Pronóstico en Afasia Post Stroke_ Control Bibliográfico 1
7
Post-stroke aphasia prognosis: a review of patient-related and stroke-related factorsEmily Plowman PhD 1 Brecken Hentz MS 2 and Charles Ellis Jr PhD 3 1 Assistant Professor, Department of Communication Sciences and Disorders, College of Behavioral and Community Sciences, University of South Florida, Tampa, FL, USA 2 Staff Therapist, Department of Speech Pathology and Audiology, Duke University Medical Center, Durham, NC, USA 3 Associate Professor, Department of Health Sciences & Research, College of Health Professions, Medical University of South Carolina, Charleston, SC, USA Keywords aphasia, prognosis, recovery Correspondence Dr Charles Ellis Jr Medical University of South Carolina Department of Health Sciences and Research College of Health Professions 77 President Street, MSC 700 Charleston, SC 29425 USA E-mail: [email protected] Accepted for publication: 9 February 2011 doi:10.1111/j.1365-2753.2011.01650.x Abstract Rationale, aims and objectives Recovery of language function in individuals with post- stroke aphasia is associated with a variety of patient and stroke-related indices. Amidst a complex interaction of a multitude of variables, clinicians are faced with the arduous challenge of predicting aphasia recovery patterns and subsequently, long-term outcomes in these individuals. Unfortunately, predictive factors are highly variable making prognosis of aphasia recovery difficult. Therefore, the objective of this review was to assess the influence of patient-related and stroke-related factors on language recovery in individuals with post-stroke aphasia. Methods We completed a literature review to assess and identify evidence-based patient and stroke-related variables shown to be influential in aphasia recovery. Results A range of patient-related (gender, handedness, age, education, socio-economic status and intelligence) and stroke-related indices (initial severity, lesion site and lesion size) were identified as potential influential factors to post-stroke aphasia recovery. Initial severity of aphasia emerged as the factor most predictive of long-term aphasia recovery. Other influential factors of post-stroke language recovery included lesion site and size. Conclusions Stroke-related factors, including aphasia severity, lesion site and lesion size, appear most critical to post-stroke aphasia recovery. The findings presented in this review offer clinicians an evidenced-based framework to assist in prediction of post-stroke aphasia recovery patterns and subsequent long-term functional communication outcomes. Introduction Each year approximately 795 000 people experience a stroke and many are left with serious long-term disability [1]. Of those who experience a stroke, approximately 100 000 will acquire aphasia during the acute phase of recovery and an estimated one million Americans are currently living with aphasia [2]. Aphasia is defined as ‘an acquired communication disorder caused by brain damage that impairs a person’s ability to understand, produce and use language’ (p. 2) [3]. Aphasia can result from a variety of neuro- logical disorders; however, stroke is the predominate neurological condition associated with aphasia and will therefore constitute the focus of this review. There exists a comprehensive literature related to prognostic indicators for general stroke recovery. For example, the presence of prior stroke, old age, urinary and bowel incontinence, visuospa- tial deficits and initial Functional Independence Measure (FIM) scores below 60 have all been identified as negative prognostic indicators for general post-stroke function [4–6]. A clear under- standing of the specific factors critical to the prediction of aphasia recovery patterns, however, is yet to emerge. Even in the absence of this much needed and critical prognostic information, clinicians are constantly challenged to predict aphasia recovery. A prognosis is a prediction of the course of a disease or condi- tion based upon experience, intuition and evidence-based informa- tion [7]. Determining a prognosis in aphasia requires consideration of a multitude of inter-related patient-specific and stroke-specific variables believed to influence functional outcomes for individuals with aphasia. Patient-related variables include: age, handedness, gender, educational level, intelligence, motivation, depression, family support, beliefs and attitude regarding health care, and access to medical treatment. In contrast, stroke-related indices include: site of lesion, size of lesion, aphasia type and pattern of recovery, and initial aphasia severity. Identifying the correct com- bination of factors critical to an accurate prognosis is a daunting task for the new and even experienced clinician. Clinicians are Journal of Evaluation in Clinical Practice ISSN 1365-2753 © 2011 Blackwell Publishing Ltd, Journal of Evaluation in Clinical Practice 18 (2012) 689–694 689
-
Upload
andre-pozo-valdes -
Category
Documents
-
view
4 -
download
2
description
paper sobre pronostico de afasia
Transcript of Pronóstico en Afasia Post Stroke_ Control Bibliográfico 1
-
Post-stroke aphasia prognosis: a review of patient-relatedand stroke-related factorsjep_1650 689..694Emily Plowman PhD1 Brecken Hentz MS2 and Charles Ellis Jr PhD3
1Assistant Professor, Department of Communication Sciences and Disorders, College of Behavioral and Community Sciences, University of SouthFlorida, Tampa, FL, USA2Staff Therapist, Department of Speech Pathology and Audiology, Duke University Medical Center, Durham, NC, USA3Associate Professor, Department of Health Sciences & Research, College of Health Professions, Medical University of South Carolina,Charleston, SC, USA
Keywordsaphasia, prognosis, recovery
CorrespondenceDr Charles Ellis JrMedical University of South CarolinaDepartment of Health Sciences andResearchCollege of Health Professions77 President Street, MSC 700Charleston, SC 29425USAE-mail: [email protected]
