Ueda 2016 3-glycemic targets & monitoring- adel el sayed
36
Glycemic Targets & Monitoring UEDA Diabetes Mini-Course Aswan Feb. 2016
-
Upload
ueda2015 -
Category
Health & Medicine
-
view
164 -
download
1
Transcript of Ueda 2016 3-glycemic targets & monitoring- adel el sayed
Glycemic Targets & Monitoring
UEDA Diabetes Mini-Course
Aswan Feb. 2016
Glycemic Targets & Monitoring “1”
Agenda
1. Assessment of Glycemic Control
2. HbA1c “Glycosylated Hemoglobin”
3. SMBG ‘Self Monitoring of Blood Glucose”
4. Hypoglycemia
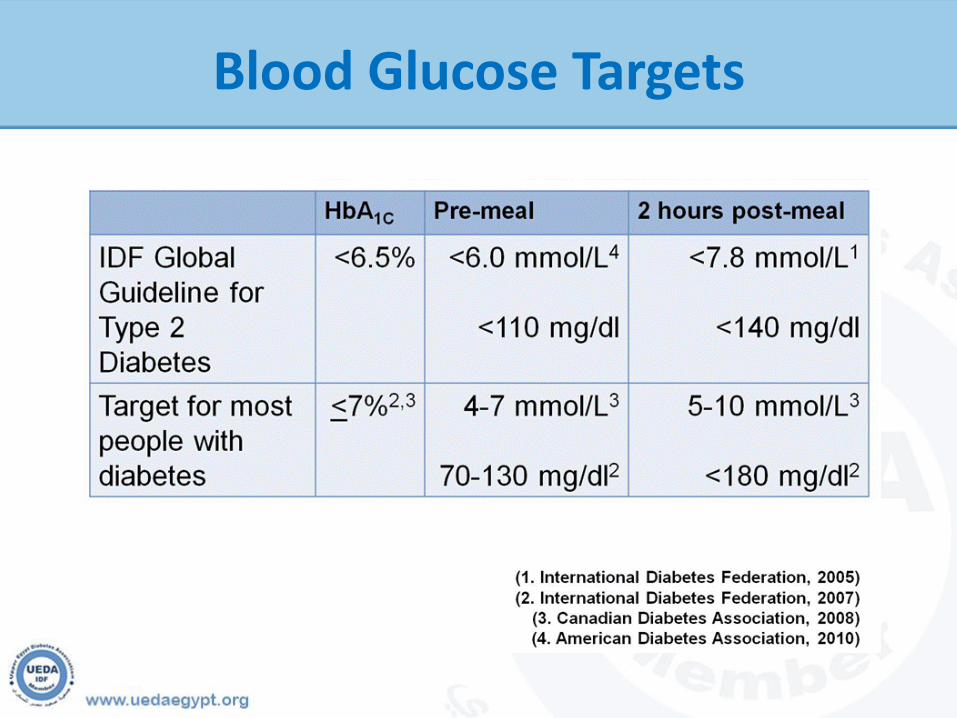
Blood Glucose Targets
TT1 Advise people with diabetes that maintaining an
HbA1c below 7.0% / minimizes the risk of
developing complications.
TT2 A lower HbA1c target may be considered if it is
easily and safely achieved.
TT3 A higher HbA1c target may be considered for
people with co-morbidities or when previous
attempts to optimize control have been associated
with unacceptable hypoglycemia.
GLUCOSE CONTROL LEVELS
TT4 An individual’s HbA1c target should be regularly
reviewed taking into account benefits, safety and
tolerability.
TT5 Treatment should be reviewed and modified if
HbA1c level is above the agreed target on two
consecutive occasions.
TT6 Advise those in whom target HbA1c levels cannot
be reached that any improvement is beneficial.
