Renal physiology
193
Renal physiology Renal physiology Dr. Ramadan Mohamed Ahmed. Dr. Ramadan Mohamed Ahmed. [email protected] [email protected]
-
Upload
ram-moh -
Category
Health & Medicine
-
view
1.636 -
download
1
description
Transcript of Renal physiology

Renal physiologyRenal physiologyDr. Ramadan Mohamed Ahmed.Dr. Ramadan Mohamed Ahmed.
[email protected]@yahoo.com

2
Chief Functions of Renal Chief Functions of Renal SystemSystem1.Regulation of water & electrolyte balance
2.Regulation of acid & base balance3.Excretion of waste products of protein
metabolism, e.g.,Urea from protein breakdownUric acid from nucleic acid breakdownCreatinine from muscle creatine breakdownEnd products of hemoglobin breakdown4.Excretion of foreign chemicals, e.g., drugs, food
additives, pesticides, …etc.5.Endocrine function: erythropoietin, renin, 1,25-
dihydoxy-vitamin D.

3
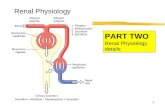
FUNCTIONAL ANATOMY OF KIDNEYS & FUNCTIONAL ANATOMY OF KIDNEYS & URINARY TRACTURINARY TRACT
•The kidneys lie high on the posterior abdominal wall below the diaphragm & on either side of the vertebral column.
•In adults each kidney is the size of a clenched fist & weighs ~150 g.
•Urine produced by the kidneys is delivered to the urinary bladder by 2 ureters.
•The bladder continuously accumulates urine and periodicallyempties its contents via urethra under the control of an external urethral sphincter – a processknown as micturition.

4
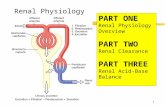
FUNCTIONAL ANATOMY: kidFUNCTIONAL ANATOMY: kid•Each kidney is formed of 2 distinct parts:
An outer cortex An inner medulla.•The medulla contains 5-10 renal pyramids. Their tips project into the renal pelvis & the dilated upper part of the ureter.
•The nephron is the functional unit of the kidney. Each kidney contains ~ 1 million nephrons.
•The nephron is composed of 2 main components:
A. The renal corpuscle
B. The renal tubule

5
Th
e
Th
e
Nep
hro
nN
ep
hro
n

6
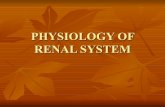
THE NEPHRONTHE NEPHRONA. Renal Corpuscle: (Site of filtration of blood)
1. The Glomerulus: - It is present in the cortex.
- Each glomerulus is formed of a tuft of capillaries that are invaginated into the Bowman’s capsule.
- Blood enters the capillaries through the afferent arteriole and leaves
through the slightly narrower efferent arteriole. - Glomerular capillaries are unique in that they are
interposed between 2 arterioles. This arrangement serves to maintain a high hydrostatic pressure in the capillaries, which is necessary for filtration.
- The capillaries in the glomerulus have large pores called fenestrae,
making them much more permeable than most capillaries elsewhere in the body.

7
THE NEPHRON THE NEPHRON A. Renal Corpuscle: 2. The Bowman’s Capsule: It is the proximal expanded portion of the renal tubule
forming a double-walled cup: a. The inner layer (visceral layer) is formed of specialized
epithelium made up of podocytes: These cells have an octopus-like structure. They have foot processes that interdigitate and
surround the glomerular capillaries. The foot processes do not form a continuous layer,
but leave gaps that provide filtration slits. b. The outer layer (parietal layer) is continuous with the
epithelium of the renal tubule.

8
The The RenalRenalCorpusclCorpusclee

9
THE GLOMERULAR MEMBRANETHE GLOMERULAR MEMBRANE
• It separates the plasma in glomerular capillaries from the fluid in Bowman’s capsule. It is formed of 3 layers:1. Endothelium of capillary with large fenestrae.2. Basement membrane: It contains large spaces,
allowing the filtration of large amounts of water & small solutes.
Yet, the basement membrane is formed of negatively charged glycoproteins &, thus, opposes the filtration of the negatively charged plasma proteins.
3. Foot processes of podocytes with large filtration slits.• Due to its special structure, the glomerular membrane
filters several hundred times as much water & solutes as a usual capillary membrane.
• The filtrate is called an ultrafiltrate as it is formed of plasma minus plasma proteins.

10
Glomerular Glomerular Membrane Membrane
Thus, the filtrability of solutes is determined by:
1. The size of molecules: The filtrability is inversely related to the molecular size of solute. Electrolytes (as Na+) & small organic solutes (as glucose) pass freely, while large molecules (as proteins) do not pass through the membrane pores.
2. Charges of molecules: Negatively charged large molecules are less filterable than positively charged molecules of the same size.

11
THE NEPHRON THE NEPHRON B. Renal Tubule:
1. Proximal convoluted tubule (PCT)2. Loop of Henle: It is further subdivided into:
► Thin descending limb ► Thin ascending limb ► Thick ascending limb3. Distal convoluted tubule (DCT)
- Many DCTs open into a collecting duct (CD). CDs pass from the
cortex (cortical CD) to the medulla (medullary CD) and finally drain
urine into the renal pelvis.- PCT & DCT are present in the cortex, while the descending
limb of loop of Henle dips into the medulla, forming a hairpin turn &
then returns back to the cortex.

12
THE NEPHRON THE NEPHRON
Juxtaglomerular Apparatus: Each DCT passes between the afferent & efferent
arterioles of its own nephron. At this point there is a patch of cells with crowded nuclei in the wall of the DCT called the macula densa. They sense the concentration of NaCl in this portion of the tubule.
The wall of the afferent arteriole opposite the macula densa contains specialized cells known as the juxtaglomerular cells (JG cells). They secrete renin.
Together, the macula densa & JG cells are called the juxtaglomerular
apparatus (JGA).


Juxtaglomerular apparatusJuxtaglomerular apparatus
* It is a structure formed when the distal convoluted * It is a structure formed when the distal convoluted tubule bends around to contact the afferent arteriole tubule bends around to contact the afferent arteriole at the place where it enters the glomerulus.at the place where it enters the glomerulus.
* It is composed of specialized tubular epithelial cells * It is composed of specialized tubular epithelial cells of distal convoluted tubule and the granular cells of of distal convoluted tubule and the granular cells of the adjacent of the afferent arteriolar wall.the adjacent of the afferent arteriolar wall.
* The granular cells secrete an enzyme called renin.* The granular cells secrete an enzyme called renin.This enzyme is responsible for the production of This enzyme is responsible for the production of angiotensins, of which angiotensin II.angiotensins, of which angiotensin II.Angiotensin II stimulates the secretion of aldosterone Angiotensin II stimulates the secretion of aldosterone hormone.hormone.

15
The Juxta-The Juxta-glomerulaglomerular r ApparatusApparatus

16
THE NEPHRON (cont.)THE NEPHRON (cont.)
N.B.
- There are 2 types of nephrons in the kidney:1. Cortical Nephrons: (80% of nephrons) Their glomeruli lie in the outer layers of the cortex. Their tubular system is relatively short. Their loops of Henle penetrate only for a short
distance into the outer portion of renal medulla.
2. Juxtamedullary Nephrons: (20% of nephrons) Their glomeruli lie at the boundary between cortex &
medulla. They have long loops of Henle, which dip deeply down
into the medulla toward the tips of the pyramids. They play a major role in the process of urine
concentration.

Types of nephronsItems Cortical nephrons Juxtamedullary nephrons
% Of total 85 % 15%
Glomeruli Out part of cortex Inner part of cortex .
Loop of Hnle Short i.e. dips to the junction between inner and outer
medulla.
Long i.e. dips deeply into the medullary pyramids to the
inner medulla
Blood supply Peritubular capillariesNo Vasa Recta
Vasa recta and peritubular capillaries
Special function Na reabsorption Urine concentration
Afferent arteriole Thick muscular wallVery sensitive to symp
Stimulation.Have JG apparatus
Exhibit autoregulationLow resistance to blood flow at
rest
Thin muscular wallLess sensitive to symp
Stimulation.Have no JG apparatusDo not exhibit autoreg
High resistance to blood flow at rest
Efferent arteriole Thin muscular wallLess sensitive to symp
Stimulation & vasopressin.
Thick muscular wallVery sensitive to symp
Stimulation & vasopressin.Tone decreased by
Prostaglandins (PGs).
JG apparatus Present Absent
Autoregulation Present Absent

NephronsNephrons
They are the They are the structural & structural &
functional functional units of the units of the
kidney kidney
Proximal Proximal convoluted tubuleconvoluted tubule
Distal convoluted Distal convoluted tubuletubule
Afferent Afferent arteriolearterioleEfferent Efferent arteriolearteriole
PeritubularPeritubularcapillariescapillaries
Renal arterioleRenal arteriole
Renal corpuscle
Renal corpuscle
There are 2 structural classes of nephrons There are 2 structural classes of nephrons which are:which are:1- Cortical nephrons: 1- Cortical nephrons: representing 85% of representing 85% of nephrons where almost all the length of which nephrons where almost all the length of which lies within the renal cortex.lies within the renal cortex.2- Juxtamedullary nephrons: 2- Juxtamedullary nephrons: representing representing 15% where their loops of Henle dip deeply 15% where their loops of Henle dip deeply into the renal medulla.into the renal medulla.

Juxtamedullary Nephron Cortical Nephron
The efferent vessels of juxtamedullary glomeruli form long looped vessels, called vasa recta which is important for urine concentration.