Accepted for publication: 9 February 2011
doi:10.1111/j.1365-2753.2011.01650.x
AbstractRationale, aims and objectives Recovery of language function in individuals with post-stroke aphasia is associated with a variety of patient and stroke-related indices. Amidsta complex interaction of a multitude of variables, clinicians are faced with the arduouschallenge of predicting aphasia recovery patterns and subsequently, long-term outcomes inthese individuals. Unfortunately, predictive factors are highly variable making prognosis ofaphasia recovery difficult. Therefore, the objective of this review was to assess the influenceof patient-related and stroke-related factors on language recovery in individuals withpost-stroke aphasia.Methods We completed a literature review to assess and identify evidence-based patientand stroke-related variables shown to be influential in aphasia recovery.Results A range of patient-related (gender, handedness, age, education, socio-economicstatus and intelligence) and stroke-related indices (initial severity, lesion site and lesionsize) were identified as potential influential factors to post-stroke aphasia recovery. Initialseverity of aphasia emerged as the factor most predictive of long-term aphasia recovery.Other influential factors of post-stroke language recovery included lesion site and size.Conclusions Stroke-related factors, including aphasia severity, lesion site and lesion size,appear most critical to post-stroke aphasia recovery. The findings presented in this reviewoffer clinicians an evidenced-based framework to assist in prediction of post-stroke aphasiarecovery patterns and subsequent long-term functional communication outcomes.
IntroductionEach year approximately 795 000 people experience a stroke andmany are left with serious long-term disability [1]. Of those whoexperience a stroke, approximately 100 000 will acquire aphasiaduring the acute phase of recovery and an estimated one millionAmericans are currently living with aphasia [2]. Aphasia is definedas an acquired communication disorder caused by brain damagethat impairs a persons ability to understand, produce and uselanguage (p. 2) [3]. Aphasia can result from a variety of neuro-logical disorders; however, stroke is the predominate neurologicalcondition associated with aphasia and will therefore constitute thefocus of this review.
There exists a comprehensive literature related to prognosticindicators for general stroke recovery. For example, the presenceof prior stroke, old age, urinary and bowel incontinence, visuospa-tial deficits and initial Functional Independence Measure (FIM)scores below 60 have all been identified as negative prognostic
indicators for general post-stroke function [46]. A clear under-standing of the specific factors critical to the prediction of aphasiarecovery patterns, however, is yet to emerge. Even in the absenceof this much needed and critical prognostic information, cliniciansare constantly challenged to predict aphasia recovery.
A prognosis is a prediction of the course of a disease or condi-tion based upon experience, intuition and evidence-based informa-tion [7]. Determining a prognosis in aphasia requires considerationof a multitude of inter-related patient-specific and stroke-specificvariables believed to influence functional outcomes for individualswith aphasia. Patient-related variables include: age, handedness,gender, educational level, intelligence, motivation, depression,family support, beliefs and attitude regarding health care, andaccess to medical treatment. In contrast, stroke-related indicesinclude: site of lesion, size of lesion, aphasia type and pattern ofrecovery, and initial aphasia severity. Identifying the correct com-bination of factors critical to an accurate prognosis is a dauntingtask for the new and even experienced clinician. Clinicians are
bs_bs_banner
Journal of Evaluation in Clinical Practice ISSN 1365-2753
2011 Blackwell Publishing Ltd, Journal of Evaluation in Clinical Practice 18 (2012) 689694 689
-
now faced with new challenges due to the widespread distributionof misleading information available to the public on the internetthat must be carefully considered when discussing and providingprognostic information to caregivers and family members. In thisreview we will examine a range of variables previously docu-mented and that are believed to influence aphasia outcomes poststroke. Unfortunately, studies designed to examine aphasia prog-nosis have either examined the natural history of aphasia orprimarily examined one aphasia outcome prognostic variable inde-pendently [8]. Consequently, few previous reports have attemptedto consolidate the evidence to present a clear picture for clinicians.Therefore, it was our goal to systematically organize availableevidence so as to provide clinicians the foundation for a moreaccurate and evidenced-based prognostic approach to aphasiarecovery in post-stroke individuals.
Research design and methodsFor this review, we considered all studies that recruited patientswith a diagnosis of aphasia following stroke and reported stan-dardized measures designed to predict aphasia outcomes. We usedthe Cochrane Collaboration Group search strategy as outlined inthe Cochrane Handbook for Systematic Reviews of Interventions[9]. We searched: Medline (from 19662007), CINAHL (from19822007), PsycINFO (19662007), REHABDATA (19662007) and the Cochrane Library. The following (MESH) termswere used in our search: stroke, aphasia, prognosis and termsassociated with the prediction of aphasia outcomes including: age;handedness; gender; educational level; intelligence; site of lesion;size of lesion; aphasia type and pattern of recovery; and initialaphasia severity. We also considered all other variables thatare known to influence general stroke outcomes such as: motiva-tion; depression; family support; beliefs and attitude regardinghealth care; and access to medical treatment. From these terms,we attempted to identify other terms associated with aphasiaprognosis.
