Occupational Dermatitis in Health Care Settings · PublicHealthOntario.ca If I had a...
60
Occupational Dermatitis in Health Care Settings Dr. Maureen Cividino, IPAC Physician PHO September 27, 2017 IPAC NEO Chapter Conference: If I had a Nickel…
-
Upload
trinhduong -
Category
Documents
-
view
217 -
download
0
Transcript of Occupational Dermatitis in Health Care Settings · PublicHealthOntario.ca If I had a...

Occupational Dermatitis in Health Care Settings
Dr. Maureen Cividino, IPAC Physician PHO September 27, 2017
IPAC NEO Chapter Conference: If I had a Nickel…

PublicHealthOntario.ca
If I had a ₂₈(Ni)ckel… I might end up with nickel dermatitis
2
• Nickel Sulphate is a common sensitizer that causes allergic contact dermatitis • 17% of women and 3% of men will have some
degree of nickel sensitivity • Most jewellery contains nickel • Also in snaps, buttons, watches, and cell phone batteries
Image Source: Creative Commons Licence http://www.nickelallergyinformation.com/atom.xml and Image Source: en.wikipedia.org a

PublicHealthOntario.ca
Authors
3
• Dr. Maureen Cividino
• Dr. Ray Copes

PublicHealthOntario.ca
Disclosures
4
• No Conflicts to disclose
• Views and opinions are those of the presenter and not necessarily those of PHO.
PublicHealthOntario.ca
Objectives
5
By the end of the presentation the participant will be able to:
• State the incidence and prevalence of occupational contact dermatitis by setting/exposures
• Describe how skin functions as a barrier and outline host and environmental factors that affect skin integrity
• Characterize exposure risks for irritant and allergic contact dermatitis and apply the industrial hierarchy of controls to reduce exposure and injury
• Recognize the role of skin colonization and infection in transmission of infection
• Outline prevention and management strategies for contact dermatitis

PublicHealthOntario.ca
Occupational skin disease not new
• Celsus – 100 AD, skin ulcers in those working with corrosive metals
• Ramazzini – 1700, describes skin disorders bath attendants, bakers, gilders, midwives, millers, miners and others
• Pott – 1775, scrotal cancer
in chimney sweeps
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1037746/pdf/brjindmed00217-0074.pdf
PublicHealthOntario.ca
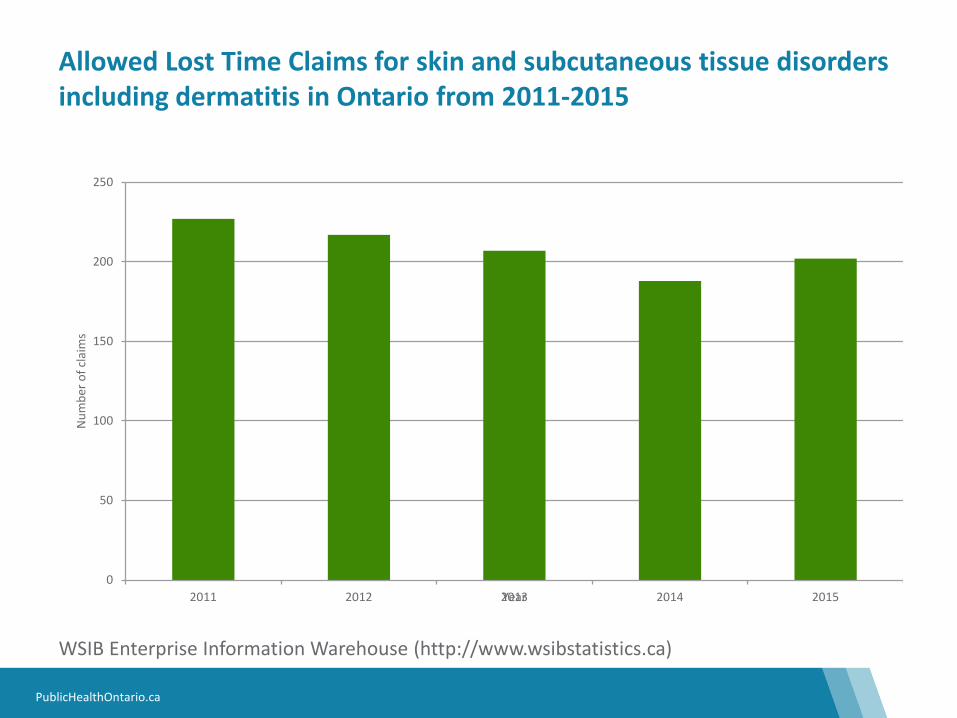
Allowed Lost Time Claims for skin and subcutaneous tissue disorders including dermatitis in Ontario from 2011-2015
WSIB Enterprise Information Warehouse (http://www.wsibstatistics.ca)
0
50
100
150
200
250
2011 2012 2013 2014 2015
Num
ber o
f cla
ims
Year

