The World Bank FOR OFFICIAL USE...
109
Document of The World Bank FOR OFFICIAL USE ONLY Report No: 52142-MX PROJECT APPRAISAL DOCUMENT ON A PROPOSED LOAN IN THE AMOUNT OF US$1,250 MILLION TO THE UNITED MEXICAN STATES FOR A SOCIAL PROTECTION SYSTEM IN HEALTH PROJECT February 23, 2010 Human Development Sector Management Unit Mexico and Colombia Country Management Unit Latin America and the Caribbean Region This document has a restricted distribution and may be used by recipients only in the performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
Transcript of The World Bank FOR OFFICIAL USE...
Document of
The World Bank
FOR OFFICIAL USE ONLY
Report No: 52142-MX
PROJECT APPRAISAL DOCUMENT
ON A
PROPOSED LOAN
IN THE AMOUNT OF US$1,250 MILLION
TO THE
UNITED MEXICAN STATES
FOR A
SOCIAL PROTECTION SYSTEM IN HEALTH PROJECT
February 23, 2010
Human Development Sector Management Unit
Mexico and Colombia Country Management Unit
Latin America and the Caribbean Region
This document has a restricted distribution and may be used by recipients only in the
performance of their official duties. Its contents may not otherwise be disclosed without World
Bank authorization.
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

CURRENCY EQUIVALENTS
(Exchange Rate Effective February 23, 2010)
Currency Unit = Mexican Peso (MXN)
12.8148 MXN = US$1
US$0.0780 = 1 MXN
FISCAL YEAR
January 1 – December 31
ABBREVIATIONS AND ACRONYMS
AIDS Acquired Immune Deficiency Syndrome
ASE State Solidary Contribution (Aportación Solidaria Estatal)
ASF Federal Solidary Contribution (Aportación Solidaria Federal)
BP Bank Procedure
CDI Commission for Indigenous Development (Comisión de Desarrollo de
los Pueblos Indígena)
CLC Payment Orders (Cuenta por Liquidar Certificada)
CNPSS or
Commission
The National Commission of Social Protection in Health (Comisión
Nacional de Protección Social en Salud)
COI Uniform Accounting System (Contabilidad Integral)
CONAPO National Population Council (Consejo Nacional de Población)
CONEVAL National Council for the Evaluation of Social Development Policy
(Consejo Nacional de Evaluación de la Política de Desarrollo Social)
COPLAMAR General Coordination of the National Plan for Deprived Zones and
Marginalized Groups (Coordinación General del Plan Nacional de
Zonas Deprimidas y Grupos Marginados)
CPS Country Partnership Strategy
CS Social Contribution (Cuota Social)
DGAF General Directorate of Administration and Finance (Dirección General
de Administración y Finanzas)
DGAO General Directorate of Affiliation and Operation (Dirección General de
Afiliación y Operación)
DGCEF General Directorate of Coordination with Federal Entities (Dirección
General de Coordinación con Entidades Federativas)
DGF General Directorate of Finance (Dirección General de Finanzas)
DGGSS General Directorate of Health Service Management (Dirección General
de Gestión de Servicios de Salud)
ENIGH Survey on Household Income and Expenditures (Encuesta de Ingresos y
Gastos de los Hogares)
ENSANUT National Health and Nutrition Survey (Encuesta Nacional de Salud y
Nutrición)
FA Financial Agent
FBS Fixed Budget Selection
FM Financial Management
FPGC Fund for the Protection Against Catastrophic Expenditures (Fondo de
Protección contra Gastos Catastróficos)
FPP Budgetary Contingency Fund (Fondo de Previsión Presupuestal)
FY Fiscal Year
GDP Gross Domestic Product
GET Global Expert Team
GHL General Health Law
GoM Government of Mexico
HDI Human Development Index
HDR Human Development Report
HIV Human Immunodeficiency Virus
IBRD International Bank for Reconstruction and Development
IDA International Development Association
IFR Interim Financial Reports
IMSS Mexican Social Insurance Institute (Instituto Mexicano del Seguro
Social)
INEGI National Institute for Statistics, Geography and Informatics (Instituto
Nacional de Estadística Geografía e Informática)
IP Implementation Process
IPP Indigenous Peoples Plan
ISDS Information Safeguards Data Sheet
ISSSTE National Institute for the Social Security of Government Workers
(Instituto de Seguridad y Servicios Sociales de los Trabajadores del
Estado)
LAC Latin America and the Caribbean Region
LCS Least Cost Selection
MDGs Millennium Development Goals
NAFIN National Finance Agent (Nacional Financiera)
NDP National Development Plan
OECD Organization for Economic Co-operation and Development
OIC Internal Control Unit (Organo Interno de Control)
OM Operational Manual
OP Operational Policy
PAC Program for Coverage Extension (Programa de Ampliación de
Cobertura de salud)
PASSPA Health Service Assistance Program for the Open Population (Programa
de Apoyo a los Servicios de Salud para Población Abierta)
PCU Project Coordination Unit
PDO Project Development Objective
PEF Federal Expenditure Budget (Presupuesto de Egresos de la Federación)
PIC Public Information Center
PID Project Information Document
PND National Development Plan (Plan Nacional de Desarrollo)
PPP Purchasing Power Parity
PROSESA Programa Sectorial de Salud

QBS Quality Based Selection
QCBS Quality and Cost Based Selection Method
REPSS Regímenes Estatales de Protección Social en Salud
RFP Request for Proposals
RVP Regional Vice-President
SAI The Supreme Audit Institution
SEED Epidemiological and Statistical System for the recording of Deaths
(Sistema Epidemiológico y Estadístico de Defunciones)
SEPA System for the Execution of Procurement Plans (Sistema de Ejecución de
Planes de Adquisiciones)
SFB Selection under a Fixed Budget
SFP Public Administration Secretariat (Secretaría de la Función Pública)
SHCP Federal Secretariat of Finance (Secretaría de Hacienda y Crédito
Público)
SINAIS National Health Information System (Sistema Nacional de Información
en Salud)
SOE Statements of Expenditures
SPSS Social Protection System in Health (Sistema de Protección Social en
Salud)
TA Technical Assistance
TESOFE Federal Treasury (Tesorería de la Federación)
UNDP United Nations Development Program
WBG The World Bank Group
WDI World Development Indicators
WHO World Health Organization
Vice President: Pamela Cox
Country Director: Gloria Grandolini
Sector Director: Evangeline Javier
Sector Manager: Keith Hansen
Task Team Leader: Christoph Kurowski

MEXICO
Social Protection System in Health
CONTENTS
Page
I. STRATEGIC CONTEXT AND RATIONALE ................................................................. 1
A. Country and sector issues.................................................................................................... 1
B. Rationale for Bank involvement ....................................................................................... 10
C. Higher level objectives to which the project contributes .................................................. 13
II. PROJECT DESCRIPTION ............................................................................................... 13
A. Lending instrument ........................................................................................................... 13
B. Project development objective .......................................................................................... 13
C. Project Key Performance Indicators ................................................................................. 13
D. Project components ........................................................................................................... 14
E. Lessons learned and reflected in the project design .......................................................... 17
F. Alternatives considered and reasons for rejection ............................................................ 18
III. IMPLEMENTATION .................................................................................................... 19
A. Institutional and implementation arrangements ................................................................ 19
B. Monitoring and evaluation of outcomes/results ................................................................ 20
C. Sustainability..................................................................................................................... 20
D. Critical risks and possible controversial aspects ............................................................... 21
E. Loan conditions and covenants ......................................................................................... 23
IV. APPRAISAL SUMMARY ............................................................................................. 23
A. Economic and financial analyses ...................................................................................... 23
B. Technical ........................................................................................................................... 24
C. Fiduciary ........................................................................................................................... 25
D. Social................................................................................................................................. 26
E. Environment ...................................................................................................................... 27
F. Safeguard policies ............................................................................................................. 28
G. Policy Exceptions and Readiness...................................................................................... 29
Annex 1: Country and Sector or Program Background ......................................................... 30
Annex 2: Major Related Projects Financed by the Bank and/or other Agencies ................. 43
Annex 3: Results Framework and Monitoring ........................................................................ 45
Annex 4: Detailed Project Description ...................................................................................... 52
Annex 5: Project Costs ............................................................................................................... 59
Annex 6: Implementation Arrangements ................................................................................. 60
Annex 7: Financial Management and Disbursement Arrangements ..................................... 66
Annex 8: Procurement Arrangements ...................................................................................... 76
Annex 9: Economic and Financial Analysis ............................................................................. 80
Annex 10: Safeguard Policy Issues ............................................................................................ 82
Annex 11: Project Preparation and Supervision ..................................................................... 89
Annex 12: Documents in the Project File ................................................................................. 90
Annex 13: Statement of Loans and Credits .............................................................................. 91
Annex 14: Country at a Glance ................................................................................................. 93
Annex 15: Map 33447R .............................................................................................................. 96
Annex 16: References ................................................................................................................. 97

MEXICO
SUPPORT TO THE SOCIAL PROTECTION SYSTEM IN HEALTH
PROJECT APPRAISAL DOCUMENT
LATIN AMERICA AND CARIBBEAN
LCSHH
Date: February, 23, 2010 Team Leader: Christoph Kurowski
Country Director: Gloria M. Grandolini
Sector Manager/Director: Keith E. Hansen
Sectors: Health (100%)
Themes: Health system performance (80%);
Indigenous peoples (10%); Social safety nets
(10%)
Project ID: P116226 Environmental category: C - Not Required
Lending Instrument: Specific Investment Loan Joint IFC:
Joint Level:
Project Financing Data
[X] Loan [ ] Credit [ ] Grant [ ] Guarantee [ ] Other:
For Loans/Credits/Others:
Total Bank financing (US$m.): 1,250.00
Proposed terms: IBRD Flexible loan, with a variable-spread, all conversion options, a bullet
repayment on January 15, 2028 and interest payments made each January 15 and July 15.
Financing Plan (US$m)
Source Local Foreign Total
Borrower 25,607.00 4.00 25,611.00
International Bank for Reconstruction and
Development
1,243.00 7.00 1,250.00
Total: 26,850.00 11.00 26,861.00
Borrower:
United Mexican States
Mexico
Responsible Agency: Secretariat of Health
Lieja No. 7, Piso 1
Colonia Juarez
DF
Mexico
06696
Tel: (52-55) 5553-0758
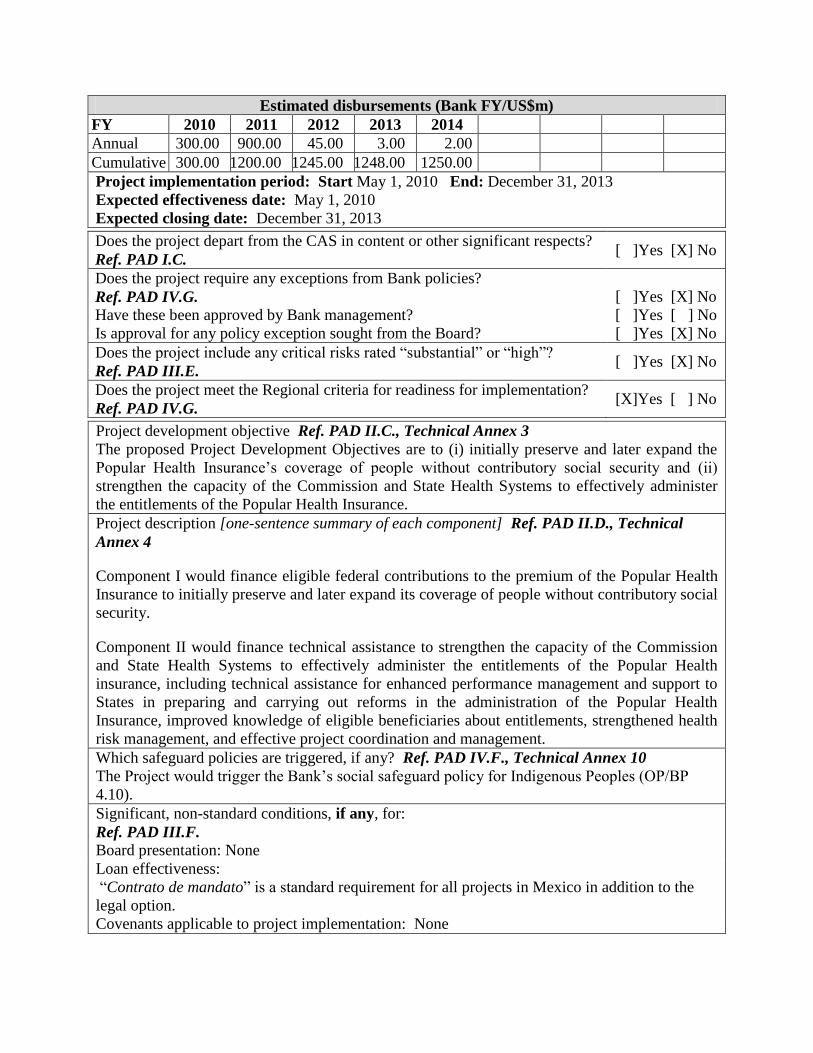
Estimated disbursements (Bank FY/US$m)
FY 2010 2011 2012 2013 2014
Annual 300.00 900.00 45.00 3.00 2.00
Cumulative 300.00 1200.00 1245.00 1248.00 1250.00
Project implementation period: Start May 1, 2010 End: December 31, 2013
Expected effectiveness date: May 1, 2010
Expected closing date: December 31, 2013
Does the project depart from the CAS in content or other significant respects?
Ref. PAD I.C. [ ]Yes [X] No
Does the project require any exceptions from Bank policies?
Ref. PAD IV.G. Have these been approved by Bank management?
[ ]Yes [X] No
[ ]Yes [ ] No
Is approval for any policy exception sought from the Board? [ ]Yes [X] No
Does the project include any critical risks rated ―substantial‖ or ―high‖?
Ref. PAD III.E. [ ]Yes [X] No
Does the project meet the Regional criteria for readiness for implementation?
Ref. PAD IV.G. [X]Yes [ ] No
Project development objective Ref. PAD II.C., Technical Annex 3
The proposed Project Development Objectives are to (i) initially preserve and later expand the
Popular Health Insurance‘s coverage of people without contributory social security and (ii)
strengthen the capacity of the Commission and State Health Systems to effectively administer
the entitlements of the Popular Health Insurance.
Project description [one-sentence summary of each component] Ref. PAD II.D., Technical
Annex 4
Component I would finance eligible federal contributions to the premium of the Popular Health
Insurance to initially preserve and later expand its coverage of people without contributory social
security.
Component II would finance technical assistance to strengthen the capacity of the Commission
and State Health Systems to effectively administer the entitlements of the Popular Health
insurance, including technical assistance for enhanced performance management and support to
States in preparing and carrying out reforms in the administration of the Popular Health
Insurance, improved knowledge of eligible beneficiaries about entitlements, strengthened health
risk management, and effective project coordination and management.
Which safeguard policies are triggered, if any? Ref. PAD IV.F., Technical Annex 10
The Project would trigger the Bank‘s social safeguard policy for Indigenous Peoples (OP/BP
4.10).
Significant, non-standard conditions, if any, for:
Ref. PAD III.F.
Board presentation: None
Loan effectiveness:
―Contrato de mandato‖ is a standard requirement for all projects in Mexico in addition to the
legal option.
Covenants applicable to project implementation: None
1
I. STRATEGIC CONTEXT AND RATIONALE
A. Country and sector issues
Trends in Socioeconomic Development
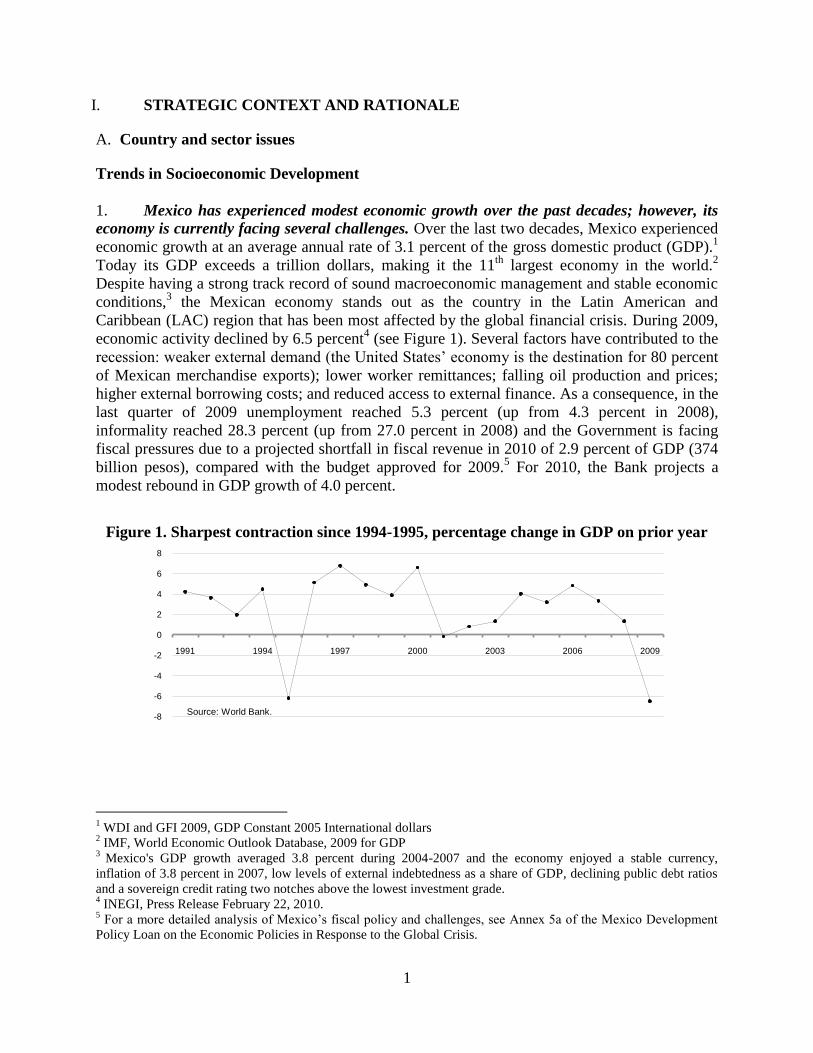
1. Mexico has experienced modest economic growth over the past decades; however, its
economy is currently facing several challenges. Over the last two decades, Mexico experienced
economic growth at an average annual rate of 3.1 percent of the gross domestic product (GDP).1
Today its GDP exceeds a trillion dollars, making it the 11th
largest economy in the world.2
Despite having a strong track record of sound macroeconomic management and stable economic
conditions,3 the Mexican economy stands out as the country in the Latin American and
Caribbean (LAC) region that has been most affected by the global financial crisis. During 2009,
economic activity declined by 6.5 percent4 (see Figure 1). Several factors have contributed to the
recession: weaker external demand (the United States‘ economy is the destination for 80 percent
of Mexican merchandise exports); lower worker remittances; falling oil production and prices;
higher external borrowing costs; and reduced access to external finance. As a consequence, in the
last quarter of 2009 unemployment reached 5.3 percent (up from 4.3 percent in 2008),
informality reached 28.3 percent (up from 27.0 percent in 2008) and the Government is facing
fiscal pressures due to a projected shortfall in fiscal revenue in 2010 of 2.9 percent of GDP (374
billion pesos), compared with the budget approved for 2009.5 For 2010, the Bank projects a
modest rebound in GDP growth of 4.0 percent.
1 WDI and GFI 2009, GDP Constant 2005 International dollars
2 IMF, World Economic Outlook Database, 2009 for GDP
3 Mexico's GDP growth averaged 3.8 percent during 2004-2007 and the economy enjoyed a stable currency,
inflation of 3.8 percent in 2007, low levels of external indebtedness as a share of GDP, declining public debt ratios
and a sovereign credit rating two notches above the lowest investment grade. 4 INEGI, Press Release February 22, 2010.
5 For a more detailed analysis of Mexico‘s fiscal policy and challenges, see Annex 5a of the Mexico Development
Policy Loan on the Economic Policies in Response to the Global Crisis.
-8
-6
-4
-2
0
2
4
6
8
1991 1994 1997 2000 2003 2006 2009
Source: World Bank.
Figure 1. Sharpest contraction since 1994-1995, percentage change in GDP on prior year

2
Table 1. HDI Rankings
2. While Mexico’s level of human
development has increased in parallel with its
economic growth, it still lags behind other LAC
countries and the OECD average, and HDI
values vary significantly across States6. Mexico
increased its Human Development Index (HDI),
which aggregates measures of life expectancy,
adult literacy and school enrollment, and income per capita, from 0.768 in 1990 to 0.854 today
(on a scale of 0 to 1).7 According to HDI rankings (see Table 1), this means Mexico has
increased its level of human development from medium to high. Despite its high level of GDP
per capita (PPP) and improvements in the HDI, however, Mexico ranks only 53rd
in terms of
human development globally and lower than other Latin American countries such as Uruguay
(0.865), Argentina (0.866), and Chile (0.878). It also remains well below the OECD average
level of human development (0.928) and ranks second to last among OECD countries, just above
Turkey. Moreover, there are considerable inequalities in human development among the States in
Mexico. While some States have nearly reached the very high level (for example the Federal
District at 0.8837), others are only at the medium level (for example Chiapas at 0.7185).8
Health Sector Issues
3. Since the 1990s, Mexico has significantly improved its health outcomes and is on track
to achieve the health-related Millennium Development Goals (MDGs), but with increasing
rates of non-communicable diseases, the country is now facing a “dual burden of disease.” As
part of the MDGs, in 2001, countries such as Mexico agreed to improve specific health outcomes
in their population by reducing under-5 child mortality and infant mortality (MDG 4) by two-
thirds and reducing maternal mortality (MDG 5) by three-quarters between 1990 and 2015.
Today, Mexico is one of the few countries in the world that is on track to achieve these Goals.
Between 1990 and 2007, it had reduced under-5 child mortality by over 55 percent and infant
mortality by 62 percent and had nearly halved its maternal mortality rate.9 Likewise, life
expectancy at birth has increased from 71 years to 75 years.10
These continuous achievements
have resulted in what is commonly referred to as a ―dual burden of disease.‖ At the same time as
the extreme poor and other marginalized groups continue to be plagued by high maternal and
child mortality —mainly from infectious diseases and perinatal conditions— an aging population
and unhealthy lifestyles produce a rapidly growing population segment that is increasingly
suffering from non-communicable diseases, such as diabetes and cancer. Today 16 percent of
Mexico‘s burden of disease is due to communicable diseases while 72 percent is due to non-
communicable diseases.11
6 The term ―States‖ refers to the 31 States and the Federal District in Mexico
7 UNDP HDR 2009 data for 2007
8 Values from the Informe sobre Desarollo Humano Mexico 2006-7.
9 UNDP 2009 and World Bank HNP Stats, 1995 and 2007 data.
10 WDI 2009, last figure for 2007.
11 WHO Global Burden of Disease database, estimates for 2004 using age-standardized DALYs, last updated in
February 2009.
HDI values Level of Human
Development
0-0.499 Low
0.5-0.799 Medium
0.8-0.899 High
0.9-1 Very High

3
4. As the HDI data and the dual burden of disease suggest, overall achievements in
health outcomes mask substantial disparities across population groups. These disparities are
closely linked to the level of socioeconomic development. The populations in the Mexican States
that have lower human and economic development, like Chiapas, Guerrero and Oaxaca, suffer
from dramatically higher mortality rates than those in States with higher human and economic
development, like Nuevo León and the Federal District. For example, in 2008, the maternal
mortality rate (maternal deaths per 100,000 live births) was 81.0 in Chiapas, while it was 23.6 in
Nuevo León (see Table 2).
Table 2. Maternal Mortality, HDI and GDP per capita by State, latest available data12
Maternal
Mortality, 2008
HDI, 2007 GDP per capita in
PPP $US, 2004
Chiapas 81.0 0.7185 $3,693
Guerrero 87.2 0.7390 $4,952
Oaxaca 97.3 0.7336 $3,978
Nuevo León 23.6 0.8513 $16,585
Federal District 55.2 0.8837 $23,029
5. In addition to broader socioeconomic determinants, Mexico’s disparities in health
outcomes, including financial protection, are associated with the fragmentation of its health
systems and, more specifically, with the historical underfunding of the public health care
service system for people without contributory social security. The Mexican health system
actually comprises several parallel sub-systems. Each of the three main sub-systems serves a
separate, specified population (as shown in Table 3), with their access being dependent on their
employment status. Two of these are ―contributory‖ social security schemes, meaning that
individuals and their employers each contribute to the cost of several benefits including health
insurance. IMSS covers workers in the formal sector and their dependents. ISSSTE covers public
sector employees and their dependents. The third sub-system, which serves the rest of the
population, is a public health care service system. The boundaries among sub-systems are not
merely administrative. The sub-systems each have their own service networks, and there is little
or no risk-pooling, information-sharing, or portability of benefits among them. These sub-
systems have been drawing on significantly different levels of funding. Between 1995 and 2000,
for the social health insurance systems of IMSS and ISSSTE, spending reached US$270 and
US$330 per capita per year, respectively. By contrast, it was a meager US$52 per capita for the
public health care service system.13
The chronically lower spending on the public health care
service system resulted in lower service quality, 20 percent lower utilization rates and ultimately
poorer health outcomes. For example, in 2000, the maternal mortality rate was nearly three times
as high among those with access only to the public health care service system as among those
with contributory social health insurance (75.8 versus 27.5 deaths per 100,000 live births). In
addition, for those dependent on the public health care service system, the added expenses of
user fees, paying for medicines, and frequent recourse to private services in lieu of low-quality
public service providers resulted in 40 percent higher out-of-pocket expenditures (as a proportion
12
Data for maternal mortality: own estimates based on INEGI/SS: 2000-2007; SEED preliminary 2008; Data for
HDI: UNDP HDR 2009 data for 2007; Data for GDP per capita in PPP $US: World Development Indicators 2006. 13
Parker & John Scott 2008, using a 1.00MXN to 0.205540971 USD exchange rate from January 2000.

4
of disposable household income) compared to beneficiaries of either IMSS or ISSSTE. This
often represented a significant share of the post-subsistence expenditures of poor households.
Table 3. Three Main Sub-systems of the Mexican Health System and their Populations
6. Apart from historically low levels of funding, the public health care service system has
faced persisting challenges of performance management and reform in a highly decentralized
form of federalism. In the 1980‘s and 1990‘s, the Federal Government14
decentralized the
delivery of primary and secondary health care services to States, thus creating 32 State Health
Systems15
. In this process, the Federal Government remained the main source of funding;
however, States were given almost complete autonomy over the use of funds. While the fiscal
coordination law requires the Federal Government and States to enter into annual results
agreements reflecting the priorities set forth in the National Development Plan, this never
became standard practice. Thus, for the time being, performance management arrangements are
only routinely used in federal health programs financed with resources above and beyond the
transfers guaranteed under the fiscal coordination law. Moreover, full implementation of policy
changes and reforms to the regulatory framework governing Mexico‘s public health care service
system requires strong buy-in from the highly autonomous States.
7. Given its historical low levels of funding and substantial performance challenges,
major investments in the public health care services for people lacking contributory social
security have been driving overall improvements in health outcomes. As early as 1973, the
Government set itself the goal of extending and strengthening health care infrastructure to
deprived areas and providing free services to marginalized groups through the program known
today as IMSS-Oportunidades. In 1996, with the Program for Coverage Extension (PAC), the
Secretariat of Health further boosted the geographic coverage of infrastructure within the public
health care service system and introduced a basic package of 34 mainly preventive health
interventions. By 2005, this package covered 89.2 percent of the rural population, with 29.3
percent of the total managed by IMSS-Oportunidades and 73.0 percent by the public health care
service (García Lopez 2009).16
Complementary to these programs, the Government implemented
14
The term ―Federal Government‖ refers to the Government of Mexico 15
The term ―State Health Systems‖ refers to the different administrative units, departments and individuals that
coordinate and administer health services in the 31 Mexican States as well as the Federal District. 16
The two programs overlap 3.2 percent of the total coverage area.
Type of Health
Subsystem Agency Eligible Population
Percent of Total
Population served
Contributory social
health insurance
Mexican Institute for
Social Insurance (IMSS)
Formally-employed private
sector workers and their
dependents
40 percent
Contributory social
health insurance
Institute for Social
Security and Services of
Government Workers
(ISSSTE)
Public sector employees and
their dependents 9 percent
Public health care
service system
Secretariat of Health and
the State Health Systems
All Mexicans, but primarily
the population not covered by
contributory social security
48 percent

5
the conditional cash transfer program Oportunidades, which targets the poor (all of them lacking
contributory social security) and holds its beneficiaries co-responsible for the regular use of
preventive health services (see Annex 1 for more details). Moreover, Mexico made great efforts
to scale up disease-specific programs for communicable diseases, which typically affect the poor
disproportionately; for example, vaccination programs, oral rehydration therapy, micronutrient
supplementation and anti-helminthic therapy (Sepúlveda et al. 2007).
8. To further invest in the health of people without contributory social security and to
reduce their persistently high out-of-pocket expenditures on health care, in 2003 Mexico
decided to transform the public health care service system into a public health insurance
system. Historically, policymakers assumed that inequalities across health subsystems were only
a transitional problem, as they expected the formal labor market to expand and automatically
make more people eligible for contributory social health insurance. However, in Mexico as in
other Latin American countries, this process has stalled. For example, between 1996 and 2006,
coverage of contributory social security stagnated at around 33-34 percent of the total workforce
(see Figure A2 in Annex 1). Drawing on the successful experiences of other countries with non-
contributory health insurance systems (see Table A4.1 in Annex 4), Mexican policymakers
decided to introduce a public health insurance scheme for people lacking contributory social
security, who tend to be mostly poor.
9. The introduction of the public health insurance scheme in 2003 brought three
fundamental changes to the public health care service system:
It replaced budgets with premiums. Prior to the reform, the Federal Government set the
federal budget envelope for the financing of State Health Systems based on expenditures
in the previous year, adjusted for inflation. It determined allocations to States based on the
payroll and infrastructure of each State Health System, with minor adjustments for
mortality rates. These rigid rules perpetuated low levels of funding for the public health
care system, ingrained large funding disparities across the States, and discouraged quality
improvements or innovation. Today, under the public health insurance, the Federal
Government bases the budget envelope and allocations to the States on an actuarially-
calculated premium; that is, a statistically determined payment based on the expected
costs of ensuring, providing, and overseeing a wide range of services and supporting
activities for the enrolled population. In turn, State Health Systems, in their role as the
administrators of the insurance, guarantee health benefits free of charge to those enrolled
in the insurance. The Federal Government finances close to 83 percent of this premium,
with States financing the remaining portion (See Box 2). These rules linked the funding of
State Health Systems to explicitly defined rights of beneficiaries. The rules were expected
to increase the resource envelope of the public health care service system and to reduce
financing disparities across States.
It eliminated user fees but, at the same time, introduced beneficiary contributions. Prior
to the reform, people without contributory social health insurance paid fees to access
health services. While these fees constituted an additional source of revenue for the
system, they created barriers to access health services, were highly regressive and
contributed to the high levels of out-of-pocket expenditures and their impoverishing
effects. Today, under the public health insurance, access to services is free at the time of
use. However, beneficiary households pay an annual contribution that States reinvest in

6
health services or use to build up reserves for the insurance scheme. This contribution is
proportional to each family‘s ability to pay, according to an income assessment. Families
belonging to the two lowest income deciles are exempted from contributing, as are low- or
middle-income families with children younger than five years old.17
The elimination of
user fees combined with the introduction of beneficiary contributions was expected to
increase health service utilization and reduce out-of-pocket expenditures among
beneficiaries. This promotes both inter-temporal risk pooling and consumption smoothing,
two of the chief objectives of a health insurance.
It introduced explicitly defined entitlements. Prior to the reform, the mandate of the
public health care service system was ambiguous. While State Health Systems aimed to
provide all citizens as needed with at least 34 primarily preventive interventions, access to
these and additional services was largely dependent on the availability of financial
resources in each State. Moreover, the system often lacked the resources to ensure service
quality, including the completeness of services. In contrast, the Public Health Insurance
explicitly defines beneficiary entitlements, disclosed in a letter to beneficiary families
along with an insurance policy; introduced an accreditation system for health facilities and
established mechanisms such as patient management, mediation and arbitration systems
that ensure that beneficiary rights are enforced. Along with the increase in resources and
the elimination of user fees, these mechanisms were expected to increase the utilization
and quality of health services and lead to better health outcomes for people without
contributory social security.
10. The public health insurance, named after a first pilot Seguro Popular (Popular Health
Insurance), has been quickly brought to scale. Since 2004, the Popular Health Insurance has
rapidly expanded health insurance coverage to eligible beneficiaries (adding on average
approximately 10 percent of the target population each year and in some years close to the
maximum annual rate of 14.3 percent set forth in the General Health Law) (Knaul et al. 2005).
At the end of 2009, there were more than 31 million individuals enrolled, more than half of the
approximately 48 million total eligible individuals. Likewise, the benefits covered by the Popular
Health Insurance have expanded significantly, from 76 health interventions at its inception to
266 interventions today. Thus, the Popular Health Insurance is the largest health insurance both
in terms of coverage and benefits for people lacking contributory social security in Latin
America (see Table A4.1 in Annex 4).
11. Even without achieving universal coverage, the Popular Health Insurance has already
improved the performance of the publicly-funded health care service system. Since its
inception, the Popular Health Insurance has been subject not only to its own internal control and
auditing systems but also internal and external evaluations (see Annex 3). Most importantly,
these evaluations found that the Popular Health Insurance has resulted in:
Increases in the spending on the health of people without contributory social security;
from, for example, US$52 per capita per year in 2001 to US$154 per capita per year in
17
Article 10 Bis 2 of Chapter 5 of the Guidelines for Affiliation, Operation, Integration of the National Beneficiary
Registry and the Determination of Family Contributions to the Social Protection System in Health States that, at the
time of affiliation, those families with at least on family member that is less than 5 years old and that is in at least
income decile III are exempt from contributing to the system.
7
2004 (González-Pier et al. 2007). This has begun to correct the financing inequalities
across health subsystems and State Health Systems. For example, the ratio of public
expenditures for IMSS compared with those on the publicly-funded health care service
changed from 5:1 to 3:1, and expenditure inequalities across State Health Systems
changed from 5:1 to 4:1.
The effective removal of financial barriers to access health services, resulting in increases
in the utilization of health services (compared with the uninsured), which in turn are
expected to translate into better health over the coming years. For example, the utilization
of health services was significantly higher for Popular Health Insurance beneficiaries
(63.6 percent) compared to the uninsured (58.3 percent) (Gakidou et al. 2006; Bleich et al.
2007; Hernández-Torres et al. 2008).
Reductions in the likelihood of suffering from catastrophic18
and impoverishing health
expenditures (compared with the uninsured). For example, from 2005 to 2006, the Popular
Health Insurance reduced the proportion of those experiencing catastrophic expenditures
by 23 percent (Knaul et al. 2005; King et al. 2009); likewise, the probability of incurring
catastrophic health expenditures was estimated as 8 percent less for households with
Popular Health Insurance affiliates than for uninsured households (Hernández-Torres et al.
2008). In addition, opinion surveys show that Popular Health Insurance beneficiaries are
satisfied with the scheme. More than 95 percent of beneficiaries are ―very satisfied‖ or
―relatively satisfied‖ with the insurance; moreover, 95 percent of health service users are
―very satisfied‖ or ―somewhat satisfied‖ with the health services provided.
12. The Popular Health Insurance constitutes the key pillar of Mexico’s Social Protection
System in Health serving people without contributory social security. It is administered by
State Health Systems. In addition to the Popular Health Insurance, the SPSS includes the Fund
for Protection against Catastrophic Health Expenditures (the Fund), which finances complex,
mostly tertiary health care interventions. Moreover, in 2006 the Federal Government established
the Health Insurance for a New Generation, a federal program, which complements the benefits
of the Popular Health Insurance and finances 116 complex maternal and child health
interventions (for example open-heart surgery for children). The 32 State Health Systems
administer the Popular Health Insurance; while in contrast, the National Commission for Social
Protection in Health (the Commission) and the State Health Systems jointly administer the
Health Insurance for a New Generation and the Commission solely administers the Fund. The
Commission also provides the general oversight for the SPSS.
Current Challenges to the System
13. With seven years of implementation, the Popular Health Insurance has produced
dramatic results for the health and social protection of families without coverage by
contributory social security (see paragraph 11); however, at the same time, it faces some
important challenges. These challenges fall into the broad categories of expanding coverage and
effectively administering the entitlements of the insurance.
18
Catastrophic expenditures are defined as out-of-pocket health expenses greater than 30 percent of post-subsistence
income.

