Dermatitis Atopik
32
dr. Archianda Arsad, SpKK Department of Dermato-Venereology Medical Faculty, North Sumatera University
-
Upload
riniadriani6817 -
Category
Documents
-
view
8 -
download
0
Transcript of Dermatitis Atopik
dr. Archianda Arsad, SpKK
Department of Dermato-Venereology
Medical Faculty, North Sumatera University

Atopic dermatitis (AD) = Atopic eczemao A chronically relapsing skin diseaseo Occurs most commonly during early
infancy and childhoodo Frequently associate with elevated
serum IgE levelso A personal/family history of atopy(+)
• Prevalence 3x than 1960s
• Industrialized countries > agricultural countries
• Female : male = 1,3:1
• AD, associated with :
- small family size
- increased income and education
- migration rural urban
- use of antibiotic

Hereditary
(genetic)
Food & aero Allergy (hypersensitivity) Irritan
allergens Infection
Climate
Cellular
immunity ATOPIC DERMATITIS
defect Xerosis
Decrease
skin barrier
Psychological effect
• Strong maternal influence• Chromosome 5q31-33, contains a clustered
family of functionally related cytokine genes :- IL-3, IL-4, IL-5, IL-13 expressed- GM-CSF by Th2 cell- Differences in transcriptional activity of the IL-4 gene influence AD predisposition- A significant association between a specific polymorphism in the mast cell chymase gene and AD
Key cells in AD skin :
• Langerhans cells
• Lymphocyte cells
• Eosinophils
• Mast cells


• Increased synthesis of IgE
• Increased specific IgE to multiple allergens, including foods, aeroallergens, microorganism, bacterial toxins, autoallergens
• Increased expression of of CD23 (affinity IgE receptor) on B cells and monocytes
• Increased basophil histamine release

• Impaired delayed-type hypersensitivity response
• Eosinophilia• Increased secretion of IL-4, IL-5 dan IL-13 by
Th2 cells• Decreased secretion of IFN-γ by Th1 cells• Increased soluble IL-2 receptor levels• Elevated levels of monocyte CAMP-
phosphodiesterase with increased IL-10 and prostaglandin E2
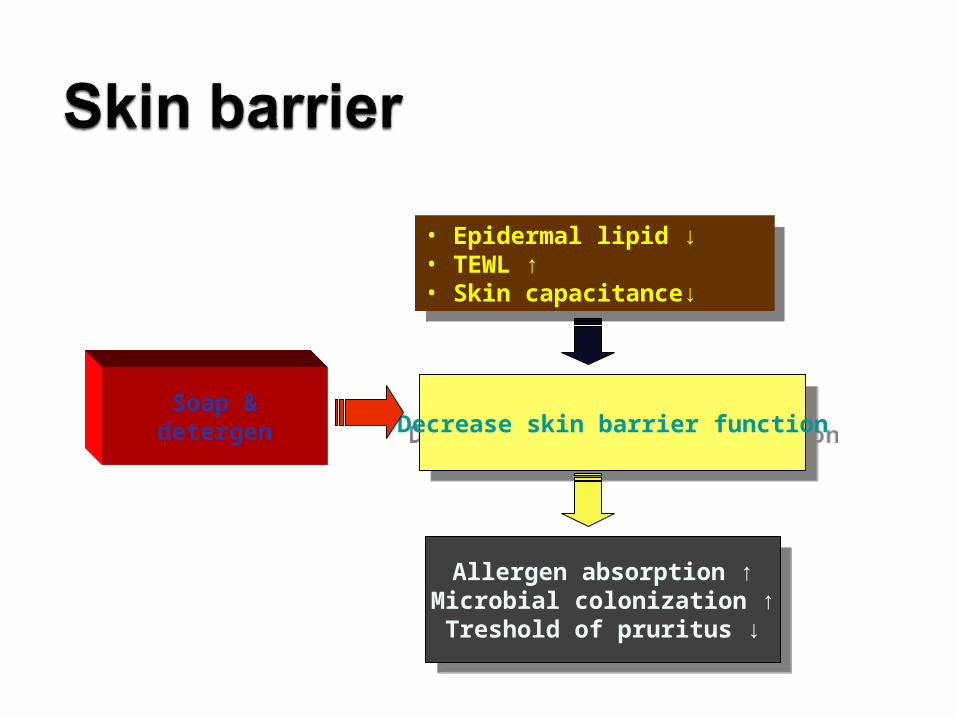
• Epidermal lipid ↓• TEWL ↑• Skin capacitance↓
• Epidermal lipid ↓• TEWL ↑• Skin capacitance↓
Soap &detergen Decrease skin barrier functionDecrease skin barrier function
Allergen absorption ↑Microbial colonization ↑Treshold of pruritus ↓
Allergen absorption ↑Microbial colonization ↑Treshold of pruritus ↓