We identified studies that reported aphasia outcomes even ifthe studys primary purpose was not designed to identify aphasiaprognosis. We completed hand searches of reference lists and asearch of Google Scholar. We also searched for reviews of aphasiaprognosis and websites that reported variables associated withaphasia prognosis. Given the heterogeneity of studies, we decideda priori not to use meta-analysis to pool the results of studies.Instead, the presentation of results provides a qualitative assess-ment of the studies.
Results
Patient-related factors
Gender
According to the National Institute of Neurological and Commu-nication Disorders and Stroke (NINCDS) Stroke Data Bank, theincidence of aphasia post stroke is slightly higher among womencompared with men in the USA [10]. Similarly, in an internationalstudy of 269 stroke patients, a higher incidence of aphasia wasobserved among women in 80 individuals with aphasia [11]. Incontrast, other investigators have reported a higher incidence of
post-stroke aphasia in men. Kertesz and Sheppard [12] reported a1.6:1.0 ratio (male : female) in 204 patients with aphasia, whileBasso et al. [13] observed a similar male to female ratio of 1.5:1.0in 192 patients with aphasia.
Consequently, evidence regarding gender and prevalence of spe-cific aphasia type is also mixed. For example, De Renzi andcolleagues [14] reported a higher prevalence of males with non-fluent aphasia, and Hier et al. [10] documented that Wernickesglobal and anomic aphasias were more common in women whileBrocas aphasia was somewhat more prevalent in men. Con-versely, other studies have not reported any association betweengender and type of aphasia. Specifically, Engelter and colleagues[11] observed no gender differences on measures of auditory com-prehension, expressive language and ratings of everyday commu-nication function, and Godefroy et al. [15] concluded that sexdid not significantly influence aphasia type in 295 individuals.In addition, evidence has shown that gender does not appear tobe related to aphasia recovery [1618]. In summary, evidence islargely equivocal and gender does not appear to significantlyimpact incidence of aphasia, aphasia type or recovery patterns inpost-stroke individuals.
Handedness
As early as the 19th century, Paul Broca proposed that the lefthemisphere was dominant for language functions in right-handedindividuals. Interestingly, in 1958, Surbirana noted that prognosisfor aphasia recovery following stroke is better for those who areleft-handed compared with right-handed individuals. A morerecent study of handedness and language dominance amonghealthy adults, however, reported that left-handedness is not nec-essarily a consequence of right-hemisphere language dominance,but rather left-handedness increases the likelihood of right-hemisphere dominance [19]. Consequently, it appears that left-handed and ambidextrous individuals are more likely to have abi-hemispheric representation of language and therefore the poten-tial for greater recovery from aphasia [20]. While it appears thatambidextrous and left-handed individuals may have a greaterneural capacity for recovery, handedness when studied as an inde-pendent factor has not been shown to influence aphasia recovery[21,22].
Age
Early studies of influential prognostic indicators of acute strokeranked age as a primary variable [23,24]. Consequently, olderindividuals are more likely to have aphasia than younger ones [11].Engelter and colleagues [11] studied 269 individuals followingtheir first ischemic stroke, and reported the mean age of aphasicpatients to be five years higher than their non-aphasic counterparts(80 vs. 75 years). In addition, Smith noted that aphasia severityincreased with advancing age [25]. Further, studies of age andaphasia type demonstrate that individuals with fluent aphasia tendto be older than individuals with non-fluent aphasia. [21,26]De Renzi and colleagues [14] reported that individuals withBrocas aphasia were significantly younger than individuals withWernickes aphasia, and similarly, Kertesz and Sheppard [12]documented that individuals with Brocas aphasia were youngerthan individuals with other aphasia types.
Aphasia prognosis E. Plowman et al.
2011 Blackwell Publishing Ltd690
-
While age does appear to influence both the incidence and typeof post-stroke aphasia, the impact of age on aphasia recovery isunclear. Younger patients have been reported to demonstrate ahigher recovery rate than older patients [27]; however, conflictingreports have deemed age to be a poor prognostic indicator ofaphasia recovery [16,17,22,28]. Thus, even though age has beenidentified as an important prognostic indicator for general strokerecovery, no consistent data have emerged regarding age andexpressive or receptive language recovery patterns post stroke. Insum, incidence of aphasia is higher in older stroke patients, andof these patients a higher likelihood of fluent forms is seen inolder adults and non-fluent forms in younger adults with no clearrelationship between age and the ability for language recovery inpost-stroke aphasia.