GLUCOSE CONTROL LEVELS
HBA1c
UEDA Diabetes Mini-Course
Aswan Feb. 2016
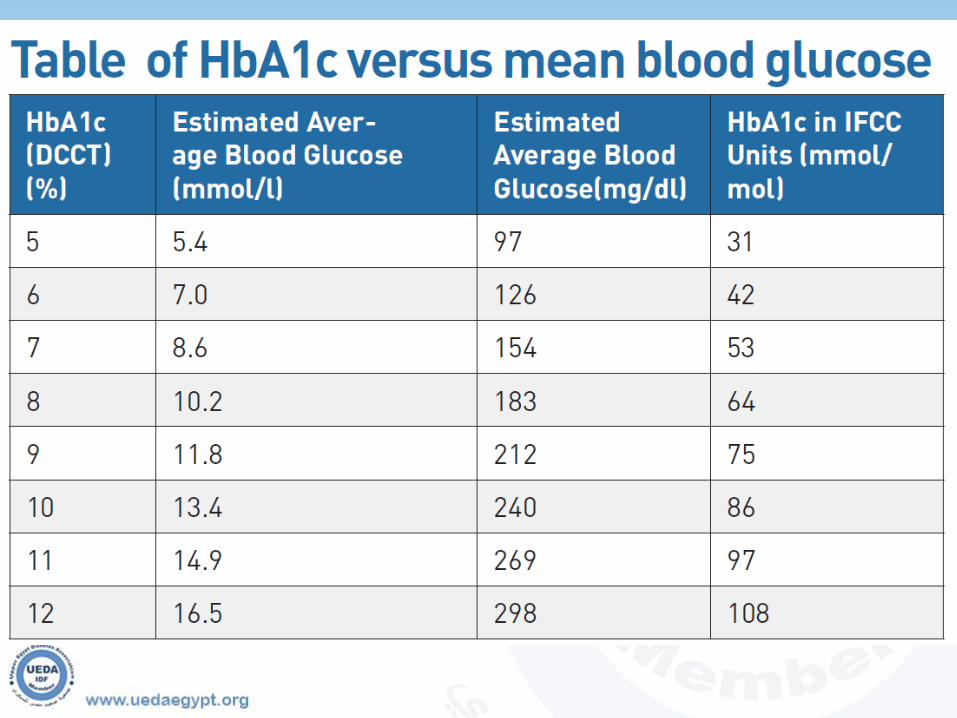
HbA1c
HbA1c (glycated haemoglobin) provides information about
average blood glucose levels over the last 2-3 months.
This test measures the amount of glucose that attaches to
haemoglobin this depends on how much glucose is in the
bloodstream.
Ideally HbA1c is measured four times per year. If resources are
limited, less frequent measurements are still helpful.
Factors Supporting Use of HbA1C forScreening and Diagnosis
A1c testing does not require overnight fast (Increase rate
of screening during non-fasting hours)
HbA1c reflects long-term glycemic burden (Relatively less
affected by acute (e.g., stress or illness related perturbations in
glucose levels)
Accepted and current guide in management of diabetes
(A1c laboratory methods now well standardized and reliable)
Suadek CD. J Clin Endocrinol Metab 93: 2447–2453, 2008International Expert Committee. Diabetes Care 32 (7):1327-1334, 2009
The Disadvantages Of Hba1c Testing
Higher cost.
Effects of abnormal red cell lifespan.
Possible age and race related disparities.
The various assay interferences.
Rare instances of rapidly evolving type 1 diabetes may take some time to result in a diagnostic HbA1c level and result in a delay in diagnosis.
Limitations in HbA1c Measures
A- Conditions that will shorten red cell lifespan and can result infalsely low HbA1c: Anemia. Hemolysis. B12/folate deficiency. Various hemoglobinopathies.
B- Conditions that will prolong red cell lifespan and can result in false high HbA1c Post splenectomy state. Polycythemia. Some instances of iron deficiency.
Recommendations 2015
Perform the A1C test at least two times a year
in patients who are meeting treatment goals
(and who have stable glycemic control).
