Wednesday, July 29 – Sunday, August 2 Indiana Convention Center Indianapolis, Indiana.
1
Gregory T. Hale, Ph.D.
Psychologist
Indianapolis, Indiana
COSTS……………..
Legitimate and expected changes in the quality of life for injured workers are real
Loss of psychological benefits related to working and being productive is often overlooked and minimized
About 95% of WC claims involve a real accident at work
About 6-7 billion of the estimated 60 billion spent on WC claims is related to fraud
Actual cost of SSA disability fraud is unknown. Why?
1
2

2
CONTEXT MATTERS
We are often examining and treating people in a context that is not neutral……people have expectations
Sometimes we evaluate because we want to know who we are dealing with (i.e., influence of preexisting psychological disorder)
When a substantial external incentive exists (PI claim, disability application, compensation seeking, evasion of criminal prosecution) then consideration of malingering must be acknowledged
Research findings – litigating patients v. controls – higher functioning and more satisfied with their lives pre-injury than the controls/also report lower functioning post-accident than controls
3
4

3
CRITICAL ISSUES FOR EMPLOYERS,
CLAIMS EXAMINERS,
CASE MANAGERS,
AND LAWYERS
Diversity of human behavior
Tend to underestimate the influence of psychological factors
Fail to fully investigate pre-existing psychological conditions
Human behavior is complex, unpredictable, rigid
Many claimants are motivated by factors that are unidentified
All of us tend to personalize our stress – “what happened to me is different and worse than anything you have ever experienced.”
Weak relationship between distress and pathology
“Who is injured is often more important than the injury”
5
6

4
SYM
PTO
MS
TIME
CONCUSSION
Force
Symptoms improve over time
24-48 hrs: headache, fatigue, cognitive px, balance px
What is the typical recovery time in healthy young adult with norisk factors for protracted recovery?
10 to 14 days
7
8

5
Keep this in mind -- Harvard Medical School study
Depression and anxiety disorders
Substance abuse
Posttraumatic stress disorder
Adjustment disorders
Pain disorders
Rarely see more serious psychological disorders
BEHAVIORAL RISK FACTORS AFFECTING
DETERMINATION OF CAUSATION
Biological predispositions and early life experiences
The meaningfulness of social supports
The role of enduring personality traits
9
10

6
WHAT DO WE KNOW ABOUT
WHAT DETERMINES COSTS IN A
MEDICAL CLAIM
Variables associated with high cost claimants:– Retained an attorney
– Required surgical intervention
– Had a diagnosable psychological disturbance
– Injured workers in litigation were more likely to exhibit psychological disturbance
High cost of litigation partially results from failure to identify and treat hidden psychological issues
Cases often produce long term disability with minimal evidence of disease
Loss of faith in medical system turns claimant to attorneys for help in receiving psychological and medical treatment
STANDARDS RELATED TO CAUSATION
Indiana and psychological injury claims
Variability between states – KY, IL
Causal Analysis needs to be objective
11
12

7
CATEGORIZATION OF
PSYCHOLOGICAL CLAIMS IN WC
Physical disorders contributing to a psychological disorder
Psychophysiological reactions in which psychological factors or disorder contribute to a physical illness
Psychological disorders resulting from a mental injury
SO WHERE DO PSYCHOLOGISTS FIT IN A WC
CLAIM?
CLARIFICATION OF BEHAVIORAL ASPECTS OF
THE CASE
MEDICAL AND BEHAVIORAL
INTERVENTIONS CAN BE DESIGNED TO ADDRESS
PSYCHOLOGICAL FACTORS
DETERMINING WHICH ASPECTS OF THE
BEHAVIOR ARE WORK-RELATED OR PRE-
EXISTING
13
14

8
Psychologists Psychiatrists Social Workers
Marriage and Family
Therapists
Mental Health Technicians
School Psychologists
Psychometrists Primary Care Physician
15
16
9
COMPONENTS OF A
PSYCHOLOGICAL EVALUATION?
Interview (avoid only using self-report)
Psychological testing
Record review
Mental status observation
Comparison of data from multiple sources
17
18

