Primary synovial osteochondromatosis of the hip: extracapsular patterns of spread
6
Skeletal Radiol (2004) 33:210–215 DOI 10.1007/s00256-003-0737-7 ARTICLE Philip Robinson Lawrence M. White Rita Kandel Robert S. Bell Jay S. Wunder Primary synovial osteochondromatosis of the hip: extracapsular patterns of spread Received: 29 September 2003 Accepted: 21 November 2003 Published online: 18 February 2004 # ISS 2004 P. Robinson Department of Radiology, St. James’ University Hospital, Leeds, UK L. M. White ( ) ) Department of Medical Imaging, Mount Sinai and University Health Network, University of Toronto, Toronto, Canada e-mail: [email protected] R. Kandel Laboratory of Pathology Medicine, Mount Sinai and University of Toronto, Toronto, Canada R. S. Bell · J. S. Wunder University Musculoskeletal Oncology Unit, Mount Sinai and University of Toronto, Toronto, Canada Abstract Objective: To identify pat- terns of extracapsular extension of synovial osteochondromatosis of the hip. Design and patients: Seven cases of synovial osteochondromatosis of the hip were retrospectively re- viewed. Imaging performed included conventional radiography (n=7), ar- thrography (n=1), CT (n=3) and MR imaging (n=3). Disease extent on imaging was assessed for each patient and the presence of intra-articular effusion, capsular abnormality and osteochondral bodies recorded. The presence and distribution of extra- articular spread was also assessed and correlated with the surgical findings. In all cases diagnosis was confirmed by biopsy, with all patients undergo- ing tumor resection with or without synovectomy. Results: In five cases (5/7) disease extended beyond the hip capsule, while the remaining two cases (2/7) were confined to the hip joint. These findings were confirmed at surgery. Two distinct patterns of extracapsular spread were identified. The first pattern, noted in three cases, involved tumor extension along ilio- psoas. The second pattern, noted in five cases, involved tumor extension along the obturator externus fat plane. In three cases both patterns were present. Conclusions: Extra-articular spread of synovial osteochondroma- tosis is common. Patterns of extra- articular spread may be predictable based on involvement of recognized periarticular bursae of the hip joint. Bursal patterns of extra-articular spread include extension into the iliopsoas bursa as well as communi- cation along the obturator externus bursa of the hip. Keywords Hip · MR, pelvis · MR, synovial osteochondromatosis Introduction Synovial osteochondromatosis, or synovial chondrometa- plasia, is a rare benign neoplastic condition of the synovium. The majority of opinion considers it to arise from the metaplastic transformation of subsynovial cells which may subsequently undergo endochondral ossifica- tion [1, 2]. These metaplastic nodules then pedunculate and may shed osteochondral or chondral bodies into the synovial cavity. The resultant intra-articular bodies can subsequently enlarge on obtaining nourishment from the synovial fluid. The disease commonly occurs in men in the fourth to fifth decades and predominantly involves the appendic- ular joints. It is usually a chronic and monoarticular disease, with the knee most commonly affected followed by the elbow, hip and ankle [1, 2, 3, 4, 5]. Pure extra- articular disease has been described arising from within tendon sheaths or bursae and there have also been reports of extra-articular spread from primary articular disease, but these are relatively rare manifestations [6, 7, 8, 9, 10, 11]. The aim of this study was to retrospectively review patterns of disease present in synovial osteochondroma- tosis of the hip and describe patterns of extra-articular spread.