Perform the A1C test every three months in
patients whose therapy has changed or who are
not meeting glycemic goals.
Self Monitoring of Blood Glucose(SMBG)
SMGB should be carried out 3 or more times daily for patients using multiple insulin injection or insulin pump therapy
For patients using MNT (Medical Nutritional Therapy) or oral therapy SMGB may be used 2 to 3 times per week to access fasting and postprandial blood glucose.
Continuous glucose monitoring may be used as a tool to lower A1C in patients above 25 years with type 1 diabetes. It may be useful in those with hypoglycemia unawareness or frequent hypoglycemic episodes.
UEDA Diabetes Mini-Course
Aswan Feb. 2016
Self Monitoring of Blood Glucose(SMBG)
SM1 Self-monitoring of blood glucose (SMBG) should only be
made available to people with diabetes when they have the
knowledge, skills and willingness to use the information
obtained through testing to actively adjust treatment,
enhance understanding of diabetes and assess the
effectiveness of the management plan on glycaemic control.
SM2 The purpose(s) of performing SMBG and using SMBG data
should be agreed between the person with diabetes and the
health-care provider.
SM3 SMBG on an ongoing basis should be available to those
people with diabetes using insulin.
Self Monitoring of Blood Glucose(SMBG)

SM4 SMBG should be considered for people using oral
glucose lowering medications as an optional component
of self-management, and in association with HbA1c
testing:
To provide information on, and help avoid hypoglycemia.
To assess changes in blood glucose control due to
medications and lifestyle changes.
To monitor the effects of foods on postprandial
glycaemia.
To monitor changes in blood glucose levels during
intercurrent illness.
Self Monitoring of Blood Glucose(SMBG)
SM5 Regular use of SMBG should not be considered part
of routine care where diabetes is well controlled by
nutrition therapy or oral medications alone.
SM6 SMBG protocols (intensity and frequency) should be
individualized to address each individual’s specific
educational / behavioral / clinical requirements,
and provider requirements for data on glycemic
patterns to monitor therapeutic decision making.
SM7 Structured assessment of self-monitoring skills, the
quality and use made of the results obtained, and of
the equipment used, should be made annually.
Self Monitoring of Blood Glucose(SMBG)
Ketone Testing
Ketone testing with either urine strips, or blood when available, should be performed:
During illness with fever and/or vomiting.
When blood glucose is above 15 mmol/l (270 mg/dl) in an unwell Diabetic or when persistent blood glucose levels above 15 mmol/l (270 mg/dl) are present.
When there is persistent polyuria with elevated blood glucose, especially if abdominal pain or rapid breathing are present.
Hypoglycemia
UEDA Diabetes Mini-Course
Aswan Feb. 2016
Hypoglycemia
Definition Of Hypoglycaemia
The development of autonomic or neuroglycopenic symptoms.
