10/2012medslides.com1 Pericardial Disease. 9/98medslides.com2 Pericardial Disease Acute Pericarditis...
53
10/2012 medslides.com1 Pericardial Disease
-
Upload
phyllis-mitchell -
Category
Documents
-
view
233 -
download
4
Transcript of 10/2012medslides.com1 Pericardial Disease. 9/98medslides.com2 Pericardial Disease Acute Pericarditis...

10/2012 medslides.com 1
Pericardial Disease
9/98 medslides.com 2
Pericardial Disease
• Acute Pericarditis
• Chronic Relapsing Pericarditis
• Constrictive Pericarditis
• Cardiac Tamponade
• Localized and Low Pressure Tamponade
• Restrictive Cardiomyopathy

9/98 medslides.com 3
Pericardial Anatomy• Two major components– serosa (viceral pericardium)
mesothelial monolayerfacilitate fluid and ion exchange
– fibroa (parietal pericardium)fibrocollagenous tissue
• Pericardial Fluid– 15 - 50 ml of clear plasma ultrafiltrate
• Ligamentous attachments– to the sternum, vertebral column, diaphragm
9/98 medslides.com 4
9/98 medslides.com 5
Pericardial Physiology
• not needed to sustain life
• physiologic functions– limit cardiac dilatation–maintain normal ventricular compliance– reduce friction to cardiac movement – barrier to inflammation– limit cardiac displacement
9/98 medslides.com 6
Pericardial Inflammationpathogenesis
• Contiguous spread– lungs, pleura, mediastinal lymph nodes,
myocardium, aorta, esophagus, liver
• Hematogenous spread– septicemia, toxins, neoplasm, metabolic
• Lymphangetic spread
• Traumatic or irradiation
9/98 medslides.com 7

