Eczema Dr. Majdy Naim. Majdy Naim Eczema 20102 Eczematous Diseases Contact Dermatitis Atopic...
83
Eczema Dr. Majdy Naim
-
Upload
berenice-mathews -
Category
Documents
-
view
241 -
download
2
Transcript of Eczema Dr. Majdy Naim. Majdy Naim Eczema 20102 Eczematous Diseases Contact Dermatitis Atopic...

Eczema
Dr. Majdy Naim

Majdy Naim Eczema 2010 2
Eczematous Diseases
Contact Dermatitis
Atopic Dermatitis
Seborrheic Dermatitis
Dyshidrotic Dermatitis
Nummular Dermatitis
Stasis Dermatitis

Majdy Naim Eczema 2010 3
Contact Dermatitis
A pruritic, epidermal and dermal inflamatory reaction caused or aggravated by items in contact with the skin.

Majdy Naim Eczema 2010 4
Contact Dermatitis
Irritant contact dermatitis Allergic contact dermatitis Phototoxic photoallegic contact dermatitis

Majdy Naim Eczema 2010 5
Irritant Contact dermatitis
Acute chronic

Majdy Naim Eczema 2010 6
Irritant Contact Dermatitis
It is the most common injury of the skin Irritant Responses include:
Wheals erythema Blistering Erosions Hyperkeratosis or thickening of the skin Pustules and skin dryness

Majdy Naim Eczema 2010 7
Factors that determine the response (Irritant Dermatitis) Individual factors Time of exposure Region of the skin exposed

Majdy Naim Eczema 2010 9
Acute dermatitis from turpentine

Majdy Naim Eczema 2010 10
Cement ulcerations

Majdy Naim Eczema 2010 11
Acute bullous contact dermatitis from a scabicide

Majdy Naim Eczema 2010 12
Weak- ICD
Prolonged contact Multiple exposure In skin that too wet or too dry Bleaches, cleansers, detergents, plants,
soaps, solvents, weak acids, weak alkalis

Majdy Naim Eczema 2010 13
W-napkin dermatitis

Majdy Naim Eczema 2010 14
Napkin dermatitis under the plastic part of the diaper

Majdy Naim Eczema 2010 15
ICD in a mechanic – caused by oil

Majdy Naim Eczema 2010 16
Irritant dermatitis due to licking
Majdy Naim Eczema 2010 17
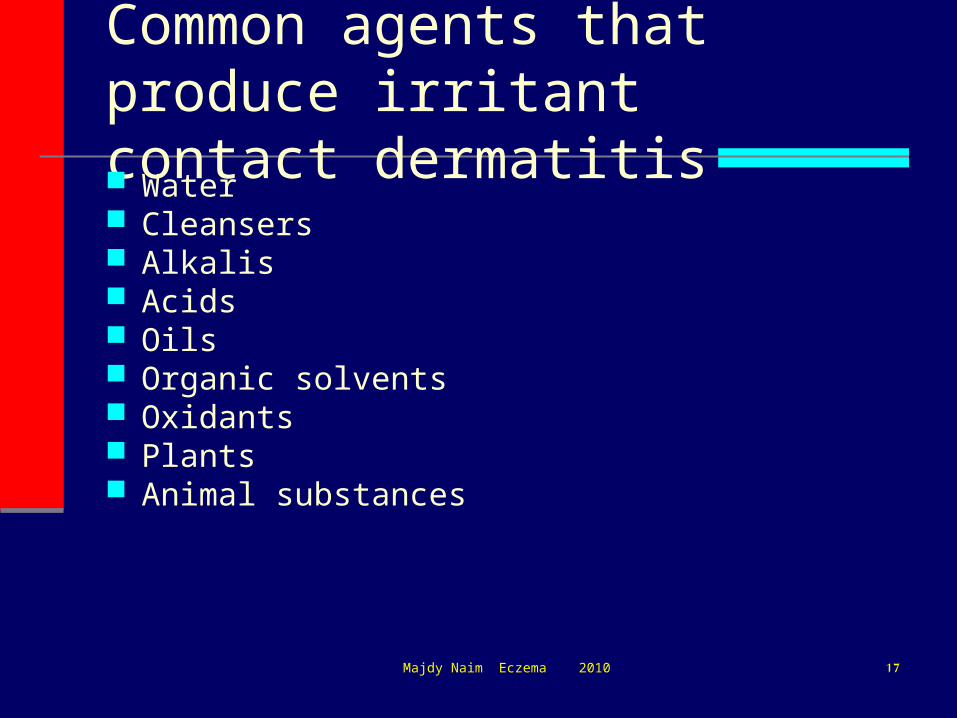
Common agents that produce irritant contact dermatitis Water Cleansers Alkalis Acids Oils Organic solvents Oxidants Plants Animal substances
Majdy Naim Eczema 2010 18
Most commonly located in the hands, forearms, face and legs

