A sneak peek into the future of vaccines A...A sneak peek into the future of vaccines GSK Asia HQ-...
35
Hui Process scientist China A/Prof Michael Nissen Director, Scientific Affairs-AP Singapore A sneak peek into the future of vaccines
Transcript of A sneak peek into the future of vaccines A...A sneak peek into the future of vaccines GSK Asia HQ-...

Hui
Process scientist
China
A/Prof Michael Nissen
Director, Scientific Affairs-AP
Singapore
A sneak peek into the future of vaccines

GSK Asia HQ- Singapore: Artistic impression
Employee of GlaxoSmithKline Vaccines& hold stock on LSTE
Adjunct Professor at Children’s Health Research Centre, University of QLD, Australia
2

Parasitic
Malaria
Viral
HIV
Ebola
RSV
Hepatitis C
Herpes zoster
GSK’s vaccine development pipeline has the potential to
help reduce the burden of many communicable diseases1,2
1. GSK. Vaccines. http://www.gsk.com/en-gb/about-us/what-we-do/vaccines/ (accessed February 2017); 2. GSK, 2016. Product pipeline – March 2016. http://www.gsk.com/en-
gb/investors/product-pipeline/ (accessed March 2017)
COPD, chronic obstructive pulmonary disease; HIV, human immunodeficiency virus; RSV, respiratory syncytial virus; TB, tuberculosis
Bacterial
TB
Group B Streptococcus
COPD
Meningococcal disease
Shigellosis
Pneumococcal disease
Poverty
Maternal
Paediatric
Therapeutic
Older
adults
Chronic
Emerging
disease
Adolescent
Drivers of vaccine
development:
$
$
$
$
$

GSK is developing innovative vaccines to help prevent
diseases
1. Ledgerwood JE et al. N Engl J Med 2017;376:928–938; 2. Dellagostin OA et al. Int J Mol Sci 2017;18:158; 3. Gerke C et al. PLoS ONE 2015;10:e0134478; 4. Di Pasquale A et al.
Vaccines 2015;3:320–343; 5. GSK. Vaccines. http://www.gsk.com/en-gb/about-us/what-we-do/vaccines/ (accessed March 2017); 6. GSK. Our vaccines. http://www.gsk.com/en-
gb/products/our-vaccines/#tab-2 (accessed March 2017); 7. Morrison C. Nat Rev Drug Discov 2016;15:521–522. 8. Feldman MF et al. PNAS 2005; 102(8): 3016-3021
Innovative technologies Vaccines for all5,6
Viral vectors1,4
Generalised
modules of
membrane antigens3
GSK Adjuvant
System4
Reverse
vaccinology2
Maternal
immunisation
Infants
Older adults
Paediatrics
Travellers
Adults
Adolescents
Self-amplifying
mRNA (SAM) 7Occupational health, e.g.
HCW*, military
*HCW = healthcare worker
Bioconjugation 8

Bexsero®
Meningococcal Group B Vaccine (rDNA, component, adsorbed)
Bexsero is a registered trademark of the
GlaxoSmithKline group of companies.
GlaxoSmithKline Biologicals S.A., Rixensart, Belgium
Prepared June 2016; VGBU/BEX/0005/16(1)
Bexsero is not registered or available in New Zealand

Neisseria meningitidis are classified into serogroups according
to the immunologic reactivity of their capsular polysaccharides1
– The polysaccharide capsule is key in determining virulence2
– Twelve serogroups have been identified based on the structure of their
polysaccharide capsule – only six (A, B, C, W, X and Y) cause invasive
meningococcal disease2,3
61. Rosenstein NE et al. N Engl J Med 2001;344:1378–1388; 2. Harrison OB et al. Emerg Infect Dis 2013;19:566–573; 3. WHO. Meningococcal meningitis fact sheet No. 141,
2015. http://www.who.int/mediacentre/factsheets/fs141/en (accessed November 2016). Images are © Hurd Studios, 2012 and courtesy of GlaxoSmithKline
Polysaccharide
capsule (serogroup)
PilusLipooligosaccharide
Cytoplasmic membrane proteins

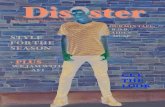
Incidence of Invasive Meningococcal Disease (IMD) by Age
IMD, invasive meningococcal disease.
Total IMD cases, N=3436 (reported cases for which age information was provided, excluding aggregated data); serogroup B IMD cases, N=2182.
*Countries: Austria, Belgium, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania,
Luxembourg (total IMD cases only), Malta, Netherlands, Norway, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden, United Kingdom.
European Centre for Disease Prevention and Control. Surveillance of invasive bacterial diseases in Europe, 2012. Stockholm: ECDC; 2015.
http://ecdc.europa.eu/en/publications/Publications/Surveillance%20of%20IBD%20in%20Europe%202012.pdf. Accessed 11Feb2016.
IMD
ca
se
s p
er
10
0,0
00
of th
e a
ge
gro
up
0
2
4
6
8
10
12
<1 1–4 5–14 15–24 25–44 45–64 ≥65Age (years)
Total IMD cases
Serogroup B IMD cases
– Incidence highest in infants and young children
– A second, smaller peak in incidence occurs in adolescents and young adults
Europe,* 2012
8

