Prevention of cardiac fibrosis and left ventricular ... · fibrosis and left ventricular (LV)...
8
Prevention of cardiac fibrosis and left ventricular dysfunction in diabetic cardiomyopathy in rats by transgenic expression of the human tissue kallikrein gene CARSTEN TSCHO ¨ PE, 1 THOMAS WALTHER, JENS KO ¨ NIGER, FRANK SPILLMANN, DIRK WESTERMANN, FELICITAS ESCHER, MATTHIAS PAUSCHINGER, JOAO B. PESQUERO,* MICHAEL BADER, † HEINZ-PETER SCHULTHEISS, AND MICHEL NOUTSIAS Department of Cardiology and Pneumonology, Campus Benjamin Franklin, Charite ´-University Medicine, Free University of Berlin; *Department of Biophysics, Universidade Federal de Sa ˜o Paulo, Sa ˜o Paulo, Brazil; and † Max-Delbru ¨ ck-Center for Molecular Medicine, Berlin, Germany ABSTRACT Diabetic cardiomyopathy includes fibro- sis. Kallikrein (KLK) can inhibit collagen synthesis and promote collagen breakdown. We investigated cardiac fibrosis and left ventricular (LV) function in transgenic rats (TGR) expressing the human kallikrein 1 (hKLK1) gene in streptozotocin (STZ) -induced diabetic condi- tions. Six weeks after STZ injection, LV function was determined in male Sprague-Dawley (SD) rats and TGR(hKLK1) (n10/group) by a Millar tip catheter. Total collagen content (Sirius Red staining) and expres- sion of types I, III, and VI collagen were quantified by digital image analysis. SD-STZ hearts demonstrated significantly higher total collagen amounts than normo- glycemic controls, reflected by the concomitant incre- ment of collagen types I, III, and VI. This correlated with a significant reduction of LV function vs. normo- glycemic controls. In contrast, surface-specific content of the extracellular matrix, including collagen types I, III, and VI expression, was significantly lower in TGR(hKLK1)-STZ, not exceeding the content of SD and TGR(hKLK1) controls. This was paralleled by a preserved LV function in TGR(hKLK1)-STZ animals. The kallikrein inhibitor aprotinin and the bradykinin (BK) B2 receptor antagonist icatibant reduced the beneficial effects on LV function and collagen content in TGR(hKLK1)-STZ animals. Transgenic expression of hKLK1 counteracts the progression of LV contractile dysfunction and extracellular matrix remodeling in STZ-induced diabetic cardiomyopathy via a BK B2 receptor-dependent pathway.OTscho ¨pe, C., Walther, T., Ko ¨niger, J., Spillmann, F., Westermann, D., Escher, F., Pauschinger, M., Pesquero, J. B., Bader, M., Schult- heiss, H.-P., Noutsias, M. Prevention of cardiac fibrosis and left ventricular dysfunction in diabetic cardiomy- opathy in rats by transgenic expression of the human tissue kallikrein gene. FASEB J. 18, 828 – 835 (2004) Key Words: diabetes mellitus diabetic cardiomyopathy kal- likrein pathogenesis therapy transgenic animal Diabetes is an independent risk factor for left ventric- ular (LV) dysfunction (1). Primary myocardial injury has been shown even in the absence of hypertension and atherosclerosis in diabetic patients and so has been called ”diabetic cardiomyopathy” (2). The histopatho- logical changes found include diffuse myocardial de- generation with changes in the myocardial extracellu- lar matrix. The composition of the extracellular matrix, a complex network of structural proteins including collagen types I and III, provides architectural support for the muscle cells and plays an important role in myocardial function (3, 4). Several studies of diabetic cardiomyopathy have demonstrated an accumulation of myocardial collagen including types I, III, and VI, leading to interstitial and perivascular fibrosis which has been correlated with LV early diastolic and systolic dysfunction (5– 8). The mechanisms involved in these changes are still not completely understood. Behind myocardial microischemia due to focal changes in microvessels, nonenzymatic glycosylation of collagens, down-regulation, or reduced activity of collagen de- grading matrix metalloproteinases (MMP), increased transforming growth factor- (TGF-) activity or up- regulation in collagen mRNA expression are discussed as hallmarks for myocardial fibrosis in diabetic cardio- myopathy (5, 7–9). Remodeling of the extracellular matrix is also regulated by profibrotic acting peptides (e.g., angiotensin II, aldosterone, endothelin) and an- tagonistically acting systems like the kallikrein-kinin system (KKS) (10, 11). Kinins are important peptides mediating a diverse range of physiological and pathological functions of the cardiovascular system (12). The effector peptides of 1 Correspondence: Charite-University Medicine, Campus Benjamin Franklin, Department of Cardiology and Pneumo- nology, Free University of Berlin, Hindenburgdamm 30, D-12220 Berlin, Germany. E-mail: [email protected] doi: 10.1096/fj.03-0736com 828 0892-6638/04/0018-0828 © FASEB
Transcript of Prevention of cardiac fibrosis and left ventricular ... · fibrosis and left ventricular (LV)...