Majdy Naim Eczema 2010 19
Diagnosis:
History
Examination
Laboratory investigations: patch testing

Majdy Naim Eczema 2010 20
Differential diagnosis:
Atopic eczema
Discoid eczema
Allergic contact dermatitis
Fungal infection

Majdy Naim Eczema 2010 21
Treatment:
- Removal of the offending contact
- Restore a protective lipid layer
- Topical steroid may be necessary

Majdy Naim Eczema 2010 22
Allergic contact dermatitis It is a form of cell-mediated, antigen-
antibody immune reaction. Sensitization phase (1 week or longer) Elicitation phase (follows)
affect few workers; many skin sensitizers are also irritants
(chromates, nickel salts, and epoxy resin hardeners)
cross-sensitivity

Majdy Naim Eczema 2010 23
Allergic Contact Dermatitis
Presentation: erythematous and edematous or vesicular skin in the pattern of contact
Mechanism: cell-mediated immune response to antigens (contact allergens)

Majdy Naim Eczema 2010 24
Contact Allergens
poison ivy, poison oak Nickel sulfate Rubber Formaldehyde and related preservatives Para-phenylenediamine Fragrance Neomycin

Majdy Naim Eczema 2010 25
Poison Ivy/Oak Dermatitis
Presentation: acute pruritic dermatitis with linear grouping of vesicles
Confirmation: history of exposure


Majdy Naim Eczema 2010 27
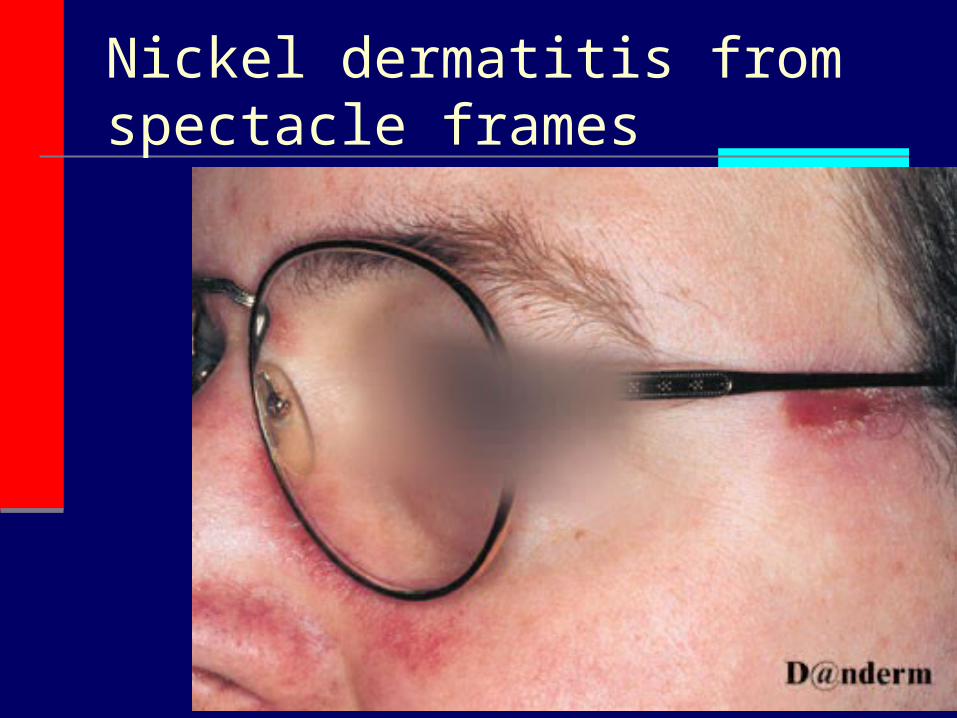
Nickel Dermatitis
Presentation: areas in contact with jewelry or metal clothing fasteners
Confirmation: skin patch testing