8%
26%
38%
26%
NEW ZEALAND(2013, n=57)13
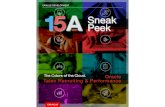
Neisseria meningitidis serogroup distribution varies between
regions/countries*
Other serogroups, not groupable, not tested, or missed
EUROPE(2014, n=2873)6
57%14%7%
9%
13%
57%12%
17%
78%
2%
10%8% 2%
53%30%
9%
7% 2%
Chart Title
7%12%
3%
42%
36%
29%
65%
6%
CANADA(2006–2011, n=1174)1
COLOMBIA(2015, n=48)3 BRAZIL
(2015, n=357)4
SOUTH AFRICA(2014, n=193)10
TURKEY(2005–2012, n=333)7
YWB CA
17%
40%36%
5% 3%
4%
64%
26%
28%
26%
10%
36%USA†
(2014, n=53)2
†USA: 36% ‘other’ serogroups includes
serogroup W and non-groupable;
surveillance data only covers some
areas of the USA, representing ~43.5
million people2
Serogroup data is across all age groups
Percentages may not total 100 due to rounding
ARGENTINA(2014, n=149)5
23%
9%
32%
16%
20%
47%
1%
49%
3%
AFRICANMENINGITIS
BELT (2015, n=1763)9
JAPAN(2014, n=59)11
AUSTRALIA(2014, n=165)12
SAUDI
ARABIA(2002–2011,
n=115)8
*Serogroup distribution cannot be directly compared across countries due to variability in surveillance data available.
<Further details on surveillance data for each country are shown on next slide for use as back-up, if required>
25%
60%
11%
2% 2%
Figure adapted from: 1. Li YA et al. Can Commun Dis Rep 2014;40(9):160–171; 2. Active Bacterial Core surveillance (ABCs). Surveillance reports, Neisseria meningitidis, 2014. Centers for Disease Control and
Prevention website. http://www.cdc.gov/abcs/reports-findings/survreports/mening14.pdf (accessed November 2016); 3. Vigilancia por laboratorio Neisseria meningitidis (aislaminetos invasores) periodo 1987–2015.
Instituto Nacional de la Salud. Grupo de Microbiologia. 2016. http://www.ins.gov.co/tramites-y-servicios/examenes-de-inter%C3%A9s-en-salud-publica/Microbiologa/informe%20Web%20N%20meningitidis%202015.pdf
(accessed November 2016); 4. Ministry of Health / SVS – Notifiable Diseases Information System – SINAN Net. http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinannet/cnv/meninbr.def (accessed November 2016);
5. Servicio Bacteriología Clínica-Departamento Bacteriología-INEI-ANLIS Dr.C.G. Malbrán-ARGENTINA. SIREVA II. http://antimicrobianos.com.ar/ATB/wp-content/uploads/2015/09/Tablas-vigilancia-SIREVA-II-Nm-2014-
Argentina1.pdf (accessed November 2016). 6. ECDC. Surveillance Atlas, 1999–2014. http://atlas.ecdc.europa.eu/public/index.aspx?Instance=GeneralAtlas (accessed November 2016); 7. Ceyhan M et al. Hum Vaccin
Immunother 2014;10:2706–2712; 8. Memish Z et al. Euro Surveill 2013;18:pii=20581; 9. WHO. 2016. Wkly Epidemiol Rec 2016;91:209–216; 10. GERMS-SA Annual Report 2014. National Institute for Communicable
Diseases. http://www.nicd.ac.za/assets/files/GERMS-SA%20AR%202014.pdf (accessed November 2016); 11. Fukusumi M et al. Vaccine 2016;34:4068–4071; 12. Australian Meningococcal Surveillance
Programme annual report 2014. www.health.gov.au/internet/main/publishing.nsf/Content/cda-pubs-annlrpt-menganrep.htm (accessed November 2016); 13. Lopez L et al. The epidemiology of meningococcal
disease in New Zealand in 2013. Institute of Environmental Science and Research Ltd (ESR), 2014
9
9%
6%
5%

Outer membrane vesicle (OMV) vaccines
Immunogenic and proven effective for a
single homologous serogroup B strain4,5
Limited protection against heterologous
meningococcal serogroup B strains4,5
Serogroup B strains are highly diverse4,5
• >5000 sequence types identified6
• >600 PorA variants (the dominant antigen in
OMV)4
A conjugate vaccine for Men B?
Vaccines with a single subcapsular antigen component do not offer broad protection
against Men B disease
Capsular vaccines
Poorly immunogenic1,2
• Structural homology between the
B polysaccharide of the capsule
and human tissue1,2
N meningitidis bacterial capsule Outer membrane “blebs” of N meningitidis
Image from Devoe et al. 19737
1. Finne J, et al. J Immunol 1987;138:4402–4407
2. Wyle FA, et al. J Infect Dis 1972;126:514–522
3. Sadarangani M, et al. Lancet Infect Dis 2010;10:112–124
4. Tan LK, et al. N Engl J Med 2010;362:1511–1520
5. Girard MP, et al. Vaccine 2006;24:4692–4700
6. Devoe IW, et al. Journal Exp Med 1973;138:1156–1167
10