Prevention of cardiac fibrosis and left ventriculardysfunction in diabetic cardiomyopathy in ratsby transgenic expression of the human tissuekallikrein gene
CARSTEN TSCHOPE,1 THOMAS WALTHER, JENS KONIGER, FRANK SPILLMANN,DIRK WESTERMANN, FELICITAS ESCHER, MATTHIAS PAUSCHINGER,JOAO B. PESQUERO,* MICHAEL BADER,† HEINZ-PETER SCHULTHEISS,AND MICHEL NOUTSIASDepartment of Cardiology and Pneumonology, Campus Benjamin Franklin, Charite-UniversityMedicine, Free University of Berlin; *Department of Biophysics, Universidade Federal de Sao Paulo,Sao Paulo, Brazil; and †Max-Delbruck-Center for Molecular Medicine, Berlin, Germany
ABSTRACT Diabetic cardiomyopathy includes fibro-sis. Kallikrein (KLK) can inhibit collagen synthesis andpromote collagen breakdown. We investigated cardiacfibrosis and left ventricular (LV) function in transgenicrats (TGR) expressing the human kallikrein 1 (hKLK1)gene in streptozotocin (STZ) -induced diabetic condi-tions. Six weeks after STZ injection, LV function wasdetermined in male Sprague-Dawley (SD) rats andTGR(hKLK1) (n�10/group) by a Millar tip catheter.Total collagen content (Sirius Red staining) and expres-sion of types I, III, and VI collagen were quantified bydigital image analysis. SD-STZ hearts demonstratedsignificantly higher total collagen amounts than normo-glycemic controls, reflected by the concomitant incre-ment of collagen types I, III, and VI. This correlatedwith a significant reduction of LV function vs. normo-glycemic controls. In contrast, surface-specific contentof the extracellular matrix, including collagen types I,III, and VI expression, was significantly lower inTGR(hKLK1)-STZ, not exceeding the content of SDand TGR(hKLK1) controls. This was paralleled by apreserved LV function in TGR(hKLK1)-STZ animals.The kallikrein inhibitor aprotinin and the bradykinin(BK) B2 receptor antagonist icatibant reduced thebeneficial effects on LV function and collagen contentin TGR(hKLK1)-STZ animals. Transgenic expressionof hKLK1 counteracts the progression of LV contractiledysfunction and extracellular matrix remodeling inSTZ-induced diabetic cardiomyopathy via a BK B2receptor-dependent pathway.OTschope, C., Walther,T., Koniger, J., Spillmann, F., Westermann, D., Escher,F., Pauschinger, M., Pesquero, J. B., Bader, M., Schult-heiss, H.-P., Noutsias, M. Prevention of cardiac fibrosisand left ventricular dysfunction in diabetic cardiomy-opathy in rats by transgenic expression of the humantissue kallikrein gene. FASEB J. 18, 828–835 (2004)
Key Words: diabetes mellitus � diabetic cardiomyopathy � kal-likrein � pathogenesis � therapy � transgenic animal
Diabetes is an independent risk factor for left ventric-ular (LV) dysfunction (1). Primary myocardial injuryhas been shown even in the absence of hypertensionand atherosclerosis in diabetic patients and so has beencalled ”diabetic cardiomyopathy” (2). The histopatho-logical changes found include diffuse myocardial de-generation with changes in the myocardial extracellu-lar matrix. The composition of the extracellular matrix,a complex network of structural proteins includingcollagen types I and III, provides architectural supportfor the muscle cells and plays an important role inmyocardial function (3, 4). Several studies of diabeticcardiomyopathy have demonstrated an accumulationof myocardial collagen including types I, III, and VI,leading to interstitial and perivascular fibrosis whichhas been correlated with LV early diastolic and systolicdysfunction (5–8). The mechanisms involved in thesechanges are still not completely understood. Behindmyocardial microischemia due to focal changes inmicrovessels, nonenzymatic glycosylation of collagens,down-regulation, or reduced activity of collagen de-grading matrix metalloproteinases (MMP), increasedtransforming growth factor-� (TGF-�) activity or up-regulation in collagen mRNA expression are discussedas hallmarks for myocardial fibrosis in diabetic cardio-myopathy (5, 7–9). Remodeling of the extracellularmatrix is also regulated by profibrotic acting peptides(e.g., angiotensin II, aldosterone, endothelin) and an-tagonistically acting systems like the kallikrein-kininsystem (KKS) (10, 11).
Kinins are important peptides mediating a diverserange of physiological and pathological functions ofthe cardiovascular system (12). The effector peptides of
1 Correspondence: Charite-University Medicine, CampusBenjamin Franklin, Department of Cardiology and Pneumo-nology, Free University of Berlin, Hindenburgdamm 30,D-12220 Berlin, Germany. E-mail: [email protected]
doi: 10.1096/fj.03-0736com
828 0892-6638/04/0018-0828 © FASEB

the KKS like bradykinin (BK) are produced after enzy-matic cleavage of kininogens by kallikrein (KLK). Sev-eral in vivo studies elucidated that the KKS is involvedin extracellular matrix regulation (13, 14). KLK itselfcan serve as a collagenase and may activate MMPs,promoting collagen breakdown (15, 16). Locally ex-pressed kinins can inhibit collagen synthesis in vivo bystimulating nitric oxide (NO) and the prostaglandinsystem via the BK B2 receptor (17). Thus, the KKScould be an ideal mediator for counteracting themechanisms contributing to cardiac fibrosis in diabeticcardiomyopathy.
To further examine the antifibrotic effect of cardiacKKS during the development of diabetic cardiomyopa-thy, we investigated cardiac collagen accumulation andLV function in transgenic rats (TGR) expressing thehuman kallikrein 1 (hKLK1) gene (14) under strepto-zotocin (STZ) -induced diabetic conditions.
MATERIALS AND METHODS
Animals and study design
Male Sprague Dawley (SD) rats and TGR(hKLK1) weighing300–330 g were maintained on a 12 h light/dark cycle andfed standard chow ad libitum (n�10/group). TGR(hKLK1)were generated as described in detail elsewhere (14). A 5.6 kbDNA fragment containing the entire (hKLK1) gene underthe control of the heavy metal-responsive mouse metallothio-nein promoter was microinjected into SD rat oocytes. Theresultant founders were bred to homozygosity. These trans-genic rats are characterized by expression of the transgene inall organs, with a rank order of expression heart�kidney�brain�lung (14).