8
14. The current recession calls for an accelerated expansion of Popular Health Insurance
coverage but, at the same time, may hamper it. Policymakers introduced the Popular Health
Insurance with the goal of achieving universal health insurance coverage. They hoped to achieve
this goal by 2010. The current Government reconfirmed the goal of universal health insurance
coverage and, based on earlier affiliation patterns, set the firm target date of 2012. However, the
current crisis calls for an accelerated expansion of the Popular Health Insurance and, at the same
time, poses a threat to the short-term goal of universal coverage. International evidence,
including Mexico‘s experience during the 1994-95 and 2000-01 crises, demonstrates the
importance of securing and, if possible, increasing financial protection in health to safeguard
health gains during downturns. As household income drops, families tend to invest less in their
health. For example, they use health services (and in particular preventive services) less
frequently, and poor and vulnerable households also cut back on food expenditures (A. Ávila &
Shamah Levy 2006). At the same time, however, with informal employment and unemployment
on the rise, fewer people have access to coverage through contributory social security systems,
which means that more people become dependent on subsidized public health insurance or the
public health care service systems. Moreover, fiscal revenues drop, forcing governments to
reduce their spending across social programs, including subsidized public health insurance
schemes and public health care service systems (Gobierno de México 2008).
15. In late 2009, Mexico took a bold step to substantially expand Popular Health
Insurance coverage during the economic crisis. In December of 2009, the Government
proposed and Congress unanimously approved changes to the General Health Law to refine the
premium system. These changes entailed a reduction of the premium level. This reduction
rectified an earlier design shortcoming; that is, a discrepancy between the information on family
size that fed into the original calculation of the premium (4.3 members per family based on
census data) and the actual average size of beneficiary families (3.1 members per family). The
adjustment of the premium level will allow the enrollment of more than 6 million additional
beneficiaries within current State health system budgets. Furthermore, the Federal and State
Governments are committed to create the necessary fiscal space to provide financial protection in
health to all Mexicans by 2012.As a consequence, the Commission will have to shift its focus
from limiting affiliation to the poor and most vulnerable (which prevailed during the early stages
of scaling-up the Popular Health Insurance) to stimulating demand for affiliation across all
eligible population groups, but while maintaining a focus on hard-to-reach groups. The changes
introduced into the General Health Law also entailed the switch from a per-family to a per-capita
premium. The originally adopted per-family premium system discriminated against States with
larger average family sizes, which tend to have less developed health systems and lower health
budgets. Hence, the switch to a per-capita system will help further alleviate the reductions in
financial imbalances resulting from the introduction of the Popular Health Insurance. At the
same time, however, the affiliation of beneficiaries will remain family-based.
16. The second major challenge is to effectively administer the entitlements of the Popular
Health Insurance. Since its inception, the policies of Popular Health Insurance have been geared
toward rapid enrollment. Having overcome many obstacles in this endeavor and moving rapidly
towards universal coverage, policymakers have shifted their attention towards the effective
administration of Popular Health Insurance entitlements. Pursuing this shift, the Commission has
identified three priorities for the coming three years: (i) strengthening performance management
9
while accelerating structural reforms of State Health Systems; (ii) improving beneficiaries‘
awareness of their rights; and (iii) fostering health promotion and disease prevention.
17. The design of the Popular Health Insurance foresees fundamental changes to the
organization and management of State Health Systems, including the development of critical
health insurance functions; yet, the implementation of these reforms has been slower than
anticipated. When health service delivery was decentralized to the States in the 1980‘s and
1990‘s, State Health Systems adopted a vertically-integrated organizational model in which the
functions of oversight (stewardship), financing and service provision were centralized in State
ministries of health. With the introduction of the Popular Health Insurance, the regulatory
framework for the State Health Systems stipulates an organizational separation of these
functions, most importantly, the creation of insurance agencies, so-called Regímenes Estatales de
Protección Social en Salud or REPSS. This separation would pave the way for stronger
accountability mechanisms between the insurance agencies and service providers and new
financing arrangements for service providers. These changes would reap further benefits; most
importantly, the possibility to purchase health services from all existing provider networks
(including the networks of IMSS and ISSSTE), which would in turn enhance access to services,
make the use of existing service infrastructure more efficient, and facilitate the portability of
insurance coverage (across State Health Systems). The above would constitute a major step
towards overcoming the fragmentation of the Mexican health system. To date, all States have
established the REPSS, eighteen have joined forces under the Commission for the Organizational
Restructuring of State Health Systems to further advance the organizational and institutional
reforms, and two have adopted the strategic purchasing of services. Further progress along this
reform path in all States will depend on the effective transfer of knowledge across States as well
as enhanced technical assistance from the Federal Government.
18. As the organizational reform of State Health Systems advances, refined and stronger
performance management arrangements between the Commission and State Health Systems
can enhance the effective administration of the Popular Health Insurance’s entitlements. As
State Health Systems continue to develop and strengthening REPSS, the onus is on the
Commission to establish incentives that promote the efficient delivery of the entitlements and
specifically the benefit package of the Popular Health Insurance. With the exception of the 1.25
percent of the federal solidarity contribution that is dependent on State Health System
performance, financial incentives currently remain geared toward affiliation, not performance
improvements. Furthermore, the regulation of responsibilities remains patchy. This weakness is
compounded by the limited capacity of State Health Systems to comprehensively collect and
analyze service delivery data. Hence, limited information flows from State Health Systems as
well as surveys carried out jointly by the Commission and State Health Systems. Also the
capacity of the Commission to comprehensively corroborate information reported by State
Health Systems requires strengthening. As such, the monitoring of the administration of
entitlements remains incomplete, which hampers an effective performance benchmarking of
State Health Systems. While a worthy goal in itself, an enhanced performance management
arrangement between the Commission and State Health Systems would also goad organizational
and management reforms in State Health Systems.
19. Improving the effective administration of Popular Health Insurance entitlements also
hinges on an improved understanding of these rights by beneficiaries. Entitlements under the
10
Popular Health Insurance (and for families with small children under the Health Insurance for a
New Generation) include a multitude of health care services, which are defined in detail through
protocols and guidelines. While surveys suggest that the beneficiaries of these insurances are
generally satisfied with the health care services they receive, there is evidence that they have
only a limited knowledge of entitlements.19
This impairs the use of preventive services in
particular, since demand for such services depends on households understanding their
importance; that is, health literacy rather than acute health needs. It also undermines efforts to
protect beneficiary rights through patient management, mediation and arbitration systems.
Efforts to improve the understanding of entitlements and more broadly the benefits of insurance
also have to go beyond current beneficiaries. They have to reach out to the broader target
population of the Popular Health Insurance – that is, those without contributory social security –
to ensure that there is sufficient demand for affiliation. These efforts need to reach marginalized
municipalities with large indigenous populations and those living in poverty, which tend to have
far below average educational levels and face other structural barriers to demand affiliation.
20. Effectively administering entitlements will also depend on promoting demand for
health promotion and disease prevention services. Currently, beneficiaries frequently seek care
for curative services. In contrast, demand for interventions that promote health and prevent
diseases—some of the most cost-effective interventions—remains relatively low in Mexico. This
lessens the overall (allocative) efficiency of the system, especially in the context of an increasing
burden of non-communicable diseases. Preventing many non-communicable diseases and their
complications is inexpensive, while treating them is costly (and sometimes impossible). Regular
contacts with the health system for disease prevention and health promotion would also allow the
Commission to establish a comprehensive epidemiological profile of the beneficiary population,
which would further help to comprehensively assess the financial risks facing the system.
B. Rationale for Bank involvement
21. The World Bank Group’s (WBG) Country Partnership Strategy (CPS) for Mexico
(Report No. 42846-MXY March 4, 2008) identified several principles of engagement including
flexibility, fast response, and selectivity driven by the key long term development challenges of
Mexico. The proposed operation demonstrates the Bank‘s flexibility and fast response capacity
to Mexico's changing financing and development needs in the context of the economic crisis. It
is closely aligned with two of the strategic development challenges identified in the CPS:
sustainable growth through investment in human capital and strengthening institutions. Toward
the former, the proposed Project (henceforth the Project) would help to remove barriers to access
health services and would strengthen financial protection for people lacking contributory social
security, mostly poor families. Toward the latter, the proposed Project would help to improve the
organizational and institutional arrangements and, ultimately, the performance of the Popular
Health Insurance.
22. The Mexican Government has requested Bank support in tackling the challenges
facing the Popular Health Insurance. The rationale for its involvement is three-fold. First,
19
This phenomenon is well documented for non-contributory health insurance schemes in the Latin American and
Caribbean region. Possible explanations include the rather short implementation periods of the schemes, moreover,
the generally low educational attainments of its target populations.
11
Bank support would be productive as it would build on two decades of successful experience
supporting the development of Mexico‘s health sector. Since the preparation of the First Basic
Health Care Project in the late 1980s, a series of Bank projects have supported the expansion and
improvement of quality health services, institutional reforms of State Health Systems for the
effective administration of the Popular Health Insurance, and improvements in monitoring
reform progress. In addition, the Influenza Preparation and Control Project, approved by the
Board in November, aims among other objectives to strengthen the national disease surveillance
system. Furthermore, ongoing programmatic analytical and advisory activities assess options to
improve the performance of the Popular Health Insurance and advance its integration with the
contributory social health insurance systems (see Box 1).
23. Second, the Bank has extensive experience in designing, implementing and
strengthening of health insurance programs to expand coverage to the poor, informal worker
families and other vulnerable groups. Globally, the Bank has been supporting more than forty
countries in the introduction and scaling up of non-contributory or subsidized-contributory health
insurance schemes, including in Argentina, the Dominican Republic, Honduras, Panama,
Nicaragua, and Paraguay. These countries have implemented non-contributory health insurance
schemes with the same broad benefits and target populations as the Popular Health Insurance in
Mexico or, for example, the “Plan Nacer” program in Argentina providing limited benefits to
mothers and children.
24. Finally, the Bank is supporting Mexico in strengthening social programs that face
similar challenges and/or contribute to the same goals of the Popular Health Insurance—
most importantly, Mexico’s conditional cash transfer program, Oportunidades—and,
therefore, can facilitate exploiting synergies. The Commission and the management of the
Oportunidades program are working towards a joint strategy with the help of the Bank. A first
successful step in this endeavor was the rapid scale-up of the Popular Health Insurance, which
will eliminate a perverse financial incentive for State Health Systems to give the affiliation of
Oportunidades beneficiaries less priority than they deserve. In addition, there is scope for
significant efficiency gains across the reform priority areas identified for the Popular Health
Insurance. For example, enhanced monitoring of State Health System performance needs to
capture information for Oportunidades beneficiaries and can use Oportunidades databases.
Efforts to empower and educate Popular Health Insurance beneficiaries can use Oportunidades
information and communication platforms. Finally, the Popular Health Insurance will be able to
draw on strategies to promote health and prevent diseases as well as general lessons learned from
the Oportunidades program.

12
Box 1: More than 20 Years of Successful Cooperation in Health System Strengthening
For more than 20 years, Mexico and the Bank have been working jointly to strengthen the
health system and improve health by expanding basic health services to the poor. In 1990, with
the First Basic Health Care Project, the Government requested the Bank support in its efforts to
strengthen the health sector. The First and Second Basic Health Care Projects supported
Government efforts to expand health service coverage to approximately 10 million people in
rural and remote areas, coming close to attaining full geographic coverage. The Third Basic
Health Care Project has further contributed to improving access to quality primary and hospital
care for 22 million poor Mexicans.
Currently the Bank is implementing two health projects that are highly relevant to the current
project: the Third Basic Health Care project and the Influenza Prevention and Control
project. The Third Basic Health Care Project has provided key support to the implementation
and expansion of the SPSS for more than seven years. This experience is essential to the
activities undertaken by the Popular Health Insurance, particularly in the areas of service
delivery and the reform efforts. Furthermore, the project builds on 5 years of programmatic
sector work (analytical and advisory services), examining options for reform of the system‘s
financing as well as functional integration. The Influenza Prevention and Control project aims to
strengthen the national surveillance system responsible for collecting the country‘s
epidemiological data on a regular basis, which is essential for the development of a benefits
package that targets high-frequency, high-cost pathologies in the population and for the better
alignment of Popular Health Insurance‘s benefit package.
The Bank is also carrying out a three-year programmatic analytical and advisory activity in
support of the functional integration of the Mexican health system. While the fragmentation of
the system is not a problem per se; design issues within this approach, such as incentive
incompatibility and a lack of cooperation impede the performance of the health system.
Functional integration aims to overcome these design issues without merging health sector
organizations. The analytical and advisory activity helps to (i) identify priorities among the many
challenges of functional integration, (ii) assess the readiness and facilitate the development of
objectives for functional integration in priority areas, and (iii) support sub-systems in developing
reforms consistent with these objectives.
The Bank also has supported Mexican Government’s efforts to improve the efficiency of
contributory social health insurance programs, IMSS and ISSSTE. When the financial
sustainability of Government insurance programs was threatened in 1998, the Bank worked with
it to design and implement critical policy changes. An adjustment loan combined with a
technical assistance loan supported the Government in developing a sound, long-term strategy to
manage liabilities, introduce user choice and competition, develop purchasing mechanisms and
strengthen health service delivery networks.
13
C. Higher level objectives to which the project contributes
25. The Project would support strategies and objectives outlined in the Government’s
National Health Sector Program (Programa Sectorial de Salud, PROSESA) 2007-2012 and
aligned with the health-related MDGs and the National Development Plan (NDP) 2007-
2012. It would directly support four of the ten strategies outlined in PROSESA: (i) consolidating
the financing reform for effective, universal access to essential health care interventions; (ii)
improving the planning, organization, development and accountability mechanisms of the health
system; (iii) developing systems, technologies and processes that improve the efficiency and
promote the integration of the sector; and (iv) strengthening health promotion and disease
prevention. Furthermore, it would contribute to central objectives of the PROSESA, including
increases in health service utilization and reductions of mortality and out-of-pocket expenditures.
As such, it would help to sustain and accelerate progress towards the health-related MDGs in the
context of the economic crisis, particularly reducing infant and maternal mortality. Likewise, the
Project would contribute to the goals and principles of the NDP; specifically, the goal of creating
equal opportunities and the principle of targeting resources to programs that have demonstrated
their effectiveness in reaching the poor.
II. PROJECT DESCRIPTION
A. Lending instrument
26. The proposed/selected lending instrument is a specific investment loan of US$1,250
million.
B. Project development objective
27. The proposed Project Development Objectives are to (i) initially preserve and later
expand the Popular Health Insurance’s coverage of people without contributory social
security and (ii) strengthen the capacity of the Commission and State Health Systems to
effectively administer the entitlements of the Popular Health Insurance.
C. Project Key Performance Indicators
28. The key performance outcome indicators for the Project are as follows:
Number of individuals affiliated with the Popular Health Insurance as a percentage of the
total number of individuals that are not affiliated with a contributory social security
system.
Number of State Health Systems that collect information on system results (including
beneficiary satisfaction and number, quality and cost of services delivered) that is
validated, widely publicized and used for performance improvement recommendations by
the Commission20
.
20
Information would be made available through State Secretariat of Health internet portal, through the press and/or
radio announcements.

14
Number of individuals affiliated with the Popular Health Insurance who have received a
―Health Risk Screening‖21
as a percentage of the total number of individuals affiliated
with the Popular Health Insurance.
Number of individuals affiliated with the Popular Health Insurance that report having
received enough information to know their rights and obligations as a percentage of the
total number of individuals affiliated with the Popular Health Insurance.
29. The proposed key intermediate outcome indicators for the Project are as follows:
Federal and State expenditure on the Popular Health Insurance (US$ constant exchange
rate (2009)).
Number of State Health Systems that collect information on system results (including
beneficiary satisfaction and number, quality and cost of services delivered) that is
validated by the Commission.
Health risk management program guidelines have been designed and rolled out.
Number of individuals affiliated with the Popular Health Insurance who report having
received a bill of rights and responsibilities at the time of affiliation as a percentage of the
total number of individuals affiliated with the Popular Health Insurance.
Expected Outcomes
30. The Project is expected to contribute to the extension of health insurance coverage and
the effective administration of entitlements and to produce four major outcomes. First, the
Popular Health Insurance coverage of people without contributory health insurance would be
gradually expanded from 31.1 million (64 percent) to 41.1 million (85 percent). Second, the
Commission would have ramped up its activities to capture, benchmark, and widely disseminate
information on the service delivery of the State Health Systems as well as to issue
recommendations to improve performance. Third, the percentage of Popular Health Insurance
beneficiaries who consider the information provided to them about their rights under the Popular
Health Insurance as adequate is expected to increase from 71 to 80 percent. Finally, 10 million
Popular Health Insurance beneficiaries would have received a health risk screening.
D. Project components
31. The Project would consist of two components. Component I would finance eligible
federal ―social contributions‖ (see Box 2) to the premium of the Popular Health Insurance to
initially preserve and later expand the Popular Health Insurance‘s coverage of people without
contributory social security. Across the globe, Bank projects have started to co-finance insurance
and in particular health insurance premiums. The proposed Project would be a logical extension
of this practice insofar that it would finance the insurance premium of the developing world‘s
largest (both in terms of population and benefits) and highly scrutinized health insurance for
people without contributory social security. Component II would finance technical assistance to
strengthen the capacity of the Commission and State Health Systems to effectively administer
the entitlements of the Popular Health Insurance, including technical assistance for enhanced
performance management and support to States in preparing and carrying out reforms in the
administration of the Popular Health Insurance, improved knowledge of eligible beneficiaries
21
Health Risk Screening is an integral part of the Health Risk Management Program.
15
about entitlements, strengthened health risk management, and effective project coordination and
management.
Component I: Popular Health Insurance’s Coverage of People without Contributory Social
Security (US$1,239 million)
32. Financing of eligible federal social contributions to the premium of the Popular
Health Insurance to initially preserve and later expand the Popular Health Insurance’s
coverage of Eligible Beneficiaries. Specifically, component I would finance the share of the
federal social contributions earmarked for financing the Popular Health Insurance premium (i.e.
the share of one of the contributions made by the federal government to such premium) as
referred to in Article 77 of the General Health Law (for details on the financing of the premium
see Box 2 and Annex 4).
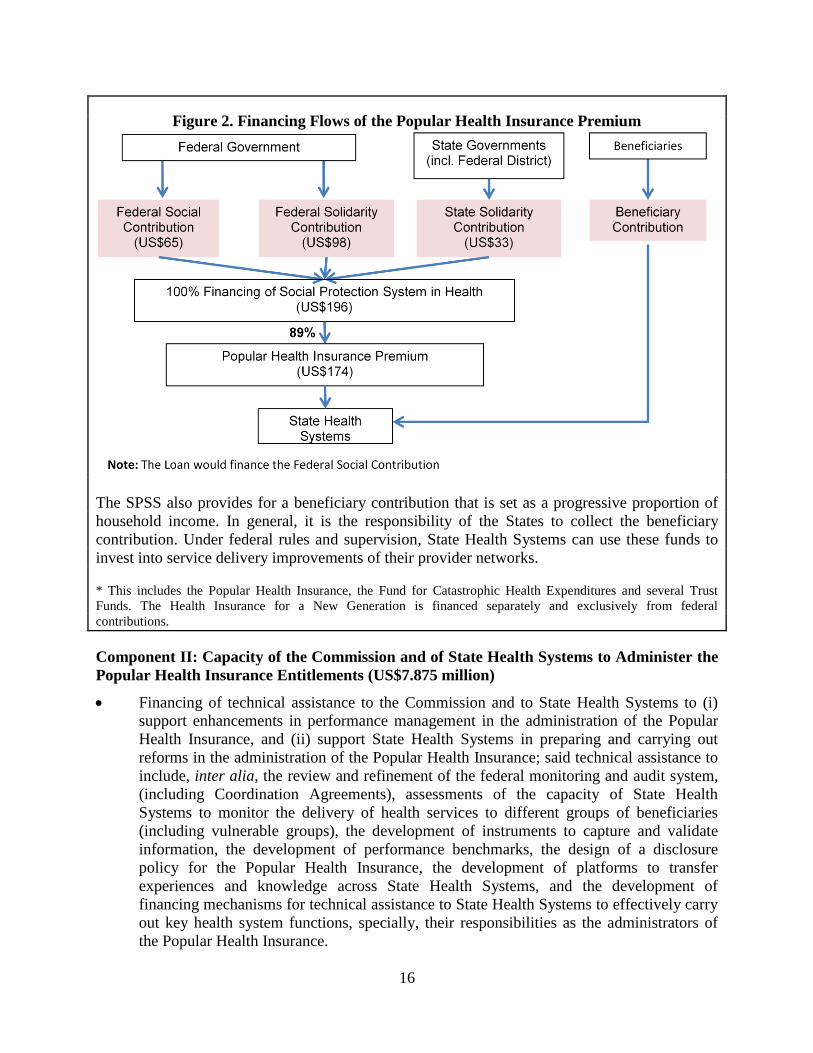
Box 2. Financing of the Popular Health Insurance
The SPSS*, including the premium of the Popular Health Insurance, is financed by the Federal
and State governments. The specific arrangements mimic the tripartite funding model of
Mexico‘s contributory social security systems (which combine employer, employee, and
Government contributions). The Federal Government makes two contributions: the social
contribution (cuota social) and the federal solidarity contribution (aportación solidaria
federal). States make their own contribution called the state solidarity contribution (aportación
solidaria estatal).
The General Health Law establishes the premium of the Popular Health Insurance as a fixed
share of all three federal and State contributions (currently 89 percen; the remaining 11 percent
finance the Fund for Catastrophic Health Expenditures as well as trust funds for infrastructure
investments and reserves). Moreover, the law sets forth the relative magnitude of the
contributions and, thus, the share of Federal and State government financing. With the federally-
financed social contribution serving as the reference point, the federal solidarity contribution is
set at 150 percent of the social contribution and the state solidarity contribution at 50 percent the
amount of the social contribution. Thus, the combined federal financing is five-sixths of the
premium compared to the State financing of one-sixth of the premium. Analogous to Mexico‘s
social security system, the General Health Law provides for a dynamic adjustment of the
premium by linking the social contribution to the minimum general salary of the Federal District.
Per labor law, the minimum general salary of the Federal District is annually adjusted for
consumer price inflation, which in the case of Mexico and other Latin American countries
corresponds well with health inflation (World Bank, forthcoming). Recent changes to the
General Health Law recalibrated the social contribution and reduced it from 4.84 to 3.92 percent
of the minimum general salary of the Federal District.
An actuarial system annually assesses the financial sustainability of the Popular Health
Insurance. More specifically, it assesses the financial impact of uncertainty and risks using
statistical probabilities for a large variety of variables, including, for example, health needs,
treatment seeking behaviors and cost structures. As in last year‘s case, the identification of
significant mismatches between the premium, reserves and insurance risks should prompt
adjustments to the premium (and possibly to the insurance benefits as well).
16
The SPSS also provides for a beneficiary contribution that is set as a progressive proportion of
household income. In general, it is the responsibility of the States to collect the beneficiary
contribution. Under federal rules and supervision, State Health Systems can use these funds to
invest into service delivery improvements of their provider networks.
* This includes the Popular Health Insurance, the Fund for Catastrophic Health Expenditures and several Trust
Funds. The Health Insurance for a New Generation is financed separately and exclusively from federal
contributions.
Component II: Capacity of the Commission and of State Health Systems to Administer the
Popular Health Insurance Entitlements (US$7.875 million)
Financing of technical assistance to the Commission and to State Health Systems to (i)
support enhancements in performance management in the administration of the Popular
Health Insurance, and (ii) support State Health Systems in preparing and carrying out
reforms in the administration of the Popular Health Insurance; said technical assistance to
include, inter alia, the review and refinement of the federal monitoring and audit system,
(including Coordination Agreements), assessments of the capacity of State Health
Systems to monitor the delivery of health services to different groups of beneficiaries
(including vulnerable groups), the development of instruments to capture and validate
information, the development of performance benchmarks, the design of a disclosure
policy for the Popular Health Insurance, the development of platforms to transfer
experiences and knowledge across State Health Systems, and the development of
financing mechanisms for technical assistance to State Health Systems to effectively carry
out key health system functions, specially, their responsibilities as the administrators of
the Popular Health Insurance.
Figure 2. Financing Flows of the Popular Health Insurance Premium

17
Financing of technical assistance to the Commission and to State Health Systems to
improve the knowledge of Eligible Beneficiaries about their entitlements under the
Popular Health Insurance; said technical assistance to include, inter alia, the design of a
communication strategy with a focus on vulnerable groups, consultations with
stakeholders, the development of communication tools, implementation support to State
Health Systems, including training and supervision of the implementation of said
communication strategy, the evaluation of communication pilots as well as evaluation of
said communication pilots and communication strategy, including the review and
development of surveys, data collection and data analysis.
Financing of technical assistance to the Commission and to State Health Systems to
strengthen their capacity to manage health risks; said technical assistance to include, inter
alia, the design of a health risk management program, consultations with stakeholders,
training and implementation support to State Health Systems, including the supervision of
the implementation of said health risk management program, the evaluation of health risk
management pilots and said health risk management program, including the design of
surveys, data collection, and data analysis.
Financing of technical assistance to allow the Commission coordinate and manage the
Project; said technical assistance to include, inter alia, the training of staff in fiduciary and
safeguard matters, the carrying out of annual external audits, and the carrying out of the
activities included in the Indigenous Peoples Plan (IPP).
E. Lessons learned and reflected in the project design
33. A number of lessons have been gleaned from the Bank’s experience in Mexico during
the past two decades as well as from the implementation of similar projects around the world. Several of these lessons informed the selection of the lending instrument, the identification of
risks and the design of the risk mitigation measures; these lessons are discussed in the
corresponding sections of this document. In addition, two essential lessons have been
incorporated into the design of the Project: the need for comprehensive incentive and support
systems to foster reform in highly decentralized contexts, and the importance of empowering
beneficiaries of insurance systems serving the poor and vulnerable.
34. In highly decentralized systems, for comprehensive health sector reforms to be
implemented successfully at the local level (which can take as long as two decades), the
central authority must develop incentive and support systems to help local agencies to
implement the reforms. The Bank‘s experience in the Dominican Republic, Hungary,
Germany, and many other countries around the globe suggest that legislative reform is just the
beginning of the reform process. Therefore, Component II would support the Commission in
developing a comprehensive incentive and support system to enhance the performance of State
Health Systems and drive the pace of reform. This system would combine good practices from
countries such as Argentina, China, Indonesia, Poland, and Turkey, including closer monitoring,
the publicizing of the results of this monitoring, setting benchmarks, making financing
conditional on results, creating platforms for the exchange of experiences and innovations, and
building capacity. Even with such incentives and support, the experience of Mexico itself as well
as that of other countries suggests that reforms take a long time to implement in very
18
decentralized health systems. Therefore, the Project‘s targets are ambitious but realistic and have
been drawn from the experiences of the Mexico Third Basic Health Care Project.
35. The introduction of health insurance can yield major improvements in the
performance of a health system, but the full potential impact will only be realized if
beneficiaries are empowered. Health insurance systems for the poor and other vulnerable
groups have been emerging in many developing countries over the past two decades and have
increasingly become a focus of the Bank‘s support to the health sector. This focus of the Bank‘s
reflects its recognition that, if properly designed and implemented, health insurance can yield
significant improvements in health system performance, including making the system more
accountable, bringing it higher levels of funding, making it more efficient, increasing people‘s
awareness of their health, empowering them and giving them more choice among providers,
increasing consumer satisfaction, widening financial protection, and improving health outcomes.
While the positive impact of health insurance in terms of increasing the use of health services
and reducing out-of-pocket expenditures has been well demonstrated, public health insurance
schemes still do not perform as well as contributory social security systems in terms of health
and financial protection outcomes. Some studies have attempted to disentangle the underlying
issues and have shown that beneficiaries of health insurance systems have only a limited
understanding of their rights under the system. For example, a study carried out in the
Dominican Republic showed that only about one-third of the beneficiaries have a basic
understanding of their rights. At the same time, there is ample evidence from around the globe
that beneficiaries need to be knowledgeable about their entitlements, first, to encourage them to
make use of important health services and, second, to encourage them to hold providers
accountable by using complaint, mediation, and arbitration systems. Taking all these experiences
and evidence into account, Component II would support the Government in empowering
beneficiaries by increasing their knowledge and understanding of their entitlements. This would
entail the development of communication strategies aimed at changing the behavior of
beneficiaries towards health service utilization that would draw specifically on the many lessons
learned from HIV/AIDS and other disease-specific programs.
F. Alternatives considered and reasons for rejection
36. A specific Investment Loan was chosen as the most appropriate instrument for the
Project; however, initially also the option of a Development Policy Loan was considered. As
discussed earlier (see paragraph 15), during a crisis, the chief challenge is to maintain, if not
increase, spending on essential health services for the poor and vulnerable. At the same time,
however, the economic crisis provides an opportunity to take on critical reforms to improve the
efficiency of health systems. Mexico is committed to achieve both, maintaining, if not increasing
spending for the Popular Health Insurance and pursuing reforms to enhance its performance in
the medium term. Therefore, a Specific Investment Loan seems most appropriate as it offers the
opportunity to combine a fast-disbursing component to help maintain and increase current levels
of federal funding during the economic crisis and a strong technical assistance component that
supports reform over the medium term. Furthermore, the supervision efforts of an investment
loan, specifically financial controls and financial management support would buttress the
Government‘s efforts to enhance performance management. In the past, the Bank has supported
countries also through Adjustment and Development Policy Loans with conditions that

19
attempted to protect public pro-poor health expenditures. When conditions were carefully
designed with strong monitoring systems in place, these operations helped to protect public pro-
poor health expenditures. Given their focus to meet short-term financing needs, however, this
type of design is less appropriate to support mid-term reforms.
III. IMPLEMENTATION
A. Institutional and implementation arrangements
37. Project activities would be coordinated and implemented using the organizational
structures and staff of the National Commission for Social Protection in Health (the
Commission). The Commission is a deconcentrated unit within the Secretariat of Health with
technical, administrative and operational autonomy. As set forth in the Reglamento Interno de la
Comisión Nacional de Protección Social en Salud22
, it is responsible for the implementation of
the Social Protection System in Health (SPSS). Within the Commission, the Office of the
Commissioner would constitute the Project Coordination Unit (PCU), responsible for overall
coordination of Project activities. Under the coordination of the PCU, three General Directorates
of the Commission, and their staff, would play critical roles in Project implementation: the
General Directorate of Finance (DGF) and the General Directorate of Affiliation and Operation
(DGAO) would jointly lead the implementation of Component I; while the General Directorate
of Coordination with Federal Entities (DGCEF) and the General Directorate for Affiliation and
Operation (DGAO would jointly lead the implementation of Component II.
38. Project implementation would hinge on close cooperation between the Commission
and the States. Every year, the Federal Secretariat of Health, through the Commission, enters
into coordination agreements with the States. These coordination agreements guide the
implementation of the SPSS, including the Popular Health Insurance. In addition, the
Commission through an official communication would require the States to commit to
implementing the activities laid out in the IPP and to collaborate with the Federal Secretariat of
Health to ensure the transparent implementation of the Project.
39. In all matters related to financial management and procurement, the PCU would be
supported by the National Finance Agent (NAFIN), a public financial agent with ample
experience in supporting the implementation of Bank-financed projects. Prior to Project
effectiveness, cooperation with NAFIN would be governed by a contract (Contrato de Mandato)
between them, the Federal Secretariat of Finance and the Federal Secretariat of Health.
40. Disbursement arrangements would follow standard procedures. Eligible expenditures
would be reimbursed on the basis of Statements of Expenditures (SOEs). As for component I,
these SOEs would be supported by Statements of Affiliation Registry. Eligible expenditures
incurred between July 1, 2009 and loan signing would be reimbursed up to an amount not to
exceed 20 percent of the loan amount.
22
Published in the official gazette (Diario Oficial de la Federación) on February 27, 2004.

20
B. Monitoring and evaluation of outcomes/results
41. The monitoring and evaluation of the Popular Health Insurance is part of a national
effort to systematically monitor and evaluate social programs and adopt a performance
informed budgeting approach. Changes to the Social Development Law introduced in 2004
established the National Council for the Evaluation of Social Development Policy (CONEVAL);
furthermore, they require the assessment of all programs and the reporting of findings to
Congress and the public. Accordingly, the Federal Government has established a system of
performance evaluation for all social programs, including the Popular Health Insurance, which
sets forth matrices of result indicators and targets. The results of these assessments are reported
to Congress, as part of a broader effort to adopt a performance informed budgeting approach.
The inputs to the annual assessments of the Popular Health Insurance include a variety of
available survey data and administrative information that capture insurance coverage, targeting,
beneficiary satisfaction and operational aspects. In response to these assessments, the
Commission informs Congress every year about plans to address shortcomings. As such, the
assessments have been a critical factor in strengthening the administration of the Popular Health
Insurance.
42. Project monitoring would primarily draw on Mexico’s monitoring and evaluation
system for the Popular Health Insurance and the health system. Information would flow from
four different sources. First, information would flow from the Commission‘s integrated
supervision tool that tracks and consolidates information on affiliation including data on the
number of beneficiary families and their characteristics (for example, number of family
members, indigenous, female or male head of household, income decile). Second, other
information would flow from surveys, most importantly, a semi-annual survey of beneficiary
satisfaction (carried out by the Commission) as well as the national health and nutrition and the
national household income and spending surveys. Third, information would flow from the
National Health Information System and the Annual Federal Budget and Expenditure Report.
Finally, the Commission would report, and Bank supervision missions would validate,
information on qualitative indicators, capturing progress towards critical milestones in capacity
building. In general, information sources and flows are well established. The Commission would
consolidate information from the various sources in the semi-annual Project report.
C. Sustainability
43. For at least four reasons, the Popular Health Insurance is here to stay and its coverage
most likely to be maintained if not expanded throughout and beyond the proposed Project.
First, it is grounded in the rights and principles enshrined in the Mexican Constitution and
established by the 2003 General Health Law. More than two decades ago, the Mexican
Constitution formally recognized the social right to health protection. In 2003, changes to the
General Health Law established the Popular Health Insurance to ensure that all individuals,
including those lacking contributory social security, are equally able to exercise this right. This
distinguishes the Popular Health Insurance from any other social program in Mexico, including
the conditional cash transfer program Oportunidades. Second, the Popular Health Insurance
enjoys broad, non-partisan political support. It is in its seventh year of operation and has
survived one presidential election cycle. Congress has been endorsing proposals for its expansion
and, more recently, for adjustments of the premium system with overwhelming majorities. Third,

21
the Popular Health Insurance has demonstrated significant improvements in health and financial
protection; furthermore, the Project activities under Component II would serve to reinforce the
efficiency of the Popular Health Insurance. During the pilot and first phase of scaling-up, the
Popular Health Insurance has been subject to rigorous, external evaluations to measure in detail
its impact on effective coverage and financial protection. Since as early as 2006, it has
demonstrated positive results. Combined, enhanced performance management, improved
knowledge by beneficiaries about their entitlements and a health risk management system would
enhance the efficiency of the insurances‘ administration. Finally, the Bank loan would constitute
only a small fraction of the federal and State contributions to the insurance premium (i.e. less
than 5 percent of the Project costs).
D. Critical risks and possible controversial aspects
44. The project presents some risks to its development objective and component results as
well as a controversial aspect; however, overall, when mitigated with the proposed measures,
these risks are moderate. The critical risks to the development objective include the risks that (i)
fiscal pressures may reduce federal funding for the Popular Health Insurance and the
Commission‘s administrative budgets; (ii) reform efforts to shift financing based on affiliation to
one based on the effective administration of entitlements may be hampered by legal limitations, a
lack of capacity and political resistance; (iii) the least developed State Health Systems may not
adequately benefit from the proposed efforts to strengthen the administration of Popular Health
Insurance entitlements; and, (iv) financial management may not fully meet Bank requirements.
In addition, the Popular Health Insurance has been criticized by some Mexican opinion leaders
for its potential effects on informality. With the proposed mitigation measures for these critical
risks and controversial aspects described in Table 4 below, the overall risk rating of the project is
Moderate.
Table 4. Critical Risk Matrix for the Project
Risks Risk Mitigation Measures Risk Rating
with
Mitigation
Project development objective and component results Fiscal pressures created by the
current economic crisis may
prompt reductions in federal
funding of:
The Public Health Insurance,
and
The Commission‘s
administrative budgets.
For the Commission, reductions
may limit its available resources
for advancing the reform
agenda.
Popular Health Insurance is a priority program of the current
administration and its expansion and strengthening is broadly
supported among political parties. The Government recently
amended the GHL, adjusting the insurance premium, which will
allow enrollment of an additional 6 million individuals.
Congress approved the 2010 budget law with a US$1.0 billion
increase for the Popular Health Insurance.
The Commission‘s leadership is highly committed to the
proposed Project. Critical expenditures in its budget would be
protected by the Bank loan. The Commission and the Bank team
have been mobilizing external technical support, including
support from within the Secretariat of Health and the Bank‘s
GET for Health System Strengthening as well as additional
resources from trust funds.
M
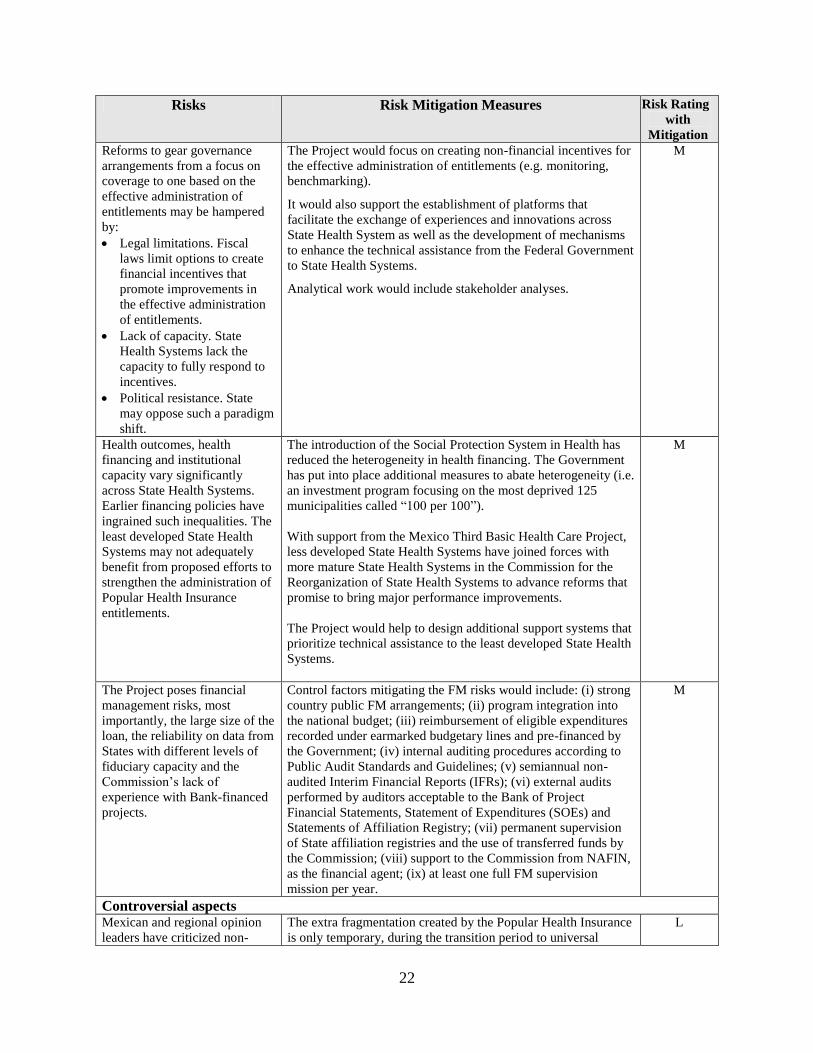
22
Risks Risk Mitigation Measures Risk Rating
with
Mitigation
Reforms to gear governance
arrangements from a focus on
coverage to one based on the
effective administration of
entitlements may be hampered
by:
Legal limitations. Fiscal
laws limit options to create
financial incentives that
promote improvements in
the effective administration
of entitlements.
Lack of capacity. State
Health Systems lack the
capacity to fully respond to
incentives.
Political resistance. State
may oppose such a paradigm
shift.
The Project would focus on creating non-financial incentives for
the effective administration of entitlements (e.g. monitoring,
benchmarking).
It would also support the establishment of platforms that
facilitate the exchange of experiences and innovations across
State Health System as well as the development of mechanisms
to enhance the technical assistance from the Federal Government
to State Health Systems.
Analytical work would include stakeholder analyses.
M
Health outcomes, health
financing and institutional
capacity vary significantly
across State Health Systems.
Earlier financing policies have
ingrained such inequalities. The
least developed State Health
Systems may not adequately
benefit from proposed efforts to
strengthen the administration of
Popular Health Insurance
entitlements.
The introduction of the Social Protection System in Health has
reduced the heterogeneity in health financing. The Government
has put into place additional measures to abate heterogeneity (i.e.
an investment program focusing on the most deprived 125
municipalities called ―100 per 100‖).
With support from the Mexico Third Basic Health Care Project,
less developed State Health Systems have joined forces with
more mature State Health Systems in the Commission for the
Reorganization of State Health Systems to advance reforms that
promise to bring major performance improvements.
The Project would help to design additional support systems that
prioritize technical assistance to the least developed State Health
Systems.
M
The Project poses financial
management risks, most
importantly, the large size of the
loan, the reliability on data from
States with different levels of
fiduciary capacity and the
Commission‘s lack of
experience with Bank-financed
projects.
Control factors mitigating the FM risks would include: (i) strong
country public FM arrangements; (ii) program integration into
the national budget; (iii) reimbursement of eligible expenditures
recorded under earmarked budgetary lines and pre-financed by
the Government; (iv) internal auditing procedures according to
Public Audit Standards and Guidelines; (v) semiannual non-
audited Interim Financial Reports (IFRs); (vi) external audits
performed by auditors acceptable to the Bank of Project
Financial Statements, Statement of Expenditures (SOEs) and
Statements of Affiliation Registry; (vii) permanent supervision
of State affiliation registries and the use of transferred funds by
the Commission; (viii) support to the Commission from NAFIN,
as the financial agent; (ix) at least one full FM supervision
mission per year.
M
Controversial aspects
Mexican and regional opinion
leaders have criticized non-
The extra fragmentation created by the Popular Health Insurance
is only temporary, during the transition period to universal
L
23
Risks Risk Mitigation Measures Risk Rating
with
Mitigation
contributory health insurance
schemes because they further
fragment the health systems as
well as for their potential effects
on informality.
coverage. Afterwards, the Popular Health Insurance will have
simply replaced the financing system of the public health care
service system.
While the argument for labor market effects is conceptually
appealing; it assumes that workers try to maximize income and
benefits by seeking informal employment; and, thus, enjoying
health insurance coverage while avoiding contributions to the
social security schemes. However, there is little evidence
substantiating this assumption and the few observed effects are
small. A Bank study in Mexico showed a significant effect of the
Popular Health Insurance roll-out on contributory health
insurance affiliation from 2004 to 2006 in rural areas only.
Additionally, this effect was small in absolute terms (with a
coverage reduction from 7.1 to 5.8 percent) and almost
negligible when comparing gains in overall insurance coverage.
As part of the ongoing programmatic Mexico Health Analytical
and Advisory Activities, the task team will repeatedly evaluate
the effect.
Overall risk rating Moderate
E. Loan conditions and covenants
45. There are no significant, non-standard conditions for Board presentation, Loan
effectiveness and/or legal covenants applicable to Project implementation.
IV. APPRAISAL SUMMARY
A. Economic and financial analyses
46. Project benefits and costs were weighed using a model and data inputs that produce
rather conservative benefit estimates. This happened mainly for two reasons. First, the model
captures only benefits that result from reductions in mortality. Thus, it does not take into account
the broader benefits to be realized from reductions in morbidity and out-of-pocket expenditures.
Second, the model hinges on the imputed age-specific elasticities of health expenditure and
mortality. For some age-groups, data have only been available from countries that are
approaching the ‗flat-of-the-curve‘. In contrast, at least for a proportion of the population
enrolled into the Popular Health Insurance, the returns from investments in health are much
higher. For example, the elasticities for health expenditure and maternal mortality in developing
countries are significantly higher than those imputed in the model.
47. Despite the conservative approach, sensitivity analysis demonstrated robust and
positive results. A multi-way sensitivity analysis (including different discount rates, which
explain the range in project costs) suggests that the Project would prevent between 163,700 and
167,400 deaths. In monetary terms, avoiding these deaths would translate into gains of US$33.7
billion to US$48.4 billion. These compare favorably to the Project costs of US$22.8 billion to