Bexsero contains 4 antigenic components
fHbp: factor H–
binding protein
• Binds factor H,
which enables bacterial
survival in the blood1,2
Class
5
PorA
Class
4
PorB
LPS
OMV*
NadA: neisserial
adhesin A
• Promotes adherence to
and invasion of human
epithelial cells3–5
• May be important for
colonization4
NHBA: neisseria heparin–
binding antigen
• Binds heparin, which may
promote bacterial survival
in the blood6
• Present in virtually all
strains6,7
NZ PorA P1.4: porin A
• Major OMV protein8
• Shown to induce strain-
specific bactericidal
response when used in
MeNZB OMV vaccine^,8
^Developed by Chiron Vaccines in
association with the Norwegian
Institute of Public Health.
OMV, outer membrane vesicle.
1. Madico G, et al. J Immunol. 2006;177:501-510
2. Schneider MC, et al. Nature. 2009;458:890-893
3. Comanducci M, et al. J Exp Med. 2002;195:1445-1454
4. Capecchi B, et al. Mol Microbiol. 2005;55:687-698
5. Mazzon C, et al. J Immunol. 2007;179:3904-3916
6. Serruto D, et al. Proc Natl Acad Sci U S A. 2010;107:3770-3775
7. Bambini S, et al. Vaccine. 2009;27:2794-2803
8. Martin DR, et al. Clin Vaccine Immunol. 2006;13:486-491
9. Vesikari T, et al. Lancet. 2013;381:825-835
10. Vogel U, et al. Lancet Infect Dis. 2013;13:416-425
Identified using a “reverse vaccinology” approach
Multiple antigens may provide synergistic killing,
improve strain coverage, and insure against mutations9,10
11

Infants and children 2 months to <2 years of age
• 5849 received at least 1 dose of Bexsero
• 3285 received booster dose in second year of life
2677 adolescents (≥11 years of age) and adults
Bexsero safety was evaluated in 13 studies
including 9 randomised controlled clinical trials
250 children 2 to 10 years of age
>9000 subjects received at least 1 dose of the vaccine.
Studies included subjects from 2 months of age
Clinical trial experience with Bexsero
1. Bexsero Product Information
Study in special populations: children and adolescents aged 2 to 17 years
• 40 with complement deficiency; 107 with asplenia or splenic dysfunction
• 85 age-matched healthy participants
12

Bexsero Licensed Immunisation Schedules
3 doses2–5 months
6–11 months
12–23 months
2–10 years
11+ years
≥1 mo 1 dose age 12–15 mo*
2 doses
≥2 mo
≥1 mo
1 dose in the 2nd year of life≥2 mo post primary series
1 dose 12–23 mo post primary series
Need not established
Age groupPrimary
immunisation
Interval between
primary dosesBooster
The use of this vaccine should be in accordance with official recommendations.
*In case of delay, the booster should not be given later than 24 months.
European Union
Bexsero® [summary of product characteristics]. 13

Bexsero Immune Response in Infants Following
Vaccination at 2-4-6-12 Months
Figure adapted and reprinted from The Lancet, Vol. 381, Vesikari T et al., Immunogenicity and safety of an investigational multicomponent, recombinant, meningococcal
serogroup B vaccine (4CMenB) administered concomitantly with routine infant and child vaccinations: results of two randomized trials, Pages 825-835, Copyright (2013),
with permission from Elsevier.
1. Vesikari T, et al. Lancet. 2013;381:825-835; 2. Bexsero® [summary of product characteristics].
†Blood drawn at 7 months, N=1149–1183.‡Blood drawn at 12 months, N=434–437.§Blood drawn at 13 months, N=421–424.ǁN=100.
3 41
33
100 100
8484
81
99
22
61
100 10095
98
0
20
40
60
80
100
% o
f su
bje
cts
with
ba
cte
ricid
al tite
rs ≥
1:5
fHbp NadA PorA P1.4 NHBAǁ
Pre-booster (12 mo)1,‡Baseline1,* Post-primary (7 mo)1,† Post-booster (13 mo)2,§
2-4-6-12 month schedule with routine vaccines
14

*Routine vaccines: PCV7 and DTaP-HBV-IPV/Hib.†N=238–248.‡Criteria not met for lower limit of the 95% confidence interval for difference in seroresponse ≥10%.
Blood drawn at 7 months.
Vesikari T, et al. Lancet. 2013;381:825-835.
Routine vaccines alone*,†Bexsero® plus routine vaccines*,†
100 100 98 95 94 95 88 97 98 99100 100 100 99 98 97 94 98 100 1000
20
40
60
80
100
Diphtheria Tetanus PT FHA PRN Polio 1 Polio 2 Polio 3 HBV PRP-Hib
Antigens
% ≥0.15
mcg/mL% ≥10
mIU/mL% ≥1:8% ≥0.1
IU/mL
% ≥0.1
IU/mL
–1%(–5, 2)
–5%‡
(–11, –1)
–1%(–4, 2)
–2%(–5, –1)
–4%(–8, –1)
–4%(–8, –1)
0%(–1, 2)
0%(–2, 2)
–2%(–5, –1)
–1%(–3, 1)
% Seroconversion
(% 4-fold increase)
% S
ero
resp
onse o
r
% s
ero
co
nve
rsio
n
Immunogenicity of Routine Infant Vaccines
Administered with BexseroRoutine vaccines given with or without Bexsero at 2, 4, and 6 months of age
15