PublicHealthOntario.ca
Allowed Lost Time Claims for different diseases in Ontario in 2015
WSIB Enterprise Information Warehouse (http://www.wsibstatistics.ca)
0
200
400
600
800
1000
1200
Num
ber o
f cla
ims
Nature of Disease

PublicHealthOntario.ca
Dermatitis in the US Working Population • Collected from the 2010 National Health Interview
Survey • Approximately 10% of current/recent workers were
recorded as having dermatitis • The highest prevalence rates were found in health care
related industries • Approximately 6% of dermatitis cases were attributed
to work by health professionals • This represents approximately 850,000 cases of work-
related dermatitis among US workers in 2010
Luckhaupt S. Dahlhamer J, Ward B, Sussell A, Sweeney M, Sestito J, Calvert G. (2013). Prevalence of Dermatitis in the Working Population, United States, 2010 National Health Interview Survey. American Journal of Industrial Medicine. 56:625–634

PublicHealthOntario.ca
Occupations affected
• Agricultural Workers
• Beauty Industry Workers
• Construction Workers
• Electricians
• Food Industry Workers
• Health Care Workers
• Mechanics/Machinists
• Metalworkers

PublicHealthOntario.ca
Common Allergens
• Cobalt
• Chromates
• Cosmetics/fragrances
• Epoxies
• Nickel
• Plants
• Preservatives
• Resins
• Acrylics
• Rubber/latex
PublicHealthOntario.ca
Common Irritants
• Solvents
• Detergents
• Acids
• Bases
• Grease/oils
• Water

PublicHealthOntario.ca
We count on our skin for so many things! • Protection from injury
• Water preservation
• Shock absorption
• Tactile sensation
• Vitamin D synthesis
• Temperature control
• Lubrication
• Waterproofing
Image Source: Microsoft Clip Art
List from NIOSH

PublicHealthOntario.ca
Skin as an Organ
• Largest organ in the body
• Affected by our genetics
• Physical, chemical, mechanical
and biological exposures
• Radiation exposure (UV)
• Occupational
• non-occupational exposures
Image Source: Microsoft Clip Art

PublicHealthOntario.ca
Layers of the skin
Image Source: Commons.wikimedia.org

PublicHealthOntario.ca
Figure 2: Transcellular permeation
Figure 1: Intercellular lipid pathway
Figure 3: Through the appendages (hair follicles, glands)
3 Routes of Diffusion
Between cells
Through cells
Hair follicles Glands
Absorption Through Diffusion-molecules move from areas of high concentration to areas of low concentration
Image Source: http://www.cdc.gov/niosh/topics/skin/

PublicHealthOntario.ca
Absorption is key to both the risk and benefit to skin health
Image Source: Microsoft Clip Art
Image Source: Wikimedia.org
PublicHealthOntario.ca 18
Contact dermatitis refers to an inflammation of the skin resulting from direct contact of a substance with the surface of the skin
Irritant contact dermatitis (OCD)* the most common form and is caused when substances such as solvents or other chemicals irritate the skin. The exposure produces red, often more painful than itchy, patches on the involved skin areas
Allergic contact dermatitis (OCD) *occurs when a substance triggers an immune response. Nickel, perfumes, dyes, rubber (latex) products, topical medications and cosmetics frequently cause allergic contact dermatitis
Occupational contact urticaria (OCU)*is a cutaneous (skin) syndrome defined by the appearance of hives within minutes of contact with the responsible substance (latex, flour, modified proteins) *BOHRF; (OCD )occupational contact dermatitis
https://www.aaaai.org/conditions-and-treatments/conditions-dictionary/contact-dermatitisDefinition