24
US$24.3 billion with benefit cost ratios of 1.5 to 2.0 and net present values of US$11.0 billion to
US$24.1 billion.
B. Technical
48. For decades, the literature has well established the benefits of public health insurance
(as opposed to being uninsured and without access to national health services) as increasing
access to health services, increasing the likelihood of early diagnosis of disease through a
higher (and appropriate) utilization of health services, and decreasing the risk of mortality.
Most of the literature comes from the US experience with Medicaid and Medicare. In general,
public health insurance coverage is associated with increased access to medical care (Kleinman
et al. 1981; Newacheck 1988; Newacheck 1989; H. E. Freeman et al. 1990; Hafner-Eaton 1993;
Braveman et al. 1993); in contrast, people without insurance delay or forego medical care for
serious symptoms (H. E. Freeman et al. 1987; Aday & Andersen 1984; Hayward 1988;
Weissman et al. 1991; Kleinman et al. 1981; Newacheck 1988b; Newacheck 1989; Braveman et
al. 1993). Furthermore, public health insurance is associated with a higher use of recommended
preventative services (Woolhandler & Himmelstein 1988; Short & Lefkowitz 1992). At the same
time, uninsured people are more likely than those with no insurance to have potentially avoidable
hospitalizations, to be sicker at the time of hospital admission (Billings & Teicholz 1990;
Weissman et al. 1992), to be sicker at the time of hospital admission (Billings & Teicholz 1990;
Weissman & Epstein 1989; Hand et al. 1991), to be more likely to experience in-hospital
(Yergan et al. 1988; Hadley et al. 1991; Young & Cohen 1991) and cancer mortality (Greenberg
et al. 1988), and to be less likely to receive invasive procedures (Weissman & Epstein 1989;
Wenneker et al. 1990). Finally, public health insurance coverage is associated with a decreased
risk of mortality (Franks et al. 1993; Lave et al. 1998; Roetzheim et al. 1999) and loss of
insurance coverage with measurable declines in health (Lurie et al. 1986; Fihn & Wicher 1988).
49. More recent literature shows similar benefits of non-contributory health insurance
schemes in comparison to the limited mandate of national health service systems in LAC
countries (World Bank Forthcoming). For example, the non-contributory health insurance
schemes in Colombia and Mexico have been shown to increase access to and the use of health
services as well as to reduce mortality (Kleinman et al. 1981; Newacheck 1988a; Newacheck
1989; Braveman et al. 1993; Gakidou et al. 2006; Bleich et al. 2007; Hernández-Torres et al.
2008). In addition, there is evidence that they have reduced household expenditures on health
care and the likelihood of suffering from catastrophic and impoverishing health expenditures for
their beneficiaries (Caldwell 1986; Bitrán et al. 2004; Knaul et al. 2005; Cavagnero et al. 2006;
Gakidou et al. 2006; Gaviria et al. 2006; Bleich et al. 2007; Giedion & Villar Uribe 2009; Sosa-
Rubi et al. 2007; Hernández-Torres et al. 2008; Castano & Zambrano 2006; King et al. 2009).
Furthermore, in LAC, public health insurance schemes23
have been particularly good conduits
for protecting the use of health services (Sparrow 2008) and for providing effective risk
protection to their beneficiary populations (M. J. Roberts et al. 2004) especially during times of
crisis (Pablo Gottret et al. Forthcoming).
50. Likewise, the proposed reforms to consolidate the Popular Health Insurance are
supported by ample evidence. The literature supports the proposed reforms to strengthen
23
To the extent they are affordable for the Government

25
performance management to improve service delivery (Méon & Weill 2005). In particular for
human development, monitoring, evaluation and benchmarking have been shown to promote
effective service delivery (Goetz & Jenkins 2002; Andrews & Shah 2003; Schedler 1999; Shah
2005; Anderson et al. 2004; World Bank 2003). Likewise, providing information and raising
awareness of rights and entitlements can improve public service provision (for an overview see
the World Development Report 2004). In health, empowerment of service users has been shown
to promote continuity of care, access and quality of care as well as patient satisfaction
(Halevy-Levin et al. 2008). Finally, establishing a health risk management program is a
promising endeavor. These programs have been implemented in OECD countries across the
globe to reduce the burden of mainly non-communicable diseases and control the costs of health
care (Linden et al. 2003; Blumel & Reinhard Busse 2009; R. Busse 2004; Fireman et al. 2004;
Koppel & Aaviksoo 2007; Miller et al. 2002; Matsuda 2007; Brown et al. 1997; Hofmarcher et
al. 2005). Other studies have demonstrated high levels of acceptance and utilization as well as
the value of early detecting health problems for early treatment (Brown et al. 1997; Hofmarcher
et al. 2005). Moreover, studies have shown reductions in risk factors such as hypertension and
hyperglycemia (Blumel & Reinhard Busse 2009; Fireman et al. 2004; Villagra & Ahmed 2004).
C. Fiduciary
51. Financial Management. Annex 7 documents the results of the Project’s financial
management (FM) assessment
52. The Project’s financial management arrangements including the Commission’s
fiduciary controls for oversight and monitoring of the funds transferred at the State level for
purposes of the program are acceptable to the Bank; the residual financial management risk
is considered moderatre. The Project would make large use of the country public FM systems,
including budgeting, accounting, treasury, internal control and auditing. At the federal level
those systems are strong and acceptable to the Bank. However, the documentation to support
disbursements under component I would rely on data from States, with different levels of
financial management capacity. Therefore, the Commission provides strong oversight,
monitoring controls and supervision procedures for the implementation of the Popular Health
Insurance by States. The Bank appraised these mitigating measures as part of the assessment of
the Project‘s financial management arrangements and considers them acceptable. More
specifically, the Bank team is comfortable that these measures are adequate to assure that States
use Project funds for the intended purposes. The mitigating controls include but are not limited
to: (i) monthly internal validation and reconciliation processes of State affiliation registries (ii)
permanent supervision of the use of Popular Health Insurance funds, including on-site visits by
the Commission. The Popular Health Insurance is also subject to local internal control and
auditing practices conducted by State internal control offices and local supreme audit institution;
furthermore, it is audited by the Auditor General‘s office. In addition, the Project‘s annual
financial audit would include a technical component to assess and review affiliation registries at
the State level, including the compliance with operational rules. For a detailed description of the
financial management assessment, please see Annex 7.
26
53. Procurement. Annex 8 documents the results of the Project’s procurement assessment.
54. The majority of the Loan resources would be transferred to States to finance the eligible
federal social contributions to the premium of the Popular Health Insurance (Component I), for
which no procurement activities would be necessary. The Bank carried out an assessment of the
Commission‘s capacity to manage procurement processes under component II of the Project. The
assessment included the review of the organizational structure for Project implementation and
the interaction and skills of staff responsible for procurement. It found the capacity in general to
be satisfactory, however, noted the lack of experience with Bank-financed projects. As
mitigation measures, it recommends the training of staff carrying out procurement activities in
the use of Bank guidelines and standard bidding documents as well as in the use of the
procurement plan execution system SEPA prior to the initiation of the procurement processes.
Considering that the Project‘s procurement activities are not considered to be complex, the
assessment concluded that the procurement risk is MODERATE.
D. Social
55. As presented earlier, the Social Protection System in Health and specifically the
Popular Health Insurance has significantly improved the performance of the health system.
Levels of public spending have been amplified, the equality of distribution of these resources
improved, the effective health service coverage has expanded and the incidence of catastrophic
health payments has been reduced. Popular Health Insurance beneficiaries are also satisfied with
both the insurance itself and the health services provided through it.
56. Cultural and social factors over the past decades have put women in Mexico at a
disadvantage for having contributory social security, including corresponding health
insurance and access to quality health services. Through a combination of cultural and
demographic changes, Mexican women increasingly have become the heads of the households,
while continuing to play the role of the primary care-taker of their families and largely working
in the informal sector. As such, they often lack the social security benefits that come with formal
work and rely heavily on the public sector for them. As the public health insurance for people
without contributory social security, the Popular Health Insurance plays an important role in the
social protection of women‘s health, in particular, through improved access to health services.
Moreover, the SPSS has given pregnant women, mothers and children priority access to health
care services through a Strategy for Healthy Pregnancies (Estrategia de Embarazo Saludable)
and the Health Insurance for a New Generation (Seguro Médico para una Nueva Generación) as
well as priority enrollment to the Popular Health Insurance.
57. The health status of indigenous peoples has been historically poor; furthermore,
indigenous peoples have not benefited from the introduction of the Popular Health Insurance
in the same way as other populations lacking contributory social security. The indigenous
population in Mexico constitutes 10 percent of the total population and can be broken down into
62 different ethnic groups. Indigenous Peoples have had a poorer health than the general
population; for example, infant and maternal mortality rates are two to three times higher than in
the general population. In the first phases of scaling up affiliation, the Popular Health Insurance
prioritized families in the first and second income deciles. Despite this, the total affiliation of the

27
indigenous peoples24
still lagged behind that of the general population. Moreover, the Popular
Health Insurance is still not accessible to a large portion of the indigenous population.
58. The proposed Project is expected to have a positive impact on indigenous peoples;
however, the Popular Health Insurance faces cultural, geographic and institutional barriers to
enrolling them. First, indigenous peoples have difficulties affiliating because of language
barriers – especially elderly and poor non-Spanish speakers. Second, they have a limited
understanding of the concept of insurance. Third, they lack of knowledge on how the system
works. Fourth, they often lack the required identification documents for affiliation. Fifth, they
commonly reside in remote areas with limited or no access to non-traditional health care services
(see paragraph 12 of Annex 1). Sixth, State promoters often do not have the means to travel to
indigenous communities to enroll them to the Popular Health Insurance. Finally, the States have
faced a financial incentive to enroll primarily population groups other than indigenous peoples.
States receive health care funding from the Federal Government for implementing both the
Popular Health Insurance and the Oportunidades program. These programs, however, overlap by
providing health services to the poor; furthermore, by law, States only receive federal funds for
either the subsidy for the health component of the Oportunidades program or the Popular Health
Insurance Premium. Since the Oportunidades subsidy is much less than the Popular Health
Insurance premium, State Health Systems can maximize federal transfers by affiliating
population groups other than Oportunidades beneficiaries into the Popular Health Insurance. As
indigenous constitute approximately 80 percent of Oportunidades beneficiaries, these financing
arrangements may have contributed to the sluggish enrollment of Oportunidades beneficiaries
and Indigenous Peoples into the Popular Health Insurance. However, as the affiliation to Popular
Health Insurance nears complete coverage, this incentive will become less powerful. State Health
Systems will have to increasingly focus on the enrollment of Oportunidades beneficiaries to
achieve the ambitious affiliation targets for the coming years and may even give them priority as
the enrollment of Oportunidades beneficiaries are streamlined (the regulatory framework allows
for the group enrollment of Oportunidades beneficiaries based on program databases).
E. Environment
59. The proposed Project would have no potentially adverse environmental effects;
accordingly, it has been classified as Environmental Category C and it would not trigger the
Bank’s environmental safeguard policy (OP/BP 4.01). The Project would finance the social
contribution to the premium of the Popular Health Insurance; furthermore, it would finance
technical assistance to strengthen the capacity of the Commission and State Health Systems to
enhance performance management and support to States in preparing and carrying out reforms in
the administration of the Popular Health Insurance, improve knowledge of eligible beneficiaries
about entitlements, strengthen health risk management, and provide effective project
coordination and management. As such, the Project would not finance the rehabilitation,
refurbishment or construction of health facilities; furthermore, it would not directly finance the
provision of health services.
24
Popular Health Insurance does not identify their beneficiaries by their specific ethnicity but by whether or not they
consider themselves to be indigenous.

28
F. Safeguard policies
60. As the proposed Project is expected to have a positive impact on indigenous peoples, it
triggers the Bank’s social safeguard policy for Indigenous Peoples (OP/BP 4.10). As mandated
by OP/BP 4.10, the Borrower has prepared an Indigenous Peoples Plan (IPP) to ensure that
indigenous peoples benefit from the Project in a culturally appropriate manner. The IPP has the
following three main objectives. The first objective is to propose a participation strategy that
addresses the barriers identified in the social assessment. This objective has two strategic activity
areas to be carried out during Project implementation, in order to i) promote the enrollment of
indigenous peoples in a way that is compatible with their socio-economic and cultural
characteristics; and (ii) raise their awareness about the importance of health insurance as well as
the rights to which they are entitled as beneficiaries to the Popular Health Insurance. The second
objective is to strengthen the capacity of the Commission: (i) to monitor the affiliation of
indigenous peoples to the Popular Health Insurance as it is scaled up; (ii) to monitor the delivery
and accreditation of health services in priority indigenous localities (as defined by the CDI) and
rural areas; (iii) to monitor indigenous peoples‘ satisfaction with the Popular Health Insurance,
incorporating indigenous localities in its semi-annual user satisfaction surveys; and (iv) to
improve the SPSS‘s information system by disaggregating data by gender and ethnicity. The
third objective is to strengthen the capacity of the State Health Systems to support the
implementation of the activities laid out in the IPP. The strategy laid out in the IPP is completed.
It incorporates recommendations from the Commission for Indigenous Development (CDI).
Consultations on the IPP took place in the States of Yucatán, Oaxaca, Chiapas and Guerrero
between December 17 and February 7, 2010. The IPP was disclosed on the Commission‘s
webpage in Spanish and in the Bank‘s InfoShop in English on February 17, 2010.
61. The proposed Project would not finance any infrastructure projects or any other
activities that require resettlements; accordingly, it would not trigger the Bank’s involuntary
resettlement safeguard policy (OP/BP 4.12).
Safeguard Policies Triggered by the Project Yes No
Environmental Assessment (OP/BP 4.01) [ ] [X]
Natural Habitats (OP/BP 4.04) [ ] [X]
Pest Management (OP 4.09) [ ] [X]
Physical Cultural Resources (OP/BP 4.11) [ ] [X]
Involuntary Resettlement (OP/BP 4.12) [ ] [X]
Indigenous Peoples (OP/BP 4.10) [X] [ ]
Forests (OP/BP 4.36) [ ] [X]
Safety of Dams (OP/BP 4.37) [ ] [X]
Projects in Disputed Areas (OP/BP 7.60)* [ ] [X]
Projects on International Waterways (OP/BP 7.50) [ ] [X]
* By supporting the proposed Project, the Bank does not intend to prejudice the final determination of the parties'
claims on the disputed areas

29
G. Policy Exceptions and Readiness
62. The proposed Project complies with all relevant Bank policies and there are no
outstanding issues with respect to readiness for implementation. The Borrower prepared an
Operational Manual and Procurement Plan acceptable to the Bank. Key Project staff is in place.
As common practice in Mexico, the Contrato de Mandato governing the cooperation between
the Federal Secretariat of Finance, the Federal Secretariat of Health and NAFIN would be signed
prior to Project effectiveness.

30
Annex 1: Country and Sector or Program Background
MEXICO: Social Protection System in Health
Trends in socio-economic development
1. Mexico, a member of the Organization for Economic Cooperation and Development
(OECD), has experienced modest economic growth over the past two decades. Mexico joined
the OECD in 1994, exhibiting the robustness of its macroeconomic policy framework, soundness
of its financial system and the consistence of its structural policies across product, labor and
financial markets to promote rapid convergence of its per-capita income toward OECD levels.
Between 1990 and 2008, it experienced economic growth at an average annual rate of 3.1
percent of the GDP.25
Today, its GDP per year exceeds a trillion dollars, making it the 11th
largest economy in the world.26
Similarly, it‘s GDP per-capita (PPP) has grown at an average
annual rate of 2.17 between 1990 and 2008. At US$14,932 today, Mexico has the largest average
GDP per-capita (PPP) in Latin America 27
and 46th
in the world.28
2. However, today, the country’s economy is facing several challenges. Despite a strong
track record of sound macroeconomic management and stable economic conditions over the last
several years,29
the Mexican economy stands out as the country in the region that has been most
affected by the global financial crisis. Economic activity declined by 6.5 percent in 200930
(see
Figure A1.1). The Mexican economy has been affected in several ways: through weaker external
demand (the United States economy is the destination for more than 80 percent of Mexican
merchandise exports); lower workers‘ remittances; falling oil production and prices; higher
external borrowing costs; and reduced access to external finance. In addition, the Government
and the Bank estimate that the macroeconomic impact of the A/H1N1 influenza epidemic ranged
from 0.3 to 0.8 percent of the GDP through reduced internal demand and tourism, further
weakening the country‘s macroeconomic situation (SHCP 2009). As consequences of all this, in
the last quarter of 2009 unemployment reached 5.3 percent (up from 4.3 percent in 2008),
informality reached 28.3 percent (up from 27.0 percent in 2008) and the Government is facing
fiscal pressures due to a projected shortfall in fiscal revenue for 2010 of 2.9 percent of GDP (374
billion pesos), compared with the budget approved for 2009. For 2010, the Bank projects a
modest rebound in GDP growth of 4.0 percent.
25
WDI and GFI 2009, GDP Constant 2005 International dollars 26
IMF, World Economic Outlook Database, 2009 for GDP, 2009 for GDP 27
IMF, Report April 2009. 28
Data refer to the year 2008. Total GDP 2008 & Population 2008, World Development Indicators database, World
Bank, September 15, 2009. Note: Per capita values were obtained by dividing the Total GDP data by the Population
data. 29
Mexico‘s GDP growth averaged 3.8 percent during 2004-2007 and the economy enjoyed a stable currency,
inflation of 3.8 percent in 2007, low levels of external indebtedness as a share of GDP, declining public debt ratios
and a sovereign credit rating two notches above the lowest investment grade. 30
INEGI, Press Release, Febrero 22, 2010.
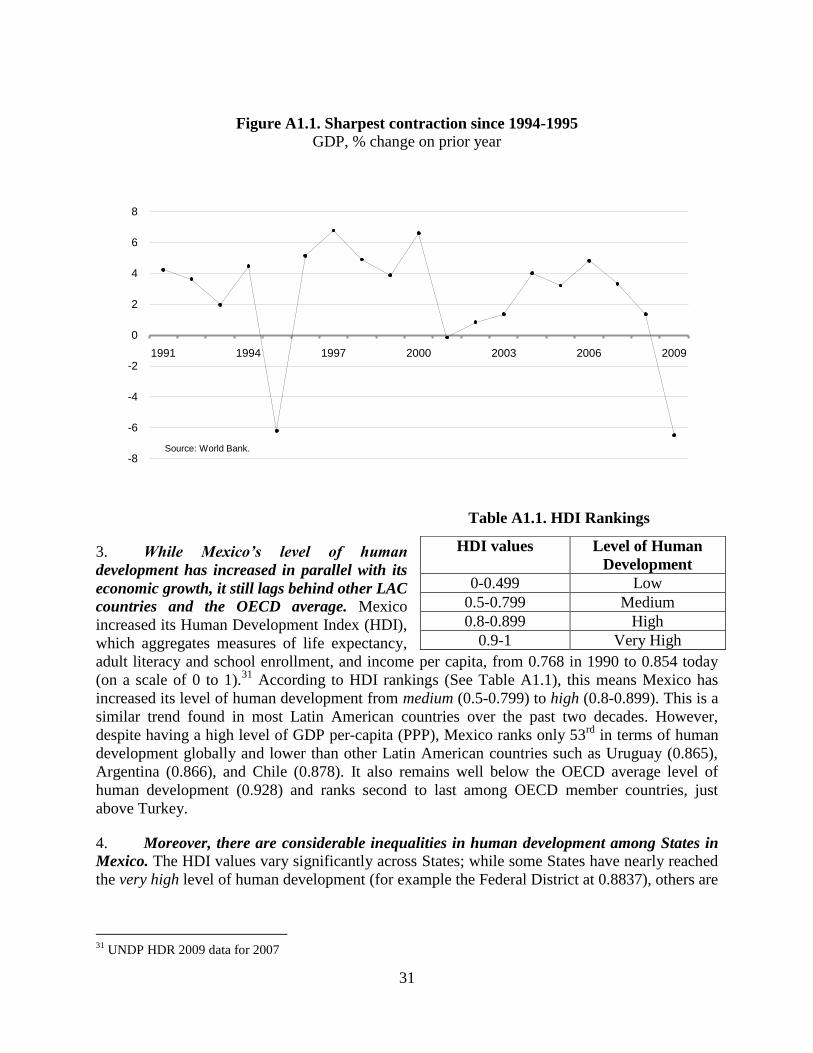
31
Figure A1.1. Sharpest contraction since 1994-1995
GDP, % change on prior year
Table A1.1. HDI Rankings
3. While Mexico’s level of human
development has increased in parallel with its
economic growth, it still lags behind other LAC
countries and the OECD average. Mexico
increased its Human Development Index (HDI),
which aggregates measures of life expectancy,
adult literacy and school enrollment, and income per capita, from 0.768 in 1990 to 0.854 today
(on a scale of 0 to 1).31
According to HDI rankings (See Table A1.1), this means Mexico has
increased its level of human development from medium (0.5-0.799) to high (0.8-0.899). This is a
similar trend found in most Latin American countries over the past two decades. However,
despite having a high level of GDP per-capita (PPP), Mexico ranks only 53rd
in terms of human
development globally and lower than other Latin American countries such as Uruguay (0.865),
Argentina (0.866), and Chile (0.878). It also remains well below the OECD average level of
human development (0.928) and ranks second to last among OECD member countries, just
above Turkey.
4. Moreover, there are considerable inequalities in human development among States in
Mexico. The HDI values vary significantly across States; while some States have nearly reached
the very high level of human development (for example the Federal District at 0.8837), others are
31
UNDP HDR 2009 data for 2007
-8
-6
-4
-2
0
2
4
6
8
1991 1994 1997 2000 2003 2006 2009
Source: World Bank.
HDI values Level of Human
Development
0-0.499 Low
0.5-0.799 Medium
0.8-0.899 High
0.9-1 Very High

32
only at the medium level (for example Chiapas at 0.7185).32
This is a large spread over the HDI
spectrum, representing significant human development inequalities across States in Mexico.
5. Committed to improving inequalities in human development across the States, the
Calderón Administration established Strategy 100 x 100 as a priority program. Strategy 100 x
100 aims to comprehensively change the lagging conditions in the 100 municipalities with the
smallest HDI in Mexico by improving their living conditions and increasing their possibilities for
greater productivity and employment. The greatest challenge that these communities face is the
dispersion of the population, together with the absence of infrastructure and the degradation of
natural resources. Strategy 100 x 100 operates in six technical areas including health, which
works with national programs to invest in nutrition, improve sanitation and service delivery
infrastructure. It covers over 1.1 million Mexicans—85 percent of which are indigenous—in
seven States. Since its inception, it has expanded to 125 municipalities.
Health sector issues
6. Since the 1990s, Mexico has significantly improved its health outcomes, making it one
of few countries in the world that are on course to achieve the health-related Millennium
Development Goals (MDGs). Countries, such as Mexico, that have agreed (in 2001) to achieve
these goals are expected to reduce under-5 child mortality and infant mortality (MDG 4) by two-
thirds and to reduce maternal mortality (MDG 5) by three-quarters between 1990 and 2015.
Today, Mexico is one of the few countries in the world that is on track to achieve these Goals.
Between 1990 and 2007, Mexico has reduced its under-5 child mortality by over 55 percent from
46 to 21 deaths per 1,000 live births33
; its infant mortality rate by 62 percent from 42 to 16 deaths
per 1,000 live births34
; and, its maternal mortality rate by nearly one-half from 110 deaths to 58
deaths per 100,000 live births.35
Furthermore, these significant advances in health outcomes in
the country have increased life expectancy at birth from 71 years to 75 years, during the same
period.36
7. However, with increasing rates of non-communicable diseases, the country is now
facing a “dual burden of disease.” Continuous achievements in health outcomes have resulted
in what is commonly referred to as the ‗dual burden of disease‘; this phenomenon is also seen in
many highly developed nations. At the same time as the extreme poor and other marginalized
groups continue to be plagued by high maternal and child mortality—mainly from
communicable diseases and perinatal conditions—an aging population and unhealthy life-styles
produce a rapidly growing population segment that is increasingly suffering from non-
communicable diseases, such as diabetes and cancer. Today, 16 percent of Mexico‘s global
burden of disease is due to communicable diseases while 72 percent is due to non-communicable
diseases.37
32
Values from the Informe sobre Desarrollo Humano Mexico 2006-7. 33
UNDP 2009 34
World Bank HNPStats, 1995 and 2007 data (per 1,000 live births). 35
Last figure for 2005 36
WDI 2009. 37
WHO Global Burden of Disease database, estimates for 2004 using age-standardized DALYs, last updated in
February 2009.
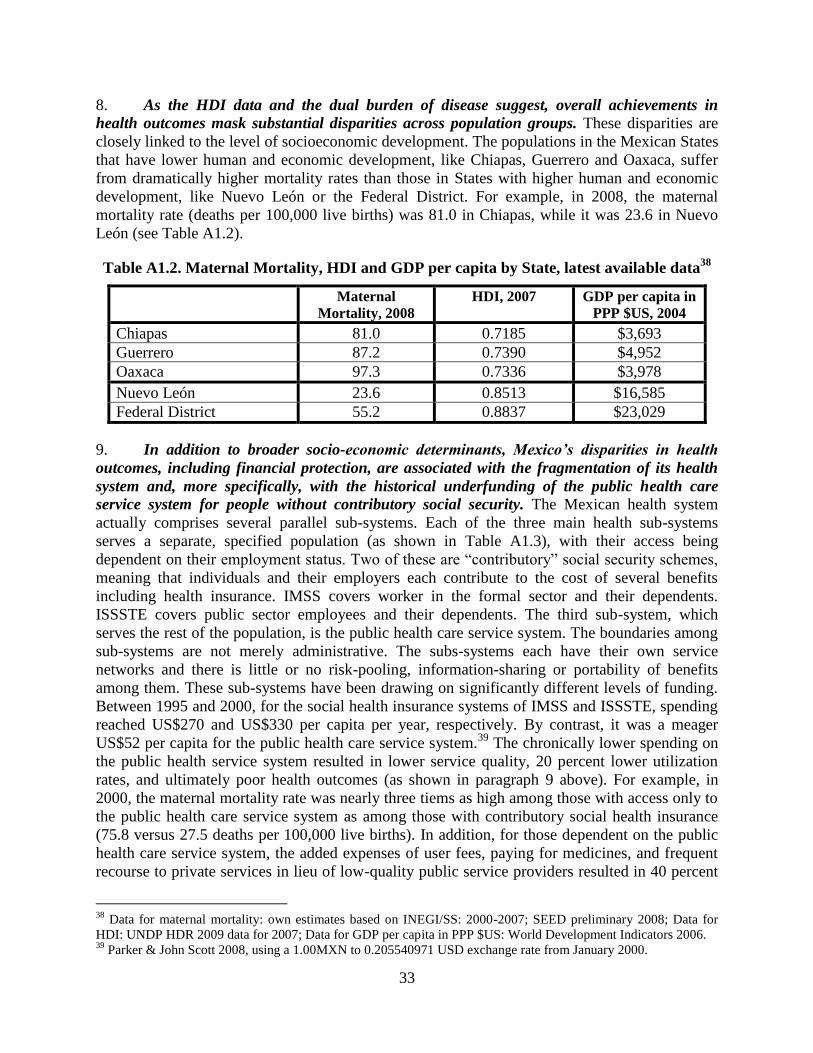
33
8. As the HDI data and the dual burden of disease suggest, overall achievements in
health outcomes mask substantial disparities across population groups. These disparities are
closely linked to the level of socioeconomic development. The populations in the Mexican States
that have lower human and economic development, like Chiapas, Guerrero and Oaxaca, suffer
from dramatically higher mortality rates than those in States with higher human and economic
development, like Nuevo León or the Federal District. For example, in 2008, the maternal
mortality rate (deaths per 100,000 live births) was 81.0 in Chiapas, while it was 23.6 in Nuevo
León (see Table A1.2).
Table A1.2. Maternal Mortality, HDI and GDP per capita by State, latest available data38
Maternal
Mortality, 2008
HDI, 2007 GDP per capita in
PPP $US, 2004
Chiapas 81.0 0.7185 $3,693
Guerrero 87.2 0.7390 $4,952
Oaxaca 97.3 0.7336 $3,978
Nuevo León 23.6 0.8513 $16,585
Federal District 55.2 0.8837 $23,029
9. In addition to broader socio-economic determinants, Mexico’s disparities in health
outcomes, including financial protection, are associated with the fragmentation of its health
system and, more specifically, with the historical underfunding of the public health care
service system for people without contributory social security. The Mexican health system
actually comprises several parallel sub-systems. Each of the three main health sub-systems
serves a separate, specified population (as shown in Table A1.3), with their access being
dependent on their employment status. Two of these are ―contributory‖ social security schemes,
meaning that individuals and their employers each contribute to the cost of several benefits
including health insurance. IMSS covers worker in the formal sector and their dependents.
ISSSTE covers public sector employees and their dependents. The third sub-system, which
serves the rest of the population, is the public health care service system. The boundaries among
sub-systems are not merely administrative. The subs-systems each have their own service
networks and there is little or no risk-pooling, information-sharing or portability of benefits
among them. These sub-systems have been drawing on significantly different levels of funding.
Between 1995 and 2000, for the social health insurance systems of IMSS and ISSSTE, spending
reached US$270 and US$330 per capita per year, respectively. By contrast, it was a meager
US$52 per capita for the public health care service system.39
The chronically lower spending on
the public health service system resulted in lower service quality, 20 percent lower utilization
rates, and ultimately poor health outcomes (as shown in paragraph 9 above). For example, in
2000, the maternal mortality rate was nearly three tiems as high among those with access only to
the public health care service system as among those with contributory social health insurance
(75.8 versus 27.5 deaths per 100,000 live births). In addition, for those dependent on the public
health care service system, the added expenses of user fees, paying for medicines, and frequent
recourse to private services in lieu of low-quality public service providers resulted in 40 percent
38
Data for maternal mortality: own estimates based on INEGI/SS: 2000-2007; SEED preliminary 2008; Data for
HDI: UNDP HDR 2009 data for 2007; Data for GDP per capita in PPP $US: World Development Indicators 2006. 39
Parker & John Scott 2008, using a 1.00MXN to 0.205540971 USD exchange rate from January 2000.
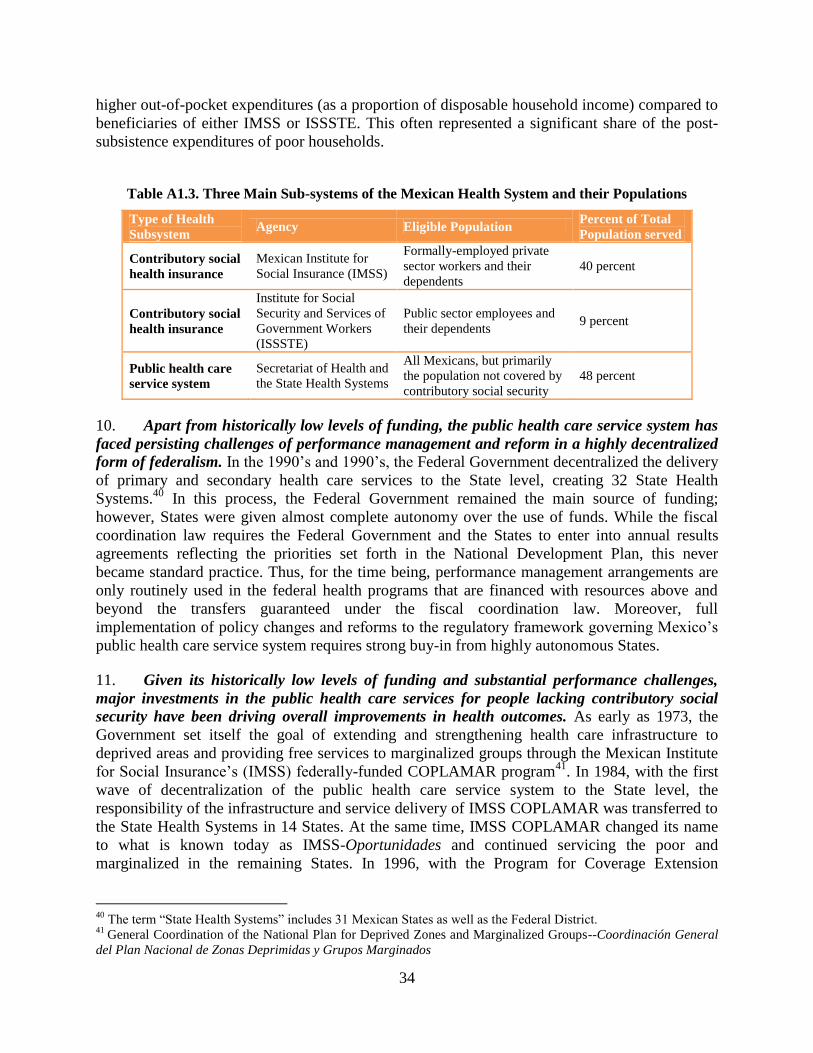
34
higher out-of-pocket expenditures (as a proportion of disposable household income) compared to
beneficiaries of either IMSS or ISSSTE. This often represented a significant share of the post-
subsistence expenditures of poor households.
Table A1.3. Three Main Sub-systems of the Mexican Health System and their Populations
10. Apart from historically low levels of funding, the public health care service system has
faced persisting challenges of performance management and reform in a highly decentralized
form of federalism. In the 1990‘s and 1990‘s, the Federal Government decentralized the delivery
of primary and secondary health care services to the State level, creating 32 State Health
Systems.40
In this process, the Federal Government remained the main source of funding;
however, States were given almost complete autonomy over the use of funds. While the fiscal
coordination law requires the Federal Government and the States to enter into annual results
agreements reflecting the priorities set forth in the National Development Plan, this never
became standard practice. Thus, for the time being, performance management arrangements are
only routinely used in the federal health programs that are financed with resources above and
beyond the transfers guaranteed under the fiscal coordination law. Moreover, full
implementation of policy changes and reforms to the regulatory framework governing Mexico‘s
public health care service system requires strong buy-in from highly autonomous States.
11. Given its historically low levels of funding and substantial performance challenges,
major investments in the public health care services for people lacking contributory social
security have been driving overall improvements in health outcomes. As early as 1973, the
Government set itself the goal of extending and strengthening health care infrastructure to
deprived areas and providing free services to marginalized groups through the Mexican Institute
for Social Insurance‘s (IMSS) federally-funded COPLAMAR program41
. In 1984, with the first
wave of decentralization of the public health care service system to the State level, the
responsibility of the infrastructure and service delivery of IMSS COPLAMAR was transferred to
the State Health Systems in 14 States. At the same time, IMSS COPLAMAR changed its name
to what is known today as IMSS-Oportunidades and continued servicing the poor and
marginalized in the remaining States. In 1996, with the Program for Coverage Extension
40
The term ―State Health Systems‖ includes 31 Mexican States as well as the Federal District. 41
General Coordination of the National Plan for Deprived Zones and Marginalized Groups--Coordinación General
del Plan Nacional de Zonas Deprimidas y Grupos Marginados
Type of Health
Subsystem Agency Eligible Population
Percent of Total
Population served
Contributory social
health insurance
Mexican Institute for
Social Insurance (IMSS)
Formally-employed private
sector workers and their
dependents
40 percent
Contributory social
health insurance
Institute for Social
Security and Services of
Government Workers
(ISSSTE)
Public sector employees and
their dependents 9 percent
Public health care
service system
Secretariat of Health and
the State Health Systems
All Mexicans, but primarily
the population not covered by
contributory social security
48 percent

