AN INTRACORPOREAL (ABDOMINAL) LEFT VENTRICULAR ...
13
AN INTRACORPOREAL (ABDOMINAL) LEFT VENTRICULAR ASSIST DEVICE, XXII: Precis and State of the Art John C. Norman, M.D. In 1974, between two and eight percent of the 50,000 adult patients undergoing cardiac surgery in this country succumbed in the early post- operative period from left ventricular failure, despite various methods of pharmacologic support and the increasing use of intra- and postoper- ative intra-aortic balloon pumping.2'8'16'17'31'42,44,49 Under NHLI auspices, our laboratories have concentrated on the de- velopment, modification, evaluation and validation of an intracorporeal left ventricular assist device,*t which has the potential of reducing these mortalities.3 ' '3'18'32'4' Its use may also broaden the criteria for operability in high risk patients. This left ventricular assist device is conservative- ly five to six times as effective as the intra-aortic balloon (Table 1) .1,11,12,19,23,24,25,26 Unlike the intra-aortic balloon, which is a volume dis- placement device that augments existing circulation and is dependent upon a regular ECG signal, this intracorporeal left ventricular assist de- vice is a definitive blood pump which can capture the entire cardiac output with the biologic heart in situ and can be actuated either synchronously or asynchronously.28'30'34'35'36'46 *The results of these efforts can be obtained from the Devices and Technology Branch Program Office, National Heart and Lung Institute, Landow Building, Room A-922, Bethesda, Maryland 20014. Of particular interest are contract proposals: 2374-200, April 1972; 2436-200, May 1973; 2494-200, September 1974; 2528-200, May 1975; 2481-200, August 1974; 2376-200, April 1972; 2441-200, August 1973; 2517-200, March 1975, and 2532-200, May 1975. Additional information can be obtained from reports: NO1-HL-73-2946, March 1975; NO1-HV-3-2946, April 1975; NO1- HV-3-2946, August 1975; NO1-HT-2910, August 1974; NOI-HV-3-2915, April 1974, and NO1-HV-3-2915. March 1975, and particularly Proposal 29208-1, May 1975. In all, more than 100 documents are available from the National Technical Information Service, US Dept. of Com- merce, Springfield, Virginia 22151. Other recent relevant summaries are available: 1) Norman JC and Huffman FN: Abdominal left ventricular assist device (ALVAD): preclinical evaluation of temporary assist pumping. Topical Report to NHLI, March 1974; 2) Hegyeli RJ, Machesko MR and Richardson LA: The left ventricular assist device: assistance of the failing circulation. DHEW Publication (NIH) 75-626, January 11, 1974; and 3) Ponn RB and Scott WC: An abdominal left ventricular assist device: experimental physiologic analyses. Honors Thesis, Har- vard Medical School, April 1974. tIn conjunction with the Thermo Electron Research and Development Center, Waltham, Massa- chusetts. Presented in part at the Second Henry Ford Hospital International Symposium on Cardiac Surgery, October 9, 1975. Proceedings to be edited by Julio C. Davila and published by Appleton-Century- Crofts, New York, New York. From the Cardiovascular Surgical Research Laboratories, Texaxs Heart Institute of St. Luke's Episcopal and Texas Children's Hospitals, Houston, Texas, 77025. Supported in part by USPHS Contract No. NO1-HLI3-2946, The John and Mary R. Markle Foundation, The Sid W. Richardson Foundation, The Kelsey-Leary Foundation, and the Mary A. Fraley Fund. Cardiovascular Diseases, Bulletin of the Texas Heart Institute, Vol. 2, Number 3, 1975 425
Transcript of AN INTRACORPOREAL (ABDOMINAL) LEFT VENTRICULAR ...
AN INTRACORPOREAL (ABDOMINAL)LEFT VENTRICULAR ASSIST DEVICE, XXII:
Precis and State of the Art
John C. Norman, M.D.
In 1974, between two and eight percent of the 50,000 adult patientsundergoing cardiac surgery in this country succumbed in the early post-operative period from left ventricular failure, despite various methodsof pharmacologic support and the increasing use of intra- and postoper-ative intra-aortic balloon pumping.2'8'16'17'31'42,44,49
Under NHLI auspices, our laboratories have concentrated on the de-velopment, modification, evaluation and validation of an intracorporealleft ventricular assist device,*t which has the potential of reducing thesemortalities.3' '3'18'32'4' Its use may also broaden the criteria for operabilityin high risk patients. This left ventricular assist device is conservative-ly five to six times as effective as the intra-aortic balloon (Table1) .1,11,12,19,23,24,25,26 Unlike the intra-aortic balloon, which is a volume dis-placement device that augments existing circulation and is dependentupon a regular ECG signal, this intracorporeal left ventricular assist de-vice is a definitive blood pump which can capture the entire cardiac outputwith the biologic heart in situ and can be actuated either synchronouslyor asynchronously.28'30'34'35'36'46
*The results of these efforts can be obtained from the Devices and Technology Branch ProgramOffice, National Heart and Lung Institute, Landow Building, Room A-922, Bethesda, Maryland20014. Of particular interest are contract proposals: 2374-200, April 1972; 2436-200, May 1973;2494-200, September 1974; 2528-200, May 1975; 2481-200, August 1974; 2376-200, April 1972;2441-200, August 1973; 2517-200, March 1975, and 2532-200, May 1975. Additional informationcan be obtained from reports: NO1-HL-73-2946, March 1975; NO1-HV-3-2946, April 1975; NO1-HV-3-2946, August 1975; NO1-HT-2910, August 1974; NOI-HV-3-2915, April 1974, andNO1-HV-3-2915. March 1975, and particularly Proposal 29208-1, May 1975. In all, more than100 documents are available from the National Technical Information Service, US Dept. of Com-merce, Springfield, Virginia 22151. Other recent relevant summaries are available: 1) NormanJC and Huffman FN: Abdominal left ventricular assist device (ALVAD): preclinical evaluationof temporary assist pumping. Topical Report to NHLI, March 1974; 2) Hegyeli RJ, MacheskoMR and Richardson LA: The left ventricular assist device: assistance of the failing circulation.DHEW Publication (NIH) 75-626, January 11, 1974; and 3) Ponn RB and Scott WC: Anabdominal left ventricular assist device: experimental physiologic analyses. Honors Thesis, Har-vard Medical School, April 1974.
tIn conjunction with the Thermo Electron Research and Development Center, Waltham, Massa-chusetts.
Presented in part at the Second Henry Ford Hospital International Symposium on Cardiac Surgery,October 9, 1975. Proceedings to be edited by Julio C. Davila and published by Appleton-Century-Crofts, New York, New York.