Tolerability Profile for Bexsero in Clinical Trials
*Pneumococcal 7-valent conjugate vaccine, diphtheria, tetanus, acellular pertussis, hepatitis B, inactivated poliomyelitis, and Haemophilus influenzae type b vaccine.†Separate vaccinations can be considered when possible. Separate injection sites must be used if more than one vaccine is administered at the same time.
Bexsero® [summary of product characteristics].
Most common adverse reactions
Bexserogiven alone
Bexsero given with other vaccines*,†
Infants and children
(less than 2 y)
Tenderness and erythema at the injection site, fever,
and irritability
Frequency of fever was similar to that associated
with routine infant vaccines* administered during clinical
trials
Higher rate of fever and systemic reactions
(irritability, change in eating habits, sleepiness,
tenderness at the injection site)
Adolescents and adults
The most common adverse reactions were pain at the injection site, malaise, and headache; fever rates were similar for Bexsero® compared with placebo
17

Impact of Prophylactic Paracetamol on Fever
0
10
20
30
40
50
60
NPP PP* NPP PP* NPP PP*
% S
ub
jects
6 hours Day 2 Day 3
Time
Post–any dose*
(2-3-4 month schedule)
38.5°C to <39°C
39°C to <40°C
≥40°C
NPP, no prophylactic paracetamol (N=181–182); PP, with prophylactic paracetamol (N=181–182).
*Subjects received 1 dose of 10–15 mg/kg oral paracetamol before vaccination, followed by 2 additional doses of paracetamol
4–6 hours after vaccination. Routine vaccines: PCV7 and DTaP-HBV-IPV/Hib.
Figure adapted and reprinted from Hum Vaccin Immunother, Vol. 10, Prymula R, et al., A phase 2 randomized controlled trial of a multicomponent meningococcal serogroup B
vaccine (I), Pages 1993-2004, Copyright (2014), with permission of the publisher (Taylor & Francis Ltd, http://www.tandfonline.com).
When Bexsero is given concomitantly with routine infant vaccines
18

UK: National MenB vaccination programme8‒10
In 2015, Bexsero was introduced to help
protect against MenB disease in the UK8 –
~700,000 infants per year were targeted
for vaccination9,10^
Canada: Regional vaccination campaign in Quebec and University outbreak in Nova Scotia5‒7
Regional campaign in Saguenay–Lac-Saint-Jean, Quebec5,6
In 2014, 57,038 residents or those in education aged ≥2 months
to ≤20 years were targeted for Bexsero vaccination to help
protect against the high incidence of MenB disease in the
region. Between 5 May and 17 June 2014, 43,740 individuals
received the first dose
Outbreak at Acadia University, Nova Scotia7
In 2015, a two-dose MenB vaccination campaign with Bexsero
was introduced at Acadia University, Nova Scotia – 2967
individuals received the first dose in February to March 2015
and 987 participants were assessed in an online safety survey
following dose 1*Under IND protocol prior to US approval (January 2015)1,3
^Using a dosing schedule outside of the approved label
Summary of Bexsero real-world experience
USA: University outbreaks
Princeton University and University of California at
Santa Barbara1,2
In 2013, the FDA authorised vaccination campaigns with
Bexsero* in response to two university outbreaks;
surveillance data for 15,236 individuals vaccinated with
Bexsero have been reported1,3
Santa Clara4
In 2016, a two-dose vaccination campaign with Bexsero
was introduced – 4921 individuals received the first
dose in February 2016
1. Watson P and Turner D. Vaccine 2016;34:875–80; 2. NMA 2016. http://www.nmaus.org/disease-prevention-information/serogroup-b-meningococcal-disease/outbreaks/
(Accessed September 2016); 3. US FDA press release 2015. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm431370.htm (Accessed September 2016);
4. Biswas HH et al. MMWR Morb Mortal Wkly Rep 2016;65:520–1; 5. INSPQ 2014 Interim report. https://www.inspq.qc.ca/pdf/publications/1902_SerogroupB_Meningococcal_Vaccine.pdf (Accessed September
2016); 6. CIUSSS 2015 Press release. http://santesaglac.com/medias/documents/communiques_presse/2015/COMMUNIQUE_meningoB__150415.pdf (Accessed September 2016);
7. Langley JM et al. Vaccine 2016;34:4046–9; 8. Ladhani SN et al. Arch Dis Child 2016;101:91–5; 9. ONS England and Wales 2014.
http://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/livebirths/bulletins/birthsummarytablesenglandandwales/2015-07-15 (Accessed September 2016); 10. NRS Scotland 2015.
http://www.nrscotland.gov.uk/news/2015/births-deaths-and-other-vital-events-preliminary-figures-for-2014-released (Accessed September 2016). Figure adapted from references 1–10
19

National vaccine
programme with the
entire UK birth cohort
Sophisticated
surveillance
Coverage:
1 dose = 95.5%
2 dose = 88.6%
2-dose effectiveness:
82.9% (24.1-95.2)
20

Summary
– Serogroup B disease affects mainly infants, is easily misdiagnosed, can kill within 24 hours
of onset, and may cause serious, lifelong disabilities despite appropriate medical treatment
– Bexsero is a novel meningococcal serogroup B vaccine for active immunisation against
invasive MenB disease
– Bexsero offers several schedule options that fit with routine vaccination visits and possible
catch-up programs
– In clinical trials, Bexsero has demonstrated a protective immune response in infants,
children, adolescents, and adults with or without routine vaccines
– Bexsero has a demonstrated safety profile based on an evaluation of >67,000 subjects
in clinical trials and postmarketing studies (from 2 months of age)
– Results from the UK, Canada and USA demonstrate real-world effectiveness of Bexsero*
21*Bexsero® is not expected to provide protection against all circulating meningococcal group B strains.