-
Upload
philip-robinson -
Category
Documents
-
view
212 -
download
0
Transcript of Primary synovial osteochondromatosis of the hip: extracapsular patterns of spread

Skeletal Radiol (2004) 33:210–215DOI 10.1007/s00256-003-0737-7 A R T I C L E
Philip RobinsonLawrence M. WhiteRita KandelRobert S. BellJay S. Wunder
Primary synovial osteochondromatosisof the hip: extracapsular patterns of spread
Received: 29 September 2003Accepted: 21 November 2003Published online: 18 February 2004� ISS 2004
P. RobinsonDepartment of Radiology,St. James’ University Hospital,Leeds, UK
L. M. White ())Department of Medical Imaging,Mount Sinai andUniversity Health Network,University of Toronto,Toronto, Canadae-mail: [email protected]
R. KandelLaboratory of Pathology Medicine,Mount Sinai and University of Toronto,Toronto, Canada
R. S. Bell · J. S. WunderUniversity Musculoskeletal Oncology Unit,Mount Sinai and University of Toronto,Toronto, Canada
Abstract Objective: To identify pat-terns of extracapsular extension ofsynovial osteochondromatosis of thehip. Design and patients: Seven casesof synovial osteochondromatosis ofthe hip were retrospectively re-viewed. Imaging performed includedconventional radiography (n=7), ar-thrography (n=1), CT (n=3) and MRimaging (n=3). Disease extent onimaging was assessed for each patientand the presence of intra-articulareffusion, capsular abnormality andosteochondral bodies recorded. Thepresence and distribution of extra-articular spread was also assessed andcorrelated with the surgical findings.In all cases diagnosis was confirmedby biopsy, with all patients undergo-ing tumor resection with or withoutsynovectomy. Results: In five cases(5/7) disease extended beyond the hipcapsule, while the remaining twocases (2/7) were confined to the hip
joint. These findings were confirmedat surgery. Two distinct patterns ofextracapsular spread were identified.The first pattern, noted in three cases,involved tumor extension along ilio-psoas. The second pattern, noted infive cases, involved tumor extensionalong the obturator externus fat plane.In three cases both patterns werepresent. Conclusions: Extra-articularspread of synovial osteochondroma-tosis is common. Patterns of extra-articular spread may be predictablebased on involvement of recognizedperiarticular bursae of the hip joint.Bursal patterns of extra-articularspread include extension into theiliopsoas bursa as well as communi-cation along the obturator externusbursa of the hip.
Keywords Hip · MR, pelvis · MR,synovial osteochondromatosis
Introduction
Synovial osteochondromatosis, or synovial chondrometa-plasia, is a rare benign neoplastic condition of thesynovium. The majority of opinion considers it to arisefrom the metaplastic transformation of subsynovial cellswhich may subsequently undergo endochondral ossifica-tion [1, 2]. These metaplastic nodules then pedunculateand may shed osteochondral or chondral bodies into thesynovial cavity. The resultant intra-articular bodies cansubsequently enlarge on obtaining nourishment from thesynovial fluid.
The disease commonly occurs in men in the fourth tofifth decades and predominantly involves the appendic-ular joints. It is usually a chronic and monoarticulardisease, with the knee most commonly affected followedby the elbow, hip and ankle [1, 2, 3, 4, 5]. Pure extra-articular disease has been described arising from withintendon sheaths or bursae and there have also been reportsof extra-articular spread from primary articular disease,but these are relatively rare manifestations [6, 7, 8, 9, 10,11]. The aim of this study was to retrospectively reviewpatterns of disease present in synovial osteochondroma-tosis of the hip and describe patterns of extra-articularspread.

211
Materials and methods
Seven cases of synovial osteochondromatosis of the hip referred toour institution between 1988 and 2000 were retrospectivelyreviewed. All seven cases were referred for imaging by experiencedorthopedic oncology surgeons for investigation of hip pain anddysfunction. Patients consisted of four men and three women with amedian age of 29 years (range 21–48 years). Imaging modalitiesavailable for review included radiography (n=7), arthrography(n=1), CT (n=3) and MR imaging (n=3). One of the patients had nocross-sectional imaging modalities available for review, withradiographs the only preoperative imaging evaluation.
Image evaluation
For each patient disease extent on imaging was retrospectivelyassessed by two experienced musculoskeletal radiologists byconsensus and correlated with the surgical findings.
All MR imaging was performed on a 1.5 T magnet (Signa,General Electric, Milwaukee, Wis.) using a quadrature surface torso(Medical Advances, Milwaukee, Wis.). Axial and coronal T1-weighted, conventional spin echo (TR/TE 583/ 8) and axial, coronaland sagittal T2-weighted fat-suppressed, fast spin echo (4166/ 104,echo train length 8) sequences were obtained through the pelvis.For MR image evaluation the hip joint was assessed for boneerosion, joint effusion, capsular abnormality (normal or thickened),intra-articular bodies and the presence or absence of extra-articularbursal extension of disease. If present the contour of the bursalmargin was assessed as normal or irregular/thickened (consistentwith capsular disease or synovitis) and the presence of bursalbodies recorded (Fig. 1). Iliopsoas bursal involvement was definedas a fluid signal (low T1-weighted, high T2-weighted signalintensity) collection extending proximally deep to iliopsoas andcontinuous with the anterior hip joint with internal heterogeneoussignal, irregular thick walls and bodies (Fig. 1) [12, 13]. MRimaging criteria of obturator externus bursal involvement weredefined as a fluid signal (low T1-weighted, high T2-weightedsignal intensity) collection with internal heterogeneous signal,
irregular thick walls and bodies extending medially along thesuperior margin of the obturator externus muscle, and contiguousposterolaterally with the hip joint (Fig. 1) [14].