35
(PAC)—formerly known as the PASSPA42
in its first phase—, the Secretariat of Health took
another major step towards increasing the geographic coverage of health services through the
public health care service system, while also providing the population with a basic package of
health services with 34 low-cost, high-impact community-based and preventative personal care
interventions. Overall, the PASSPA increased the physical infrastructure for services to the poor
and marginalized by 12 percent in the pilot States (Gómez-Dantés et al. 1999). The PAC
extended the basic package of health services to 10.9 million of the 11.4 million target rural
population, covering over 42,900 rural localities in 19 States.43
To reach this number of
beneficiaries, 613 mobile health units (up from 125) were mobilized for the large number of
communities with 500 or less families and without any other type of health unit. Today, IMSS-
Oportunidades covers approximately 5 million families; that is, 20 percent of the total Mexican
population. Together, IMSS-Oportunidades and the Secretariat of Health, provide health service
coverage to 89.2 percent of the rural population, with 29.3 percent of the total managed by
IMSS-Oportundades and 73.0 percent by the public health care service system (García Lopez
2009). Furthermore, Mexico made great efforts to scale up disease-specific programs for
communicable diseases, which typically affect the poor disproportionately; for example,
vaccination programs, oral rehydration therapy, micronutrient supplementation and anti-
helminthic therapy.
12. Complementary to these health programs, the Government implemented the
Conditional Cash Transfer Program, Oportunidades. Oportunidades was established in
response to the severe economic crisis and devaluation of the Mexican peso in 1995. It is a
conditional cash transfer program which disburses cash transfers (grants) to families, conditional
on compliance with certain requirements, including that all household members visit health
centers at least twice a year (more frequently for pregnant women, newborns and children under
24 months and that an adult member of the family attends a monthly health information
workshop. Oportunidades targets poor families using a combination of geographical targeting
and a proxy-means test instrument. Today, it provides support to more than 5.2 million families
(approximately 20 percent of Mexico‘s population) including 60 percent of households in the
bottom decile and 30 percent in the second lowest decile of household consumption. The
program also benefits a much larger percentage of the population in indigenous than in non-
indigenous municipalities, reflecting the higher incidence of poverty in these localities. A wide
body of impact evaluations has demonstrated the program‘s large and significant impact on
health, nutrition and education indicators.
13. To further invest in the health of people without contributory social security and to
reduce their persistently high out-of-pocket expenditures on health care, in 2003 Mexico
decided to transform the public health care service system into a public health insurance
system. Historically, policymakers assumed that inequalities across health sub-systems were only
a transitional problem, as they expected the formal labor market to expand and automatically
make more people eligible for contributory social health insurance. However, in Mexico, as in
other Latin American countries, this process has stalled. For example, between 1996 and 2006,
42
Health Service Assistanca Program for the Open Population—Programa de Apoyo a los Servicios de Salud para
la Población Abierta 43
Campeche, Chihuahua, Chiapas, Durango,
Guanajuato, Guerrero, Hidalgo, Jalisco, Estado de México, Michoacán, Nayarit, Oaxaca, Puebla, Querétaro, San
Luis Potosí, Sinaloa, Veracruz, Yucatán y Zacatecas
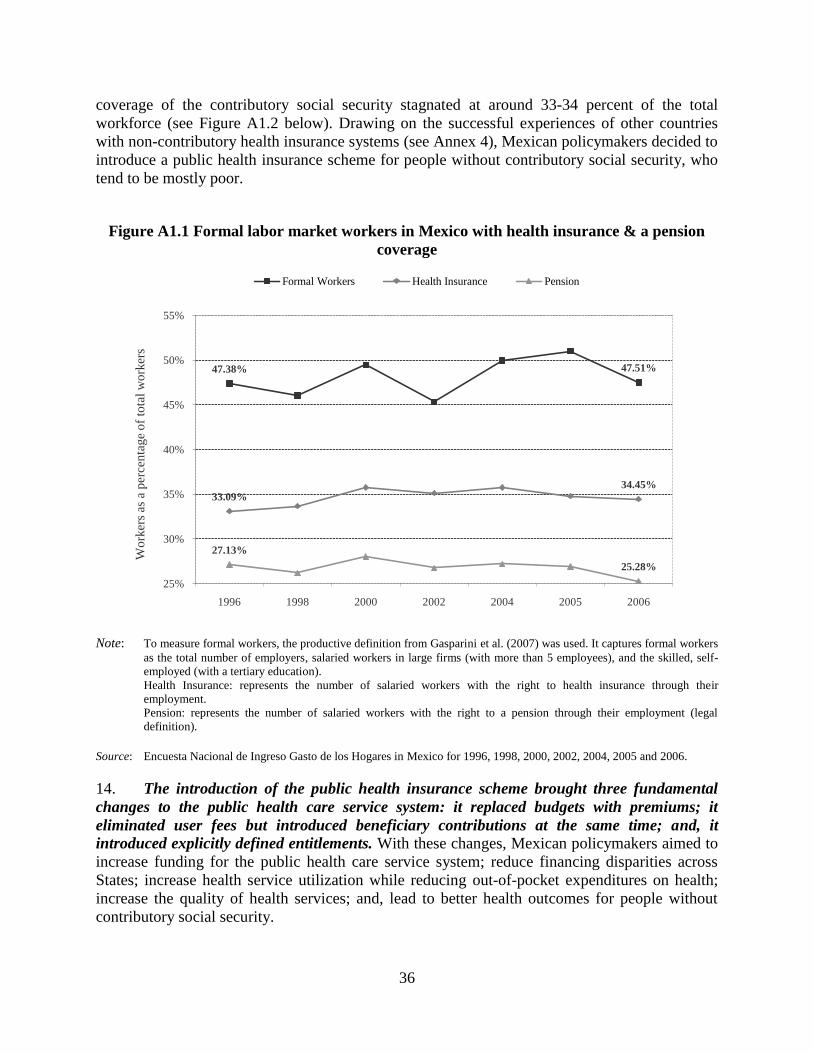
36
coverage of the contributory social security stagnated at around 33-34 percent of the total
workforce (see Figure A1.2 below). Drawing on the successful experiences of other countries
with non-contributory health insurance systems (see Annex 4), Mexican policymakers decided to
introduce a public health insurance scheme for people without contributory social security, who
tend to be mostly poor.
Figure A1.1 Formal labor market workers in Mexico with health insurance & a pension
coverage
Note: To measure formal workers, the productive definition from Gasparini et al. (2007) was used. It captures formal workers
as the total number of employers, salaried workers in large firms (with more than 5 employees), and the skilled, self-
employed (with a tertiary education).
Health Insurance: represents the number of salaried workers with the right to health insurance through their
employment.
Pension: represents the number of salaried workers with the right to a pension through their employment (legal
definition).
Source: Encuesta Nacional de Ingreso Gasto de los Hogares in Mexico for 1996, 1998, 2000, 2002, 2004, 2005 and 2006.
14. The introduction of the public health insurance scheme brought three fundamental
changes to the public health care service system: it replaced budgets with premiums; it
eliminated user fees but introduced beneficiary contributions at the same time; and, it
introduced explicitly defined entitlements. With these changes, Mexican policymakers aimed to
increase funding for the public health care service system; reduce financing disparities across
States; increase health service utilization while reducing out-of-pocket expenditures on health;
increase the quality of health services; and, lead to better health outcomes for people without
contributory social security.
47.38% 47.51%
33.09%
34.45%
27.13%
25.28%
25%
30%
35%
40%
45%
50%
55%
1996 1998 2000 2002 2004 2005 2006
Wo
rker
s as
a p
erce
nta
ge
of
tota
l w
ork
ers
Formal Workers Health Insurance Pension

37
15. Replacing budgets with premiums: Prior to the reform, the Federal Government set the
federal budget envelope for the financing of State Health Systems based on expenditures in the
previous year adjusted for inflation. It determined allocations to States based on the payroll and
infrastructure of each State Health System, with minor adjustments for mortality rates. These
rigid rules perpetuated low-levels of funding for the public health care service system, ingrained
large funding disparities across States, and discouraged quality improvements or innovation.
Today, under the public health insurance, the Federal Government bases the budget envelope and
allocations to the States on an actuarially-calculated premium; that is, a statistically determined
payment based on the expected costs of ensuring, providing, and overseeing a wide range of
services and supporting activities for the enrolled population. In turn, State Health Systems, in
their role as the administrators of the insurance, guarantee health benefits free of charge to those
enrolled to the insurance. The federal budget finances 83 percent of the premium, with States
financing the remaining portion (see Annex 4). These rules linked the funding of State Health
Systems to explicitly defined rights of beneficiaries. The rules were expected to increase the
resource envelop of the public health care service system and to reduce financing disparities
across States.
16. Eliminating user fees and introducing beneficiary contributions: Prior to the reform,
people without contributory social security paid fees to access health services. While these fees
constituted an additional source of revenue, they created barriers to access health services, were
highly regressive and contributed to the high levels of out-of-pocket expenditures and their
impoverishing effects. Today, under the public health insurance, access to services is free at the
time of use. However, beneficiary households pay an annual contribution that States reinvest in
health services or use to build up reserves for the insurance scheme. This contribution is
proportional to each family‘s ability to pay, according to an income assessment. Families
belonging to the two lowest income deciles are exempted from contributing, as are low- and
middle-income families with children younger than five years old.44
The elimination of user fees
combined with the introduction of beneficiary contributions was expected to increase health
service utilization among beneficiaries and reduce out-of-pocket expenditures among
beneficiaries. This promotes both inter-temporal risk pooling and consumption smoothing; two
of the chief objectives of a health insurance.
17. Introducing explicitly defined entitlements: Prior to the reform, the mandate of the
public health care service system was ambiguous. While State Health Systems aimed to provide
all citizens as needed with at least 34 primarily preventive interventions, access to these and
additional services was largely on the availability of financial resources in each State. Moreover,
the system often lacked the resources to ensure service quality, including the completeness of
services. In contrast, the Public Health Insurance explicitly defines beneficiary entitlements,
disclosed in a letter to beneficiary families along with an insurance policy; introduced an
accreditation system for health facilities and established mechanisms such as patient
management, mediation and arbitration systems that ensure that beneficiary rights are enforced.
Along with the increase in resources and the elimination of user fees, these mechanisms were
44
Article 10 Bis 2 of Chapter 5 of the Guidelines for Affiliation, Operation, Integration of the National Beneficiary
Registry and the Determination of Family Contributions to the Social Protection System in Health states that, at the
time of affiliation, those families with at least on family member that is younger than 5 years and that is in at least
income decile III are exempt from contributing to the system.
38
expected to increase the utilization and quality of health services and lead to greater health
outcomes for those without contributory social security, including poor families.
18. The public health insurance, named after a first pilot Seguro Popular (Popular Health
Insurance), has been quickly brought to scale. Since 2004, coverage of the Popular Health
Insurance has rapidly expanded to eligible beneficiaries (adding on average approximately 10
percent of the target population each year and in some years close to the maximum annual rate of
14.3 percent set forth in the General Health Law) (Knaul et al. 2005). At the end of 2009, there
are more than 31 million individuals enrolled, more than half of the approximately 48 million
eligible individuals.45
Likewise, the benefits covered by the Popular Health Insurance have
expanded significantly, from 76 health interventions at its inception to 266 interventions today.
Thus, the Popular Health Insurance is the largest health insurance both in terms of coverage and
benefits for people lacking contributory social security in Latin America (see Table A4.1 in
Annex 4).
19. Even without achieving full universal coverage, Popular Health Insurance has already
improved the performance of the public health care service system. Since its inception, the
Popular Health Insurance has been subject not only to its own internal control and auditing
systems but also to internal and external evaluations (See Annex 3). Most importantly, these
evaluations have demonstrated increases in the spending on the health of people without
contributory social security; the effective removal of financial barriers to access health services;
and, reductions in the likelihood of suffering from catastrophic and impoverishing health
expenditures. Since the inception of the Popular Health Insurance, spending on the health of
people without contributory social security has considerably augmented from, for example,
US$52 per capita per year in 2001 to US$154 per capita per year in 2004 (González-Pier et al.
2007). As such, this increase is beginning to correct the inequalities in public expenditures across
health subsystems. Previously, ratios of public expenditures for ISSSTE and IMSS compared for
those directed to the public health care services changed from 6:1 and 5:1. These ratios have
narrowed with the introduction of the Popular Health Insurance changed from 4:1 and 3:1. In
addition, with the change in resource allocation rules for the public health care service, the
inequalities in public expenditures across State Health Systems have narrowed from 5:1 to 4:1.
Moreover, there is evidence that affiliation to the Popular Health Insurance has removed
financial barriers to access health services, resulting in the higher utilization of inpatient and
outpatient services than for the uninsured (Gakidou et al. 2006; Bleich et al. 2007; Hernández-
Torres et al. 2008). For example, the utilization of services by those who perceived that they
needed health care attention increased from 61 in 2005 to 64 percent in 2006. At the same time,
utilization was significantly higher for Popular Health Insurance affiliates (63.6 percent)
compared to the uninsured (58.3 percent). In turn, the higher utilization rates are expected to
translate into better health over the coming years. Furthermore, affiliation with Popular Health
Insurance has been shown to reduce the likelihood of suffering from catastrophic46
and
impoverishing health expenditures as compared to the uninsured. For example, from 2005 to
2006, the Popular Health Insurance reduced the proportion of those experiencing catastrophic
expenditures by 23 percent (King et al. 2009; Knaul et al. 2005); likewise, the probability of
45
As of September 2009, official data from the National Commission of the Social Protection System in Health. 46
Catastrophic expenditures are defined as out-of-pocket health expenditures greater than 30 percent of post-
subsistence income.

39
incurring catastrophic health expenditures was estimated as 8 percent less for households with
Popular Health Insurance affiliates than for uninsured households (Hernández-Torres et al.
2008).
20. Regional experiences confirm that non-contributory health insurance systems increase
the utilization of health services and reduce out-of-pocket health expenditures for people
without contributory social security. Non-contributory health insurance schemes, like the
Popular Health Insurance, have been shown to play a significant role in achieving universal
health insurance coverage in Latin America and the Caribbean (LAC). Most countries that have
been able to reach high levels of health coverage in LAC have done so by ambitiously expanding
non-contributory health insurance sub-systems. Chile, Colombia and Uruguay are good examples
of this today. Non-contributory health insurance schemes have also been shown to improve
health system performance. For instance, taking the country of Colombia, the non-contributory
health insurance program improved both utilization and financial access to health care services
for its affiliates relative to similar but uninsured individuals: 75 percent of the insured used
health services when needed as compared to 58 percent of the uninsured (Giedion & Villar Uribe
2009); and the probability of incurring catastrophic health expenditures was reduced by 4 percent
for the insured compared to the uninsured (Florez 2008) Additionally, in Colombia, general out-
of-pocket expenditures were reduced with the introduction of the non-contributory health
insurance from 43.7 percent of the total health expenditures before 1993 to less than 8 percent
today.
21. Finally, opinion surveys show that Popular Health Insurance beneficiaries are
satisfied with the scheme. Since 2008 the Congress established the obligation to carry out bi-
annual opinion surveys to assess beneficiaries‘ satisfaction with the Popular Health Insurance.
These surveys have mechanisms to identify perceptions about service providers. According to
the two surveys carried out in 2008, more than 95 percent of affiliates are ―very satisfied‖ or
―relatively satisfied‖ with the Popular Health Insurance; moreover, 95 percent of health service
users are ―very satisfied‖ or ―somewhat satisfied‖ with the health services provided. Regarding
waiting times, the data show improvement over time, with Popular Health Insurance users
waiting 58 minutes on average to receive medical attention.
22. The Popular Health Insurance constitutes the key pillar of Mexico’s Social Protection
System in Health (SPSS) serving people without contributory social security. It is administered
by State Health Systems. In addition to the Popular Health Insurance, the SPSS includes the
Fund for the Protection against Catastrophic Health Expenditures (the Fund), which finances
complex, mostly tertiary health interventions. Moreover, in 2006, the Federal Government
established the Health Insurance for a New Generation, a federal program, which complements
the benefits of the Popular Health Insurance and finances 116 complex maternal and child health
interventions (e.g. open-heart surgery for children). The 32 State Health Systems administer the
Popular Health Insurance; in contrast, the National commission for Social Protection in Health
(the Commission) and the State Health Systems jointly administer the Health Insurance for a
New Generation and the Commission solely administers the Fund. The Commission also
provides the general oversight for the SPSS (CNPSS 2009).
40
Current challenges to the system
23. With seven years of implementation, the Popular Health Insurance has produced
dramatic results for the health and social protection of families without contributory social
security (see paragraph 19 of this Annex); however, at the same time, it faces some important
challenges. These challenges fall into the broad categories of expanding coverage and
effectively administering the entitlements of insurance. Resolving these challenges requires close
cooperation between the Commission and the States, especially for the challenges impacting
system efficiency. As such, the development of further mechanisms to strengthen effective
collaboration will be critical.
24. The current recession calls for an accelerated expansion of Popular Health Insurance
coverage but, at the same time, may hamper it. Policymakers introduced the Popular Health
Insurance with the goal of achieving universal health insurance coverage. They hoped to achieve
this goal by 2010. The current Government reconfirmed the goal of universal health insurance
coverage and, based on earlier affiliation patterns, set the firm target date of 2012. However, the
current crisis calls for an accelerated expansion of the Popular Health Insurance and, at the same
time, poses a threat to the short-term goal of universal coverage. International evidence,
including Mexico‘s experience during the 1994-95 and 2000-01 crises, demonstrates the
importance of securing and, if possible, increasing financial protection in health to safeguard
health gains during downturns. As household income drops, families tend to invest less in their
health. For example, they use health services (and in particular preventive services) less
frequently, and poor and vulnerable households also cut back on food expenditures (A. Ávila &
Shamah Levy 2006). At the same time, however, with informal employment and unemployment
on the rise, fewer people have access to coverage through contributory social security systems or,
which means that more people become dependent on subsidized public health insurance or the
public health care service systems. Moreover, fiscal revenues drop, forcing governments to
reduce their spending across social programs, including subsidized public health insurance
schemes and public health care service systems (Gobierno de México 2008).
25. In late 2009, Mexico took a bold step to substantially expand Popular Health
Insurance coverage during the economic crisis. In December of 2009, the Government
proposed and Congress unanimously approved changes to the General Health Law to refine the
premium system. These changes entailed a reduction of the premium level. This reduction
rectified an earlier design shortcoming; that is, a discrepancy between the information on family
size that fed into the original calculation of the premium (based on 4.3 members per family based
on census data) and the actual average size of beneficiary families (3.1 members per family). The
adjustment of the premium level will allow the enrollment of more than 6 million additional
beneficiaries within current State Health System budgets. Furthermore, the Federal and State
governments are committed to create the necessary fiscal space to provide financial protection in
health to all Mexicans by 2012. As a consequence, the Commission will have to shift its focus
from limiting affiliation to the poor and most vulnerable (which prevailed during the early stages
of scaling-up the Popular Health Insurance) to stimulating demand for affiliation across all
eligible population groups, but while maintaining a focus on hard to reach groups. The changes
introduced into the General Health Law also entailed the switch from a per-family to a per-capita
premium. The originally adopted per-family premium system discriminated against States with
larger average family sizes, which tend to have less developed health systems and lower health
41
budgets. Hence, the switch to a per-capita system will help to further alleviate the financial
imbalances resulting from the introduction of the Popular Health Insurance. At the same time,
however, the affiliation of beneficiaries will remain family-based.
26. The second major challenge is to effectively administer the entitlements of the Popular
Health Insurance. Since its inception, the policies of the Popular Health Insurance have been
geared toward rapid enrollment. Having overcome many obstacles in this endeavor and moving
rapidly towards universal coverage, policy makers have shifted their attention towards the
effective administration of Popular Health Insurance entitlements. Pursuing this shift, the
Commission has identified three priorities for the coming three years: (i) strengthening
performance management while accelerating structural reforms of State Health Systems; (ii)
improving beneficiaries‘ awareness of their rights; and (iii) fostering health promotion and
disease prevention.
27. The design of the Popular Health Insurance foresees fundamental changes to the
organization and management of State Health Systems, including the development of critical
health insurance functions; yet, the implementation of these reforms has been slower than
anticipated. When health service delivery was decentralized to the States in the 1980‘s and
1990‘s, State Health Systems adopted a vertically-integrated organizational model in which the
functions of oversight (stewardship), financing and service provision were centralized in State
ministries of health. With the introduction of the Popular Health Insurance, the regulatory
framework for the State Health Systems stipulates an organizational separation of these
functions, most importantly, the creation of insurance agencies, so-called Regímenes Estatales de
Protección Social en Salud or REPSS. This separation would pave the way for stronger
accountability mechanisms between the insurance agencies and service providers and new
financing arrangements for service providers. These changes would reap further benefits; most
importantly, the possibility to purchase health services from all existing provider networks
(including the networks of IMSS and ISSSTE), which would in turn enhance access to services,
make the use of existing service infrastructure more efficient, and facilitate the portability of
insurance coverage (across State Health Systems). The above would constitute a major step
toward overcoming the fragmentation of the Mexican health system. To date, all States have
established the REPSS, eighteen have joined forces under the Commission for the Organizational
Restructuring of State Health Systems to further advance the organizational and institutional
reforms and two have adopted the strategic purchasing of services. Further progress along this
reform path in all States will depend on the effective transfer of knowledge across States as well
as enhanced technical assistance from the Federal Government.
28. As the organizational reform of State Health Systems advances, refined and stronger
performance management arrangements between the Commission and State Health Systems
can enhance the effective administration of the Popular Health Insurance’s entitlements. As
State Health Systems continue to develop and strengthening REPSS, the onus is on the
Commission to establish incentives that promote the efficient delivery of the entitlements and
specifically the benefit package of the Popular Health Insurance. With the exception of 1.25
percent of the federal solidarity contribution that is dependent on State Health System
performance, financial incentives currently remain geared toward affiliation, not performance
improvements. Furthermore, the regulation of responsibilities remains patchy. This weakness is
compounded by the limited capacity of State Health Systems to comprehensively collect and

42
analyze service delivery data. Hence, limited information flows from State Health Systems as
well as surveys carried out jointly by the Commission and State Health Systems. Also the
capacity of the Commission‘s to comprehensively corroborate information reported by State
Health Systems requires strengthening. As such, the monitoring of the administration of
entitlements remains incomplete, which hampers an effective performance benchmarking of
State Health Systems While a worthy goal in itself, an enhanced performance management
between the Commission and State Health Systems would also goad organizational and
management reforms in State Health Systems.
29. Improving the effective administration of Popular Health Insurance entitlements also
hinges on an improved understanding of these rights by beneficiaries. Entitlements under the
Popular Health Insurance (and for families with small children under the Health Insurance for a
New Generation) include a multitude of health care services, which are defined in detail through
protocols and guidelines. While surveys suggest that the beneficiaries of these insurances are
generally satisfied with the health care services they receive, there is evidence that they have
only a limited knowledge of entitlements.47
This impairs the use of preventive services in
particular, since demand for such services depends on households understanding their
importance; that is, health literacy rather than acute health needs. It also undermines efforts to
protect beneficiary rights through patient management, mediation and arbitration systems.
Efforts to improve the understanding of entitlements and more broadly the benefits of insurance
also have to go beyond current beneficiaries. They have to reach out to the broader target
population of the Popular Health Insurance –that is those without contributory social security-- to
ensure that there is sufficient demand for affiliation. These efforts need to specifically target
indigenous peoples and those living in poverty, which tend to have far below average
educational levels and face other structural barriers to demand affiliation.
30. Effectively administering entitlements will also depend on promoting demand for
health promotion and disease prevention services. Currently, beneficiaries frequently seek care
for curative services. In contrast, demand for interventions that promote health and prevent
diseases—some of the most cost-effective interventions—remains relatively low in Mexico. This
lessens the overall (allocative) efficiency of the system; especially in the context of an increasing
burden of non-communicable diseases. Preventing many non-communicable disease and their
complications is inexpensive, while treating them is costly (and sometimes impossible). Regular
contacts with the health system for disease prevention and health promotion would also allow the
Commission to establish a comprehensive epidemiological profile of the beneficiary population,
which would further help to comprehensively assess the financial risks facing the system.
47
This phenomenon is well documented for non-contributory health insurance schemes in the Latin American and
Caribbean region. Possible explanations include the rather short implementation periods of the schemes, as well as,
the generally low educational attainments of its target populations.
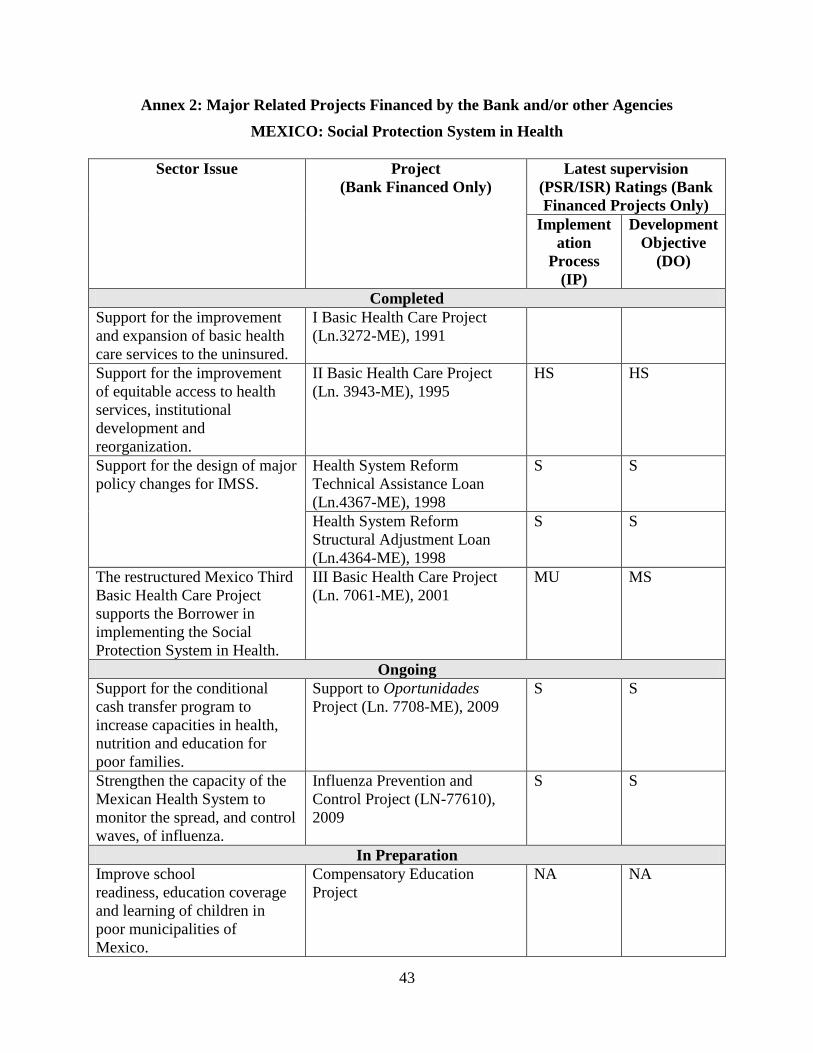
43
Annex 2: Major Related Projects Financed by the Bank and/or other Agencies
MEXICO: Social Protection System in Health
Sector Issue Project
(Bank Financed Only)
Latest supervision
(PSR/ISR) Ratings (Bank
Financed Projects Only)
Implement
ation
Process
(IP)
Development
Objective
(DO)
Completed
Support for the improvement
and expansion of basic health
care services to the uninsured.
I Basic Health Care Project
(Ln.3272-ME), 1991
Support for the improvement
of equitable access to health
services, institutional
development and
reorganization.
II Basic Health Care Project
(Ln. 3943-ME), 1995
HS HS
Support for the design of major
policy changes for IMSS.
Health System Reform
Technical Assistance Loan
(Ln.4367-ME), 1998
S S
Health System Reform
Structural Adjustment Loan
(Ln.4364-ME), 1998
S S
The restructured Mexico Third
Basic Health Care Project
supports the Borrower in
implementing the Social
Protection System in Health.
III Basic Health Care Project
(Ln. 7061-ME), 2001
MU MS
Ongoing
Support for the conditional
cash transfer program to
increase capacities in health,
nutrition and education for
poor families.
Support to Oportunidades
Project (Ln. 7708-ME), 2009
S S
Strengthen the capacity of the
Mexican Health System to
monitor the spread, and control
waves, of influenza.
Influenza Prevention and
Control Project (LN-77610),
2009
S S
In Preparation
Improve school
readiness, education coverage
and learning of children in
poor municipalities of
Mexico.
Compensatory Education
Project
NA NA