• Food infant and children :milk and eggs
adult : seafood and nuts
• Aeroallergens : dust mites, animal danders, molds, pollens.
• Temperature & humidity
• Intense perspiration
• Emotional stress


• Diagnostic criteria of AD : various
• The UK working party’s : proposed alternative system, the criteria of Hanifin & Rajka (1994)
• Diagnose of AD:
-Three or more of the major criteria
-Three or more of the minor criteria

• Pruritus
• Typical morphology & distribution
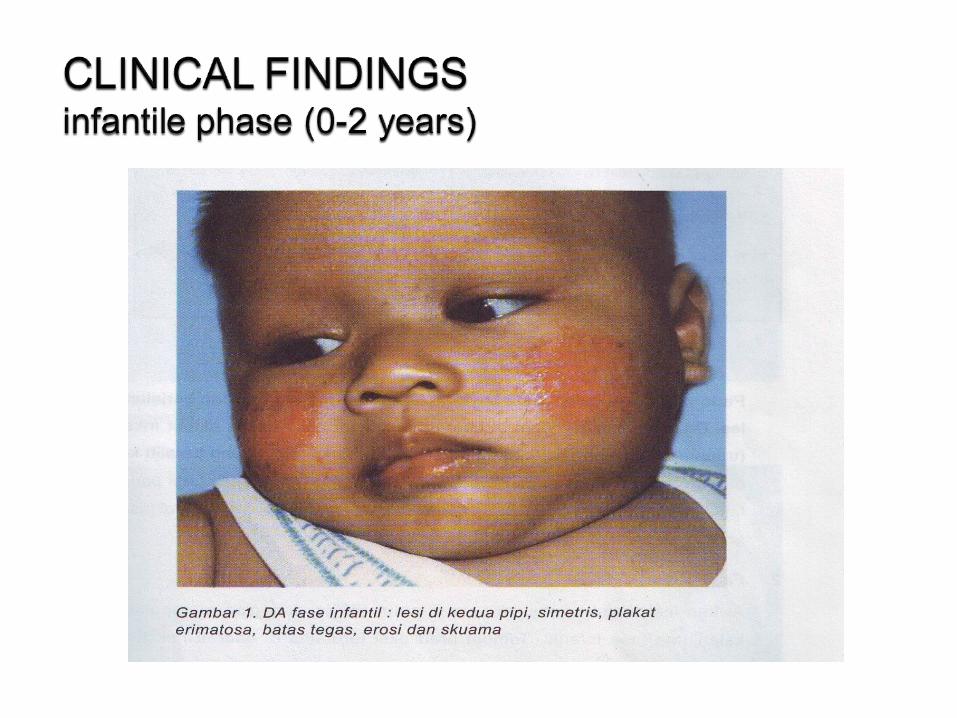
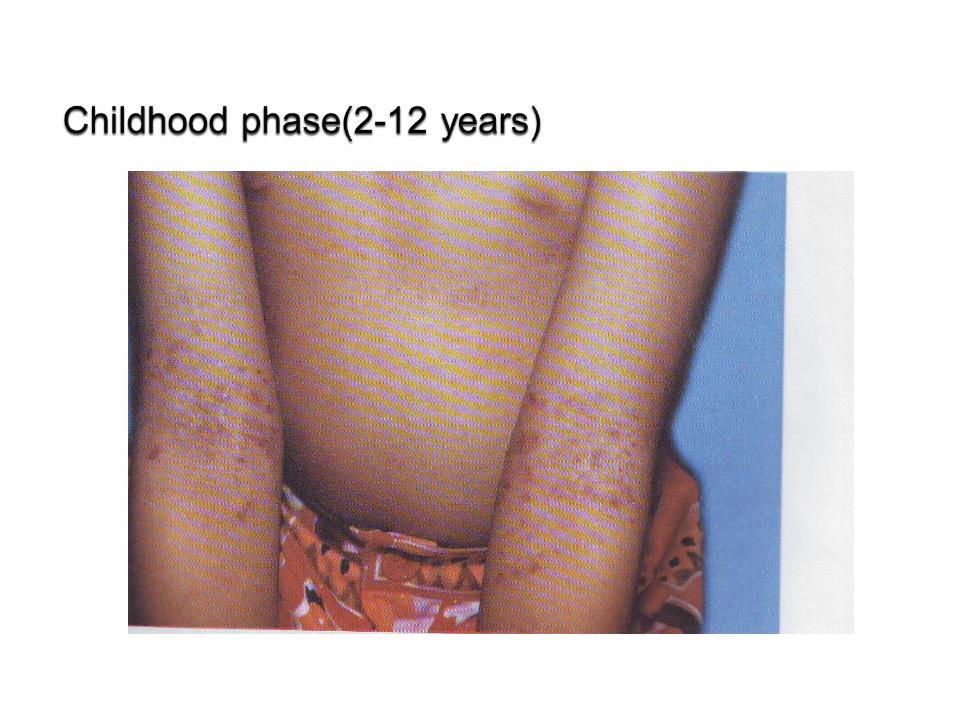
• Involvement during infancy & early childhood flexural
• Flexural dermatitis in adult
• Chronic or chronically relapsing dermatitis
• Personal or family history of atopy
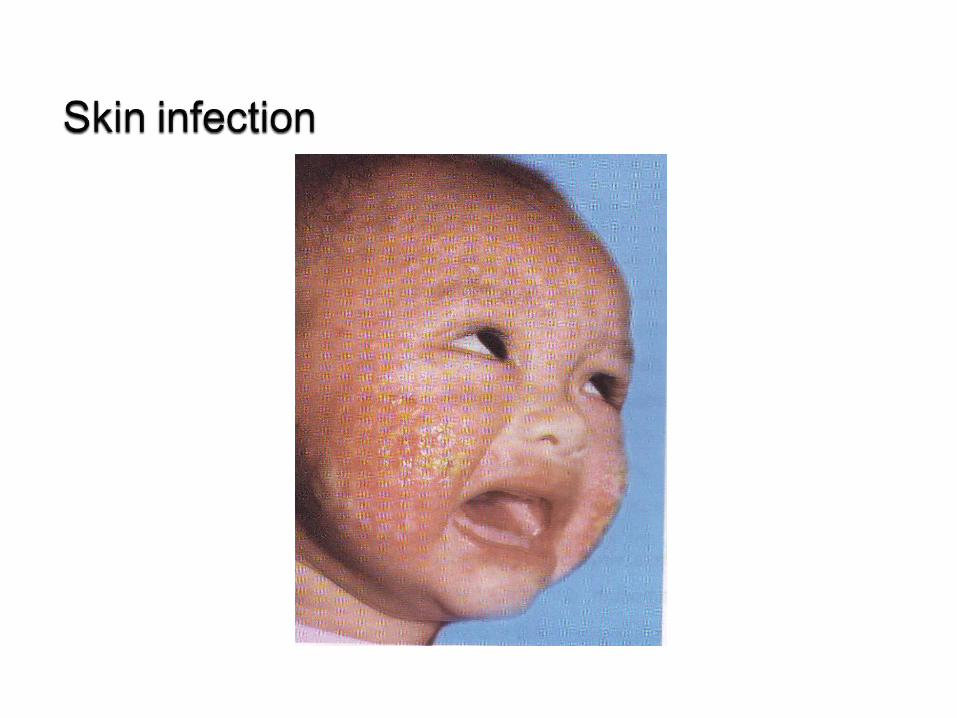
• Xerosis• Skin infection• Hand/foot dermatitis• Ichthyosis/palmar hyperlinearity/keratosis
pilaris• Pityriasis alba• Nipple eczema• White dermatografism & delayed blanched
response
• Cheilitis
• Infra orbital fold
• Anterior subcapsular cataracts
• Orbital darkening
• Facial pallor
• Itchiness when sweating