Education, socio-economic status and intelligence
Carl Wernicke (1874) proposed that aphasia in highly educatedindividuals would differ from those with less education; however,a clear relationship between educational level and aphasia recov-ery has yet to emerge [25]. This is likely due to the existence of aplethora of confounds, such as literacy levels, general intelligence,existence of learning disabilities, socio-economic status (SES) andcultural influences, that make this area particularly challenging tostudy. Indeed, the existence of these confounds requires adjust-ments and careful planning of experimental designs in order todraw any valid conclusions regarding the impact of education onaphasia.
Educational achievement is frequently linked to SES, a variableinvolving the complex interaction of a wide range of associatedfactors including: income, insurance status, access to health careand health-related beliefs that are associated with stroke-relatedoutcomes [11,2933]. Thus, one might hypothesize that SES rep-resents a related variable critical to aphasia prognosis. Two studieshave examined the relationship between SES and educationwith aphasia. Connor and colleagues examined 39 individuals withaphasia at both 4 and 103 months post onset to determine thedegree to which educational achievement and SES influencedinitial aphasia severity and recovery [34]. These authors noted thatboth educational achievement and SES did not impact aphasiarecovery rate; however, initial aphasia severity was worse in thosewith less education then in those with a higher level of education.In contrast to this later finding, Lazar and colleagues reported norelationship between education level, initial aphasia severity orrecovery [35]. While data regarding the influence of educationallevels on aphasia outcomes remain limited, data to date suggestno consistent relationship between education level and aphasiaseverity or recovery.
Closely associated with educational achievement level, higherpre-morbid intelligence has been examined as a potential posi-tive prognostic factor for individuals with aphasia. Kertesz andMcCabe measured non-verbal intelligence in 111 individuals withaphasia and 52 control patients taken from the same hospital witha range of medical diagnoses [36]. The authors observed that whilenon-verbal intelligence was impaired in the former, overall therewere no significant differences between the two groups. In asimilar study, David and Skilbeck investigated the impact ofintelligence on aphasia severity and recovery of language functionpost-stroke in 148 patients [37]. These authors reported a correla-
tion between intelligence level and initial aphasia severity but notwith recovery of language function following stroke. In an earlyreview of prognostic indicators of aphasia recovery, Ferro et al.concluded that intelligence did not appear to influence aphasiarecovery [20]. Thus, there is some data to suggest that intelligencemay impact initial aphasia severity; however, it appears that thisvariable does not influence aphasia recovery patterns post stroke.
Stroke-related factors
Initial stroke and aphasia severity
Recent studies indicate that initial stroke severity is associatedwith initial aphasia severity, which in turn, is associated withpoorer outcomes [27,28,38]. For example, Laska et al. docu-mented that individuals with milder aphasia tended to have ahigher degree of aphasia recovery [27]. Similar findings werereported by Pedersen and colleagues, who studied 270 aphasiapatients post-stroke using the Western Aphasia Battery AphasiaQuotient (WAB AQ) [28]. These authors observed that languageoutcomes could be predicted by initial stroke and aphasia severitybut not by other factors such as age, gender or aphasia type. At1-year post-neurological insult, aphasic symptoms still remainedfor 61% of these individuals; however, the majority demonstrateda reduction in the severity of language deficits with some degree offunctional improvement [28]. While a strong relationship existedbetween initial aphasia severity and language outcomes, the rela-tionship was most predictive of long-term language outcomesduring the 2- to 4-week post-stroke period, suggesting an optimalprognostic time window. Thus, clinicians are encouraged to con-sider initial stroke, and subsequently initial aphasia severity, aspredictive factors when determining aphasia prognosis.
Site and size of lesion
A wealth of literature supports the notion that lesion size andlocation constitute important clinical predictors of aphasia type.For example, certain semantic deficits are correlated with damageto the left posterior temporal and inferior parietal region [39].Similarly, large lesions to the third frontal gyrus involving Brocasarea and the lower part of the precentral gyrus, in conjunction withlesions in the opercular and insular regions, are associated withmore severe naming difficulties and overall expressive languagedeficits in individuals with Brocas aphasia [40]. Likewise, lesionslocalized to the left superior temporal gyrus are common inpatients with significant and persisting global aphasia and gener-ally associated with poor language recovery [41].
Lesion location and size have also been documented to influ-ence aphasia recovery patterns in post-stroke individuals. Mazzoniand colleagues documented different recovery patterns based onlesion size in 45 patients with aphasia [42]. Specifically, patientswith small lesions exhibited significant improvement in auditorycomprehension, verbal expression and written expression; patientswith medium sized lesions improved in both auditory compre-hension and verbal expression; while patients with large lesionsimproved in only auditory comprehension. Goldenberg and Sprattexamined lesion size specific to Wernickes area in 18 individualswith aphasia over an 8-week recovery period [43]. Size of lesionnegatively influenced overall recovery, with larger lesions to the
E. Plowman et al. Aphasia prognosis
2011 Blackwell Publishing Ltd 691
-
temporobasal area associated with lower improvement and lesstotal recovery. Likewise, Knopman and colleagues noted that per-sistent non-fluency was associated with large lesions located in theRolandic cortical regions extending into underlying white matter[44]. Finally, a recent study of 669 patients with aphasia by Maasand colleagues indicated that better outcomes were associated withclinically and radiographically smaller strokes as well as lowerprestrike disability [8].