44
Sector Issue Project
(Bank Financed Only)
Latest supervision
(PSR/ISR) Ratings (Bank
Financed Projects Only)
Implement
ation
Process
(IP)
Development
Objective
(DO)
Relevant World Bank Projects in the LAC region (Completed, On-going and Planned)
Support for the provision
of health insurance to
mothers and children.
Argentina: Provincial Maternal-
Child Health investment project I,
(Ln. 7225-AR) 2004 (completed )
S S
Argentina: Provincial Maternal-
Child Health investment project II,
(Ln. 7409-AR) 2006 (on-going)
MS U
Support for the
implementation and
advancement in the
Health Reform.
Dominican Republic Health Reform
Support Project I,
(Ln. 7185-DO) 2003 (completed)
MS MS
Dominican Republic Health Reform
Support Project II
(Ln. 7777-DO), 2009 (ongoing)
S S
Support for the expansion
of basic health care
services.
Honduras: Improving Access and
Quality of Basic Health Care
Services Project, 2009 (planned)
NA NA
Support for health system
modernization.
Nicaragua: Health Service Extension
and Modernization Project
(Cr-4050-NI), 2005 (completed)
MS S
Support for improvements
in health service delivery.
Panama Health Equity and
Performance Improvement Project,
(Ln. 7587-PA) 2008 (on-going)
S S
Support for the
implementation of a
Maternal and Child Basic
Health Insurance.
Paraguay: Mother and Child Basic
Health Insurance Project
(Ln. 7333-PY), 2005 (on-going)
MU MU
Ratings: Highly Satisfactory (HS); Moderately Satisfactory (MS); Satisfactory (S); Unsatisfactory (U); Moderately
Unsatisfactory (MU); Non-applicable (NA).
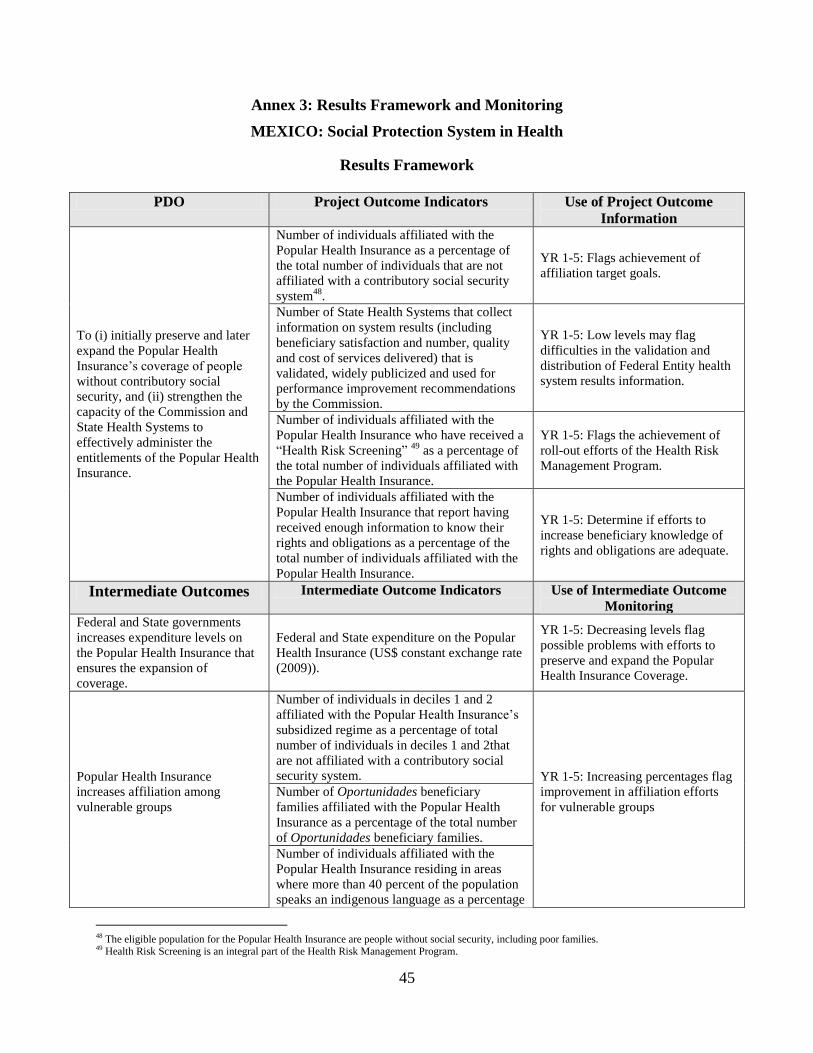
45
Annex 3: Results Framework and Monitoring
MEXICO: Social Protection System in Health
Results Framework
PDO Project Outcome Indicators Use of Project Outcome
Information
To (i) initially preserve and later
expand the Popular Health
Insurance‘s coverage of people
without contributory social
security, and (ii) strengthen the
capacity of the Commission and
State Health Systems to
effectively administer the
entitlements of the Popular Health
Insurance.
Number of individuals affiliated with the
Popular Health Insurance as a percentage of
the total number of individuals that are not
affiliated with a contributory social security
system48
.
YR 1-5: Flags achievement of
affiliation target goals.
Number of State Health Systems that collect
information on system results (including
beneficiary satisfaction and number, quality
and cost of services delivered) that is
validated, widely publicized and used for
performance improvement recommendations
by the Commission.
YR 1-5: Low levels may flag
difficulties in the validation and
distribution of Federal Entity health
system results information.
Number of individuals affiliated with the
Popular Health Insurance who have received a
―Health Risk Screening‖ 49
as a percentage of
the total number of individuals affiliated with
the Popular Health Insurance.
YR 1-5: Flags the achievement of
roll-out efforts of the Health Risk
Management Program.
Number of individuals affiliated with the
Popular Health Insurance that report having
received enough information to know their
rights and obligations as a percentage of the
total number of individuals affiliated with the
Popular Health Insurance.
YR 1-5: Determine if efforts to
increase beneficiary knowledge of
rights and obligations are adequate.
Intermediate Outcomes Intermediate Outcome Indicators Use of Intermediate Outcome
Monitoring
Federal and State governments
increases expenditure levels on
the Popular Health Insurance that
ensures the expansion of
coverage.
Federal and State expenditure on the Popular
Health Insurance (US$ constant exchange rate
(2009)).
YR 1-5: Decreasing levels flag
possible problems with efforts to
preserve and expand the Popular
Health Insurance Coverage.
Popular Health Insurance
increases affiliation among
vulnerable groups
Number of individuals in deciles 1 and 2
affiliated with the Popular Health Insurance‘s
subsidized regime as a percentage of total
number of individuals in deciles 1 and 2that
are not affiliated with a contributory social
security system. YR 1-5: Increasing percentages flag
improvement in affiliation efforts
for vulnerable groups
Number of Oportunidades beneficiary
families affiliated with the Popular Health
Insurance as a percentage of the total number
of Oportunidades beneficiary families.
Number of individuals affiliated with the
Popular Health Insurance residing in areas
where more than 40 percent of the population
speaks an indigenous language as a percentage
48 The eligible population for the Popular Health Insurance are people without social security, including poor families. 49 Health Risk Screening is an integral part of the Health Risk Management Program.
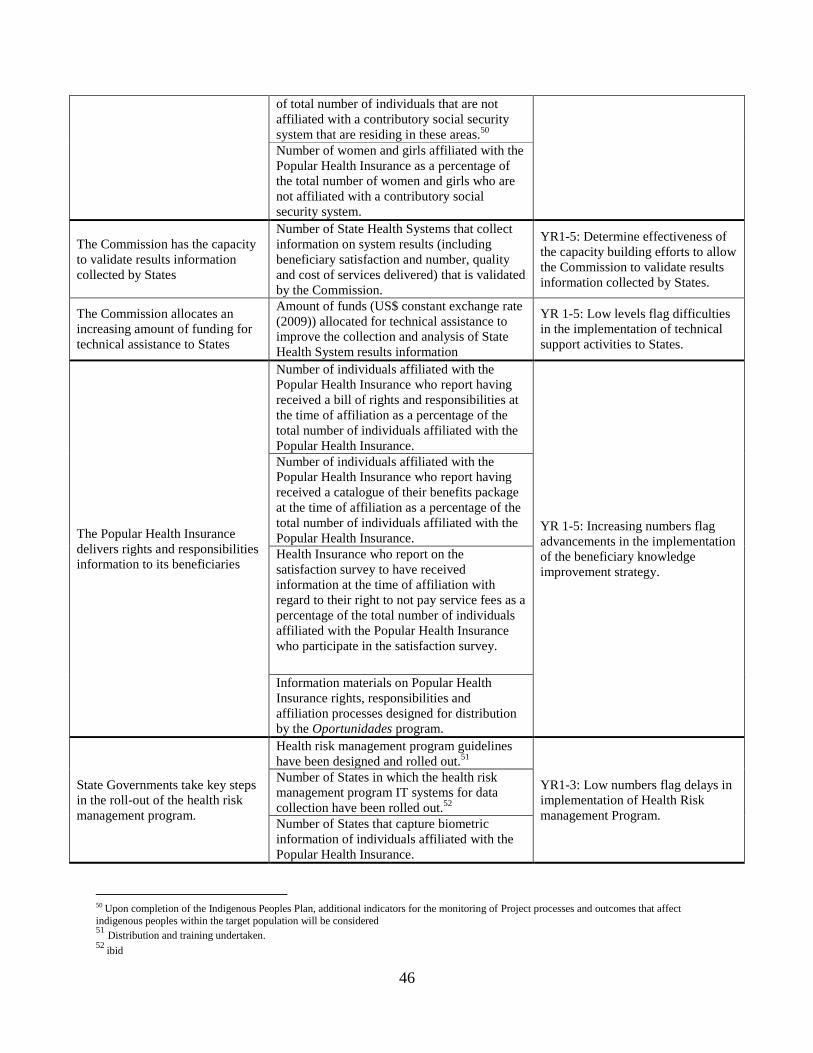
46
of total number of individuals that are not
affiliated with a contributory social security
system that are residing in these areas.50
Number of women and girls affiliated with the
Popular Health Insurance as a percentage of
the total number of women and girls who are
not affiliated with a contributory social
security system.
The Commission has the capacity
to validate results information
collected by States
Number of State Health Systems that collect
information on system results (including
beneficiary satisfaction and number, quality
and cost of services delivered) that is validated
by the Commission.
YR1-5: Determine effectiveness of
the capacity building efforts to allow
the Commission to validate results
information collected by States.
The Commission allocates an
increasing amount of funding for
technical assistance to States
Amount of funds (US$ constant exchange rate
(2009)) allocated for technical assistance to
improve the collection and analysis of State
Health System results information
YR 1-5: Low levels flag difficulties
in the implementation of technical
support activities to States.
The Popular Health Insurance
delivers rights and responsibilities
information to its beneficiaries
Number of individuals affiliated with the
Popular Health Insurance who report having
received a bill of rights and responsibilities at
the time of affiliation as a percentage of the
total number of individuals affiliated with the
Popular Health Insurance.
YR 1-5: Increasing numbers flag
advancements in the implementation
of the beneficiary knowledge
improvement strategy.
Number of individuals affiliated with the
Popular Health Insurance who report having
received a catalogue of their benefits package
at the time of affiliation as a percentage of the
total number of individuals affiliated with the
Popular Health Insurance.
Health Insurance who report on the
satisfaction survey to have received
information at the time of affiliation with
regard to their right to not pay service fees as a
percentage of the total number of individuals
affiliated with the Popular Health Insurance
who participate in the satisfaction survey.
Information materials on Popular Health
Insurance rights, responsibilities and
affiliation processes designed for distribution
by the Oportunidades program.
State Governments take key steps
in the roll-out of the health risk
management program.
Health risk management program guidelines
have been designed and rolled out.51
YR1-3: Low numbers flag delays in
implementation of Health Risk
management Program.
Number of States in which the health risk
management program IT systems for data
collection have been rolled out.52
Number of States that capture biometric
information of individuals affiliated with the
Popular Health Insurance.
50
Upon completion of the Indigenous Peoples Plan, additional indicators for the monitoring of Project processes and outcomes that affect
indigenous peoples within the target population will be considered 51
Distribution and training undertaken.
52 ibid
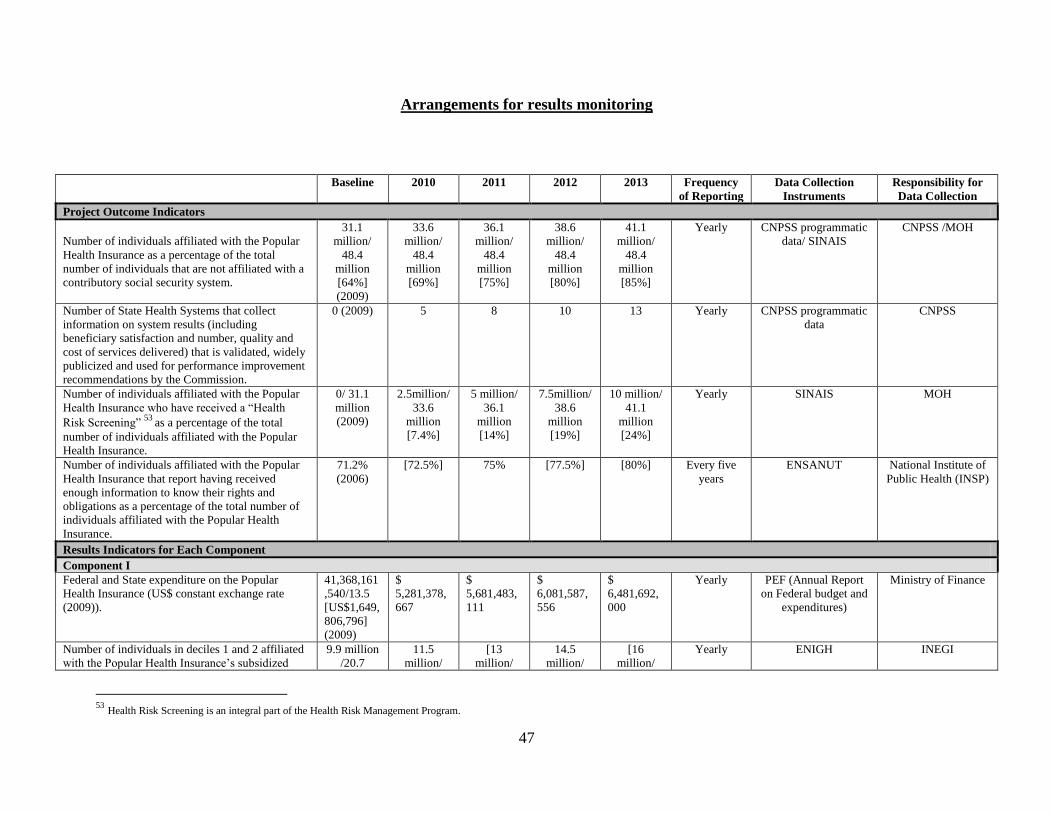
47
Arrangements for results monitoring
Baseline 2010 2011 2012 2013 Frequency
of Reporting
Data Collection
Instruments
Responsibility for
Data Collection
Project Outcome Indicators
Number of individuals affiliated with the Popular
Health Insurance as a percentage of the total
number of individuals that are not affiliated with a
contributory social security system.
31.1
million/
48.4
million
[64%]
(2009)
33.6
million/
48.4
million
[69%]
36.1
million/
48.4
million
[75%]
38.6
million/
48.4
million
[80%]
41.1
million/
48.4
million
[85%]
Yearly CNPSS programmatic
data/ SINAIS
CNPSS /MOH
Number of State Health Systems that collect
information on system results (including
beneficiary satisfaction and number, quality and
cost of services delivered) that is validated, widely
publicized and used for performance improvement
recommendations by the Commission.
0 (2009) 5 8 10 13 Yearly CNPSS programmatic
data
CNPSS
Number of individuals affiliated with the Popular
Health Insurance who have received a ―Health
Risk Screening‖ 53 as a percentage of the total
number of individuals affiliated with the Popular
Health Insurance.
0/ 31.1
million
(2009)
2.5million/
33.6
million
[7.4%]
5 million/
36.1
million
[14%]
7.5million/
38.6
million
[19%]
10 million/
41.1
million
[24%]
Yearly SINAIS MOH
Number of individuals affiliated with the Popular
Health Insurance that report having received
enough information to know their rights and
obligations as a percentage of the total number of
individuals affiliated with the Popular Health
Insurance.
71.2%
(2006)
[72.5%] 75% [77.5%] [80%] Every five
years
ENSANUT National Institute of
Public Health (INSP)
Results Indicators for Each Component
Component I
Federal and State expenditure on the Popular
Health Insurance (US$ constant exchange rate
(2009)).
41,368,161
,540/13.5
[US$1,649,
806,796]
(2009)
$
5,281,378,
667
$
5,681,483,
111
$
6,081,587,
556
$
6,481,692,
000
Yearly PEF (Annual Report
on Federal budget and
expenditures)
Ministry of Finance
Number of individuals in deciles 1 and 2 affiliated
with the Popular Health Insurance‘s subsidized
9.9 million
/20.7
11.5
million/
[13
million/
14.5
million/
[16
million/
Yearly ENIGH INEGI
53
Health Risk Screening is an integral part of the Health Risk Management Program.
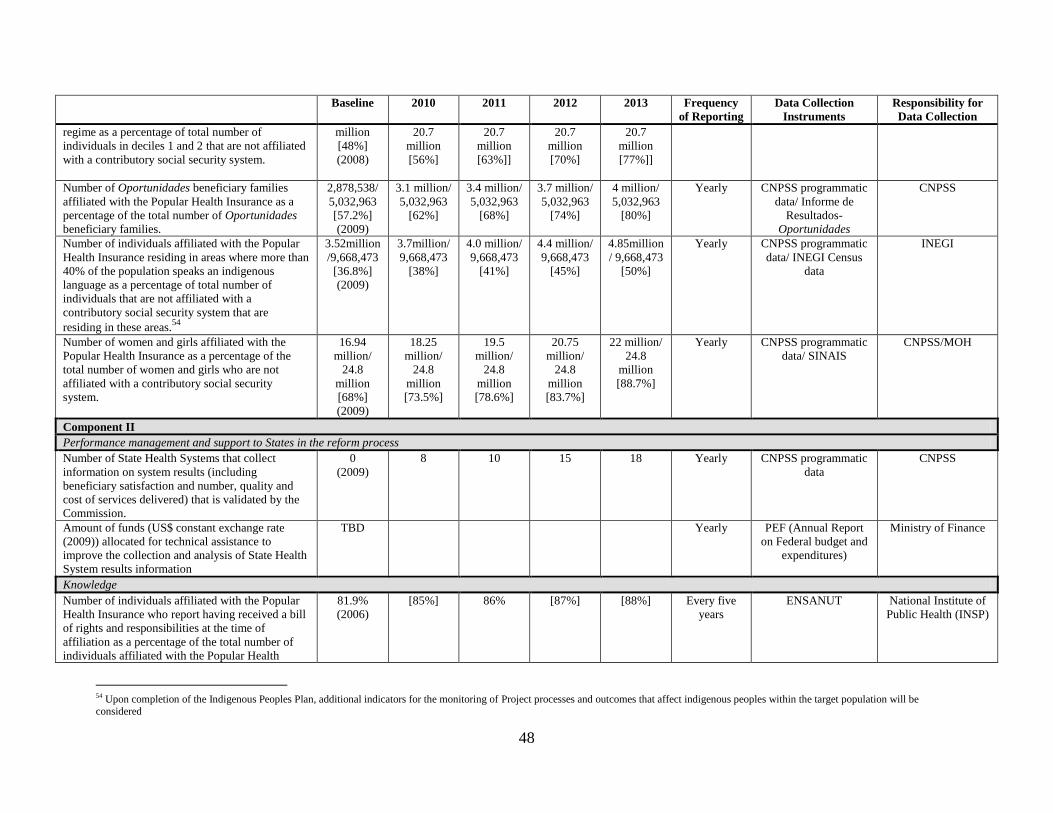
48
Baseline 2010 2011 2012 2013 Frequency
of Reporting
Data Collection
Instruments
Responsibility for
Data Collection
regime as a percentage of total number of
individuals in deciles 1 and 2 that are not affiliated
with a contributory social security system.
million
[48%]
(2008)
20.7
million
[56%]
20.7
million
[63%]]
20.7
million
[70%]
20.7
million
[77%]]
Number of Oportunidades beneficiary families
affiliated with the Popular Health Insurance as a
percentage of the total number of Oportunidades
beneficiary families.
2,878,538/
5,032,963
[57.2%]
(2009)
3.1 million/
5,032,963
[62%]
3.4 million/
5,032,963
[68%]
3.7 million/
5,032,963
[74%]
4 million/
5,032,963
[80%]
Yearly CNPSS programmatic
data/ Informe de
Resultados-
Oportunidades
CNPSS
Number of individuals affiliated with the Popular
Health Insurance residing in areas where more than
40% of the population speaks an indigenous
language as a percentage of total number of
individuals that are not affiliated with a
contributory social security system that are
residing in these areas.54
3.52million
/9,668,473
[36.8%]
(2009)
3.7million/
9,668,473
[38%]
4.0 million/
9,668,473
[41%]
4.4 million/
9,668,473
[45%]
4.85million
/ 9,668,473
[50%]
Yearly CNPSS programmatic
data/ INEGI Census
data
INEGI
Number of women and girls affiliated with the
Popular Health Insurance as a percentage of the
total number of women and girls who are not
affiliated with a contributory social security
system.
16.94
million/
24.8
million
[68%]
(2009)
18.25
million/
24.8
million
[73.5%]
19.5
million/
24.8
million
[78.6%]
20.75
million/
24.8
million
[83.7%]
22 million/
24.8
million
[88.7%]
Yearly CNPSS programmatic
data/ SINAIS
CNPSS/MOH
Component II
Performance management and support to States in the reform process
Number of State Health Systems that collect
information on system results (including
beneficiary satisfaction and number, quality and
cost of services delivered) that is validated by the
Commission.
0
(2009)
8 10 15 18 Yearly CNPSS programmatic
data
CNPSS
Amount of funds (US$ constant exchange rate
(2009)) allocated for technical assistance to
improve the collection and analysis of State Health
System results information
TBD Yearly PEF (Annual Report
on Federal budget and
expenditures)
Ministry of Finance
Knowledge
Number of individuals affiliated with the Popular
Health Insurance who report having received a bill
of rights and responsibilities at the time of
affiliation as a percentage of the total number of
individuals affiliated with the Popular Health
81.9%
(2006)
[85%] 86% [87%] [88%] Every five
years
ENSANUT National Institute of
Public Health (INSP)
54 Upon completion of the Indigenous Peoples Plan, additional indicators for the monitoring of Project processes and outcomes that affect indigenous peoples within the target population will be considered
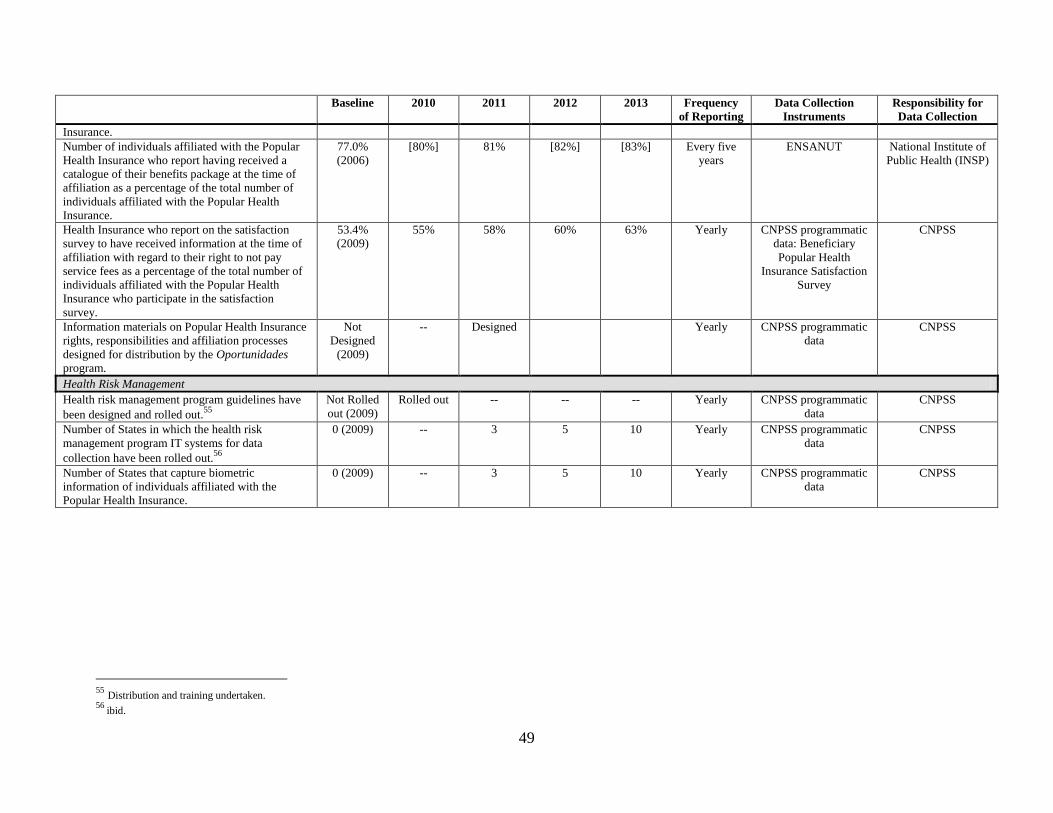
49
Baseline 2010 2011 2012 2013 Frequency
of Reporting
Data Collection
Instruments
Responsibility for
Data Collection
Insurance.
Number of individuals affiliated with the Popular
Health Insurance who report having received a
catalogue of their benefits package at the time of
affiliation as a percentage of the total number of
individuals affiliated with the Popular Health
Insurance.
77.0%
(2006)
[80%] 81% [82%] [83%] Every five
years
ENSANUT National Institute of
Public Health (INSP)
Health Insurance who report on the satisfaction
survey to have received information at the time of
affiliation with regard to their right to not pay
service fees as a percentage of the total number of
individuals affiliated with the Popular Health
Insurance who participate in the satisfaction
survey.
53.4%
(2009)
55% 58% 60% 63% Yearly CNPSS programmatic
data: Beneficiary
Popular Health
Insurance Satisfaction
Survey
CNPSS
Information materials on Popular Health Insurance
rights, responsibilities and affiliation processes
designed for distribution by the Oportunidades
program.
Not
Designed
(2009)
-- Designed Yearly CNPSS programmatic
data
CNPSS
Health Risk Management
Health risk management program guidelines have
been designed and rolled out.55
Not Rolled
out (2009)
Rolled out -- -- -- Yearly CNPSS programmatic
data
CNPSS
Number of States in which the health risk
management program IT systems for data
collection have been rolled out.56
0 (2009) -- 3 5 10 Yearly CNPSS programmatic
data
CNPSS
Number of States that capture biometric
information of individuals affiliated with the
Popular Health Insurance.
0 (2009) -- 3 5 10 Yearly CNPSS programmatic
data
CNPSS
55
Distribution and training undertaken.
56 ibid.
50
1. Project monitoring would primarily draw on Mexico’s monitoring and evaluation
system for the Popular Health Insurance and the health system. Information would flow from
four different sources. First, information would flow from the Commission‘s integrated
supervision tool that tracks and consolidates information on affiliation including data on the
number of beneficiary families and their characteristics (for example, number of family
members, indigenous, female or male head of household, income decile). Second, other
information would flow from surveys, most importantly, a semi-annually survey of beneficiary
satisfaction (carried out by the Commission) and the national health and nutrition and the
national household income and spending surveys. Third, information would flow from the
National Health Information System. Finally, the Commission would report and Bank
supervision missions would validate information on qualitative indicators capturing progress
towards critical milestones in capacity building.
Data sources from which Project monitoring would draw, include:
2. SINAIS: The Secretariat of Health has established the National Health Information
System (SINAIS) for the collection and management of health related information gathered by
separate sub secretariats and States including information gathered by the Social Protection
System in Health. The SINAIS gathers information on three main topic areas: I. Basic Health
Statistics: Service utilization, birthrates, mortality, morbidity and disability statistics. II.
Demographic, economic, social and environmental factors linked to health and III. Physical,
human and financial resources available in the Health System. The SINAIS depends on the
General Directorate of Information in Health and is regulated by the National Health Law and
the Statistical and Geographic Information Law.
3. ENSANUT: The National Health and Nutrition Survey (ENSANUT) is part of a group of
health sector surveys regularly implemented in Mexico; it is designed to collect information
related with the health and nutrition status of the Mexican population, the quality and
responsiveness of Health services, policies and programs that affect health and household
expenditure on health. ENSANUT was first implemented in 2006, in an effort to create
continuity and merge the National Nutrition Surveys from 1988 and 1999 with the National
Health Surveys from 1986, 1994 and 2000. The next survey will take place in 2011. ENSANUT
2006 is the first Health Survey representative at a State level, interviewing 48,304 households
including the measurement of 50,027 individuals‘ serum micronutrient concentration and 90,267
individuals‘ anthropometric measures (questionnaires with incomplete information were not
considered). The data is collected through household and individual questionnaires specific to
three age groups: Children (0 to 9 years old), teenagers (10 to 19 years old) and adults (older
than 20). Additionally, anthropometric measures, blood samples and arterial tension are
analyzed. The implementation, analysis and publication of the ENSANUT are the responsibility
of National Institute of Public Health (INSP).
4. ENIGH: The National Survey on Household Income and Expenditures (ENIGH) collects
data on the income and expenditure of Mexican families. The survey was first implemented in
1984, and since 1992, it has been implemented every two years, with an additional edition in
2005. The last survey took place in 2008, where 35,146 households (27,406 urban and 7,740
rural households) were interviewed over a period of three months through questionnaires
51
covering the following topics: household expenditures, daily expenditures, household business,
and two additional individual questionnaires for children and adults (older and younger than 12
years). Around 85 percent of the questionnaires were completed over the three month period.
The survey is representative at a National level, and also for the following States: Federal
District, México, Guanajuato, Jalisco, Querétaro, Sonora and Yucatán. The ENIGH collects
specific health sector-related information: affiliation to the different health subsystems,
expenditure on medical services, and expenditure on medicines. The implementation, analysis
and publication of the ENIGH is the responsibility of the National Institute of Statistics and
Geography (INEGI).
5. CNPSS Programmatic Data: The Commission uses an integral supervision tool to track
and consolidate information on the Popular Health Insurance, tracking trends in affiliation,
financing and service delivery producing a Results Report twice yearly. Trends in affiliation are
monitored through data on the number of families enrolled and their characteristics (indigenous,
female headed households, income decile, etc.) collected through the affiliation questionnaire
called CECASOEH, as well as the processes and accuracy of the beneficiary lists reported by
each Federal Entity based on this data. Trends in financing are monitored through data on the
amounts transferred, the amounts contributed by the States, and the amounts contributed by
beneficiaries. Service delivery is monitored through information on the availability of medicines,
technology and training of service providers in each Federal Entity. Beneficiary satisfaction
information is collected through surveys twice yearly that represent a selected sample of health
service users in health facilities.
6. PEF Annual Report on Federal Budget and Expenditures: The Ministry of Finance‘s
Under Secretariat of Expenditures collects and reports, on an annual basis, on expenditures as
established in the annual Federal Expenditure Budget (PEF). The information included in these
reports disaggregates expenditures by sectors, States, financing flows and expenditure categories.
7. The Commission would be responsible for the consolidation, analysis and distribution
of information gathered through the national monitoring and evaluation systems as well as its
own monitoring system. The Commission would consolidate information from the various data
sources in the semi-annual Project report. The data sources that would be used for program
monitoring have been in existence for many years producing information that is representative
and reliable. Data would be reported to the Bank directly by the PCU. Reported data would flag
activities for which implementation efforts need to be changed or enhanced. As data collected
begin to show the achievements or lessons in the implementation of the project, these will be
shared within the Commission, with States and within the Bank. Given the reliability of data
sources and the lengthy experience of the Commission in data collection, analysis and
distribution of information, their capacity to monitor the program is reliable.

52
Annex 4: Detailed Project Description
MEXICO: Social Protection System in Health
1. After seven years of implementation, the Popular Health Insurance has produced
dramatic results for the health and social protection of families without contributory social
security. It has significantly augmented the spending on the health of people without
contributory social security from US$52 per capita in 2001 to US$154 per capita in 2004.
Moreover, it has reduced the inequalities in State Health System financing from 5:1 to 4:1. There
is evidence that it has removed financial barriers to access health services, resulting in the higher
utilization of inpatient and outpatient services than the uninsured. In turn, the higher utilization
rates are expected to translate into better health over the coming years. Furthermore, affiliation
with Popular Health Insurance has been shown to reduce the likelihood of suffering from
catastrophic and impoverishing expenditures on health compared to the uninsured.
2. At the same time, the Popular Health Insurance faces some important challenges that
fall into the broad categories of expanding coverage and effectively administering the
entitlements of insurance (see Annex 1 paragraphs 24 to 31). Though revenues have been
falling sharply, the current economic crisis calls for the accelerated expansion of the Popular
Health Insurance to protect the health and finances of those lacking contributory social security,
some of them relying on the system due to the crisis. Moreover, as universal coverage nears,
policy attention has to shift towards the effective administration of Popular Health Insurance
entitlements. To promote this shift, further changes to the organization and management of the
State Health Systems are necessary; most importantly, further autonomy of the REPSS and the
strengthening of its functions. In the meantime, refined and stronger performance management
arrangements between the Commission and State Health Systems have to be put in place.
Enhancing the effective administration of Popular Health Insurance entitlements will also hinge
on improvements in the understanding of entitlements under the Popular Health Insurance by
beneficiaries as well as on fostering demand for health promotion and disease prevention.
3. The Government of Mexico acknowledges the challenges facing the health and social
protection of people without contributory social security and, more specifically, Popular
Health Insurance; accordingly, it has developed plans to expand and strengthen the system.
Most importantly, because the crisis threatens health gains of the country and the finances of
poor and vulnerable families, the Government decided to preserve and expand – as possible – the
insurance‘s coverage. Moreover, the Commission has developed plans to strengthen the Popular
Health Insurance. These plans are ambitious given their implementation timeframe of three years
(that is, their completion prior to the presidential elections in 2012). At the same time, however,
they are feasible as they focus on change within the existing regulatory framework and recognize
political realities.
Project Development Objective
4. The proposed Project Development Objectives are to (i) initially preserve and later
expand the Popular Health Insurance’s coverage of people without contributory social
security, and (ii) strengthen the capacity of the Commission and State Health Systems to
effectively administer the entitlements of the Popular Health Insurance.

53
Project Components
5. The Project would consist of two components. Component I would finance the eligible
federal ―social contributions‖ (see Figure A4.1) to the premium of the Popular Health Insurance
to initially preserve and later expand the Popular Health Insurance‘s coverage of people without
contributory social security. Across the globe, Bank projects have started to co-finance insurance
and in particular health insurance premiums. The proposed Project would be a logical extension
of this practice insofar that it would finance the insurance premium of the developing world‘s
largest (both in terms of population and benefits) and highly scrutinized health insurance for
people without contributory social security. Component II would finance technical assistance to
strengthen capacity of the Commission and State Health Systems to effectively administer the
entitlements of the Popular Health Insurance, including technical assistance for enhanced
performance management and support to States in preparing and carrying out reforms in the
administration of the Popular Health Insurance, improved knowledge of eligible beneficiaries
about entitlements, strengthened health risk management, and effective project coordination and
management.
Component I: Popular Health Insurance’s Coverage of People without Contributory Social
Security (US$1,240 million)
6. Financing of eligible federal social contributions to the premium of the Popular Health
Insurance to initially preserve and later expand the Popular Health Insurance‘s coverage of
Eligible Beneficiaries. Specifically, component I would finance the share of the federal social
contributions earmarked for financing the Popular Health Insurance premium as referred to in
Article 77 of the General Health Law.
7. The SPSS57
, including the premium of the Popular Health Insurance, is financed by
the Federal and State governments. The specific arrangements mimic the tripartite funding
model of Mexico‘s contributory social security systems (which combine employer, employee,
and Government contributions). The Federal Government makes two contributions: the social
contribution (cuota social) and the federal solidarity contribution (aportación solidaria
federal). States make their own contribution called state solidarity contribution (aportación
solidaria estatal).
8. The General Health Law defines the different contributions and analogous to the
social security schemes provides for a dynamic adjustment mechanism. The General Health
Law establishes the premium of the Popular Health Insurance as a fixed share of all three federal
and State contributions (currently 89 percent; the remaining 11 percent finance the Fund for
Catastrophic Health Expenditures as well as trust funds for infrastructure investments and
reserves). Moreover, the law sets forth the relative magnitude of the contributions and, thus, the
share of Federal and State Government financing. With the federally-financing social
contribution serving as the reference point, the federal solidarity contribution is set at 150
57 This includes the Popular Health Insurance, the Fund for Catastrophic Health Expenditures and several Trust
Funds. The Health Insurance for a New Generation is financed separately and exclusively from federal
contributions.
54
percent of the social contribution and the state solidarity contribution at 50 percent of the social
contribution. Thus, the combined Federal financing is five-sixths of the premium compared to
the State financing of one-sixth of the premium. Analogous to Mexico‘s social security system,
the General Health Law provides for a dynamic adjustment of the premium by linking the social
contribution to the minimum general salary of the Federal District. Per labor law, the minimum
general salary of the Federal District is annually adjusted for consumer price inflation, which in
the case of Mexico and other Latin American countries corresponds well with health inflation
(World Bank, forthcoming). Recent changes to the General Health Law recalibrated the social
contribution and reduced it from 4.84 to 3.92 percent the minimum general salary of the Federal
District.58
9. The federal solidarity contribution is adjusted for other health financing sources to
correct historical fiscal imbalances across State Health Systems. Before the Popular Health
Insurance, the Federal Government made transfers to the States for the public health care service
system based on prior-year (historical) budgets of two major funding channels: i) personal health
care services, including payroll for State health workers and maintenance of infrastructure; and,
ii) national health programs, for example, allocations to finance health services from the
conditional cash transfer program, Oportunidades. Given that the federal fiscal coordination law
protects historical flows of funds, the federal solidarity contribution is adjusted for them. More
specifically, it is first calculated as the national average of 1.5 times the social contribution as
according to the General Health Law.59
Then, the amounts scheduled through other funding
channels to each State are subtracted from the national average. If the federal solidarity
contribution still has not been met through these channels in a State, then the Federal
Government transfers the remaining amount (known as the complementary federal solidarity
contribution) to that State. Because of this alignment, there are some States who do not receive
resources directly from the federal solidarity contribution as it has been covered in full by the
other financing sources. For example, in 2008, there were nine States that did not receive the
complementary federal solidarity contribution: Baja California Sur, Campeche, Colima,
Coahuila, Durango, Aguascalientes, Nayarit, Yucatán and Sonora. The remaining States,
however, received the complementary contribution because they had either less budgetary funds
from other sources considered in the alignment or a large population without contributory social
security, or both. The allocation rules of the federal solidarity contribution have been
instrumental in adjusting for historical, fiscal imbalances across State Health Systems.
10. An actuarial system annually assesses the financial sustainability of the Popular
Health Insurance. More specifically, it assesses the financial impact of uncertainty and risks
using statistical probabilities for a large variety of variables, including, for example, health
needs, treatment seeking behaviors and cost structures. As in last year‘s case, the identification
of significant mismatches between the premium, reserves and insurance risks should prompt
adjustments to the premium (and possibly to the insurance benefits as well).
58
In late 2009, Mexico took a bold step to substantially expand the coverage of the Popular Health Insurance by
changing the General Health Law to refine the premium system (see Annex 1 for details). 59
This is the national average that the States receive under the federal solidarity contribution. The formula that is
used to calculate exactly how much each State receives from the federal solidarity contribution is based on the
following four weighted components (which can vary by year): 1) at least 80 percent (by law) for the number of
beneficiaries to Popular Health Insurance; 2) 18.5 percent for the health needs of the State; 3) 0.25 percent for State
efforts; and, 4) 1.25 percent for performance.

55
11. The SPSS also provides for a beneficiary contribution that State Health Systems can
use to invest into service delivery improvements of their provider networks. This beneficiary
contribution is set as a progressive proportion of household income. Since the 2003 GHL,
families in the lowest two income deciles as well as those with two or more children in the third
income decile are exempt from having to make a contribution. More recently, with establishment
of the Health Insurance for a New Generation, all children born after December 1, 2006 and their
families that are in the third through seventh decile are exempt from contributing as well until the
child‘s fifth birthday. De jure, all other beneficiaries are expected to pay up to 4.5 percent of
their base salary, with the percentage increasing proportionally to their level of income. The
socio-economic development (including income) of households is assessed with a short proxy-
means test. However, de facto, beneficiary contributions have been difficult to collect as
approximately five percent of all beneficiaries contribute to the insurance and annual
contributions totaled only US$35 million in 2008. In general, it is the legal responsibility of the
States to assess and collect the beneficiary contribution. Under federal rules and supervision,
States can then use these funds to invest in service delivery improvements, mainly for the hiring
of additional staff and the purchasing of equipment, but excluding civil works.
12. Each year, the Commission and State Health Systems agree on affiliation targets
commensurate with the overall budget envelope for the Popular Health Insurance; affiliation
itself is governed by strict controls. Targets have given priority to families in the lower income
deciles and those enrolled into social assistance programs (such as the conditional cash transfer
program, Oportunidades, and the food supplementation program, Diconsa). Moreover, since
December 2006, pregnant women, sick children and newborns can enroll with Popular Health
Insurance through the Health Insurance for a New Generation at any time. Affiliation is subject
only to proof of citizenship and a lack of contributory social security. A birth certificate or an
official document including the national identification number can be presented as the proof of
citizenship. The lack of contributory social security is assessed through a survey applied at the
Figure A4.1. Financing Flows of the Popular Health Insurance Premium

56
point of affiliation. To identify the closest health center that will serve as an entry point to the
health care delivery system, a document confirming the beneficiary family‘s address is required
(usually a utility bill is sufficient). In addition, during the affiliation process, the family member
present at affiliation has to complete a proxy means test to determine the family contribution
level. All data collected in this process are submitted and confirmed at the federal level. Upon
confirmation, the State Health Systems issue an insurance policy to the beneficiary family along
with a letter describing their rights and obligations (Carta de Derechos and Obligaciones).
Finally, the Federal Government carries out annual audits of the affiliation processes.
13. The Popular Health Insurance introduced a package of explicitly defined entitlements
into the public health care service system. This package includes most importantly 266 health
interventions that correspond to 100 percent of services commonly delivered at public health
care centers, including community hospitals, and more than 80 percent of services commonly
delivered at public hospitals (CNPSS 2009). Each intervention in the package is defined through
a service delivery protocol and confirmed as cost-effective by economic evaluations.
14. As the Government’s flagship program for improving health sector outcomes including
financial protection in health, the Popular Health Insurance is comprehensively and
transparently monitored and evaluated by the Commission. The Commission has adopted a
three-pronged approach to the monitoring of the insurance. First, it assesses trends in affiliation
including the number of beneficiary families, their characteristics (e.g. income decile, indigenous
versus non-indigenous, gender of the head of the household) as well as information on the
accuracy of the affiliation process by State. Second, the Commission monitors the various
contributions to the system, including transfers to States, the state solidarity contributions and the
beneficiary family contributions as well as their impact on the financing of State Health Systems.
Third, it monitors the volume and quality of service delivery, including the provision of
medicines, training of health providers and the accreditation of facilities. In addition to this
monitoring approach, it carries out patient satisfaction surveys every six months. Furthermore,
the National Commission for Evaluation carries out annual evaluations of the insurance, drawing
on monitoring data and national surveys (e.g. census and health and nutrition surveys). The
Commission compiles the monitoring data twice a year in a report that is submitted to Congress.
These reports and the findings of the National Commission for Evaluation are further made
publicly available.
15. In comparison with other non-contributory health insurance schemes in the region,
Mexico’s Popular Health Insurance is one of the youngest but the largest scheme both in
scale and scope (see Table A4.1). Drawing from the experiences of other Latin American
countries with non-contributory health insurance programs, in 2003, Mexico established the
Popular Health Insurance with the GHL. The Popular Health Insurance has the largest target
population among all similar programs. Moreover, it is the largest scheme in scale by far,
guaranteeing the most comprehensive benefits package in number of interventions as well as the
level of the premium. As most schemes, the Popular Health Insurance is designed to include a
per capita premium (which, in contrast to other programs, is adjusted for fiscal imbalances
across State Health Systems) and non-competing purchasing agencies (in Mexico‘s case, State
Health Systems).
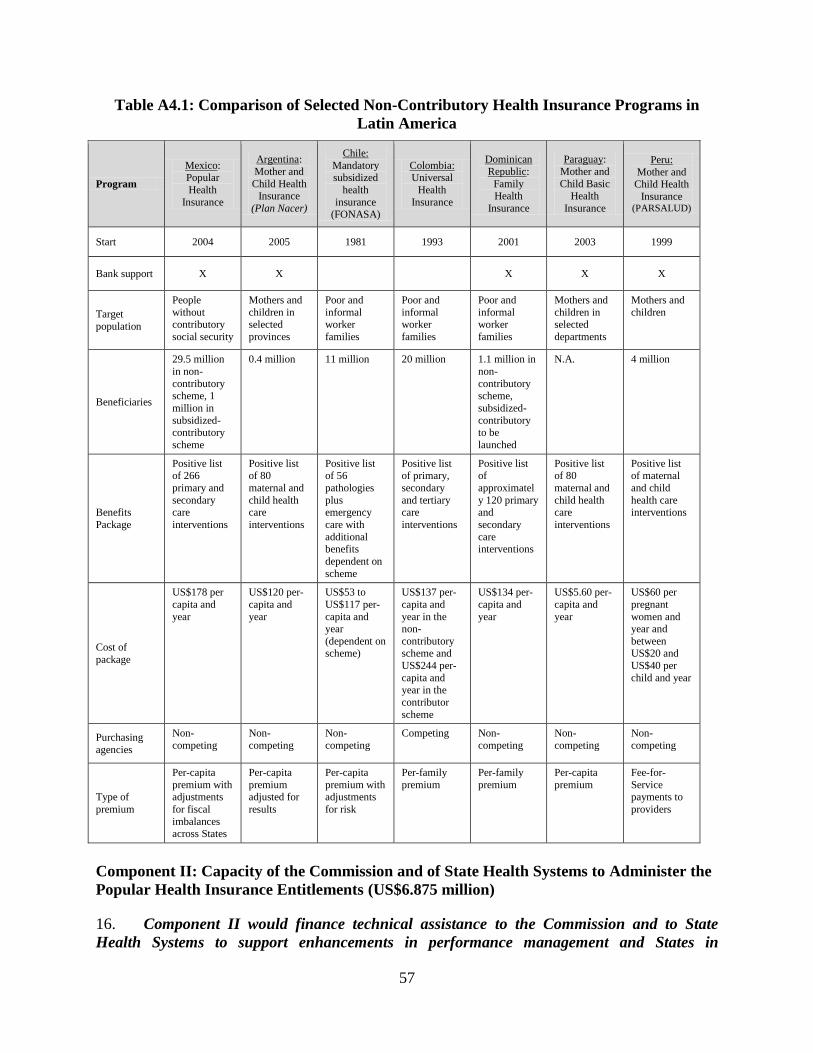
57
Table A4.1: Comparison of Selected Non-Contributory Health Insurance Programs in
Latin America
Program
Mexico: Popular
Health
Insurance
Argentina:
Mother and
Child Health Insurance
(Plan Nacer)
Chile:
Mandatory subsidized
health
insurance (FONASA)
Colombia: Universal
Health
Insurance
Dominican
Republic:
Family Health
Insurance
Paraguay:
Mother and
Child Basic Health
Insurance
Peru:
Mother and Child Health
Insurance (PARSALUD)
Start 2004 2005 1981 1993 2001 2003 1999
Bank support X X X X X
Target
population
People
without contributory
social security
Mothers and
children in selected
provinces
Poor and
informal worker
families
Poor and
informal worker
families
Poor and
informal worker
families
Mothers and
children in selected
departments
Mothers and
children
Beneficiaries
29.5 million
in non-
contributory scheme, 1
million in
subsidized-contributory
scheme
0.4 million 11 million 20 million 1.1 million in
non-
contributory scheme,
subsidized-
contributory to be
launched
N.A. 4 million
Benefits
Package
Positive list of 266
primary and
secondary care
interventions
Positive list of 80
maternal and
child health care
interventions
Positive list of 56
pathologies
plus emergency
care with
additional benefits
dependent on
scheme
Positive list of primary,
secondary
and tertiary care
interventions
Positive list of
approximatel
y 120 primary and
secondary
care interventions
Positive list of 80
maternal and
child health care
interventions
Positive list of maternal
and child
health care interventions
Cost of
package
US$178 per
capita and
year
US$120 per-
capita and
year
US$53 to
US$117 per-
capita and year
(dependent on scheme)
US$137 per-
capita and
year in the non-
contributory scheme and
US$244 per-
capita and year in the
contributor
scheme
US$134 per-
capita and
year
US$5.60 per-
capita and
year
US$60 per
pregnant
women and year and
between US$20 and
US$40 per
child and year
Purchasing
agencies
Non-
competing
Non-
competing
Non-
competing
Competing Non-
competing
Non-
competing
Non-
competing
Type of
premium
Per-capita
premium with adjustments
for fiscal
imbalances across States
Per-capita
premium adjusted for
results
Per-capita
premium with adjustments
for risk
Per-family
premium
Per-family
premium
Per-capita
premium
Fee-for-
Service payments to
providers
Component II: Capacity of the Commission and of State Health Systems to Administer the
Popular Health Insurance Entitlements (US$6.875 million)
16. Component II would finance technical assistance to the Commission and to State
Health Systems to support enhancements in performance management and States in

58
preparing and carrying out reforms in the administration of the Popular Health Insurance;
improved knowledge of eligible beneficiaries about entitlements; strengthened health risk
management; and effective Project coordination and management.
17. Enhancements in performance management in the administration of the Popular
Health Insurance and support to State Health Systems in preparing and carrying out reforms
in the administration of the Popular Health Insurance: The component would support the
strengthening of performance management arrangements between the Commission and the State
Health Systems, specifically, to establish non-financial incentives that promote the effective
delivery of the entitlements and the benefit package of the Popular Health Insurance. The
component would strengthen the capacity of State Health Systems to monitor the delivery of
health services to different groups of beneficiaries (including vulnerable groups). At the same
time, it would strengthen the capacity of the Commission to capture, validate (including to carry
out audits) and publicize information as well as to set benchmarks and issue recommendation to
improve performance. At the same time, the component would support the development of
mechanisms to help State Health Systems to carry out management and organizational reforms;
most importantly, the development of critical health insurance functions. Such mechanisms
would include platforms that foster learning and, specifically, the transfer of experiences and
innovations across State Health Systems as well as the development of financing mechanisms for
technical assistance.
18. Improvements in the knowledge of eligible beneficiaries about their entitlements under
the Popular Health Insurance. The component would strengthen the capacity of the
Commission and State Health Systems to improve the knowledge of beneficiaries about
entitlements to foster their demand for health services, specifically for promotion and prevention
services and enhance the effectiveness of mediation and arbitration systems. Moreover, it would
strengthen their capacity not only to inform beneficiaries but reach out to individuals that are
eligible for coverage under the Popular Health Insurance to foster their demand for affiliation;
specifically, those in hard-to-reach groups, including indigenous peoples and the poor. The
component would strengthen the capacity of the Commission and State Health Systems to
design, carry out and evaluate behavior change communication strategies.
19. Strengthening health risk management. The component would strengthen the capacity
of the Commission and State Health Systems to manage health risks of beneficiaries to
specifically reduce the burden of non-communicable diseases and improve the allocative
efficiency of the system. At the same time, this would enhance the Commission‘s capacity to
better assess the demographic and epidemiological risk profile of the beneficiary population and,
consequently, the financial risks facing the systems. The component would strengthen the
capacity of the Commission and State Health Systems to design and evaluate health risk
management programs and the capacity of State Health Systems to implement such programs.
20. Effective Project management. The component would strengthen the capacity of the
Commission to manage the Project. It would strengthen its capacity to audit the financing of the
Popular Health Insurance as well as to carry out procurement processes according to practices
acceptable to the Bank. Furthermore, it would strengthen its capacity to implement the
Indigenous Peoples Plan.