• Perifollicular accentuation
• Food hypersensitivity
• Duration of AD influenced by environment and psychis factors
• Immediate skin test reactivity
• Elevated serum IgE
• Early age of AD



Hyperlinearity of palmaris
Dennie Morgan folds


1. Seborrhoic dermatitis2. Contact dermatitis3. Numular dermatitis4. Scabies5. Ichthyosis6. Psoriasis 7. Dermatitis herpetiformis8. Sezary syndrome9. Leterrer-Siwe disease
In infant
1. Wiskott-Aldrich syndrome
2. Hyper- IgE syndrome
• Education
• Appropriate skin hydration & use of emollient skin barrier repair measure
• Avoidance of irritants
• Identification & treatment of complication bacterial, viral of fungal infection
• Treatment of psychosocial aspect of disease
• Antipruritic intervention

1. Topical therapy
2. Systemic therapy
1. Cutaneus hydration
2. Topical glucocorticoid
3. Topical calcineurine inhibitor
(tacrolimus & pimocrolimus)
1. Tar preparation
2. Topical anti histamine : not recommended except : doxepine cream 5%

1. Systemic glucocorticoid
2. Anti histamine
3. Infection agent
4. Interferon
5. Cyclosporine
6. Phototherapy (UVB, UVA+UVB, PUVA)

• Many factor correlate with AD → difficult to predict prognosis
• The predictive factors correlate with a poor prognosis of AD :
1. Widespread AD in childhood2. Associated allergenic rhinitis & asthma3. Family history of AD in parents or sibling4. Early age at onset of AD5. Being an only children6. Very high serum IgE levels
• 30-35% infatile AD → asthma / hay fever
• Often develop non specific irritant hand dermatitis