From the Cardiovascular Surgical Research Laboratories, Texaxs Heart Institute of St. Luke'sEpiscopal and Texas Children's Hospitals, Houston, Texas, 77025. Supported in part by USPHSContract No. NO1-HLI3-2946, The John and Mary R. Markle Foundation, The Sid W. RichardsonFoundation, The Kelsey-Leary Foundation, and the Mary A. Fraley Fund.
Cardiovascular Diseases, Bulletin of the Texas Heart Institute, Vol. 2, Number 3, 1975 425
DESIDERATA
The desiderata of such an implantable left ventricular assist device are:
1) It should reduce all indices of left ventricular work and oxygen con-sumption regardless of biologic cardiac output.23'24'30'46'48
2) It should maintain and/or increase systemic and pulmonary perfusion,regardless of biologic cardiac output.10 45
3) It should not result in undue trauma to the formed elements of thecirculating blood.15
4) It should have geometric and volumetric compatibility with a widerange of adult human somatotypes.18
5) It should not produce deleterious physiologic effects on parenchy-matous organs.48
6) Its implantation (and removal) techniques should be simple, rapid,and easily learned.
7) It should have easily variable pump capacities to assure accurate andcontrolled initiation, continuation and weaning of pumping.'14'2029
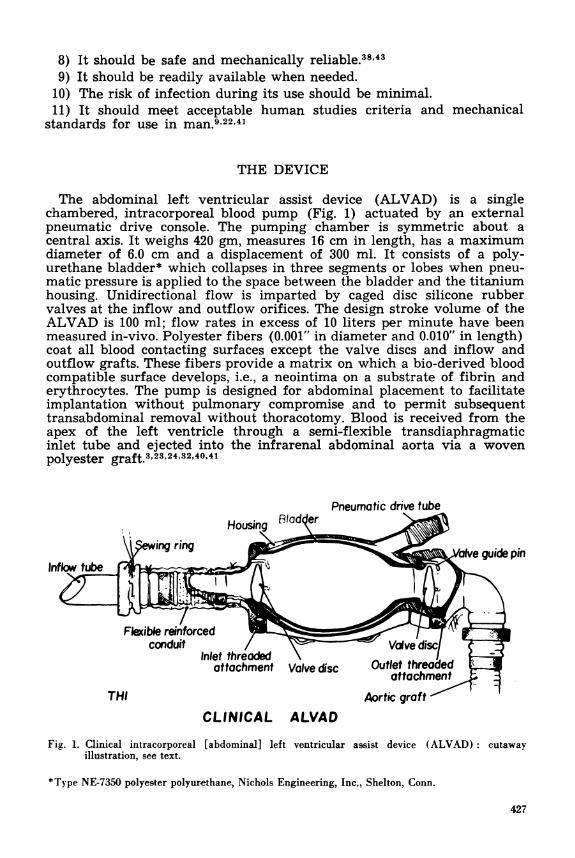
TABLE I
SUMMARY OF HEMODYNAMIC EFFECTIVENESSOF VARIOUS LEFT VENTRICULAR ASSIST DEVICES*
Roller Pump Roller PumD ALVADHemodynamic IABP (LA-Ao) (LV-Ao) (LV-Ao) EffectivenessVariable (MGH) (Penn) (Penn) (THI) ALVAD/IABP
LV peak sys-tolic pressure ;09 414 96 ;88 9.8
LV stroke work ;20 ;82 4100 484 4.2
LV dP/dt +01 428 ; 80 483 83.0
Coronary sinusflow 407 416 42 425 3.6
Myocardialoxygenconsumption i13 422 ± 47 t40 3.1
*Based on studies done at the Massachusetts General Hospital, Pennsyl-vania State University Hospital, and Texas Heart Institute. All valuesin the first four columns are percentages.
IABP= intra-aortic balloon pumping; LA = left atrium; Ao = aorta;LV = left ventricle; ALVAD = abdominal left ventricular assist device;dP/dt = rate of pressure rise.
426
8) It should be safe and mechanically reliable.38'439) It should be readily available when needed.
10) The risk of infection during its use should be minimal.11) It should meet acceptable human studies criteria and mechanical
standards for use in man.9'22'41
THE DEVICE
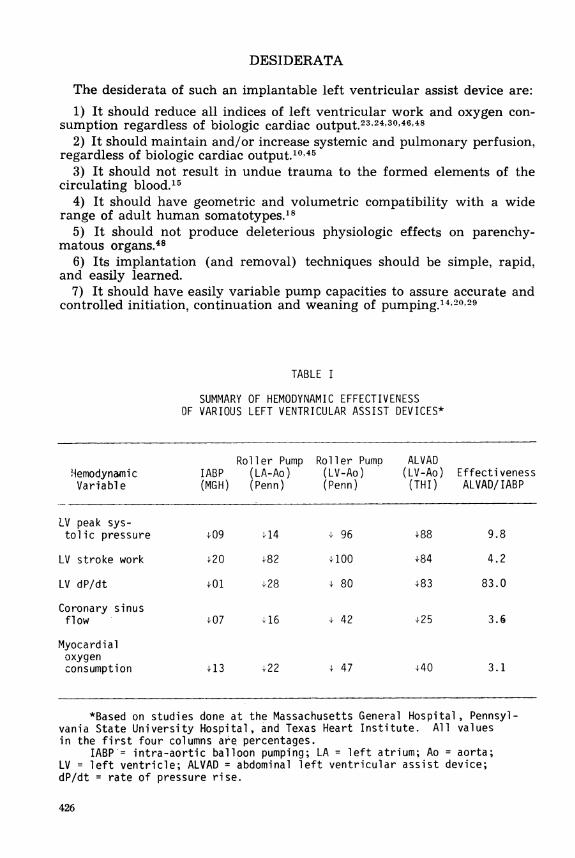
The abdominal left ventricular assist device (ALVAD) is a singlechambered, intracorporeal blood pump (Fig. 1) actuated by an externalpneumatic drive console. The pumping chamber is symmetric about acentral axis. It weighs 420 gm, measures 16 cm in length, has a maximumdiameter of 6.0 cm and a displacement of 300 ml. It consists of a poly-urethane bladder* which collapses in three segments or lobes when pneu-matic pressure is applied to the space between the bladder and the titaniumhousing. Unidirectional flow is imparted by caged disc silicone rubbervalves at the inflow and outflow orifices. The design stroke volume of theALVAD is 100 ml; flow rates in excess of 10 liters per minute have beenmeasured in-vivo. Polyester fibers (0.001" in diameter and 0.010" in length)coat all blood contacting surfaces except the valve discs and inflow andoutflow grafts. These fibers provide a matrix on which a bio-derived bloodcompatible surface develops, i.e., a neointima on a substrate of fibrin anderythrocytes. The pump is designed for abdominal placement to facilitateimplantation without pulmonary compromise and to permit subsequenttransabdominal removal without thoracotomy. Blood is received from theapex of the left ventricle through a semi-flexible transdiaphragmaticinlet tube and ejected into the infrarenal abdominal aorta via a wovenpolyester graft.3 23'24'32,40'41
Pneumatic drive tube
Qewingring p : v a l v e guide pin
Infoftb
Fleible reinforced de;
attachment Valve disc Outlet threabdattachment
THI Aortic graftCLINICAL ALVAD
Fig. 1. Clinical intracorporeal [abdominal] left ventricular assist device (ALVAD): cutawayillustration, see text.