59
Annex 5: Project Costs
MEXICO: Social Protection System in Health
Project Cost by Component and/or
Activity
Local
US $ million
Foreign
US $ million
Total
US $ million
Premium for the Popular Health
Insurance 26,825.000
26,825.000
Technical assistance 25.000 7.875 32.875
Total Baseline Cost
Total Project Costs 26,850.000 7.875 26,857875
Front-end Fee* 3.125 3.125
Total Financing Required 26,850.000 11.000 26,861.000
*0.25 percent of the total amount of the loan
60
Annex 6: Implementation Arrangements
MEXICO: Social Protection System in Health
1. The 2003 General Health Law, and its regulations, establishes and governs over the
Popular Health Insurance. In 2003, the General Health Law (GHL) was modified to ensure that
all individuals, including those lacking contributory social security, were guaranteed the social
right to health protection. To carry out this right, it created the Popular Health Insurance (or
Seguro Popular) as part of the overarching Social Protection System in Health (SPSS). The GHL
has three main regulations regarding the implementation arrangements of the SPSS: (i)
Regulations for the Social Protection System in Health (Reglamento en Materia de Protección
Social en Salud); (ii) Internal Regulations for the Council of Social Protection in Health
(Reglamento Interno del Consejo Nacional de Protección Social en Salud); and (iii) the Internal
Regulations for the National Commission of Social Protection in Health (Reglamento Interno de
la Comisión Nacional de Protección Social en Salud).
2. The Federal and State governments play key implementing roles in the Social
Protection System in Health, including the Popular Health Insurance. Through the Secretariat
of Health, the Federal Government is responsible for the overall regulation, organization and
monitoring of the health system and, in particular, the Social Protection System in Health. Both
the Federal Government and States60
finance the Social Protection System in Health. The Federal
Government transfers funds to the States for the Popular Health Insurance. In return, the States
guarantee health benefits free of charge to those enrolled in the Popular Health Insurance. The
Federal Government and the States have coordination agreements that legally establish the duties
of each party involved in the implementation of the SPSS.
Main Actors and Implementation Arrangements of the SPSS, including the Popular Health
Insurance
3. The Secretariat of Health is responsible for developing, coordinating, monitoring,
evaluating and regulating the health system, including the SPSS.61
It is responsible for
defining the organizational framework and general actions of the Social Protection System in
Health at all levels of government – Federal, State and municipal.
4. The National Commission of Social Protection in Health (the Commission)62
, a
deconcentrated unit of the Secretariat of Health, is responsible for the overall implementation
of the SPSS. The Commission is a unit within the Secretariat of Health with technical,
administrative and operational autonomy. It has the mandate to manage the Popular Health
Insurance, including the affiliation process, the transfer of financial resources to the States, and
60
The term ―States‖ refers to the 31 States and Federal District in Mexico. 61
pursuant to Art. 7 GHL. 62
The creation of the Commission was published in the official gazette (Diario Oficial de la Federación) on May
15, 2003.
61
the implementation of SPSS activities as established in Articles 3 and 4 of the Reglamento
Interno de la Comisión Nacional de Protección Social en Salud63
.
5. The States are responsible for organizing, coordinating, operating, supervising and
evaluating health services pursuant to Article 9 of the GHL64
. With regard to the Popular
Health Insurance, they are in charge of affiliating, including the issuing of insurance policies,
ensuring the delivery of health services to beneficiaries, accrediting and paying service
providers, and demonstrating their achievement of affiliation targets and proper use of monies to
the Federal Government. These functions are to be carried out by the State Regimes of Social
Protection in Health (Regímenes Estatales de Protección Social en Salud or REPSS),
administrative structures within the State Health Systems.
6. Coordination agreements between the Secretariat of Health and the State Health
Systems guide the implementation of the SPSS. These are multi-year agreements through which
a State commits to remaining in the SPSS after the initial signing. They have four Annexes,
specifying different commitments: (i) affiliation; (ii) health system management; (iii) targets; (iv)
the budget. They are subject to annual ratification and signed by the Commissioner of the
National Commission of Social Protection in Health, the Secretaries of the State Health Systems,
and representatives from each State‘s REPSS.
Roles and Responsibilities in Project Implementation
7. The National Commission of Social Protection in Health would be responsible for
Project implementation. Within the Commission, the Office of the Commissioner would
constitute the Project Coordination Unit (PCU), which would be responsible for coordinating all
of Project activities. The Head of the Office of the Commissioner would serve as the head of the
PCU.
8. The PCU would have the following responsibilities:
To ensure all legal requirements of the Project are met, including compliance with the
Bank‘s social safeguard policies (specifically the Project‘s Indigenous Peoples Plan
(IPP)), timely reporting of Project activities to the Bank and the Project audit;
To ensure that the States comply with the Bank‘s anti-corruption guidelines and the
activities laid out in the Project‘s IPP;
To supervise the Project, including the monitoring of Project indicators;
To regularly assess the progress of the Project‘s implementation, identifying bottlenecks
as well as strategies for their resolution;
To prepare and, as necessary, update the Project‘s Operational Manual;
To prepare, update and monitor the Project‘s operational and procurement plans;
To coordinate ex-post procurement reviews;
To coordinate the preparation of the semi-annual Project reports, which would include the
unaudited Interim Financial Reports (see next paragraph) and the Project audits; and
63
Published in the official gazette (Diario Oficial de la Federación) on February 27, 2004. 64
Published in the official gazette (Diario Oficial de la Federación) on February 24, 2005.
62
To ensure that fiduciary staff that carrying out procurement and financial management
activities are properly trained.
9. Accordingly, the PCU would prepare semi-annual “Project Reports” that include
unaudited “Interim Financial Reports” (IFRs) and progress reports on Project indicators. The
PCU would prepare these reports periodically, including financial information for the IFRs and
results from its monitoring and evaluation activities. It would submit these reports to the Bank no
later than 45 days after the end of each calendar semester, with Project outcome indicators
reported annually, and intermediate outcome indicators for each Component every 6 months (or
as information becomes available).
10. The National Finance Agent (NAFIN) would support the PCU in financial
management and procurement activities related to Project implementation. As the Mexican
Government‘s public finance agent, NAFIN has ample experience supporting the
implementation of several Bank-financed projects. Prior to Project effectiveness, its cooperation
with the Project would be governed by a contract (Contrato de Mandato) between them, the
Federal Secretariat of Finance and the Federal Secretariat of Health.
11. Under the coordination of the PCU, three General Directorates of the Commission, and
their staff, would play critical roles in the Project’s implementation. The General Directorate of
Finance (DGF) and the General Directorate of Affiliation and Operation (DGAO) would jointly
lead the implementation of Component I (Initially preserve and later expand the Popular Health
Insurance’s coverage of people without contributory social security). The General Directorate of
Coordination with Federal Entities (DGCEF) and the General Directorate for Affiliation and
Operation (DGAO) would jointly lead the implementation of Component II (Strengthen the
capacity of the Commission and State Health Systems to effectively administer the entitlements of
the Popular Health Insurance). Activities of these three lead General Directorates would be
supported by the General Directorate of Health Service Management (DGGSS) and the General
Directorate of Administration and Finance (DGAF).
12. The General Directorate of Finance (DGF)65
would have the following responsibilities:
To support the formalization of the coordination agreements for the implementation and
operation of the SPSS as well as the monitoring of the REPSS, within its area of
competence;
To contribute to the design of the indicators for the Project monitoring framework;
To calculate the liquid part of Federal Government‘s transfer of the social contribution to
the States, based on the financing criteria established in the GHL and the reports provided
by the DGAO;
To transfer the funds of the Federal Government‘s social contribution to the States,
together with the participation of the administrative units of the Secretariat of Health and
to carry out the accounting of the records;
To confirm that the resources from the state solidarity contributions and the beneficiary
contributions are in agreement with the list of beneficiaries;
65
See Article 9 of the Reglamento Interno as published in the official gazette (Diario Oficial de la Federación) on
November 28, 2006.

63
To supervise of the execution of the transferred funds; and
To prepare Project Financial Statements of Expenditures SOEs and the unaudited IFRs.
13. The General Directorate for Affiliation and Operation (DGAO)66
would have the
following responsibilities:
To support the formalization of the coordination agreements for the implementation and
operation of the SPSS as well as monitoring of the REPSS, within its area of competence;
To contribute to the design and follow up of the indicators in the Project monitoring
framework;
To administer the beneficiary database, including the review of affiliation applications and
registries as well as reconciled affiliation registries;
To agree each year with the States on the number of eligible beneficiaries to be
incorporated into the Popular Health Insurance, as well as the criteria and procedures for
the promotion and the affiliation of beneficiaries;
To assess trends in affiliation, including the number of beneficiaries and their
characteristics, as well as information on the accuracy of the affiliation process by State;
To carry out annual audits on the affiliation process for a sample of newly affiliated
beneficiaries;
To develop, implement and evaluate the health risk management program;
To carry out consultations with stakeholders; and
To provide implementation support to State Health Systems, including supervision and
training, surveys design, and data collection and analysis.
14. The General Directorate of Coordination with Federal entities (DGCEF)67
would have
the following responsibilities:
To participate in the negotiation and management of the signing of the coordination
agreements;
To contribute to the design and follow up of the indicators in the Project monitoring
framework;
To define and coordinate the guidelines of the States‘ strategic plan;
To coordinate the implementation of the Commission‘s strategic supervision plan;
To review and refine the federal monitoring and audit system of the Popular Health
Insurance, including the coordination agreements;
To assess the capacity of the State Health Systems to monitor health service delivery and
costs;
To develop instruments to capture and audit information;
To develop benchmarks for improving the States‘ administration of the Popular Health
Insurance; and
66
See Article 8 of the Reglamento Interno as published in the official gazette (Diario Oficial de la Federación) on
November 28, 2006. 67
See Article 10 BIS 2 of the Reglamento Interno as published in the official gazette (Diario Oficial de la
Federación) on November 28, 2006.

64
To design a disclosure policy, along with a financing mechanism, to provide technical
assistance to the State Health Systems in the process of separating and strengthening key
health system functions.
15. The General Directorate of Health Service Management (DGGSS)68
would have the
following responsibilities:
To support the formalization of the coordination agreements for the implementation and
operation of the SPSS as well as monitoring of the REPSS, within its area of competence;
To contribute to the design and follow up of the indicators in the Project monitoring
framework;
To review the States‘ annual accreditation plans;
To supervise the State Health Systems in their implementation of the activities laid out in
the Project‘s IPP; and
To support the DGAO in developing and implementing the health risk management
program.
16. The General Directorate of Administration and Finance (DGAF)69
would have the
following responsibilities:
To carry out the procurement of services as well as the preparation and facilitation of ex-
post procurement reviews;
To consolidate financial and budget information for the Commission;
To perform and keep accounting and budget control records, including those of all
expenditures under component II of the Project, and;
To participate in and support the preparation of the Project‘s financial statements and the
process of annual audits.
Operational Rules
17. The Commission through an official communication would require the States to commit
to implementing the activities laid out in the IPP. Article 4 of the Commission‘s Reglamento
Interno70
empowers it to direct and carry out the necessary actions for the operation of the
Popular Health Insurance, including those related to the improvement of the health of vulnerable
groups, including indigenous populations, with the support of different units of the Ministry of
Health.
18. The Project’s Operational Manual (OM) specifies the processes and procedures
governing Project implementation. The Commission has presented an OM for the Project that is
acceptable to the Bank. It includes detailed arrangements for carrying out the Project, including:
(i) procurement, disbursement and financial management arrangements; (ii) reporting and
68
See Article 10 of the Reglamento Interno as published in the official gazette (Diario Oficial de la Federación) on
November 28, 2006. 69
See Article 10 BIS 1 of the Reglamento Interno as published in the official gazette (Diario Oficial de la
Federación) on November 28, 2006. 70
See Article 4 f. XI of the Reglamento Interno as published in the official gazette (Diario Oficial de la Federación)
on November 28, 2006.
65
auditing requirements; (iii) the Indigenous Peoples Plan; (iv) key performance indicators; (v) the
eligibility criteria of eligible beneficiaries; ; (vi) transparency and anticorruption provisions; and
(vii) the roles and responsibilities of the different administrative units for Project
implementation.
19. For additional information on the implementation arrangements for the monitoring,
financial management and procurement of the Project please see Annexes 3, 7 and 8.

66
Annex 7: Financial Management and Disbursement Arrangements
MEXICO: Social Protection System in Health
1. Introduction. This annex documents the results of the Financial Management (FM)
Assessment of the National Commission of Social Protection in Health (the Commission), which
would be the implementing entity for the Mexico: Support to the Social Protection System in
Health Project (the Project). The assessment was conducted by Bank staff in accordance with
OP/BP 10.02 and Guidelines for Assessment of Financial Management Arrangements in World
Bank-Financed Projects. It takes into account the considerable experience of the National
Finance Agent (NAFIN) as financial agent of Bank‘s resources.
2. Summary. The Project’s financial management arrangements including the
Commission’s fiduciary controls for oversight and monitoring of the funds transferred at the
State level for purposes of the program are acceptable to the Bank; the residual financial
management risk is considered modest. The Project would make large use of the country public
FM systems, including budgeting, accounting, treasury, internal control and auditing. At the
federal level those systems are strong and acceptable to the Bank. However, the documentation
to support disbursements under component I would rely on data from States, with different levels
of financial management capacity. Therefore, the Commission provides strong oversight,
monitoring controls and supervision procedures for the implementation of the Popular Health
Insurance by States. The Bank appraised these mitigating measures as part of the assessment of
the Project‘s financial management arrangements and considers them acceptable. More
specifically, the Bank team is comfortable that these measures are adequate to assure that States
use Project funds for the intended purposes. The mitigating controls include but are not limited
to: (i) monthly internal validation and reconciliation processes of State affiliation registries (ii)
permanent supervision of the use of Popular Health Insurance funds, including on-site visits by
the Commission. The Popular Health Insurance is also subject to local internal control and
auditing practices conducted by State internal control offices and local supreme audit institution;
furthermore, it is audited by the Auditor General‘s office. In addition, the Project‘s annual
financial audit would include a technical component to assess and review affiliation registries at
the State level, including the compliance with operational rules.
Description and Assessment of Project FM arrangements
3. Country issues relevant to the Project. In general, public financial management in the
Mexican Federal Administration relies on strong budgeting, treasury, accounting and control
systems. These FM country systems would apply to Project execution at the Federal level; the
Project would be implemented through the national budget as described below.
4. Implementing entity. The National Commission of Social Protection in Health (the
Commission), which has relatively strong institutional structures and control systems, would be
responsible for overall implementation of the Project. From the FM perspective, the role of the
Commission‘s following administrative units would be critical for Project implementation: (i)
the General Directorate of Financing (DGF); (ii) the General Directorate for Affiliation and
Operation (DGAO), (iii) the General Directorate of Administration and Finance (DGAF), and
(iv) the General Directorate of Coordination with Federal Entities (DGCEF). Given that the
67
Commission does not have previous experience with the implementation of Bank-financed
projects, a FM expert of the Commission will be designated to carry out FM tasks, in
coordination with NAFIN, such as the process of submitting disbursement applications,
preparation of financial and audit reports. This specialist will be trained at Bank-related matters,
as needed.
5. Financial administration. NAFIN would act as the financial agent of the Borrower. In
that capacity, NAFIN would manage loan disbursement processes and provide other
implementation support and oversight, drawing on its many years of experience with Bank-
financed projects.
6. Budgeting arrangements. Project funds would be part of the Federal Expenditure Budget
(PEF). Thus, Project funds would be subject to provisions of the annual PEF Law, the Federal
Budget and Fiscal Responsibility Law, the General Government Accounting Law, the Guidelines
on Budget Procedures, and others. This set of legal and regulatory arrangements, together with
their implementation systems, provides sound budget formulation, execution and control
arrangements. As per usual practice in Mexico for the operations implemented on the national
level, the Government would pre-finance the Project and the Bank would subsequently
reimburse eligible expenditures recorded under budgetary lines earmarked for the Project (dígito
2).
7. Accounting system. The CNPSS, through the PCU, DGF and DGAF, would maintain
records and accounts adequate to reflect this Bank-financed operation and would be responsible
for keeping files of all supporting documentation for project expenditures, including the federal
contributions to the insurance premium of the Popular Health Insurance Program and technical
assistance (under component II). Both DGF, which is responsible for the accounting records of
all funds transferred to the States, and DGAF, which is responsible for the institutional
accounting and budgeting records and control, as well as for the consolidation of overall
institutional financial and budgeting data, have implemented a Contabilidad Integral (COI)
accounting information system. COI is a well-known commercial IT application, which is
considered acceptable to the Bank. Project records would be kept in accordance with accounting
practices acceptable to the Bank and in compliance with national requirements established by the
Federal Ministry of Finance (Integrated System of Governmental Accounting - SICG). Some
Bank-specific data, such as Statements of Expenditures (SOEs) and Interim Financial Reports
(see below), would be extracted from the institutional systems and arranged in spreadsheets only
for presentational but not recording purposes.
8. Internal control and internal auditing. In addition to the budget regulations and
procedures mentioned above, the Commission is subject to the Federal Public Administration
Internal Control Standards issued by the Public Administration Ministry (SFP), which provide
sound internal control arrangements. The internal auditing function is carried out by the
Secretariat of Health‘s (SS) Internal Control Unit (OIC), which reports to SFP and follows the
Public Audit Standards and Guidelines issued by SFP. The SFP also approves the OIC‘s annual
work programs, oversees its operation, and receives its audit reports. Good systems are in place
for timely follow-up to internal audit observations and implementation of recommendations.
68
9. Once funds are transferred to States, local internal control and auditing practices apply,
whose quality can differ widely from one sub-national government to another. However, the
Commission has the prerogative to undertake evaluations of the State affiliation registries (see
below). Accordingly, the DGAO and DGF, under coordination of the DGCEF, carry out a
permanent supervision plan, including periodic field visits. This is in order to validate the
affiliation registry as well as the use of transferred funds. Both aspects are verified in accordance
with the coordination agreements between the Federal and State governments. The results of
these supervisions would be made available to the Bank and the project auditors.
Flow of Funds
10. Federal contributions to the insurance premium of the Popular Health Insurance. As
detailed in Annex 4, contributions from the Federal Government (federal social contribution and
federal solidarity contribution) and the States (state solidarity contribution) finance the SPSS.
The federal social contribution equals 3.92 percent of the minimum salary in the Federal
District, the latter being annually adjusted for the consumer price index and is a fixed amount
received by each State. A share of the federal social contribution, that is 89 percent, is
earmarked for the financing of the Popular Health Insurance. The federal solidarity contribution
equals on average 1.5 times the federal social contribution and it varies by State in accordance
with the allocation formula set forth in the General Health Law and adjusted for other Federal
Government transfers71
. As for the federal social contribution, a share of the federal solidarity
contribution is earmarked for the financing of the Popular Health Insurance. Because of the
adjustments for other Federal transfers, some States do not receive a federal solidarity
contribution at all.
11. As per the recently approved changes to the General Health Law and starting on January
1, 2010, the federal social contribution and federal solidarity contribution are calculated for each
affiliated individual.
12. Based on the number of persons affiliated and validated by the Commission, the
Commission transfers on a monthly basis the share of the federal social contribution earmarked
for the financing of the Popular Health Insurance to States; furthermore, it also retroactively
transfers the federal solidarity contribution to the States each month. As per the regulatory
framework of the SPSS, affiliation rates and transfers are reconciled each quarter.
13. To affiliate with the Popular Health Insurance, families need to provide several
identification documents. Eligibility is limited to those lacking contributory social security. To
ensure that Popular Health Insurance affiliates continue to be eligible for coverage, a system of
re-affiliation was established.72
At the time of affiliation, beneficiaries receive an insurance
policy. The States keep a file for each enrolled family, including a copy of the insurance policy
as well as copies of the documents gathered at the time of affiliation. These files are subject to
71
Not all funds go directly the States. Eight percent of the combined federal social contribution, federal solidarity
contribution and state solidarity contribution is assigned to the Fund for the Protection against Catastrophic
Expenses (FPGC) and three percent is assigned to the Budgetary Contingency Fund (FPP). 72
Families in the contributory scheme are re-affiliated annually upon payment of the annual family contribution.
Families in the non-contributory scheme are re-affiliated every three years.
69
reviews by the Commission as well as external evaluations. In 2007, an external evaluation
found that not all States used electronic formats of affiliation documents
14. The national affiliation registry is a compilation of all State affiliation registries. The
States are required to update and submit their registries to the Commission. After internal
validation processes, the number of beneficiaries per State is made public on a semi-annual basis.
The national registry is reconciled with registries from other federal social programs by the
Commission on monthly basis.
15. In general, external evaluations of the registry have shown satisfactory results. However,
these evaluations have raised some issues; for example, in the 2006 financing evaluation of the
Social Protection System in Health conducted by the Secretariat of Health (SPSS 2006), five
percent of visited families reported that they were not affiliated with the Popular Health
Insurance. Furthermore, 15 percent of families reported information on family members
inconsistent with registration data.
16. The Supreme Audit Institution (SAI‘s) latest published audit report of the Popular Health
Insurance (CY 2006) was qualified with exceptions. The main auditor‘s finding pertained to
several inconsistencies in the process of distributing credentials to beneficiaries, a procedure that
terminated in 2007.
17. Bank financing of Component I. The scope of the FM Assessment is not dealing with
the definition of eligibility of expenditures which is based on the principles covered by OP 6.0,
but rather with the assessment that FM arrangements for this project are acceptable and in place
to ensure that the loan proceeds are used for the purposes for which the loan is granted.
18. The Bank would reimburse transfers for the federal social contribution to all States. A cap
for Bank financing (e.g. 70 percent) may be established.
19. Calculations would be made on a quarterly basis and would be based on reports of
transfers to the States prepared by the DGF on a monthly basis. The total amount to be
reimbursed by the Bank would be determined by the number of beneficiary individuals derived
from the official national affiliation registry and the federal social contribution; it would be
presented using the SOE format as well as the Statement of the Affiliation Registry.
20. Flow of funds for the Bank Loan. Except for the front-end-fee (for the payment of which
the Bank shall, on behalf of the Borrower, withdraw funds from the Loan Amount), the Loan
would be disbursed in US Dollars into a bank account opened by NAFIN. These funds would be
transferred into a US Dollar account at the Federal Treasury. The Federal Treasury shall use
those funds in accordance with the Borrower‘s applicable laws. The Federal Treasury, through
its annual budget laws and mechanisms, would transfer to the Commission an amount equivalent
to the amount disbursed in US Dollars under the Loan to finance Eligible Expenditures. The
general arrangements are described in the following chart and explained below:

70
Reimbursement Component I
1. The Commission finances project expenditures from the national budget (PEF). The funds
are received from the National Treasury Office through the Integrated Financial Information
System for the Federal Government (SIAFF).
2. Federal contributions to the insurance premium of the Popular Health Insurance Program are
processed by the Commission, through the DGF.
3. Once national affiliation records are reconciled, the PCU would aggregate and summarize
reports of transfers, and present the information in a draft Statement of Expenditures (SOE),
supported by a Statement of Affiliation Registry, to NAFIN.
4. NAFIN would review the SOE and Statement of Affiliation Registry and submit it formally,
together with a loan withdrawal application, to the Bank.
5. The Bank would reimburse the eligible expenditures into a bank account opened by NAFIN.
6. NAFIN would reimburse TESOFE.
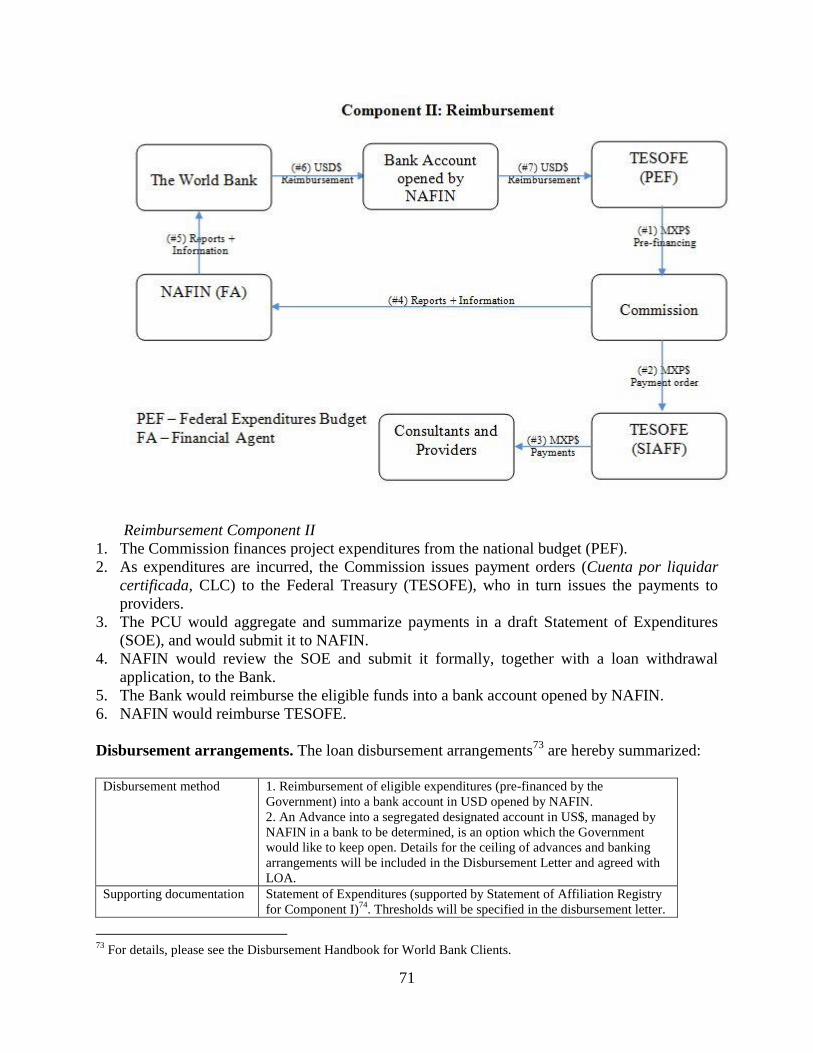
71
Reimbursement Component II
1. The Commission finances project expenditures from the national budget (PEF).
2. As expenditures are incurred, the Commission issues payment orders (Cuenta por liquidar
certificada, CLC) to the Federal Treasury (TESOFE), who in turn issues the payments to
providers.
3. The PCU would aggregate and summarize payments in a draft Statement of Expenditures
(SOE), and would submit it to NAFIN.
4. NAFIN would review the SOE and submit it formally, together with a loan withdrawal
application, to the Bank.
5. The Bank would reimburse the eligible funds into a bank account opened by NAFIN.
6. NAFIN would reimburse TESOFE.
Disbursement arrangements. The loan disbursement arrangements73
are hereby summarized:
Disbursement method 1. Reimbursement of eligible expenditures (pre-financed by the
Government) into a bank account in USD opened by NAFIN.
2. An Advance into a segregated designated account in US$, managed by
NAFIN in a bank to be determined, is an option which the Government
would like to keep open. Details for the ceiling of advances and banking
arrangements will be included in the Disbursement Letter and agreed with
LOA.
Supporting documentation Statement of Expenditures (supported by Statement of Affiliation Registry
for Component I)74
. Thresholds will be specified in the disbursement letter.
73
For details, please see the Disbursement Handbook for World Bank Clients.

72
Retroactive expenditures Eligible payments:
Period is within one calendar year before the signing of the LA;
That do not exceed 20 percent of the loan amount.
Expenditures would be subject to the same systems, controls, and eligibility
filters described above. Expenditures would also be subject to the Project‘s
external audit (see below).
Other procedures None
Disbursement Table.
Category Amount of the Loan
Allocated
(expressed in USD)
Percentage of Expenditures
to be financed
(inclusive of Taxes)
(1) Eligible federal social contributions under
Part 1 of the Project
1,239,000,000 70%
(2) [Goods] Consultant Services, Non-
Consultant Services, Training and Operating
Costs under Part 2 of the Project
7,875,000 100%
(3) Front-end Fee 3,125,000 Amount payable pursuant to
Section 2.03 of this
Agreement in accordance
with Section 2.07 (b) of the
General Conditions
(4) Premia for Interest Rate Caps and Interest
rate Collars (amounts due under section 2.07
(c) of this Agreement)
-0-
TOTAL AMOUNT 1,250,000,000
21. Financial reporting. The Commission, through the PCU, would prepare and submit to the
Bank not later than 45 days after the end of each calendar semester unaudited Interim Financial
Reports (IFRs) for the Project covering each semester. These reports would be based on the
formats of the annual financial statements, as established in the general framework for the audit
of all national level Bank-financed projects (the technical MOU on auditing), which has been
agreed upon by the Government and the Bank. The IFR format would also be based on the
financial report that the Commission sends to the OIC on a quarterly basis.
22. After loan effectiveness, the financial and audit reports would be presented by the
Commission to NAFIN for review and further submission to the Bank, as follows:
Report Due date (World Bank receipt)
Semi-annual unaudited project IFRs. Within 45 days after the end of each calendar semester.
Annual audit report on project financial
statements, including the Statements of
Affiliation Registry, and eligibility of
expenditures.
Within six months after the end of each calendar year of
loan disbursements (or any other period agreed upon with
the Bank).
74
All SOE supporting documentation, including Statement of Affiliation Registry, will be available for review by
the external auditors and Bank staff at all time during Project implementation, and at least until one year after the
audit report covering the last disbursement has been received by the Bank.
73
23. External audit. The project annual external audit scope and opinions would have two
components: (i) a technical audit on the Statement of Affiliation Registry; and (ii) a regular audit
of project financial statements and the eligibility of expenditures. The audit would be performed
in accordance with Bank policies, as reflected in the audit terms of reference and the
memorandum of understanding agreed between the Bank and SFP. However, specific terms of
reference would be agreed upon in order to establish that the technical audit would include an
opinion on the reliability of the Statements of Affiliation Registries submitted in support of
withdrawal applications. It would also consider that, as a minimum, the external auditor would
perform sample-based reviews of the affiliation database management systems of the
Commission and the States, verification of individual insurance policies, files, and field
interviews with beneficiaries. The specific Terms of Reference for these reviews would be
agreed upon with the Bank prior to a first disbursement under Component I.
24. It is also important to mention that the technical audit component would be performed
taken into account the results of the concurrent supervision activity carried out by the
Commission itself, through GDAO and DGF, as explained in the internal control and internal
auditing section of this annex. The results of these supervisions will be available to the project
auditors in order to be able to focus on any specific issue identified during the previous reviews.
25. An external audit firm, designated by SFP and acceptable to the Bank, would conduct the
project audits, which could be financed with resources from Component II.
26. Written procedures. Project FM procedures would be documented in an Operational
Manual (OM) that would define the roles and responsibilities of the Commission, including
DGAO, DGF, DGAF, DGCEF and the PCU. The OM would include, among other financial
procedures: (i) budgeting, treasury, accounting, and internal control policies and procedures; (ii)
formats of the SOEs, Statements of Affiliation Registry, and IFRs; and (iii) audit and other
supervision arrangements.
27. Risk assessment. On the basis of the Bank‘s Project FM assessment, the overall FM
residual risk is considered modest, as explained in the following table:
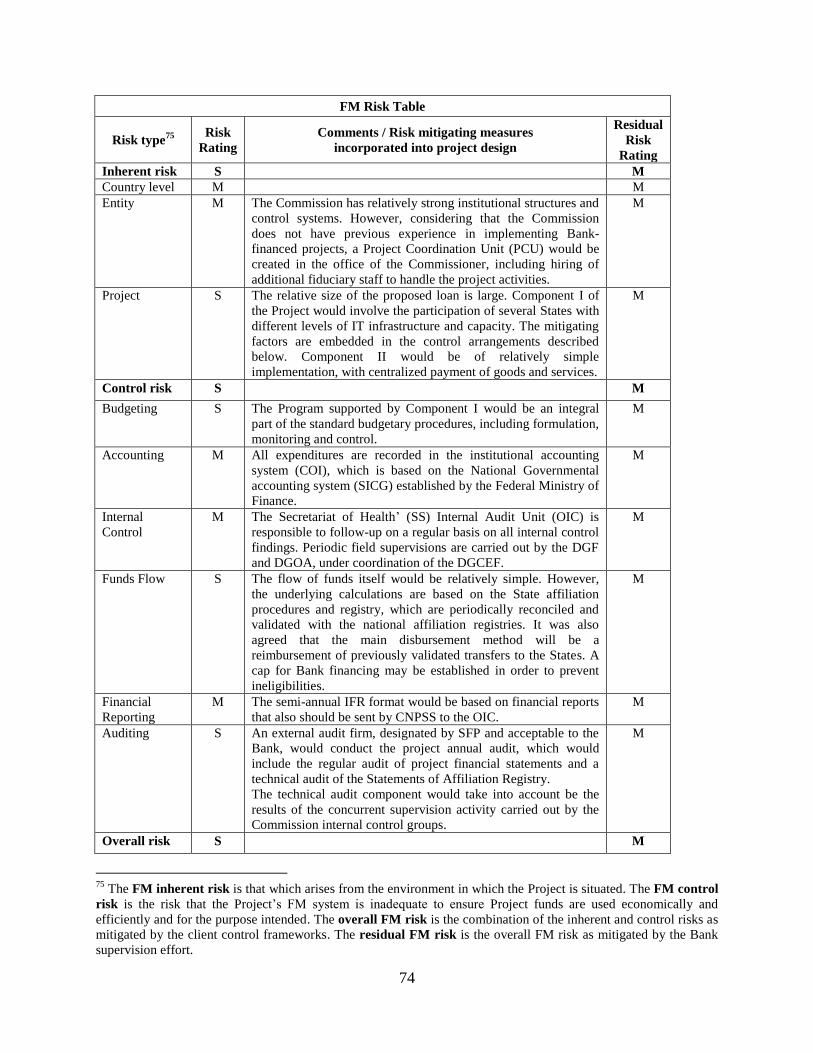
74
FM Risk Table
Risk type75
Risk
Rating
Comments / Risk mitigating measures
incorporated into project design
Residual
Risk
Rating
Inherent risk S M
Country level M M
Entity M The Commission has relatively strong institutional structures and
control systems. However, considering that the Commission
does not have previous experience in implementing Bank-
financed projects, a Project Coordination Unit (PCU) would be
created in the office of the Commissioner, including hiring of
additional fiduciary staff to handle the project activities.
M
Project S The relative size of the proposed loan is large. Component I of
the Project would involve the participation of several States with
different levels of IT infrastructure and capacity. The mitigating
factors are embedded in the control arrangements described
below. Component II would be of relatively simple
implementation, with centralized payment of goods and services.
M
Control risk S M
Budgeting S The Program supported by Component I would be an integral
part of the standard budgetary procedures, including formulation,
monitoring and control.
M
Accounting M All expenditures are recorded in the institutional accounting
system (COI), which is based on the National Governmental
accounting system (SICG) established by the Federal Ministry of
Finance.
M
Internal
Control
M The Secretariat of Health‘ (SS) Internal Audit Unit (OIC) is
responsible to follow-up on a regular basis on all internal control
findings. Periodic field supervisions are carried out by the DGF
and DGOA, under coordination of the DGCEF.
M
Funds Flow S The flow of funds itself would be relatively simple. However,
the underlying calculations are based on the State affiliation
procedures and registry, which are periodically reconciled and
validated with the national affiliation registries. It was also
agreed that the main disbursement method will be a
reimbursement of previously validated transfers to the States. A
cap for Bank financing may be established in order to prevent
ineligibilities.
M
Financial
Reporting
M The semi-annual IFR format would be based on financial reports
that also should be sent by CNPSS to the OIC.
M
Auditing S An external audit firm, designated by SFP and acceptable to the
Bank, would conduct the project annual audit, which would
include the regular audit of project financial statements and a
technical audit of the Statements of Affiliation Registry.
The technical audit component would take into account be the
results of the concurrent supervision activity carried out by the
Commission internal control groups.
M
Overall risk S M
75
The FM inherent risk is that which arises from the environment in which the Project is situated. The FM control
risk is the risk that the Project‘s FM system is inadequate to ensure Project funds are used economically and
efficiently and for the purpose intended. The overall FM risk is the combination of the inherent and control risks as
mitigated by the client control frameworks. The residual FM risk is the overall FM risk as mitigated by the Bank
supervision effort.

75
Risk type76
Risk
Rating
Comments / Risk mitigating measures
incorporated into project design
Residual
Risk
Rating
Standard
conditions
The Commission, with support of NAFIN, would prepare and
submit for the Bank‘s No Objection the Project Operational
Manual.
Bank FM
supervision
At least one full FM supervision mission would be carried out
per year, which would look into the operation of the control
systems and arrangements described in this annex. Desk reviews
of IFRs and audit reports would also be carried out.
76
The FM inherent risk is that which arises from the environment in which the Project is situated. The FM control
risk is the risk that the Project‘s FM system is inadequate to ensure Project funds are used economically and
efficiently and for the purpose intended. The overall FM risk is the combination of the inherent and control risks as
mitigated by the client control frameworks. The residual FM risk is the overall FM risk as mitigated by the Bank
supervision effort.
76
Annex 8: Procurement Arrangements
MEXICO: Social Protection System in Health
A. General
1. Procurement for the proposed Project would be carried out in accordance with the World
Bank‘s ―Guidelines: Procurement Under IBRD Loans and IDA Credits‖ (May 2004, revised
October 2006) and ―Guidelines: Selection and Employment of Consultants by World Bank
Borrowers‖ (May 2004, revised October 2006), and in line with the provisions stipulated in the
Loan Agreement. The various items under different expenditure categories are described below.
The different procurement or consultant selection methods, the need for pre-qualification, the
estimated costs, prior review requirements and the timeframe for each contract to be financed by
the Loan would be agreed upon between the Borrower and the Bank in the Procurement Plan.
The Procurement Plan would be updated at least annually or as required to reflect actual project
implementation needs and improvements in institutional capacity.
2. Procurement of Works: Not expected.
3. Procurement of Goods: Not expected.
4. Procurement of Non-Consulting Services: Under Component II, the Loan would finance
non-consultant services including capacity building activities such as training and workshops as
well as any expenditure incurred in connection with these activities; and printing, reproducing,
publishing and disseminating information and training materials. Most of these services would
be procured by shopping.
5. Selection of Consultants: Component II of the Project would entail the financing of
consultant services, training, and operational costs to strengthen the capacity of the Commission
and State Health Systems to effectively administer the entitlements of the Popular Health
insurance, including technical assistance for enhanced performance management and support to
States in preparing and carrying out reforms in the administration of the Popular Health
Insurance, improved knowledge of eligible beneficiaries about entitlements, strengthened health
risk management, and effective project coordination and management.
6. Firms: Most contracts for firms are expected to be procured using the Quality and Cost
Based Selection Method (QCBS). Consultant assignments of specific types, as agreed upon
previously with the Bank in the Procurement Plan, may be procured using the following
selection methods: (i) Quality Based Selection (QBS); (ii) Selection under a Fixed Budget (SFB),
especially for works supervision contracts; (iii) Least Cost Selection (LCS); (iv) Selection Based
on Consultants‘ Qualifications (CQS) for contracts estimated to cost below the equivalent of US
$200,000; and, exceptionally (v) Single Source Selection (SSS), under the circumstances
explained in paragraph 3.9 of the Consultants‘ Guidelines. The harmonized RFP (request for
proposals) would be used.
7. Individuals: Individual consultants would be hired to provide technical advisory and
Project support services and would be selected in accordance with Section V of the Consultants‘
Guidelines.

77
8. Operating Costs: Under Component II, the loan would finance reasonable expenditures
on recurrent costs, including logistics services for trainings and workshops, travel expenses of
approved personnel commissioned under Project activities, internet connectivity,
communications expenses, office consumables, printing and reproduction services, publication of
procurement notices, and publicity and marketing activities.
9. Others: The majority of the Loan resources would be transferred to States to finance the
eligible federal social contributions to the premium of the Popular Health Insurance (Component
I), for which no procurement activities would be necessary.
10. The procurement procedures and SBDs (standard bidding documents) to be used for each
procurement method, as well as model contracts, are presented in the Operational Manual.
B. Assessment of the agency’s capacity to implement procurement.
11. Project activities would be coordinated and implemented using the organizational
structures and staff of the CNPSS. The Office of the Head of the Commission would serve as the
Project Coordination Unit which will be responsible for overall Project coordination.
Procurement activities would be carried out by the CNPSS‘s General Directorate of
Administration and Finance with the assistance of the legal unit. Given that these units have not
had previous experience in Bank operations, their staff would be trained in the use of Bank
Guidelines.
12. The Procurement Specialist assigned to the Project carried out an assessment of the
capacity of the Commission to manage procurement processes under component II of the Project
on November 2009. The assessment reviewed the organizational structure for Project
implementation and the interaction and skills of staff responsible for procurement in the
Commission. The assessment concluded that the capacity is in general satisfactory, however,
identified key issues and risks concerning procurement management for Project implementation,
most importantly, the Commission‘s lack of experience with Bank-financed projects. The
recommended, main mitigation measures are summarized below:
Issue Responsible Target Date
Procurement training for staff carrying out
procurement activities within CNPSS
Bank May 31, 2010
SEPA training for technical and administrative staff Bank/Financial
Agent
May 31, 2010
13. The overall project risk for procurement is MODERATE.
C. Procurement Plan
14. At appraisal the Borrower presented a Procurement Plan which would serve as the basis
for Project implementation. This plan has been agreed upon between the Borrower and the
Project Team and will be made available in SEPA, in the Project‘s database and in the Bank‘s
external website. The Procurement Plan would be updated upon agreement with the Project Team

78
on an annual basis or as required, to reflect actual Project implementation and institutional
capacity needs.
D. Frequency of Procurement Supervision
15. In addition to the prior review of procurement processes, the assessment recommends an
annual supervision mission that would include an ex-post review of procurement processes. The
capacity assessment of the executing agency would be reviewed as part of the supervision
missions.
E. Details of the Procurement Arrangements Involving International Competition
1. Goods, Works, and Non-Consulting Services. Not expected
2. Consulting Services
(a) List of consulting assignments with a short list of international firms
1 2 3 4 5 6 7
Ref. No.
Description of
Assignment
Estimated
Cost
Selection
Method
Review
by Bank
(Prior / Post)
Expected
Proposals
Submission
Date
Comments
1 Base line study
for the health
risk management
program
220,000.00 QCBS Prior May 2010
2 Study of
supervision of
processes to
States
100,000.00 SFB Post May 2010
3 Final survey for
the evaluation of
the design of the
health risk
management
program
250,000.00 QCBS Prior June 2010
4 Evaluation of the
design of the
health risk
management
program
210,000.00
QCBS Prior August
2010
5 Evaluation of the
design of the
strategy to
empower
beneficiaries
200,000.00 QCBS Prior August 2010

79
(b) All consultant services (firms) costing above US $200,000, consultant services (individuals)
costing above US $100,000, and all single-source selection of consultants would be subject to
prior review by the Bank. (c) Short lists composed entirely of national consultants: services
estimated to cost less than the equivalent of US $500,000 per contract may be composed entirely
of national consultants as stipulated by paragraph 2.7 of the Consultant Guidelines.

