







Languages
Pages
Legal


04/15/23 1
Dialysis Access and the Role of the Non-Dialysis Nurse
Joe Atkins, RN,MBA,CNN,CHT
And
Cheryl Harter, RN,MSN
ObjectivesThe participant will be able to:
1. Compare and contrast the benefits, deficits and safety needs of each dialysis access type
2. List the attributes of dialysis access that facilitate cannulation/connection
3. Understand the role of non-dialysis nurses in aiding dialysis staff and nephrologists in the safety, maintenance and care of dialysis accesses.
04/15/23 2
04/15/23 3
Introduction
Goal: Help all VA Nursing Staff see the value in gaining knowledge of dialysis access, being able to see the importance of their role in dialysis access maintanence, safety and care.
04/15/23 4
Key Resources for Dialysis Access Nephrologists S. Miller-Ward Nurse Manager C. Harter, Charge Nurse Joe Atkins, Dialysis Access
Coordinator Donna Woerner, Dialysis
Educator/Researcher Joy Spears and Spencer
Howard: Master Cannulators
04/15/23 5
It Takes a Team to Create and Maintain Dialysis Accesses Patient/Patient’s Family Nephrologist (office staff) Vascular Surgeon (office
staff) Interventional Radiology Dialysis Staff Dialysis Access Coordinator You
The Role of the Non-Dialysis Nurse in creation and maintenance of Dialysis Access. Often, NDNs can help veterans
and families work through fears concerning Dialysis Access
NDNs can help reinforce Dialysis Access education
NDNs participate in maintenance, safety and care of Dialysis Access.
04/15/23 6
04/15/23 7
Types of Dialysis Access Temporary/Permanent
Hemodialysis Catheter
AV Fistula (hemodialysis)
AV Graft (hemodialysis)
Peritoneal Dialysis Catheter
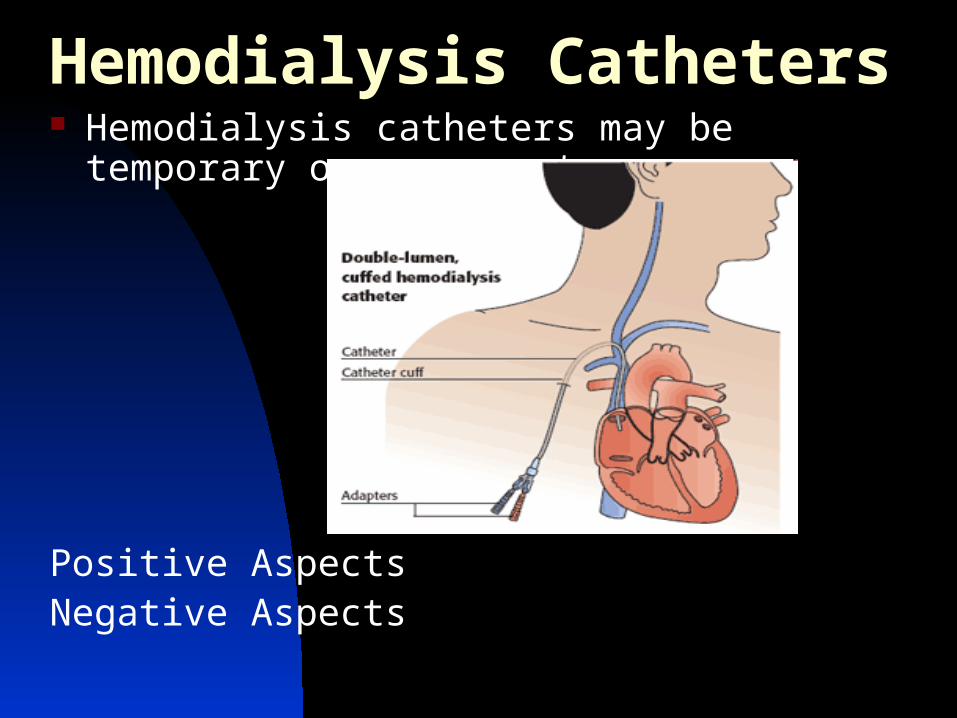
Hemodialysis Catheters Hemodialysis catheters may be temporary or
permanent.