*Type NE-7350 polyester polyurethane, Nichols Engineering, Inc., Shelton, Conn.
427
DRIVING AND MONITOR CONTROL CONSOLE
Reliability and safety have been prime considerations in the initialdesign and subsequent modifications of the control console. There are twomodes of operation: ECG-triggered synchronous counterpulsation andvariable fixed-rate asynchronous pumping. There are four fail-safe mech-anisms: (1) redundant drive systems-if the primary subsystem fails forany reason, a secondary pneumatic system is automatically actuated; (2)logic circuitry-should the ECG be interrupted or fail to discriminate,the control automatically assumes fixed-rate operation; (3) internalpneumatic source-in normal operation pneumatic pressure is suppliedby an external source (usually wall outlets from hospital compressors);however, if the system is interrupted, an internal carbon dioxide cylinderprovides pneumatic pressure; and (4) electrical systems-upon interrup-tion of AC line power, an integral rechargeable battery pack suppliespower (the integral battery and pneumatic supply may also be used duringtransfer of the pump recipient).The console incorporates monitoring and alarm systems to augment
the control system. A four-channel oscilloscope displays the ECG, thedrive signal, and two physiological signals. Interruption of any primarycontrol component is signaled by audio and visual alarms. Reliabilitystudies have been performed in conjunction with a four-month continu-ous life test. No failure occurred that would warrant discontinuance ofpumping.7"17'20'29'45
STROKE VOLUME LIMITER SYSTEM
A stroke volume limiter (SVL) has been developed to prevent overcollapse of the polyurethane bladder. Without the SVL, decreases in peri-pheral vascular resistance could result in trilobular bladder wall segmentsimpinging on one another, causing wear, reduction of bladder life, andpossibly particulate embolism of bladder pseudointima. The ALVAD hasa maximum stroke volume of 100 ml; the SVL limits stroke output toapproximately 85 ml. A linear voltage displacement transformer (LVDT)that can be used to monitor stroke volumes, minute flow, and derived func-tions has been developed. Its incorporation in the present ALVAD systemprovides on-line, digital readouts of pump performance.'7'48
ANTICOAGULATION
The anticoagulation regimen employed in our series of long-term bovineALVAD implantations is a modification of that proposed by Mansfieldand associates.33 Anticoagulation is initiated with 500 ml of low-molecular-weight dextran intravenously, repeated every twelve hours, and continuedthrough the third postoperative day. Beginning on the first postoperativeday the animal receives 600 mg of aspirin, 200 mg of dipridamole, andwarfarin orally on a daily basis. The warfarin dose is varied between 0and 10 mg to maintain prothrombin times at two to three times the valueestablished for the species (16 seconds). 37,48
428
MONITORING EQUIPMENT
During several series of experiments, simultaneous hemodynamic eventsand the sequential relationships of prosthetic and biological effects havebeen examined. On-line data are recorded by direct-writing and magnetictape recorders (Hewlett-Packard Model 7758A recorder with 8800 seriesamplifiers and Model 3955D tape recorder). Arterial and venous pressuresare monitored using fluid-filled catheters and differential transformertransducers (Hewlett-Packard Model 267BC pressure transducers). In-tracardiac pressures are measured by indwelling transducer-tip catheters(Konigsberg Model PlOD and Millar Model PC370 catheter-tip trans-ducers). Stroke volumes are determined with electromagnetic probes*and flowmeters (In Vivo Metric System Model NQ-2 flow probes and Bio-tronex BL-610 flowmeter). On-line digital information is available whichis processed by a dedicated computer (Hewlett-Packard Model 5690Bcatheterization computer system). The computer can also be utilized asa data retrieval system by entering off-line information such as bloodgases and chemistries.23.24'25'26
ACCOUNTABILITY
The development, in-vivo testing, and validation of this device for usein man have been closely monitored through the mechanisms of contrac-tural agreements with the National Heart and Lung Institute and serialperiodic external Ad Hoc reviews. The projected clinical trials have under-gone six federal reviews.** During these periods, approximately 200canine and bovine experiments were undertaken. In excess of 20,000 hoursof chronic in-vivo evaluation in calves were performed. Acute and chronichemodynamic effectiveness with maintenance or augmentation of thesystemic circulation during profound ventricular unloading without undueblood trauma were demonstrated. In-vivo reliability and durability fortwo times the periods of intended use (two weeks to one month) weredemonstrated. Absence of thrombotic and embolic phenomena during andafter in-vivo testing with anticoagulation were documented.* Compatibilitywith a wide range of human somatotypes was demonstrated in serialcadaver fitting studies.'8 Categorizations of the patient population at riskin our institutions and the needs for such a device were documented.22Weaning procedures and the possibility of pump dependence were de-fined. The legal, moral, ethical, and informed consent aspect (see AppendixI) were also addressed with serial internal and external reviews. Clinicalprotocols (anesthesia, surgical, cardiologic, hematologic, engineering, com-puterized data acquisition,21 and cost analyses47) have been formulated.
*Previous experience with rigid flow probes, which have been left in situ for extended periods,demonstrated erosion of the main pulmonary artery. The use of "soft" probes constructed ofsilicone rubber as opposed to rigid epoxy alleviated the erosion problem.