80
Annex 9: Economic and Financial Analysis
MEXICO: Social Protection System in Health
1. In this annex, we describe the costs and benefits of the Project, specifically the gradual
expansion of the Popular Health Insurance to an additional 10 million individuals lacking
contributory social security.
2. For the purpose of the analysis, we used a model that hinges on age-specific elasticities
for health expenditure and mortality. We used this approach for all age-groups except neonates.
For the latter, elasticity data were not available. Instead, modeled reductions in neonatal
mortality were based on evidence for the impact of the utilization of a basic health care package.
The model produced estimates for avoided deaths. Using these estimates, we calculated the net
present value of deaths averted as:
PMV=GDPppp/total population)] / (1+)T} * (avoided deaths)
where is the discount rate and T is the expected remaining life years (based on the average life
expectancy at birth in Mexico of 75 years77
).
Furthermore, we estimated the net present value of the Project as:
NPV = ∑(Bt/(1+)t) -∑(Ct/(1+)
t)
where ∑ refers to the sum of all periods, t is the year of reference (ranges from 0 to T), Bt is the
estimate of the monetized benefits in a given period, is the discount rate, Ct is the monetized
cost in period t, and T refers to the implementation period of the Project.
3. For age-specific elasticities for health expenditure and mortality, we used data from
Mexico and the United States. We reviewed data from developing and developed countries. For
age-groups younger than 5 years of age, we obtained data from Mexico; for age-groups older
than 5 years, we only obtained data from the United States. Studies for the latter showed a wide
range of estimates (0.12 to 1.00). Upon a critical review of these studies, we chose a conservative
estimate of 0.17.
4. We believe that our approach is likely to underestimate the benefits of the Project for
two main reasons. First, the model captures only benefits that result from reductions in
mortality. Thus, it does not take into account benefits from reductions in morbidity and out-of-
pocket expenditures. Second, given the level of health expenditures in the United States, some of
the employed elasticity data reflect the ‗flat-of-the-curve‘. In contrast, at least for a proportion of
the population enrolled into the Popular Health Insurance, the returns from investment in health
are likely to be much higher. For example, the elasticities for health expenditure and maternal
mortality reported from other developing countries are significantly higher than those used in the
model.78
77
Based on Proyecciones de Población 2005-2050, CONAPO. 78
Bokhari et al (2006) reported maternal mortality elasticities ranging from 0.42 to 0.52.
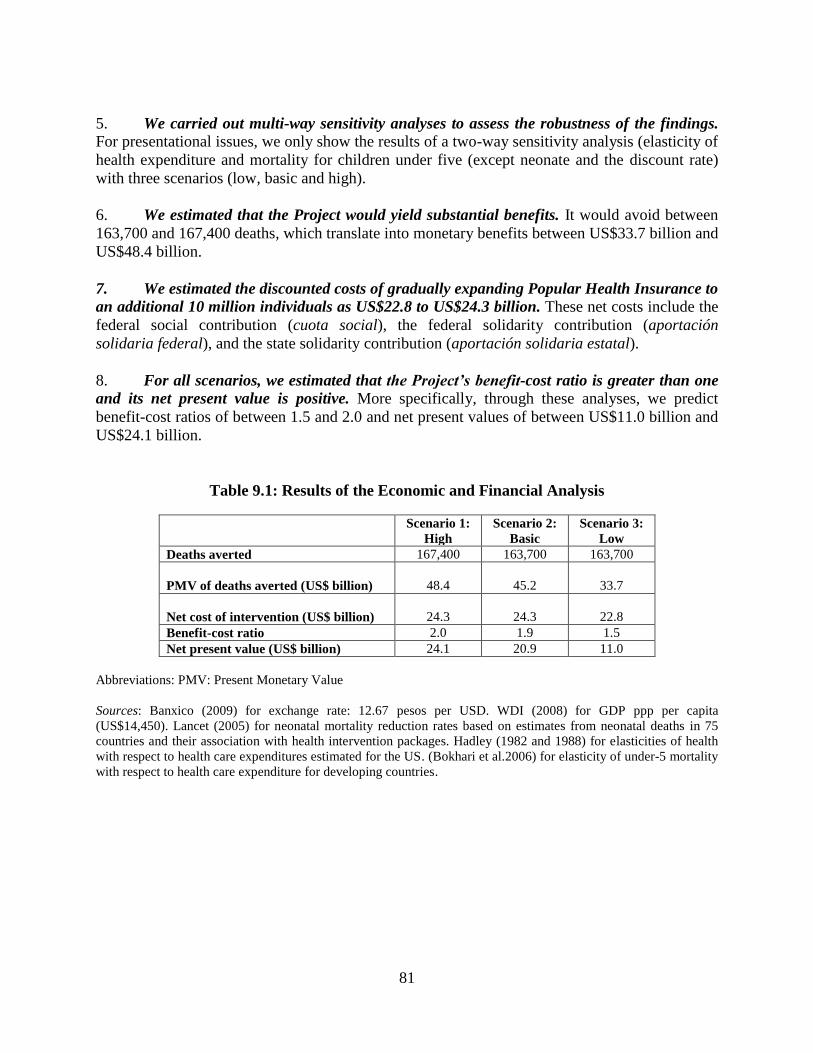
81
5. We carried out multi-way sensitivity analyses to assess the robustness of the findings.
For presentational issues, we only show the results of a two-way sensitivity analysis (elasticity of
health expenditure and mortality for children under five (except neonate and the discount rate)
with three scenarios (low, basic and high).
6. We estimated that the Project would yield substantial benefits. It would avoid between
163,700 and 167,400 deaths, which translate into monetary benefits between US$33.7 billion and
US$48.4 billion.
7. We estimated the discounted costs of gradually expanding Popular Health Insurance to
an additional 10 million individuals as US$22.8 to US$24.3 billion. These net costs include the
federal social contribution (cuota social), the federal solidarity contribution (aportación
solidaria federal), and the state solidarity contribution (aportación solidaria estatal).
8. For all scenarios, we estimated that the Project’s benefit-cost ratio is greater than one
and its net present value is positive. More specifically, through these analyses, we predict
benefit-cost ratios of between 1.5 and 2.0 and net present values of between US$11.0 billion and
US$24.1 billion.
Table 9.1: Results of the Economic and Financial Analysis
Scenario 1:
High
Scenario 2:
Basic
Scenario 3:
Low
Deaths averted 167,400 163,700 163,700
PMV of deaths averted (US$ billion)
48.4
45.2
33.7
Net cost of intervention (US$ billion)
24.3
24.3
22.8
Benefit-cost ratio 2.0 1.9 1.5
Net present value (US$ billion) 24.1 20.9 11.0
Abbreviations: PMV: Present Monetary Value
Sources: Banxico (2009) for exchange rate: 12.67 pesos per USD. WDI (2008) for GDP ppp per capita
(US$14,450). Lancet (2005) for neonatal mortality reduction rates based on estimates from neonatal deaths in 75
countries and their association with health intervention packages. Hadley (1982 and 1988) for elasticities of health
with respect to health care expenditures estimated for the US. (Bokhari et al.2006) for elasticity of under-5 mortality
with respect to health care expenditure for developing countries.

82
Annex 10: Safeguard Policy Issues
MEXICO: Social Protection System in Health
1. The proposed Project Development Objectives are to (i) initially preserve and later
expand the Popular Health Insurance’s coverage of people without contributory social
security, and (ii) strengthen the capacity of the Commission and State Health Systems to
effectively administer the entitlements of the Popular Health Insurance. Component I would
finance the Federal Government‘s social contribution to the premium of the Popular Health
Insurance to initially preserve and later expand the Popular Health Insurance‘s coverage of
eligible beneficiaries. Component II would finance technical assistance to strengthen the capacity
of the Commission and State Health Systems to effectively administer the entitlements of the
Popular Health insurance, including activities to enhance performance management, support
States in preparing and carrying out reforms in the administration of the Popular Health
Insurance, improve the knowledge of eligible beneficiaries about entitlements, strengthen health
risk management, and provide effective project coordination and management.
Environment
2. The proposed Project is not expected to have potentially adverse environmental effects;
accordingly, it has been classified as Environmental Category C and would not trigger the
Bank’s environmental safeguard policy (OP/BP 4.01). According to the Project description
above, the Loan would not finance the rehabilitation, refurbishment or construction of health
facilities, nor would it directly finance the provision of health services.
Social
3. The proposed Project is not expected to require any resettlements; therefore, it would
not trigger the Bank’s involuntary resettlement safeguard policy (OP 4.12). According to the
Project description above, the Loan would not finance the rehabilitation, refurbishment or
construction of health facilities, nor would it finance any other type of activity that could
potentially lead to resettlement.
4. The proposed Project is expected to have a positive impact on indigenous peoples; as
such, it triggers the Bank’s social safeguard policy for Indigenous Peoples (OP/BP 4.10).
5. Over the past decades, women in Mexico have been affected by cultural and social
factors that put them at a disadvantage for having contributory social security, including
corresponding health insurance and access to quality health services. The evaluation of the
Oportunidades program has shown that the migration of men for work and cultural changes have
lead Mexican women to increasingly become the heads of the households. Today, they constitute
30 percent of all Mexican households. Moreover, they generally play the role of the primary
care-taker of their families, caring for their children, grandchildren, elderly and sick family
members. Moreover, Mexican women often lack the social security benefits – including social
health insurance and access to quality health care services – that come with formal work and rely
heavily on the public sector for these. As the public health insurance for people lacking

83
contributory social security, the Popular Health Insurance can play an important role in the social
protection of these women‘s health, in particular, through improved access to health services.
6. With the goal of reducing maternal and child mortality, the SPSS has given pregnant
women, mothers and children priority enrollment in health insurance and access to health
care services.79
Accordingly, for pregnant women, it has designed and implemented a Strategy
for Healthy Pregnancies (Estrategia de Embarazo Saludable). Through the implementation of
the Health Insurance for a New Generation (Seguro Médico para una Nueva Generación), which
operates in conjunction with the Popular Health Insurance, the SPSS also has underscored the
importance of maternal and child health care by prioritizing their affiliation processes to mothers
and children. This strategy has lead to an increase in the number of female-headed beneficiary
families to the Popular Health Insurance, which in 2009 reached over 82 percent of the total
number of beneficiary families. Furthermore, 84.5 percent of Popular Health Insurance
beneficiary families living in localities that have an indigenous population of at least 40 percent
were headed by women.80
7. Also at a disadvantage for access health insurance and quality health services, the
indigenous population in Mexico is poor and lives mainly in marginalized rural areas with
unfavorable living-conditions. The indigenous population in Mexico is relatively diverse.81
It
constitutes nearly 10 percent of the total Mexican population and can be broken down into 62
different ethnic groups. Almost all of the indigenous population lives below the poverty line82
and, most of it, is located in marginalized rural areas. These areas usually have no clean water,
basic sewage systems, electricity, or flooring in the houses. For example, in 2005, nearly 30
percent of indigenous households in Mexico had no clean water, 45 percent lacked a basic
sewage system, 10 percent had no electricity, and 38 percent lived in houses with dirt floors.83
Moreover, such areas often prevent indigenous populations from being able to access even the
most basic services, including health care.
In addition to these poverty-associated disadvantages, the indigenous peoples have different
cultural perspectives about health and illness, for which the response of non-traditional health
care service and information systems need to be strengthened. Indigenous peoples face many
cultural barriers to accessing non-traditional health care services, such as language, difficulties in
describing symptoms, and different notions about sickness and the use of traditional medicine.
Often these barriers are due to a lack of adequate information for decision-making and,
indirectly, to differences in individual characteristics, such as lifestyle, place of residence, type
of occupation and income level. Moreover, the majority of indigenous peoples lack adequate
access to high quality, culturally-sensitive health care services84
. By the same token, the limited
understanding of indigenous cultures and perceptions by health care providers create another
barrier for indigenous peoples to access health services. Furthermore, their health status and
79
Still considering women as a target group, another objective of this strategy was to decrease maternal mortality. 80
CNPSS, Informe de Resultados, Primer Semestre, 2009. 81
Taken from 2005 Census. 82
Taken from 2005 Census. 83
Comisión Nacional para el Desarrollo de los Pueblos Indígenas; Indicadores Socioeconómicos de los Pueblos
Indígenas, 2000-2005. 84
Some progress has been achieved in this regard, such as an intercultural model that has been developed by the
Secretariat of Health.

84
needs are not properly identified by the health system‘s information systems. These cultural
barriers, together with poor economic and living conditions, have contributed to the health status
inequalities between the indigenous and the general population.
8. As a result, there are inequalities in health status between the indigenous population
and the general population in Mexico. The indigenous population in Mexico has a greater
tendency than the general population to suffer from so-called ‗poverty illnesses‘, such as acute
diarrheal diseases, acute respiratory infections, vector borne diseases and under-nutrition. For
example, 44 percent of indigenous children are malnourished, compared with a national average
of only 17 percent.85 In addition, the indigenous population is experiencing higher mortality
rates than the general population. For example, the mortality rate for children under 5 years
old86 in indigenous municipalities (55 deaths per 1,000 live births) is almost twice the national
average (30 deaths per 1,000 live births).87 Moreover, in some geographically isolated
indigenous communities (e.g., Coras, Tarahumaras and Huicholes), this rate reaches up to 100
deaths per 1,000 live births. Furthermore, the mortality rate of indigenous women during
pregnancy, childbirth, or puerperium is nearly triple that of non-indigenous women.
9. However, indigenous peoples have not benefited from the introduction of the Popular
Health Insurance as much as other populations, which means that a large portion of the
indigenous population is still not covered under it. In the first phases of scaling up affiliation,
the Popular Health Insurance prioritized families in the first and second income deciles. Despite
this, the total affiliation of the indigenous peoples88
still lagged behind that of the general
population. For example, in 2008, 60 percent of the total eligible population as compared to only
30 percent of the indigenous population was affiliated. Moreover, there is still a large eligible
indigenous population that lacks Popular Health insurance. For example, the Popular Health
Insurance has reached only 68.8 percent of the localities that have an indigenous population of at
least 40 percent. This equals 16,571 localities with approximately 4 million inhabitants out of a
total of 24,090 localities with 6.5 million inhabitants. Furthermore, only 27.5 percent of the
indigenous population has declared that it is enrolled in any type of health insurance at all (public
or private), 38 percent of whom are enrolled with the Popular Health Insurance.89
10. The proposed Project is expected to have a positive impact on indigenous peoples;
however, the Popular Health Insurance faces well-established cultural, geographic and
institutional barriers to enrolling them. First, indigenous peoples have a limited understanding
of the concept of insurance, which explains their sub-par demand for enrollment. Second, as
mentioned previously, they commonly reside in remote areas with limited or no access to non-
traditional health care services (see paragraph 12 of Annex 1). Data from external evaluations of
the Oportunidades program show that localities with a high proportion of indigenous peoples
have less access to health care services than localities with smaller indigenous populations. In
fact, the lack of health care services is the principal reason why the Oportunidades program has
85
Carlos Zolla, La Salud de Los Indigenas de Mexico, 2007. 86
In cities with more than 15,000 inhabitants. 87
2001-2006 National Program for the Development of Indigenous Peoples. 88
Popular Health Insurance does not identify their beneficiaries by their specific ethnicity but by whether or not they
consider themselves to be indigenous. 89
Of the rest of the 27.5 percent, 44 percent are enrolled in IMSS-Oportunidades and 18 percent in other
institutions. CDI-UNDP study.
85
not been able to cover some small, remote localities. However, since the establishment and
expansion of the Popular Health Insurance, health care services have also begun to reach more
remote areas. Third, the States have faced a financial incentive to enroll primarily population
groups other than indigenous peoples. States receive health care funding from the Federal
Government for implementing both the Popular Health Insurance and the Oportunidades
program. These programs, however, overlap by providing health services to the poor;
furthermore, by law, States only receive federal funds for either the subsidy for the health
component of the Oportunidades program or the Popular Health Insurance premium. Since the
Oportunidades subsidy is much less than the Popular Health Insurance premium, State Health
Systems can maximize federal transfers by affiliating population groups other than
Oportunidades beneficiaries into the Popular Health Insurance. As indigenous constitute
approximately 80 percent of Oportunidades beneficiaries, these financing arrangements may
have contributed to the sluggish enrollment of Oportunidades beneficiaries and indigenous
peoples into the Popular Health Insurance. However, as the affiliation to Popular Health
Insurance nears complete coverage, this incentive will become less powerful. State Health
Systems will have to increasingly focus on the enrollment of Oportunidades beneficiaries to
achieve the ambitious affiliation targets for the coming years and may even give them priority as
the enrollment of Oportunidades beneficiaries are streamlined (the regulatory framework allows
for the group enrollment of Oportunidades beneficiaries based on program databases).
11. In addition, new challenges facing the enrollment of indigenous peoples into the
Popular Health Insurance have emerged during the field research and consultations of the
IPP. Field research and consultations with indigenous communities, undertaken as part of the
IPP preparation, identified new challenges that affect the enrollment of process of the
indigenous. From the demand side, there is a lack of knowledge on how the system operates, for
instance, the need to renew enrollment after a three-year span. In addition, affiliation is also
difficult for the monolingual population – particularly, those that are older and poorer. From the
supply side, due to their remote location, State promoters of the Popular Health Insurance do not
have the means to travel to indigenous communities to carry out enrollment. Moreover, the
indigenous often lack identification documents, such as birth and marriage certificates, that are
needed for the enrollment process.
Indigenous Peoples Plan
12. To comply with the Bank’s social safeguard policy for Indigenous Peoples (OP/BP
4.10), the borrower has prepared an Indigenous Peoples Plan (IPP). As part of the IPP, a
social assessment has been prepared drawing on the monitoring, evaluation and supervision
activities of the National Commission for Social Protection in Health as well as field research
and consultations carried out during the project preparation. The overall assessment has
identified the main issues hindering the enrollment of indigenous peoples to the Popular Health
Insurance, which are summarized in paragraph 12. On the basis of these findings, a strategy has
been prepared, incorporating recommendations from the Commission for Indigenous
Development (CDI) that consider the many ethnic groups and languages of the indigenous as
well as their existing community structures. Consultations on the IPP took place in the States of
Yucatán, Oaxaca, Chiapas and Guerrero between December 17 and February 7, 2010. The IPP
was disclosed on the Commission‘s webpage in Spanish and in the Bank‘s InfoShop in English
86
on February 17, 2010. A summary of the main findings and recommendations of the IPP follows
(a full version of the IPP is available in the Project‘s file).
13. The IPP aims to address the identified enrollment issues to the Popular Health
Insurance and ensure that the indigenous population benefits from the Project in a culturally
appropriate manner. It has the following three main objectives:
1) To propose a participation strategy that addresses the barriers identified in the social
assessment in order to: (i) promote the enrollment of indigenous peoples in a way that is
compatible with their socio-economic and cultural characteristics; and (ii) raise their
awareness about the importance of health insurance as well as the rights to which they are
entitled as beneficiaries to the Popular Health Insurance.
2) To strengthen the capacity of the Commission: (i) to monitor the affiliation of indigenous
peoples to the Popular Health Insurance as it is scaled up; (ii) to monitor the delivery and
accreditation of health services in priority indigenous localities (as defined by the CDI)
and rural areas; (iii) to monitor indigenous peoples‘ satisfaction with the Popular Health
Insurance, incorporating indigenous localities in its semi-annual user satisfaction surveys;
and (iv) to improve the SPSS‘s information system by disaggregating data by gender and
ethnicity.
3) To strengthen the capacity of the State Health Systems to support the implementation of
the activities laid out in the IPP.
Strategy for the Participation of Indigenous Peoples in Popular Health Insurance90
14. Under its three objectives, the IPP proposes the following strategy for the participation
of indigenous peoples in the Popular Health Insurance. The PCU would ensure that this
strategy is carried out. It would perform a mid-term review of the progress of affiliating the
indigenous population, adjusting the affiliation strategy as necessary to achieve its objectives.
Lessons learned from the strategy may be used by the other areas of the Secretariat of Health
towards the improvement of their technical, operational and administrative processes for
indigenous municipalities.
15. The strategy is broken down into five activity areas that will be carried out during
Project implementation:
Under Objective 1:
1) A national dissemination campaign on the entitlements (guaranteed access to specific
health care interventions) and benefits (financial protection in health) of Popular Health
Insurance enrollees to promote the affiliation of indigenous populations as well as
increase their demand for quality, culturally-sensitive health services.
2) Strengthening the outreach capacity of State Health Systems to extend affiliation and
service delivery to priority indigenous and rural communities.
3) A complaint system for indigenous beneficiaries to exercise their rights regarding
Popular Health Insurance entitlements.
90
Indigenous Peoples Plan.

87
Under Objective 2:
4) Strengthening the capacity of the Commission to analyze the affiliation process for
indigenous peoples, the delivery and accreditation of health services in marginalized and
rural localities (as identified by the CDI), and the service utilization data for indigenous
peoples.
Under Objective 3:
5) Strengthen the capacity of the State Health Systems to support the implementation of
the activities laid out in the IPP.
A National Dissemination Campaign
16. The first activity area of the strategy is a national dissemination campaign with two
components: i) to promote the enrollment of the indigenous population to the Popular Health
Insurance through an improved understanding of the concept of insurance; and ii) to empower
indigenous beneficiaries through the active dissemination of knowledge about their beneficiary
rights and entitlements under the Popular Health Insurance. Together, both components are
expected to motivate indigenous beneficiaries to increase their demand for Popular Health
Insurance as well as quality, culturally-sensitive health services. The Commission would be
responsible for the design, execution and assessment of the national dissemination campaign. In
its design, the dissemination campaign would take into account the cultural backgrounds and
languages of different indigenous groups, and use appropriate media for reaching indigenous
peoples, such as community radio and the CDI radio system. Direct campaigns should be carried
out during the affiliation and re-affiliation processes. Forming a partnership with IMSS-
Oportunidades would further strengthen the campaign‘s implementation.
Strengthening of the Outreach Capacity of State Health Systems
17. The second activity area of the strategy is to strengthen the State Health Systems to
reach the indigenous population. This activity area comprises: (i) the strengthening of
enrollment systems at the State-level to better reach indigenous populations, including the use of
strategically located enrollment modules and mobile units; (ii) the incorporation of bilingual
indigenous peoples to facilitate enrollment; and (iii) training teams to better understand
indigenous population.
A Complaint System
18. The third activity area of the strategy is the establishment of a complaint system for
indigenous beneficiaries to exercise their rights regarding Popular Health Insurance
entitlements. The Commission would supervise the establishment of a simple mechanism for the
Popular Health Insurance‘s indigenous beneficiaries to present their complaints and grievances.
To this aim, the Commission would set up a specific complaint system to channel complaints and
find means to resolve them.
88
Strengthening of the Capacity of the Commission
19. The fourth activity area of the strategy regards the strengthening of the capacity of the
Commission to analyze indigenous population data and information. Activities would include:
i) improving the information system to track the affiliation of beneficiaries according to ethnicity
and gender; ii) ensuring that the indigenous population has access to the health care services they
need; and iii) following up with indigenous peoples who receive services on the quality and
appropriateness of those services.
Develop an action plan
20. The fifth activity area of the strategy is to strengthen the capacity of the State Health
Systems to support the implementation of the activities laid out in the IPP. The Commission, in
consultation with the States, would define an action plan for the implementation of these
activities. The action plan would take into consideration the areas of low implementation
capacity within the States and look for means to improve them.
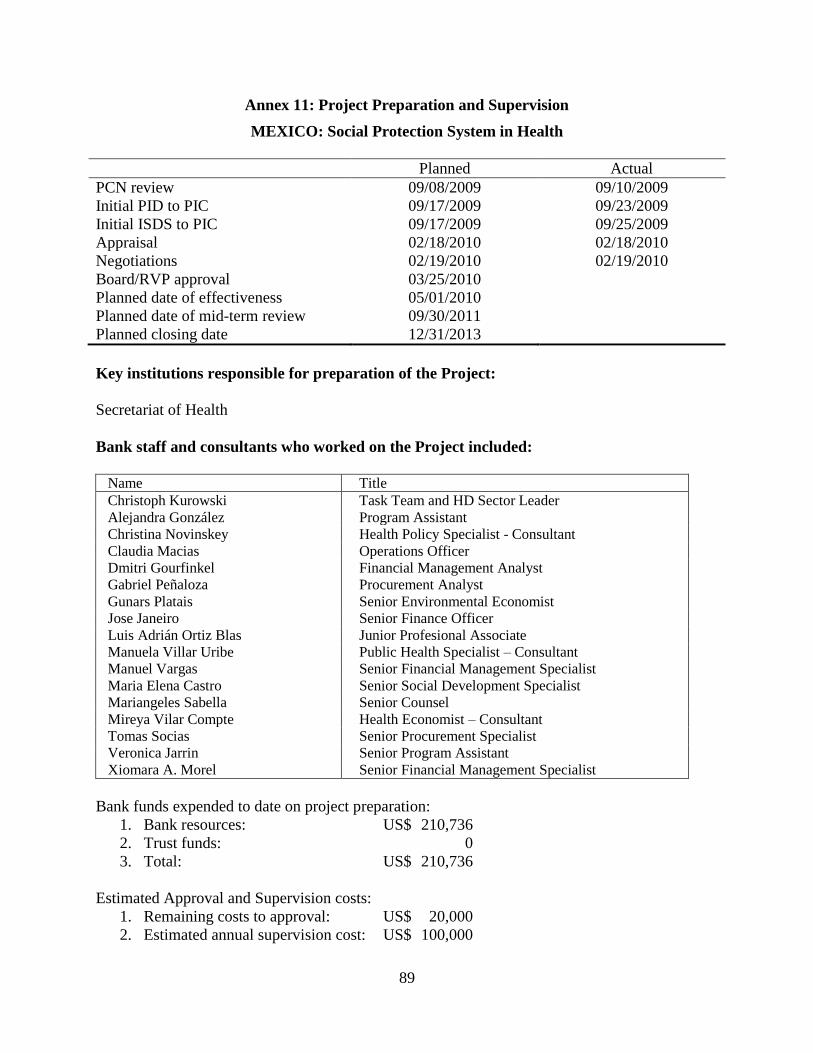
89
Annex 11: Project Preparation and Supervision
MEXICO: Social Protection System in Health
Planned Actual
PCN review 09/08/2009 09/10/2009
Initial PID to PIC 09/17/2009 09/23/2009
Initial ISDS to PIC 09/17/2009 09/25/2009
Appraisal 02/18/2010 02/18/2010
Negotiations 02/19/2010 02/19/2010
Board/RVP approval 03/25/2010
Planned date of effectiveness 05/01/2010
Planned date of mid-term review 09/30/2011
Planned closing date 12/31/2013
Key institutions responsible for preparation of the Project:
Secretariat of Health
Bank staff and consultants who worked on the Project included:
Name Title
Christoph Kurowski Task Team and HD Sector Leader
Alejandra González Program Assistant
Christina Novinskey Health Policy Specialist - Consultant
Claudia Macias Operations Officer
Dmitri Gourfinkel Financial Management Analyst
Gabriel Peñaloza Procurement Analyst
Gunars Platais Senior Environmental Economist
Jose Janeiro Senior Finance Officer
Luis Adrián Ortiz Blas Junior Profesional Associate
Manuela Villar Uribe Public Health Specialist – Consultant
Manuel Vargas Senior Financial Management Specialist
Maria Elena Castro Senior Social Development Specialist
Mariangeles Sabella Senior Counsel
Mireya Vilar Compte Health Economist – Consultant
Tomas Socias Senior Procurement Specialist
Veronica Jarrin Senior Program Assistant
Xiomara A. Morel Senior Financial Management Specialist
Bank funds expended to date on project preparation:
1. Bank resources: US$ 210,736
2. Trust funds: 0
3. Total: US$ 210,736
Estimated Approval and Supervision costs:
1. Remaining costs to approval: US$ 20,000
2. Estimated annual supervision cost: US$ 100,000
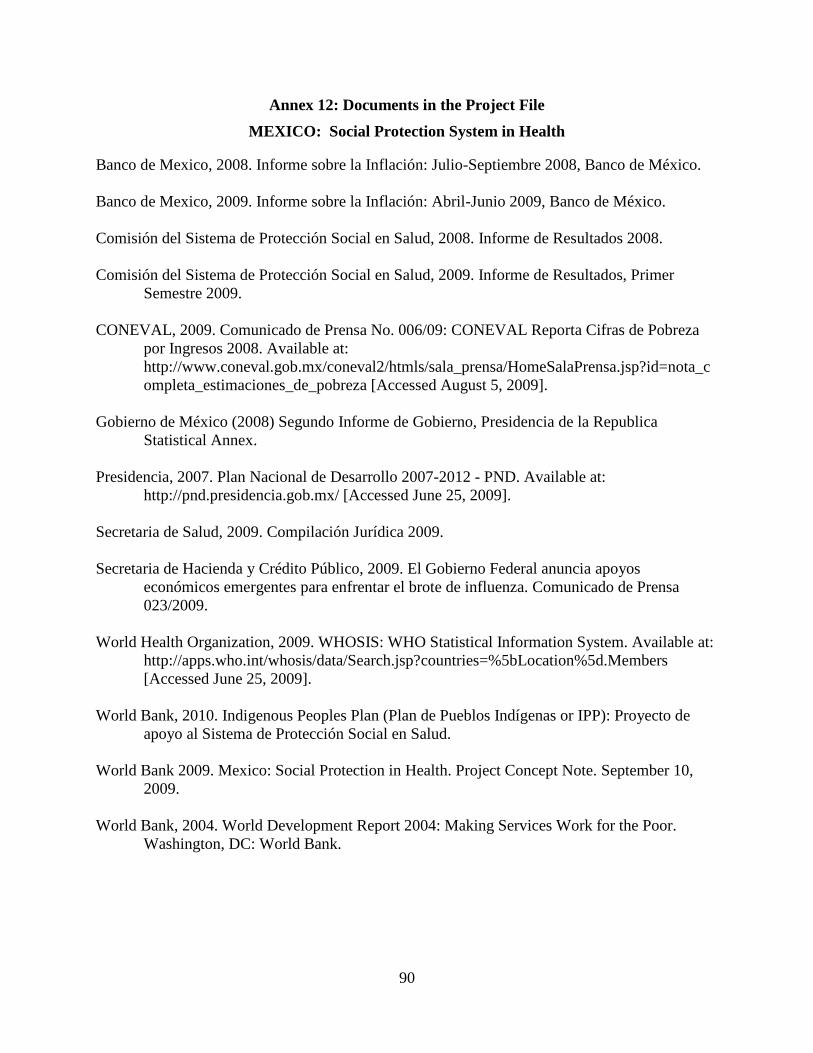
90
Annex 12: Documents in the Project File
MEXICO: Social Protection System in Health
Banco de Mexico, 2008. Informe sobre la Inflación: Julio-Septiembre 2008, Banco de México.
Banco de Mexico, 2009. Informe sobre la Inflación: Abril-Junio 2009, Banco de México.
Comisión del Sistema de Protección Social en Salud, 2008. Informe de Resultados 2008.
Comisión del Sistema de Protección Social en Salud, 2009. Informe de Resultados, Primer
Semestre 2009.
CONEVAL, 2009. Comunicado de Prensa No. 006/09: CONEVAL Reporta Cifras de Pobreza
por Ingresos 2008. Available at:
http://www.coneval.gob.mx/coneval2/htmls/sala_prensa/HomeSalaPrensa.jsp?id=nota_c
ompleta_estimaciones_de_pobreza [Accessed August 5, 2009].
Gobierno de México (2008) Segundo Informe de Gobierno, Presidencia de la Republica
Statistical Annex.
Presidencia, 2007. Plan Nacional de Desarrollo 2007-2012 - PND. Available at:
http://pnd.presidencia.gob.mx/ [Accessed June 25, 2009].
Secretaria de Salud, 2009. Compilación Jurídica 2009.
Secretaria de Hacienda y Crédito Público, 2009. El Gobierno Federal anuncia apoyos
económicos emergentes para enfrentar el brote de influenza. Comunicado de Prensa
023/2009.
World Health Organization, 2009. WHOSIS: WHO Statistical Information System. Available at:
http://apps.who.int/whosis/data/Search.jsp?countries=%5bLocation%5d.Members
[Accessed June 25, 2009].
World Bank, 2010. Indigenous Peoples Plan (Plan de Pueblos Indígenas or IPP): Proyecto de
apoyo al Sistema de Protección Social en Salud.
World Bank 2009. Mexico: Social Protection in Health. Project Concept Note. September 10,
2009.
World Bank, 2004. World Development Report 2004: Making Services Work for the Poor.
Washington, DC: World Bank.
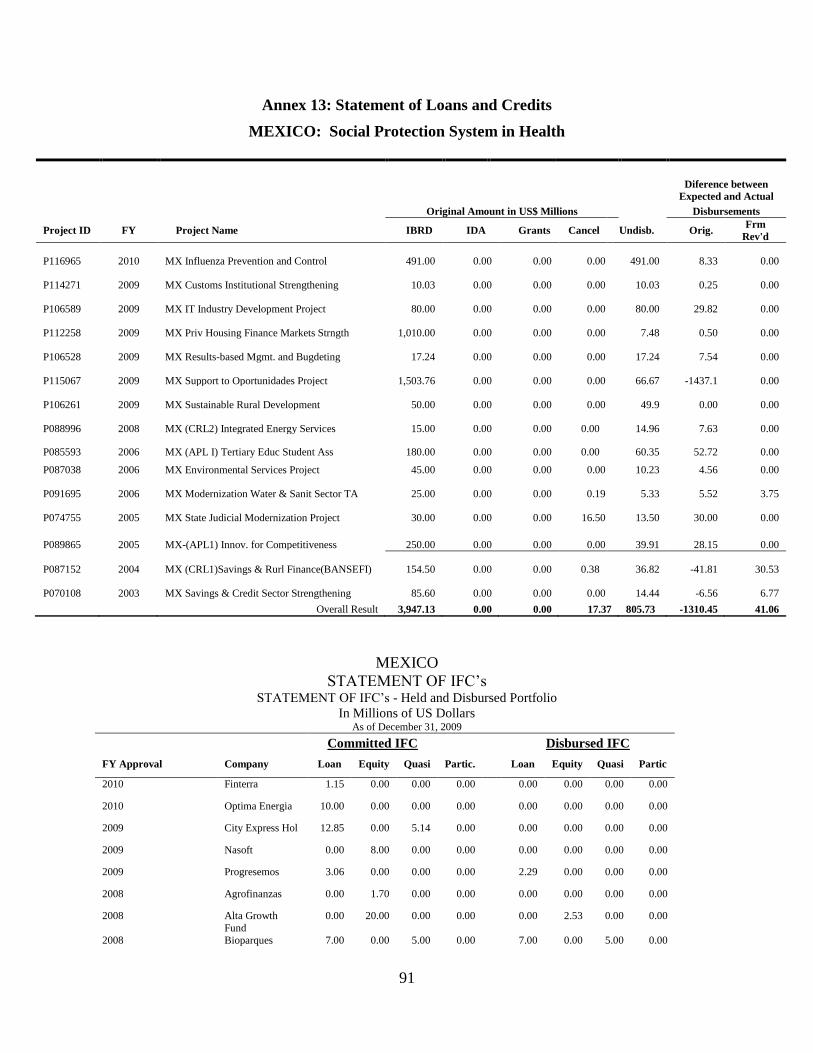
91
Annex 13: Statement of Loans and Credits
MEXICO: Social Protection System in Health
Diference between
Expected and Actual
Original Amount in US$ Millions Disbursements
Project ID FY Project Name IBRD IDA Grants Cancel Undisb. Orig. Frm
Rev'd
P116965 2010 MX Influenza Prevention and Control 491.00 0.00 0.00 0.00 491.00 8.33 0.00
P114271 2009 MX Customs Institutional Strengthening 10.03 0.00 0.00 0.00 10.03 0.25 0.00
P106589 2009 MX IT Industry Development Project 80.00 0.00 0.00 0.00 80.00 29.82 0.00
P112258 2009 MX Priv Housing Finance Markets Strngth 1,010.00 0.00 0.00 0.00 7.48 0.50 0.00
P106528 2009 MX Results-based Mgmt. and Bugdeting 17.24 0.00 0.00 0.00 17.24 7.54 0.00
P115067 2009 MX Support to Oportunidades Project 1,503.76 0.00 0.00 0.00 66.67 -1437.1 0.00
P106261 2009 MX Sustainable Rural Development 50.00 0.00 0.00 0.00 49.9 0.00 0.00
P088996 2008 MX (CRL2) Integrated Energy Services 15.00 0.00 0.00 0.00 14.96 7.63 0.00
P085593 2006 MX (APL I) Tertiary Educ Student Ass 180.00 0.00 0.00 0.00 60.35 52.72 0.00
P087038 2006 MX Environmental Services Project 45.00 0.00 0.00 0.00 10.23 4.56 0.00
P091695 2006 MX Modernization Water & Sanit Sector TA 25.00 0.00 0.00 0.19 5.33 5.52 3.75
P074755 2005 MX State Judicial Modernization Project 30.00 0.00 0.00 16.50 13.50 30.00 0.00
P089865 2005 MX-(APL1) Innov. for Competitiveness 250.00 0.00 0.00 0.00 39.91 28.15 0.00
P087152 2004 MX (CRL1)Savings & Rurl Finance(BANSEFI) 154.50 0.00 0.00 0.38 36.82 -41.81 30.53
P070108 2003 MX Savings & Credit Sector Strengthening 85.60 0.00 0.00 0.00 14.44 -6.56 6.77
Overall Result 3,947.13 0.00 0.00 17.37 805.73 -1310.45 41.06
MEXICO
STATEMENT OF IFC‘s STATEMENT OF IFC‘s - Held and Disbursed Portfolio
In Millions of US Dollars As of December 31, 2009
Committed IFC Disbursed IFC
FY Approval Company Loan Equity Quasi Partic. Loan Equity Quasi Partic
2010 Finterra 1.15 0.00 0.00 0.00 0.00 0.00 0.00 0.00
2010 Optima Energia 10.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
2009 City Express Hol 12.85 0.00 5.14 0.00 0.00 0.00 0.00 0.00
2009 Nasoft 0.00 8.00 0.00 0.00 0.00 0.00 0.00 0.00
2009 Progresemos 3.06 0.00 0.00 0.00 2.29 0.00 0.00 0.00
2008 Agrofinanzas 0.00 1.70 0.00 0.00 0.00 0.00 0.00 0.00
2008 Alta Growth
Fund
0.00 20.00 0.00 0.00 0.00 2.53 0.00 0.00
2008 Bioparques 7.00 0.00 5.00 0.00 7.00 0.00 5.00 0.00
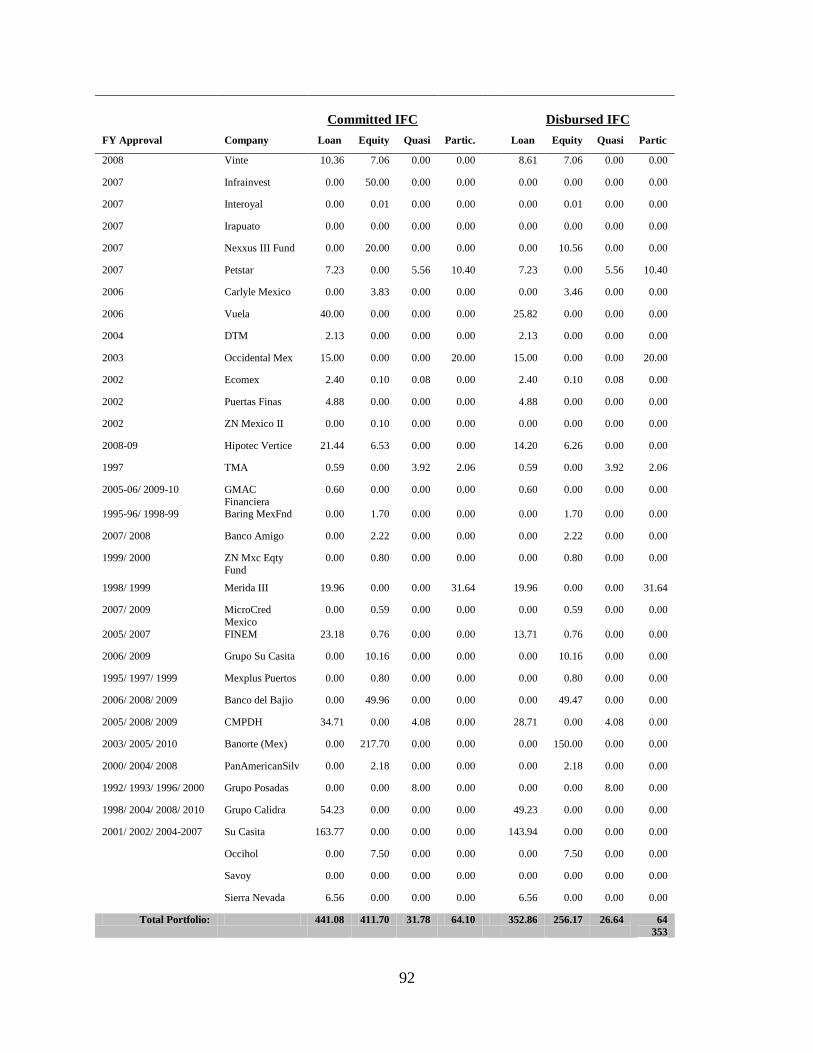
92
Committed IFC
Disbursed IFC
FY Approval Company Loan Equity Quasi Partic. Loan Equity Quasi Partic
2008 Vinte 10.36 7.06 0.00 0.00 8.61 7.06 0.00 0.00
2007 Infrainvest 0.00 50.00 0.00 0.00 0.00 0.00 0.00 0.00
2007 Interoyal 0.00 0.01 0.00 0.00 0.00 0.01 0.00 0.00
2007 Irapuato 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
2007 Nexxus III Fund 0.00 20.00 0.00 0.00 0.00 10.56 0.00 0.00
2007 Petstar 7.23 0.00 5.56 10.40 7.23 0.00 5.56 10.40
2006 Carlyle Mexico 0.00 3.83 0.00 0.00 0.00 3.46 0.00 0.00
2006 Vuela 40.00 0.00 0.00 0.00 25.82 0.00 0.00 0.00
2004 DTM 2.13 0.00 0.00 0.00 2.13 0.00 0.00 0.00
2003 Occidental Mex 15.00 0.00 0.00 20.00 15.00 0.00 0.00 20.00
2002 Ecomex 2.40 0.10 0.08 0.00 2.40 0.10 0.08 0.00
2002 Puertas Finas 4.88 0.00 0.00 0.00 4.88 0.00 0.00 0.00
2002 ZN Mexico II 0.00 0.10 0.00 0.00 0.00 0.00 0.00 0.00
2008-09 Hipotec Vertice 21.44 6.53 0.00 0.00 14.20 6.26 0.00 0.00
1997 TMA 0.59 0.00 3.92 2.06 0.59 0.00 3.92 2.06
2005-06/ 2009-10 GMAC
Financiera
0.60 0.00 0.00 0.00 0.60 0.00 0.00 0.00
1995-96/ 1998-99 Baring MexFnd 0.00 1.70 0.00 0.00 0.00 1.70 0.00 0.00
2007/ 2008 Banco Amigo 0.00 2.22 0.00 0.00 0.00 2.22 0.00 0.00
1999/ 2000 ZN Mxc Eqty
Fund
0.00 0.80 0.00 0.00 0.00 0.80 0.00 0.00
1998/ 1999 Merida III 19.96 0.00 0.00 31.64 19.96 0.00 0.00 31.64
2007/ 2009 MicroCred
Mexico
0.00 0.59 0.00 0.00 0.00 0.59 0.00 0.00
2005/ 2007 FINEM 23.18 0.76 0.00 0.00 13.71 0.76 0.00 0.00
2006/ 2009 Grupo Su Casita 0.00 10.16 0.00 0.00 0.00 10.16 0.00 0.00
1995/ 1997/ 1999 Mexplus Puertos 0.00 0.80 0.00 0.00 0.00 0.80 0.00 0.00
2006/ 2008/ 2009 Banco del Bajio 0.00 49.96 0.00 0.00 0.00 49.47 0.00 0.00
2005/ 2008/ 2009 CMPDH 34.71 0.00 4.08 0.00 28.71 0.00 4.08 0.00
2003/ 2005/ 2010 Banorte (Mex) 0.00 217.70 0.00 0.00 0.00 150.00 0.00 0.00
2000/ 2004/ 2008 PanAmericanSilv 0.00 2.18 0.00 0.00 0.00 2.18 0.00 0.00
1992/ 1993/ 1996/ 2000 Grupo Posadas 0.00 0.00 8.00 0.00 0.00 0.00 8.00 0.00
1998/ 2004/ 2008/ 2010 Grupo Calidra 54.23 0.00 0.00 0.00 49.23 0.00 0.00 0.00
2001/ 2002/ 2004-2007 Su Casita 163.77 0.00 0.00 0.00 143.94 0.00 0.00 0.00
Occihol 0.00 7.50 0.00 0.00 0.00 7.50 0.00 0.00
Savoy 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
Sierra Nevada 6.56 0.00 0.00 0.00 6.56 0.00 0.00 0.00
Total Portfolio: 441.08 411.70 31.78 64.10 352.86 256.17 26.64 64
353