Herpes zoster (shingles)
and GSK’s adjuvanted
subunit vaccine candidate
(HZ/su)
©2017 GlaxoSmithKline. All rights reserved. GlaxoSmithKline Biologicals SA, Rixensart, Belgium
Date of Preparation: June 2017; Zinc job bag: VGBU/ZOS/0005/17
HZ/su is not registered or available in New Zealand

23*From American Academy of Pediatrics. Varicella-Zoster Virus Infections. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red Book©: 2015 Report of the Committee on Infectious
Diseases. Elk Grove Village, IL: American Academy of Pediatrics; 2015:846-860. Copyright © 2015. Reproduced with permission. HZ, herpes zoster; VZV, varicella zoster virus
HZ is caused by the reactivation of the dormant varicella
zoster virus1
1. Kimberlin DW, et al. New Engl J Med 2007;356:1338‒43; 2. Harpaz R, et al. MMWR Recomm Rep 2008;57:1‒30
Approximately 99.5% of adults ≥40 years of age show serologic evidence of VZV
infection, and one in three people develop shingles in their lifetime2
Primary infection:
varicella (chickenpox)1
© loflo6
9,
Dep
ositp
ho
tos,
Inc.
*see footnote
VZV becomes latent in
the sensory ganglia
nerves1
Thoracic
spinal
column
Chickenpox
lesion
Sensory
neurons
Zoster
lesions
Dorsal-root
ganglion
(latent virus)
Ima
ge
so
urc
e S
hu
tte
rsto
ck
Reactivation of infection:
HZ (shingles)1
Ima
ge
so
urc
e S
hu
tte
rsto
ck

24
The natural course of HZ is made of an acute phase
often followed by chronic complications
1. Harpaz R, et al. MMWR Recomm Rep 2008;57:1‒30; 2. Kawai K, et al. BMJ Open 2014;4:e004883; 3. Opstelten W, et al. Fam Pract 2002;19:471‒5; 4. Dworkin RH, et
al. J Pain 2008;9:S37‒4; 5. Dworkin RH, et al. Clin Infect Dis 2007;44:S1‒26; 6. Nagel MA and Gilden D. Curr Neurol Meurosci rep 2015:15:16; 7. Yawn BP, et al. Mayo
Clin Proc 2011;86:88‒93
Headache,
fever,
myalgia1
Localised rash,
associated
acute pain1
Prodrome Acute (2-4 weeks)1
Recurrence
rate
~5%7
HZO, herpes zoster ophthalmicus; PHN, postherpetic neuralgia
Others: stroke, bacterial superinfection, hearing loss,
palsy, scarring, nerve cell/fiber damage1,5,6
Chronic (1‒ 3 months)3 years
5‒30% of
patients2
PHN1,2,4
HZO1,2
ima
ge
so
urc
e: iS
tock P
ho
to

25
The risk of HZ increases with the decline in
immune system function1
Patients on immunosuppressant drugs,
with immunodeficient conditions or
receiving transplants
Compromised immune system
(immunocompromised)1
Older adults (≥50 years of age)
Aging immune system
(immunosenescence)1
1. Harpaz R, et al. MMWR Recomm Rep 2008;57:1‒30
Image source Shutterstock Image source Getty images

26
HZ/su vaccine compositionHZ/su: for the prevention of HZ and HZ-related complications, such as PHN, in adults ≥50 years of age
HZ/su vaccineNon live
Adjuvant systemAS01B: QS-21* and MPL - 50 µg each
AntigengE - 50 µg
Glycoprotein spikes
Lipid envelope
DNA
Nucleocapsid
Tegument
MPL QS-21 Saponin
Ad
ap
tatio
n o
f a
Sh
utt
ers
tock im
ag
e
*QS-21 adjuvant licensed from Antigenics Inc, a wholly owned subsidiary of Agenus Inc.
a Delaware USA corporation; gE, glycoprotein; MPL, 3-O-desacyl-4’-monophosphoryl
lipid A; QS-21, Quillaja saponaria Molina, fraction 21
Ima
ge
of tr
ee
by
Fra
nz
Eu
ge
n K
öh
ler,
Kö
hle
r's
Me
diz
ina
l-P
fla
nze
n
1. Lal H et al., N Eng J Med 2015, 372: 2087-96; 2. Cunnigham A et al, N Eng J Med 2016,75:1019-32

27
HZ/su pivotal phase III programme: ZOE-50 and ZOE-701,2
New England Journal of Medicine, 2015, 2016
ZOE-50 and ZOE-70 studies conducted at the same sites
Subjects ≥70 years of age were randomly assigned to ZOE-50 or ZOE-70
Study design
and objectivesZOE-501
(Zoster-006)
ZOE-702
(Zoster-022)
Study designRandomised, observer-blind, placebo-controlled, multicentre,
multinational (North America, Europe, Latin America, Asia-Pacific)
Schedule 2 doses administered 2 months apart
Primary objectivesVEHZ in subjects
≥50 years of age
VEHZ in subjects
≥70 years of age
Primary objectives
(pooled analysis)
VEPHN in individuals ≥70 years of age
VEHZ efficacy in individuals ≥70 years of age
Actual enrollment 16160 14816
1.Lal H, et al. N Engl J Med 2015;372:2087‒96; 2. Cunningham AL, et al. N Engl J Med 2016;75:1019‒32
PHN, postherpetic neuralgia; VE, vaccine efficacy