Studies by Naeser and colleagues have generally concluded thataphasia recovery is associated with both the specific location andthe size of lesion, rather than just the later [4548]. Specifically, asignificant correlation was present between comprehension skillsand the amount of temporal lobe involvement in Wernickes area,however not between comprehension abilities and total tempo-ro-parietal lesion size. Furthermore, patients with lesions that en-compassed more than half of Wernickes area generally had poorcomprehension skills, even 1 year post stroke [46]. Finally, theseauthors reported that anteriorinferior temporal lobe lesions thatextended into the middle temporal gyrus were associated with theworst language recovery. A later study by this group did not iden-tify a single neuroanatomical area where extent of lesion coulddiscriminate outcomes for spontaneous speech fluency; however,Naeser et al. concluded that spontaneous speech fluency was sig-nificantly influenced by lesion size in two subcortical white matterareas when combined [48]. These two areas consisted of the mostmedial and rostral portion of the subcallosal fasiculus and theperiventricular white matter area near the body of the lateral ven-tricle and deep to the lower motor/sensory cortex area of themouth.
Alexander and colleagues also noted that size of lesion in criti-cal language areas was highly predictive of aphasia severity andrecovery patterns [49]. While shallow lesions of the frontal oper-culum resulted in transient disorders of language output withnormal articulation and repetition, lesions that extended into thedeep white matter of the frontal isthmus and anterior periventricu-lar white matter resulted in more severe and prolonged non-fluentverbal output. Alexander et al. concluded that a more severelyimpaired expressive language profile resulted from disruption ofthe limbic-frontal projections and cingulatedstriatalfrontal con-nections critical to expressive language output [49]. Similarly,Kertesz et al. reported that poor recovery in comprehension abili-ties was associated with larger lesions involving the supramarginalgyrus, angular gyri and superior temporal area, while sparing ofthe superior temporal and middle temporal gyri was associatedwith good recovery of auditory comprehension in 22 individualswith Wernickes aphasia [50]. Finally, Selness and colleaguesexamined 39 individuals with aphasia to determine the relationshipbetween lesion localization, lesion volume and auditory com-prehension outcomes [51]. In this study, poorer outcomes wereassociated with lesions to the posterior superior temporal andinfrasylvian supramarginal region and lesion volume was gener-ally not associated with auditory comprehension abilities unlessextremely large or small.
Metabolic factors, not typically measured by clinicians, havealso been noted to influence short- and long-term aphasia progno-sis. Evidence suggests that cerebral metabolic rates of glucosein language regions, and cerebral blood flow adjacent to lesionsduring the early post-stroke period, are critical to aphasia recovery.[52,53] Furthermore, the proposed mechanism by which adequate
cerebral blood flow returns to the damaged brain is a dynamic andcomplex process occurring bilaterally and might therefore influ-ence aphasia recovery because the right hemisphere appears tohave a definitive role in the early recovery of language function[5357]. For example, Karbe and colleagues reported that whilethe left superior temporal cortex was critical in determining long-term prognosis in aphasia, the right hemisphere was important forspeech processing when the left hemisphere areas were perma-nently damaged [56]. This has led to the hypothesis that long-termaphasia recovery is linked to the right hemispheres slow andgradual compensatory role in language function, particularlyduring the early post-stroke time period [53].
Finally, the continuous advent of more sophisticated neuroim-aging techniques has significantly advanced our current under-standing of the neural mechanisms by which aphasia recovers[58]. Recent neuroimaging studies have provided compelling evi-dence to support the notion that the brain has the ability to engagein structural and functional plasticity that supports language recov-ery in individuals with aphasia [58]. For example, Schlaug et al.,using diffusion tensor imaging, reported increases in the numberand volume of fibres in the right arcuate fasiculus (AF), a largewhite matter tract with reciprocal connections between Brocasand Wernickes area, in six individuals with moderate to severeexpressive aphasia [59]. Schlaug et al. observed increases inthe number and volume of AF fibres that were accompaniedby improvements in verbal expression following 75 sessions ofmelodic intonation therapy [59]. Furthermore, a significant trendemerged between the relative improvement in conversationalinformation units (elicited from a picture description task andduring conversational speech) and the absolute change in thenumber of AF fibres. In this small sample, it appears that structuralbrain plasticity may have facilitated functional improvement inexpressive language function following an intensive and salientrehabilitation program.
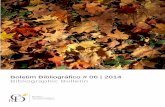
ConclusionsA multitude of inter-related variables must be considered whendetermining a prognosis for aphasia (see Table 1). While a prog-nosis may only represent a clinicians best guess, the currentliterature offers evidence, that when integrated, could offer clini-cians a framework to facilitate a more accurate evidence-based
Table 1 Summary of patient and stroke-related aphasia prognosticvariables
Variable Prognostic Evidence
Patient-related variablesGender -Handedness -Age *Education/socio-economic status -Intelligence *
Stroke-related variablesInitial stroke and aphasia severity +Site/size of lesion +
+, positive evidence; *, mixed/unclear evidence; -, no significantevidence.