**April 13, 1972; May 22, 1973; October 28, 1973; October 28, 1973; October 17, 1974; May 15,1975, and August 21, 1975.
*NIH Guide for Grants and Contracts, US Dept HEW 3:11, Aug. 7, 1974
429
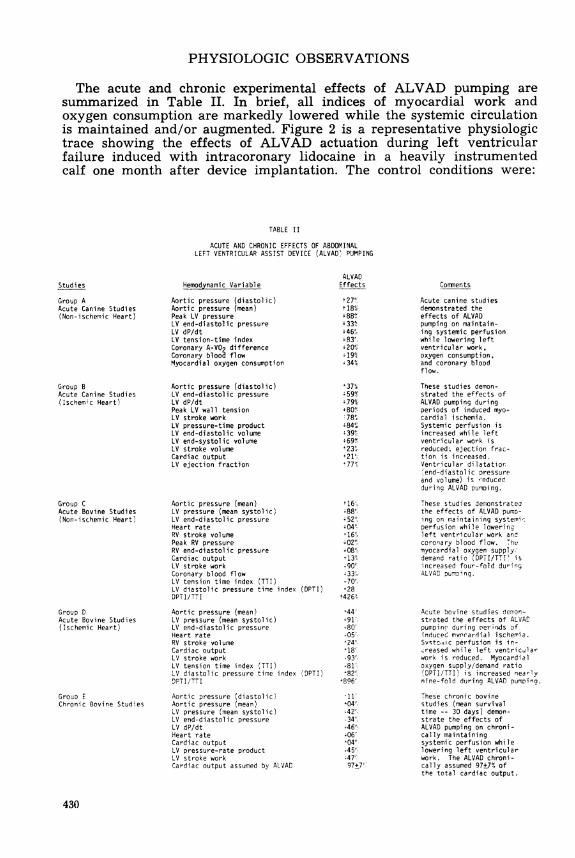
PHYSIOLOGIC OBSERVATIONS
The acute and chronic experimental effects of ALVAD pumping aresummarized in Table II. In brief, all indices of myocardial work andoxygen consumption are markedly lowered while the systemic circulationis maintained and/or augmented. Figure 2 is a representative physiologictrace showing the effects of ALVAD actuation during left ventricularfailure induced with intracoronary lidocaine in a heavily instrumentedcalf one month after device implantation. The control conditions were:
TABLE II
ACUTE AND CHRONIC EFFECTS OF ABDOMINALLEFT VENTRICULAR ASSIST DEVICE (ALVAD' PUMPING
Hemodynamic Variable
Aortic pressure (diastolic)Aortic pressure (mean)Peak LV pressureLV end-diastolic pressureLV dP/dtLV tension-time indexCoronary A-VOR differenceCoronary blood flowMyocardial oxygen consumption
Aortic pressure (diastolic)LV end-diastolic pressureLV dP/dtPeak LV wall tensionLV stroke workLV pressure-time productLV end-diastolic volumeLV end-systolic volumeLV stroke volumeCardiac outputLV ejection fraction
Aortic pressure (mean)LV pressure (mean systolic)LV end-diastolic pressureHeart rateRV stroke volumePeak RV pressureRV end-diastolic pressureCardiac outputLV stroke workCoronary blood flowLV tension time index (TTI)LV diastolic pressure time index (DPTI)DPTI/TTI
Aortic pressure (mean)LV pressure (mean systolic)LV end-diastolic pressureHeart rateRV stroke volumeCardiac outputLV stroke workLV tension time index (TTI)LV diastolic pressure time index (DPTI)9PTI/TTI
Aortic pressure (diastolic)Aortic pressure (mean)LV pressure (mean systolic)LV end-diastolic pressureLV dP/dtHeart rateCardiac outputLV pressure-rate productLV stroke workCardiac output assumed by ALVAD
ALVADEffects
t27>t 18"'u88'%4 33%; 46'-+83%,+20%19%34%
-37%;59%'79%,~8O~:78%'84"; 3911-
23%,21D77%
-88'-452'
402%+08%
-90S433,--70'-28
t426'°
,44'~
4-90'80's05 -
'24'18'.93'--81'82-896'
51104'.42-*.34--46'--06'04'.4 5%.47'97+7:
Comnnents
Acute canine studiesdemonstrated theeffects of ALVADpumping on maintain-ing systemic perfusionwhile lowering leftventricular work,oxygen consumption,and coronary bloodflow.
These studies demon-strated the effects ofALVAD pumping duringperiods of induced myo-cardial ischemia.Systemic perfusion isincreased while leftventricular work isreduced; ejection frac-tion is increased.Ventricular dilatationend-diastolic pressureand volume) is -educedduring ALVAD Dumping.
These studies demonstratedthe effects of ALVAD pump-ing on maintaining systemirperfusion while lowerin9left ventricular work andcoronary blood flow. Themyocardial oxygen supply.'demand ratio )DPTI/TT!' isincreased four-fold duringALVAD pumpDing.
Acute bovine studies demion-strated the effects of ALVADpumpino during oernirds ofinduced mvonardial ischerria.Svsotc,iic perfusion is in-.reased while left ventricularwork is reduced. Myocardialoxygen supply/demand ratio(DPTI/TTI) is increased nearlynine-fold during ALVAD pumping.
These chronic bovinestudies (mean survivaltime -- 30 days) demon-strate the effects ofALVAD pumping on chroni-cally maintainingsystemic perfusion whilelowering left ventricularwork. The ALVAD chroni-cally assumed 97±7%, ofthe total cardiac output.
