Renal Physiology
8
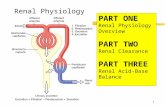
Renal Physiology Review
description
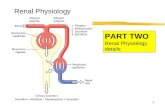
Renal Physiology. Review. 1 Arcuate artery 2 Interlobular artery 3 Afferent arteriole 4 Efferent arteriole. 5. 6. 7. 7. What is this process called?. Describe the mechanism when MAP drops from 160mm to 80mm - PowerPoint PPT Presentation
Transcript of Renal Physiology

Renal PhysiologyReview

1 Arcuate artery2 Interlobular artery3 Afferent arteriole4 Efferent arteriole
7
76
5


What is this process called?
Describe the mechanism when MAP drops from 160mm to 80mm Interlobular arteries and afferent arterioles dilate while efferent arterioles constrict What happens when MAP falls below 80mm Hg Acute renal failure

ElectrolytesWithin the proximal tubule sodium is
reabsorbed by active transport, which is regulated by angiotensin II
The reabsorption of sodium in the collecting ducts is increased by the action of aldosterone which activates ENaC channels in principal cells
ADH binds to V2 receptors on the basolateral surface of the cells of the collecting ducts causing insertion of aquaporins causing urine to become more concentrated Abnormally low levels of this hormone or defective V2 receptors results in diabetes insipidus

Phosphate and CalciumPTH inhibits phosphate reabsorption in the
proximal tubulePTH increases reabsorption of calcium and
magnesium from the distal tubule.The net increase in the ratio of serum
calcium to serum phosphate means PTH greatly increases the concentration of free calcium

Substance Proximal tubule Loop of Henle Distal tubule Collecting duct
GlucoseSLGT-2 (Apical) and GLUT-2
(basolateral)
Ureareabsorption (50%) via passive transport (solvent drag)
Secretion (urea transporter)
Reabsorption (urea transporter) in medullary collecting ducts
Sodiumreabsorption (65%) via Na-H antiporter & Na-Glucose symporter
reabsorption (25%, thick ascending, Na-K-2Cl symporter)
reabsorption (5%, Na-Cl symporter – aldosterone
reabsorption (5%, principal cells), stimulated by aldosterone via ENaC
Chloride reabsorption
reabsorption (passive by thin ascending, thick ascending, Na-K-2Cl symporter)
reabsorption (sodium-chloride symporter)
Waterabsorbed osmotically along with solutes
reabsorption (descending tubule)
reabsorption (regulated by ADH activating aquaporin channels
Bicarbonate
reabsorption (80-90%) via intra/extracellular carbonic anhydrase + denovo synthesis using glutamine -> ammonium
DeNovo synthesis by intercalated cells secreting H+
PotassiumPassive reabsorption (65%) due to concentrating effect
reabsorption (20%, thick ascending, Na-K-2Cl symporter)
-
secretion (common, via Na+/K+-ATPase, increased by aldosterone), or reabsorption (rare, hydrogen potassium ATPase)
Calcium
Reabsorption via basolateral calcium ATPase, Na-Ca exchanger & apical Ca channels
reabsorption (thick ascending) via passive transport
-
Magnesium
Reabsorption: Ca & magnesium compete, an excess of one can lead to excretion of the other
reabsorption (thick ascending)
reabsorption
Phosphatereabsorption (85%) via Na-phosphate cotransporter Inhibited by PTH
Carboxylatereabsorption (100%) via carboxylate transporters.
Where and by which transporters are the following substances reabsorbed or excreted:

Acid Base Balance
De-Novo bicarbonate is producedwithin the proximal tubules via theexcretion of NH4+ originating from circulating glutamine. Failure of thisoccurs in Addison’s disease resultingin a mild Type 4 RTA
De-Novo bicarbonate is producedwithin alpha intercalated cells of the cortical collecting duct via theexcretion of H+ which is buffered by phosphate. Failure results in Type 1 RTA
Bicarbonate is reabsorbed by this processin the proximal tubule. Failure of this process in Falconi’s syndrome causesrenal tubular acidosis (Type 2 RTA)