Aphasia prognosis E. Plowman et al.
2011 Blackwell Publishing Ltd692
-
assessment of a patients potential for recovery [7]. This paperhighlights evidence that can serve as a guide for such evidence-based prognostic statements. Specifically, we report that whilepatient-related variables (age, gender, handedness, education andintelligence) do not appear to significantly influence aphasia prog-nosis; stroke-related variables such as initial stroke and aphasiaimpairment level, lesion size and lesion location, do influencerecovery patterns. Clinicians are encouraged to consider thesestroke-related prognostic indicators when faced with the arduoustask of predicting an individuals potential for functional recoveryin post-stroke aphasia.
AcknowledgementsPortions of this paper were presented at the 2008 AnnualMeeting of the American Speech-Language-Hearing Associationin Chicago Illinois. We would also like to acknowledge SarahKnauff, Lacy Stephens, Brittni Carnes, Laura Shaffer and MaureenMahan for their contributions to this work.
References1. Lloyd-Jones, D., Adams, R. J., Brown, T. M., et al. (2010) Heart
disease and stroke statistics 2010 update: a report from the AmericanHeart Association. Circulation, 121 (7), e46e215.
2. National Aphasia Association (2008) Aphasia Frequently AskedQuestions. http://www.aphasia.org/Aphasia%20Facts/aphasia_faq.html (last accessed 1 July 2008).
3. LaPointe, L. (2005) Foundations: adaptation, accomodation, aristos.Aphasia and Related Neurogenic Language Disorders, 3rd edn (ed. L.LaPointe), pp. 118. New York: Thieme.
4. Jongbloed, L. (1986) Prediction of function after stroke: a criticalreview. Stroke, 17 (4), 765776.
5. Kelly, P. J., Furie, K. L., Shafqat, S., Rallis, N., Chang, Y. & Stein, J.(2003) Functional recovery following rehabilitation after hemorrhagicand ischemic stroke. Archives of Physical Medicine and Rehabilita-tion, 84 (7), 968972.
6. Ween, J. E., Mernoff, S. T. & Alexander, M. P. (2000) Recovery ratesafter stroke and their impact on outcome prediction. Neurorehabilita-tion and Neural Repair, 14 (3), 229235.
7. Brookshire, R. H. (2007) Introduction to Neurogenic CommunicationDisorders, 7th edn. St. Louis, MO: Mosby Elsevier.
8. Maas, M. B., Lev, M. H., Ay, H., Singhal, A. B., Greer, D. M., Smith,W. S., Harris, G. J., Halpern, E. F., Koroshetz, W. J. & Furie, K. L.(2010) The Prognosis for Aphasia in Stroke. Journal of Stroke andCerebrovascular Diseases (in press); E-pub ahead of print, Dec 27.
9. The Cochrane Corporation (2009) The Cochrane Handbook forSystematic Reviews 2.09. http://www.cochrane.org/training/cochrane-handbook (last accessed 11 February 2011).
10. Hier, D. B., Yoon, W. B., Mohr, J. P., Price, T. R. & Wolf, P. A. (1994)Gender and aphasia in the Stroke Data Bank. Brain and Language, 47(1), 155167.
11. Engelter, S. T., Gostynski, M., Papa, S., Frei, M., Born, C., Ajdacic-Gross, V., Gutzwiller, F. & Lyrer, P. A. (2006) Epidemiology ofaphasia attributable to first ischemic stroke: incidence, severity,fluency, etiology, and thrombolysis. Stroke, 37 (6), 13791384.
12. Kertesz, A. & Sheppard, A. (1981) The epidemiology of aphasic andcognitive impairment in stroke: age, sex, aphasia type and lateralitydifferences. Brain, 104 (Pt 1), 117128.
13. Basso, A., Capitani, E. & Moraschini, S. (1982) Sex differences inrecovery from aphasia. Cortex, 18, 469375.
14. De Renzi, E., Faglioni, P. & Ferrari, P. (1980) The influence of sex
and age on the incidence and type of aphasia. Cortex, 16 (4), 627630.
15. Godefroy, O., Dubois, C., Debachy, B., Leclerc, M. & Kreisler, A.(2002) Vascular aphasias: main characteristics of patients hospitalizedin acute stroke units. Stroke, 33 (3), 702705.
16. Inatomi, Y., Yonehara, T., Omiya, S., Hashimoto, Y., Hirano, T. &Uchino, M. (2008) Aphasia during the acute phase in ischemic stroke.Cerebrovascular Diseases, 25 (4), 316323.
17. Lendrem, W. & Lincoln, N. B. (1985) Spontaneous recovery of lan-guage in patients with aphasia between 4 and 34 weeks after stroke.Journal of Neurology, Neurosurgery, and Psychiatry, 48 (8), 743748.
