Myocardial oxygen consumption during isotonic and ... · thick-walled spherical model for the LV....
7
AMERICAN JOURNAL OF PHYSIOLOGY Vol. 223, No. 6, December 1972. Printed zn U.S.A. Myocardial oxygen consumption during isotonic and isovolumic contractions in the intact heart JOHN W. BURNS AND JAMES W. COVELL University of California, San Diego, School of Medicine, Department of Medicine, La Jolla, California 92037 BURNS, JOHN W., AND JAMES W. COVELL. Myocardial oxygen consumption during isotonic and isovolumic contractions in the intact heart. Am. J. Physiol. 223(6): 1491-1497. 1972.-There is now sub- stantial evidence that the oxygen cost of performing external cardiac work is less than that associated with the development of active tension. However, because of the complex geometry of the contracting heart, it has not been possible to measure the oxygen cost of shortening against a load and to directly compare it with that of tension development. In the present study, an isolated sup- ported heart preparation was utilized and left ventricular (LV) wall stress (a> was calculated with an analog computer using a thick-walled spherical model for the LV. Isotonic contractions were produced by rapidly altering LV volume to maintain a constant level of wall c during each beat. In seven experiments myocardial oxygen consumption (Mvo,) during isovolumic con- tractions was compared to Mqoz during isotonic contractions at matched levels of peak LV wall CT ranging from 14.8 to 105.3 g/cm2. MVoz during isotonic contractions averaged 48.3 =t 3.4 (SEM) pi/beat per 100 g LV and was increased to an average of 52.1 & 3.9 pi/beat per 100 g LV during isotonic contractions at comparable levels of wall C. The increment in MVo2 above that associated with tension development was 5.9 =t 1.1 y0 of the total MVo2, and there was a significant positive correlation between this increment in Mvo2 and the external work performed. When this relationship is extrapolated to the intact heart performing higher levels of external work and shortening to a greater extent, external work might comprise an average of as much as 17 y0 and explain the relatively low oxygen cost of augmenting stroke work by increasing stroke volume. external work; cardiac energy utilization; wall force; tension- generation work IN 1915, EVANS AND MATSUOKA (11) first demonstrated that there was a larger increment in myocardial oxygen con- sumption (MVo2) observed when external cardiac work was increased by increasing arterial pressure than when it was increased by increasing cardiac output, and this ob- servation has been substantiated by other investigators utilizing different techniques (10, 16, 2 1, 29, 30). In 1923, Fenn (12) demonstrated that there is an increment in energy utilization above that associated with the maintenance of tension that is related to the amount of work performed. These observations, which were the subject of a recent review (19), were obtained in skeletal muscle. These ob- servations have been confirmed in isolated cardiac muscle by altering end-diastolic length and examining isotonic and isovolumic contractions at the same level of tension generation (5, 6). However, other investigators have failed to show a significant correlation between external work and oxygen consumption in in vivo skeletal (28) or isolated cardiac muscle (31) where initial length was held constant as in Fenn’s (12) experiments. Although the conclusions of Evans and Matsuoka (11) in the intact heart have been repeatedly confirmed, attempts to define a single quantitative relationship between external work alone and oxygen consumption under a variety of circumstances in which aortic pressure and contractile state are varied, have not been successful (2, 14, 24, 27). In the intact circulation it is difficult to examine the role of external work without simultaneously inducing changes in the relative amounts of tension-generation work or vol- ume work or without reflex adjustments in the contractile state. Accordingly, in the present study, to determine if there is a portion of total MVoz that could be attributed only to external work in the intact heart, an isolated heart preparation was devised in which MVoz could be compared in isovolumic and isotonic contractions at the same level of inotropic state that generated the same degree of active wall stress (a> and differed only in the the amount of external work performed. METHODS The experimental preparation, which has been described in detail previously (7), employed a computer regulated servo system to control wall G during systole. However, in the current study, instead of utilizing total cardiopulmonary bypass, an isolated supported heart preparation was em- ployed (Fig. 1). H earts were obtained from seven mongrel dogs weighing from 15.9 to 22.7 kg. Both the support dog and the heart-donor dog were anesthetized with 25-30 mg/kg of sodium pentobarbital. The heart was exposed through a midsternal incision and ligatures were placed around the superior and inferior venae cavae and the azygos vein. Heparin was then administered (3 mg/kg), the heart rapidly excised, and immediately placed in an iced-saline bath (0 C). With the heart in the iced bath, the left and right coronary arteries were isolated and a 1.5-cm diameter nylon plug was tied in place at the level of the aortic valve just below the coronary ostia (Fig. 1). The mitral valve and chordae tendineae were excised and a purse-string suture was placed around the mitral annulus at the base of the left atrium. The main pulmonary artery was ligated and the heart was removed from the ice bath and suspended over a large collection funnel. A reservoir connected by 1491 by 10.220.32.246 on April 3, 2017 http://ajplegacy.physiology.org/ Downloaded from
Transcript of Myocardial oxygen consumption during isotonic and ... · thick-walled spherical model for the LV....

AMERICAN JOURNAL OF PHYSIOLOGY Vol. 223, No. 6, December 1972. Printed zn U.S.A.
