Pericarditis Cours DCEM. Most Common Causes of Acute Pericarditis Infectious Viral Tuberculosis...
25
Pericarditis Cours DCEM
-
Upload
unique-bates -
Category
Documents
-
view
218 -
download
1
Transcript of Pericarditis Cours DCEM. Most Common Causes of Acute Pericarditis Infectious Viral Tuberculosis...

Pericarditis
Cours DCEM

Most Common Causes of Acute Pericarditis
Infectious
Viral
Tuberculosis
Pyogenic Bacteria
Noninfectious
Postmyocardial infarction
Uremia
Neoplastic disease
Radiation induced
Connective tissue disease
Drug induced
Pathology of Acute PericarditisSerous pericarditis• Few PMN, lymphcytes and histiocytes• The exudate is a thin fluid secreted by mesothelial cells
Serobibrinous pericarditis• Most common form• Exsudate is rich in plasma proteins including fibrinogen• Appearance of “bread and butter”• Portions of the visceral and parietal pericardium may
become thickened and fused• May lead to constrictive pericarditis
Suppurative (or purulent) pericarditis
Hemorrhagic pericarditis

Clinical Features
• Chest pain• Fever• Dyspnea: reluctance of the patient to breathe deeply
because of the pleuritic pain• Pericardial friction rub: sharp; best heard with patient
leanign forward while exhaling; evanescent

ECG in Pericarditis
• Diffuse ST elevation in multiple leads
• No “mirror” image
• PR segment depression

Additional Tests in Pericarditis
• Echo: May or may not show a pericardial effusion
• ESR and CRP: Frequently elevated, but non specific
• Chest X-Ray: May or may not show a pericardial effusion; may show etiology of pericarditis: pneumonia, pleural effusion, cancer…
• Serological tests: ANA, Rheumatic factor…

The yield of diagnostic pericardiocentesis in
uncomplicated acute pericarditis is low, and
should be reserved for patients with very
large effusions or evidence of cardiac
chamber compression

Treatment of Acute Pericarditis
Idiopathic or viral pericarditis• Self-limited disease (runs its course in 1-3 weeks)• Rest + pain relief (analgesics, aspirin, anti-inflammatory
drugs)• Oral corticosteroids are often effective for severe or
recurrent pericardial pain, but should not be used in uncomplicated cases, because of potentially devastatin side effects and because of increased risk of recurrence
Post-MI pericarditis rest + aspirin
Purulent pericarditis catheter drainage + antibiotics
Uremia Intensive dialysis
Neoplastic

Pericardial Effusion
• 3 factors determine whether a pericardial effusion remains clinically silent, or whether symptoms of cardiac compression ensue:– The volume of fluid– The rate at which the fluid accumulates– The compliance characteristics of the pericardium

Clinical Features of Pericardial Effusion
• Asymptomatic• Dull constant ache in the left side of the chest• Symptoms of cardiac tamponade• Compression of adjacent structures: dysphagia,
dyspnea, hoarseness, hiccups• Decrease in intensity of heart sounds• No friction rub• Dullness to percussion of the left lung over the angle of
the scapula (Ewart’s sign)

Diagnostic Studies of Pericardial Effusion
Chest X ray: normal; if > 250 ml, enlarged cardiac silhouette in a globular, symmetric fashion
ECG: Decrease voltage; electrical alternans
Echo: Most important test; gives the diagnosis; can identify pericardial collections as small as 20 ml; determine whether ventricular filling is compromised

Treatment of Pericardial Effusion
• Treatment of the cause
• An asymptomatic effusion may be left for years without specific intervention
• If hemodynamic compression occurs, pericardiocenthesis should be performed
Cardiac Tamponade
Most common etiologies• Neoplastic• Postviral• Uremic• Acute pericardial hemorrhage
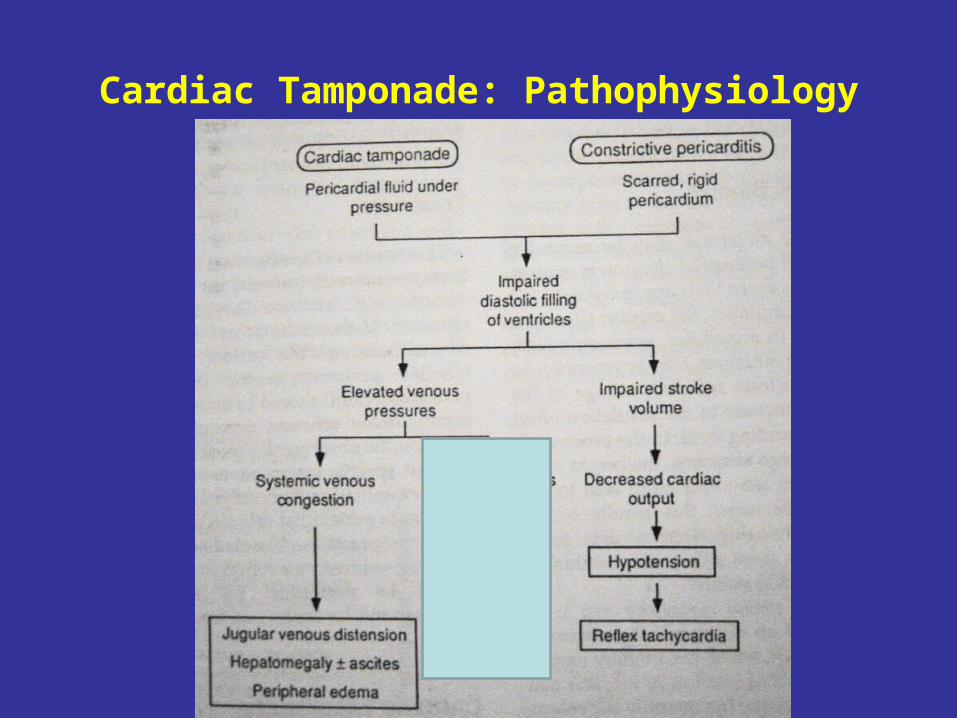
Cardiac Tamponade: Pathophysiology

