Tashia Seeba - Antibiotics and maxillofacial fractures
3
Prophylactic Antibiotics in Maxillofacial Fractures: A Requisite? S. Adalarasan, MDS, Alexander Mohan, MDS, MOMSRCPS(Glasgow), and Sanjay Pasupathy, MDS, DNB, MOMSRCPS(Glasgow) Abstract: The role of prophylactic antibiotics to prevent surgical wound infection (SWI) in the management of maxillofacial fractures is controversial. We carried out a retrospective study in 67 patients with 114 maxillofacial fractures, of which 9 patients each were in group 1 (no antibiotic) and group 3 (cefotaxime) and 49 in group 2 (penicillin). We had an overall SWI rate of 16.66%, of which 3 of group 1 (33.33%), 12 of group 2 (24.48%), and 2 of group 3 (22.22%) constituted the SWIs. Statistical analysis showed no significant dif- ference between the infection rates. A strong positive correlation was found between infection rate and the delay in treatment, and a similar correlation was found in the use of catgut and SWI. Our study sug- gests that prophylactic antibiotic therapy may not alter the incidence of surgical wound infection. Key Words: Prophylactic antibiotics, maxillofacial fractures, penicillin, maxilla, mandible (J Craniofac Surg 2010;21: 1009Y1011) M anagement of facial fractures is an important component of the practice of maxillofacial surgery. With the advent of im- proved armamentarium, open reductionYinternal fixation has gained increased popularity. As with any other surgical procedure, infection is one of the major factors complicating the healing process. Antibiotics have been used not only in the management of postsurgical infections, but also prophylactically to prevent them. With the scare of antibiotic resistance, the use of antibiotics for pre- vention of infections needs to be reviewed. In this context, a retrospective study was carried out to evaluate the necessity of routine antibiotic administration for prevention of infections in the management of patients with maxillofacial fractures. MATERIALS AND METHODS Patients who visited the department of maxillofacial surgery in our institution for the management of maxillofacial fractures between April 2002 and February 2005 were included in the study. Patients, irrespective of sex, with maxillofacial fractures re- quiring surgical treatment and patients who were willing to give informed consent were included in the study. Patients with pre- existing infections at the site of fracture, medically compromised patients, patients allergic to penicillin and cephalosporin group of drugs, and patients with a history of antibiotic intake during the preceding 30 days were excluded. Patients were divided into 3 groups as follows: & group 1: Control group (no antibiotic group), & group 2: crystalline penicillin 2 million units intravenously 30 min before surgery, or & group 3: cefotaxime 2 g intravenously 30 minutes before surgery. A total of 67 patients who fulfilled the previously mentioned criteria were included in the study. Of these, 9 patients were in group 1, 49 in group 2, and 9 in group 3. Surgical procedures were performed under general anesthe- sia. The surgical site was thoroughly prepared with povidone-iodine, and all universal aseptic measures were adhered to. Access to the surgical site was obtained intraorally, extraorally, or both, depending on the type and site of fracture. Open reductionYinternal fixation using miniplates was done in all the cases. The number of miniplates differed according to site of fracture and the adequacy of fixation. RESULTS The mean age in the study group was 33.4 years, ranging from 14 to 72 years. There were 62 males and 5 females in the study. A total of 38 patients had multiple fractures, whereas the remaining patients had fracture at a single site only, resulting in a total of 114 fractures. The distribution of fractures and the postoperative infec- tion rates in the corresponding sites are shown in Figure 1. The eti- ology of the fractures and their distribution are shown in Figure 2. Of the 114 fractures, 19 developed surgical wound infection (SWI), resulting in an overall infection rate of 16.66%. The age-wise distribution of fractures and the corresponding infection rates are shown in Figure 3. Three patients of group 1 (33.33%), 14 of group 2 (24.48%), and 2 (22.22%) of group 3 were diagnosed with SWI. Although all the cases of SWI in groups 1 and 3 contained multiple fractures, only 9 of 14 patients in group 2 had multiple fractures. Except for 2 pa- tients in group 2 in whom both the fractures were infected, all the others