Myocardial oxygen consumption during isotonic and
isovolumic contractions in the intact heart
JOHN W. BURNS AND JAMES W. COVELL University of California, San Diego, School of Medicine, Department of Medicine, La Jolla, California 92037
BURNS, JOHN W., AND JAMES W. COVELL. Myocardial oxygen consumption during isotonic and isovolumic contractions in the intact heart. Am. J. Physiol. 223(6): 1491-1497. 1972.-There is now sub- stantial evidence that the oxygen cost of performing external cardiac work is less than that associated with the development of active tension. However, because of the complex geometry of the contracting heart, it has not been possible to measure the oxygen cost of shortening against a load and to directly compare it with that of tension development. In the present study, an isolated sup- ported heart preparation was utilized and left ventricular (LV) wall stress (a> was calculated with an analog computer using a thick-walled spherical model for the LV. Isotonic contractions were produced by rapidly altering LV volume to maintain a constant level of wall c during each beat. In seven experiments myocardial oxygen consumption (Mvo,) during isovolumic con- tractions was compared to Mqoz during isotonic contractions at matched levels of peak LV wall CT ranging from 14.8 to 105.3 g/cm2. MVoz during isotonic contractions averaged 48.3 =t 3.4 (SEM) pi/beat per 100 g LV and was increased to an average of 52.1 & 3.9 pi/beat per 100 g LV during isotonic contractions at comparable levels of wall C. The increment in MVo2 above that associated with tension development was 5.9 =t 1.1 y0 of the total MVo2, and there was a significant positive correlation between this increment in Mvo2 and the external work performed. When this relationship is extrapolated to the intact heart performing higher levels of external work and shortening to a greater extent, external work might comprise an average of as much as 17 y0 and explain the relatively low oxygen cost of augmenting stroke work by increasing stroke volume.
external work; cardiac energy utilization; wall force; tension- generation work
IN 1915, EVANS AND MATSUOKA (11) first demonstrated that
there was a larger increment in myocardial oxygen con- sumption (MVo2) observed when external cardiac work was increased by increasing arterial pressure than when it was increased by increasing cardiac output, and this ob- servation has been substantiated by other investigators utilizing different techniques (10, 16, 2 1, 29, 30). In 1923, Fenn (12) demonstrated that there is an increment in energy utilization above that associated with the maintenance of tension that is related to the amount of work performed. These observations, which were the subject of a recent review (19), were obtained in skeletal muscle. These ob- servations have been confirmed in isolated cardiac muscle by altering end-diastolic length and examining isotonic and isovolumic contractions at the same level of tension
generation (5, 6). However, other investigators have failed to show a significant correlation between external work and oxygen consumption in in vivo skeletal (28) or isolated cardiac muscle (31) where initial length was held constant as in Fenn’s (12) experiments.
Although the conclusions of Evans and Matsuoka (11) in the intact heart have been repeatedly confirmed, attempts to define a single quantitative relationship between external work alone and oxygen consumption under a variety of circumstances in which aortic pressure and contractile state are varied, have not been successful (2, 14, 24, 27). In the intact circulation it is difficult to examine the role of external work without simultaneously inducing changes in the relative amounts of tension-generation work or vol- ume work or without reflex adjustments in the contractile state. Accordingly, in the present study, to determine if there is a portion of total MVoz that could be attributed only to external work in the intact heart, an isolated heart preparation was devised in which MVoz could be compared in isovolumic and isotonic contractions at the same level of inotropic state that generated the same degree of active wall stress (a> and differed only in the the amount of external work performed.
METHODS
The experimental preparation, which has been described in detail previously (7), employed a computer regulated servo system to control wall G during systole. However, in the current study, instead of utilizing total cardiopulmonary bypass, an isolated supported heart preparation was em- ployed (Fig. 1). H earts were obtained from seven mongrel dogs weighing from 15.9 to 22.7 kg. Both the support dog and the heart-donor dog were anesthetized with 25-30 mg/kg of sodium pentobarbital. The heart was exposed through a midsternal incision and ligatures were placed around the superior and inferior venae cavae and the azygos vein. Heparin was then administered (3 mg/kg), the heart rapidly excised, and immediately placed in an iced-saline bath (0 C). With the heart in the iced bath, the left and right coronary arteries were isolated and a 1.5-cm diameter nylon plug was tied in place at the level of the aortic valve just below the coronary ostia (Fig. 1). The mitral valve and chordae tendineae were excised and a purse-string suture was placed around the mitral annulus at the base of the left atrium. The main pulmonary artery was ligated and the heart was removed from the ice bath and suspended over a large collection funnel. A reservoir connected by
1491
by 10.220.32.246 on April 3, 2017
http://ajplegacy.physiology.org/D
ownloaded from

1492 J. W. BURNS AND J. W. COVELL
Tom, , 0 Err. /\ I
L L.V. Pressure \ __-*’ /
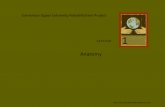
FIG. 1. Schematic diagram of preparation. Temp = temperature probe; Stim = stimulating electrodes attached to the right atrium; LCA = left coronary artery; LV = left ventricular; SM = servo-
motor; LVDT = linear variable differential transformer used to
sense position of plunger and thereby volume in left ventricle and piston-plunger system. This signal (vol) along with left ventricular pressure (LV Pressure) is used to calculate wall Q.