Majdy Naim Eczema 2010 28

Majdy Naim Eczema 2010 29

Majdy Naim Eczema 2010 30
Nickel dermatitis from brassiere clasps
Majdy Naim Eczema 2010 31
Nickel dermatitis from spectacle frames

Majdy Naim Eczema 2010 32
Rubber Dermatitis
Presentation: sites of exposure to… shoes (adhesive), elastic in clothing, surgical gloves, etc.
Confirmation: patch test to accelerators and antioxidants

Majdy Naim Eczema 2010 33

Majdy Naim Eczema 2010 34

Majdy Naim Eczema 2010 35
Chromate dermatitis from leather in work shoes

Majdy Naim Eczema 2010 36
Allergic contact dermatitis from thiuram in latex gloves

Majdy Naim Eczema 2010 37
Allergic contact dermatitis from fragrance in a cosmetic

Majdy Naim Eczema 2010 38
Allergic contact dermatitis from gluein sticking plaster

Majdy Naim Eczema 2010 39
Allergic contact dermatitis from plants in the compositae

Majdy Naim Eczema 2010 40
Allergic contact dermatitis from toluenesulfonyl urea in nail varnish

Majdy Naim Eczema 2010 41
Allergic contact dermatitis from toluenesulfonyl urea in nail varnish

Majdy Naim Eczema 2010 42
Allergic contact dermatitis caused by garlic

Majdy Naim Eczema 2010 43
Allergic contact stomatitis caused by the mercury in amalgam dental fillings in a mercury-sensitive
person

Majdy Naim Eczema 2010 44
Phototoxic contact dermatitis
Striped and bullous dermatitis of the legs after exposure to plant juices on a sunny day
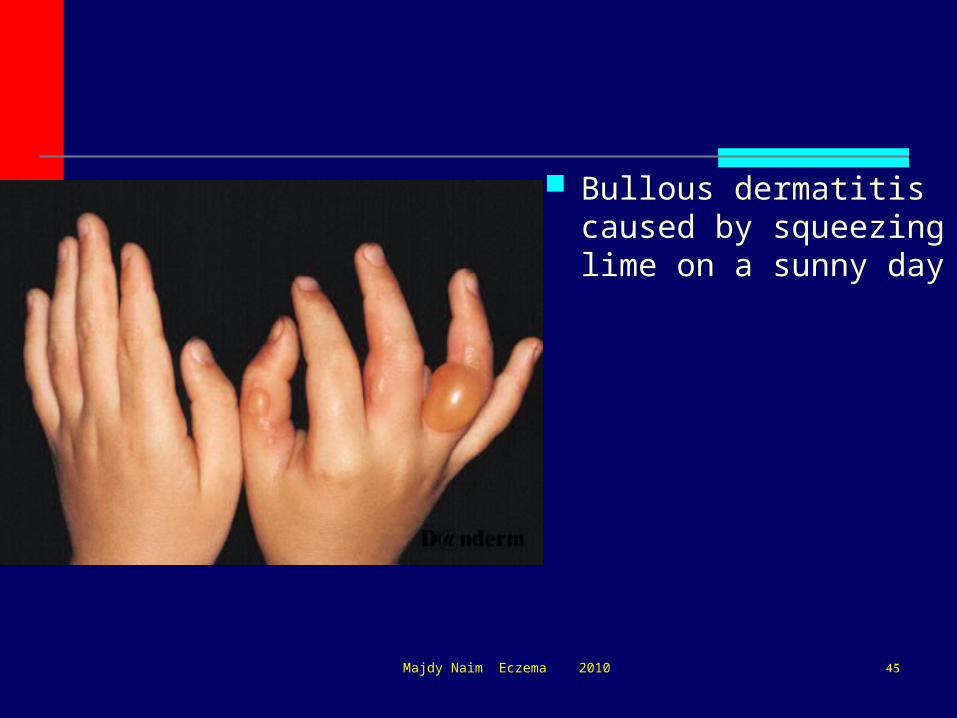
Majdy Naim Eczema 2010 45
Bullous dermatitis caused by squeezing lime on a sunny day