18. Sarno, M. T., Buonaguro, A. & Levita, E. (1985) Gender and recoveryfrom aphasia after stroke. The Journal of Nervous and Mental Disease,173 (10), 605609.
19. Knecht, S., Drager, B., Deppe, M., Bobe, L., Lohmann, H., Floel, A.,Ringelstein, E. B. & Henningsen, H. (2000) Handedness and hemi-spheric language dominance in healthy humans. Brain, 123 (Pt 12),25122518.
20. Ferro, J. M., Mariano, G. & Madureira, S. (1999) Recovery fromaphasia and neglect. Cerebrovascular Diseases, 9 (Suppl. 5), 622.
21. Pedersen, P. M., Jorgensen, H. S., Nakayama, H., Raaschou, H. O. &Olsen, T. S. (1995) Aphasia in acute stroke: incidence, determinants,and recovery. Annals of Neurology, 38 (4), 659666.
22. Pickersgill, M. J. & Lincoln, N. B. (1983) Prognostic indicatorsand the pattern of recovery of communication in aphasic strokepatients. Journal of Neurology, Neurosurgery, and Psychiatry, 46 (2),130139.
23. Millikan, C. H. & Moersch, F. P. (1953) Factors that influence prog-nosis in acute focal cerebrovascular lesions. A.M.A. Archives ofNeurology and Psychiatry, 70 (5), 558562.
24. Smith, A. (1962) Ambiguities in concepts and studies of braindamage and organicity. The Journal of Nervous and MentalDisease, 135, 311326.
25. Smith, A. (1971) Objective indices of severity of chronic aphasia instroke patients. The Journal of Speech and Hearing Disorders, 36 (2),167207.
26. Miceli, G., Caltagirone, C., Gainotti, G., Masullo, C., Silveri, M. C. &Villa, G. (1981) Influence of age, sex, literacy and pathologic lesion onincidence, severity and type of aphasia. Acta Neurologica Scandinav-ica, 64 (5), 370382.
27. Laska, A. C., Hellblom, A., Murray, V., Kahan, T. & Von Arbin, M.(2001) Aphasia in acute stroke and relation to outcome. Journal ofInternal Medicine, 249 (5), 413422.
28. Pedersen, P., Vinter, K. & Olsen, T. (2004) Aphasia after stroke: type,severity, and prognosis. Cerebrovascular Diseases, 17, 3543.
29. Asch, S. M., Kerr, E. A., Keesey, J., Adams, J. L., Setodji, C. M.,Malik, S. & McGlynn, E. A. (2006) Who is at greatest risk for receiv-ing poor-quality health care? The New England Journal of Medicine,354 (11), 11471156.
30. Bernheim, S. M., Ross, J. S., Krumholz, H. M. & Bradley, E. H.(2008) Influence of patients socioeconomic status on clinical man-agement decisions: a qualitative study. Annals of Family Medicine, 6(1), 5359.
31. Cox, A. M., McKevitt, C., Rudd, A. G. & Wolfe, C. D. (2006) Socio-economic status and stroke. Lancet Neurology, 5 (2), 181188.
32. Franks, P., Fiscella, K., Beckett, L., Zwanziger, J., Mooney, C. &Gorthy, S. (2003) Effects of patient and physician practice socioeco-nomic status on the health care of privately insured managed carepatients. Medical Care, 41 (7), 842852.
33. Kurth, T. & Berger, K. (2007) The socioeconomic stroke puzzle.Stroke, 38 (1), 45.
34. Connor, L. T., Obler, L. K., Tocco, M., Fitzpatrick, P. M. & Albert, M.L. (2001) Effect of socioeconomic status on aphasia severity andrecovery. Brain and Language, 78 (2), 254257.
E. Plowman et al. Aphasia prognosis
2011 Blackwell Publishing Ltd 693
-
35. Lazar, R. M., Speizer, A. E., Festa, J. R., Krakauer, J. W. & Marshall,R. S. (2008) Variability in language recovery after first-time stroke.Journal of Neurology, Neurosurgery, and Psychiatry, 79 (5), 530534.
36. Kertesz, A. & McCabe, P. (1975) Intelligence and aphasia: perfor-mance of aphasics on Ravens coloured progressive matrices (RCPM).Brain and Language, 2 (4), 387395.
37. David, R. M. & Skilbeck, C. E. (1984) Raven IQ and language recov-ery following stroke. Journal of Clinical Neuropsychology, 6 (3),302308.
38. Berthier, M. L. (2005) Poststroke aphasia: epidemiology, pathophysi-ology and treatment. Drugs and Aging, 22 (2), 163182.
39. Hart, J., Jr & Gordon, B. (1990) Delineation of single-word semanticcomprehension deficits in aphasia, with anatomical correlation.Annals of Neurology, 27 (3), 226231.
40. Hojo, K., Watanabe, S., Tasaki, H., Sato, T. & Metoki, H. (1985)[Localization of lesions in aphasia clinical-CT scan correlations(Part III): Paraphasia and meaningless speech]. No To Shinkei, 37 (2),117126.