Tamponade: Clinical Features
• Jugular venous distension• Hypotension• Quiet heart on examination• Sinus tachycardia• Dyspnea and tachypnea• Pulsus paradoxus• Clear lungs +++

Pulsus paradoxus
• Inspiration
• Decrease intra-thoracic pressure
• Increase in venous return to the RV
• The RV cannot expand because of the external compression by pericardial fluid
• Bulging of the interventricular septum to the LV
• Decrease LV filling
• Decrease blood pressure

Diagnostic Approach to Tamponade
• Echo
• Cardiac catheterization

Echocardiographic Findings in Tamponade

Hemodynamic Findings in Tamponade and Constrictive Pericarditis

Constrictive Pericarditis
• Etiology:• Any cause of acute pericarditis• Most common: idiopathic pericarditis• In the past, the most common form was tuberculous
pericarditis
• Pathology:• Following acute pericarditis, there is resorption of pericardial
fluid• In some patients (rare), the fluid undergoes organization with
fusion of the 2 layers followed by fibrous scar formation• Sometimes, calcification of the layers may ensue, leading to
further stiffening of the pericardium

Constrictive Pericarditis: Pathophysiology
• Abnormality occurs during diastole• Systolic contraction of the ventricle is normal• The scarred pericardium inhibits normal filling of the cardiac
chambers• As blood passes from the RA into the RV, the RV size expands and
quickly reaches the limit imposed by the constricting pericardium• At that point, further filling is suddently arrested and venous return
to the RV ceases• Systemic venous pressure increases and signs of right-sided heart
failure• In addition, impaired filling of the LV causes a reduction in stroke
volume, cardiac output and blood pressure

Clinical Features of Constrictive Pericarditis• Reduced cardiac output: fatigue, hypotension,
tachycardia• Elevated systemic venous pressure: jugular distension,
hepatomegaly, ascites, peripheral edema• On auscultation: early diastolic “knock” may follow S2. It
represents the sudden cessation of ventricular diastolic filling imposed by the rigid pericardial sac
• No pulsus paradoxus• Kussmaul’s sign: during inspiration the increased venous
return accumulates in the intrathoracic systemic veins because the negative intrathoracic pressure cannot be transmitted to the RV through the rigid pericardial sac. This causes the jugular veins to become more distended during inspiration
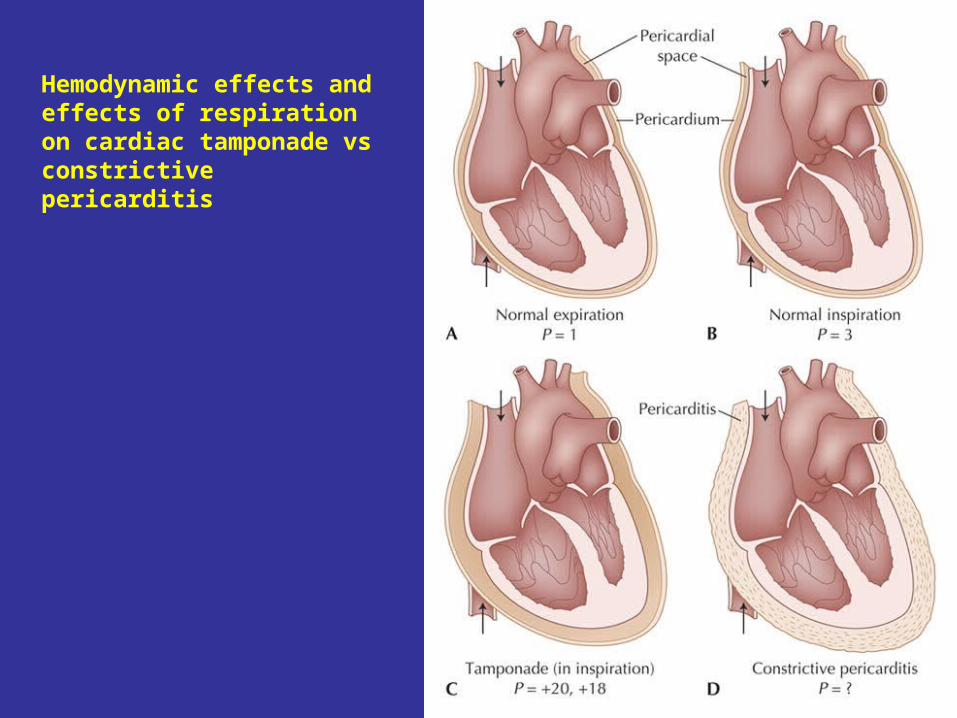
Hemodynamic effects and effects of respiration on cardiac tamponade vs constrictive pericarditis

Diagnostic Approach to Constrictive Pericarditis
• Chest X Ray: normal or mildly increased cardiac silhouette. Calcifications of the pericardium in 50%
• ECG: non specific ST/T abnormalities, atrial arrythmia• Echo: The ventricular cavities are small and contract vigorously;
diastolic ventricular filling terminates abruptly in early diastole• CT or MRI: Increased pericardial thickness• Cardiac catheterization:
• Elevation and equalization of diastolic pressures in the 4 cardiac chambers
• LV and RV: dip and plateau• Prominent y descent in right atrial tracing

Hemodynamic Findings in Constrictive Pericarditis