93
Annex 14: Country at a Glance
MEXICO: Social Protection System in Health
Mexico at a glance 1/25/10
Latin Upper
Key D evelo pment Indicato rs America middle
M exico & Carib. income
(2008)
Population, mid-year (millions) 106.4 561 824
Surface area (thousand sq. km) 1,964 20,421 41,497
Population growth (%) 1.0 1.2 0.7
Urban population (% of to tal population) 77 78 75
GNI (Atlas method, US$ billions) 1,062.1 3,252 5,854
GNI per capita (Atlas method, US$) 9,990 5,801 7,107
GNI per capita (PPP, international $) 13,910 9,678 12,072
GDP growth (%) 1.3 5.7 5.8
GDP per capita growth (%) 0.3 4.4 5.0
(mo st recent est imate, 2003–2008)
Poverty headcount ratio at $1.25 a day (PPP, %) <2 8 ..
Poverty headcount ratio at $2.00 a day (PPP, %) 5 17 ..
Life expectancy at birth (years) 75 73 71
Infant mortality (per 1,000 live births) 29 22 21
Child malnutrition (% of children under 5) 3 4 ..
Adult literacy, male (% of ages 15 and o lder) 94 92 95
Adult literacy, female (% of ages 15 and o lder) 91 90 93
Gross primary enro llment, male (% of age group) 114 120 112
Gross primary enro llment, female (% of age group) 111 116 109
Access to an improved water source (% of population) 95 91 95
Access to improved sanitation facilities (% of population) 81 78 83
N et A id F lo ws 1980 1990 2000 2008 a
(US$ millions)
Net ODA and official aid 55 156 -56 121
Top 3 donors (in 2007):
United States 9 23 24 84
Germany 15 9 15 28
France 15 51 -11 16
Aid (% of GNI) 0.0 0.1 0.0 0.0
Aid per capita (US$) 1 2 -1 1
Lo ng-T erm Eco no mic T rends
Consumer prices (annual % change) 26.3 26.7 9.5 5.1
GDP implicit deflator (annual % change) 33.4 28.1 12.1 6.6
Exchange rate (annual average, local per US$) 0.0 2.8 9.5 11.1
Terms of trade index (2000 = 100) 194 106 100 116
1980–90 1990–2000 2000–08
Population, mid-year (millions) 67.6 83.2 98.0 106.4 2.1 1.6 1.0
GDP (US$ millions) 194,851 262,710 581,428 1,088,128 1.1 3.1 2.7
Agriculture 9.0 7.8 4.2 3.8 0.8 1.5 2.1
Industry 33.6 28.4 28.0 37.1 1.1 3.8 1.9
M anufacturing 22.3 20.8 20.3 18.8 1.5 4.3 1.8
Services 57.4 63.7 67.8 59.1 1.4 2.9 3.1
Household final consumption expenditure 65.1 69.6 67.0 65.5 1.4 2.3 3.8
General gov't final consumption expenditure 10.0 8.4 11.1 10.3 2.4 1.8 0.4
Gross capital formation 27.2 23.1 23.9 26.4 -3.3 4.7 1.5
Exports o f goods and services 10.7 18.6 30.9 28.3 7.0 14.6 5.7
Imports of goods and services 13.0 19.7 32.9 30.5 1.0 12.3 6.3
Gross savings 22.0 20.3 20.5 24.9
Note: Figures in italics are for years other than those specified. 2008 data are preliminary. .. indicates data are not available.
a. A id data are for 2007.
Development Economics, Development Data Group (DECDG).
(average annual growth %)
(% of GDP)
6 4 2 0 2 4 6
0-4
15-19
30-34
45-49
60-64
75-79
percent of total population
Age distribution, 2007
Male Female
0
10
20
30
40
50
60
1990 1995 2000 2007
Mexico Latin America & the Caribbean
Under-5 mortality rate (per 1,000)
-10
-8
-6
-4
-2
0
2
4
6
8
95 05
GDP GDP per capita
Growth of GDP and GDP per capita (%)

94
Mexico
B alance o f P ayments and T rade 2000 2008
(US$ millions)
Total merchandise exports (fob) 166,121 291,343
Total merchandise imports (cif) 174,458 308,603
Net trade in goods and services -10,661 -24,340
Current account balance -18,684 -15,806
as a % of GDP -3.2 -1.5
Workers' remittances and
compensation of employees (receipts) 6,573 25,137
Reserves, including gold 35,577 95,298
C entral Go vernment F inance
(% of GDP)
Current revenue (including grants) 21.4 23.7
Tax revenue 10.6 8.2
Current expenditure 21.4 19.8
T echno lo gy and Infrastructure 2000 2007
Overall surplus/deficit -3.4 -2.1
Paved roads (% of to tal) 32.8 50.0
Highest marginal tax rate (%) Fixed line and mobile phone
Individual 40 28 subscribers (per 100 people) 27 82
Corporate 35 28 High technology exports
(% of manufactured exports) 22.4 17.1
External D ebt and R eso urce F lo ws
Enviro nment
(US$ millions)
Total debt outstanding and disbursed 150,901 203,984 Agricultural land (% of land area) 55 55
Total debt service 58,509 41,332 Forest area (% of land area) 33.7 33.0
Debt relief (HIPC, M DRI) – – Nationally protected areas (% of land area) .. 5.3
Total debt (% of GDP) 26.0 18.7 Freshwater resources per capita (cu. meters) 4,090 3,885
Total debt service (% of exports) 30.4 12.1 Freshwater withdrawal (billion cubic meters) 78.2 ..
Foreign direct investment (net inflows) 18,466 18,978 CO2 emissions per capita (mt) 3.9 4.1
Portfo lio equity (net inflows) 447 -3,503
GDP per unit o f energy use
(2005 PPP $ per kg of o il equivalent) 7.9 7.7
Energy use per capita (kg of o il equivalent) 1,533 1,702
Wo rld B ank Gro up po rtfo lio 2000 2009
(US$ millions)
IBRD
Total debt outstanding and disbursed 11,444 10,142
Disbursements 1,748 4,882
Principal repayments 1,330 654
Interest payments 892 204
IDA
Total debt outstanding and disbursed – –
Disbursements – –
P rivate Secto r D evelo pment 2000 2010 Total debt service – –
2000 2007
Time required to start a business (days) – 13 IFC (fiscal year)
Cost to start a business (% of GNI per capita) – 11.7 Total disbursed and outstanding portfo lio 1,234 1,184
Time required to register property (days) – 74 o f which IFC own account 723 798
Disbursements for IFC own account 179 209
Ranked as a major constraint to business 2000 2007 Portfo lio sales, prepayments and
(% of managers surveyed who agreed) repayments for IFC own account 66 134
Anticompetitive or informal practices .. 19.0
Corruption .. 17.8 M IGA
Gross exposure – –
Stock market capitalization (% of GDP) 21.5 38.8 New guarantees – –
Bank capital to asset ratio (%) 9.6 14.4
Note: Figures in italics are for years other than those specified. 2008 data are preliminary. 1/25/10
.. indicates data are not available. – indicates observation is not applicable.
Development Economics, Development Data Group (DECDG).
0 25 50 75 100
Control of corruption
Rule of law
Regulatory quality
Political stability
Voice and accountability
Country's percentile rank (0-100)higher values imply better ratings
2008
2000
Governance indicators, 2000 and 2008
Source: Kaufmann-Kraay-Mastruzzi, World Bank
IBRD, 5,769Other multi-
lateral, 4,883
Bilateral, 1,769
Private, 167,136
Composition of total external debt, 2008
US$ millions
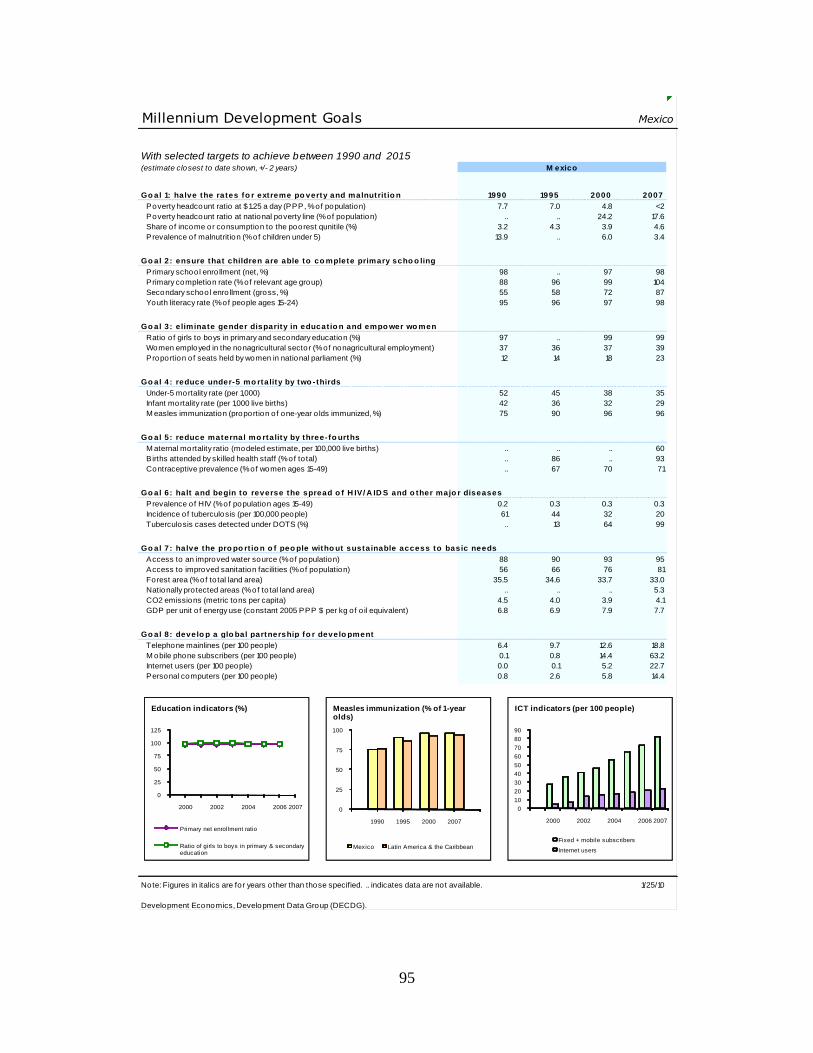
95
Millennium Development Goals Mexico
With selected targets to achieve between 1990 and 2015(estimate closest to date shown, +/- 2 years)
Go al 1: halve the rates fo r extreme po verty and malnutrit io n 1990 1995 2000 2007
Poverty headcount ratio at $1.25 a day (PPP, % of population) 7.7 7.0 4.8 <2
Poverty headcount ratio at national poverty line (% of population) .. .. 24.2 17.6
Share of income or consumption to the poorest qunitile (%) 3.2 4.3 3.9 4.6
Prevalence of malnutrition (% of children under 5) 13.9 .. 6.0 3.4
Go al 2: ensure that children are able to co mplete primary scho o ling
Primary school enro llment (net, %) 98 .. 97 98
Primary completion rate (% of relevant age group) 88 96 99 104
Secondary school enro llment (gross, %) 55 58 72 87
Youth literacy rate (% of people ages 15-24) 95 96 97 98
Go al 3: e liminate gender disparity in educat io n and empo wer wo men
Ratio of girls to boys in primary and secondary education (%) 97 .. 99 99
Women employed in the nonagricultural sector (% of nonagricultural employment) 37 36 37 39
Proportion of seats held by women in national parliament (%) 12 14 18 23
Go al 4: reduce under-5 mo rtality by two -thirds
Under-5 mortality rate (per 1,000) 52 45 38 35
Infant mortality rate (per 1,000 live births) 42 36 32 29
M easles immunization (proportion of one-year o lds immunized, %) 75 90 96 96
Go al 5: reduce maternal mo rtality by three-fo urths
M aternal mortality ratio (modeled estimate, per 100,000 live births) .. .. .. 60
B irths attended by skilled health staff (% of to tal) .. 86 .. 93
Contraceptive prevalence (% of women ages 15-49) .. 67 70 71
Go al 6: halt and begin to reverse the spread o f H IV/ A ID S and o ther majo r diseases
Prevalence of HIV (% of population ages 15-49) 0.2 0.3 0.3 0.3
Incidence of tuberculosis (per 100,000 people) 61 44 32 20
Tuberculosis cases detected under DOTS (%) .. 13 64 99
Go al 7: halve the pro po rt io n o f peo ple witho ut sustainable access to basic needs
Access to an improved water source (% of population) 88 90 93 95
Access to improved sanitation facilities (% of population) 56 66 76 81
Forest area (% of to tal land area) 35.5 34.6 33.7 33.0
Nationally protected areas (% of to tal land area) .. .. .. 5.3
CO2 emissions (metric tons per capita) 4.5 4.0 3.9 4.1
GDP per unit o f energy use (constant 2005 PPP $ per kg of o il equivalent) 6.8 6.9 7.9 7.7
Go al 8: develo p a glo bal partnership fo r develo pment
Telephone mainlines (per 100 people) 6.4 9.7 12.6 18.8
M obile phone subscribers (per 100 people) 0.1 0.8 14.4 63.2
Internet users (per 100 people) 0.0 0.1 5.2 22.7
Personal computers (per 100 people) 0.8 2.6 5.8 14.4
Note: Figures in italics are for years other than those specified. .. indicates data are not available. 1/25/10
Development Economics, Development Data Group (DECDG).
M exico
0
25
50
75
100
125
2000 2002 2004 2006 2007
Primary net enrollment ratio
Ratio of girls to boys in primary & secondary education
Education indicators (%)
0
10
20
30
40
50
60
70
80
90
2000 2002 2004 2006 2007
Fixed + mobile subscribers
Internet users
ICT indicators (per 100 people)
0
25
50
75
100
1990 1995 2000 2007
Mexico Latin America & the Caribbean
Measles immunization (% of 1-year olds)
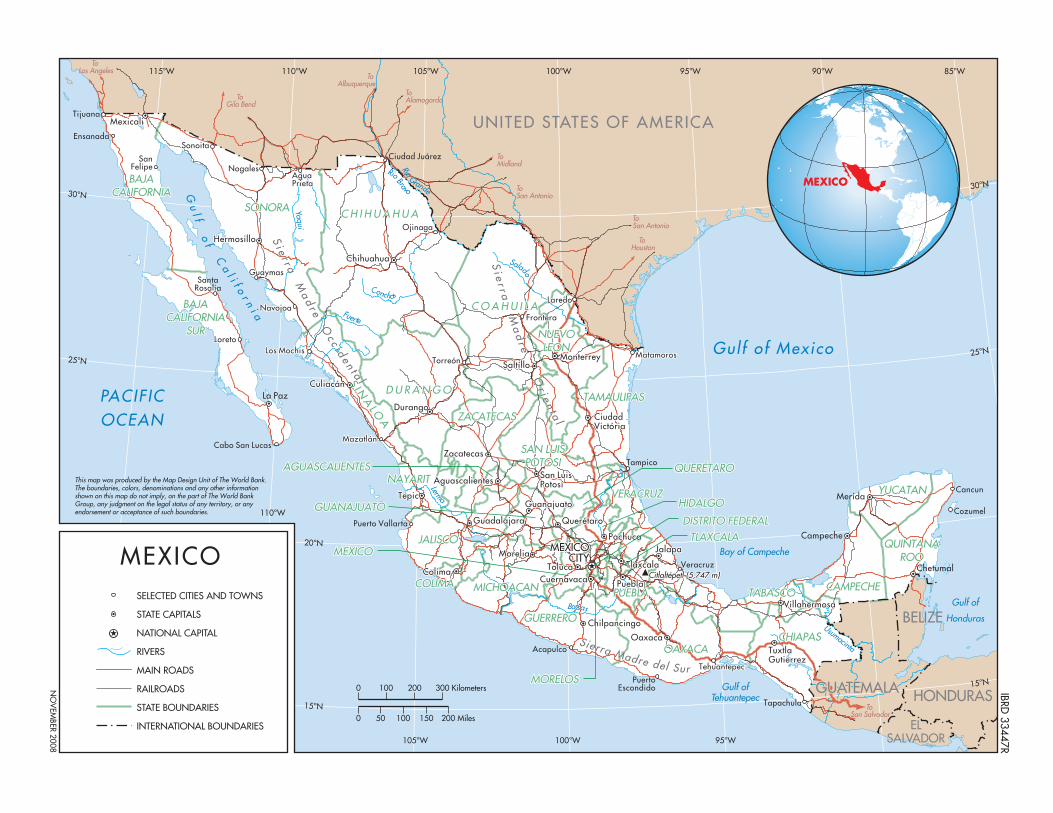
Citlaltépetl (5,747 m) Citlaltépetl (5,747 m)
Si e r r a
Ma
dr e O
c c i d e n t a l
S ierra Madre del Sur
Si e
r r a M
ad
r e O
r i e nt a
l
CAMPECHECAMPECHE
CHIAPASCHIAPAS
TABASCOTABASCO
OAXACAOAXACA
GUERREROGUERRERO
COLIMACOLIMA
JALISCOJALISCO
NAYARITNAYARIT
ZACATECASZACATECAS
TAMAULIPASTAMAULIPAS
NUEVONUEVOLEONLEON
C O A H U I L AC O A H U I L A
C H I H U A H U AC H I H U A H U ASONORASONORA
D U R A N G OD U R A N G O
SAN LUISSAN LUISPOTOSIPOTOSI
MICHOACANMICHOACAN PUEBLAPUEBLA
VERACRUZVERACRUZ YUCATANYUCATAN
QUINTANAQUINTANAROOROO
S INA
LOA
S I NA
LOA
MazatlánMazatlán
TorreónTorreónMatamorosMatamoros
LaredoLaredo
OjinagaOjinaga
Los MochisLos Mochis
NavojoaNavojoa
NogalesNogalesSanSan
FelipeFelipe
LoretoLoreto
SonoitaSonoita
AguaAguaPrietaPrieta
GuaymasGuaymas
TehuantepecTehuantepec
FronteraFrontera
VillahermosaVillahermosa
TuxtlaTuxtlaGutierrezGutierrez
OaxacaOaxaca
ChilpancingoChilpancingo
ColimaColima
GuadalajaraGuadalajara
TepicTepic
DurangoDurango
SaltílloSaltíllo
ChihuahuaChihuahua
CuliacánCuliacán
HermosilloHermosillo
MexicaliMexicali
GuanajuatoGuanajuato
PachucaPachuca
AguascalientesAguascalientes
QuerétaroQuerétaro
MoreliaMoreliaTolucaToluca
CuernavacaCuernavaca PueblaPuebla
TlaxcalaTlaxcala
JalapaJalapa
San LuisSan LuisPotosíPotosí
CiudadCiudadVictóriaVictória
ZacatecasZacatecas
MonterreyMonterrey
MEXICOMEXICOCITYCITY
Yaqui
Rio Bravo
Fuerte
Salado
Lerma
Balsas
Conchos
BAJABAJACALIFORNIACALIFORNIA
BAJABAJACALIFORNIACALIFORNIA
SURSUR
MEXICOMEXICO
MORELOSMORELOS
DISTRITO FEDERALDISTRITO FEDERAL
HIDALGOHIDALGOGUANAJUATOGUANAJUATO
AGUASCALIENTESAGUASCALIENTES
TLAXCALATLAXCALA
QUERÉTAROQUERÉTARO
Usuummacinta Rio Grande
GUATEMALAGUATEMALATapachula
PuertoEscondido
Acapulco
Puerto Vallarta
Mazatlán
TorreónMatamoros
Laredo
Ojinaga
Los Mochis
Navojoa
Nogales
Ensanada
Tijuana
SanFelipe
SantaRosalia
Loreto
Cabo San Lucas
Sonoita
AguaPrieta
Ciudad Juárez
Guaymas
Veracruz
Tampico
Tehuantepec
Cozumel
Cancun
Frontera
Chetumal
Merida
Villahermosa
Campeche
TuxtlaGutierrez
Oaxaca
Chilpancingo
Colima
Guadalajara
Tepic
Durango
Saltíllo
Chihuahua
Culiacán
Hermosillo
Mexicali
La Paz
Guanajuato
Pachuca
Aguascalientes
Querétaro
MoreliaToluca
Cuernavaca Puebla
Tlaxcala
Jalapa
San LuisPotosí
CiudadVictória
Zacatecas
Monterrey
MEXICOCITY
CAMPECHE
CHIAPAS
TABASCO
OAXACA
GUERRERO
COLIMA
JALISCO
NAYARIT
ZACATECAS
TAMAULIPAS
NUEVOLEON
C O A H U I L A
C H I H U A H U A
BAJACALIFORNIA
BAJACALIFORNIA
SUR
SONORA
D U R A N G O
SAN LUISPOTOSI
MICHOACAN
MEXICO
MORELOS
DISTRITO FEDERAL
PUEBLA
HIDALGOVERACRUZ
GUANAJUATO
AGUASCALIENTES
TLAXCALA
YUCATAN
QUINTANAROO
S INA
LOA
QUERÉTARO
UNITED STATES OF AMERICA
GUATEMALA
BELIZE
HONDURAS
ELSALVADOR
Yaqui
Rio Grande
Rio Bravo
Fuerte
Salado
Lerma
Balsas
Usumacinta
Conchos
PACIFICOCEAN
Gulf of Mexico
Bay of Campeche
Gulf ofTehuantepec
Gulf of
Honduras
Gu
l f of C
al i f o
r ni a
To Los Angeles
To Gila Bend
To Albuquerque
To Alamogordo
To Midland
To San Antonio
To San Antonio
To Houston
To San Salvador
Si e r r a
Ma
dr e O
c c i d e n t a l
S ierra Madre del Sur
Si e
r r a M
ad
r e O
r i e nt a
l
Citlaltépetl (5,747 m)
115°W
30°N30°N
25°N
15°N
25°N
20°N
15°N
110°W
110°W
105°W 100°W 95°W 90°W
105°W 100°W 95°W
85°W
MEXICO
This map was produced by the Map Design Unit of The World Bank. The boundaries, colors, denominations and any other informationshown on this map do not imply, on the part of The World BankGroup, any judgment on the legal status of any territory, or anyendorsement or acceptance of such boundaries.
0 100 200
0 50 100 150 200 Miles
300 Kilometers IBRD 33447R
NO
VEM
BER 2008
MEXICOSELECTED CITIES AND TOWNS
STATE CAPITALS
NATIONAL CAPITAL
RIVERS
MAIN ROADS
RAILROADS
STATE BOUNDARIES
INTERNATIONAL BOUNDARIES
97
Annex 16: References
Mexico: Social Protection System in Health
Aday, L.A. & Andersen, R.M., 1984. The national profile of access to medical care: where do we
stand? American Journal of Public Health, 74(12), 1331-1339.
Anderson, J., Kaufmann, D. & Recanatini, F., 2004. Service Delivery, Poverty, and Corruption:
Common Threads from Diagnostic Surveys. Background paper for the WDR 2004.
Andrews, M. & Shah, A., 2003. Towards Citizen-oriented Local-level Budgets in Developing
Countries. Ensuring Accountability When there is No Bottom Line. Washington, DC:
World Bank.
Ávila, A. & Shamah Levy, 2006. "Diagnóstico de la magnitud de la desnutrición infantil en
México. In México ante los desafíos de desarrollo del milenio, Consejo Nacional de
Población, McKenzie. México: The University of Chicago.
Billings, J. & Teicholz, N., 1990. Uninsured patients in District of Columbia hospitals. Health
affairs (Project Hope), 9(4), 158-165.
Bitrán, R., Giedion, U. & Muñoz, R., 2004. Risk pooling, ahorro y prevención: Estudio regional
de Políticas para la protección de los más pobres de los efectos de los shocks de salud.
Washington, DC: World Bank.
Bleich, S.N. et al., 2007. Impact of insurance and supply of health professionals on coverage of
treatment for hypertension in Mexico: population based study. British Medical Journal,
335(7625), 875.
Blumel, M. & Busse, R., 2009. Disease Management Programs – Time to evaluate, Available at:
http://www.hpm.org/survey/de/a13/2 [Accessed January 20, 2010].
Bokhari, F., Gai, Y. & Gottret, P. 2006, Government health expenditures and health outcomes.
Health Economics, 16(3), 257-273.
Braveman, P. et al., 1993. Access to prenatal care following major Medicaid eligibility
expansions. Journal of the American Medical Association, 269(10), 1285.
Brown, K. et al., 1997. Problems found in the over-75s by the annual health check. The British
Journal of General Practice, 47(414), 31.
Busse, R., 2004. Disease management programs in Germany's statutory health insurance system.
Health Affairs, 23(3), 56.
Caldwell, J.C., 1986. Routes to low mortality in poor countries. Population and development
review, 12(2), 171-220.

98
Castano, R. & Zambrano, A., 2006. Biased selection within the social health insurance market in
Colombia. Health policy, 79(2-3), 313-324.
Cavagnero, E. et al., 2006. Health financing in Argentina: An empirical study of health care
utilization and health care expenditure, Discussion paper.
CNPSS, 2006 Indicadores Socioeconómicos de los Pueblos Indígenas, 2000-2005.
CNPSS, 2009. Informe de Resultados, Primer Semestre 2009.
Fihn, S.D. & Wicher, J.B., 1988. Withdrawing routine outpatient medical services. Journal of
general internal medicine, 3(4), 356-362.
Fireman, B., Bartlett, J. & Selby, J., 2004. Can disease management reduce health care costs by
improving quality? Health Affairs, 23(6), 63.
Florez, C., 2008. El impacto sobre el hogar de un evento adverso en salud: El efecto amortiguador
del aseguramiento. Informe final preliminar.
Franks, P., Clancy, C.M. & Gold, M.R., 1993. Health insurance and mortality. Jama, 270(6), 737-
741.
Freeman, H.E. et al., 1990. Uninsured working-age adults: characteristics and consequences.
Health Services Research, 24(6), 811-823.
Freeman, H.E. et al., 1987. Americans report on their access to health care. Health affairs
(Project Hope), 6(1), 6-8.
Gakidou, E. et al., 2006. Evaluating the Impact of the 2001-2006 Mexican Health Reform: an
Interim Report Card. The Lancet.
García Lopez, J., 2009. Grado de acceso geográfico a los servicios de salud. In La situación
demográfica de México 2008.
Gaviria, A., Medina, C. & Mejía, C., 2006. Evaluating The Impact Of Health Care Reform In
Colombia: From Theory To Practice. Bogota, Universidad de Los Andes-CEDE,
Documentos CEDE, 2682.
Giedion, U. & Villar Uribe, M., 2009. Colombia's Universal Health Insurance System. Health
Affairs, 28(3), 853-863.
Gobierno de México, 2008. Segundo Informe de Gobierno. Presidencia de la República
Statistical Annex,

99
Goetz, A.M. & Jenkins, R., 2002. Voice, accountability and human development: The emergence
of a new agenda. Background Paper for UNDP, Human Development Report 2002,
Occasional Paper 2002/4, New York.
Gómez-Dantés, O. et al., 1999. Evaluación de un programa de salud para población no asegurada.
Rev Saude Publica, 33(4), 401-412.
González-Pier, E. et al., 2007. Definición de prioridades para las intervenciones de salud en el
Sistema de Protección Social en Salud de México. Salud Pública de méxico,
49(suplemento 1).
Gottret, P. et al., Forthcoming. The Financial Crisis and Health: Lessons and Recommendations
from Previous Experience.
Greenberg, E.R. et al., 1988. Social and economic factors in the choice of lung cancer treatment.
A population-based study in two rural States. New England Journal of Medicine, 318(10),
612-617.
Hadley, J., Steinberg, E.P. & Feder, J., 1991. Comparison of uninsured and privately insured
hospital patients. Condition on admission, resource use, and outcome. Jama, 265(3), 374-
379.
Hafner-Eaton, C., 1993. Physician utilization disparities between the uninsured and insured:
comparisons of the chronically ill, acutely ill, and well nonelderly populations.
JOURNAL-AMERICAN MEDICAL ASSOCIATION, 269, 787-787.
Halevy-Levin, S. et al., 2008. Information Center on Patients'Rights & Services.
Hand, R. et al., 1991. Hospital variables associated with quality of care for breast cancer patients.
Jama, 266(24), 3429-3432.
Hayward, R., 1988. Inequalities in health services among insured Americans: do working-age
adults have less access to medical care than the elderly? New England Journal of
Medicine, 318:1507-1512.
Hernández-Torres, J. et al., 2008. Seguro Popular's initial evaluation of household catastrophic
health spending in Mexico. Revista de salud pública (Bogotá, Colombia), 10(1), 18.
Hofmarcher, M.M., Lietz, C. & Schnabl, A., 2005. Inefficiency in Austrian inpatient care: An
attempt to identify ailing providers. Department of Economics and Finance, HIS Institute
of Advances Studies, Vienna.
INEGI. 2009. Press Release. February 22, 2010
King, G. et al., 2009. Public policy for the poor? A randomised assessment of the Mexican
universal health insurance programme. The Lancet, 373, 1447-1454.

100
Kleinman, J.C., Gold, M. & Makuc, D., 1981. Use of ambulatory medical care by the poor:
another look at equity. Medical Care, 19(10), 1011-1029.
Knaul, F., Arreola, H. & Méndez, O., 2005. Protección Financiera en Salud: México 1992-2004.
Salud Pública de México, 47, 430-439.
Koppel, A. & Aaviksoo, A., 2007. Evaluation of health prevention projects - Estonia, Available
at: http://www.hpm.org/survey/ee/a10/1 [Accessed January 20, 2010].
Lave, J.R. et al., 1998. Cost-effectiveness of treatments for major depression in primary care
practice. Archives of General Psychiatry, 55(7), 645.
Linden, A., Adams, J.L. & Roberts, N., 2003. An assessment of the total population approach for
evaluating disease management program effectiveness. Disease Management, 6(2), 93-
102.
Lurie, N. et al., 1986. Termination of Medi-Cal benefits. A follow-up study one year later. The
New England journal of medicine, 314(19), 1266-1268.
Matsuda, R., 2007. Detailed planning for secure health care delivery.
Méon, P.G. & Weill, L., 2005. Does better governance foster efficiency? An aggregate frontier
analysis. Economics of Governance, 6(1), 75-90.
Miller, G. et al., 2002. The Well Person's Health Check: a population screening program in
indigenous communities in north Queensland. Australian health review: a publication of
the Australian Hospital Association, 25(6), 136.
Newacheck, P.W., 1988. Access to ambulatory care for poor persons. Health Services Research,
23(3), 401.
Newacheck, P.W., 1989. Improving access to health services for adolescents from economically
disadvantaged families. Pediatrics, 84(6), 1056.
Roberts, M.J. et al., 2004. Getting health reform right: a guide to improving performance and
equity, Oxford University Press, USA.
Roetzheim, R.G. et al., 1999. Effects of health insurance and race on early detection of cancer.
JNCI Journal of the National Cancer Institute, 91(16), 1409.
Schedler, A., 1999. Conceptualizing accountability. The self-restraining state: Power and
accountability in new democracies, 13–28.
Sepúlveda, J. et al., 2007. Improvement of child survival in Mexico: the diagonal approach. Salud
Pública de México, 49, 110-125.

101
Shah, A., 2005. On getting the giant to kneel: Approaches to a change in the bureaucratic culture.
Fiscal Management, 211–227.
SHCP, 2009. El Gobierno Federal anuncia apoyos económicos emergentes para enfrentar el brote
de influenza. Comunicado de Prensa 023/2009.
Short, P.F. & Lefkowitz, D.C., 1992. Encouraging preventive services for low-income children:
The effect of expanding Medicaid. Medical Care, 766-780.
Sosa-Rubi, S., Galarraga, O. & Harris, J., 2007. Heterogeneous Impact of the "Seguro Popular"
Program on the Utilization of Obstetrical Services in Mexico, 2001-2006: A Multinomial
Probit Model with a Discrete Endogenous Variable. NBER Working Paper.
Sparrow, R., 2008. Targeting the poor in times of crisis: the Indonesian health card. Health Policy
and Planning, 23(3), 188.
SPSS, 2006. Evaluación Financiera.
Villagra, V.G. & Ahmed, T., 2004. Effectiveness of a disease management program for patients
with diabetes. Health Affairs, 23(4), 255.
Weissman, J. & Epstein, A.M., 1989. Case mix and resource utilization by uninsured hospital
patients in the Boston metropolitan area. JAMA, 261(24), 3572-3576.
Weissman, J.S., Gatsonis, C. & Epstein, A.M., 1992. Rates of avoidable hospitalization by
insurance status in Massachusetts and Maryland. Jama, 268(17), 23882394.
Weissman, J.S. et al., 1991. Delayed access to health care: risk factors, reasons, and
consequences. Annals of Internal Medicine, 114(4), 325-331.
Wenneker, M.B., Weissman, J.S. & Epstein, A.M., 1990. The association of payer with utilization
of cardiac procedures in Massachusetts. Jama, 264(10), 1255-1260.
Woolhandler, S. & Himmelstein, D.U., 1988. Reverse targeting of preventive care due to lack of
health insurance. Jama, 259(19), 2872-2874.
World Bank, Forthcomming. A LAC Regional Study on Social Protection, Chapter 3 on Health.
World Bank, 2003. World Development Report 2004: Making services work for poor people.
Yergan, J. et al., 1988. Relationship between patient source of payment and the intensity of
hospital services. Medical Care, 26(11), 1111-1114.
Young, G.J. & Cohen, B.B., 1991. Inequities in hospital care, the Massachusetts experience.
Inquiry: a journal of medical care organization, provision and financing, 28(3), 255.
Zolla, C., 2007. La salud de los pueblos indígenas de México.