So,why is the loop of Henle useful?• The longer the loop, the
more concentrated the filtrate and the medullary IF become
• Importance: the collecting tubule runs through the hyperosmotic medulla more ability to reabsorb H2O
Desert animals have long nephron Loop More H2O is reabsorbed

22
BLOOD VESSELS in the BLOOD VESSELS in the NEPHRONSNEPHRONS • Each kidney receives its blood supply from a renal
artery, which arises directly from the abdominal aorta.• In the kidney, the renal artery progressively subdivides
into smaller branches until they form afferent arterioles, which break up into a tuft of capillaries, the glomerulus. Then the capillaries form the efferent arteriole.
• The efferent arteriole again subdivides to form peritubular capillaries, which surround the various segments of the renal tubules.N.B. There are 2 sets of capillaries & 2 sets of arterioles!!
• The efferent arterioles of juxtamedullary nephrons form a special type of peritubular capillaries called vasa recta. They are straight & long capillaries that form hairpin
loops along side the loops of Henle. They play an important role in the process of urine
concentration.

Blood supply of the kidney

BLOOD SUPPLY• Renal artery from aorta; enters hilum; divides• Interlobar arteries – renal column; divide• Arcuate arteries – at boundary of cortex & medulla;
divide• Interlobular arteries – into cortex; divide into several• Afferent arterioles: supply one nephron; end in cluster
of capillaries –GLOMERULUS ( capillary filtration)– • Drained by • Efferent arterioles – which form plexus – PERITUBULAR
CAPILLARIES - surround renal tubule• From capillaries blood flows• Interlobular veins• Arcuate veins• Interlobar veins• Renal vein• Inferior vena cava• Nephrons with tubes deep in medulla – Efferent arterioles
give rise to VASA RECTA (capillaries).

Portal system (capillary beds in series), paralleling the nephron Renal ==> afferent ==> glomerular ==> efferent ==> peritubular arteries ==> arterioles ==> capillaries ==> arterioles ==> capillaries.

Major renal capillariesGlomerular capillary bed
Peritubular capillary bed
1. Receives bl from afferent art.
Receives bl from efferent art.
2. High presure bed 55 mmHg
Low pressure bed 13 mmHg
3.Represents arterial end of cap.
Represents venous end of cap.
4. allows fluid filtration. Allows fluid reabsorption.

27
Blood Blood Supply of Supply of Cortical & Cortical & JuxtamedullJuxtamedullary ary NephronsNephrons

RENAL BLOOD FLOW (RBF)
Renal blood flow is about 20% of the cardiac outputThis is a very large flow relative to the weight of the kidneys (≈350 g)
RBF determines GFR
RBF also modifies solute and water reabsorption and delivers nutrients to nephron cells.
Renal blood flow is autoregulated between 70 and 170 mm Hg by varying renal vascular resistance (RVR).
i.e. the resistances of the interlobular artery, afferent arteriole and efferent arteriole

Factors affecting RBF
1) Autoregulation:– RBF is kept relatively constant between
ABP; 70-170 mmHg, It is present in denervated, isolated kidney, this proving
that this property is intrinsic property.
2) Sympathetic stimulation:– VC of afferent arteriole of cortical
nephrons decreased cortical blood flow.– Less effect on juxtamedullary nephrons
remains well perfused.– VC of vasa recta decrease medullary
blood flow more urine concentration.

Autoregulation of RBF & GFR• Note:
Autoregulation is important to prevent large changes in GFR that would greatly affect urinary output.

Autoregulation (Myogenic mechanism)• Response to changes in pressure within
the nephron’s vascular component• Arterioles contract inherently in response
to the stretch accompanying ↑ pressure. Vessel automatically constricts, which helps limit blood flow into glomerulus despite increased systemic pressure
• Opposite reaction occurs when smooth muscles sense a drop in pressure

40 80 120 160 200 240
0.5
1.0
1.5
RB
F (
L/m
in)
BP (mmHg)
AUTOREGULATORY RANGE
AUTOREGULATION

50 100 150 200
50
100
150
RB
F o
r G
RF
(%
of
norm
al)
Arterial Pressure (mmHg)
Urine Output
GFR
RBF
EFFECT OF ARTERIAL PRESSURE CHANGESON GFR, RBF AND URINE OUTPUT

Tubuloglomerular feedback • Juxtaglomerular apparatus
– the combination of tubular and vascular cells where the tubule passes through the angle formed by the afferent and efferent arterioles as they join the glomerulus
• Smooth muscle cells within the afferent arteriole form granular cells
• Specialized tubular cells in this region known as macula densa- sense changes in salt level of tubular fluid


• Macula Densa
Arterial pressure
GFR Fluid reabsorption in proximal tubule
Tubular flow rate
Na+ and Cl- delivery to Macula Densa
Na+ and Cl- reabsorption in Macula Densa
Renin release
Arterial pressure
GFR
Tubular flow rate
Na+ and Cl- delivery to Macula Densa
Na+ and Cl- reabsortion in Macula Densa
Renin release

Autoregulation of High Filtration Pressure

Importance of Autoregulation • The myogenic and tubuloglomerular
feedback mechanisms work in tandem to autoregulate GFR within a MAP range of 80-180 mmHg
• Autoregulation greatly blunts the direct effect that changes in arterial pressure might otherwise have on GFR and preserves water and solute homeostasis and allows waste excretion to carry on as usual

Impact of autoregulation• Autoregulation:
– GFR=180L/day and tubular reabsorption=178.5L/day
– Results in 1.5L/day in urine
• Without autoregulation:– Small ↑ in BP 100 to 125mm Hg, ↑GFR
by 25% (180 to 225L/day)– If tubular reabsorption constant, urine
flow of 46.5 L/day• What would happen to plasma volume?

40
MEASUREMENT OF RENAL BLOOD MEASUREMENT OF RENAL BLOOD FLOWFLOW
• Renal blood flow (RBF) is determined by measuring first the renal plasma flow (RPF) and then calculating the RBF.
• We measure RPF using paraaminohippuric acid (PAH).• PAH is a substance that is:
freely filtered by the glomeruli, secreted in the tubules,but not reabsorbed.If PAH is given by intravenous (IV) infusion so that its concentration is kept low in plasma (e.g., 2 mg%), it is almost completely removed with a single circulation of plasma in the kidneys.
10% of PAH remain in blood, because 10% of the blood that goes to
the kidneys does not reach the nephrons, but supplies other renal
tissues.

41
MEASUREMENT OF RENAL BLOOD FLOW MEASUREMENT OF RENAL BLOOD FLOW • If we apply Fick’s principle, we can calculate RPF:
• Amount of PAH filtered & secreted = P x ERPF• Amount of PAH excreted in urine/min. = U x V
where, P = conc. of PAH in plasma ERPF = effective RPF (90% of plasma only, i.e., taking into account that 10% bypasses the nephrons).
U = conc. of PAH in urine V = volume of urine/min.
P x ERPF = U x V U x V
ERPF = P
Amount of PAH Amount of PAH=
filtered & secreted/min excreted in urine/min

MEASUREMENT OF RENAL BLOOD MEASUREMENT OF RENAL BLOOD FLOWFLOWExample: In a patient, if PAH is infused so that its conc. in
plasma (P) is
2 mg% (= 0.02 mg/ml) and the urine vol. (V) is 1.3 ml/min. & PAH
conc. in urine (U) is l0 mg/ml, then
ERPF = 10 mg/ml x 1.3 ml/min. / 0.02 mg/ml
= 650 ml/min.
Since EPRF is 90% of actual RPF,
RPF = 650 x 100 / 90 = 720 ml/min.
If the hematocrit value is 45%, then plasma constitutes 55%
RBF = 720 x 100 / 55 = 1300 ml/min.
Since cardiac output is 5 L/min, RBF (1300 / 5000 x100) is ~25% of C.O..

Urine formation



Urine Formation
• Glomerular Filtration• substances move from blood to glomerular capsule
• Tubular Reabsorption• substances move from renal tubules into blood of peritubular capillaries• glucose, water, urea, proteins, creatine• amino, lactic, citric, and uric acids• phosphate, sulfate, calcium, potassium, and sodium ions
• Tubular Secretion• substances move from blood of peritubular capillaries into renal tubules• drugs and ions

Overall fluid movement in the kidneys

Glomerular filtration.Glomerular filtration.
It takes place between glomerular capillaries endothelium It takes place between glomerular capillaries endothelium (characterized by the presence of numerous small pores (characterized by the presence of numerous small pores (fenestrations)(fenestrations) and Bowmanand Bowman’’s capsule (characterized by the presence of podocytes).s capsule (characterized by the presence of podocytes).
Podocytes are modified squamous epithelial cells with numerous Podocytes are modified squamous epithelial cells with numerous elongated branches called foot processes which are separated by narrow elongated branches called foot processes which are separated by narrow gaps called filtration slits (slit pores).gaps called filtration slits (slit pores).
Fluid and small solutes dissolved in the plasma such as glucose, amino Fluid and small solutes dissolved in the plasma such as glucose, amino acids, Na, K, Cl, HCOacids, Na, K, Cl, HCO33- , other salts, and urea pass through the - , other salts, and urea pass through the
membrane and become part of the filtrate.membrane and become part of the filtrate.
The glomerular membrane hold back blood cells, platelets and most The glomerular membrane hold back blood cells, platelets and most plasma proteins.plasma proteins.
The filtrate is about 10% of the plasma.The filtrate is about 10% of the plasma.
The volume of fluid filtered per unite time is called the glomerular The volume of fluid filtered per unite time is called the glomerular filtration rate (GFR). The GFR is about 180 L/day (=125 ml/min.).filtration rate (GFR). The GFR is about 180 L/day (=125 ml/min.).

a- Contents: - water- ions: Na+, K+, Cl-- freely filtered substances e.g. glucose,
amino acids.- 0.03% albumin (molecular weight 6900).b- Osmolality: 300 mosmol/L, isotonic
(same osmolality as plasma).C- Specific gravity: 1010D- pH: drops to 6 in urine due to
acidification by the kidney.
COMPOSITION OF GFR

–In an average man: 125 ml/minute. In women : 10% less.–High renal blood flow (20-25% of cardiac output) needed for high GFR.–GFR equals about 180 L/day so plasma volume (3L) filtered about 60 times daily, More than 99% of GFR is normally reabsorbed.–Normal volume of urine is about 1.5 litre/day.
GFR

Filtration fraction
It is the fraction of the renal plasma flow (RPF) that becomes glomerular filtrate. the average filtration fraction about 16-20%.It is calculated as (GFR/RPF X100).