PublicHealthOntario.ca 19
Healthy Skin vs.
Dermatitis
Allergens
Infection
Physical agents
Irritants

PublicHealthOntario.ca
Wet work causes irritant contact dermatitis
• HCWs clean their hands dozens of times per shift
• 25% of nurses report symptoms of dermatitis
• 85% give a history of skin problems at some point
• Frequent hand washing is a primary cause of
chronic irritant contact dermatitis
• Non-intact skin can become infected then pass infection to others
Image Source: Microsoft Clip Art
Irritants

PublicHealthOntario.ca
• Detergents (soaps) damage skin
• Hot water
• Low relative humidity (winter)
• Failure to use lotion/cream
• Moisture in gloves
• Powder in gloves
• Friction
• Shear forces
• Traditional surgical scrub brushes
Image Source: Microsoft Clip Art
Irritants

PublicHealthOntario.ca
Wet Work Irritant Contact Dermatitis
www.habia.org/.../ Dermatitis_300.jpg
• CrackingIrritants
• Peeling
• Dryness
• Itching
• Blisters
• Can become infected
• Can transmit infection Image Source: Commons.wikimedia.org
Pruney finger
Irritants

PublicHealthOntario.ca
Allergens
IgE reaction to specific allergen
Read in minutes
Latex must be under physician care
Food proteins: bananas, kiwi, avocado, cherries, tomatoes, shrimp, flour, modified soy
Pollens, grasses, ragweed
Moulds
Animals: cats, dogs, horses, mice
Dust: mites, cockroach
Type 1 Allergy (immediate ) Skin Prick Test; hive and redness (wheal and flare)
Image Source: enwikipedia.org
A

PublicHealthOntario.ca
• Rubber accelerators (sensitizer) benzothiazoles; MBT
• Carbamates; dithiocarbamates, diphenylguanidine
• Thiurams
• Hexamethylenetetramine
• Metals: nickel, platinum, chromium
• Biocides: formaldehyde, Quaternium 15, OPA, glutaraldehyde, isothiozolinones
• Bone cement (methyl methacrylate)
• Enzymatic Cleaners
Type IV Allergy Skin Patch test: delayed hypersensitivity (immune reaction-cell mediated)
Allergens
Sensitized T cell migrate to area of allergen Test read 48 to 72 and up to 96 hours later Image Source: enwikipedia.org

PublicHealthOntario.ca
• The resin of the plant is a sensitizer
• The vines and branches contain much more allergen than leaves
• Subsequent exposures result in greater reactions—can be severe
• Of relevance to health care for outdoor workers and can also be misdiagnosed as shingles or herpes
Type IV Allergy Poison Ivy
Image Source: CDC/Richard S. Hibbits from http://phil.cdc.gov/phil/details.asp
Allergens

PublicHealthOntario.ca
Infection
• HCW can become colonized or infected
• Hand hygiene and proper precautions (PPE) important
• Non-intact skin more likely to colonize
• HCWs have been epidemiologically linked to ongoing outbreaks
Bacterial Infection: Soft tissue (MRSA)
Image Source: CDC/Bruno Coignard, M.D.; Jeff Hageman, M.H.S., from http://phil.cdc.gov/phil/details.asp

PublicHealthOntario.ca
Image Source: CDC • Common cause of outbreaks in hospitals and long term care
• Often simultaneous infection in staff and patients
• Up to 6 weeks to develop symptoms for first exposure
• Prophylaxis and treatment with Nix which is effective but drying to the skin
Parasitic Infection: Sarcoptes scabiei skin scraping and clinical rash
http://www.medicinenet.com/scabies/page6.htmhttps://en.wikipedia.org/wiki/Sarcoptes_scabiei
Infection

PublicHealthOntario.ca
• Most common in dental settings, ICU, anesthesia and other settings where a hand will be in a mouth
• Painful and takes several days to settle
• Direct patient care should not be provided until lesion has completely healed, even if wearing gloves
Viral Infection: Herpetic Whitlow Infection
Image Source: CDC