Positive AspectsNegative Aspects
04/15/23 9
Temporary (uncuffed) Hemodialysis Catheters Bennefits
Risks
Safety
Care
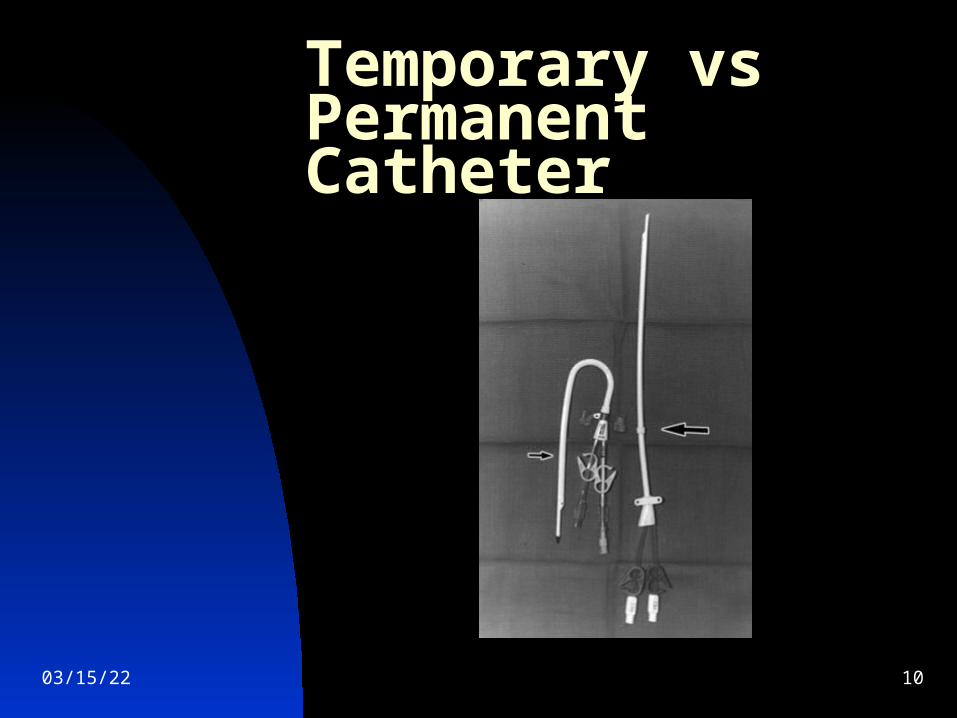
Temporary vs Permanent Catheter
04/15/23 10
04/15/23 11
Permanent (cuffed) Hemodialysis Catheters Benefits
Risks
Safety
Care
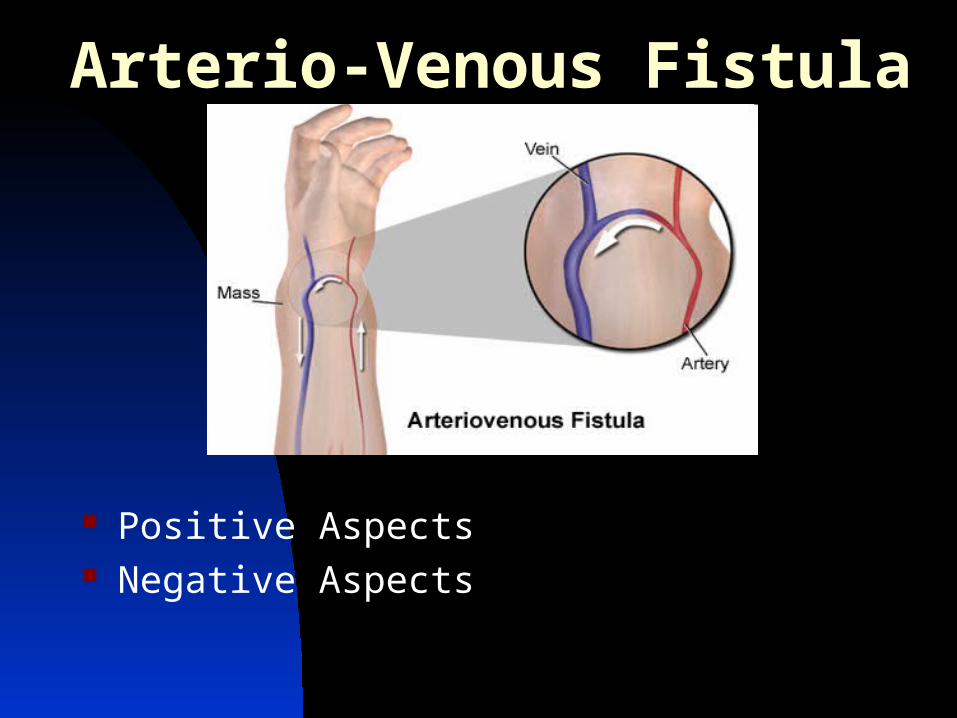
Arterio-Venous Fistula
Positive Aspects Negative Aspects
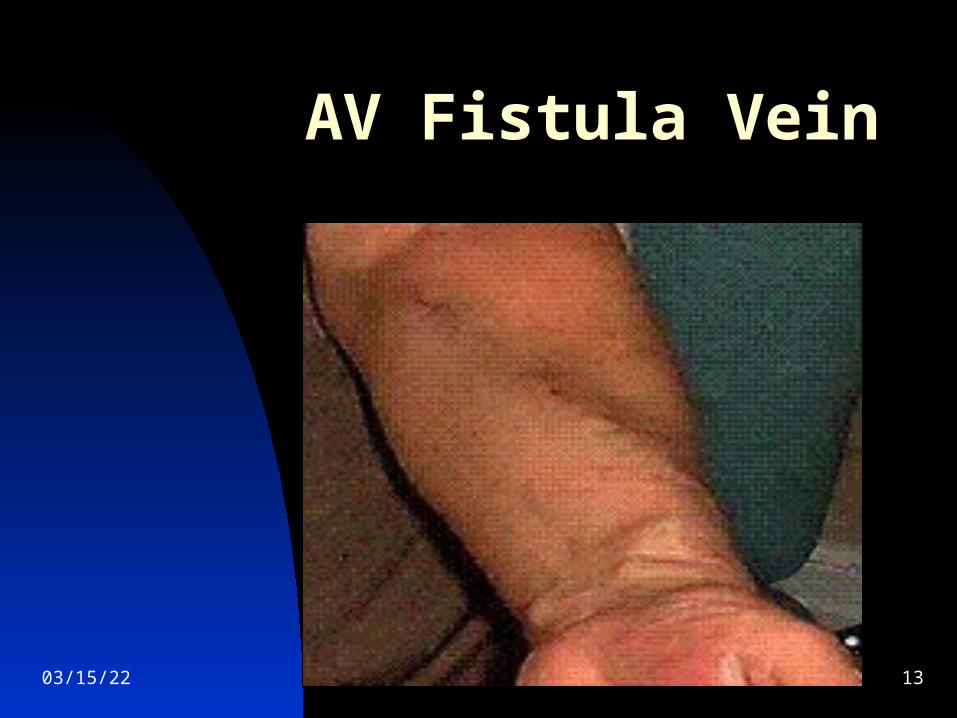
AV Fistula Vein
04/15/23 13

Sapheno-Femoral AV Fistula
04/15/23 14
Hemodialysis
04/15/23 16
Artio-Venous Fistula Benefits
Risks
Care
Safety
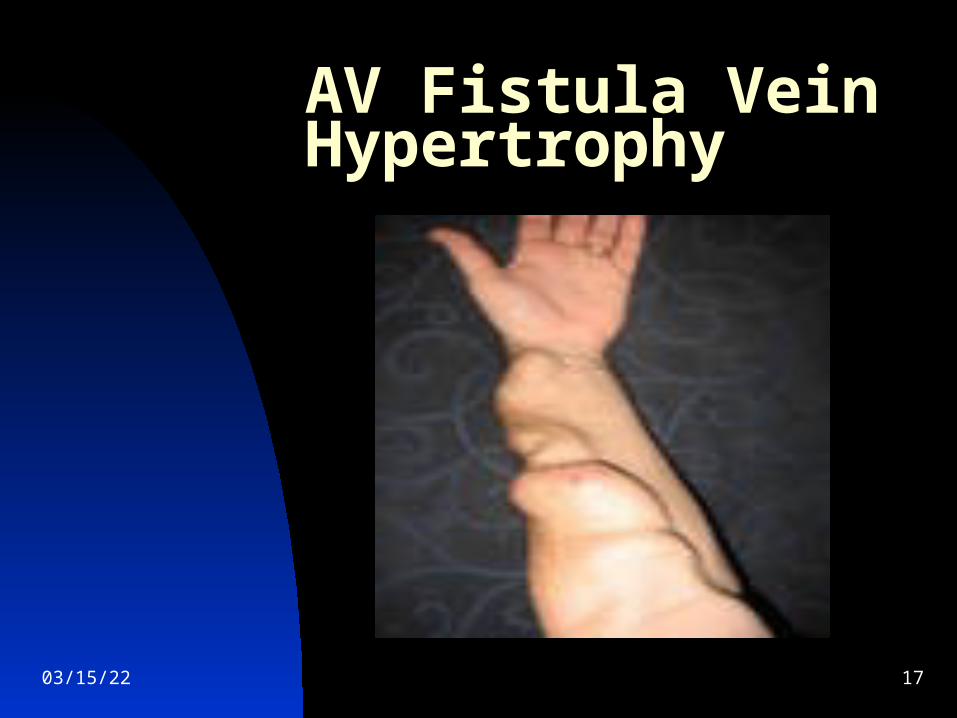
AV Fistula Vein Hypertrophy
04/15/23 17
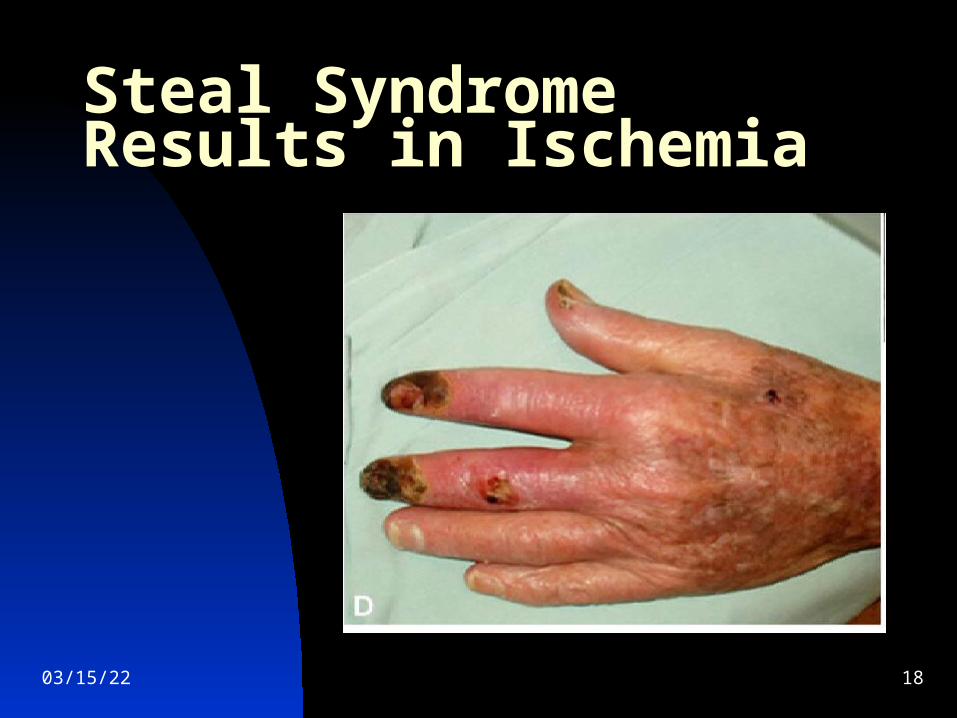
Steal Syndrome Results in Ischemia
04/15/23 18

Arterio-Venous Graft
Left: AV Graft Right: AV Fistula Positive Aspects Negative Aspects

Gortex ® Graft Material From electrical insulator to medical device
04/15/23 20
04/15/23 21
Arterio-Venous Graft
Bennefits
Risks
Care
Safety
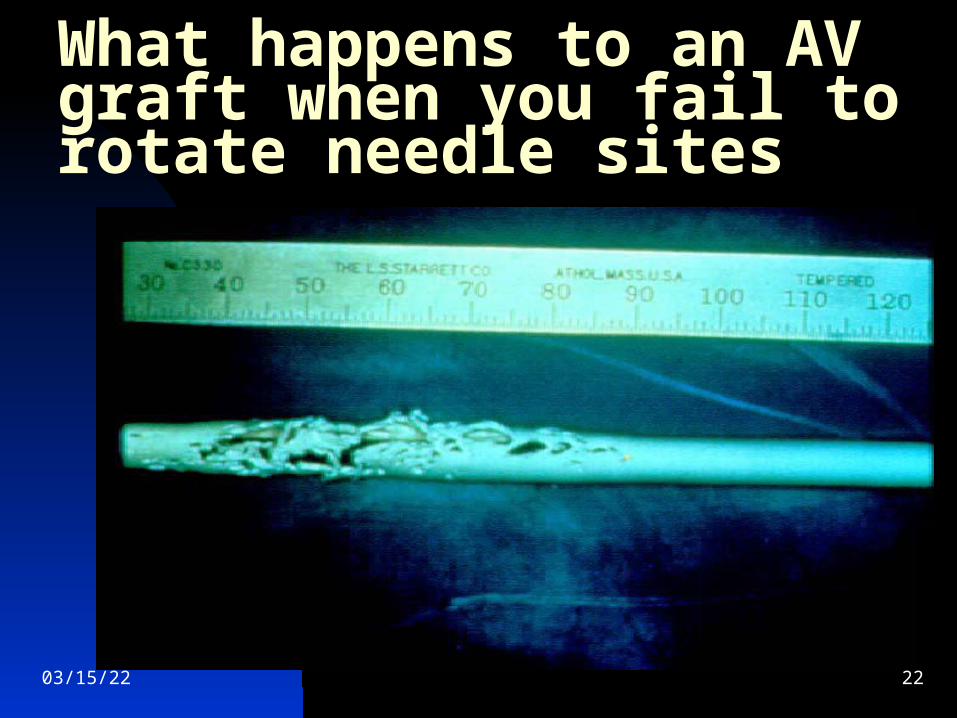