Glomerular membrane
Capillary endothelium; It has small holes (70-90 nm). It does not act as a barrier
against plasma protein filtration. Basement membrane; (BM)
filamentous layer attached to glomerular endothelium & podocytes, carry strong-ve charges which prevent the
filtration of plasma proteins, but filters large amount of H2O and solutes.
Podocytes; Epithelial cells that line the outer surface of the glomeruli. They have numerous foot processes that attach to the BM,
forming filtration slits (25 nm wide).

Layers of Glomerular Membrane

Permeability of the glomerular membrane Size of the molecules• Substances having diameters less than 4
millmicrons (molecular weight 5500) are freely filtered while those having diameters more than 8 millimicrons (molecular weight more than 7000) are not filtered.
Charges of the molecules• -ve charged molecules are filtered Less
easily than neutral molecules of equal size. (possibly due to negative charges in the basement membrane).

Filterability of the Membrane• Filterability is a term used to describe
membrane selectivity based on the molecular size and charge
• Pore size would favor plasma protein (albumin) passage, but negative charge on protein is repelled by the (-) charged basement membrane (proteoglycan filaments & podocytes)
• Loss of this (-) charge causes proteinuria condition called minimal change nephropathy

What Drives Filtration?How does fluid move from the
plasma across the glomerular membrane into Bowman’s capsule?
• No active transport mechanisms• No local energy expenditureSimple passive physical forces
accomplish filtration- Filtration occurs throughout the
length of the capillaries

Forces involved in Filtration• Glomerular capillary blood
pressure (favors filtration)• Plasma-colloid osmotic pressure
(opposes filtration)• Bowman’s capsule hydrostatic
pressure (opposes filtration)

Forces affecting the GFR:Forces affecting the GFR:
A) A) ForcesForces helping filtration: helping filtration:1- Hydrostatic pressure of the blood inside glomerular capillaries (HP1- Hydrostatic pressure of the blood inside glomerular capillaries (HPGG) (= 50 mmHg) ) (= 50 mmHg)
due to:due to:i- The afferent arteriole is 3 times wider than the efferent arteriolei- The afferent arteriole is 3 times wider than the efferent arterioleii- The diameter of the renal artery is large in relation to the relelatively small size of ii- The diameter of the renal artery is large in relation to the relelatively small size of the kidney.the kidney.iii- The renal artery comes directly from the aorta.iii- The renal artery comes directly from the aorta.2- Colloidal osmotic pressure of the fluid inside the Bowman2- Colloidal osmotic pressure of the fluid inside the Bowman’s capsule (COP’s capsule (COPBCBC).).
Where the filtrate is free of proteins, so this force normally equals to zero mmHg.Where the filtrate is free of proteins, so this force normally equals to zero mmHg.
Accordingly,Accordingly,The net filtering force= The forces helping filtration - The forces opposing filtrationThe net filtering force= The forces helping filtration - The forces opposing filtration = (HP = (HPGG + COP + COPBCBC) - (COP) - (COPGG + HP + HPBCBC))
= (50 + 0) - (30 + 10) = 10 mmHg. = (50 + 0) - (30 + 10) = 10 mmHg.
B) Forces opposing filtration:B) Forces opposing filtration:
1- Colloidal osmotic pressure of the glomerular capillary blood1- Colloidal osmotic pressure of the glomerular capillary blood (COP (COPGG).).
This pressure is due to plasma proteins and equals 30 mmHg.This pressure is due to plasma proteins and equals 30 mmHg.2- 2- 1- Hydrostatic pressure of 1- Hydrostatic pressure of tthe fluid inside the Bowmanhe fluid inside the Bowman’s capsule ’s capsule (HP(HPBCBC) (= 10 ) (= 10
mmHg). mmHg).

Forces affecting filtration
Favoring FiltrationFavoring FiltrationOpposing FiltrationOpposing Filtration
Glomerular hydrostatic
pressure60 mm Hg
Bowman’s capsule hydrostatic pressure
18 mm Hg
Bowman’s capsule colloid osmotic pressure
0 mm Hg
Glomerular capillary colloid osmotic pressure
32 mm Hg
Net = +10 mm Hg

Determinants of GFRGFR=Kf x Net filtration pressure
KKff = Capillary filtration coeficient = Capillary filtration coeficient

Filtration coefficient (Kf)
• It is the GFR / mmHg of net filtration pressure, it is normally 12.5ml/min/mmHg. It is constant (normally).
• Glomerular filtration rate = Net filtration pressure X Filtration coefficient
• GFR = NFP (l0) X Kf (12.5) = 125ml/min.
-Kf is determined by 2 factors:1- The permeability of the capillary bed.2- The surface area of the capillary bed.

Glomerular Filtration Rate• Depends on
– The net filtration pressure– How much glomerular surface area is available
for penetration– How permeable the glomerular membrane is
GFR = Kf x net filtration pressure
Where (Kf)= filtration coefficient (a product of the above two glomerular properties)
- Roughly 125 ml/min in males

Regulation of Filtration(1) Changes in glomerular hydrostatic
pressure. (1) Diameter of the afferent arterioles.
– VD of afferent arterioles ++ Hydrostatic pr. in glomerular capillary ++ GFR.
– VC of afferent arterioles e.g ++ sympathetic activity -- Hydrostatic pr. in glomerular capillary (HPGC) -- GFR.
(2) Diameter of the efferent arterioles.– Moderate VC ++ HPGC slight ++ of
GFR.– Severe VC -- RBF -- GFR.
(3) ABP; Between 70 & 170 mmHg: GFR and RBF are kept
relatively constant by autoregulatory mechanisms.
(4) Renal blood flow: direct relation (5) Sympathetic stimulation: VC of aff. Arteriole.


65
Changes in GFR by constriction or Changes in GFR by constriction or dilation of afferent (AA) or efferent dilation of afferent (AA) or efferent (EA) arterioles(EA) arterioles

Regulation of Filtration(2) Changes in Bowman’s Capsule hydrostatic pressure
++ Hydrostatic pr in Bowman’s capsule e.g. stone in ureter -- GFR .
(3) Change in glomerular colloidal osmotic pressureIncreased Colloidal osmotic pressure in glomerular capillary
• e.g in dehydration decreased GFR.Decreased Colloidal osmotic pressure in glomerular capillary
• e.g in hypoproteinemia increased GFR.(4) Functioning kidney mass (5) Glomerular surface area according to the state of mesangial cells. Contracted: ADH & ang II.Relaxed: ANP.

List five conditions in which glomerular filtration rate (GFR) decreases.
1- glomerular hydrostatic pressure is reduced (i.e. hypotensive shock)
2-Bowman's space hydrostatic pressure are increase ureteric obstruction.
3- plasma oncotic pressure rises to unusually high levels in dehydration.
4- decreased rates of renal blood and plasma flow (e.g. heart failure).
5- Reduced permeability and / or total filtering surface area.

review autoregulation

Measurement of GFR: (1) Inulin clearance; Inulin has the following
characteristics:• Freely filtered i.e. plasma conc.= filtrate
concentration.– not reabsorbed or secreted by renal tubules i.e. amount filtered
per min.= amount excreted in urine/min.– Not metabolized.– Not stored in the kidney.– Does not affect filtration rate & its conc. is easily measured.
(2) Creatinine clearance • Freely filtered• Not reabsorbed• partially secreted by renal tubules. • Endogenous so used easily but inaccurate.

Renal ClearanceDefinition: Volume of the plasma
cleared from the substance per minute.
RC = UV/P
RC = renal clearance rateU = concentration (mg/ml) of the substance
in urineV = flow rate of urine formation (ml/min)
P = concentration of the same substance in plasma

Inulin clearance






Free Water Clearance (CH20)
Quantifies relative loss or gain of water in the urine
• Clearance of osmoles (Cosm) is the volume of water necessary to secrete the osmotic load in a urine isotonic with plasma– Difference between urine flow and the
clearance of osmoles (Cosm)• CH20 = Ṽ – UosmṼ Posm
– Negative when urine concentrated (hypertonic)
– Positive when urine dilute (hypotonic)

78
TUBULAR FUNCTIONTUBULAR FUNCTION•The glomerular filtrate is formed at a rate of 125 ml/min. or 180 L/day. It passes to the renal tubules.
•In the tubules, the tubular fluid is subjected to the 2 main tubular functions, reabsorption & secretion.
•It is finally excreted as urine at a rate of about 1-2 ml/min. or ca. 1.5 L/day.