Vaccine efficacy against HZ in subjects
50 years and older
†p-value for all efficacy comparisons with placebo <0.001*Excludes subjects not receiving Dose 2 or who developed HZ within 1 month after Dose 2^Number per 1,000 person-years
Age range
(years)
HZ/su
N=7,344
Placebo
N=7,415
VE (95% CI)†HZ cases Rate of HZ^ HZ cases Rate of HZ^
Overall (≥50) 6 0.3 210 9.197.2
(93.7-99.0)
50−59 3 0.3 87 7.896.6
(89.6-99.3)
60−69 2 0.3 75 10.897.4
(90.1-99.7)
≥70 1 0.2 48 9.497.9
(87.9-100)
Secondary objectivePrimary objective
ZOE-50 mTVC*
28Lal H,Cunningham A, Godeaux O, et al. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. NEJM 2015;372:2087-96
CI, confidence interval; HZ/su, herpes zoster subunit vaccine; mTVC, modified total vaccinated cohort; VE, vaccine efficacy
Age independent
efficacy

29
High efficacy for HZ/su sustained with minimal decline
up to 4 years post initial vaccination (ZOE-70)*
Years†
HZ/su Placebo
VEHZ
(95% CI)‡
HZ cases
(n)
Rate(cases per 1000
person-years)
HZ cases
(n)
Rate(cases per 1000
person-years)
Year 1 2 (8250) 0.2 83 (8346) 10.1 97.6%(90.9, 99.8)
Year 2 7 (8039) 0.9 87 (8024) 11.1 92.0%(82.8, 96.9)
Year 3 9 (7736) 1.2 58 (7661) 7.7 84.7%(69.0, 93.4)
Year 4 7 (7426) 1.0 56 (7267) 8.2 87.9%(73.3, 95.4)
Va
cc
ine
eff
ica
cy b
y
ye
ar
po
st
va
cc
ina
tio
n
*Subjects followed-up for a mean of 3.7 years at the time of this publication†Year 1:30‒395 days after the second vaccination; Year 2: 396‒760 days after the second vaccination; Year 3: 761‒1125 days after
the second vaccination; Year 4: >1125 after the second vaccination to the last contact date. n=number of subjects within each age
group‡p<0.001 for all comparisons
CI, confidence interval; HZ/su, herpes zoster subunit vaccine; VE, vaccine efficacy
1. Cunningham AL, et al. N Engl J Med 2016;75:1019‒32

30
HZ/su greatly reduced HZ complications, such as PHN,
among all groups ≥50 years of age*1,2
PHN defined as HZ-associated pain rated as ≥3 on a 0‒10 scale, occurring or persisting for at least 90 days following the onset of
rash using Zoster Brief Pain Inventory questionnaire. Pooled data from ZOE-50 (subjects ≥50 years of age) and ZOE-70 (subjects
≥70 years of age)
*All subjects randomised in the study who received a second dose of the vaccine. Final analysis data cut-off date: July 1, 2014;
mean follow-up 3.8 years; †p<0.001 for both comparisons
CI, confidence interval; HZ/su, herpes zoster subunit vaccine ; PHN, postherpetic neuralgia; VE, vaccine efficacy
Pre-specified, pooled analyses from ZOE-50 and ZOE-70
1. Cunningham AL, et al. N Engl J Med 2016;75:1019‒32; 2. GlaxoSmithKline Data on File for the Investigational Herpes Zoster subunit vaccine Candidate - VGBU/ZOS/0005/17 –
29/JUNE/2017
Age,
years
HZ/su Placebo
VEHZ
(95% CI)†
PHN cases
(n)
Rate(cases per
1000
person-years)
PHN cases
(n)
Rate(cases per
1000
person-years)
≥50 4 (13881) 0.1 36 (8346) 1.2 91.2%(75.9, 97.7)
≥70 4 (8250) 0.1 46 (14035) 0.9 88.8%(68.7, 97.1)
• In a post-hoc pooled analysis from ZOE-50 and ZOE-70, HZ/su also reduced non-PHN
complications (HZ vasculitis, stroke, disseminated, ophthalmic, neurological and visceral disease)2
o VE in subjects ≥50 years of age: 93.7% (95% CI 59.5, 99.9)
o VE in subjects ≥70 years of age: 91.6% (95% CI 43.4, 99.8)

31
Local adverse reactions to HZ/su were transient;
(mean duration 2‒3 days)1,2
Solicited local symptoms reported during 7 days post vaccination:
any grade overall by subject
0
20
40
60
80
100
Pain Redness Swelling
HZ/su ZOE-50(n=4382)
Placebo ZOE-50(n=4377)
HZ/su ZOE-70(n=505)
Placebo ZOE-70(n=505)
ZOE-50: Overall median duration of 3 days for pain, redness and swelling3
ZOE-70: Overall median duration of 2 days for pain; 3 days for redness and swelling2
Pe
rce
nta
ge
(%
)
n= Number of subjects with at least 1 documented dose
%= Percentage of subjects reporting the symptom at least once when the intensity is maximum
1. Lal H, et al. N Engl J Med 2015;372:2087‒96; 2.Cunningham AL, et al. N Engl J Med 2016;75:1019‒32; 3. Colindres R. Safety summary of investigational vaccine: SHINGRIX
(HZ/su). ACIP February 22, 2017 [last accessed 2017 June]. Available from: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2017-02/zoster-02-gsk.pdf