tubing to the ascending aorta maintained coronary per- fusion pressure (by gravity) at a constant level (100 mm Hg) and temperature was controlled at 36 C by a heat exchanger placed between the blood reservoir and the heart. The entire procedure from excision of the heart to reperfusion required a maximum of 45 min. The perfusion reservoir was initially primed with blood obtained by exsan- guination from dogs anesthetized with sodium thiamylal
(30 =%/kg) d an was replenished by pumping arterial blood from the support dog’s femoral artery. The support dog blood pressure was monitored and remained above 100 mm Hg in all animals without volume replacement or other means of support. Coronary venous blood flow was drained through a cannula in the right atrium and right ventricle (Fig. l), the drainage being filtered and returned to the support dog via a cannula in the external jugular vein.
A latex balloon containing a micromanometer (Konigs- berg model P20) was then placed in the left ventricle (LV) and secured to a 1.7 cm id glass cannula that was tied into the mitral annulus. Drainage of LV arterioluminal flow was accomplished by a cannula with multiple side holes placed through the apex between the balloon and the LV wall. Heart rate was maintained constant by crushing the sinus node and pacing the atrium with an electronic stimu- lator (A.E.L., model 104A). Coronary blood flow was de- termined by timed collection of the right atria1 and ven- tricular outflow, and MVoz was calculated as the product of the coronary arteriovenous blood oxygen difference ob- tained by Van Slyke analysis (22) and coronary blood flow. The reproducibility of this technique in our laboratory has been previously described (7). MVoz was expressed as microliters per beat per 100 g LV. The LV volume was con- trolled by a high-speed servomotor connected to the mitral cannula through a piston and cylinder arrangement (Fig. 1). The position of the piston and thereby the volume in the LV was sensed by a linear variable differential transformer (LVDT). The voltage signals proportional to LV pressure and LV volume were connected to an analog computer for the on-line calculation of wall g from the equation:
PRr2 c
= Ro2 - RI2
where P = intraventricular pressure in grams per square centimeter, Rr = internal left ventricular radius, R9 = external left ventricular radius. This equation assumes a geometric model for the LV (a thick-walled sphere). Recent studies from this laboratory (3) have shown that this rela- tionship tends to underestimate peak wall G (avg 19 YG) over the range of end-diastolic pressure (EDP) employed in the present experiment (6.0-10.0 mm Hg). However, this error was relatively constant, averaging 18.4 % at an LVEDP of 3.0 zt 0.6 (SEM) and 19.5 % at an average LVEDP of 6.4 & 0.8 (3). The analog computer contin- uously compared calculated G with a preset G control level. When calculated 0 exceeded the preset control level the servomotor was activated by a 0 error signal to withdraw volume from the LV at a sufficient rate to achieve wall G control at the desired level.
Experimental protocol. The experimental protocol was simi- lar in all experiments. Following calibration of the comput- ing system, the LV end-diastolic volume was varied by adjusting the volume within the balloon to change LVEDP from approximately 2 mm Hg to that necessary to produce an LVEDP of 15 mm Hg while the ventricle was beating isovolumetrically. This sequence was repeated, and the preparation was considered to be stable as soon as two suc- cessive curves relating end-diastolic volume (EDV) to peak developed pressure revealed peak pressures within 5 mm Hg for a given EDV. MJYo2 was then compared during steady- state conditions with the heart contracting both isovolu- mically and isotonically. By increasing end-diastolic volume slightly during the isotonic contractions, peak wall stress could be maintained at the same level as that in the iso- volumic contraction. In these experiments LVEDP was not increased above 10 mm Hg. The matched pairs of beats analyzed at the same level of active wall 0 of necessity oc- curred at different end-diastolic volumes (the isovolumic beats originating at a lower diastolic volume), and the iso- tonic beats exhibited varying amounts of shortening and therefore external work. With these data a relationship between the increment in MVo2 above that necessary for tension development and external work could be deter- mined at various levels of external work.
Calculations and data analysis. During an individual experi- ment, LV muscle volume was estimated from the average relationship between body weight and muscle volume for the purpose of on-line calculation of wall g (7). LV pressure, LV volume, and the rate of change of volume were recorded on magnetic tape (Honeywell model 7600). Following the experiment these data were replayed, A/D converted, and analyzed utilizing an Electronic Associates, Inc., model 590 hybrid computing system. Wall 0 and extent of short- ening, assuming the ventricle to be a thick-walled sphere, were then calculated using LV pressure, and the LV volume determined from the amount in the balloon. LV muscle volume for these calculations was obtained by weighing the LV. The external work performed by the ventricle was calculated as the product of midwall circumferential short- ening and average wall u during systole.