41. Hanlon, R. E., Lux, W. E. & Dromerick, A. W. (1999) Global aphasiawithout hemiparesis: language profiles and lesion distribution. Journalof Neurology, Neurosurgery, and Psychiatry, 66 (3), 365369.
42. Mazzoni, M., Vista, M., Pardossi, L., Avila, L., Bianchi, F. & Moretti,P. (1992) Spontaneous evolution of aphasia after ischaemic stroke.Aphasiology, 6 (4), 387396.
43. Goldenberg, G. & Spatt, J. (1994) Influence of size and site of cerebrallesions on spontaneous recovery of aphasia and on success of languagetherapy. Brain and Language, 47 (4), 684698.
44. Knopman, D. S., Selnes, O. A., Niccum, N., Rubens, A. B., Yock, D.& Larson, D. (1983) A longitudinal study of speech fluency in aphasia:CT correlates of recovery and persistent nonfluency. Neurology, 33(9), 11701178.
45. Naeser, M. A., Gaddie, A., Palumbo, C. L. & Stiassny-Eder, D. (1990)Late recovery of auditory comprehension in global aphasia. Improvedrecovery observed with subcortical temporal isthmus lesion vs. Wer-nickes cortical area lesion. Archives of Neurology, 47 (4), 425432.
46. Naeser, M. A., Helm-Estabrooks, N., Haas, G., Auerbach, S. & Srini-vasan, M. (1987) Relationship between lesion extent in Wernickesarea on computed tomographic scan and predicting recovery of com-prehension in Wernickes aphasia. Archives of Neurology, 44 (1),7382.
47. Naeser, M. A. & Palumbo, C. L. (1994) Neuroimaging and languagerecovery in stroke. Journal of Clinical Neurophysiology, 11 (2), 150174.
48. Naeser, M. A., Palumbo, C. L., Helm-Estabrooks, N., Stiassny-Eder,D. & Albert, M. L. (1989) Severe nonfluency in aphasia. Role of themedial subcallosal fasciculus and other white matter pathways inrecovery of spontaneous speech. Brain, 112 (Pt 1), 138.
49. Alexander, M. P., Naeser, M. A. & Palumbo, C. (1990) Brocas areaaphasias: aphasia after lesions including the frontal operculum. Neu-rology, 40 (2), 353362.
50. Kertesz, A., Lau, W. K. & Polk, M. (1993) The structural determinantsof recovery in Wernickes aphasia. Brain and Language, 44 (2), 153164.
51. Selnes, O. A., Knopman, D. S., Niccum, N., Rubens, A. B. & Larson,D. (1983) Computed tomographic scan correlates of auditory compre-hension deficits in aphasia: a prospective recovery study. Annals ofNeurology, 13 (5), 558566.
52. Karbe, H., Kessler, J., Herholz, K., Fink, G. R. & Heiss, W. D. (1995)Long-term prognosis of poststroke aphasia studied with positron emis-sion tomography. Archives of Neurology, 52 (2), 186190.
53. Mimura, M., Kato, M., Sano, Y., Kojima, T., Naeser, M. & Kashima,H. (1998) Prospective and retrospective studies of recovery in aphasia.Changes in cerebral blood flow and language functions. Brain, 121 (Pt11), 20832094.
54. Crinion, J. & Price, C. J. (2005) Right anterior superior temporalactivation predicts auditory sentence comprehension followingaphasic stroke. Brain, 128 (Pt 12), 28582871.
55. Jodzio, K., Drumm, D. A., Nyka, W. M., Lass, P. & Gasecki, D. (2005)The contribution of the left and right hemispheres to early recoveryfrom aphasia: a SPECT prospective study. Neuropsychological Reha-bilitation, 15 (5), 588604.
56. Karbe, H., Thiel, A., Weber-Luxenburger, G., Herholz, K., Kessler, J.& Heiss, W. D. (1998) Brain plasticity in poststroke aphasia: what isthe contribution of the right hemisphere? Brain and Language, 64 (2),215230.
57. Knopman, D. S., Rubens, A. B., Selnes, O. A., Klassen, A. C. &Meyer, M. W. (1984) Mechanisms of recovery from aphasia: evidencefrom serial xenon 133 cerebral blood flow studies. Annals of Neurol-ogy, 15 (6), 530535.
58. Raymer, A. M., Beeson, P., Holland, A., et al. (2008) Translationalresearch in aphasia: from neuroscience to neurorehabilitation. Journalof Speech Language and Hearing Research, 51 (1), S259S275.
59. Schlaug, G., Marchina, S. & Norton, A. (2009) Evidence for plasticityin white-matter tracts of patients with chronic Brocas aphasia under-going intense intonation-based speech therapy. Annals of the New YorkAcademy of Sciences, 1169, 385394.
Aphasia prognosis E. Plowman et al.
2011 Blackwell Publishing Ltd694
-
Copyright of Journal of Evaluation in Clinical Practice is the property of Wiley-Blackwell and its content maynot be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express writtenpermission. However, users may print, download, or email articles for individual use.