32
Systemic adverse reactions to HZ/su were transient
(mean duration 1‒2 days)1,2
0
20
40
60
80
100
Fatigue Fever (≥37.5°C/≥99.5°F)
GI* Headache Myalgia Shivering
HZ/su ZOE-50(n=4375)
Placebo ZOE-50(n=4378)
HZ/su ZOE-70(n=504)
Placebo ZOE-70(n=505)
Solicited systemic symptoms reported during 7 days post vaccination:
any grade overall by subject
Pe
rce
nta
ge
(%
)
ZOE-50: Median duration of 2 days for fatigue, GI, HA and myalgia; 1 day for fever and shivering3
ZOE-70: Median duration of 2 days for fatigue, GI, HA myalgia and fever; 1 day for shivering2
*GI symptoms included nausea, vomiting, diarrhoea, and/or abdominal pain
GI, gastrointestinal; HA, headache; n= Number of subjects with at least 1 documented dose; % = Percentage of subjects reporting
the symptom at least once when the intensity is maximum
1. Lal H, et al. N Engl J Med 2015;372:2087‒96; 2.Cunningham AL, et al. N Engl J Med 2016;75:1019‒32; 3. Colindres R. Safety summary of investigational vaccine: SHINGRIX
(HZ/su). ACIP February 22, 2017 [last accessed 2017 June]. Available from: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2017-02/zoster-02-gsk.pdf

33
HZ/su provided efficacy across all age groups ≥50 years of
age with an acceptable safety and tolerability profile
1.Lal H, et al. N Engl J Med 2015;372:2087‒96; 2. Cunningham AL, et al. N Engl J Med 2016;75:1019‒32; 3. Colindres R. Safety summary of investigational vaccine: SHINGRIX (HZ/su). ACIP February 22, 2017 [last accessed 2017 June].
Available from: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2017-02/zoster-02-gsk.pdf ; 4. Study 113077 clinical study summary; 2016 [last accessed 2017, June]. Available from: www.gsk-clinicalstudyregister.com/study/113077#rs;
5. GlaxoSmithKline Data on File for the Investigational Herpes Zoster subunit vaccine Candidate - VGBU/ZOS/0005/17 – 29/JUNE/2017; ; 6. Study 110390 clinical study summary; 2016 [last accessed 2017 June]. Available from: www.gsk-
clinicalstudyregister.com/study/110390#rs
>90% efficacy shown in all age groups ‒from 50 to over 80 years of age
(pooled data from 2 pivotal phase 3 trials)1,2
There was no significant decline in efficacy during an ongoing follow-up period
(median 4.4 years),2 and immunogenicity was maintained for at least 9 years3
HZ/su eliminated almost all occurrences of PHN and non-PHN complications*2,4,5
Adverse reactions were mostly transient and of mild-to-moderate intensity, with a
median duration of 3 days2,3,4,6
– z
– z
– z
Efficacy
Safety
– z
*HZ vaculitis, disseminated disease, ophthalmic disease, neurological disease visceral disease, stroke

Q&A

Prescribing Information— Bexsero Meningococcal Group B Vaccine
(rDNA, Component, Adsorbed)
Active ingredients:
One dose (0.5 ml) contains:
Recombinant Neisseria meningitidis group B NHBA fusion protein - 50 µg;
Recombinant Neisseria meningitidis group B NadA protein - 50 µg;
Recombinant Neisseria meningitidis group B fHbp fusion protein - 50 µg;
Outer membrane vesicles (OMV) from Neisseria meningitidis group B strain NZ98/254 measured as amount of total protein
containing the PorA P1.4 - 25 µg
Indications: Bexsero is indicated for active immunization of individuals from 2 months of age and older against invasive
meningococcal disease caused by Neisseria meningitidis group B.*
Method of administration: The vaccine is given by deep intramuscular injection.
Dosage information:
From 2 to 5 months: Three doses each of 0.5 ml, with first dose given at 2 months of age, with no less than 2-month interval
between primary doses and a booster dose between 12 and 15 months. Unvaccinated infants, 6 months to 11 months: Two
doses each of 0.5 ml, with no less than 2-month interval and a booster dose in the second year of life, respecting at least a 2-
month interval between primary doses and booster dose. Unvaccinated children, 12 months to 23 months: Two doses each
of 0.5 ml, with no less than 2-month interval between the primary doses and a booster dose, respecting an interval of 12 to
23 months between primary doses and booster dose. Children, 2 years to 10 years: Two doses each of 0.5 ml, with no less
than 2-month interval between the primary doses. Adolescents (from 11 years of age) and adults: Two doses each of 0.5 ml,
with no less than 1-month interval between the primary doses. A booster dose was not established in children from 2 to 10
years old, adolescents and adults.
*Bexsero is not expected to provide protection against all circulating meningococcal group B strains.
Bexsero is a registered trademark of the GlaxoSmithKline group of companies.