79
TUBULAR REABSORPTIONTUBULAR REABSORPTION• Renal tubules transport substances across their membranes to
interstitial fluid and then through the peritubular capillary membrane back to blood.
• Substances can be transported by:1. Transcellular Route:
- Substances pass through the cell membranes: –crossing the luminal membrane & then the basolateral membrane.
- The transport by this route may be active by means of a protein carrier or passive by diffusion.
2. Paracellular Route:
- Substances pass across tight junctions between tubular cells. - Transport by this route occurs passively by diffusion.

Tubular Reabsorption is a Function of the Epithelial Cells Making up the
Tubule
Lumen
Plasma
Cells

Tubular ReabsorptionA) Active transport; against electrochemical gradient.
(1) Primary active transportRequires energy directly from ATP.
►Example; Na+ reabsorption in PCT (2) Secondary active transport
-It does not require energy direct from ATP. a) Co-transport
two substances bind to a specific carrier are cotransported in one direction. b) Counter-transport
two substances bind to a specific carrier aretransported in two directions.
B) Passive reabsorption;(1) Simple diffusion
Passive reabsorption of chloride & Osmosis of water(2) Facilitated diffusion
Need carrier.C) Pinocytosis
It is an active transport mechanism for reabsorption of proteins and peptides in the proximal convoluted tubules.

82
Primary active transport of sodium through the tubular epithelial cell

Proximal Convoluted Tubule
• 65% of the nephron function occurs in PCT.
• The PCT has a single layer of cuboidal cells with millions of microvilli.
– Increased surface area for reabsorption.
• PCT's main function is reabsorption.
• The PCT is full of mitochondria

Reabsorption in Proximal Tubule
• 100% Glucose, protein and Amino Acids
• 60% Sodium, Cl, and H2O.• 80% PH, HCO3, K. • 60% Ca.• 50% of Filtered Urea.

Na reabsorptionNa reabsorption At basolateral side of the tubular epithelial cell there is
an extensive Na+-K+ ATPase system (= Na+-K+ pump).It pumps 3 Na+ actively out of the cell into the
interstitium, and at the same time carries 2 K+ into the cell.
But K+ will diffuse immediately back into the interstitium due to:(1) high concentration gradient & (2) high permeability of epithelial cells to K+.
As a result of this there is:- intracellular Na+ concentration- intracellular negativity (-70 mV)
At luminal membrane there will therefore be passive diffusion of Na+ into the cell along both concentration and electric gradients created by the Na+-K+ ATPase pump. This diffusion is facilitated by a protein carrier.

Na reabsorptionNa reabsorption

Water Reabsorption

Glucose reabsorption
• The transporter for glucose on the basolateral membrane has a limited capacity to carry glucose back into the blood. If blood glucose rises above 180 mg/dl, some of the glucose fails to be reabsorbed and remains in the urine glucosuria.

Glucose reabsorption

Tubular maximum for glucose (TmG):
• The maximum amount of glucose (in mg ) that can be reabsorbed per min.
• It equals the sum of TmG of all nephrons.• TmG not the same in all nephrons• It is an indication of the reabsorptive
capacity of the kidney.• It is determined by the number of glucose
carriers in PCT.• The maximum reabsorption rate is reached
when all the carriers are fully saturated so they can not handle any additional amounts at that time.
• Value; 300 mg/min in ♀ , 375 mg/ min in ♂.

Renal Threshold for Glucose • Is approximately 180 mg/dl• If plasma glucose is greater than
180 mg/dl:– Tm of tubular cells is exceeded
– glucose appears in urine

GLUCOSE REABSORPTION HAS A TUBULAR MAXIMUM
Plasma Concentration of Glucose
GlucoseReabsorbedmg/min
Filtered Excreted
Reabsorbed

Glucosuria
presence of glucose in urine1. Diabetes mellitus –blood glucose level > renal threshold.2. Renal glucosuria –It is caused by the defect in the glucose transport mechanism.3. Phlorhizin–A plant glucoside which competes with glucose for the carrier and results in glucosuria (phloridzin diabetes).4. Pregnancy–due to altered glucose handling in distal nephrons.
17-59

Bicarbonate reabsorption

Secretion in Proximal Tubule
• Hydrogen secretion for acid/base regulation.
• Ammonia secretion for acid/base regulation.
• PAH.• Creatinine.• Uric acid.• Penicillin.

Reabsorption: Loop of Henle

97
SPECIFIC FUNCTIONS OF DIFFERENT SPECIFIC FUNCTIONS OF DIFFERENT TUBULAR SEGMENTS (cont.)TUBULAR SEGMENTS (cont.)
II. Loop of Henle:• The loop of Henle with its 3 segments (that differ structurally &
functionally) contributes to creating a gradually increasing hyperosmolality (300 1200 mosmol/L) in the renal medullary interstitium.
A. Thin descending limb:- highly permeable to water. 20% of H2O is reabsorbed here.- only moderately permeable to solutes.
Osmolality of tubular fluid gradually as loop dips deep into the medullary pyramid (reaches 1200 mosmol).
B. Thin ascending limb:- impermeable to water- low absorptive power for solutes.
C. Thick ascending limb:- impermeable to water- high reabsorptive power for solutes: It actively reabsorbs 25% of filtered Na+, K+, & Cl- (by 1 Na+, 2 Cl-, 1 K+ cotransport) to medullary interstitium.
Osmolality of tubular fluid gradually as it reaches DCT (becomes hypoosmotic). It is called the diluting segment.


99
SPEC. FUNCTIONS OF DIFF. TUBULAR SEGMENTSSPEC. FUNCTIONS OF DIFF. TUBULAR SEGMENTS
III. Distal Convoluted Tubule (DCT) & Collecting Duct (CD):A. Early DCT: This part of the renal tubules is in effect an extension of the thick
ascending limb of loop of Henle:- It is impermeable to water.- There is continued removal of Na+, K+, Cl- & other ions without H2O.
There is further dilution of tubular fluid and its osmolality even more (100 mosmol).
This part is called the cortical diluting segment.
B. Late DCT & Cortical CD: They are impermeable to urea. They have 2 cell types:
(1) Principal Cells:a. They actively reabsorb Na+ in exchange for K+ secretion. This action is increased by aldosterone.b. Antidiuretic hormone (ADH) causes the insertion of H2O channels (aquaporins) in luminal membrane of these cells allows reabs. of H2O.In the absence of ADH, the principal cells are impermeable to H2O.

DCT and CD

101
SPECIFIC FUNCTIONS OF DIFFERENT TUBULAR SPECIFIC FUNCTIONS OF DIFFERENT TUBULAR SEGMENTS (cont.)SEGMENTS (cont.)
B. Late DCT & Cortical CD: (cont.)(2) -Intercalated Cells:- These cells secrete H+ by H+-ATPase independent of Na+
reabsorption. This action is increased by aldosterone.
C. Medullary CD:• In this last portion of the nephron there is final adjustment of
volume & concentration of urine. The permeability of this segment to water, same as that of the late
DCT & cortical CD, is variable & depends on the level of circulating ADH (= facultative water reabsorption).
With high blood levels of ADH, there is reabsorption of H2O by osmosis, as tubular fluid in CD is subjected to gradually increasing hyperosmolality of the medullary interstitium.
This part is also permeable to urea, that diffuses into the interstitium when its concentration in tubular fluid due to H2O reabsorption.Thus, urea contributes to the hyperosmolality of medullary interstitium.
In the presence of ADH: urine excreted is concentrated & small in volume.
In the absence of ADH: urine excreted is dilute urine & large in volume.

Medullary Collecting Duct
• reabsorbs < 10% of filtered Na+ and water
• final site for processing of urine
functional characteristics:1.permeability to water is controlled by
ADH level - ADH water reabsorption
2. permeable to urea - urea is reabsorbed into the medullary interstitium where it help increase the osmolality of the interstitium and
therefore help to concentrate urine.

Summary For Tubular Functions

Summary of changes in osmolality of tubular fluid in various parts of the nephron

REGULATION OF REGULATION OF TUBULAR TUBULAR
REABSORPTIONREABSORPTION

1. Glomerulotubular Balance• intrinsic ability of the tubules to increase
their reabsorption rate in response to an increase in glomerular filtration
• changes in GFR induces a proportional change in tubular reabsorption
• total rate of reabsorption increases as filtered load increases but the percentage of GFR reabsorbed remains relatively constant
• second line of defense for preventing changes in renal hemodynamics from causing large changes in sodium or fluid excretion
• blunts sodium excretion response to changes in GFR induced by changes in arterial pressure

2. Peritubular Capillary and Renal Interstitial Fluid Starling’s ForcesA. Peritubular Capillary Hydrostatic
Pressure: PPC reabsorption Systemic arterial pressure (PA): PA PPC reabsorptionB. PTC Osmotic Pressure (PC): PC reabsorptionC. Renal intersitial fluid hydrostatic
pressure: - Decreased reabsorption in the peritubular capillaries
will result in: 1. PIF due to accumulation of fluid in the interstitial
compartment 2. IF due to dilution of interstitial fluid proteins

3. Arterial Pressure• small increases in arterial pressure
often cause marked increases in urinary excretion of water and sodium (pressure diuresis and pressure natriuresis)
mechanism:1. slight increase in GFR.2. increased PPC reabsorption from
interstitial space PIF reabsorption of water and
sodium from tubular lumen3. decreased Angiotensin II Na+ reabs