10
ADMINISTRATION AND
INTERPRETATION OF
PSYCHOLOGICAL TESTING
Utilize properly trained evaluators
Tests need to be administered in a professional manner
Issues of reliability and validity are extremely important in litigated cases
Use of multiple tests can enhance the strength of the testing data
Can help evaluate progress in treatment and impairment
Test battery:– Personality inventories
– Cognitive tests
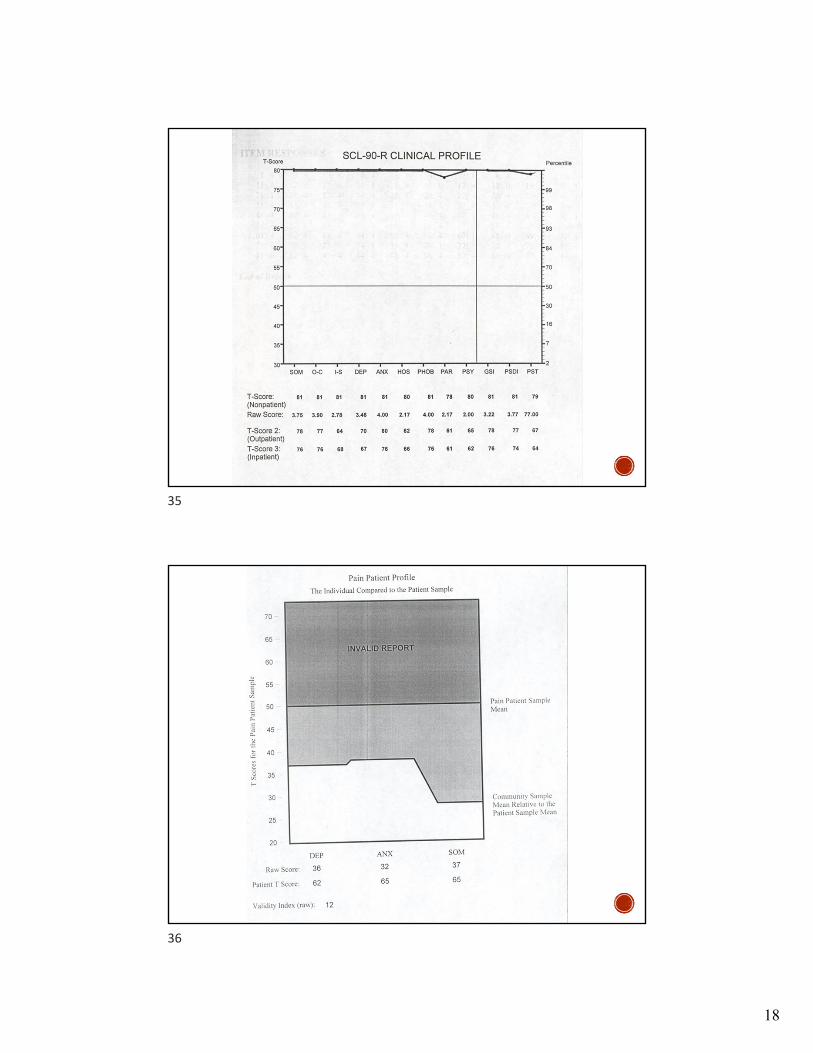
– Symptom checklists
– Specialized inventories
Limitations of psychological tests
19
20
11
QUESTIONS OF CAUSATION
Understanding base rate data for psychological disorders
Was there an accident or injury?
Did the injury arise out of and in the course of employment, personal injury, or ordinary life events?
Did the injury aggravate or accelerate the course and severity of the existing condition?
Is there a relationship between the understood pre-existing condition and the current symptoms?
APPROACHES TO THE
EXAMINATION
Malingering
Defensiveness
Irrelevant or Random Responding
Honest Responding
Hybrid Responding
Responses maybe adaptive to an adversarial evaluation and when the stakes for the claimant are high
Sometimes there is a hidden desired outcome
21
22
12
23
24
13
25
26
14
DECEPTION AND
MALINGERING
Excessive symptom report
Overly favorable presentation in the context of significant symptom report
Reporting unusual combinations of symptoms or experiencing all symptoms
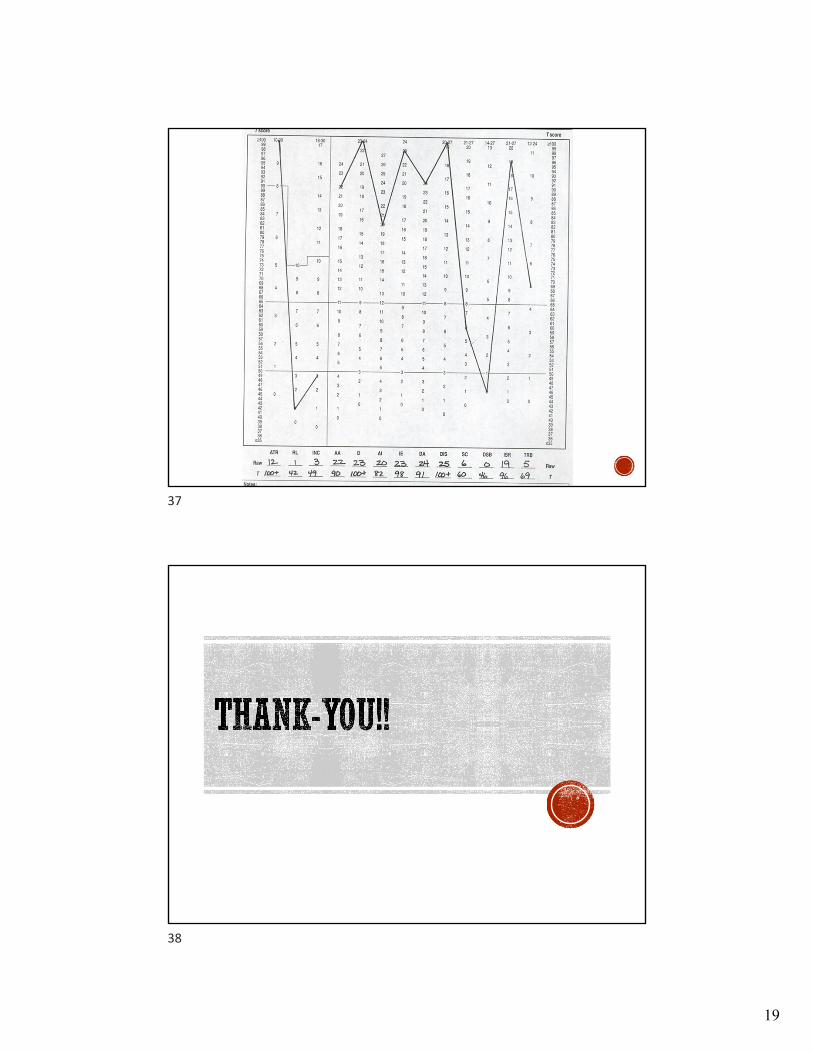
Invalid response patterns on psychometric testing
Profile not fitting normative groups
WHAT ARE THE NUMBERS? PROBABLE SYMPTOM
EXAGGERATION AND
MALINGERING
29% Personal Injury
30% SSA disability
8% Medical cases
However, recent research suggests………