Diabetes mellitus was induced by a single injection of STZ(70 mg/kg; i.p.) prepared in 0.1 M sodium citrate buffer, pH4.5 (Sigma, Munich, Germany) as described in detail else-where (18). Hyperglycemia was confirmed 48 h later by areflectance meter (Acutrend, Hoffmann-La Roche, Grenzach-Wyhlen, Germany). Vehicle-treated SD and TGR(hKLK1)served as controls (n�10). To investigate whether a KLK-and/or BK B2 receptor-dependent pathway is responsible fordifferences observed in TGR(hKLK1)-STZ, we treated in aseparate experiment TGR(hKLK1)-STZ with the KLK inhibi-tor aprotinin (19) (Trasylol 500,000 KIE by Bayer, Le-verkusen, Germany; n�9) or with the BK B2 receptor antag-onist icatibant (HOE140) (500 �L/kg 24 h by Aventis,Frankfurt, Germany; n�6). Both drugs were administered 5days after STZ injection for 6 wk.
Hemodynamic characterization
Six weeks after injecting STZ or vehicle, heart rate (HR, inbpm), LV peak systolic pressure (LVP, in mmHg), the maxi-mal rate of LV pressure rise (dP/dtmax., in mmHg/s) as ameasure of LV systolic contraction, the minimal rate of LVpressure fall (dP/dtmin, in mmHg/s) as a measure of LVsystolic relaxation and the LV end-diastolic pressure (LVEDP,in mmHg) were recorded via a Millar-tip catheter (2F) systemin anesthetized (ketamine [50 mg/kg; i.p.], 2% xylasine [5mg/kg; i.p.], ventilated, open-chest animals as described indetail elsewhere (20). After the experiment, the hearts wereexcised and �0.2 cm-thick transverse sections of the heartswere rapidly frozen in liquid nitrogen and stored at –80°C for
immunohistochemistry. Another section was paraffin embed-ded for Sirius Red staining.
Sirius Red staining, immunohistology, and quantification ofcollagen
Total collagen content of the Sirius Red (Polyscience, Inc.,Warrington, PA, USA) stained sections was measured undercircularly polarized light according to published methods (3).Representative aspects of Sirius Red stainings are illustratedin Fig. 1. Serial 5 �m-thick transverse cryosections of TissueTec� embedded SD, SD-STZ, TGR(hKLK1), TGR(hKLK1)-STZ, TGR(hKLK1)-STZ-aprotinin and TGR(hKLK1)-STZ-icatibant (HOE 140) hearts were placed on poly-L-lysineprecoated slides and fixed in cold acetone for 10 min.Immunohistochemistry with rabbit anti-collagen subtypes I,III, and VI specific antibodies (optimal working dilution:1:500; kindly donated by Dr. Schuppan; ref 21) and peroxi-dase-conjugated IgG (heavy and light chains) polyclonal
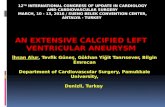
Figure 1. Sirius Red staining (original magnification �100).a) Baseline total collagen expression by Sirius Red staining ina nondiabetic SD rat heart. b) Collagen abundance in adiabetic SD-STZ rat heart. c) Baseline total collagen contentin a normoglycemic TGR(hKLK1) rat heart, comparable toSD rat hearts (compare panel a). d) Baseline total collagencontent in a diabetic TGR(hKLK1)-STZ rat heart, comparableto SD and TGR(hKLK1) rat hearts baseline expression levels(compare panels a and c). e) Total collagen expression bySirius Red staining in an aprotinin-treated TGR(hKLK1)-STZrat heart. f) Total collagen expression by Sirius Red stainingin an icatibant-treated TGR(hKLK1)-STZ rat heart.
829KALLIKREIN IN DIABETIC CARDIOMYOPATHY

anti-rabbit secondary antibody (working dilution: 1:500) wasquantified by digital image analysis as described in detailelsewhere (22). All available fields (�30 fields) were mea-sured, including the septum, right and left ventricles. Repre-sentative immunohistochemical stainings of collagen type IIIare demonstrated in Fig. 2. Immunohistochemistry on colla-gen types I and VI provided comparable results.
Statistical analysis
Statistical analysis was performed using JMP Statistical Discov-ery Software™ Version 4.05 (SAS Institute, Cary, NC, USA).Since normal distribution was excluded regarding all param-eters in conducting the Shapiro-Wilk W test (P�0.05), exclu-sively nonparametric tests were performed. Quantitative andqualitative data were compared conducting the Wilcoxon-Kruskal-Wallis test on rank sums. The honestly significantdifference for multiple comparisons of all pairs was calculatedby the Tukey-Kramer posthoc analysis. Multivariate (multiplebivariate) analysis was conducted for the Spearman Rhocorrelation coefficient. P � 0.05 was considered statisticallysignificant.
RESULTS
Functional characteristics
Throughout the 6 wk study period, SD-STZ andTGR(hKLK1)-STZ displayed severe hyperglycemia anda loss in body weight. No differences within the diabeticgroups were observed. Aprotinin and icatibant treat-ment had no influence on these parameters (Table 1).
LV function did not differ between SD andTGR(hKLK1) controls. SD-STZ showed significant im-pairment in LVP, LVEDP, dP/dtmax. and dP/dtmin.. Incontrast, LV function in TGR(hKLK1)-STZ was signifi-
cantly improved compared with SD-STZ rats andshowed no significant difference with the normoglyce-mic controls by Tukey-Kramer post hoc analysis. Ad-ministration of TGR(hKLK1)-STZ with the kallikreininhibitor aprotinin led to a significant deterioration ofLV function compared with untreated TGR(hKLK1)-STZ and there was a statistically nonsignificant trendtoward improved LV function compared with SD-STZrats (Table 1). Except for an increase in LVEDP,icatibant treatment did not lead to significant changesin the remaining hemodynamic parameters vs. un-treated TGR(hKLK1)-STZ.