PublicHealthOntario.ca
Image Source: CDC/Sherry Brinkman, from http://phil.cdc.gov/phil/details.asp
Image Source: enWikipedia.org
Image Source: CDC, from http://phil.cdc.gov/phil/details.asp
Image Source: Commons.wikipedia.org
Eczema
Fungal infection nails
Psoriasis
Host Factors: Underlying Skin Diseases

PublicHealthOntario.ca
Image Source: CDC/Sherry Brinkman, from http://phil.cdc.gov/phil/details.asp
Image Source: enWikipedia.org
Image Source: CDC, from http://phil.cdc.gov/phil/details.asp
Image Source: Commons.wikipedia.org
Eczema
Fungal infection nails
Psoriasis
Host Factors: Underlying Skin Diseases

PublicHealthOntario.ca 31
Importance of Hand Hygiene 5 steps to transmission of pathogens Outbreaks related to artificial nails
Infection Transmission

PublicHealthOntario.ca
4 Moments of Hand Hygiene
32

PublicHealthOntario.ca
WHO 5 steps to transmission of pathogens from one patient to another patient via HCW hands
Step 1
• Organisms present on patient’s skin AND/OR • Organisms shed on inanimate objects near patient
Step 2 • Organisms must be transferred to the hands of HCW
Step 3 • Organisms must be capable of surviving for a least several minutes on
HCW’s hands
Step 4 • Hand hygiene by the HCW must be inadequate, omitted, or inappropriate
cleaning agent
Step 5 • Contaminated hands of HCW has direct contact with another patient or
inanimate object that will come into direct contact with the patient
PublicHealthOntario.ca
Image Source: Public Health Ontario, 2013
• Organisms can be recovered from colonized intact skin
• Nearly 1,000,000 skin squames containing viable microorganisms are shed daily from normal skin!!
Transmission of Health Care Associated Pathogens

PublicHealthOntario.ca
New England Journal of Medicine Jan 15 2009 (Donskey) Curtis Donskey
HCW hand imprint after abd exam
After using ABHR
MRSA growth
Image Source: Curtis Donskey, with permission

PublicHealthOntario.ca
Jewelry and Artificial Nails
PublicHealthOntario.ca
Components for an effective hand care program
• Occupational Health support of “healthy hands” program at time of hire and throughout career
• Occupational history including skin health/exposures • Product selection matters • Education • Technique matters • Protection of hands a 24 hours 7 days a week commitment • Protecting Your Hands Fact Sheet for HCP • Your Hand Care Assessment Tool
Image Source: Public Health Ontario, 2013

PublicHealthOntario.ca
Product selection matters
• Preferably 70% to 90% ABHR at point of care
• Select ABHR with emollients
• Use hand hygiene products with low irritancy potential
• Get input from HCWs on products
• Get information from manufacturers regarding potential interaction with products
• Provide hand moisturizing skin care products
• Avoid barrier creams (not effective and false sense of security BOHRF)

PublicHealthOntario.ca
It’s not just oil and vinegar that don’t mix
• Know the ingredients in your products
• Know any interactions between products
• Label appropriately • MSDS must be
available and up to date
Image Source: Microsoft Clip Art

PublicHealthOntario.ca
Education • Education at orientation
and ongoing basis
• Document education sessions and attendance
• Know your hands by self-assessment
• Verify hand hygiene technique
• Specific education regarding moisturizing
• Educate regarding correct glove selection and usage
Image Source: Microsoft Clip Art

PublicHealthOntario.ca
Technique Matters
• Remove hand and arm jewelry when performing hand hygiene
• Use warm running water
• Rinse thoroughly
• Pat hands dry with paper towel
• Apply moisturizer
• Dry hands well before putting
on gloves
Image Source: Microsoft Clip Art

PublicHealthOntario.ca
Moisturizers
• Lotions, creams, ointments
• Oil-based and water-based
• Humectants (attract moisture through stratum corneum)
• Emollients are lipid-based and make the skin softer (aloe, rose oil, glycerin, shea butter, lanolin, eucarin, cocoa butter)
• Replace lipids (fats) which are important for barrier function
Image Source: Microsoft Clip Art

