated in the interventions presentedVerbalized that was willing to comply with health teachings provided as to fluid and dietary restrictions.

IMBALANCED BODY TEMPERATURE (FEVER)
ASSESSMENT DIAGNOSIS PLANNING
Subjective:
“Kanina pa sya mainit”
– as verbalized by the
mother
Objective:
VS: Temp=38.4 °C
Imbalanced body
temperature related to
unknown etiology
(possible infection) as
evidenced by Temp=38.4
°C
Short Term:
After 4 hours of
intervention, the client
will:
Maintain body
temperature at a
functional level as
evidenced by Temp
<37.8 °C.

INTERVENTION RATIONALE EVALUATIONIndependentAssess and evaluate client’s current status:Assess vital signs: Temperature.Note environmental factors that may contribute to increased body temperature (tight clothing, poor ventilation, hot and humid environment)Perform measures to reduce body temperature:Continuous TSB for 15-30 minutes, repeated as needed.Loosen clothing.Promote adequate ventilation.Turn on air conditioner, if applicable.Provide and/or encourage frequent oral hygieneAssist client and family in planning and performing future self-care needs:Demonstrate proper procedure for TSB.Explain the rationale behind intervention doneEncourage the family to provide a supportive and caring atmosphereDependentAdminister IV fluids and meds as prescribed.
Obtain baseline for comparison. Objective and subjective data help identify underlying cause and monitor progress. These procedures promote heat loss via various mechanisms.Heat can cause dryness, which may lead to damage or injury of the mucosa. Understanding and comfort promotes compliance. Enhanced knowledge can lead to better health practices. To address underlying factors.
After performing interventions for 4 hours, the client: Temp = 37.9 °C. Although target body temperature was not achieved, the reduction is significant enough. Further management may be indicated if temperature is not maintained at current level or increases in the future.Complied and actively participated in the interventions presented

IMBALANCED NUTRITION: LESS THAN BODY REQUIREMENTS
ASSESSMENT DIAGNOSIS PLANNINGSubjective: “Andaming bawal ipakain sa kanya” – as verbalized by the mother Objective:UA: Protein = +2 Glucose = +1
Imbalanced nutrition: less than body requirements related to increased glomerular permeability as evidenced by proteinuria
Short Term: After 2 days of intervention, the client and/or his relatives will: Comply with dietary restrictionsHave increased energy levels and appetite.Prevent symptoms associated with protein deficiency

INTERVENTION RATIONALE EVALUATIONIndependent1.Assess nutritional status:Assess body weight, lab values (serum creatinine, BUN, UA protein).Determine cliet’s dietary patterns and preferencesAssess for other factors that influence nutritional status (current diet not to client’s liking, lack of resources, lack of understanding about diet)1.Promote a diet based on current nutritional status:Promote a low-sodium, low-potassium, high-calorie, protein- restricted but albumin-rich diet (graham crackers, low-salt crackers, egg whites, dairy products)Identify food within the client’s preferences but comply with dietary restrictions. Provide a list.Advise family members to remove water, food or drinks from bedside.1. Assist client and family to cope with the discomfort caused by restrictions in the diet:Explain the rationale behind dietary restriction.Encourage the family to provide a supportive and caring atmosphere Provide alternatives for improving diet without deviating from the prescribed one.1. Monitor and record client’s progress:Weigh patient dailyAssess for signs of inadequate protein intake (edema, delayed healing, decreased serum albumin levels)CollaborativeCoordinate with other health care personnel (physician, nutritionist).
Obtain baseline for comparison. Objective and subjective data help identify underlying cause, aid in planning of care and monitor progress. Reduces the sources of restricted foods, at the same time provides the caloric and nutritional needs of the client and spares protein.Preferences are considered to promote compliance.Prevents deviations from prescribed diet. Understanding and comfort promotes compliance and also increases appetite. Makes diet more palatable to the client. To evaluate progress and to detect complications early Ensures continuity of care.
After performing interventions for 2 days, the client and/or relatives: Had observably increased energy levels.Consumed high-calorie food within restrictions.Reported increased appetiteComplied and actively participated in the interventions presentedVerbalized that was willing to perform health teachings provided as to diet restrictions and modifications.Reported no signs of progression of edema.

DISCHARGE PLAN

MEDICATION•Nifedipine 10mg PO TID•Furosemide 20mg x 1 tab PO ODEXERCISE/ENVIRONMENT •Advise client to have non-strenuous and non jarring exercise such as walking.• Tell client to initiate exercise through repetitive low intensity exercises first.•As time and experiences increases the client can move to higher intensity exercises.•Advice client and her family to try to have or maintain safe , clean, comfortable and calm environment .•Advise significant others to be supportive.

TREATMENT•Ensure follow up and self care.•Advice client or significant others to take in time prescribed medicines specially high blodd pressures•Ensures dietary restrictions on salt, fluids protein ad other substances may be recommended•Tell significant others to closely watched and monitor for signs of developing kidney failureHEALTH TEACHING/ HYGIENE • Describe to the client the signs and symptoms to be reported immediately (Blood in the urine , foamy urine, swelling on he face , legs and abdomen.•Clearly and specifically explain the nature of the disease, its coarse and eventual prognosis of the condition to the child ( if old enough to understand ) and parents or caregivers, They need to understand the while complete resolution is expected a small possibility exists for persistent disease and that an even smaller possibility exists for progression . This info. Is necessary for some pt. to ensure that compliance with the follow up program occurs.

• Clearly outline a follow-up plan and discuss the plan with the family . BP measurements and urine examinations for proteins and blood constitutes the basis of follow up plan. Perform examination at 4 week 6 week intervals for the first 6 months .and at 3 months to 6 months
• Intervals there after until both hematuria and proteinuria have been absent and bp has been normal for 1yr . documenting that low C3 Has returned to normal after 8-10 weeks may be useful
• OPD• Advise significant others to immediately consult her
physician if signs and symptoms of the diseases occurs or persist.
• Remind client of her check-up schedules and appointments . tell him to attend them as diligently as he can . this is to rule out the recurrence or progression of the problem.

DIET •Assure a low sodium, low protein diet.•Limitation of fluid and salt intake to minimize vascular overload and hypertension.SPIRITUAL• Counseling: Tell the client that neither he nor GOD is to blame for her condition , everything happens for a reason , GOD will not give you a problem you cant handle.•Advise relatives or significant others to provide moral support and widen their understanding •Also tell them to pray for the client to help with the recovery