Majdy Naim Eczema 2010 46
Diagnosis:
History
Examination
Laboratory investigations: patch testing
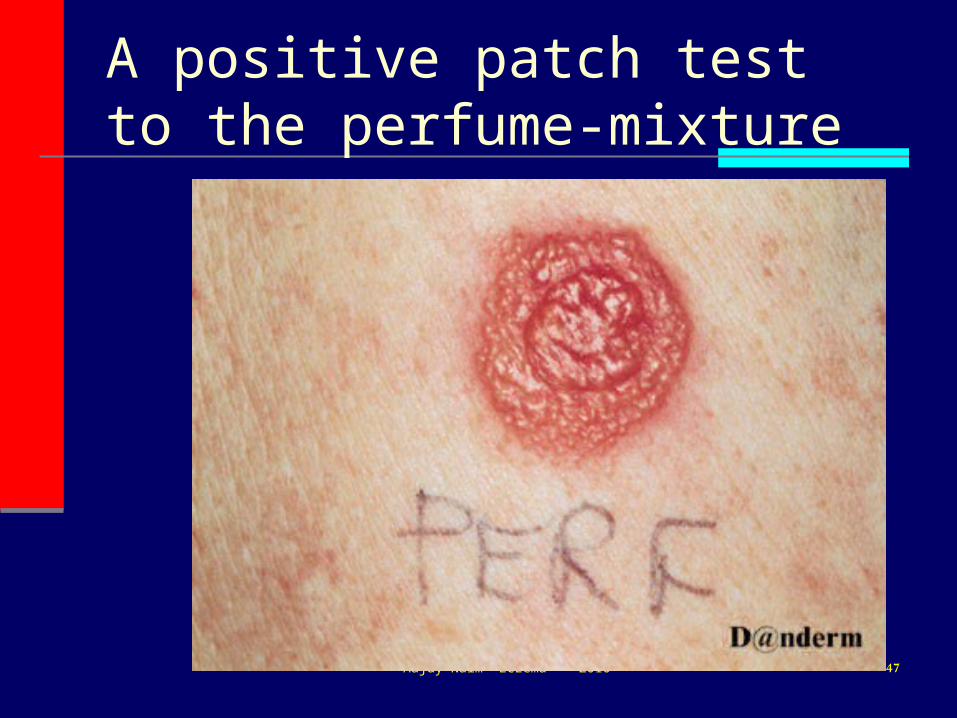
Majdy Naim Eczema 2010 47
A positive patch test to the perfume-mixture

Identification of Contact Allergens
Patch Testing
Finn Chamber

Majdy Naim Eczema 2010 49Patch Test

Majdy Naim Eczema 2010 50
Atopic Dermatitis

Majdy Naim Eczema 2010 51
What is the Cause? nobody has identified a single “cause” atopic dermatitis is a genetic disorder atopic children or their relatives may also
have asthma allergic rhinoconjunctivitis food allergies urticaria

Majdy Naim Eczema 2010 52
Atopic Dermatitis

Majdy Naim Eczema 2010 53
Environmental Suspects???
urbanization outdoor pollution indoor pollution/insulated homes fewer infections/infestations changes in food processing
NOBODY KNOWS FOR SURE

Majdy Naim Eczema 2010 54
Pathophysiology
specific gene abnormality not yet identified
may be more than one disease down regulation of TH1 lymphocytes (TH1
cells activate IFN- which inhibits IgE synthesis)
upregulation of TH2 lymphocytes (TH2 cells activate IL-4 which inhibits IFN-)

Majdy Naim Eczema 2010 55
Is it a Food Allergy?
no conclusive evidence that eczema is “a food allergy”
atopic children have a higher incidence of urticaria or anaphylaxis to peanuts, eggs, fish, milk
certain foods cause contact irritation and erythema eg. tomato sauce

Majdy Naim Eczema 2010 56
What about milk?
breast-feeding does not protect against atopic dermatitis
“allergen-free” diets in lactating women can compromise nutrition of the baby and mother
Effect of cow’s milk formula or soy formula in infants with eczema difficult to evaluate

Majdy Naim Eczema 2010 57
What about Allergy Testing? negative tests may be helpful 80% of atopic children have positive prick and
RAST tests often leads to unnecessary food and lifestyle
restrictions with consequences for child’s emotional and nutritional well-being
parents must be told that positive tests are < 20% predictive of clinical allergy