What happens to an AV graft when you fail to rotate needle sites
04/15/23 22
04/15/23 23
Early Referral to Nephrologist Screen patients at high risk:
Age >60, African-American, Native American, Diabetes, Hypertension
Refer to nephrologist if stable or rising Creatinine >1.5 female, >2.0 male
Proteinuria > 2 gm/day
04/15/23 24
Glomerular Filtration Rate Nephrologist should direct when
patient gets referred for dialysis access.
GFR is widely accepted as the best overall measure of kidney function.
GFR Calculator is on Nephron.com
04/15/23 25
When to Refer for Hemodialysis Access When GFR <30 (CKD Stage 4) and
patient chooses hemodialysis, nephrologist should refer to surgeon for AV fistula consultation.
Best for AV fistula to be created 6 months to 1 year prior to dialysis start to allow for maturation time.
Goal should be to avoid hemodialysis catheter whenever possible.
If patient is not a candidate for an AV fistula, nephrologist may want to wait until GFR lower before graft placement.
04/15/23 26
Early Education of Pre- ESRD Patients Education should start when GFR is
<30ml/min (CKD Stage 4). Modality choices need to be presented
before appropriate access referral can be made.
Consider AV Fistula creation even if patient chooses peritoneal dialysis.
Educate patients to “Save Their Veins”
04/15/23 27
AV Fistulas Need to Be Created Early!
Helpful if veteran understands the process Referral to surgeon Ultrasound (vein) mapping is necessary
before surgery can be scheduled Important patient have follow-up
post AV fistula creation to monitor development of AV fistula.
An AV fistula attempted and not successful should not be considered a failure! An AV fistula attempted is better than starting out with a catheter or graft.
04/15/23 28
Provide Realistic Expectations
Access may take maintenance angiography, angioplasty, thrombectomy, revision.
Grafts clot much more often than fistulas
AV Fistulas can be fragile and can infiltrate
AV Fistulas can clot - and can be successfully de-clotted.
04/15/23 29
Best Outcome:
Patient starts first dialysis treatment with a functioning AV fistula. Non-Dialysis Nurses are invaluable in helping ESRD patients accept and understand the need for their access.
04/15/23 30
No Access in Place for Dialysis Start - Options
Temporary or Permanent Tunneled Catheter with AV fistula placed, if possible.
If veteran desires Peritoneal Dialysis a temporary hemodialysis catheter, along with a PD Catheter will suffice until PD catheter has healed and training can be initiated.
04/15/23 31
Next Steps:
Vein mapping (as necessary) AV Graft only if veteran is not a
good candidate for AV fistula. Veterans should have a temporary
catheter for no longer than 30 days, due to risk of infection.
Although cuffed, permanent catheters are still at risk of infection.
04/15/23
Non-Dialysis Nurse Reporting Potential Access ProblemsWhat’s important to report? Exit site redness or discharge from any
catheter, whether it be for PD or hemodialysis.
AV Fistula or Graft has lost Bruit and/or Thrill.