4. Hormonal Control
HormoneHormone Site of ActionSite of Action EffectsEffects
AldosteroneAldosterone Collecting tubule and ductCollecting tubule and duct ↑ ↑ NaCl, HNaCl, H22O O
reabsorption, ↑Kreabsorption, ↑K+ +
secretionsecretion
Angiotensin IIAngiotensin II Proximal tubule, thick Proximal tubule, thick ascending loop of ascending loop of Henle/distal tubule, Henle/distal tubule, collecting tubulecollecting tubule
↑ ↑ NaCl, HNaCl, H22O O
reabsorption, ↑Hreabsorption, ↑H++ secretionsecretion
Antidiuretic Antidiuretic hormonehormone
Distal tubule/ collecting Distal tubule/ collecting tubule and ducttubule and duct
↑ ↑ HH22O reabsorptionO reabsorption
Atrial natriuretic Atrial natriuretic peptide peptide
Distal tubule/ collecting Distal tubule/ collecting tubule and ducttubule and duct
↓ ↓ NaCl reabsorptionNaCl reabsorption
Parathyroid Parathyroid hormonehormone
Proximal tubule, thick Proximal tubule, thick ascending loop of ascending loop of Hental/distal tubuleHental/distal tubule
↓ ↓ POPO44------ reabsorption, ↑ reabsorption, ↑
CaCa- - reabsorption reabsorption


5. Sympathetic Stimulation• will decrease sodium and water excretion
(increase sodium and water reabsorption) by the following mechanisms:
1. vasoconstriction of both afferent and efferent arteriole thereby decreasing GFR.2. increase sodium reabsorption in the proximal tubule and thick ascending limb.3. increase renin release increased Ang II
increased sodium reabsorption.

112
Hormones acting on the Hormones acting on the kidneykidney
1. Aldosterone:• Stimulus for its secretion:
Blood volume (via renin-angiotentin system).• Actions & their site:
It stimulates Na+ reabsorption in DCT & cortical CD through: 1) In principal cells: Na+ reabsorption in exchange with K+. 2) In -intercalated cells: Na+ reabsorption in exchange with H+.2. Angiotensin II: It is the most powerful Na+ retaining
hormone.• Stimulus for its secretion:
arterial bl. pressure & blood volume, e.g., hemorrhage (via renin).• Actions & their site: 1. It Na+ reabsorption by several mechanisms: a. By stimulating aldosterone secretion. b. In PCT: - By directly stimulating Na+-K+ ATPase at basolateral
border. - By directly stimulating Na+-H+ countertransp. at
luminal border. 2. It constricts efferent arterioles.


114
Hormones acting on the Hormones acting on the kidneykidney
3. Atrial Natriuretic Peptide (ANP): It facilitates NaCl & H2O excretion.
• Stimulus for its secretion: Atrial pressure (released from specific atrial fibers when blood volume is )
• Actions & their site: 1. It GFR by VD of afferent & VC of efferent arteriole. 2. It Na+ reabsorption from DCT & cortical CD .
4. ADH:• Stimulus for its secretion:
Plasma osmolarity & blood volume.• Actions & their site:
water reabsorption in late DCT, cortical & medullary CD: by inserting aquaporin water channels into their luminal membranes.
5. Parathormone (PTH): • Stimulus for its secretion:
Plasma Ca2+ concentration.• Actions & their site:
1. Ca2+ reabsorption from DCT. 2. Phosphate reabsorption from PCT.


116
HANDLING OF CERTAIN HANDLING OF CERTAIN IMPORTANT SOLUTES IMPORTANT SOLUTES
BY RENAL TUBULESBY RENAL TUBULES

117
I. GLUCOSEI. GLUCOSE:At normal blood glucose levels (~100 mg%), glucose is freely filtered at a rate of 125 mg/min. (= plasma conc. X GFR = 100 mg% x 125 ml/min.). The amount filtered is completely reabsorbed from the upper half of PCT by Na+-glucose cotransport (mechanism: see before).
There is, however, a limited number of Na+-glucose carriers:a- At a blood glucose level of less than 180 mg%, all the filtered glucose can be reabsorbed because plenty of carriers are available. b- At a blood glucose level of 180 mg%, glucose starts to appear in urine. This level of blood glucose is called the renal threshold for glucose. It corresponds to a renal tubular load of 220 mg/min.
c- At a renal tubular load of glucose of 320 mg/min, all the carriers are saturated, i.e., the transport maximum for glucose, TmG, is reached. Any further in filtered glucose is not reabsorbed & is excreted in urine.

Glucose reabsorption

119
Glucose Titration CurvesGlucose Titration Curves

120
I. GLUCOSEI. GLUCOSE: (cont.)
I. GLUCOSEI. GLUCOSE: (cont.)Splay:- It is the region of glucose curves between renal threshold & TmG.
- It occurs between renal tubular glucose loads of 220 - 320 mg/min..- It represents the excretion of glucose in urine before full saturation of the glucose carriers for reabsorption (TmG) is achieved.
- It is explained by the heterogeneity of nephrons: Not all nephrons have exactly the same TmG. Some nephrons
reach saturation at lower plasma concentrations than others, and glucose will be excreted in urine before the average TmG is reached.

121
GLUCOSURIA:
•Definition:It is the presence of glucose in urine. It is usually accompanied by polyuria due to osmotic diuresis.
•Causes:1. Diabetes Mellitus: - The blood glucose level is high, exceeding the
normal renal glucose threshold of 180 mg%. - In this condition, the plasma clearance of glucose is
above zero, & the more advanced the condition of diabetes, the higher the glucose clearance.
2. Renal Glucosuria: - In this condition the blood glucose level is normal. - The defect lies in the renal tubules themselves.
There is a decreased renal glucose threshold below its normal value due to a congenital defect in the glucose transport mechanism, so that there is loss of glucose in urine at normal blood glucose levels.

122
SodiumSodium HandlingHandling
-Na+ is freely filtered across glomerular capillaries. Thus, its
concentration in glomerular filtrate equals that in plasma.-99% of Na+ are reabsorbed along all segments of the renal tubule, except the thin descending limb of the loop of Henle.
Na+ reabsorption along the nephron:1. Proximal convoluted tubule:
Reabsorbs 2/3 (67%) of filtered Na+ & H2O. This process is isoosmotic. a. Early PCT:
- Na+ is reabsorbed by cotransport with glucose, amino acids, phosphate & lactate.- Na+ is also reabsorbed by countertransport via Na+-H+
exchange. b. Late PCT:
Na+ is reabsorbed (1ry active transport) with Cl- (passive diffusion).

123
SodiumSodium HandlingHandling
2. Thick ascending limb of loop of Henle: Reabsorbs 25% of filtered Na+ by the Na+-K+-2Cl-
cotransporter in the luminal membrane.3. Distal convoluted tubule & collecting duct: Together they reabsorb 8% of the filtered Na+. a. Early DCT: Contains a Na+-K+-2Cl- cotransporter in luminal
membrane similar to that in thick ascending limb of loop of Henle.
b. Late DCT & CD: (This effect is increased by aldosterone). i. Principal cells: reabsorb Na+ in exchange for K+. ii. -Intercalated cells: reabsorb Na+ in exchange for H+.

124
Na+ handling along the nephron

125
Factors affecting Na+ reabsorption:1. Rate of tubular flow:
Slow rate of flow reabsorption of Na+ in loop of Henle, e.g., in GFR.
2.Glomerulotubular balance in PCT: - It represents the ability of the PCT to reabsorb a
constant fraction (2/3 or 67%) of the filtered load of Na+ & water.
- If GFR for any reason, the filtered load of Na+ also . This will lead to an increase in the amount of Na+
reabsorbed in PCT, so that the amount of Na+ excreted increases only slightly.
- Importance:It is an intrinsic mechanism that can be seen in denervated kidneys. It helps prevent overloading of distal tubular segments when GFR .

126
2. Glomerulotubular balance in PCT: - Mechanism:
Glomerulotubular balance is based on Starling forces in peritubular capillaries, which alter Na+ & H2O reabsorption:
in GFR results in in protein conc. & oncotic pressure (C), as well as a hydro-
static pressure (PC) of peritubular capillaries.
This, in turn, causes an in water reabsorption from PCT. Since water reabsorption is accompanied by Na+ reabsorption, there is matching filtration & reabsorption, or glomerulotubular balance.
3. Hormones: (see before)1. Aldosterone, 2. Angiotensin II, 3. ANP
Factors affecting Na+ reabsorption

127
1. Glomerular capillaries:Filtration of K+ occurs freely across the glomerular capillaries.
2. PCT:It reabsorbs 67% of the filtered K+ along with Na+ & water.
3. Thick ascending limb of loop of Henle & early DCT:It reabsorbs 20% of the filtered K+ by the Na+-K+-2Cl- cotransporter in the luminal membrane.
4. Late DCT & collecting duct:They either reabsorb or secrete K+.a. Reabsorption of K+: - It occurs only in K+ depletion (= low K+ diet). Under these conditions K+ excretion can be as low as 1% of filtered load because the kidney conserves as much K+ as possible. - It involves a K+-H+ exchange at luminal membrane of -intercalated cells.b. Secretion of K+:
- It occurs in principal cells by Na+-K+ exchange. - It is variable. It depends on dietary K+, aldosterone & acid-
base status.
PotassiumPotassium Handling

128
K+ handling along the nephron

129
Mechanism of distal K+ secretion in principal cells
- At basolateral membrane: K+ is actively transported into the cell by the Na+-K+ ATPase This mechanism maintains a high I.C. K+ conc.
- At luminal membrane: K+ is passively secreted into the lumen through K+ channels.
The amount of this passive secretion is determined by the concentration gradient acting on K+ across the luminal membrane:
In conditions that I.C. K+ conc. or the luminal K+ conc. the driving force for secretion.
In conditions that I.C. K+ conc. or the luminal K+ conc. the driving force for secretion.