Glove Selection Risk assessment: choose correct glove for task
Glove Selection • Surgical glove: sterile;
consider latex allergy
• Nitrile glove: cleaning chemicals • Consider cuff length and
duration of task
• Vinyl glove: satisfactory for shorter task duration
• Chemotherapy glove: • Specific qualities re drug permeation
• Sandwich glove: not for patient care!
ASTM certified
Latex surgical glove
Vinyl glove
Nitrile glove
Chemotherapy glove
Sandwich glove
Images Source: All photos courtesy of St. Joseph’s Healthcare, Hamilton
Powder free

Elimination: remove the hazard
Substitution: replace with a safer alternative
Engineering Controls: enclose or automate the process, ventilation
Administrative Controls: safe work practices, health surveillance
Personal Protective Equipment- gloves, gown, eye protection, mask/respirator
Hazard
Worker
Images Source: Microsoft Clip Art

45
Eliimination
• Latex gloves; scented products; antimicrobial soaps (triclosan) • Spray nozzles for cleaning agents
Substitution
• lower concentrations of cleaning agents that are still effective • ABHR with emollients; better quality paper towel
Engineering Controls
• Alcohol Based Hand rub at point of use • Ready to use cleaning agents; automatic mixer at tap
Administrative Controls
• Policies and Procedures • Education and Training
PPE
• Gloves appropriate to exposure and to task • Cotton liners can benefit those with dermatitis
PublicHealthOntario.ca
Ten Key recommendations from the British Occupational Health Research Foundation (BOHRF) Systematic Review: Occupational Contact Dermatitis and Urticaria
46
Employers and their health and safety personnel should:
1. Implement programs to remove or reduce exposure to agents that cause OCD and OCU
2. Provide appropriate gloves and cotton liners where the risk of developing OCD or OCU cannot be eliminated by removing exposure to its causes
3. Make after-work (conditioning) creams readily available in the workplace and encourage workers to use them regularly

PublicHealthOntario.ca
Top 10 key recommendations from BOHRF
47
4. Do not promote the use of prework (barrier) creams, as this may confer on workers a false sense of security and encourage them to be complacent in following more effective preventative measures
5. Provide workers with appropriate health and safety information and training
6. Ensure that workers who develop OCD or OCU are properly assessed by a physician who has expertise in occupational skin disease for recommendations regarding appropriate workplace adjustments

PublicHealthOntario.ca
Top 10 Key Recommendations from BOHRF
48
7. Ask a worker who has been offered a job that will expose them to causes of OCD if they have a personal history of dermatitis, particularly in adulthood, and advise them of their increased risk, and care for and protect their skin
8. Ask the worker who has been offered a job that will expose them to causes of OCU if they have a personal history of atopy and advise them of their increased risk, and care for and protect their skin
9. Take a full occupational history whenever someone of working age presents with a skin rash, asking about their job, the materials with which they work, the location of the rash and any temporal relationship with work
PublicHealthOntario.ca
Final Recommendation from BOHRF
49
10. Arrange for a diagnosis of OCD or OCU to be confirmed objectively (patch tests and/or skin-prick tests) and not on the basis of a compatible history alone because of the implications for future employment

PublicHealthOntario.ca
Hand Care Program Summary • Hand Care Program should start at time of hire
• Education and Assessment including review of hand hygiene technique
• Include HCW in selection and placement of products
• Underlying hand condition and allergy important
• Ensure correct glove selection, use and technique
• Don’t forget importance of moisturizer
• Healthy hands are less likely to become infected and less likely to transmit infection
• Remember hand care is a 24/7 operation

PublicHealthOntario.ca
Occupational Health support “healthy hands” at Preplacement • Proactive Program
• Provide all HCPs with “Protecting Your Hands Fact Sheet for Health Care Providers”
• Review HCP correct hand hygiene technique
• Review factors to protect skin integrity
• Encourage early reporting of any skin irritation
• Do self skin assessment: • Appearance • Intactness • Moisture content • Sensation