Prescribing Information— Bexsero Meningococcal Group B Vaccine
(rDNA, Component, Adsorbed)
Adverse events: See the local label for details.
Infants and children (up to 10 years): Very common: Eating disorders, sleepiness, unusual crying, diarrhea, vomiting (uncommon after booster), rash (children aged
12 to 23 months, uncommon after booster), fever (≥38°C), erythema, swelling, induration and tenderness at the injection site (including severe injection site
tenderness, defined as crying when injected limb is moved), irritability; Common: Rash (children aged between 12 and 23 months); Uncommon: Seizures (including
febrile seizures), pallor (rare after booster); Rare: Kawasaki syndrome, urticaria. Adolescents (from 11 years of age) and adults: Very common: headache, nausea,
swelling, induration, erythema, and pain at the injection site (including severe injection site pain, defined as unable to perform normal daily activity), malaise, myalgia,
arthralgia.
Contraindications:
Hypersensitivity to the active substances or to any of the excipients listed in the formulation.
Interaction with other medicinal products:
The safety profile of the coadministered routine vaccines were unaffected by concomitant administration of Meningococcal group B Vaccine (rDNA, component,
adsorbed), except for an increased risk of fever, tenderness at the injection site, change in eating habits, and irritability. The coadministration of whole-cell pertussis
with Meningococcal group B vaccine (rDNA, component, adsorbed) has not been studied and therefore is not recommended. When coadministered with other
vaccine, the Meningococcal group B Vaccine (rDNA, component, adsorbed) must be applied in a distinct injection site.
Precautions and warnings:
Administration of Meningococcal group B Vaccine (rDNA, component, adsorbed) should be postponed in subjects suffering from acute severe febrile illness. The
presence of a minor infection is not a contraindication for immunization. The vaccine should under no circumstances be injected via intravascular. Appropriate medical
treatment and supervision should always be available in case of anaphylactic event following administration of the vaccine. Reactions related to anxiety including
vasovagal reactions (syncope), hyperventilation, or stress-related reactions can occur in association with vaccination as a psychogenic response to the needle
injection. The vaccine should not be administered in patients with thrombocytopenia or bleeding disorder that may contraindicate intramuscular injection, unless the
potential benefit clearly outweighs the risk of administration. As with any vaccine, Meningococcal group B Vaccine (rDNA, component, adsorbed) may not fully protect
all of those who are vaccinated. It is not expected that the vaccine provides protection against all meningococcal strains circulating in group B.
Medicinal product subject to medical prescription.
Cost: Please contact the local Key account manager from GSK for pricing information if applicable.
Agency Product Number: EMEA/H/C/002333
Marketing Authorization Holder:
Bexsero is a registered trademark of the GlaxoSmithKline group of companies.

Succinct Safety Statement— Bexsero Meningococcal Group B Vaccine
(rDNA, Component, Adsorbed)
Side effects:
Infants and children (up to 10 years): Very common: Eating disorders, sleepiness, unusual crying, diarrhea, vomiting (uncommon after booster),
rash (children aged 12 to 23 months, uncommon after booster), fever (≥38°C), erythema, swelling, induration and tenderness at the injection site
(including severe injection site tenderness, defined as crying when injected limb is moved), irritability; Common: Rash (children aged between 12 and
23 months); Uncommon: Seizures (including febrile seizures), pallor (rare after booster); Rare: Kawasaki syndrome, urticaria. Adolescents (from 11
years of age) and adults: Very common: Headache, nausea, swelling, induration, erythema, and pain at the injection site (including severe injection
site pain, defined as unable to perform normal daily activity), malaise, myalgia, arthralgia.
Interactions:
The safety profile of the coadministered routine vaccines were unaffected by concomitant administration of Meningococcal group B Vaccine (rDNA,
component, adsorbed), except for an increased risk of fever, tenderness at the injection site, change in eating habits, and irritability. The
coadministration of whole-cell pertussis with Meningococcal group B vaccine (rDNA, component, adsorbed) has not been studied and therefore is not
recommended. When coadministered with other vaccine, the Meningococcal group B Vaccine (rDNA, component, adsorbed) must be applied in a
distinct injection site.
Contraindications:
Hypersensitivity to the active substances or to any of the excipients listed in the formulation.
Precautions:
Administration of Meningococcal group B Vaccine (rDNA, component, adsorbed) should be postponed in subjects suffering from acute severe febrile
illness. The presence of a minor infection is not a contraindication for immunization. The vaccine should under no circumstances be injected via
intravascular. Appropriate medical treatment and supervision should always be available in case of anaphylactic event following administration of the
vaccine. Reactions related to anxiety including vasovagal reactions (syncope), hyperventilation, or stress-related reactions can occur in association
with vaccination as a psychogenic response to the needle injection. The vaccine should not be administered in patients with thrombocytopenia or
bleeding disorder that may contraindicate intramuscular injection, unless the potential benefit clearly outweighs the risk of administration. As with any
vaccine, Meningococcal group B Vaccine (rDNA, component, adsorbed) may not fully protect all of those who are vaccinated. It is not expected that
the vaccine provides protection against all meningococcal strains circulating in group B.
Bexsero is a registered trademark of the GlaxoSmithKline group of companies.