130
Mechanism of KMechanism of K++ secretion in the secretion in the principal cell of the DCTprincipal cell of the DCT
1
3
2

131
HANDLING OF CERTAIN IMPORTANT HANDLING OF CERTAIN IMPORTANT SOLUTES BY RENAL TUBULES SOLUTES BY RENAL TUBULES
Factors affecting distal K+ secretion:1. Dietary K+:
High K+ diet I.C. K+ driving force K+ secretion.Low K+ diet I.C. K+ driving force K+ secretion.
2. Aldosterone: - At the basolateral membrane: It stimulates Na+-K+ ATPase K+
uptake by principal cells I.C. K+ concentration driving force for K+ secretion.
- At the luminal membrane: It the number of K+ channels.
3. Acid-base status: As Na+ ions are reabsorbed in exchange for the secretion of K+ or H+
ions, there is competition for Na+ ions in the tubular fluid:In acidosis: More H+ than K+ enters tubular epithelial cell across the basolateral membrane I.C. K+ driving force for K+ secretion.In alkalosis: Less H+ than K+ enters tubular epithelial cell across the basolateral membrane I.C. K+ driving force for K+ secretion.

132
HANDLING OF CERTAIN IMPORTANT HANDLING OF CERTAIN IMPORTANT SOLUTES BY RENAL TUBULES SOLUTES BY RENAL TUBULES
V. Phosphate: - 85% of filtered phosphate is reabsorbed in PCT by
cotransport with Na+ and the rest is excreted in urine.
- Parathyroid hormone (PTH) inhibits phosphate reabsorption in PCT & causes phosphaturia.
- Phosphate is a urinary buffer for H+.

HANDLING OF CERTAIN IMPORTANT HANDLING OF CERTAIN IMPORTANT SOLUTES BY RENAL TUBULES SOLUTES BY RENAL TUBULES
VI. Calcium: - Normally, 99% of filtered calcium are reabsorbed by renal
tubules. - It should be noted, however, that only 50% of plasma
calcium, which is ionized calcium, is filtered across the glomerular capillaries, while the other 50% of plasma calcium are bound to plasma proteins and cannot be filtered. 67% are reabsorbed in PCT. 25-30%% are reabsorbed in the loop of Henle. 5-10% are reabsorbed in DCT & CD. PTH stimulates Ca2+
reabsorp-tion from DCT.

Urea Handling(1) PCT
About 50% of the filtered urea is passively reabsorbed
The wall of PCT is partially permeable to urea but highly permeable to water so
water reabsorption from PCT → increases urea concentration in tubular
lumen. This creates concentration gradient → Urea reabsorption.
(2) Thick ascending limb of loop of Henle, DCT and cortical collecting tubules
All are relatively impermeable to urea.
H2O reabsorbed in DCT and cortical collecting tubule (in presence
of ADH) increased urea concentration in tubular fluid.
(3) Inner medullary portion of the collecting duct Urea diffuses into the medullary interstitium to increase its osmolality.
Diffusion of urea is facilitated by ADH.
40 - 60% of the tubular load of urea is excreted in urine.
►Urea cycle • Urea moves from the medullary interstitium into the thin
loop of• the Henle and back down into the medullary collecting
• duct and again to medullary interstitium• several times before urea is excreted.

Urea recycling

Handling of Hydrogen1. PCT 85%
2. Thick ascending loop of Henle 10%3. DCT and collecting tubule 5%.
Mechanism of H+ secretionA) In PCT, LH and initial part of DCT:
Most of H+ is secreted by secondary active transport.
It is Na dependent.
Antiport carrier at luminal border bind Na and H.
B) In late part of DCT and CD:
Hydrogen is secreted by primary active transport By
Intercalated cells,
hydrogen secretion is stimulated by aldosterone and both
hydrogen and potassium compete for secretion.

Bicarbonate Handling Plasma HCO3 plays an important
role in the regulation of pH of
plasma.
Most of the filtered bicarbonate
(99 % or more) is reabsorbed.
1) About 80 to 90 % of the
bicarbonate reabsorption
occurs in the PCT.
2) In the thick ascending loop of
Henle, 10 % of the filtered
bicarbonate is reabsorbed,
3) the remainder of the
reabsorption takes place in
the distal tubule
and collecting duct.

Bicarbonate Handling

Amino acid handling
• Secondary active transport coupled with sodium

Subs Description Proximal tubule Loop of Henle Distal tubule Collecting duct
glucose
If glucose is not reabsorbed by the kidney, it appears in the
urine, in a condition known as glucosuria. This is associated
with diabetes mellitus..
reabsorption (almost 100%) via sodium-glucose transport proteins(apical)
and GLUT(basolateral).
- - -
amino acids Almost completely conserved. Reabsorption (active) - - -
urea Regulation of osmolality. Varies with ADH
reabsorption (50%) via passive transport secretion - reabsorption in
medullary ducts
sodium Uses Na-H antiport, Na-glucose symport, sodium ion channels
reabsorption (65%, isosmotic)
reabsorption (25%, thick
ascending, Na-K-2Cl symporter)
reabsorption (5%, sodium-
chloride symporter)
reabsorption (5%, principal cells), stimulated by aldosterone
chlorideUsually follows sodium. Active
(transcellular) and passive (paracellular)
reabsorptionreabsorption
(thin ascending, thick ascending,
Na-K-2Cl
reabsorption (sodium-
chlorid symp-
water Uses aquaporin. - reabsorption (descending) -
reabsorption (with ADH, via vasopressin receptor 2)
HCO3 Helps maintain acid-base balance. [8]
reabsorption (80-90%) [9]
reabsorption (thick ascending)
[10]-
reabsorption (intercalated
cells,
H Uses [[vacuolar H+ATPase]] - - -secretion
(intercalated cells)
K Varies upon dietary needs. reabsorption (80%)reabsorption (20%, thick
ascending, Na-K-2Cl symporter)
secretion increased by aldosterone)
calcium reabsorptionreabsorption (thick
ascending) via passive transport
reabsorption stimulated
by PTH-
phosp Excreted as titratable acid.reabsorption (80%)
Inhibited by parathyroid hormone.
- - -

Table 41-3 NaCl transport along the nephronTable 41-3 NaCl transport along the nephron
SegmentSegment Percentage filtered Percentage filtered reabsorbedreabsorbed
Mechanism of NaMechanism of Na++ entry across the entry across the apical membraneapical membrane
Major regulatory Major regulatory hormoneshormones
Proximal tubuleProximal tubule 67%67% NaNa++-H-H++exchange, exchange, NaNa++-cotransport with -cotransport with amino acids and amino acids and organic solutes, organic solutes, NaNa++/H/H++-Cl-Cl--/anion /anion exchange exchange
Angiotensin IIAngiotensin II
NorepinephrineNorepinephrine
EpinephrineEpinephrine
DopamineDopamine
ParacellularParacellular
Loop of HenleLoop of Henle 25%25% 1 Na1 Na++-1K-1K++-2Cl-2Cl-- symportsymport
AldosteroneAldosterone
Distal tubuleDistal tubule ~4%~4% NaCl symportNaCl symport AldosteroneAldosterone
Late distal tubule Late distal tubule and collecting ductand collecting duct
~3%~3% NaNa+ + channelschannels AldosteroneAldosterone
Atrial natriuretic Atrial natriuretic peptidepeptide
UrodilatinUrodilatin

Table 41-4 Water transport along the nephronTable 41-4 Water transport along the nephron
SegmentSegment Percentage of Percentage of filtered load filtered load reabsorbedreabsorbed
Mechanism of Mechanism of water water
reabsorptionreabsorption
Hormones Hormones that regulate that regulate
water water permeabilitypermeability
Proximal tubuleProximal tubule 67%67% PassivePassive None None
Loop of HenleLoop of Henle 15%15% DTL only; DTL only; passivepassive
None None
Distal tubuleDistal tubule 0%0% No water No water reabsorptionreabsorption
None None
Late distal Late distal tubule and tubule and collecting ductcollecting duct
~8%-17%~8%-17% Passive Passive ADH, ANPADH, ANP


URINE CONCENTRATION

Mechanisms to Concentrate Urine• Countercurrent Multiplication--
creation of osmotic gradient– Loop of Henle– Generates a urine that is concentrated as high
as 600 mosm/L
• Urea recycling– Medullary Collecting Duct– Needed to increase the osmolar gradient from
600 to 1200 mosm/L– Kidneys use urea to do osmotic work when in
state of antidiuresis
• Countercurrent exchange--vasa recta maintains the medullary insterstitial osmotic gradient set up by the countercurrent multiplier

146
PRODUCTION OF CONCENTRATED URINEPRODUCTION OF CONCENTRATED URINE
• Concentrated urine is also called hyperosmotic urine (urine osmolarity > blood osmolarity).
• The kidney excretes excess solutes, but does not excrete excess amounts of water.
• The basic requirements for forming a concentrated urine are:
1. a high level of ADH, e.g., in water deprivation or hemorrhage permeability of late DCT & CDs to water, allowing these segments to reabsorb a large amount of water.
2. a high osmolarity of the renal medullary interstitial fluid provides the osmotic gradient necessary for water reabsorption to occur in the presence of high levels of ADH.
• After passing to the interstitium, water is carried by the vasa recta back into the blood.