had only a single fracture site infected. With the exception of one, all the other 18 infected patients had an average delay in treatment of 6 or more days (5Y15 days). The overall delay in treatment averages around 3.94 days (2Y15 days) for all the 67 cases. This delay in treatment could be attributed to delay in referral from other hospitals. Approximately 39% patients in- cluded in the study had a period of delay of more than 4 days. A positive correlation (r = 0.44) between the delay in treatment and infection was observed. Of the 67 patients, an extraoral incision was required in 16, intraoral incisions in 15, and a combined approach in 36 patients. Of the 16 patients requiring extraoral approach, 3 patients (18.75%) had SWI, whereas only 2 (13.33%) of the 15 patients needing intraoral ORIGINAL ARTICLE The Journal of Craniofacial Surgery & Volume 21, Number 4, July 2010 1009 From Sri Manakula Vinayagar Medical College and Hospital, Pondicherry, India. Received December 16, 2009. Accepted for publication January 24, 2010. Address correspondence and reprint requests to Sanjay Pasupathy, MDS, DNB, MOMSRCPS(Glasgow), No. 16, Cannon St, Priyadarshini Nagar, Gorimedu, Pondicherry, India 605006; E-mail: sanjaypasupathy@ yahoo.co.in The authors report no conflict of interest. Copyright * 2010 by Mutaz B. Habal, MD ISSN: 1049-2275 DOI: 10.1097/SCS.0b013e3181e47d43 Copyright © 2010 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
-
Upload
tashia-seeba -
Category
Health & Medicine
-
view
63 -
download
1
Transcript of Tashia Seeba - Antibiotics and maxillofacial fractures

Prophylactic Antibiotics in MaxillofacialFractures: A Requisite?
S. Adalarasan, MDS, Alexander Mohan, MDS, MOMSRCPS(Glasgow),and Sanjay Pasupathy, MDS, DNB, MOMSRCPS(Glasgow)
Abstract: The role of prophylactic antibiotics to prevent surgicalwound infection (SWI) in the management of maxillofacial fracturesis controversial. We carried out a retrospective study in 67 patientswith 114 maxillofacial fractures, of which 9 patients each were ingroup 1 (no antibiotic) and group 3 (cefotaxime) and 49 in group 2(penicillin). We had an overall SWI rate of 16.66%, of which 3 ofgroup 1 (33.33%), 12 of group 2 (24.48%), and 2 of group 3 (22.22%)constituted the SWIs. Statistical analysis showed no significant dif-ference between the infection rates. A strong positive correlation wasfound between infection rate and the delay in treatment, and a similarcorrelation was found in the use of catgut and SWI. Our study sug-gests that prophylactic antibiotic therapy may not alter the incidenceof surgical wound infection.
Key Words: Prophylactic antibiotics, maxillofacial fractures,penicillin, maxilla, mandible
(J Craniofac Surg 2010;21: 1009Y1011)
M anagement of facial fractures is an important component ofthe practice of maxillofacial surgery. With the advent of im-
proved armamentarium, open reductionYinternal fixation has gainedincreased popularity. As with any other surgical procedure, infectionis one of the major factors complicating the healing process.
Antibiotics have been used not only in the management ofpostsurgical infections, but also prophylactically to prevent them.With the scare of antibiotic resistance, the use of antibiotics for pre-vention of infections needs to be reviewed.
In this context, a retrospective study was carried out to evaluatethe necessity of routine antibiotic administration for prevention ofinfections in the management of patients with maxillofacial fractures.
MATERIALS AND METHODSPatients who visited the department of maxillofacial surgery
in our institution for the management of maxillofacial fracturesbetween April 2002 and February 2005 were included in the study.
Patients, irrespective of sex, with maxillofacial fractures re-quiring surgical treatment and patients who were willing to give
informed consent were included in the study. Patients with pre-existing infections at the site of fracture, medically compromisedpatients, patients allergic to penicillin and cephalosporin group ofdrugs, and patients with a history of antibiotic intake during thepreceding 30 days were excluded.
Patients were divided into 3 groups as follows:& group 1: Control group (no antibiotic group),& group 2: crystalline penicillin 2 million units intravenously 30 min
before surgery, or& group 3: cefotaxime 2 g intravenously 30 minutes before surgery.
A total of 67 patients who fulfilled the previously mentionedcriteria were included in the study. Of these, 9 patients were in group1, 49 in group 2, and 9 in group 3.