PublicHealthOntario.ca
Over the Counter Treatments • Mild hydrocortisone treatment for minor dermatitis
• Best to apply when skin is still damp
• Use a small amount and rub in well
• Ointments are best for very dry skin
• Creams for normal dryness
• Lotions for weeping areas
• Oral antihistamines can help for itch; use non-drowsy
• If skin does not settle seek medical attention through your family doctor, occupational health and if necessary a dermatological referral can be made
Hand protection 24/7
Image Source : Microsoft Clip Art
Image Source : Microsoft Clip Art
Image Source : Microsoft Clip Art

PublicHealthOntario.ca
General Summary
54
• Healthy intact skin is our primary barrier against occupational and non-occupational skin exposures
• Irritant/allergic contact dermatitis and urticaria are prevalent in health care and community settings
• Wet work is a common occupation
• Potential for infection transmission through HCW hands
• Application of the industrial hierarchy of controls to reduce hazards in the workplace can be effective

PublicHealthOntario.ca
Acknowledgements
55
• Lori Schatzler
• Cassandra Taylor
• IPAC NEO Chapter
Public Health Ontario keeps Ontarians safe and healthy. Find out more at PublicHealthOntario.ca
For More Information About This Presentation, Contact:
Dr. Maureen Cividino at [email protected]
Works Cited • Dermatitis, Allergic Contact. (2008, October 15). Retrieved July 6, 2016, from Canadian Centre for Occupational Health & Safety:
https://www.ccohs.ca/oshanswers/diseases/allergic_derm.html
• Dermatitis, Irritant Contact. (2008, October 15). Retrieved July 6, 2016, from Canadian Centre for Occupational Health & Safety: https://www.ccohs.ca/oshanswers/diseases/dermatitis.html
• Belsito, D. V. (2005). Occupational Contact Dermatitis: Etiology, Prevalence, and Resultant Impairment/disability. J Am Acad Dermatol, 53(2), 303-313.
• Holness, D. L. (2013). Recent Advances in Occupational Dermatitis. Curr Opin Allergy Clin Immunol, 13(2), 145-150.
• Holness, D. L., & Kudla, I. (2012). Workers with Occupational Contact Dermatitis: Workplace Characteristics and Prevention Practices. Occup Med (Lond), 62(6), 455-457.
• Holness, D. L., Beaton, D., Harniman, E., DeKoven, J., Skotnicki, S., Nixon, R., et al. (2013). Hand and Upper Extremity Function in Workers With Hand Dermatitis. Dermatitis, 24(3), 131-136.
• Lampel, H. P. (2011). Occupational Contact Dermatitis. The Dermatologist, 19(12).
• Lurati, A. R. (2015). Occupational Risk Assessment and Irritant Contact Dermatitis. Workplace Health Saf, 63(2), 81-87.
• Nicholson, P. J. (2011). Occupational Contact Dermatitis: Known Knowns and Known Unknowns. Clin Dermatol, 29(3), 325-330.
• Saary, J., Qureshi, R., DeKoven, J., Pratt, M., Skotnicki-Grant, S., & Holness, D. L. (2005). A Systematic Review of Contact Dermatitis Treatment and Prevention. J Am Acad Dermatol, 53(5), 845-855.
• Wiszniewska, M., & Walusiak-Skorupa, J. (2015). Recent Trends in Occupational Contact Dermatitis. Curr Allergy Asthma Rep, 15(7), 43.

References • Bikowksi J. Moisturizers in Various Dermatologic Disorders. Cutis. 2001 Dec;68(5 Suppl):3-11
• Bikowski J. A Controlled Three-Part Trial to investigate the Barrier Function and Skin Hydration Properties of Six skin Protectants. Ostomy/Wound Management 2005; 51(12):30-42;
• Boyce JM, Kelliher S, Vallance N. Skin irritation and dryness associated with two hand-hygiene regimens: soap-and-water hand washing versus hand antisepsis with an alcoholic hand gel. Infect Control Hosp Epidemiol. 2000;21:80–85
• Centers for Disease Control. The National Institute for Occupational Health and Safety. Skin exposures and Effects. Available from: http://www.cdc.gov/niosh/topics/skin/
• De Vries JJ et al. Outbreak of Serratia marcescens colonizationadn infection traced to a healthcare worker with long-term carriage onteh hands. Infect. Control Hosp. Epidemiol. 2006. 27:1153-8.
• Diaz MBS, Habert AB, Borrasca V, Stempliuk V. Ciolli A, Araujo RE, Costa SF, Levin AS. Infection Control and Epidemiology. 2008;29(2):125-130.
• Donskey CJ, Eckstein BC. The hands give it away. 3rd ed. Massachusetts Medical Society. 2009;360.
• Fagernes M. Impact of finger rings on transmission of bacteria during hand contact. Infect Control Hosp Epidemiol 2009;30:427–432
58