147
PRODUCTION OF CONCENTRATED URINE PRODUCTION OF CONCENTRATED URINE Reabsorption of Water in Presence of ADH:In PCT, loop of Henle & early DCT:
- Same as in formation of dilute urine (see before).
- The tubular fluid reaching the late DCT is hyposmotic (100 mOsm/L).
Late DCT:
- ADH the water permeability of the principal cells of the late DCT.
Water is reabsorbed until the osmolarity of the DCT equals that of surrounding interstitial fluid in renal cortex (300 mOsm/L).
CDs:
- ADH the water permeability of principal cells of CDs.
- As the tubular fluid flows through the CDs, it passes through regions of increasing hyperosmolarity toward the inner medulla.
- Water is reabsorbed from the CDs until the osmolarity of the tubular fluid equals that of the surrounding interstitial fluid.
The osmolarity of the final urine reaches 1200 mOsm/L.

148
II. PRODUCTION OF CONCENTRATED URINE II. PRODUCTION OF CONCENTRATED URINE (cont.)(cont.)

149
II. PRODUCTION OF CONCENTRATED URINE II. PRODUCTION OF CONCENTRATED URINE (cont.)(cont.)

150
The Countercurrent SystemThe Countercurrent System• The countercurrent system is responsible for the creation &
maintenance of a gradually increasing hyperosmolarity in the renal medullary interstitium, which is essential for enabling the kidney to concentrate urine in the presence of enough circulating ADH.
• This osmotic gradient is due to accumulation of solutes (primarily NaCl & urea) in great excess of water in the medullary interstitium.
• Once the high solute concentration in medulla has been achieved, it is maintained by a balanced outflow of solutes & water in the medulla.
• This osmotic gradient is1. established by the loop of Henle, which acts as a countercurrent multiplier.
2. potentiated by the collecting duct, which allows urea recycling to occur.
3. maintained by the vasa recta, which act as countercurrent exchangers.

151
THE COUNTERCURRENT SYSTEM THE COUNTERCURRENT SYSTEM Loop of Henle Acting as Counter Current Loop of Henle Acting as Counter Current
MultiplierMultiplierHow does the renal medulla become
hyperosmotic?1. Before the osmotic gradient of the medulla is established,
the osmolarity is the same throughout the nephron (300 mOsm/L).
2. The active pumping of NaCl out of the thick ascending limb occurs without concomitant movement of water in osmolarity of tubular fluid inside ascending limb (200 mOsm/L) & in osmolarity of medullary interstitial fluid (400 mOsm/L).
3. As fluid passes down the descending limb, it reaches osmotic equilibrium with medullary interstitium due to osmosis of water out of descending limb. [Interstitial osmolarity is maintained at 400 mOsm/L due to continued transport of ions out of thick ascending limb.] Thus, there is a gradual in tubular fluid osmolarity as it flows towards the hairpin bend.
4. As more fluid enters descending limb from PCT, hyperosmotic fluid previously present in descending limb now flows into thick ascending limb.

152
THE COUNTERCURRENT SYSTEMTHE COUNTERCURRENT SYSTEMLoop of Henle Acting as Counter Loop of Henle Acting as Counter
Current MultiplierCurrent Multiplier5. More NaCl is pumped from thick ascending limb into
interstitium, but water remains in tubule. This continues until a 200 mOsm/L osmotic gradient is established. Now osmolarity in medullary interstitium has risen further to 500 mOsm/L.
6. Once again the fluid in descending limb equilibrates with hyperosmotic medullary interstitial fluid, now reaching 500 mOsm/L at the tip.
7. These steps are repeated over & over, adding more & more solute to the medulla in excess of water. This process gradually traps solutes in the medulla, eventually raising the interstitial osmolarity to 1200 mOsm/L.
• Overall, the progressive transport of NaCl from the tubular fluid into the interstitium results in the establishment of a longitudinal osmotic gradient in the medulla.
Thus, the countercurrent arrangement of the loop of Henle multiplies a relatively small transepithelial osmotic gradient into a large longitudinal gradient.

153
COUNTERCURRENT MULTIPLIER COUNTERCURRENT MULTIPLIER SYSTEM IN LOOP OF HENLESYSTEM IN LOOP OF HENLE

154
Role of DCT & CDs in Urine Role of DCT & CDs in Urine ConcentrationConcentration
• Tubular fluid flowing from loop of Henle into DCT is dilute.• The early DCT further dilutes the fluid, because this segment,
like the ascending limb of loop of Henle, actively transports NaCl out of tubule, but is impermeable to water.
• With high ADH concentrations, late DCT & cortical CD become highly permeable to water large amounts of water are reabsorbed from the tubule into the cortical interstitium, where it is swept away by the peritubular capillaries.
• With high ADH levels, there is further water reabsorption from medullary CDs to interstitium. However, the amount of water is relatively small compared with that added to the cortical interstitium. Reabsorbed water is quickly carried away by vasa recta into venous blood.
N.B. The fact that large amounts of water are reabsorbed into the cortex, rather than into the medulla, helps to preserve the high medullary interstitial fluid osmolarity.
• Thus, in the presence of ADH, the fluid at the end of CDs has the same osmolarity as the medullary interstitium (1200 mOsm/L).
By reabsorbing as much water as possible, the kidneys form a highly concentrated urine while adding water back to ECF & compensating for deficit of body water.

155
Urea RecyclingUrea Recycling• In the presence of ADH, urea contibutes 40% to the
medullary interstitial osmolarity (= 500 mOsm/L) by passive urea reabsorption from the inner medullary CDs into the interstitium.
Mechanism: - Ascending limb of loop of Henle, DCT, cortical CDs & outer
medullary CDs are impermeable to urea. - As water is reabsorbed from late DCT, cortical & outer
medullary CDs, urea concentration rapidly. - In inner medullary CDs, further water reabsorption takes
place, so that urea concentration rises even more. Thus, urea diffuses out of the tubule into renal interstitium because this segment is highly permeable to urea, and ADH increases this permeability even more.
- A moderate share of the urea that moves into medullary interstitium diffuses into thin descending limb of loop of Henle, so that it passes again in tubular fluid. It recirculates several times before it is excreted. Each time around it contributes to a higher concentration of urea in interstitium.
Urea recirculation provides an additional mechanism for forming a hyperosmotic medulla.

156
UREA RECYCLINGUREA RECYCLING

157
THE COUNTERCURRENT SYSTEM THE COUNTERCURRENT SYSTEM Vasa Recta as Countercurrent Vasa Recta as Countercurrent
ExchangerExchanger•Blood must be provided to renal medulla to supply its metabolic
needs, but without a special blood flow system, solutes pumped into the medulla by countercurrent multiplier would rapidly get lost.
•There are 2 special features in medullary blood flow that contribute to the preservation of the high solute concentrations:
1. The medullary blood flow is low (only 1-2% of total RBF) sufficient for metabolic needs of tissues, but minimizes solute loss.
2. The vasa recta serve as countercurrent exchangers.Countercurrent Exchange Mechanism:•As blood descends into medulla, it becomes more & more
concentrated, by gaining salt & losing water. At the tips of vasa recta blood has a concentration of 1200 mOsm/L.
•As blood ascends back toward cortex, the reverse sequence occurs, and blood leaving vasa recta is only slightly hyperosmotic to normal plasma.
During its passage through medulla, blood has removed the excess salt & water that have been added by the transport processes occurring in the deeper regions of the medulla.
Thus, the U-shape of vasa recta maintains the concentration of solutes established by countercurrent system.

158
Vasa Recta as Countercurrent Vasa Recta as Countercurrent ExchangerExchanger

Diuresis and diuretics Diuresis is an increase in the rate of urine output.
(A) H2O diuresis
Increase H2O intake decrease Osmotic. Pr decrease ADH
decrease facultative H2O reabsorption i.e. Urine large
volume and hypotonic.
(B) Osmotic diuresis
Unreabsorbable solute in PCT decrease obligatory H2O reabsorption decrease Na+ concentration in tubular fluid decrease osmolarity of medullary interstitium decrease facultative H2O reabsorption.
-Urine: large volume and isotonic or hypertonic.
(C) Pressure diuresisIncrease in arterial blood pressure leads to:• ↑ GFR.• Inhibition of rennin angiotensin system → ↓ renin and
angiotensin II production.• ↑ Hydrostatic pressure in peritubular capillaries which →
increase Na+ & H2O excretion.

(4) Diuretic drugs (A)Thiazides: inhibit Na reabsorption in DCT.
(B) Aldosterone inhibitors: (Potassium-sparing diuretics) e.g. alldactone: inhibit Na-K exchange in DCT and collecting tubules
decrease serum Na and increase serum K+.
(C) Carbonic anhydrase inhibitors e.g. acetazolamide (Diamox).
It inhibits carbonic anhydrase enzyme → decrease H secretion → decrease Na
and HCO3- reabsorption in PCT and increase K secretion in DCT → increase Na, HCO3 & K excretion in urine.
May lead to acidosis.
(D) Loop diuretics e.g. frusemide (lasix): inhibit Na-K-2Cl cotransporters in the thick ascending limb
of loop of Henle.


The act of Micturition

Micturition Reflex• As bladder fills sensory stretch
receptors send signals via pelvic nerves to sacral segments of spinal cord.
• Parasympathetic stimulation of the bladder smooth muscle via the same pelvic nerves occurs.
• It is “self-regenerative”, subsides, then re-generates again until the external sphincter is relaxed and urination can occur.