9/98 medslides.com 8
Pericardial Inflammationpathology
• inflammation provokes a fibrinous exudate with or without serous effusion
• the normal transparent and glistening pericardium is turned into a dull, opaque, and “sandy” sac
• can cause pericardial scarring with adhesions and fibrosis
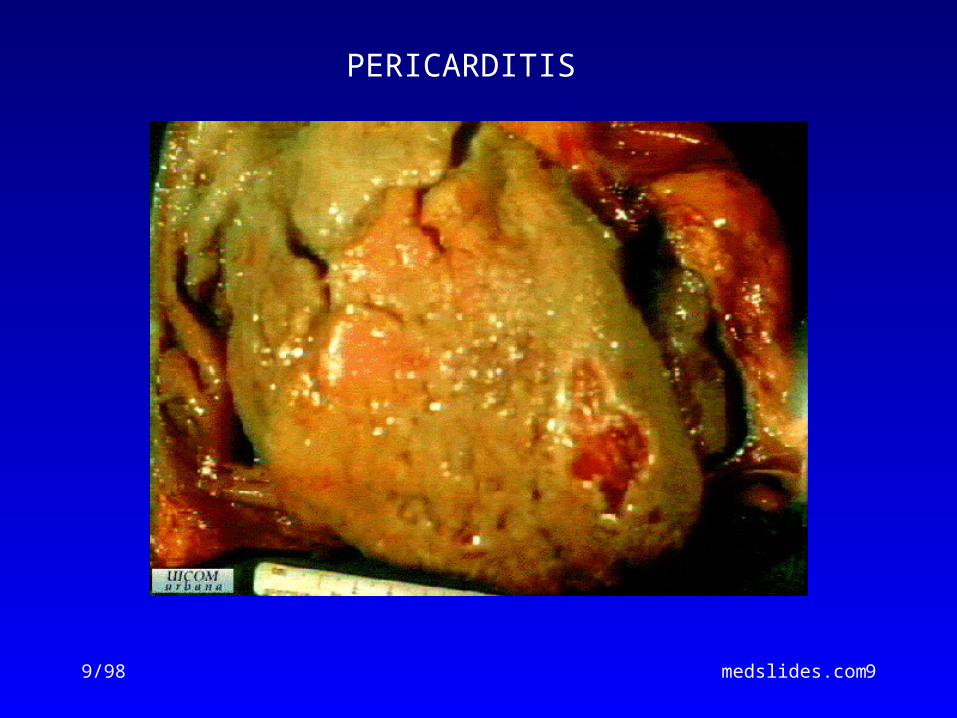
9/98 medslides.com 9
PERICARDITIS
9/98 medslides.com 10
Acute Pericarditiscommon causes
• Outpatient setting– usually idiopathic– probably due to viral infections– Coxsackie A and B (highly cardiotropic)
are the most common viral cause of pericarditis and myocarditis
– Others viruses: mumps, varicella-zoster, influenza, Epstein-Barr, HIV
9/98 medslides.com 11
Acute Pericarditiscommon causes
• Inpatient settingT = Trauma, TUMORU = UremiaM = Myocardial infarction (acute, post)
Medications (hydralazine, procain)O = Other infections (bacterial, fungal, TB)R = Rheumatoid, autoimmune disorder
Radiation
9/98 medslides.com 12
Acute PericarditisDiagnostic Clues
• Historysudden onset of anterior chest pain that
is pleuritic and substernal
• Physical exampresence of two- or three-component rub
• ECGmost important laboratory clue
9/98 medslides.com 13
Chest Pain Historypericarditis vs infarction
• Common characteristics– retrosternl or precordial with raditaion
to the neck, back, left shoulder or arm
• Special characteristics (pericarditis)–more likely to be sharp and pleuritic with coughing, inspiration, swallowing– worse by lying supine, relieved by
sitting and leaning forward
9/98 medslides.com 14
Heart Murmurs of Pericarditis
• Pericardial friction rub is pathognomic for pericarditis
• scratching or grating sound
• Classically three components:– presystolic rub during atrial filling– ventricular systolic rub (loudest)– ventricular diastolic rub (after A2P2)
9/98 medslides.com 15
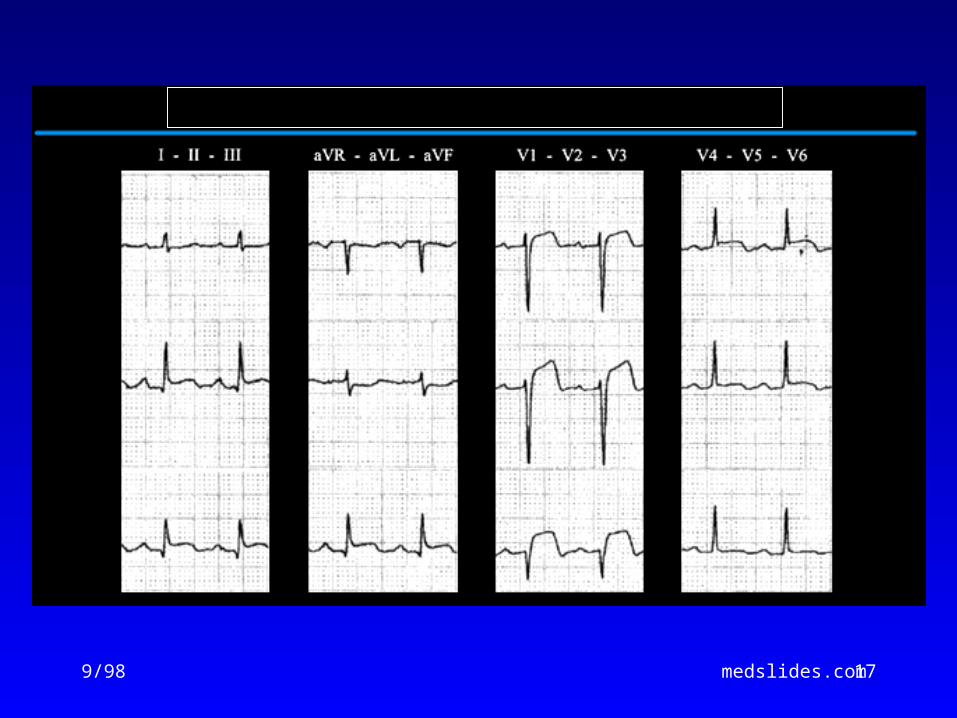
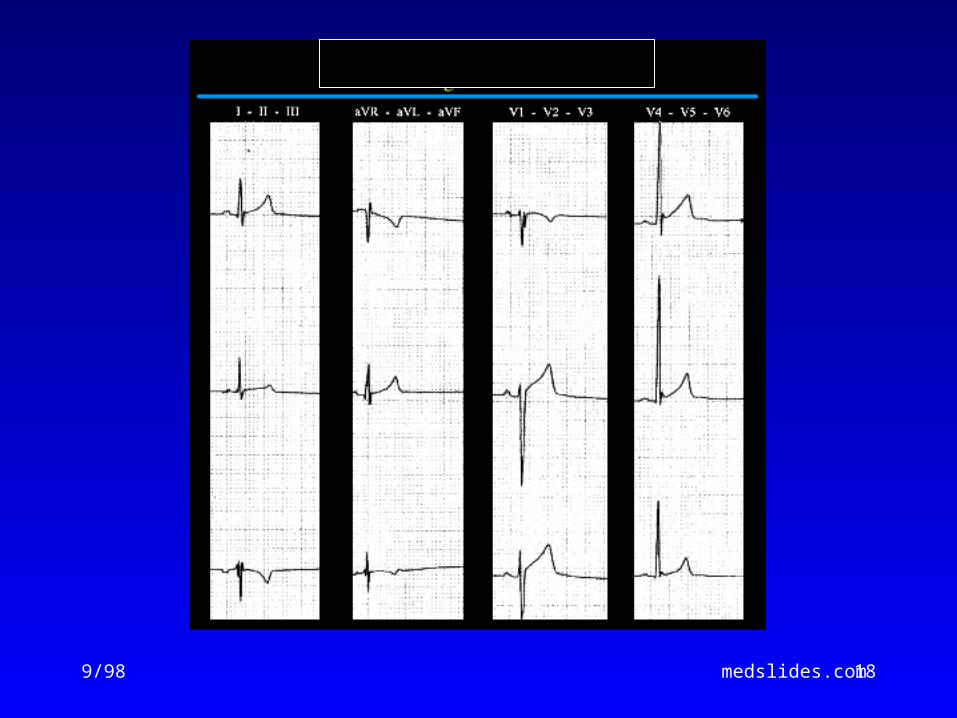
Acute PericarditisECG features
• ST-segment elevation– reflecting epicardial inflammation– leads I, II, aVL, and V3-V6– lead aVR usually shows ST depression
• ST concave upward – ST in AMI concave downward like a “dome”
• PR segment depression (early stage)• T-wave inversion– occurs after the ST returns to baseline