To compare the relative energy cost of “internal” and “external” work performed by the ventricular muscle a model for myocardial contraction was assumed. In this case a simple two-component model for contraction was
by 10.220.32.246 on April 3, 2017
http://ajplegacy.physiology.org/D
ownloaded from

MVo, IN ISOTONIC CONTRACTIONS 1493a
utilized (17). Ig noring shape changes occurring during runs. All comparisons of matched data were statistically isovolumic contraction, the rate of contractile element analyzed by the paired t test (25). shortening was estimated from the stiffness of the series elastic element (9, 26), and the calculated rate of change in RESULTS tension and contractile element external work was calcu- lated as the integral of the product of contractile element Table 1 contains data from seven studies in which myo- (CE) velocity and instantaneous pressure (contractile ele- cardial oxygen consumption was measured during iso- ment power). External work and internal work were utilized volumic and isotonic contractions at similar levels of wall to compare the relative efficiencies of oxygen utilization in U. Figure 2 illustrates typical oscillographic recordings taken isovolumic and isotonic contractions. from one of these studies. Panel A shows an isovolumic con-
In order to ascertain that changes in the contractile state traction at a volume of 31.2 ml in which the MVoa was of the isolated supported heart due to neurohumoral altera- 65.0 I-cl/beat per 100 g LV. Panel B is a succeeding isovolu- tions in the support dog did not occur during the experi- mic beat at an increased ventricular volume of 39.0 ml mental period, myocardial force-velocity relationships in with a concurrent increase in LV pressure and wall 0. In isovolumic contractions (14) were determined at the same level of end-diastolic volume prior to and following each determination of MVoz. Data were then selected for the comparison of isovolumic and isotonic oxygen consumption by two criteria: first, peak wall c in the isovolumic beat and wall CT in the matching isotonic beat were within 15 %; and second, V max estimated from the isovolumic contractions at comparable end-diastolic volumes determined just follow- ing the MVoz determination was within 10 % for the two
panel C, at the same end-diastolic volume as in panel B, O- was controlled at the same level as in panel A by withdrawing volume (7.25 ml) from the LV during contraction. In this contraction MVo2 averaged 71.5 pi/beat per 100 g LV. As shown in Table 1, in all studies the mean increase in end-diastolic volume from the isovolumic contraction (25.4 =t 3.2 ml) to the isotonic contraction (30.5 + 4.0 ml) was 5.1 ml. Pressure development in the isotonic contraction was slightly lower, averaging 73.5 & 3.9 mm Hg in the
TABLE 1. Myocardial oxygen cons24mbtion measured during zkovoZum~c and iSOiOniC contraction at similar levels of waZZ u L
3R, beats/mir
- -
1
.
Exp No. LV wt, g EDV, ml SV, ml Pk Press, mm Hg A L, cm Active u,
g/cm2 Ext Wk, Int Wk, Mbo2, J/beat
g/cm2 X cm g/cm2 X cm per 100 g LV . _ -
20-1 ISV 84.6 135 6.13 55.0 14.88 6.55 37.85 I IST 7.48 1.44 55.0 0.31 14.82 4.59 6.68 39.33 2 IST 16.43 4.26 60.0 0.60 30.10 18.06 15.09 47.93 2 ISV 12.53 85.0 28.60 13.79 43.19 3 IST 20.14 2.37 ‘77.0 0.30 48.72 14.62 25.25 48.52 3 ISV 17.41 81 .O 49.12 24.84 45.41
22-1 IST 82.8 126 22.24 3.04 60.0 0.35 33.78 11.82 16.20 35.95 I ISV 20.90 60.0 39.64 19.74 34.13
23-1 ISV 84.0 120 28.50 77.0 61.91 33.98 43.67 I IST 28.88 1.13 73.0 0.12 57.19 6.86 31.47 44.83
25-1 IST 98.1 144 26.49 5.82 47.0 0.62 25.06 15.54 13.92 44.58 I ISV 19.51 70.0 27.03 14.29 45.76
27-1 ISV 89.0 126 31.95 64.0 58.97 33.34 45 .oo I IST 44.44 7.62 57.0 0.61 57.81 35.26 34.83 50.00
28-1 IST 91.1 126 39.46 7.25 67.0 0.62 57.15 35.43 33.74 62.14 I ISV 35.53 69.0 57.92 33.51 57.22 2 IST 46.80 5.70 49.5 0.44 54.10 23.80 33.04 51.98 2 ISV 39.02 63.0 58.57 34.49 49.05
29-1 ISV 86.2 126 31.23 86.0 79.61 44.61 65 .OO I IST 39.02 7.25 80.9 0.63 78.22 49.28 45.73 71.51 2 ISV 36.69 98.0 105.33 60.83 70.63 2 IST 44.43 8.89 83.0 0.73 91.80 67 .Ol 55.08 76.27
Isovolumic Mean 88.0 129 .o 25.40 73.5 52.87 29.09 48.81 SE zt2 .o *3 .o rt3.24 zt3.9 zt7.71 zt4.68 zt3.35
Isotonic Mean 30.53 4.98 64.5 0.48 49.89 25.66 28.28 52.09 SE rt3.96 ztO.80 h3.8 &O .06 zt6.90 ziz5.82 jz4.40 zt3.85
- Exp No. = matched isovolumic (ISV) and isotonic (IST) pairs of contractions; LV wt = left ventricular weight; HR = heart rate;
EDV = end-diastolic volume; SV = stroke volume; Pk Press = peak left ventricular pressure; AL = extent of circumferential shortening; Active u = peak left ventricular stress minus end-diastolic stress; Ext Wk = external work; Int Wk = internal work (see text).