Radiographs (anteroposterior and lateral oblique) (Fig. 2) andCT examinations (contiguous axial 5 mm sections, Lightspeed,General Electric, Milwaukee, Wis.) (Figs. 3, 4) were assessed forthe presence or absence of bone erosion, joint space loss and thedistribution of any soft tissue mass or osteochondral bodies. Thediagnosis of specific bursal involvement was made with the sameanatomical criteria used for MR imaging assessment (Figs. 3, 4)[15, 16]. Arthrography was performed after fluoroscopically guidedinjection of iodinated contrast [9 ml, diatrizoate meglumine 60%(Hypaque), Nycomed Amersham, Princeton, N.J.] into the hip joint.Images were assessed for the extent of the capsular recesses and thepresence of bodies or filling defects [17].
Surgical and pathological evaluation
In six cases (6/7) diagnosis was confirmed by image-guided biopsybut in one patient no preoperative biopsy was performed. Allpatients subsequently underwent tumor resection surgery with orwithout synovectomy (mean time from imaging to surgery 22 days,range 5–36 days). Operative details were obtained from dictatedsurgical notes and discussion with the operative surgeons. Atoperation the surgeons prospectively recorded the presence ofperiarticular bursae with all detected bursae resected and sent forpathological analysis regarding disease involvement and synovitis.Pathological analysis consisted of gross evaluation, paraffin-em-bedding of representative tissue and histopathological evaluation ofhematoxylin and eosin (H&E)-stained sections by light microscopy(Fig. 4D).
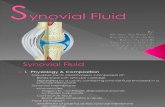
Fig. 1A–C A 21-year-old man with synovial osteochondromatosisof the left hip. MR imaging showed obturator externus andiliopsoas bursa involvement confirmed at surgery. A Coronal T2-weighted fat-suppressed, fast spin echo (4,166/104, echo trainlength 8) image shows a hip joint effusion, capsular thickening andintracapsular debris. On the medial aspect of the femoral neck thereis continuous extension in the obturator externus bursa (arrows)along the upper border of the obturator externus muscle (asterisk).
B Axial T2-weighted fat-suppressed, fast spin echo (4,166/104,echo train length 8) image shows an anterior iliopsoas bursa(asterisk) herniating around the iliopsoas tendon (arrow) with asimilar intrinsic signal to the hip effusion. C Coronal T2-weightedfat-suppressed, fast spin echo (4,166/104, echo train length 8)image shows the iliopsoas bursa (arrowheads) extending proxi-mally into the pelvis. Note the multiple low-signal bodies (arrow)in the bursa

212
Results
Image evaluation
Evaluation of all imaging modalities showed distension ofthe hip joint with bodies or filling defects in six cases.The remaining case had only radiographs available forreview. Two distinct patterns of extracapsular spreadwere identified. The first pattern, noted in three cases,involved tumor extension along the iliopsoas bursal plane.
The second pattern, noted in five, cases involved tumorextension from the hip joint inferomedially along theobturator externus fat plane. In three cases both patternsof spread were present.
On MR evaluation (n=3) there was an effusion in allhip joints with evidence of synovial thickening andmultiple small filling defects present. Mild anterior andposterior erosion of the femoral neck was present in onecase. On MR imaging one case illustrated diseaseconfined to the hip joint with no erosion. The additionaltwo cases with MR imaging showed extra-articularspread: one case into both the iliopsoas and obturatorexternus bursa and one case into the obturator externusbursa alone.
On radiographic evaluation (n=7) calcified/ossifiedbodies were present in five cases; however, in the twocases with no mineralized bodies evident MR imagingconfirmed intra-articular bodies. Anterior and posteriorbone erosion was present in two (2/7) cases. Extra-articular extension along the obturator externus bursacould only be identified on one radiograph (no otherimaging modalities available for review in this case).
On CT evaluation (n=3) a hip joint effusion andosteochondral bodies were present in all cases. No boneerosions were identified. Extra-articular extension alongboth the obturator externus and iliopsoas bursae wasidentified in two cases with the other case showingdisease confined to the hip joint.
Arthrography (n=1) performed in one case confirmedcapsular thickening and filling defects in the hip joint butdid not define any communication with periarticularbursae. However, MR imaging in the same patient didshow disease in the obturator externus bursa.