Histochemical quantification of collagen content
Quantification of collagen content by digital imageanalysis revealed significantly increased total collagencontent (Sirius Red staining; Fig. 1 and Table 1) andimmunohistochemically detected collagen types I,III, and VI (Fig. 2, Figs. 3, 4 and Table 2) in theSD-STZ group compared with nondiabetic SD andTGR(hKLK1) and diabetic TGR(hKLK1)-STZ litter-mates, with the TGR(hKLK1) not being statisticallydifferent from the SD rats. Aprotinin- and icatibant-treated TGR(hKLK1)-STZ hearts demonstrated signifi-cantly raised total collagen content compared withuntreated TGR(hKLK1)-STZ hearts, but still signifi-cantly lower than the SD-STZ rat group (Fig. 1 andTable 1).
Multivariate analysis of LV function parameters andcollagen expression
Multivariate analysis of collagen expression and LVfunction parameters revealed that total collagen con-
Figure 2. Immunohistochemistry ofcollagen type I (original magnifica-tion �100). a) Baseline collagentype I expression in a nondiabeticSD rat heart. b) Collagen type Iabundance in an SD-STZ rat heart.c) Baseline collagen type I expressionin a normoglycemic TGR(hKLK1) ratheart, comparable to SD rathearts (compare panel a). d) Base-line collagen type I expression ina diabetic TGR(hKLK1)-STZ ratheart, comparable to SD andTGR(hKLK1) rat hearts baselineexpression levels (compare panelsa and c).
830 Vol. 18 May 2004 TSCHOPE ET AL.The FASEB Journal

tent (Sirius Red staining) and collagen types I, III, andVI expression were significantly (P�0.01) interrelatedwith parameters of LV function (Table 3).
DISCUSSION
The important finding of this study is the cardioprotec-tive effect of transgenic hKLK1 gene transfer in exper-imental STZ-induced diabetic cardiomyopathy in termsof a preservation of several LV function parameters,which was significantly related to an inhibition ofcollagen content accumulation in this model. Thetransgenic expression did not exert an antidiabeticeffect per se, since TGR(hKLK1)-STZ rats had equallyhigh blood glucose levels and body weight loss com-pared with SD-STZ rats. The findings on total collagencontent (Sirius Red staining) and expression of thecollagen subtypes I, III, and VI suggest a beneficialeffect on remodeling in experimental diabetic cardio-myopathy that is further substantiated by the significantcorrelations between all investigated LV function pa-rameters and collagen expression quantification re-sults. Treatment with the KLK inhibitor aprotininblunted these beneficial effects on LV function param-eters and total collagen content, indicating a KLK-specific effect in this rat model. Antagonism by icati-bant confirmed that these beneficial matrix regulationeffects are mediated via the B2 receptor. However,icatibant treatment indicates that B2 receptor-indepen-dent mechanisms are also involved, since the beneficialeffects of the transgenic hKLK1 gene transfer on he-modynamic parameters were blunted only with respectto LVEDP, not dP/dtmin or dP/dtmax.
Collagen types I, III, IV, and VI, in addition to type Vcollagen and elastin, constitute the main componentsof the extracellular cardiac matrix. Changes in theextracellular matrix, especially in the collagen compo-sition, decisively influence the passive mechanical prop-erties of the myocardium and thus are important forcardiac hemodynamics (4).
Massive interstitial and perivascular fibrosis with focalcollagen accumulation and fibrillar fragmentation hasbeen reported in diabetic patients (9). Apart fromreplacement fibrosis, hearts from diabetic patients dis-play reactive fibrosis including thickening of the basalvascular and cellular membrane. The etiology of thiscollagen accumulation is multifactorial. Increased glu-cose levels stimulate fibroblasts. Findings on increasedTGF-� levels in diabetic hearts indicate that cytokinesare also involved in the collagen accumulation underdiabetic conditions (8). Moreover, collagen digestionby collagenases is impaired due to the increased glyco-sylation level (7). Increased cardiac hydroxyprolinecontent, an index of total collagen, was described indiabetic patients and animals depending on the severityand duration of the disease (5). This finding wasconfirmed in STZ diabetic rats after 6 wk and isconsistent with the significantly increased Sirius Redstaining observed in the hearts of SD-STZ rats. SimilarT
AB
LE
1.B
asal
and
hem
odyn
amic
char
acte
rist
ics
SDSD
-ST
ZT
GR
(hK
LK
1)T
GR
(hK
LK
1)-S
TZ
TG
R(h
KL
K1)
-ST
Zap
roti
nin
TG
R(h
KL
K1)
-ST
Zic
atib
ant
Blo
odgl
ucos
e(m
g/dL
)83
(80–
98)
580
(533
–595
)*87
(80–
105)
610
(538
–628
)*59
5(5
73–6
20)*
584
(552
–611
)*B
ody
wei
ght
(g)
318
(308
–346
)21
0(1
86–2
48)*
337
(316
–355
)21
6(1
95–2
64)*
274
(267
–281
)*24
0(2
05–2
62)*
Hea
rtra
te(b
pm)
255
(240
–258
)24
0(2
38–2
51)
265
(237
–279
)23
2(2
22–2
43)
250
(235
–260
)24
8(2
28–2
73)
LV
pres
sure
(mm
Hg)
78.5
(72.
4–83
.4)
56.5
(45.
0–61
.8)*
81.5
(78.
3–87
.1)
73.0
(69.
9–79
.8)
68.0
(61.