- 7
- - - - - -
by 10.220.32.246 on April 3, 2017
http://ajplegacy.physiology.org/D
ownloaded from

1494 J. W. BURNS AND . J. W. COVELL
WALL STRESS
52.8 Lo “OL”ME
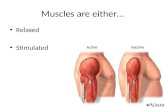
(ml 1 I -I_------ FIG. 2. Original recordings from an experiment showing wall
stress, left ventricular pressure (LVP) and left ventricular internal volume (LV Volume) at a low left ventricular end-diastolic volume (panel A), a higher volume (panel B), and during stress control at this higher volume (panel C). M’ijoz was determined during steady-state conditions represented by panels A and C.
isovolumic contraction and 64.5 =t 3.8 mm Hg in the iso- tonic contraction. Moreover, as shown in Fig. 2, there was a consistent fall in LVEDP at the same end-diastolic volume in the isotonically contracting ventricle. Thus, in all matched pairs LVEDP averaged 3.2 =t 0.8 mm Hg lower (range 2.0-7.0 mm Hg) in the isotonically contracting left ventricle when compared to the isovolumic contractions at the same end-diastolic volume. In all experiments the stroke volume was varied from 1.1 to 8.9 ml and the stroke volume-to-end-diastolic volume ratio averaged 16.6 rt 1.8 %.
Calculated peak active isovolumic 0 ranged from 14.9 to 105.3 g/cm2 and the comparable isotonic G control levels ranged from 14.8 to 91.8 g/cm2. During the isotonic con- tractions the extent of circumferential midwall fiber short- ening varied from 0.12 to 0.73 cm (0.8-4.5 Yo of end-diastolic midwall circumference), for an average of 0.48 & 0.06 cm of shortening.
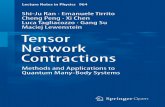
Examples of the difference in MTjo2 determined from matched pairs of contractions in two different experimental animals are shown in Fig. 3. In these two experiments, at every level of wall CT MVo2 in the isotonic beat was greater than that in the corresponding isovolumic beat at the same peak wall u values. For all but 1 of the 11 matched pairs, MVo2 from isotonic beats was significantly greater than MVo2 from isovolumic beats at comparable CT levels (P < .005, Table 1). The relation between the difference of MVo2 in isotonic and isovolumic beats (A MVoJ and external work is shown in Fig. 4. The points above the zero line represent data from matched pairs in which the MVo2 from the isotonic beat was greater than MVO~ from the corre- sponding isovolumic beat. The data has a correlation coefficient of .76 and the least-squares linear regression equa- tion was: MVO2 = .09 external work + .94. Moreover, the slope of the relationship between external work and A MVO2 was positive and this slope was significantly different from zero (P < .005), indicating that A MVO2 increased
80
70
30
ISOTONIC ISOVOL
# 20 0 a
# 29 A A
UMIC
20 40 60 80 100 120
FIG. 3. Relationship between MJ?02 and active wall stress in isovolumic and isotonic contractions in two experiments developing similar levels of wall stress.
8
0
8 0
MtiO, = .09 Ext. wk. + .94
OO 0
r = .76 PK.005
0
t I I I I I I I 1
0 10 20 30 40 pm, 60 7o 8o
EXTERNAL WORK
FIG. 4. Relationship between external work and the difference in MVo, between isotonic and isovolumic contractions developing the same levels of peak stress (Ab’lvo,). r = Correlation coefficient. Slope of this relationship is significantly different from zero (P < .005).
with the amount of external work performed. The intercept in this relationship (.94 ml/beat per 100 g LV) was not significantly different from zero, thus suggesting that basal oxygen consumption in these two types of contractions was similar, since contractile state and heart rate were similar in the isotonic and isovolumic contractions.
If one assumes a fixed stiffness for the series elastic element and a two-component model, it is possible to calculate the extent of contractile element shortening (equal to the series elastic elongation), during an isovolumic contraction (2, 14). The extent of contractile element shortening can then be used to calculate the internal work performed in generating tension. Thus, for each determination of MVO2, either iso- tonic or isovolumic, an amount of external and/or internal
by 10.220.32.246 on April 3, 2017
http://ajplegacy.physiology.org/D
ownloaded from

Mvoz IN ISOTONIC CONTRACTIONS
work could be calculated. In the isovolumic contraction, the amount of external work performed is assumed to be zero (ignoring possible shape changes). Utilizing data from seven experiments (all pairs of data, Table l), an average rela- tionship between MVo 2, internal work, and external work was determined using a multivariant regression analysis technique. was MVo2
The average relationship for all experiments = 3 1.2 + .19 external work + .57 internal
work, where 31.2 in the linear regression equation would represent the remaining determinants of oxygen consump- tion such as contractile state and basal oxygen consump- tion (14).