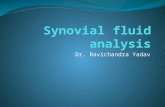
Fig. 2 A 30-year-old man with synovial osteochondromatosis ofthe left hip. Obturator externus bursal involvement confirmed atsurgery. A Anteroposterior radiograph shows a well-defined masscontaining multiple fine osseous bodies (arrows) extending medi-ally and overlapping the obturator foramen. B Oblique radiographconfirms medial extension of the mass as well as anterior femoralneck erosion (arrowheads) and a small lateral osteophyte
Fig. 3 A 23-year-old man with synovial osteochondromatosis ofthe left hip. CT imaging showed obturator externus and iliopsoasspread confirmed at surgery. Axial CT image at the level of thelesser trochanter shows a well-defined soft tissue mass (asterisk) inthe obturator externus muscle plane with multiple peripheralosseous bodies of varying sizes

213
Surgical and pathological evaluation
At surgery synovial osteochondromatosis was present inall hip joints with an effusion and capsular thickening. Intwo cases disease was confined to the hip joint. In theremaining five cases continuous extra-articular spread ofdisease into the iliopsoas bursa (n=3) and obturatorexternus bursa (n=5) (with both bursae involved in threecases) was confirmed. The iliopsoas bursal involvementextended proximally from the anterior hip joint capsuledeep to the iliopsoas tendon extending superiorly andinferiorly. The obturator externus bursa extended alongthe superior margin of the obturator externus muscle andoriginated from the posterior and inferior aspect of the hipjoint. This correlated with the extent of the bursaidentified on imaging preoperatively.
Gross analysis of the surgically resected bursae (n=5)and hip joint capsules (n=7) confirmed bursal diseasecontinuous with the primary hip pathology in all cases.Histologically synovial membrane containing nodules ofbenign hyaline-like chondroid was present. There wasvariable cellularity. Calcification and/or ossification waspresent in some nodules.
Discussion
To the best of our knowledge this paper describes thelargest review of synovial osteochondromatosis (or chon-dromatosis) of the hip with detailed extra-articular bursalinvolvement [1, 2, 3, 4, 8, 18, 19, 20]. The knee is thecommonest site of synovial osteochondromatosis, withthe hip varying between the second and fourth mostcommonly affected site (along with the elbow and ankle)[1, 2, 3, 8, 18]. Primary extra-articular synovial osteo-chondromatosis is rare but has been described in thetendon sheaths of the wrist, foot, arm and surrounding theknee [7, 8, 11]. Disease development in bursae is alsodescribed in primary bursae (e.g., ischial) as well asbursae associated with osteochondromata [7, 9, 21]. Inrelation to the hip joint there has been one report ofsynovial osteochondromatosis involving the iliopsoasbursa without primary hip joint involvement or commu-nication [7].
True extra-articular spread has rarely been reported inthe setting of synovial osteochondromatosis from aprimarily affected joint. This association has been mostcommonly reported in the knee with breaching of thecapsule posterolaterally or medially and one case ofextension into a popliteal bursa [2, 6, 7, 20]. Spread fromthe hip joint into the iliopsoas bursa with tracking into the
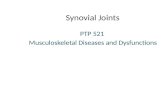
Fig. 4A–D A 29-year-old man with synovial osteochondromatosisof the right hip. CT imaging showed obturator externus andiliopsoas spread confirmed at surgery. A Axial CT image at thelevel of the sacroiliac joint shows an iliopsoas bursa (arrow)containing multiple osteochondral bodies. B Axial CT image at thelevel of the inferior symphysis pubis shows extensive osteochondralbodies in the iliopsoas (arrows) and obturator externus (arrowhead)
bursae. C Axial CT image just inferior to B shows better definitionof the separate iliopsoas (arrow) and obturator externus (arrow-head) involvement. D Photomicrograph showing a nodule ofhyaline-like cartilage in synovium. There are no binucleate chon-drocytes or cellular atypia. (Hematoxylin and eosin, originalmagnification �63)

214
pelvis has also been described [10, 20, 22, 23]. Theiliopsoas bursa is often present normally and lies deep tothe iliopsoas myotendon anterior to the hip capsule. In10–15% of cases the bursa normally communicates withthe anterior hip joint through a capsular defect betweenthe iliofemoral and iliopectineal ligaments (Fig. 1B) [12,13, 24]. However, the incidence of communicationincreases in the presence of synovitis and raised intra-capsular pressure, when the thin area of capsule separat-ing the bursa from the hip joint may potentially breakdown [12, 13, 14].