0–71
.0)#
71(6
8.2–
78.1
)dP
/dt m
ax(m
mH
g/s)
4578
(413
9–58
00)
2876
(199
9–31
38)*
5116
(486
8–55
88)
4281
(395
0–50
01)
3600
(336
5–37
50)#
4000
(380
0–49
62)
dP/d
t min
(mm
Hg/
s)�
2,35
8(�
2778
–�22
79)
�18
13(�
1963
–�13
88)*
�30
55(�
3195
–�26
54)
�26
04(�
2727
–�23
44)
�21
00(�
2350
–�18
50)#
�24
21(�
2623
–�22
22)
LV
ED
P(m
mH
g)2.
8(1
.9–3
.6)
4.7
(4.3
–6.9
)*2.
6(2
.3–4
.1)
3.3
(2.6
–4.8
)5.
3(5
.0–7
.7)*
4.4
(4.1
–5.9
)*T
otal
colla
gen
con
ten
t(S
iriu
sR
edst
ain
ing)
0.01
4(0
.013
–0.0
17)
0.03
7(0
.034
–0.0
48)*
0.01
5(0
.013
–0.0
17)
0.01
8(0
.013
–0.0
20)
0.02
4(0
.019
–0.0
32)†
0.02
2(0
.021
–0.0
66)†
Val
ues
depi
ctm
edia
ns
and
inte
rqua
rtile
ran
ges
(25%
–75%
thpe
rcen
tile
inpa
ren
thes
es).
*H
ones
tly
sign
ifica
ntl
ydi
ffer
ent
leve
lsas
calc
ulat
edby
post
hoc
Tuk
ey-K
ram
eran
alys
is.
#Si
gnifi
can
tly
diff
eren
tva
lues
ofth
eT
GR
(hK
LK
1)-S
TZ
apro
tin
in-tr
eate
dra
tsvs
.th
eSD
and
TG
R(h
KL
K1)
grou
ps,n
otbe
ing
sign
ifica
ntl
ydi
ffer
ent
from
the
SD-S
TZ
grou
p.†
Val
ues
sign
ifica
ntl
ydi
ffer
ent
com
pare
dw
ith
the
SD-S
TZ
onon
eh
and
and
SDan
dT
GR
(hK
LK
1)gr
oups
onth
eot
her
.
831KALLIKREIN IN DIABETIC CARDIOMYOPATHY

to findings in hearts of diabetic patients, we found anincrease in cardiac types I, III, and VI collagen in theextracellular matrix of SD-STZ rats (7, 9). While anincrease of type I and III collagen probably contributesto changed cardiac hemodynamics in SD-STZ animalsdue to increased stiffness and loss of elasticity, theobserved additional perivascular increase of type IIIand VI collagen may impede the exchange of cellularsubstrate. This might further intensify oxidative stressand endothelial dysfunction.
Although both SD-STZ and TGR(hKLK1)-STZ dia-betic strains developed comparable values of hypergly-cemia and weight loss, STZ diabetic rats with transgenicexpression of the hKLK1 gene showed preserved LVfunction and significantly lower levels of the threeinvestigated collagen types than wild-type SD-STZ ani-mals. Collagen content of TGR(hKLK1)-STZ did notdiffer significantly from normoglycemic TGR(hKLK1)and SD rats. Hemodynamically, the latter correspondsespecially with the improvement in LVEDP. Chronic
Figure 3. Immunohistochemistry ofcollagen type III (original magnifi-cation �100). a) Baseline collagentype III expression in a nondiabeticSD rat heart. b) Collagen type IIIabundance in an SD-STZ ratheart. c) Baseline collagen type IIIexpression in a normoglycemicTGR(hKLK1) rat heart, compara-ble to SD rat hearts (compare panela). d) Baseline collagen type III expres-sion in a diabetic TGR(hKLK1)-STZ rat heart, comparable to SD andTGR(hKLK1) rat hearts baseline ex-pression levels (compare panels aand c).
Figure 4. Immunohistochemistry ofcollagen type VI (original magnifi-cation �100). a) Baseline collagentype VI expression in a nondiabeticSD rat heart. b) Collagen type VIabundance in an SD-STZ ratheart. c) Baseline collagen type VIexpression in a normoglycemicTGR(hKLK1) rat heart, comparableto SD rat hearts (compare panel a).d) Baseline collagen type VI expres-sion in a diabetic TGR(hKLK1)-STZ rat heart, comparable to SD andTGR(hKLK1) rat hearts baseline ex-pression levels (compare panels aand c).
832 Vol. 18 May 2004 TSCHOPE ET AL.The FASEB Journal

treatment with the KLK inhibitor aprotinin bluntedthese effects in TGR(hKLK1)-STZ, but not in SD-STZrats (data not shown), confirming the KLK dependencyof our findings. However, apart from KLK-inhibition,aprotinin exerts a variety of KLK-independent effects.We therefore investigated the BK B2 receptor-specificinhibitor icatibant, which significantly blunted the ef-fects on collagen content in TGR(hKLK1)-STZ. As tothe LV function parameters, only LVEDP, the hemody-namic parameter for passive LV stiffness, was impairedin diabetic TGR(hKLK1) after B2 receptor-specificinhibition. This agrees with data by Cheng et al. (23)showing that icatibant treatment led to an increase inLVEDP without influencing dP/dtmax and dP/dtmin ina dog heart failure model. Thus, the BK B2 receptorcontributes to the cardioprotective effects ofTGR(hKLK1) under STZ diabetic conditions. Since werecently found an up-regulation in cardiac BK B2 andBK-B1 receptor mRNA expression in SD-STZ diabeticrats (24), it is possible that the different effects betweenaprotinin and icatibant on LVP, dP/dtmax, and
dP/dtmin in diabetic TGR(hKLK1) depends on themore comprehensive degree of KKS inhibition afteraprotinin treatment in our model.