430
Studies
Group AAcute Canine Studies(Non-ischemic Heart)
Group BAcute Canine Studies(Ischem;c Heart)
Group CAcute Bovine Studies(Non-ischemic Heart)
Group DAcute Bovine Studies(Ischemic Heart)
Grouo EChronic Bovine Studies
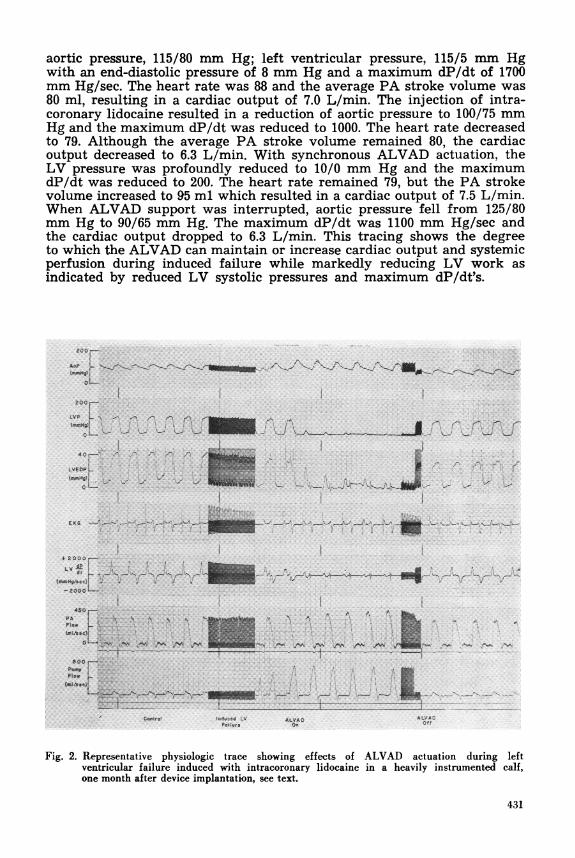
aortic pressure, 115/80 mm Hg; left ventricular pressure, 115/5 mm Hgwith an end-diastolic pressure of 8 mm Hg and a maximum dP/dt of 1700mm Hg/sec. The heart rate was 88 and the average PA stroke volume was80 ml, resulting in a cardiac output of 7.0 L/min. The injection of intra-coronary lidocaine resulted in a reduction of aortic pressure to 100/75 mmHg and the maximum dP/dt was reduced to 1000. The heart rate decreasedto 79. Although the average PA stroke volume remained 80, the cardiacoutput decreased to 6.3 L/min. With synchronous ALVAD actuation, theLV pressure was profoundly reduced to 10/0 mm Hg and the maximumdP/dt was reduced to 200. The heart rate remained 79, but the PA strokevolume increased to 95 ml which resulted in a cardiac output of 7.5 L/min.When ALVAD support was interrupted, aortic pressure fell from 125/80mm Hg to 90/65 mm Hg. The maximum dP/dt was 1100 mm Hg/sec andthe cardiac output dropped to 6.3 L/min. This tracing shows the degreeto which the ALVAD can maintain or increase cardiac output and systemicperfusion during induced failure while markedly reducing LV work asindicated by reduced LV systolic pressures and maximum dP/dt's.
04 -
LVEDP_-
EOG -EG-----
-2000
450
PA.
F'.LfEDP r we-o-v --
..............
2 ALVA0AtV A
.wWr. Of
Fig. 2. Representative physiologic trac-e showing effects of ALVAD actuation during leftventricular failure induced with intracoronary lidocaine in a heavily instrumented calf,one month after device implantation, see text.
431
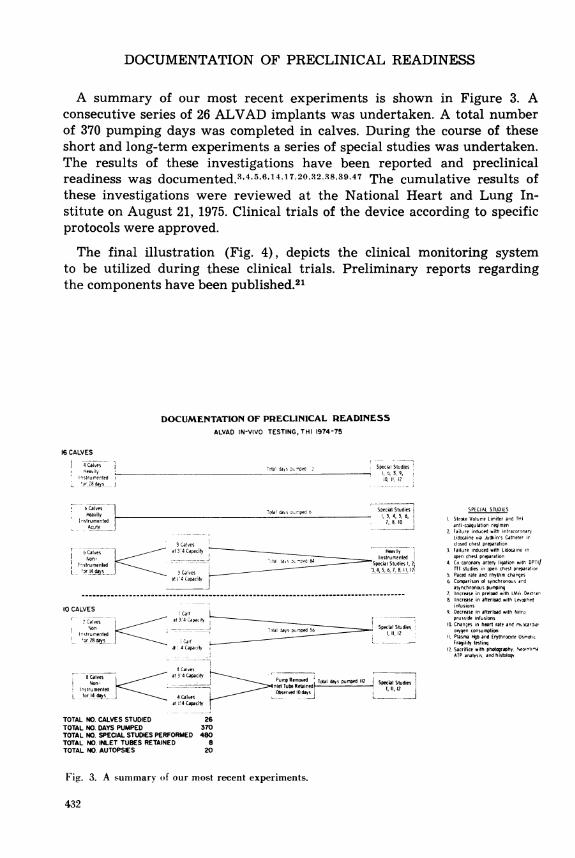
DOCUMENTATION OF PRECLINICAL READINESS
A summary of our most recent experiments is shown in Figure 3. Aconsecutive series of 26 ALVAD implants was undertaken. A total numberof 370 pumping days was completed in calves. During the course of theseshort and long-term experiments a series of special studies was undertaken.The results of these investigations have been reported and preclinicalreadiness was documented.3r4,5GrG14,l172032.38,39 47 The cumulative results ofthese investigations were reviewed at the National Heart and Lung In-stitute on August 21, 1975. Clinical trials of the device according to specificprotocols were approved.
The final illustration (Fig. 4), depicts the clinical monitoring systemto be utilized during these clinical trials. Preliminary reports regardingthe components have been published.21
DOCUMENTATION OF PRECLINICAL READINESSALVAD IN-VIVO TESTING, THI 1974-75
16 CALVES
4 Caves -HeavilysIysrumented
*gr_28 (joys _J
Total Tspumped Special Studies_ 1. S. 9.
10 II. 12J
6 CalvesHeavily
nstrumentedAcute
Special Studies- 3, 4, 5 6,
7, 8.10
3 Ca!vesr Calves 3 4 Capacity Heavily
nEsstrurnenteds Non- I Special Studies 2
l 7IE4 s_ 3 Calves 34, 5, 6 7. 8. I I?atJ14 Capacity
10 CALVES Calfales / at 3'4Capacil[-_
Calvs- -a pSpecial StudiesastrupepnteSE 11, 12
or _28calvs Calfal1 4 Capacity¢
4 Cacves8 Calves at 3 4 Capacity P drem d
E p c
PubeyRemcined~ =,,1nstru.Ik.e _Calmed Observedldayl
at 14 CapacA t
TOTAL NO. CALVES STUDIED 26TOTAL NO. DAYS PUMPED 370TOTAL NO. SPECIAL STUDIES PERFORMED 480TOTAL NO. INLET TUBES RETAINED 8TOTAL NO. AUTOPSIES 20
SPECIAL STUDIES
1. Stroke Volume Limiter and TH1anti-coagulation regimen
2 Failure induced with intracororariLidocaine via Judkins Catheter irclosed chest preparation
3. Failure induced with Lidocaine inopen chest preearation
4. Cx coronary artery ligation with DPTI/TTE studies in open chest preparatior
S. Paced rate and rhythm changes6. Comparison o synchronous and
asynchronous pumping7. Increase in prelsad with LAW' Dexirar
Encrease in afterload with Lecophedinfusions
9. Decrease in alterload with Nitroprusside infusions
IS Changes in heart rate and mrardiloxygen consumption
11 Plasma fHgb and Erythrocyte OsmoticFragility teslirq
1C Sacrifice with photography NeointslaATP analysss and histolep
Fig. 3. A summary of our most recent experiments.