The obturator externus bursa lies on the superior aspectof the obturator externus muscle and tendon and extendsmedially from the posterior and inferior aspect of the hipjoint [14, 24, 25]. A paper recently described one case ofsynovial osteochondromatosis of the hip with extensioninto the obturator externus bursa [14]. In a similar mannerto the iliopsoas bursa it is thought there is a potentialposterior inferior communication of the hip capsule whichcan develop because of a chronic process involving thesynovium [13, 14]. A review of the literature shows anumber of cases of synovial osteochondromatosis thathave reported extra-articular spread from the hip joint, inwhich obturator externus bursa involvement may havebeen mistakenly attributed to a capsular breach oriliopsoas extension. One case reported by Eisenberg andJohnston [10] described primary hip disease with iliopso-as extension; however, there was also a collection in theobturator externus muscle plane although a formal obtu-rator externus bursa and communication was not de-scribed. Another case report of iliopsoas extension byGinai [26] presented a radiograph which shows extensionof osteochondral bodies medially toward the obturatorforamen. At surgery a large bursa was described andpresumed to be a medially displaced iliopsoas bursa.However, we also believe this may have been an obturatorexternus bursa because the radiograph presented isidentical to one in a surgically confirmed case ofobturator externus involvement in this study (Fig. 2). Arecent review by Kim et al. [22] presented MR imagingfindings in 15 cases of synovial osteochondromatosis ofthe hip. They described six cases (6/15) of extra-articularspread but did not detail the exact patterns of spread orassociated surgical features. However, two figures in thepaper show what is termed a medial herniation sac that issimilar in appearance to the obturator externus bursaextension described in the current study. The findings ofKim et al. along with those of the current study suggestthat bursal involvement is common in symptomaticsynovial osteochondromatosis of the hip.
Perhaps one reason why bursal extension associatedwith primary synovial osteochondromatosis of the hip hasnot been more frequently reported is that the majority ofpapers concerning the larger series of this condition were
collected before the advent of advanced cross-sectionalimaging [1, 2, 8, 18]. It is recognized that approximatelyone third of cases of synovial osteochondromatosis willnot have radio-opaque bodies evident on radiographs atpresentation. The radiographic evaluation in this studyshowed that opacities were not evident in two of sevencases and only in one case could periarticular extension ofmineralized bodies be accurately assessed. CT evaluationcan assess iliopsoas and extra-articular disease involvingthe hip joint [8, 16]. CT imaging in this study showedjoint-based disease in all cases and was accurate indefining periarticular extent. However, we found itsubjectively easier to define the tissue planes of thebursae on MR imaging, especially when both bursalpatterns were present [Fig. 4B). The use of MR imagingin evaluating synovial osteochondromatosis of the hip hasnot been evaluated extensively. MR imaging can accu-rately define synovitis and filling defects but this in itselfis still a nonspecific feature [22, 27]. We believe the truevalue of MR imaging lies in the accurate staging ofprimary disease and any extracapsular spread. Currentadvances in CT technology may negate some of theadvantages of MR imaging but these techniques could notbe evaluated in this current study. Arthrography has in thepast been utilized for evaluating synovial osteochondro-matosis but has been superseded by MR imaging [14, 17,22, 27]. In this study arthrography proved inaccurate fordefining the extent of the obturator externus bursa,presumably because the synovial tissue around the com-munication between the hip capsule and the bursa did notallow free flow of contrast.
Limitations of this study include the relatively smallnumber of patients for review; however, synovial osteo-chondromatosis is a rare condition. In this particularpatient group there may have been a referral bias as all thecases were referred by orthopedic oncology surgeons. Thestudy was also retrospective, with not all types of imagingmodality available for review.
This study confirms that extra-articular spread ofsynovial osteochondromatosis does occur and the patternsof extra-articular spread may be predictable based oninvolvement of recognized periarticular bursae of the hipjoint. From the small number of cases we have describedit appears that bursal extent is more common thanrestricted intracapsular disease in symptomatic patients.This may be due to the fact that symptomatic disease maynot present until late in the course of synovial osteochon-dromatosis and that the chronically raised intra-articularpressure determines the formation of the communicationbetween the joint and the adjacent bursa [13, 14]. Thisstudy confirms that the disease process can extend alongthis communication and is recognizable on imaging. It isimportant to recognize this finding for the preoperativeplanning in synovial osteochondromatosis of the hip.

215
References
1. Murphy F, Dahlin D, Sullivan C.Articular synovial chondromatosis.J Bone Joint Surg Am 1962; 44:77–86.
2. Milgram JW. Synovial osteochondro-matosis: a histopathological study ofthirty cases. J Bone Joint Surg Am1977; 59:792–801.