The present evidence for kinins as antifibrotic agentsis to some extent contradictory. In the absence of NOproviding endothelial cells, kinins may act as growthfactors on cultured cardiomyocytes and smooth musclecells via the extracellular signal-regulated/mitogen-ac-tivated (ERK/MAP) kinase cascade (25). However,Cellier et al. reported the opposite effect after B2receptor stimulation in isolated glomeruli under highglucose conditions (26). BK reduces type I and IIIcollagen and fibronectin mRNA expression in culturedfibroblasts, probably by a NO/prostaglandin-depen-dent pathway (13, 17). The latter agrees with datashowing that the antifibrotic effects of angiotensin-converting enzyme inhibition are reduced after cotreat-ment with icatibant in a model of LV hypertrophy (27)as well as in a model of myocardial infarction using B2receptor knockout mice (28). Accordingly, we showedrecently that cardiac fibrosis is less severe in
TABLE 3. Multivariate analysis of hemodynamic data and collagen expressiona
Variable by Variable Spearman Rho Prob � �Rho� �.8 �.6 �.4 �.2 0 .2 .4 .6 .8
Col I-AF Sirius-Red-AF 0.5315 0.0004Col III-AF Sirius-Red-AF 0.5320 0.0004Col III-AF Koll I-AF 0.8493 �0.0001Col VI-AF Sirius-Red-AF 0.4891 0.0014Col VI-AF Koll I-AF 0.7685 �0.0001Col VI-AF Koll III-AF 0.8385 �0.0001LVP Sirius-Red-AF �0.7013 �0.0001LVP Koll I-AF �0.4818 0.0016LVP Koll III-AF �0.5467 0.0003LVP Koll VI-AF �0.5991 �0.0001LV dP/dt max Sirius-Red-AF �0.7366 �0.0001LV dP/dt max Koll I-AF �0.4659 0.0024LV dP/dt max Koll III-AF �0.4962 0.0011LV dP/dt max Koll VI-AF �0.4946 0.0012LV dP/dt max LVP 0.8967 �0.0001LV dP/dt min Sirius-Red-AF 0.6469 �0.0001LV dP/dt min Koll I-AF 0.4863 0.0015LV dP/dt min Koll III-AF 0.4983 0.0011LV dP/dt min Koll VI-AF 0.4790 0.0018LV dP/dt min LVP �0.8074 �0.0001LV dP/dt min LV dP/dt max �0.8084 �0.0001
a Spearman Rho correlation coefficients (third column) are illustrated by horizontal bars; corresponding P values are listed in the fourthcolumn.
TABLE 2. Immunohistological quantification of cardiac collagen expression
SD SD-STZ TGR(hKLK1) TGR(hKLK1)-STZ
Collagen I-AF 0.025 0.142* 0.071 0.020(0.007–0.057) (0.095–0.161) (0.009–0.023) (0.006–0.022)
Collagen III-AF 0.018 0.061* 0.019 0.014(0.002–0.041) (0.051–0.082) (0.016–0.026) (0.009–0.020)
Collagen VI-AF 0.013 0.116* 0.037 0.015(0.006–0.054) (0.089–0.162) (0.024–0.039) (0.007–0.055)
Values depict the medians and interquartile ranges (25%–75%th percentile in parentheses). AF refers to the area fraction. * Honestlysignificantly different levels as calculated by post hoc Tukey-Kramer analysis.
833KALLIKREIN IN DIABETIC CARDIOMYOPATHY

TGR(hKLK1) after isoproterenol-induced stress; simi-lar to the present results in diabetic cardiomyopathy,this effect was B2 receptor dependent (14). By pharma-cological B2 receptor blockade, genetic ablation of theB2 receptor, and transgenic expression of the KLKgene, Schanstra et al. recently demonstrated a B2receptor antifibrotic effect in the unilateral ureteralobstruction animal model (29). Thus, several in vivoexperiments, including our investigations, clearly showthe importance of kinins in reducing extracellularmatrix accumulation under pathophysiological condi-tions. IKLK itself increases collagen breakdown by itsown collagenase activity and by increasing MMP activity(15, 16, 30). Since we and others have shown thatcardiac KLK activity is reduced under severe STZdiabetic conditions (18, 31), it is reasonable to suggestthat direct KLK-dependent effects might have contrib-uted to the prohibiting effect on collagen accumulationin TGR(hKLK1)-STZ.
The antifibrotic effects of kinins have been eluci-dated by prostaglandin- and NO-dependent pathways(17, 32). Several studies have shown that transientexpression of hKLK in rats by somatic gene transfer canattenuate hypertension, cardiac remodeling, renal in-jury and induce angiogenesis in a hindlimb ischemicmodel and normoperfused skeletal muscle (33–36); thebeneficial effect on hypertension was blunted by theKLK inhibitor aprotinin (33). More important, localKLK gene transfer protects from diabetes-induced mi-croangiopathy by attenuating apoptosis of endothelialcells and promoting collateralization, thus ensuringimproved hemodynamic recovery in case of superven-ing vascular occlusion (37). In this setting, insulinsupplementation did not exert an additive effect inpreventing diabetic microangiopathy. Kinins can in-crease coronary perfusion (38) and stimulate myocar-dial glucose uptake (39–41). It is therefore conceivablethat apart from the primary reduction of collagenabundance, additional kinin-dependent cardioprotec-tive effects might have contributed to the preserved LVfunction under STZ-induced diabetic conditions. How-ever, direct antifibrotic effects of the KKS and the abovementioned additional effects of KLK are not mutuallyexclusive, since the latter might ultimately exert sec-ondary antifibrotic effects via inhibition of cell deathmechanisms and improved supply of nutrients andoxygen.