432

PATIENT ROOM MONITOR ROOM CVSRL
Fig. 4. Clinical monitoring system to be used during initial trials. This system has been evolvedfrom a similar system used in long-term bovine experiments, see text.
SUMMARY
An intracorporeal left ventricular assist device capable of capturing theentire cardiac output, profoundly lowering left ventricular pressure andwork throughout the cardiac cycle while maintaining and/or augmentingsystemic pressure has been developed, extensively tested in-vitro and in-vivo, and validated. Comprehensive federal criteria and protocols for itsuse in man have been formulated and fulfilled. Through the process ofserial external peer review, the legal, moral, social, and ethical concernshave been defined and resolved. Controlled, limited, initial clinical trialsare imminent.
The Informed Consent forms to be utilized are included as Appendix 1.
433
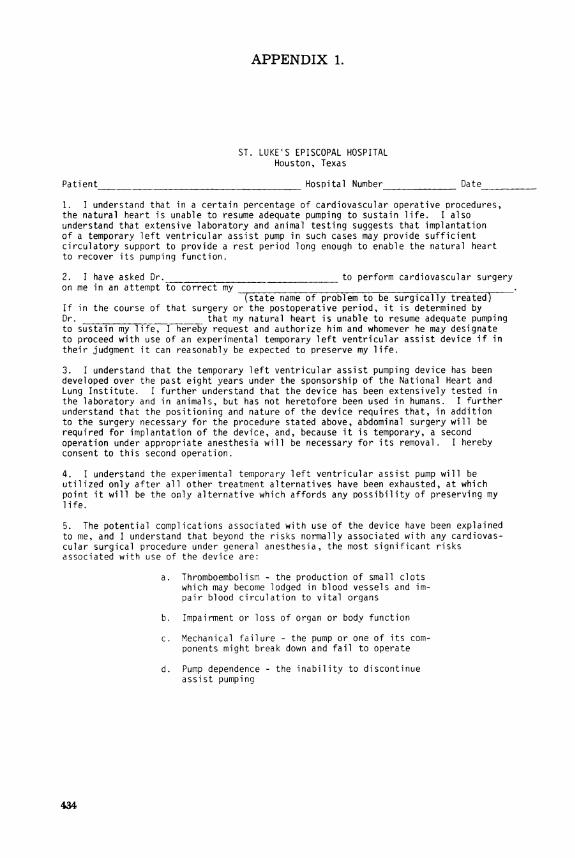
APPENDIX 1.
ST. LUKE'S EPISCOPAL HOSPITALHouston, Texas
Patient Hospital Number Date
1. I understand that in a certain percentage of cardiovascular operative procedures,the natural heart is unable to resume adequate pumping to sustain life. I alsounderstand that extensive laboratory and animal testing suggests that implantationof a temporary left ventricular assist pump in such cases may provide sufficientcirculatory support to provide a rest period long enough to enable the natural heartto recover its pumping function.
2. I have asked Dr. to perform cardiovascular surgeryon me in an attempt to correct my
(state name of problem to be surgically treated)If in the course of that surgery or the postoperative period, it is determined byDr. that my natural heart is unable to resume adequate pumpingto sustain my life, I hereby request and authorize him and whomever he may designateto proceed with use of an experimental temporary left ventricular assist device if intheir judgment it can reasonably be expected to preserve my life.
3. I understand that the temporary left ventricular assist pumping device has beendeveloped over the past eight years under the sponsorship of the National Heart andLung Institute. I further understand that the device has been extensively tested inthe laboratory and in animals, but has not heretofore been used in humans. I furtherunderstand that the positioning and nature of the device requires that, in additionto the surgery necessary for the procedure stated above, abdominal surgery will berequired for implantation of the device, and, because it is temporary, a secondoperation under appropriate anesthesia will be necessary for its removal. I herebyconsent to this second operation.
4. I understand the experimental temporary left ventricular assist pump will beutilized only after all other treatment alternatives have been exhausted, at whichpoint it will be the only alternative which affords any possibility of preserving mylife.
5. The potential complications associated with use of the device have been explainedto me, and I understand that beyond the risks normally associated with any cardiovas-cular surgical procedure under general anesthesia, the most significant risksassociated with use of the device are:
a. Thromboembolism - the production of small clotswhich may become lodged in blood vessels and im-pair blood circulation to vital organs
b. Impairment or loss of organ or body function
c. Mechanical failure - the pump or one of its com-ponents might break down and fail to operate
d. Pump dependence - the inability to discontinueassist pumping
434
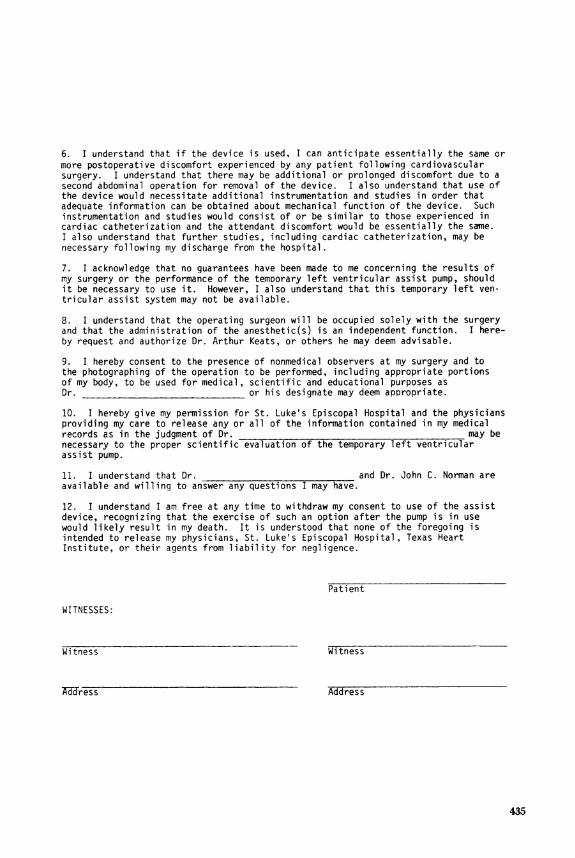
6. I understand that if the device is used, I can anticipate essentially the same ormore postoperative discomfort experienced by any patient following cardiovascularsurgery. I understand that there may be additional or prolonged discomfort due to asecond abdominal operation for removal of the device. I also understand that use ofthe device would necessitate additional instrumentation and studies in order thatadequate information can be obtained about mechanical function of the device. Suchinstrumentation and studies would consist of or be similar to those experienced incardiac catheterization and the attendant discomfort would be essentially the same.I also understand that further studies, including cardiac catheterization, may benecessary following my discharge from the hospital.