Majdy Naim Eczema 2010 58
Eczema – Psychological Issues
How does it affect sleep? How does it impact on the patient’s
behavior and family life? Is the patint’s diet or lifestyle restricted? Are there psychosocial factors that cause
anxiety eg. At home, at school

Majdy Naim Eczema 2010 59
Atopic Dermatitis
There is no “cure” Eczema can be
controlled 60% of children
“outgrow” eczema by 11 years of age
Treatment better than searching for the “cause”

Majdy Naim Eczema 2010 60
Treatment
Skin care and emollients Treatment of infection Topical anti-inflammatory agents
STEROIDS NEW NON-STEROID TOPICAL
IMMUNOMODULATORS Antihistamines

Majdy Naim Eczema 2010 61
Is the eczema infected? most cases of eczema are colonized by Staphylococcus
Aureus - staphylococcal superantigens may play a pathogenetic role
consider antistaphylococcal antibiotic therapy in all cases of weeping, crusted or very excoriated eczema
also consider STREPTOCOCCUS, HERPES SIMPLEX

Majdy Naim Eczema 2010 62
Treatment
Antibiotics, topical steroids, baths and emollients are safe and effective therapy

Majdy Naim Eczema 2010 63
Eczema Checklist 1
do parents have a basic understanding of the disease
what have they been told by other health care professionals, pharmacists, naturopaths, family and friends
do they have realistic expectations

Majdy Naim Eczema 2010 64
Eczema – Checklist 2
is skin care adequate Baths and emollients
is topical therapy optimal Topical
steroids/steroid-free agents
is the eczema infected Antibiotics oral/topical

Majdy Naim Eczema 2010 65
Eczema Checklist 3
Are other measures necessary? Wet wraps Higher potency topical steroids for short
periods Phototherapy Psychological evaluation/counselling for
child, parents, parent/child interaction Cyclosporin, Azathioprine

Majdy Naim Eczema 2010 66
Quality of Life

Majdy Naim Eczema 2010 67
Atopic Dermatitis
Aim of treatment is to improve the child’s quality of life and that of the family

Majdy Naim Eczema 2010 68
“Patients aren’t as concerned about how much you know until they know how much you care”
“Compassion without competence is dangerous”

Seborrheic dermatitis
Dr. Majdy Naim

Seborrheic dermatitis
a papulosquamous disorder patterned on the sebum-rich areas of the scalp, face, and trunk
In addition to sebum, this dermatitis is linked to Malassezia, immunologic abnormalities, and activation of complement
70Majdy Naim Eczema 2010

71Majdy Naim Eczema 2010

72Majdy Naim Eczema 2010

Commonly aggravated by changes in humidity, changes in seasons, trauma (eg, scratching), or emotional stress.
The severity varies from mild dandruff to exfoliative erythroderma.
73Majdy Naim Eczema 2010

Pathophysiology
normal levels of Malassezia but an abnormal immune response
74Majdy Naim Eczema 2010

Age
The usual onset occurs with puberty. It peaks at age 40 years and is less severe,
but present, among older people. In infants, it occurs as cradle cap or,
uncommonly, as a flexural eruption or erythroderma.
75Majdy Naim Eczema 2010

Frequency :3-5 %, dandruff 15-20% Race: Seborrheic dermatitis occurs in
persons of all races. Sex: The condition is slightly worse in males
than in females.
76Majdy Naim Eczema 2010

Scalp appearance varies from mild, patchy scaling to widespread, thick, adherent crusts
Skin lesions manifest as greasy scaling over red, inflamed skin
Distribution follows the oily and hair-bearing areas of the head and the neck, such as the scalp, the forehead, the eyebrows, the lash line, the nasolabial folds, the beard, and postauricular skin.
77Majdy Naim Eczema 2010

78Majdy Naim Eczema 2010

79Majdy Naim Eczema 2010

80Majdy Naim Eczema 2010

81Majdy Naim Eczema 2010

82Majdy Naim Eczema 2010

Treatment
Topical corticosteroids Dandruff responds to more frequent
shampooing Selenium sulfide (2.5%), ketoconazole, and
ciclopirox shampoos may help by reducing Malassezia yeast scalp reservoirs
83Majdy Naim Eczema 2010

Majdy Naim Eczema 2010 84
Thank you for your attention!