Surgical procedures were performed under general anesthe-sia. The surgical site was thoroughly prepared with povidone-iodine,and all universal aseptic measures were adhered to. Access to thesurgical site was obtained intraorally, extraorally, or both, dependingon the type and site of fracture. Open reductionYinternal fixationusing miniplates was done in all the cases. The number of miniplatesdiffered according to site of fracture and the adequacy of fixation.
RESULTSThe mean age in the study group was 33.4 years, ranging
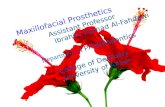
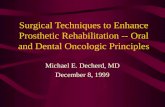
from 14 to 72 years. There were 62 males and 5 females in the study.A total of 38 patients had multiple fractures, whereas the remainingpatients had fracture at a single site only, resulting in a total of 114fractures. The distribution of fractures and the postoperative infec-tion rates in the corresponding sites are shown in Figure 1. The eti-ology of the fractures and their distribution are shown in Figure 2.
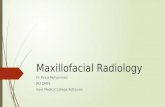
Of the 114 fractures, 19 developed surgical wound infection(SWI), resulting in an overall infection rate of 16.66%. The age-wisedistribution of fractures and the corresponding infection rates areshown in Figure 3.
Three patients of group 1 (33.33%), 14 of group 2 (24.48%),and 2 (22.22%) of group 3 were diagnosed with SWI. Although allthe cases of SWI in groups 1 and 3 contained multiple fractures, only9 of 14 patients in group 2 had multiple fractures. Except for 2 pa-tients in group 2 inwhomboth the fractureswere infected, all the othershad only a single fracture site infected.
With the exception of one, all the other 18 infected patientshad an average delay in treatment of 6 or more days (5Y15 days). Theoverall delay in treatment averages around 3.94 days (2Y15 days) forall the 67 cases. This delay in treatment could be attributed to delayin referral from other hospitals. Approximately 39% patients in-cluded in the study had a period of delay of more than 4 days. Apositive correlation (r = 0.44) between the delay in treatment andinfection was observed.
Of the 67 patients, an extraoral incision was required in 16,intraoral incisions in 15, and a combined approach in 36 patients. Ofthe 16 patients requiring extraoral approach, 3 patients (18.75%) hadSWI, whereas only 2 (13.33%) of the 15 patients needing intraoral
ORIGINAL ARTICLE
The Journal of Craniofacial Surgery & Volume 21, Number 4, July 2010 1009
From Sri Manakula Vinayagar Medical College and Hospital, Pondicherry,India.
Received December 16, 2009.Accepted for publication January 24, 2010.Address correspondence and reprint requests to Sanjay Pasupathy, MDS,
DNB, MOMSRCPS(Glasgow), No. 16, Cannon St, Priyadarshini Nagar,Gorimedu, Pondicherry, India 605006; E-mail: [email protected]
The authors report no conflict of interest.Copyright * 2010 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181e47d43
Copyright © 2010 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

incisions developed SWI. Twelve (33.33%) of 36 patients in whomacombined approach was required developed SWI. Of these 12,both incisions were infected in 2 patients (16.66%), whereas intraoralincisions alone were infected in 7 patients (58.33%), and extraoralincisions alone were infected in the remaining 3 patients (25%).
In a majority of patients with SWI (10/19), the duration ofsurgery were more than 90 minutes, ranging from 50 to 200 minutes.Also, no correlation was found between number of miniplates andscrews used and SWI.
In 7 (41.18%) of 19 patients with SWI, catgut sutureswere used for wound closure. There is a positive correlation (r = 1)between the use of catgut suture material and infection in the sur-gical site.
In the management of SWI, 9 patients required deliberateopening of the incision by the surgeon to evacuate pus and wereprescribed concomitant antibiotic therapy. Seven patients neededantibiotic therapy alone. Only one required readmission for incisionand drainage.
Statistical analysis was donewith Pearson W2 test. The infectionrates in all the 3 groups were found to be not statistically significant(the P values for groups 1, 2, and 3 were 0.71, 0.85, and 0.43, re-spectively), and also, intergroup evaluation did not reveal any statis-tical significance.
DISCUSSIONThe use of antibiotics in the management of maxillofacial
fractures is widespread with questionable rationale. Antibiotics havebeen used preoperatively to decrease the risk of SWI, but its role inpreventing infection has not been evaluated properly. The main goalsof antibiotic prophylaxis are to reduce incidence of SWI and to min-imize the adverse effect of antibiotics, especially the emergence ofresistant microorganisms.