DISCUSSION
The results of the current study clearly indicate that when the level of peak stress generation is maintained con- stant, there is an increment in oxygen consumption as- sociated with performing external work. Moreover, there was a significant positive relationship between the level of external work performed and the amount of oxygen con- sumption required above that necessary for generation of tension. In the present study this additional increment in oxygen consumption averaged 5.9 & 1.1 % of the total oxygen consumption in isotonic contractions. These hearts were developing an average peak isovolumic LV pressure of 74 mm Hg at an LVEDP of 6-10 mm Hg and the amount of external work done in this isolated supported heart preparation was considerably lower than that usually encountered in the intact circulation. Thus the extrapola- tion of these data to a more intact preparation capable of developing more pressure and shortening to a greater ex- tent is hazardous. However, in order to evaluate the distribu- tion of myocardial oxygen consumption in a more intact preparation, an average relationship which expressed the portion of MVo2 that could be attributed to external and internal work as a percentage of total oxygen consumption was calculated using a multivariant linear regression tech- nique. These average values were then applied to distribu- tion of MVo2 in a single contraction from an intact ejecting left ventricle utilizing a right heart bypass preparation ( 15). In this preparation the circulation is essentially intact. The left ventricle ejects normally into the aorta and the average SV/EDV (ejection fraction) is similar to that observed clinically (4). Of the total MVo2 in this example 48.1% (90.2 pi/beat p er 100 g LV) could be related to internal or pressure-generation work, 17.5 to external work, and 34.4 % was associated with other factors such as contractile state and basal MVo2 . The proportion of MVo2 related to basal fac- tors, contractile state, and tension development is similar to that observed previously ( 14). In many previous studies, even in isolated muscle preparations it has been difficult to specifically determine whether the increment in energy ex- penditure associated with performing external work can be related to shortening against a load or to shortening alone ( 13). Moreover, Mommaerts has recently made a critical summary of the shortening heat controversy and has argued that shortening should be accompanied by a waste heat be- cause this process cannot be carried out with unit enthalpy efficiency. In the final analysis the energy requirements must be related to the turnover of cross-links between actin
1495
and myosin and in this sense the distinction between tension generation and shortening may be artificial. However, in the intact heart it is clear that the efficiency of augmenting cardiac work by increasing tension generation and by aug- menting shortening is different, and this study has provided the first direct evidence that the oxygen cost associated with performing external work is related to the amount of work performed and is substantially less than the oxygen cost associated with the generation of tension.
Several factors, all the result of the preparation and ex- perimental design, could have influenced the augmentation of MVo2 in the isotonic contraction. First, in order to pro- duce an isotonic contraction having a level of peak wall c equivalent to that in an isovolumic beat, it was necessary to increase end-diastolic volume. Although augmentation of resting tension has been shown to significantly increase high-energy phosphate utilization (23), no augmentation of resting oxygen consumption with increases in muscle length has been observed in the intact heart or papillary muscle (13, 2 1). Moreover, in the present study the dif- ferences in end-diastolic volume were small, and in the isotonic contraction ventricular volume decreased during contraction, continuously reducing the length difference during contraction. As might be anticipated from the shape of the resting and active length-tension curves in the intact heart, the relationship between the increment in end-dia- stolic volume necessary to match peak left ventricular tensions and increment in oxygen consumption associated with shortening at this slightly higher end-diastolic volume, was not statistically different (correlation coefficient = 26; probability of a nonzero correlation = .54), while the correlation of A MVo2 with external work was significant. Thus, it is not likely that in the present study the augmenta- tion of end-diastolic volume significantly influenced the results. Secondly, since Monroe (20) has shown that 90 % of the oxygen consumption is determined by the time peak 0 is reached, it is quite likely that matching peak wall c in the isovolumic contraction to the c developed by the iso- tonic contraction is the most appropriate way to compare the relative energy utilization. However, since the altera- tions in oxygen consumption observed were small and since previous studies have clearly shown that under certain circumstances oxygen consumption is directly related to tension or pressure area (24), several contractions were examined in which isovolumic wall 0 was greater than peak isotonic wall 0 and the area under the tension curve in the two contractions was similar. For example, in Fig. 5, the 0 area (expressed in g/cm2 X set) was slightly larger in the isovolumic contraction. However, MVo2 was 9.7 pi/beat greater in the isotonic contraction despite the fact that peak wall g was significantly less. Thus, in this par- ticular example, it is apparent that the amount of external work performed (in this case 25.1 g/cm per cm2) was suffi- cient to exceed the influence of both tension area and the difference in peak wall 0 in the two contractions. It also is possible that the geometric model used to calculate wall c influenced the comparison between isovolumic and isotonic contractions. However, recent studies (3, 18) have shown that there is relatively good agreement between different methods of calculating wall C, and the correlation between- directly measured wall 0 and that calculated using a spheri- r
by 10.220.32.246 on April 3, 2017
http://ajplegacy.physiology.org/D
ownloaded from

1496
90 L.V. WALL STRESS
(gm/cm2)
L.V. I , 1 ) : +
VOLUME ’ I I I’ -! 1
(ml) f I f 4 ’ I 1 I
. _ i I I
Peok stress (gm /cm2) 64.4 47.8 Stress oreo(gm se&m21 7.0 6.2 Ext wk (gm cm/cd) 0.0 25.1 M\j0~(~i/beat1100gm L.Lc) 53.6 63.3
. , . . : 1
_- -1 . . _ . -- !