InnervationParasympathetic Pre-glanglionic S2, S3, S4 unite to form Pelvic nerves Post-ganglionic onto detrusor muscle & internal sphincter
Sympathetic Pre-ganglionic L1, L2, L3
Post-ganglionic onto trigone, neck, & internal sphincter Little to do with bladder contraction o--------- o------------------------------------------ Ach NE

Innervation con’t…Afferents (sensory nerves) Pelvic nerve: impulses due to bladder fullness; micturition reflex; pain impulses Hypogastric nerve: pain impulses Pudendal nerve: sensory impulses from urethra
Somatic Efferent (Pudendal nerve)Impulses originate in S1 and S2; innervate external
sphincterMediate voluntary control of micturition

Anatomy of Micturition

• Internal sphincter- detrusor muscle in the bladder neck
whose tone normally keeps the bladder neck and posterior
urethra empty of urine and therefore prevents
emptying of the bladder until the pressure in the main part of the bladder exceeds a critical level
• External sphincter- layer of voluntary skeletal muscle which
surrounds the urethra as it passes through the urogenital diaphragm
- under voluntary control and can conciously prevent urination even when involuntary controls are attempting to empty the bladder

Bladder Filling and Micturition
Bladder Filling:1. Empty bladder: 0 pressure2. 30 - 50 mls of urine 5 - 10 cm
H2O3. 50 - 300 ml little pressure
change 4. With filling, increased activity of external sphincter (maintains continence, or control
of excretory functions)5. > 300 - 400 ml discomfort; leads to urgency
Start of Micturition:1. As bladder fills, micturition
(bladder) contractions begin to appeara. Last from a few seconds to more than a minuteb. Pressure peaks (micturition waves) may rise a few cm H2O to more than 100 cm H2Oc. Caused by micturition reflex

Micturition Con’t…
2. Micturition reflex (does not need the brain)a. Filling stimulates sensory stretch receptorsb. Afferent impulses in Pelvic nervec. Signal reflexively sent back to bladder via efferent parasympathetic fibers in the Pelvic nerved. Detrusor muscle contracts, then relaxes 2. Micturition reflex - continued
e. As bladder fills, micturition reflex occurs more frequently, with greater contraction of bladder wall (positive feedback loop)
f. Micturition powerful enough then another signal is sent through Pudendal nerve to inhibit external sphincter (internal relaxes passively when pressure is 20 - 40 cm H2O)
g. Voluntary relaxation of external sphincter allows for urination
h. Flow thru urethra stimulates parasympathic system, sustaining bladder contraction

Micturition Reflex• stretch reflex initiated by filling of the bladder with
urine which results in bladder wall contraction• mediated by sensory stretch receptors in the
bladder wall,specially by receptors in the posterior urethra
BLADDER
SPINAL CORD(sacral segments)
Sensory stretch receptorDetrusor muscle
PELVIC NERVE(Sensory Fibers)
PELVIC NERVE(Parasympathetic
Motor Fibers)

Voluntary Control of Micturition
1. Micturition reflex can be inhibited by:a. Ponsb. Cerebral cortex
2. Voluntary contraction of external bladder sphincter means emptying can be delayed even if a micturition reflex occurs (can go and stop voluntarily)
3. Voluntary emptying:a. Contraction of abdominal muscles causes ↑ pressure in bladder
micturition reflex and inhibition of external sphincterb. Voluntary relaxation of external sphincter
Problems:Atonic Bladder - destruction of sensory fibers
Traumatic spinal cord injuryOverflow incontinence.
Automatic Bladder - spinal cord injury above sacral region
Micturition reflex is intact but uncontrolled

Micturition Abnormalities• Atonic Bladder - destruction of
sensory fibers– Traumatic spinal cord injury– Overflow incontinence.
• Automatic Bladder - spinal cord injury above sacral region– Micturition reflex is intact
but uncontrolled

Evaluation of
Kidney function

The kidney function tests are grouped into:
• Testing renal blood flow.
• Testing glomerular filtration.
• Testing tubular activity.

The volume by PAH clearance • PAH is freely filtered and secreted but not
reabsorbed.• The extraction ratio of PAH is 90% i.e. only 90%
of PAH in renal arterial blood is removed in a single circulation. This is because only 90% of RPF go to the nephrons.
RPF = about 625 mL/min.• A derivative of PAH, radioactive iodine PAH may
be used. The concentration of this substance in blood and urine is estimated by determination of its radioactivity.
The distribution • The distribution of renal blood flow may be
monitored by radio-active xenon.
Assessment of Renal Blood Flow

1. Inulin clearance.2. Creatinine clearance. 3. Urea clearance. 4. Blood urea and serum
creatinineblood urea; normal 20-40
mg/dL. (nonspecific test)Plasma creatinine; normal 0.6 –
1.5 mg/dL. (more accurate).
Assessment of Glomerular Filtration

Inulin• Polyssacharide molecule with MW =
5200• Not produced in the body• Requires IV infusion• Freely filtered• Not reabsorbed or secreted• Used to determine GFR ~
radioactive iothalamate and creatinine

Inulin• Generalizations:1. Filtered and not reabsorbed or
secreted – clearance rate of a substance equals that of inulin
2. Reabsorbed - clearance rate of a substance is less than that of inulin
3. Secreted - clearance rate of a substance is greater than that of inulin

Creatinine• By-product of muscle metabolism• Cleared almost entirely by
glomerular filtration• Ca also be used to assess GFR• Errors:A small amount is secreted by the
tubules: excreted creatinine exceeds amount filtered
Error in measurin plasma creatinine: overestimate of plasma cratinine


(1) Tests of tubular ability to concentrate and dilute urine
• Specific gravity of urine• Water concentration test
• Water dilution test(2) Tests of tubular ability to
absorbe glucose and secrete PAH Glucose tubular maximum (Tm
Glucose)Para-amino hippuric acid tubular
maximum (Tm PAH)
Assessment of Tubular Function

Tubular transport maximum (Glucose & PAH)

PAHA tubular maximum (Tm PAHA)

Use of Clearance to Quantify Kidney Function Use of Clearance to Quantify Kidney Function
TermTerm EquationEquation UnitsUnits
Clearance rate (CClearance rate (Css)) ml/minml/min
Glomerular filtration rate Glomerular filtration rate (GFR)(GFR)
Clearance ratio Clearance ratio NoneNone
Effective renal plasma flow Effective renal plasma flow (ERPF)(ERPF)
ml/minml/min

Renal plasma flow Renal plasma flow (RPF)(RPF)
ml/minml/min
Renal blood flow (RBF)Renal blood flow (RBF) ml/minml/min
Excretion rate Excretion rate Excretion rate = UExcretion rate = Uss x V x V mg/min, mg/min, mmol/min, or mmol/min, or mEq/minmEq/min
Reabsorption rateReabsorption rate Reabsorption rate = Filtered load – Excretion Reabsorption rate = Filtered load – Excretion raterate = (GFR x P= (GFR x Pss) – (U) – (Uss x V) x V)
mg/min, mg/min, mmol/min, or mmol/min, or mEq/minmEq/min
Secretion rateSecretion rate Secretion rate = Excretion rate – Filtered loadSecretion rate = Excretion rate – Filtered load mg/min, mg/min, mmol/min, or mmol/min, or mEq/minmEq/min

SubstanceSubstance Clearance rate Clearance rate (ml/min)(ml/min)
GlucoseGlucose 00
SodiumSodium 0.90.9
ChlorideChloride 1.31.3
PotassiumPotassium 12.012.0
PhosphatePhosphate 25.025.0
InulinInulin 125.0125.0
CreatinineCreatinine 140.0140.0

Water and
Electrolyte Balance

I. Control of ECF volume (defense of volume)
Factors controlling ECF volumel) ADH
When ECF volume decreasesADH causing increase in water reabsorption by distal tubules
and collecting ducts of the kidney → increase ECF volume.
When ECF volume increases It causes inhibition of ADH secretion that increases water
excretion and decreases ECF volume.
2) Role of the kidneyWhen ECF volume decreases
stimulation of aldosterone secretion. increase in tubular reabsorption of Na.
When ECF volume increases inhibit release of aldosterone which increase urinary excretion
of Na and water causing decrease of ECF volume.

I. Control of ECF volume (defense of volume)
3) Renin-angiotensin-aldosterone system: When ECF volume decreases, decrease in blood pressure
stimulates renin secretion from the juxtaglumerular apparatus of the kidney.

I. Control of ECF volume (defense of volume)
4) Thirst mechanism:When ECF volume decrease: this stimulates thirst
center in hypothalamus that leads to increase in water intake.
5) Volume receptors: Present in the atria and great veins near the heart. When ECF volume decreases, they send impulses to the
hypothalamus causing reflex increase in sympathetic discharge with activation of renin-angiotensin system.
6) Atrial natriuretic peptide (ANP):Increase in ECF volume causes release of ANP which
acts on the kidney to increase Na+ and water excretion.

II. Control of ECF Osmolarity (defense of tonicity)
Factors controlling ECF osmolarity
1) ADH osmoreceptor mechanism.
2) Thirst mechanism.When ECF osmolarity increase (hypertonicity)a) Stimulate osmoreceptors in hypothalamus:
which increase ADH secretion and increase water reabsorption in kidney.
b) Stimulation of thirst sensation:Hypertonicity stimulates thirst center in the hypothalamus that
increase water intake.
Stimuli which increase thirst includeIncreased extracellular fluid osmolarity.Decrease in extracellular fluid volume.Decrease in arterial pressure.Angiotensin II.Dryness of mouth.
Conversely when osmolarity decrease (hypotonicity)a- Inhibition of ADH secretion .b- Inhibition of thirst center.

II. Control of ECF Osmolarity (defense of tonicity)