In his landmark animal study that defined the scientific basisfor prophylaxis, Burke1 clearly demonstrated that the use of post-operative antibiotics alone actually violates the basic tenets of pro-phylaxis, as there is no antibiotic either in the systemic circulation orat the site of surgery when the microorganisms invade the wound.This has been supported by other research articles in the litera-
ture.2Y5 Hence, use of postoperative antibiotics in the name of pro-phylaxis seems to have no role in the prevention of SWI.
The criteria to identify SWI have been under a lot of scrutinyin recent times. Many studies3,4,6,7 have included pain and swellingas criteria for diagnosing SWI. But these factors are commonly seenas sequelae of routine inflammatory reaction after any surgicaltrauma, and they need not be pure indicators of SWI. Hence, we didnot include these factors in our study for assessing SWI. We in-cluded systemic increase in temperature and purulent discharge fromwound as the main parameters to diagnose SWI. It is well docu-mented in literature4,8 that systemic increase in temperature is one ofthe reliable indicators of infection, especially on the third postop-erative day, and the presence of purulent discharge from the woundwithin the first month postoperatively will obviously confirm thepresence of SWI.4,8
There are multiple risk factors involved, independent of eachother, which are predictive for subsequent SWI. These factors in-clude length of preoperative stay in hospital, compromised hostdefenses, surgical wound class, and duration of surgery. Garibaldiet al9 collected prospective epidemiological data, and their analysisof those data revealed that SWI was related to the length of preop-erative stay in hospital. A clinical practical evidence-based guide-lines by the Ministry of Health, Malaysia, suggest that preoperativestay of more than 3 days is associated with an increased risk of SWI.But in our institute, we had a standard protocol of admitting thepatients just 1 day before surgery.
Certain medical conditions such as poorly controlled diabe-tes, AIDS, and so on are said to result in decreased host defenses anda reduced resistance to infection and a high probability of devel-oping SWI. But there is no conclusive evidence for compromisedhost defenses and increased SWI in literature. Hence, in our study, tomaintain the homogeneity of sample, we excluded patients withthese conditions.
As the overwhelming majority of surgical management ofmaxillofacial fractures falls into class 2 (clean contaminated) varietyand all the cases in our study too were class 2 in nature, whether theroutine use of prophylactic antibiotics will fulfill those goals iscontroversial. Garibaldi et al9 and Culver et al10 showed that post-operative wound infection rate was related to the class of surgery.They also stated that the infection rate associated with class 1 sur-gery may be sufficiently low as not to warrant the use of prophylacticantibiotics. The infection rate associated with class 2 surgery,however, may be high enough to warrant the use of prophylacticantibiotics. The infection rate in class 2 surgeries varies between 6%
FIGURE 1. Distribution of fractures and the SWI.
FIGURE 2. Etiology of fractures and their distribution.
FIGURE 3. Age-wise distribution of fractures and thecorresponding SWI rates.
Adalarasan et al The Journal of Craniofacial Surgery & Volume 21, Number 4, July 2010
1010 * 2010 Mutaz B. Habal, MD
Copyright © 2010 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

and 20% in literature. The SWI rate in our study was 16.66%, whichfalls well within the SWI range of class 2 surgeries.
The use of preoperative antibiotics for management of max-illofacial fractures is well documented in literature.4,6,11,12 All thesestudies are having wide variance of infection rates, and this may beattributed to various factors such as patient selection, choice of an-tibiotics, and so forth. But in our study, the infection rates are muchless (16.66%) compared with those previous studies.
Surgical wound infections in maxillofacial trauma patientsdepend on various factors such as the type of fracture, delay intreatment, number of fractures, and treatment modality. The mostimportant among these seem to be the type of fracture, whether it iscompound, and the period of delay in treatment.
In the literature, many studies have shown that compoundfractures have more chance of infection than the others.7,13,14 In ourstudy in group 1, 3 of 14 compound fractures were infected, leadingto an infection rate of 21.42%, and in group 2, 14 of 78 compoundfractures were infected, leading to an infection rate of 17.94%. Asthe infection rate in both groups is similar in compound fractures, itis suggested that antibiotics are not playing much of a role in theprevention of SWI in this kind of fractures.