9/98 medslides.com 16
9/98 medslides.com 17
9/98 medslides.com 18
9/98 medslides.com 19
Acute PericarditisManagement
• Treat underlying cause
• Analgesic agents– codeine 15-30 mg q 4-6 hr
• Anti-inflmmatory agents– ASA 648 mg q 3-4 hrs– NSAID (indomethacin 25-50 mg qid)– Corticosteroids are symptomatically
effective , but preferably avoided
9/98 medslides.com 20
Chronic Relapsing Pericarditis
• occurs in a small % of patients with acute idiopathic pericarditis
• steroid dependency requiring gradual tapering over 3-12 months; NSAIDs, analgesics, and colchicine may be beneficial
• pericardiectomy for relief of symptoms is not always effective
9/98 medslides.com 21
Dressler’s Syndrome• Described by Dressler in 1956
• fever, pericarditis, pleuritis(typically with a low grade fever and a pericardial friction rub)
• occurs in the first few days to several weeks following MI or heart surgery
• incidence of 6-25%
• treat with high-dose aspirin
9/98 medslides.com 22
Acute PericarditisDifferential Diagnosis
• Acute myocardial infarction
• Pulmonary embolism
• Pneumonia
• Aortic dissection
9/98 medslides.com 23
Case Study 1
A 56-year-old man develops recurrent chest discomfort 5 days after an anterior myocardial infarction, which was managed initially with tissue plasminogen activator.
The pain is sharp and positional, radiating toward both clavicles. It is different from the pain associated with his infarction.
9/98 medslides.com 24
Case Study 1
Physical Exam:AfebrileNo pericardial friction rub
ECG: mild PR depression in lead 2no significant change in the evolution pattern of his Q-wave anteroseptal myocardial infarction
9/98 medslides.com 25
Case Study 1
The most appropriate therapy for this patient is:– Salicylates– Indomethacin– Corticosteroids– Colchicine
9/98 medslides.com 26
Case Study 2
A 36-year old woman presents to the ER for the second time in a week with pleuritic chest and left shoulder discomfort and a low-grade fever. She had been in an argument with her boy friend 6 days earlier during which he grabbed her by both shoulders and shook her violently.

9/98 medslides.com 27
Case Study 2
HR 82, BP 94/70.Left iris is green, right is blueShe is slender, has a straight back, long fingers, high-arched palate, and slight pectus excavatum.A pericardial friction rub is present.