>50% of SSA disability cases involve either malingering or probable malingering based on PVT data
27
28
15
HOW DO I DETERMINE IF
SOMEONE “INTENDS” TO
DECEIVE?
Need multiple indicators of symptoms exaggeration or test underperformance
Absence of viable alternative explanations for atypical performance
It is the combined improbability of findings, in the context of external incentive, without any viable alternative explanation that establishes intent.
CLINICAL PICTURE OF MALINGERING
Eager to discuss and call attention to symptoms
Attributes symptoms unrelated to the accident to the litigation/claim
Overdramatically magnifies symptoms
Over endorses symptoms
Endorses rare symptoms
Endorses overly specific symptoms with unrealistic accuracy
Endorses bizarre or ridiculous symptoms
Symptoms and their course are inconsistent with recognizable mental disorder
Symptom report and functional limitations are inconsistent with claimant’s previous report and the observation of others
Symptoms worsen when observed
Focuses on the degree of impairment rather than the condition itself
Rarely mentions the ability to learn new skills or perform different or modified job
Scores above the cutoff for malingering on psychological and/or neuropsychological tests
29
30

16
PROFILE OF THE
DISABILITY PRONE
PATIENT
Symptom magnification
Pain avoidance behavior
Psychological distress
Job dissatisfaction
Treatment dependency
Catastrophizing as a coping strategy
Pending litigation
IMPAIRMENT AND
DISABILITY
Relationship between physical impairments, pain, and disability is modest
Disability and impairment is affected by factors other than structural pathology
Physical pathology has a minor role in predicting disability
31
32
17
33
34
18
35
36
19
37
38