References 2 • Girou E, Loyeau S, Legrand P, et al. Efficacy of handrubbing with alcohol based solution versus standard handwashing with
antiseptic soap: randomised clinical trial. BMJ. 2003;325(7360):362.
• Gordin FM, Schultz ME, Huber R, Zubairi S, Stock F, Kariyil J. A cluster of hemodialysis-related bacteremia linked to artificial fingernails. Infect Control Hosp Epidemiol 2007;28:743–744.
• Grunewald AM, Gloor M, Gehring W, Kleesz P. Damage to the skin by repetitive washing. Contact Dermatitis. 1995;32(4):225-32.
• Gustafson DR, Vetter EA, Larson DR, et al. Effects for 4 hand-drying methods for removing bacteria from washed hands: a randomized trial. Mayo Clin Proc. 2000;75(7):705-8.
• Larmer PJ, Tillson TM, Scown FM, Grant PM, Exton J. Evidence-based recommendations for hand hygiene for health care workers in New Zealand. The New Zealand Medical Journal [homepage on the internet]. C2008 [cited 2013 Sept 16]; 121(1272). Available from: http://journal.nzma.org.nz/journal/121-1272/3004/content.pdf
• McCormick RD, Buchman RL, Maki DG. Double-blind, randomized trial of scheduled use of a novel barrier cream and an oil-containing lotion for protecting the hands of health care workers. Am J Infect Control. 2000;28(4):302-10.
• Moolenaar RL. Prolonged outbreak of Pseudomonas aeruginosa in a Neonatal Intensive Care Unit. Infect Control Hosp Epidemiol 2000;21:80–85
• Nicholson PJ & Llewellyn D (Editors). Occupational contact dermatitis & urticaria. British Occupational Health Research Foundation. London. 2010.
• Price PB. The bacteriology of normal skin: a new quantitative test applied to a study of the bacterial flora and the disinfectant action of mechanical cleansing. Journal of Infectious Diseases. 1938;63:301–318.
59

References 3 • Provincial Infectious Diseases Advisory Committee. 2010. Best Practices for Hand Hygiene in All Healthcare Settings.
Available from: http://www.publichealthontario.ca/en/eRepository/2010-12%20BP%20Hand%20Hygiene.pdf
• Provincial Infectious Diseases Advisory Committee. 2012. Best Practices for Routine Practices and Additional Precautions in All Healthcare Settings; Available from: http://www.publichealthontario.ca/en/eRepository/RPAP_All_HealthCare_Settings_Eng2012.pdf
• Public Health Ontario. Just Clean Your Hands. Ontario’s evidence-based hand hygiene program. Released 2008.; Available from: http://www.publichealthontario.ca/en/BrowseByTopic/InfectiousDiseases/JustCleanYourHands/Pages/Just-Clean-Your-Hands.aspx
• Sasseville, D. (2004), Hypersensitivity to preservatives. Dermatologic Therapy, 17: 251–263. doi:10.1111/j.1396-0296.2004.04028.x
• Saary J et al. A Systematic review of contact dermatitis treatment and prevention. J Am Acad Dermatol. 2005; 53:845-55.
• World Health Organization. WHO guidelines on hand hygiene in health care. Geneva: World Health Organization; 2009. Available from: http://www.who.int/gpsc/5may/tools/9789241597906/en/
• Zhai H et al. A bioengineering study on the efficacy of a skin protectant lotion in prevention SLS-induced dermatitis. Skin Research and Technology. 2000; 6:77-80.
60