A low plasma glucose (<4.0 mmol/L or 72 mg/dl)
Symptoms responding to the administration of carbohydrate
(Cryer, Davis, Shamoon, 2003)
Risk of hypoglycaemia (1 of 2)
Only those taking glucose-lowering medicines or insulin are at risk
Risk increases with: Not enough carbohydrate consumption Late or missed meal Fasting or malnourishment Too much insulin or insulin secretagogues Prolonged or unplanned activity Risk increases with: Recent severe hypoglycaemia Over-correction with insulin Pregnancy
Risk of hypoglycaemia (2 of 2)
Liver disease or kidney failure
Gastroparesis
Endocrine disease
Hypoglycaemia unawareness
Failure to notice symptoms due to distractions or sleeping
Intensive glucose control
Long duration of diabetes
Other medications/drugs including alcohol
Increased Risk Of Hypoglycaemia
Diabetes Control and Complications Trial (DCCT) Intensively treated group three times the number of severe hypoglycaemic episodes
United Kingdom Prospective Diabetes Study (UKPDS) 30% of intensively treated experienced hypoglycaemia; events rare in the conventional group
(Diabetes Control and Complications Trial, 1993)
(UK Prospective Diabetes Study, 1998)
Hypoglycemia In Older People
Risk of injury from falls May be missed or mistaken for dementia Malnutrition may increase risk of
hypoglycaemia Avoid long-acting sulphonylureas in older
people Repaglinide, acarbose and DPP-IV inhibitors
may be safer options
(Johnson, Brosseau, Sobule, Kolberg, 2008)
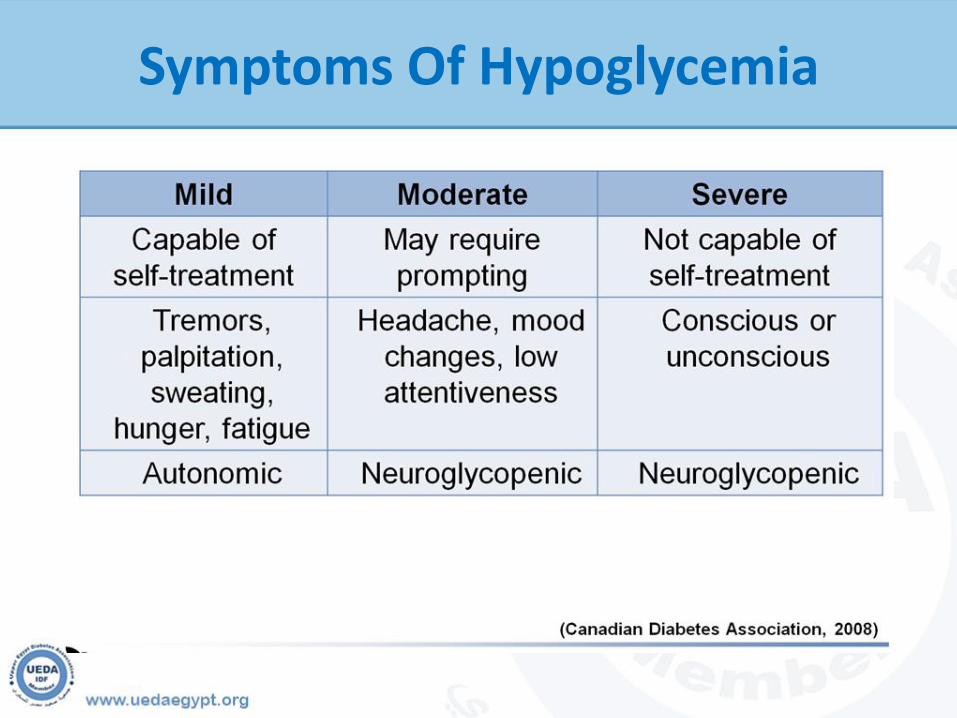
Symptoms Of Hypoglycemia
Mild-Moderate
Fear
Anxiety
Affects self-care
Social stigma
Prejudice
Severe
Injury
Seizures
Transient paralysis
Cognitive impairment
Death
Possible Consequences Of Hypoglycaemia
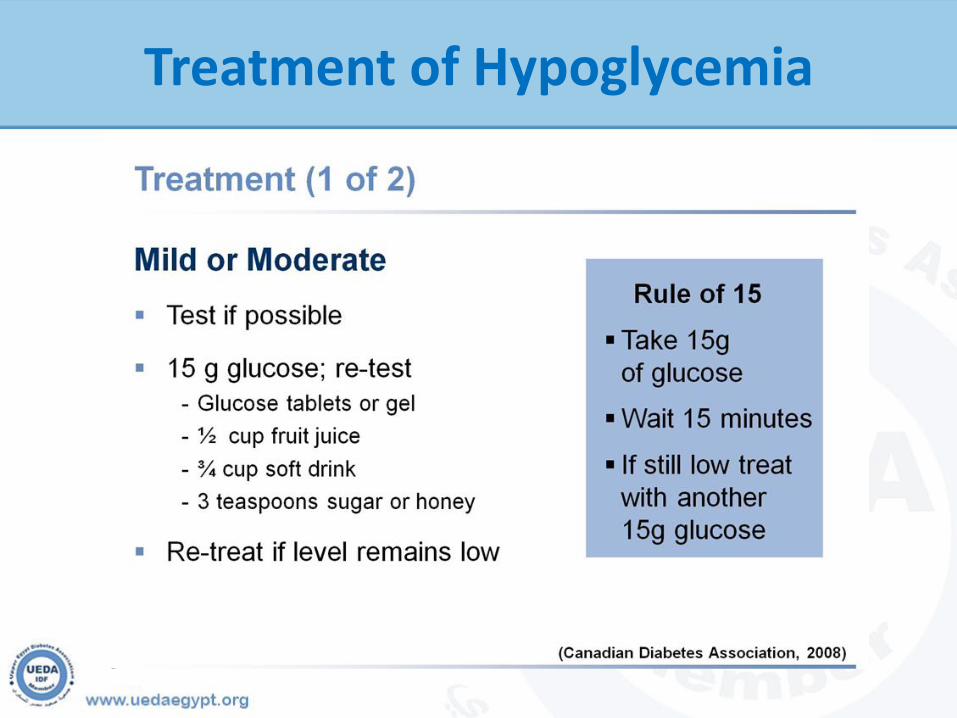
Treatment of Hypoglycemia
Treatment (2 of 2)
Severe
20 g glucose
Glucagon
Intravenous dextrose
Manage seizure - place person on their side if not too agitated
Treatment of Hypoglycemia
Follow-up management
Meal or snack (15-20 g carbohydrate + a protein source)