7. I acknowledge that no guarantees have been made to me concerning the results ofmy surgery or the performance of the temporary left ventricular assist pump, shouldit be necessary to use it. However, I also understand that this temporary left ven-tricular assist system may not be available.
8. I understand that the operating surgeon will be occupied solely with the surgeryand that the administration of the anesthetic(s) is an independent function. I here-by request and authorize Dr. Arthur Keats, or others he may deem advisable.
9. I hereby consent to the presence of nonmedical observers at my surgery and tothe photographing of the operation to be performed, including appropriate portionsof my body, to be used for medical, scientific and educational purposes asDr. or his designate may deem appropriate.
10. I hereby give my permission for St. Luke's Episcopal Hospital and the physiciansproviding my care to release any or all of the information contained in mv medicalrecords as in the judgment of Dr. _ may benecessary to the proper scientific evaluation of the temporary left ventricularassist pump.
11. I understand that Dr. and Dr. John C. Norman areavailable and willing to answer any questions I may have.
12. I understand I am free at any time to withdraw my consent to use of the assistdevice, recognizing that the exercise of such an option after the pump is in usewould likely result in my death. It is understood that none of the foregoing isintended to release my physicians, St. Luke's Episcopal Hospital, Texas HeartInstitute, or their agents from liability for negligence.
Patient
WITNESSES:
Witness Witness
Address Address
435
REFERENCES
1. Arthur J, Dove GB, Migliore JJ, Fuqua J, Hood W and Norman JC: A comparison of acutehemodynamic effects of abdominal left ventricular assist device (ALVAD) pumping in thenon-failing and failing canine heart. Clin Res 21:401, 1973
2. Bregman D, Parodi EN, Reemtsma K, Malm JR: Advances in clinical intraaortic balloonpumping. Coronary Artery Medicine and Surgery. J. C. Norman (ed), Appleton-Century-Crofts, New York, 1975
3. Carlos C, Daly B, Migliore J, Igo S, Hibbs W and Norman J: Improved design and experi-mental management modifications in abdominal left ventricular assist device: preclinicaltesting. Medical Instrumentation 9:66, 1975
4. Carlos CJ, Nitta S, Igo SR, Hibbs CW, Fuqua JM, Edmonds CH, Robinson WJ and NormanJC: Production of controlled left ventricular failure in calves using intracoronary lidocainehydrochloride. Ann Thorac Surg, 1975 (in press)
5. Carlos CJ, Nitta S, Igo SR and Norman JC: Abdominal left ventricular assist device(ALVAD): Hemodynamic effects after lidocaine-induced left ventricular failure. Proc of28th Ann Conf on Eng in Med and Biol 17:358, 1975
6. Carlos CJ, Igo SR, Hibbs CW, Nitta S, and Norman JC: Physiologic effects of varying degreesof afterloading with levarterenol and nitroprusside during abdominal left ventricular assistdevice (ALVAD) pumping in the awake, unanesthetized calf. ASAIO Abstracts 4:8, 1975
7. Coleman S, Whalen R, Robinson W, Huffman F and Norman J: A preclinical drive console fora pneumatically-powered left ventricular assist device. Clin Res 20:854, 1972
8. Concepts of Intraaortic Balloon Pumping: An Interdisciplinary Approach. MassachusettsGeneral Hospital, 1974
9. Curran WJ: The first mechanical heart transplant: informed consent and experimentation.N Engl J Med 291:1015, 1974
10. Daly BDT, Edmonds CH, Igo SR, Hughes DA, Migliore JJ and Norman JC: Right ventriculareffects of left ventricular unloading with an abdominal left ventricular assist device (ALVAD)in the calf. The Physiologist 17(3) :205, 1974.
11. Dove GB, Migliore JJ, Fuqua JM, Edmonds CH, Robinson WJ, Huffman FN and Norman JC:An abdominal left ventricular assist device (ALVAD): experimental physiologic analyses, III.Cardiac output. Proc of 26th Ann Conf on Eng in Med and Biol 15:148, 1973
12. Dove G, Arthur J, Migliore J, Fuqua J, Hood W and Norman JC: End-diastolic segmentlength (EDSL) and derived muscle length (ML) analyses during abdominal left ventricularassist device (ALVAD) pumping. Clin Res XXI(3) :415, 1973
13. Edmonds CH, Igo SR, Huffman FN and Norman JC: Effects of blood pump inflow tubesretained in the left ventricular apex. ASAIO Abstracts 3:21, 1974
14. Edmonds CH, Fuqua JM, Carlos CJ and Norman JC: Effects of increasing preload duringabdominal left ventricular assist device (ALVAD) pumping. Proc of 28th Ann Conf on Engin Med and Biol 17:357, 1975
15. Edmonds CH, Fuqua JM, McMillan MK, Migliore JJ and Norman JC: The effects of an ab-dominal left ventricular assist device on erythrocyte osmotic fragility. Medical Instrumentation9:67, 1975
16. Ford PJ, Weintraub RM: Intraaortic Balloon Pumping Manual, 2nd edition, Beth IsraelHospital, Boston, Massachusetts, 1975
17. Fuqua JM, Hibbs CW, Gernes DB and Norman JC: Non-invasive quantitation and maximiza-tion of blood flow in pneumatically-actuated cardiac assist or replacement devices. Proc of 28thAnn Conf on Eng in Med and Biol 17:355, 1975
18. Fuqua JM, Edmonds CH, Carlos CJ and Norman JC: An intracorporeal left ventricularassist device: human fitting studies. ASAIO Abstracts 4:19, 1975
19. Galioto FM, Dawson JT, Migliore JJ, Daly BDT, Messer JV and Norman JC: Serialechocardiographic assessment of left ventricular function in the calf before and after abdominalleft ventricular assist device implantation. Proc FASEB 32:332, 1973
20. Hibbs CW, Fuqua JM, Robinson WJ and Norman JC: Deleterious effects of impropersynchronization during implantable left ventricular assist pumping. ASAIO Abstracts4:25, 1975
21. Hibbs CW, Fuqua JM, Robinson WJ and Norman JC: Computerized monitoring system forclinical left ventricular assist device evaluations. Proc of 28th Ann Conf on Eng in Medand Biol 17:356, 1975