This study was supported by the Deutsche Forschungsge-meinschaft (DFG; TS-64/2-2).
REFERENCES
1. Kannel, W. B., Hjortland, M., and Castelli, W. P. (1974) Role ofdiabetes in congestive heart failure: the Framingham study.Am. J. Cardiol. 34, 29–34
2. Zarich, S. W., and Nesto, R. W. (1989) Diabetic cardiomyopathy.Am. Heart J. 118, 1000–1012
3. Pauschinger, M., Knopf, D., Petschauer, S., Doerner, A., Poller,W., Schwimmbeck, P. L., Kuhl, U., and Schultheiss, H. P. (1999)
Dilated cardiomyopathy is associated with significant changes incollagen type I/III ratio. Circulation 99, 2750–2756
4. Spinale, F. G. (2002) Matrix metalloproteinases: regulation anddysregulation in the failing heart. Circ. Res. 90, 520–530
5. Modrak, J. (1980) Collagen metabolism in the myocardiumfrom streptozotocin-diabetic rats. Diabetes 29, 547–550
6. Shimizu, M., Umeda, K., Sugihara, N., Yoshio, H., Ino, H.,Takeda, R., Okada, Y., and Nakanishi, I. (1993) Collagenremodelling in myocardia of patients with diabetes. J. Clin.Pathol. 46, 32–36
7. Spiro, M. J., and Crowley, T. J. (1993) Increased rat myocardialtype VI collagen in diabetes mellitus and hypertension. Diabeto-logia 36, 93–98
8. Mizushige, K., Yao, L., Noma, T., Kiyomoto, H., Yu, Y., Hosomi,N., Ohmori, K., and Matsuo, H. (2000) Alteration in leftventricular diastolic filling and accumulation of myocardialcollagen at insulin-resistant prediabetic stage of a type II dia-betic rat model. Circulation 101, 899–907
9. Shimizu, M., and Isogai, Y. (1993) Nippon Rinsho 51, 1362–1366(Heart failure due to metabolic heart disorders)
10. Weber, K. T., Sun, Y., Katwa, L. C., and Cleutjens, J. P. (1995)Connective tissue: a metabolic entity? J. Mol. Cell. Cardiol. 27,107–120
11. Dostal, D. E. (2001) Regulation of cardiac collagen: angiotensinand cross-talk with local growth factors. Hypertension 37, 841–844
12. Tschope, C., Schultheiss, H. P., and Walther, T. (2002) MultipleInteractions Between the Renin-Angiotensin and the Kallikrein-Kinin Systems: Role of ACE Inhibition and AT1 ReceptorBlockade. J. Cardiovasc. Pharmacol. 39, 478–487
13. Kim, N. N., Villegas, S., Summerour, S. R., and Villarreal, F. J.(1999) Regulation of cardiac fibroblast extracellular matrixproduction by bradykinin and nitric oxide. J. Mol. Cell. Cardiol.31, 457–466
14. Silva, J. A., Jr., Araujo, R. C., Baltatu, O., Oliveira, S. M.,Tschope, C., Fink, E., Hoffmann, S., Plehm, R., Chai, K. X.,Chao, L., et al. (2000) Reduced cardiac hypertrophy and alteredblood pressure control in transgenic rats with the human tissuekallikrein gene. FASEB J. 14, 1858–1860
15. Tschesche, H., Michaelis, J., Kohnert, U., Fedrowitz, J., andOberhoff, R. (1989) Tissue kallikrein effectively activates latentmatrix degrading metalloenzymes. Adv. Exp. Med. Biol. 247A,545–548
16. Clements, J., Hooper, J., Dong, Y., and Harvey, T. (2001) Theexpanded human kallikrein (KLK) gene family: genomic or-ganisation, tissue-specific expression and potential functions.Biol. Chem. 382, 5–14
17. Gallagher, A. M., Yu, H., and Printz, M. P. (1998) Bradykinin-induced reductions in collagen gene expression involve prosta-cyclin. Hypertension 32, 84–88
18. Tschope, C., Walther, T., Yu, M., Reinecke, A., Koch, M.,Seligmann, C., Heringer, S. B., Pesquero, J. B., Bader, M.,Schultheiss, H., et al. (1999) Myocardial expression of ratbradykinin receptors and two tissue kallikrein genes in experi-mental diabetes. Immunopharmacology 44, 35–42
19. Wang, C., Chao, L., and Chao, J. (1995) Direct gene delivery ofhuman tissue kallikrein reduces blood pressure in spontane-ously hypertensive rats. J. Clin. Invest. 95, 1710–1716
20. Tschope, C., Heringer-Walther, S., Koch, M., Spillmann, F.,Wendorf, M., Hauke, D., Bader, M., Schultheiss, H. P., andWalther, T. (2000) Myocardial bradykinin B2-receptor expres-sion at different time points after induction of myocardialinfarction. J. Hypertens. 18, 223–228
21. Somasundaram, R., and Schuppan, D. (1996) Type I, II, III, IV,V, and VI collagens serve as extracellular ligands for theisoforms of platelet-derived growth factor (AA, BB, and AB).J. Biol. Chem. 271, 26884–26891
22. Noutsias, M., Pauschinger, M., Ostermann, K., Escher, F.,Blohm, J. H., Schultheiss, H., and Kuhl, U. (2002) Digital imageanalysis system for the quantification of infiltrates and celladhesion molecules in inflammatory cardiomyopathy. Med. Sci.Monit. 8, 59–71
23. Cheng, C. P., Onishi, K., Ohte, N., Suzuki, M., and Little, W. C.(1998) Functional effects of endogenous bradykinin in conges-tive heart failure. J. Am. Coll. Cardiol. 31, 1679–1686
24. Spillmann, F., Altmann, C., Scheeler, M., Barbosa, M., Wester-mann, D., Schultheiss, H. P., Walther, T., and Tschope, C.