Next dose taken as usual
Consider reducing insulin
Assess cause
Prevent recurrence
Avoid BG levels < 4 mmol/L (72 mg/dl)
Determine the cause
Other management strategies
Self-management education and supportLong acting analogues instead of NPHRapid acting analogues instead of
regular/soluble insulinInsulin pumpAbdomen provides most consistent
absorption of insulin
(Garg, Gottlieb, Hisamoti, D’Souza, Walker, Izuora, 2004) (Garg, Paul, Karsten, Menditto, Gottlieb, 2004) (Rosenstock, Dailey, Massi-Benedetti, Fritsche, Lin, Salzman, 2005)
Rebound Hyperglycaemia
After nocturnal hypoglycaemia
Hypoglycaemia between 2 - 4 am
Elevated blood glucose in the morning - after 6 am
Treatment options
Decrease evening intermediate-acting insulin
Move intermediate insulin to bedtime if previously taken at evening meal
Change intermediate to long-acting insulin analogue
Increase bedtime snack(Rosenstock et al., 2005)
•
Developing Unawareness
Glucagon response often lost with type 1 diabetes
Epinephrine response may be blunted and delayed
Adrenergic symptoms blunted
People with diabetes should learn to recognize neuroglycopenic symptoms
Managing Hypoglycaemic Unawareness
Unawareness is sometimes reversible
Encourage hypoglycaemia-free state
Medical alert identification
Monitor blood glucose before certain activities, such as sports, driving
(Thomas, Aldibbiat, Griffin, Cox, Leech, Shaw, 2007)
(Amiel, 2009)
(Leiter, Yale, Chiasson, Harris, Kleinstiver, Sauriol, 2005)
(Cox, Gonder-Frederick, Polonsky, Schlundt, Kovatchev, 2001)

Summary
Incidence reduced through education, self-monitoring and self-care
Frightening for person with diabetes and family
Often hypoglycaemia can be prevented Must be addressed at every visit to
healthcare professional Treatment must be revised if recurrent
(Canadian Diabetes Association, 2008)
Lastly we hope that course will achieve
its goals and help you all in getting the
best of the forthcoming conference
UEDA Board
UEDA Diabetes Mini-Course
Aswan Feb. 2016