Any sign of bleeding from any access. Risk of veteran pulling out catheter. Change in bruit or Thrill (weaker than
usual).
Major Problems/Risks with Catheters Dislodgement. Infection Air Emboli (loss of caps,
unclamping of lines) Sutures that have torn through skin
and need replaced Cracked or damaged tubing
04/15/23 33
Major Problems/Risks of AV Fistula and/or Graft Thrombosis=loss of bruit and thrill Infection=redness and/or swelling Discharge of pus from old needle
sites Venous thrombosis or stenosis
resulting in swelling of access arm Bleeding from needle sights post
dialysis Aneurysms
04/15/23 34
04/15/23 35
Non-Dialysis Nurse Care of the Hemodialysis Catheter
Check to see that catheter is secure, sutures in, caps on, clamps closed
Veterans should not shower with hemodialysis catheter, temporary or permanent (risk of infection)
Hemodialysis catheter dressings that have come loose can be replaced
Clamp the catheter if it starts to bleed what to do if the catheter falls out who to call if they have a problem with
the catheter
04/15/23 36
Care of the New Dialysis Access AV Fistula/Graft Maturation time takes 2-6 weeks for
AVG and 2-3 months for AVF Carefully assess VA before at the
beginning and end of each shift or when the patient enters or leaves your specialty area/floor.
Checking the Bruit and Thrill Avoiding anything that restricts flow of
blood (no ID or blood bands on access arm.
Educate patients on s/s of infection, clotting, and other complications
04/15/23 37
Identification of Veteran’s Dialysis Access (safety)
Wallet Cards
ID bracelet
Signs/Small Posters
Passing on information about access in shift report
04/15/23 38
Long Term Care of the Hemodialysis Access Routine monitoring and
surveillance and safety, at the facility level
Prompt referral and early intervention
Veteran’s vascular access history Veteran’s education Veteran Independence: self-
cannulation, holding own needle sites, knowledge of safety and care of access.
Peritoneal Dialysis Catheter

Peritoneal Dialysis Training
Home Peritoneal Dialysis
The Home Choice CCPD Unit
Role of the Non-Dialysis Nurse in Peritoneal Dialysis Monitoring and assessment of the PD
Catheter Supporting independent veterans as
they carry out their own PD exchanges Actually carrying out the PD exchange
for those veterans who are unable to do it, themselves
04/15/23 43
04/15/23 44
Conclusion
Non-Dialysis Nurses play a vital and beneficial role in helping veterans, nephrologists, surgeons and dialysis staff in the coordination, care and safety of dialysis accesses.
Nephro The Wonder Dog
04/15/23 45

Bibliography All photos and illustrations were sourced from the
public domain. AV Fistula First Initiative by CMS/Renal Networks “The Arteriovenous Fistula”, Konner,Nonnast-
Daniel, Ritz, JASN June 1, 2003 vol. 14 no. 6 1669-1680
“Long Term Survival of arteriovenous fistulas in home dialysis” Lynn, Buttimore, Wells, Roake and Morton, Kidney International (2004) 65, 1890-1896
“Vascular Access for Haemodialysis”, The Renal Association, Fluck and Kumwenda, 1/5/2011
04/15/23 46
Bibliography Continued “Preventing Infections in Hemodialysis Fistula and
Graft Vascular Accesses” Nephrology Nursing Journal/Sept-Oct 2012, Kim Deaver
“Prevention of hemodialysis central line-associated bloodstream infections in acutely ill individuals” Nephrology Nursing Journal/ Sept/Oct, 2012, Nancy Colobong Smith
“The culture of vascular access cannulation among nurses in a chronic hemodialysis unit” CANNT Journal, 2012 Jul-Sep;20(3):35-42, Wilson, Harwood, Oudshoom, Thompson
04/15/23 47

Bibliography Continued “Impact of multidisciplinary, early renal education
on vascular access placement” Nephrology News Issues, 2005, Fed:19(3):35-6, 41-3. Linberg, Husserl, Ross, Jackson, Scarlata, Nussbaum, Cohen, Elzein
“Peritoneal dialysis and hemodialysis: similarities and differences” Nephrology Nursing Journal/Sep-Oct, 2004 Mary M. Zorzanello
“A Patient Centered Decision Making Dialysis Access Algorithm” The Journal of Vascular Access 2007; 8: 59-68, Davidson, Gllieni, Saxena, Dolmatch
04/15/23 48
Top Related