3. Trias A, Quintana O. Synovial chon-drometaplasia: review of world litera-ture and a study of 18 Canadian cases.Can J Surg 1976; 19:151–158.
4. Bloom R, Pattinson J. Osteochondro-matosis of the hip joint. J Bone JointSurg Br 1951; 33:80–84.
5. Hamada G. Osteochondromatosis of thehip joint. J Bone Joint Surg Br 1951;33:85–86.
6. Dunn AW, Whisler JH. Synovialchondromatosis of the knee withassociated extracapsular chondromas.J Bone Joint Surg Am 1973; 55:1747–1748.
7. Sim F, Dahlin D, Ivins JC. Extra-articular synovial chondromatosis. JBone Joint Surg Am 1977; 59:492–495.
8. Maurice H, Crone M, Watt I. Synovialchondromatosis. J Bone Joint Surg Br1988; 70:807–811.
9. Pope TL Jr, Keats TE, de Lange EE,Fechner RE, Harvey JW. Idiopathicsynovial chondromatosis in two unusualsites: inferior radioulnar joint and is-chial bursa. Skeletal Radiol 1987;16:205–208.
10. Eisenberg KS, Johnston JO. Synovialchondromatosis of the hip joint pre-senting as an intrapelvic mass: a casereport. J Bone Joint Surg Am 1972;54:176–178.
11. Lynn MD, Lee J. Periarticular teno-synovial chondrometaplasia. Report ofa case at the wrist. J Bone Joint SurgAm 1972; 54:450–452.
12. Steiner E, Steinbach LS, SchnarkowskiP, Tirman PF, Genant HK. Ganglia andcysts around joints. Radiol Clin NorthAm 1996; 34:395–425, xi–xii.
13. Steinbach LS, Schneider R, GoldmanAB, Kazam E, Ranawat CS, GhelmanB. Bursae and abscess cavities com-municating with the hip. Diagnosisusing arthrography and CT. Radiology1985; 156:303–307.
14. Robinson P, White LM, Agur A,Wunder J, Bell RS. Obturator externusbursa: anatomic origin and MR imagingfeatures of pathologic involvement.Radiology 2003; 228:230–234.
15. Zimmerman C, Sayegh V. RoentgenManifestations of synovial osteochon-dromatosis. AJR Am J Roentgenol1960;83:680–686.
16. Ginaldi S. Computed tomography fea-ture of synovial osteochondromatosis.Skeletal Radiol 1980; 5:219–222.
17. Prager RJ, Mall JC. Arthrographic di-agnosis of synovial chondromatosis.AJR Am J Roentgenol 1976; 127:344–346.
18. Christensen JH, Poulsen JO. Synovialchondromatosis. Acta Orthop Scand1975; 46:919–925.
19. McIvor R, King D. Osteochondroma-tosis of the hip joint. J Bone Joint SurgAm 1962; 44:87–97.
20. Blacksin MF, Ghelman B, FreibergerRH, Salvati E. Synovial chondromato-sis of the hip. Evaluation with aircomputed arthrotomography. Clin Im-aging 1990; 14:315–318.
21. Borges AM, Huvos AG, Smith J. Bursaformation and synovial chondrometa-plasia associated with osteochondro-mas. Am J Clin Pathol 1981; 75:648–653.
22. Kim SH, Hong SJ, Park JS, Cho JM,Kim EY, Ahn JM, et al. Idiopathicsynovial osteochondromatosis of thehip: radiographic and MR appearancesin 15 patients. Korean J Radiol 2002;3:254–259.
23. Lehner A. Zur Schleimbeutel- und Ge-lenkosteochondromatose. Schweiz MedWochenschr 1937; 67:634–636.
24. Agur A. Grant’s atlas of anatomy, 9thedn. Baltimore: Williams and Wilkins,1991.
25. Guerra J, Armbuster T, Resnick D,Goergen T, Feingold D, Niwayama G,et al. The adult hip: an anatomic study.Radiology 1978; 128:11–20.
26. Ginai AZ. Case report 607: Synovial(osteo) chondromatosis of left hip jointand iliopsoas bursa. Skeletal Radiol1990; 19:227–231.
27. Sundaram M, McGuire MH, Fletcher J,Wolverson MK, Heiberg E, Shields JB.Magnetic resonance imaging of lesionsof synovial origin. Skeletal Radiol1986; 15:110–116.