9/98 medslides.com 28
Case Study 2
A chest radiograph shows an increased cardiac silhouette and a small left pleural effusion.
ECG shows NSR with diffuse J-point elevation and PR-segment depression in lead 2.
9/98 medslides.com 29
Case Study 2
Which one of the following tests should you order?– An erythrocyte sedimentation rate– A creatine kinase determination– An echocardiogram– An antinuclear antibody– A D-dimer
9/98 medslides.com 30
Constrictive Pericarditis
• rarely develop after an episode of acute idiopathic pericarditis
• more likely to develop after subacute pericarditis with effusion that evolve over several weeks
• more frequent after purulent bacterial or tuberculous pericarditis
9/98 medslides.com 31
Constrictive Pericarditisin the United States
• Idiopathic
• radiotherapy
• cardiac surgery
• connective tissue disorders
• dialysis
• bacterial infection
9/98 medslides.com 32
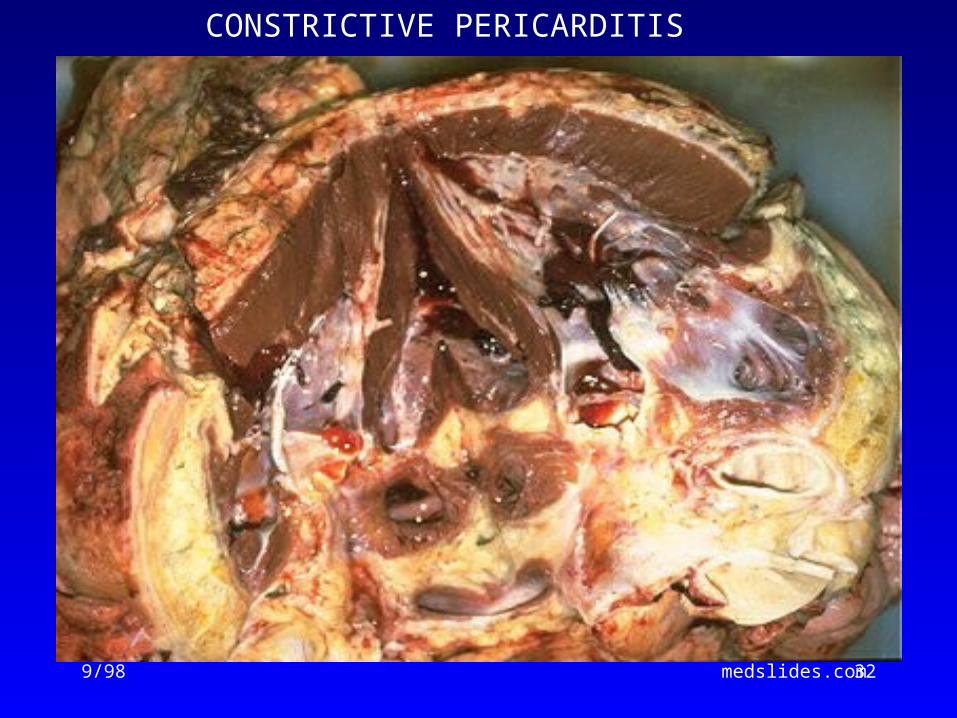
CONSTRICTIVE PERICARDITIS
9/98 medslides.com 33
Tuberculous Pericarditis
• Incidence of pericarditis in patients with pulmonary TB ranged from 1-8%
• Physical findings: fever, pericardial friction rub, hepatomegaly
• TB skin test usually positive
• Fluid smear for TB often negative
• Pericardial biopsy more definitive
9/98 medslides.com 34
Constrictive Pericarditis Physical Findings
• Jugular veins– prominent X and Y descent with inspiration (Kussmaul’s sign)
• Lungs - possible pleural effusion
• Heart - diastolic pericardial knock
• Abdomen: ascites, pulsatile liver
• Extremities: peripheral edema