The maximum recommended delay in treatment of mandibularfractures and the type of treatment rendered have been the subject ofattention of numerous studies.14,15 The literature shows that delayedtreatment of fractures is associated with a greater rate of infection.14
Although Champy et al16 recommended treatment within the first12 hours of trauma, in our setup this is not practically possiblealways because of various factors such as availability of operationtheaters, cost factor associated with open reductions, and so on. Themean delay in treatment of fractures in our study is 4 days, and there isa positive correlation (r = +0.44) found between the delay and in-creased SWI. This could be attributed to the mobility of the frac-tured segments and concomitant development of infection.
A strong positive correlation (r = +1) was also found betweenthe use of catgut in multiple layer closures and SWI (7/17), leadingto an infection rate of 41.18%, which is also documented inliterature.17
CONCLUSIONSOur study suggests that prophylactic antibiotic therapy may
not alter the incidence of SWI. A multicenter, prospective, ran-domized controlled trial with large sample size is essential to eval-uate the advantage of prophylactic antibiotic therapy, if any, in themanagement of maxillofacial fractures.
REFERENCES1. Burke JF. The effective period of preventive antibiotic action in
experimental incisions and dermal lesions. Surgery 1961;50:161Y1682. Laskin DM. The use of prophylactic antibiotics for prevention of
postoperative infections. Oral Maxillofac Surg Clin North Am2003;15:155Y160
3. Miles BA, Porter JK, Ellis E. The efficacy of postoperative antibioticregimens in the open treatment of mandibular fractures: a prospectiverandomized trial. J Oral Maxillofac Surg 2006;64:576Y582
4. Abubaker O, Rollert MK. Post-operative antibiotic prophylaxis inmandibular fractures: a preliminary randomized, double blind, andplacebo-controlled clinical study. J Oral Maxillofac Surg 2001;59:1415Y1419
5. Peterson LJ. Principles of antibiotic therapy. In: Topazian RG, ed.Oral and Maxillofacial Infections. 3rd ed. Philadelphia, PA: WBSaunders Company, 1994:160Y197
6. Heit JM, Stevens MR, Jeffords K. Comparison of ceftriaxone withpenicillin for antibiotic prophylaxis for compound mandibular fractures.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;83:423Y426
7. Moreno JC, Fernandez A, Ortiz JA, et al. Complication rates associatedwith different treatments for mandibular fractures. J Oral MaxillofacSurg 2000;58:273Y280
8. Larson EL, Pearson ML. Guideline for prevention of surgical siteinfection. Infect Control Hosp Epidemiol 1999;20:248Y264
9. Garibaldi RA, et al. Risk factors for post-operative infections. Am J Med1991;91(suppl 3B):158Y163
10. Culver DH, Horan TC, Gaynes RP, et al. National Nosocomial InfectionsSurveillance System: surgical wound infection rates by wound classoperative procedure and patient risk index. Am J Med 1991;91(Suppl 3B):152Y157
11. Chole RA, Yee J. Antibiotic prophylaxis for facial fractures.A prospective, randomized clinical trial. Arch Otolaryngol Head NeckSurg 1987;113:1055Y1057
12. Zallen RD, Curry JT. A study of antibiotic usage in compoundmandibular fractures J Oral Surg 1975;33:431Y434
13. Edwards TJ, David DJ, Simpson DA, et al. The relationship betweenfracture severity and complication rate in miniplate osteosynthesis ofmandibular fractures. Br J Plast Surg 1994;47:310Y311
14. Maloney PL, Lincoln RE, Coyne CP. A protocol for management ofcompound mandibular fractures based on the time of injury to treatment.J Oral Maxillofac Surg 2001;60:133Y134
15. Biller JA, Pletcher SD, Goldberg AN, et al. Complications and time torepair of mandibular fractures. Laryngoscope 2002;115:769Y772
16. Champy, et al. Mandibular osteosynthesis by miniature screwed platesvia buccal approach. J Oral Maxillofac Surg 1978;6:14
17. Gabrielli F, Potenza C, Puddu P, et al. Suture materials and other factorsassociated with tissue reactivity, infection, and wound dehiscenceamong plastic surgery outpatients. Plast Reconstr Surg 2001;107:38Y45
The Journal of Craniofacial Surgery & Volume 21, Number 4, July 2010 Prophylactic Antibiotics in Maxillofacial Fracture
* 2010 Mutaz B. Habal, MD 1011
Copyright © 2010 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.