! , . I : . _ _ 1
1
~
__ .
. .
1 t---
FIG. 5. Oscillographic recordings from 2 contractions at slightly different left ventricular volumes in which stress area was greater in . isovolumic contraction but MVo2 was higher in ejecting contraction .
cal model is good. Errors in this model tend to underesti- mate wall c at higher volumes (3), a factor that would tend to increase the amount of external work performed in the present study. Moreover, since ejected volume was usually low, it is unlikely that large errors due to shape change were introduced in comparing isovolumic and isotonic beats in the same heart, although it is certainly possible that shape changes and changes in fiber orientation may have influenced the results. These alterations in shape and changes in fiber orientation could also be expected to in- fluence the extrapolation of these data to higher levels of left ventricular work where the alterations in ventricular shape during isovolumic and isotonic contractions might well be different. Thus, as discussed previously, the extrapo- lation of these data would clearly depend on the validity of these assumptions and of the validity of the calculations for average work.
It is interesting that a fall in LVEDP was observed dur- ing volume withdrawal. The factors responsible for this ap- parent decrease in the diastolic pressure-volume relation-
REFERENCES
1. BRADY, A. J. Time and displacement dependence of cardiac con- tractility: problems in defining the active state and force velocity relations. Federation Proc. 24: 1410-1420, 1965.
' BRITMAN, N. A., AND H. J. LEVINE. Contractile element work: a major determinant of myocardial oxygen consumption. J. Clin. Invest. 43 : 1397-1408, 1964.
3. BURNS, J. W., J. W. COVELL, R. MYERS, AND J. Ross, JR. A comparison of directly measured left ventricular wall stress and stress calculated from geometric reference figures. Circulation Res. 28: 611-621, 1971. ,
4. CHAPMAN, C. B., 0. BAKER, AND J. G. MITCHELL. Left ventricular function at rest and during exercise. J. Clin. Invest. 38: 1202-l 2 13, 1959.
5. COLEMAN, H. N. Effect of alterations in shortening and external work on oxygen consumption of cat papillary muscle. Am. J. Physiol. 214: 100-106, 1968.
6. COLEMAN, H.N., E. H. SONNENBLICK, AND E. BRAUNWALD. Myo- cardial oxygen consumption associated with external work: the Fenn effect. Am. J. Physiol. 217: 291-296, 1969.
7. COVELL, J. W., E. BRAUNWALD, J. Ross JR., AND E. H. SONNEN- BLICK. Studies on digitalis. XVI. Effects on myocardial oxygen consumption. J. CZin. Invest. 45: 1535-1545, 1966.
8. COVELL, J. W.,J. S. FUHRER, R. C. BOERTH, AND J. Ross, JR.
J. W. BURNS AND J. W. COVELL
ship are not clear. However, rapid systolic changes in length during contraction have been shown to produce changes in peak isovolumic tension development (1) beyond that proportional to the increase in length alone (and in proportion to the time and rate of stretch), and it is possible that these essentially viscous changes may also be responsi- ble for alterations in the diastolic pressure-volume relation- ship during the control cycle. However, since intracavity volume was directly measured in the present studies and the changes in pressure were small (3.2 & 0.8 mm Hg) it is unlikely that these changes significantly influenced the results.
In summary, the present study has demonstrated a sig- nificant relationship between the amount of external work performed in isotonic contractions and the increment in myocardial oxygen consumption above that required for tension generation. Accordingly, it is now possible to quantitatively add a fifth important determinant of myo- cardial oxygen consumption to those elucidated by earlier studies (14) : 1) basal oxygen consumption, which is neces- sary for maintenance of membranes, electrical activity, etc.; 2) oxygen consumption associated with tension de- velopment; 3) oxygen consumption associated with con- tractile state; 4) oxygen consumption related to variations in heart rate; and 5) oxygen consumption associated with external work.
The authors wish to acknowledge the excellent technical assistance of Mr. Richard S. Pavelec, Mr. Frank R. Trousdale, and Mr. Donald F. Rippon, and the editorial efforts of Mr. Charles E. Smith.
This paper was presented at the Federation of American Societies for Experimental Biology. Federation Proc. 29: 1150, 1970.
This study was supported by National Heart and Lung Institute Program Project Grant No. HE12373.
During the course of this work, J. W. Burns was a Postdoctoral Fellow of the National Heart and Lung Institute, Grant No. HE28547 His present address is Biodynamics Branch (VNB), United States Air Force School of Aerospace Medicine, Brooks Air Force Base, Texas 78235.
J. W. Cove11 is the recipient of National Heart and Lung Institute Career Development Award No. HE2 1132.
Received for publication 10 February 1972.