9/98 medslides.com 35
Constrictive PericarditisDiagnosis
• often not recognized in its early phases by exam, x-ray, ECG, echo
• tendency to overlook elevated JVP
subacute chronic
diastolic knock + ++
Kussmaul’s + ++
paradoxical pulse ++ ++
9/98 medslides.com 36
Constrictive Pericarditiscatheterization findings
• Right and left heart pressure are measured simultaneously– right and left ventricular diastolic
pressure are elevated and nearly equal; may show classic “square root sign”
– RA pressure has steep X and Y descents and may rise during inspiration (Kussmaul’s sign)
9/98 medslides.com 37
Case Study 3
A 42-year old man presented because of increasing abdominal girth and lower extremity edema. A decade ago he underwent treatment for Hodgkin’s disease that included mantle field radiation therapy and MOPP chemotherapy.
9/98 medslides.com 38
Case Study 3
HR 84, BP 100/70
JVD not observed at 45 degrees
Absent vocal fremitus at right base
Heart sound is distant
An early-mid diastolic sound
3+ pitting edema bilaterally
9/98 medslides.com 39
Case Study 3
What is the most likely diagnosis?– Effusive pericarditis– Occult constrictive pericarditis– Constrictive pericarditis– Idiopathic dilated cardiomyopathy– Restrictive cardiomyopathy
9/98 medslides.com 40
Types of Effusive Fluid
• serous– transudative - heart failure
• suppurative– pyogenic infection with cellular debris and
large number of leukocytes
• hemorrhagic– occurs with any type of pericarditis– especially with infections and malignancies
• serosanguinous

9/98 medslides.com 41
Dignostic Evaluation
• Chest x-ray– usually requires > 200 ml of fluid– cannot distinguish between pericardial
effusion and cardiomegly
• Echocardiography– standard for diagnosing pericardial effusion– convenient, highly reliable, cost effective– false positives (M-mode)- left pleural effusion,
epicardial fat, tumor tissue, pericardial cysts
9/98 medslides.com 42
Noncompressing Effusion
• asymptomatic unless they are large enough to compress adjacent organs– dysphagia– cough– dyspnea– hoarseness– hiccups– abdminal fullness– nausea

9/98 medslides.com 43
ECG in Pericardial Effusion
• Diffuse low voltage– amount of fluid– electrical conductivity of the fluid
• Electrical alternans– alternating amplitude of the QRS– produced by heart swinging motion– also seen in PSVT, HTN, ischemia

9/98 medslides.com 44
Cardiac Tamponade
• Decompensated cardiac compression from increased intracardaic press
9/98 medslides.com 45
Cardiac Tamponade
• Early stage–mild to moderate elevation of central
venous pressure
• Advanced stage intrapericardial pressure
ventricular filling, stroke volume– hypotension – impaired organ perfusion

9/98 medslides.com 46
Beck’s Triad
• Described in 1935 by thoracic surgeon Claude S. Beck
• 3 features of acute tamponade – Decline in systemic arterial pressure– Elevation in systemic venous pressure
(e.g. distended neck vein)– A small, quiet heart
9/98 medslides.com 47
Cardiac TamponadeBedside Diagnosis
• Elevated jugular venous pressure
• Paradoxical pulse

9/98 medslides.com 48
Pulsus Paradoxus
• an exaggerated drop in blood pressure with inspiration (>10mmHg)
• tamponade without pulsus– atrial septal defect– aortic insufficiency– LVH with LVEDP
• pulsus without tamponade– COPD, RV infarct, pulmonary embolism
9/98 medslides.com 49
Echocardiography
• Pericardial effusion– highly reliable
• Cardiac tamponade– RA and RV diastolic collapse– reduced chamber size– distension of the inferior vena cava– exaggerated respiratory variation of the
mitral and tricuspid valve flow velocities
9/98 medslides.com 50
Pericardiocentesis
• Diagnostic tap– usually not indicated– rarely have positive cytology or
infection that can be diagnosed
• Therapeutic drainage– indicated for significant elevation of the
central venous pressure
9/98 medslides.com 51
Pericardial Window
• Balloon dilatation of a needle pericardiostomy
• subxyphoid surgical pericardiostomy
• video-assisted thoracoscopy with localized pericardial resection
• anterolateral thoracotomy with parietal pericardial resection
9/98 medslides.com 52
Localized and Low PressureCardiac Tamponade
• Localized tamponadedue to loculated pericardial effusion
• Low pressure tamponadedue to relative intravascular volume depletion

9/98 medslides.com 53
Restrictive Cardiomyopathy
• Differentiation from constrictive pericarditis may be difficult from intracardiac pressure tracings
• clues from history, physical exam, ECG, echo, CT and MR scan
• amyloidosis is most likely to simulate constrictive pericarditis