834 Vol. 18 May 2004 TSCHOPE ET AL.The FASEB Journal

(2002) Regulation of cardiac bradykinin B1- and B2-receptormRNA in experimental ischemic, diabetic, and pressure-over-load-induced cardiomyopathy. Int. Immunopharmacol. 2, 1823–1832
25. Douillet, C. D., Velarde, V., Christopher, J. T., Mayfield, R. K.,Trojanowska, M. E., and Jaffa, A. A. (2000) Mechanisms bywhich bradykinin promotes fibrosis in vascular smooth musclecells: role of TGF-beta and MAPK. Am. J. Physiol. Heart Circ.Physiol. 279, H2829–H2837
26. Cellier, E., Duchene, J., Pecher, C., Alric, C., Bascands, J. L.,Schanstra, J. P., and Girolami, J. P. (2002) B2 receptor activationreduces Erk1 and Erk2 phosphorylation induced by insulin-likegrowth factor-1, platelet-derived growth factor-BB, and highglucose in rat isolated glomeruli. Can. J. Physiol. Pharmacol. 80,341–345
27. Hu, K., Gaudron, P., Anders, H. J., Weidemann, F., Turschner,O., Nahrendorf, M., and Ertl, G. (1998) Chronic effects of earlystarted angiotensin converting enzyme inhibition and angioten-sin AT1-receptor subtype blockade in rats with myocardialinfarction: role of bradykinin. Cardiovasc. Res. 39, 401–412
28. Yang, X. P., Liu, Y. H., Mehta, D., Cavasin, M. A., Shesely, E., Xu,J., Liu, F., and Carretero, O. A. (2001) Diminished cardiopro-tective response to inhibition of angiotensin-converting enzymeand angiotensin II type 1 receptor in B(2) kinin receptor geneknockout mice. Circ. Res. 88, 1072–1079
29. Schanstra, J. P., Neau, E., Drogoz, P., Arevalo Gomez, M. A.,Lopez Novoa, J. M., Calise, D., Pecher, C., Bader, M., Giro-lami, J. P., and Bascands, J. L. (2002) In vivo bradykinin B2receptor activation reduces renal fibrosis. J. Clin. Invest. 110,371–379
30. Rittenhouse, H. G., Finlay, J. A., Mikolajczyk, S. D., and Partin,A. W. (1998) Human Kallikrein 2 (hK2) and prostate-specificantigen (PSA): two closely related, but distinct, kallikreins in theprostate. Crit. Rev. Clin. Lab. Sci. 35, 275–368
31. Sharma, J. N., and Kesavarao, U. (1996) Cardiac kallikrein inhypertensive and normotensive rats with and without diabetes.Immunopharmacology 33, 341–343
32. Weber, K. T., Sun, Y., Katwa, L. C., Cleutjens, J. P., and Zhou, G.
(1995) Connective tissue and repair in the heart. Potentialregulatory mechanisms. Ann. N.Y. Acad. Sci. 752, 286–299
33. Chao, J., Zhang, J. J., Lin, K. F., and Chao, L. (1998) Humankallikrein gene delivery attenuates hypertension, cardiac hyper-trophy, and renal injury in Dahl salt-sensitive rats. Hum. GeneTher. 9, 21–31
34. Wolf, W. C., Yoshida, H., Agata, J., Chao, L., and Chao, J. (2000)Human tissue kallikrein gene delivery attenuates hypertension,renal injury, and cardiac remodeling in chronic renal failure.Kidney Int. 58, 730–739
35. Emanueli, C., Minasi, A., Zacheo, A., Chao, J., Chao, L., Salis,M. B., Straino, S., Tozzi, M. G., Smith, R., Gaspa, L., et al. (2001)Local delivery of human tissue kallikrein gene acceleratesspontaneous angiogenesis in mouse model of hindlimb isch-emia. Circulation 103, 125–132
36. Emanueli, C., Zacheo, A., Minasi, A., Chao, J., Chao, L., Salis,M. B., Stacca, T., Straino, S., Capogrossi, M. C., and Madeddu,P. (2000) Adenovirus-mediated human tissue kallikrein genedelivery induces angiogenesis in normoperfused skeletal mus-cle. Arterioscler. Thromb. Vasc. Biol. 20, 2379–2385
37. Emanueli, C., Salis, M. B., Pinna, A., Stacca, T., Milia, A. F.,Spano, A., Chao, J., Chao, L., Sciola, L., and Madeddu, P. (2002)Prevention of diabetes-induced microangiopathy by humantissue kallikrein gene transfer. Circulation 106, 993–999
38. Groves, P., Kurz, S., Just, H., and Drexler, H. (1995) Role ofendogenous bradykinin in human coronary vasomotor control.Circulation 92, 3424–3430
39. Shanahan, M. F., and Edwards, B. M. (1989) Stimulation ofglucose transport in rat cardiac myocytes by guanosine 3,5-monophosphate. Endocrinology 125, 1074–1081
40. Mayfield, R. K., Shimojo, N., and Jaffa, A. A. (1996) Skeletalmuscle kallikrein. Potential role in metabolic regulation. Diabe-tes 45, S20–S23
41. Kudoh, A., and Matsuki, A. (2000) Effects of angiotensin-converting enzyme inhibitors on glucose uptake. Hypertension36, 239–244
Received for publication August 4, 2003.Accepted for publication November 21, 2003.
835KALLIKREIN IN DIABETIC CARDIOMYOPATHY