Production of isotonic contractions in the intact canine left ven- tricle. J. A$@. Physiol. 27: 577-581, 1969.
9. COVELL, J. W., R. R. TAYLOR, AND J. Ross, JR. Series elasticity in the intact left ventricle determined by a quick release technique. Federation Proc. 26: 382, 1967.
10. DECHERD, G., AND M. B. VISSCHER. The relative importance of the performance of work and the initial fiber length in determining the magnitude of energy liberation in the heart. Am. J. Physiol. 103: 400-406, 1933.
11. EVANS, C. L., AND Y. MATSUOKA. The effect of various mechanical conditions on the gaseous metabolism and efficiency of the mam-
malian heart. J. PhysioZ., London 49: 378-405, 1915. 12. FENN, W. 0. A quantitative comparison between the energy lib-
erated and the work performed by the isolated sartorius muscle of
the frog. J. Physiol., London 58: 1 K-203, 1923. 13. GIBBS, C. L., AND W. R. GIBSON. Energy production in cardiac
isotonic contractions. J. Gen. Physiol. 56: 732-750, 1970. 14. GRAHAM, T. P., JR., J. W. COVELL, E. H. SONNENBLICK, J. Ross,
JR.3 AND E. BRAUNWALD. Control of myocardial oxygen con- sumption: relative influence of contractile state and tension de- velopment. J. CZin. Invest. 47: 375-385, 1968.
15. GRAHAM, T. P., JR., J. Ross, JR., J. W. COVELL, E. H. SONNEN- BLICK, AND R. L. CLANCY. Myocardial oxygen consumption in
by 10.220.32.246 on April 3, 2017
http://ajplegacy.physiology.org/D
ownloaded from

Mvoz IN ISOTONIC CONTRACTIONS
acute experimental cardiac depression. Circulation Res. 2 1: 123- 138, 1967.
16. HEMINGWAY, A., AND A. R. FEE. The relationship between the volume of the heart and its oxygen usage. J. Physiol., London 63: 299-303, 1927.
17. HILL, A. V. The heat of shortening and the dynamic constants of muscle. Proc. Roy. Sot., London, Ser. B. 126: 136-l 95, 1938.
18. HOOD, W. P., JR., W. J. THOMPSON, C. E. RACKLEY, AND E. L. ROLETT. Comparison of calculations of left ventricular wall stress in man from thin-walled and thick-walled ellipsoidal models. Circulation Res. 24: 575-582, 1969.
19. MOMMAERTS, W. F. H. M. Energetics of muscular contraction. Physiol. Rev. 49: 427-508, 1969.
20. MONROE, R. G. Myocardial oxygen consumption during ven- tricular contraction and relaxation. Circulation Res. 14: 294-300, 1964.
21. MONROE, R. G., AND G. N. FRENCH. Left ventricular pressure- volume relationships and myocardial oxygen consumption in the isolated heart. Circulation Res. 9: 362-374, 1961.
22. PETERS, J. P., AND D. D. VAN SLYKE. Quantitative Clinical Chemistry. Baltimore: Williams & Wilkins, 1932, vol. 2, p. 32 1.
23. POOL, P. E., B. M. CHANDLER, S. C. SEAGREN, AND E. H. SON- NENBLICK. Mechano-chemistry of cardiac muscle. II. The isotonic contraction. Circulation Res. 22 : 465-472, 1968.
1497
24. SARNOFF, S. J., E. BRAUNWALD, G. H. WELCH, JR., R. B. CASE, W. N. STAINSBY, AND R. MACRUZ. Hemodynamic determinants of oxygen consumption of the heart with special reference to the tension-time index. Am. J. Physiol. 192: 148-156, 1958.
25. SNEDECOR, G. W., AND W. G. COCHRAN. Statistical Methods (6th ed.). Ames, Iowa: Iowa State Univ. Press, 1967.
26. SONNENBLICK, E. H. Series elastic and contractile elements in heart muscle: Changes in muscle length. Am. J. Physiol. 207: 1330-1338, 1964.
27. SONNENBLICK, E. H., J. Ross, JR., J. W. COVELL, G. A. KAISER, AND E. BRAUNWALD. Velocity of contraction as a determinant of myocardial oxygen consumption. Am. J. Physiol. 209: 919-927, 1965.
28. STAINSBY, W. M. Oxygen uptake for isotonic and isometric twitch contractions of dog skeletal muscle in situ. Am. J. Physiol. 219:
435-439, 1970. 29. STARLING, E. H., AND M. B. VISSCHER. The regulation of the
energy output of the heart. J. Physiol., London 62: 243-261, 1927. 30. TAYLOR, R. R., H. E. CINGOLANI, T. P. GRAHAM, JR., AND R. L.
CLANCY. Myocardial oxygen consumption, left ventricular fiber shortening and wall tension. Cardiovascular Res. 1: 2 19-228, 1967.
31. WHALEN, W. J. The relation of work and oxygen consumption in isolated strips of cat and rat myocardium. J. Physiol., London 157: 1-17, 1961.
by 10.220.32.246 on April 3, 2017
http://ajplegacy.physiology.org/D
ownloaded from