22. Hughes DA, Edmonds CH and Norman JC: An abdominal left ventricular assist device(ALVAD): patient acceptability survey. ASAIO Abstracts 3:32, 1974
23. Hughes DA, Edmonds CH, Igo SR, Daly BDT and Norman JC: An abdominal left ventricularassist device: experimental physiologic analyses. J Surg Res 17:255, 1974
24. Hughes DA, Igo SR, Daly BDT, Fuqua JM, Edmonds CH and Norman JC: The effects ofan abdominal left ventricular assist device on myocardial oxygen supply/demand ratios inthe normally perfused and ischemic bovine myocardium. Ann Thorac Surg 19:301, 1975
436
25. Igo SR, Migliore JJ, Fuqua JM and Norman JC: Effects of an abdominal left ventricularassist device (ALVAD) on myocardial contractility during acute coronary occlusion: experi-mental physiologic analyses, III. J Surg Res 17:177, 1974
26. Igo S, Edmonds C, Daly B, Hughes D and Norman J: Determinants of induced subendocardialischemia as reflected by DPTI/TTI ratios, in occluded and non-occluded zones of bovineleft ventricle. The Physiologist 17(3) :253,1974
27. Igo SR, Hibbs CW, Fuqua JM, Nitta S, Edmonds CH, Norman JC: Non-invasive determinantsof left ventricular function by echocardiography: Value during intraaortic balloon pumping(IABP) in man. Proc. of 28th Ann Conf on Eng in Med and Biol 17:123, 1975
28. Igo SR, Carlos CJ, Hibbs CW, and Norman JC: Chronic evaluation of cardiac output andleft ventricular assist device (ALVAD) pumping. ASAIO Abstracts 4:29, 1975
29. Igo SR, Hibbs CW, Fuqua JM and Norman JC: Comparisons of synchronous and asynchronousabdominal left ventricular assist device (ALVAD) pumping. ASAIO Abstracts 4:29, 1975
30. Johnson MD, Igo SR, Carlos CJ and Norman JC: Indirect measurements of myocardialoxygen consumption (MVO2) during acute and chronic abdominal left ventricular assistpumping in calves using pressure-rate-time (PRT) calculations. ASAIO Abstracts 4:30, 1975
31. Kolff WJ: The mechanical heart on the medical horizon. Cardiovascular Diseases, Bulletinof the Texas Heart Institute 2(3) :265, 1975
32. Liss RH, Edmonds CH, Fuqua JM and Norman JC: Pseudo or neointimal viability: acontroversial criteria of artificial heart pump linings. J Med Instrumentation 9:81, 1975
33. Mansfield PR, Sauvage LR, and Smith JC: Factors Inducing Thrombus in Artificial Hearts.In J. C. Norman (Ed), Coronary Artery Medicine and Surgery. Appleton-Century-Crofts,New York, 1975. Page 968
34. Migliore JJ, Robinson WJ, Fuqua J, Dove G, Huffman FN and Norman JC: An abdominalLVAD: experimental physiologic analyses, I. Proc 8th Congr of Europ Soc for Exper Surg. Oslo,Norway, May 2-5, 1973. Page 97
35. Migliore JJ, Dove GB, Fuqua JM, Edmonds CH, Robinson WJ, Huffman FN and NormanJC: An abdominal left ventricular assist device (ALVAD)): experimental physiologic analyses,IV. Myocardial blood flow. Proc of 26th Ann Conf on Eng in Med and Biol 15:149, 1973
36. Migliore J, Arthur J, Fuqua J, Dove G and Norman J: Myocardial arteriovenous oxygencontent and derived consumption (qO.,) during abdominal left ventricular assist device(ALVAD) pumping. Clin Res 21:438, 1973
37. Molokhia FA, Asimacopoulos PJ, Robinson WJ, Huffman FN and Norman JC: Left ventricularassist devices (LVAD) in the calf: anesthesia, ventilation, antiarrhythmic regimen andimplantation. Research Animals in Medicine. Lowell T. Harmison (Ed). DHEW PublicationNo (NIH) 72-333. Pages 383-389, October 2, 1973
38. Nitta S, Edmonds CH, Carlos CJ, Migliore JJ and Norman JC: Systematic searches forflock emboli in the calf following intracorporeal left ventricular assist device (ALVAD)implantation. ASAIO Abstracts 4:45, 1975
39. Nitta S, Igo SR, Carlos CJ, Fuqua JM, Hibbs CW, Edmonds CH, Trono R, Robinson WJand Norman JC: Chronic evaluations of mean left ventricular outflow impedance (LVZo)during abdominal left ventricular assist device (ALVAD) pumping: preclinical readinessstudies. Japanese Soc for Artif Organs, 1975 (in press)
40. Norman JC, Whalen RL, Daly BDT, Migliore J and Huffman FN: An implantable abdominalleft ventricular assist device (LVAD). Clin Res 20:855, 1972
41. Norman JC: An abdominal left ventricular assist device (ALVAD): perspectives and prospects.Cardiovascular Diseases, Bulletin of the Texas Heart Institute 1:251, 1974
42. Norman JC, Cooley DA: Coronary artery occlusive disease: current pandemic and surgicalCardiovascular Diseases, Bulletin of the Texas Heart Institute 2:26, 1975
43. Norman JC: The artificial heart: perspectives, prospects and problems of a high appliedtechnology. Cardiovascular Diseases, Bulletin of the Texas Heart Institute 2(3) :259, 1975
44. Norman JC (Ed): Coronary Artery Medicine and Surgery, Concepts and Controversaries.Appleton-Century-Crofts, New York, 1975
45. Robinson WJ, Migliore JJ, Arthur J, Fuqua J, Dove G, Coleman S, Huffman F and NormanJC: An abdominal left ventricular assist device (ALVAD): experimental physiologic analyses,II. Trans ASAIO 19:229, 1973
46. Robinson WJ, Igo SR, Daly BDT, Migliore JJ, Hughes DA, Edmonds CH, Fuqua JM Jr,Huffman FN and Norman JC: An abdominal left ventricular assist device (ALVAD):chronic hemodynamic analyses in the calf. Trans ASAIO 19:709, 1974
47. Robinson WJ, Maddeaux PR, France NE and Norman JC: Preliminary cost estimates forclinical application of left ventricular assist devices (LVADD). Proc 28th Ann Conf on Engin Med and Biol 17:359, 1975
48. Robinson W, Daly B, Hughes D, Migliore J, Igo S and Norman J: An abdominal leftventricular assist device: preclinical studies. Ann Thorac Surg 19:540, 1975
49. Wilson WS: Bypass Grafts for Coronary Artery Disease: State of the Art. In CoronaryArtery Medicine and Surgery. JC Norman (Ed). Appleton-Century-Crofts. New York, 1975
437