
Multi -parametric MRI in prostate cancer practice … internal structure and un -sharp margins 5...
28
Anwar Padhani Anwar Padhani [email protected] [email protected] Mount Vernon Cancer Centre Mount Vernon Cancer Centre London London Multi Multi - - parametric MRI in prostate parametric MRI in prostate cancer practice made easy cancer practice made easy
Transcript of Multi -parametric MRI in prostate cancer practice … internal structure and un -sharp margins 5...

Anwar PadhaniAnwar [email protected]@stricklandscanner.org.uk
Mount Vernon Cancer CentreMount Vernon Cancer Centre
LondonLondon
MultiMulti--parametric MRI in prostate parametric MRI in prostate
cancer practice made easycancer practice made easy

OutlineOutline
�� To briefly illustrate the expanded role of functional MRI techniTo briefly illustrate the expanded role of functional MRI techniques ques
in clinical practicein clinical practice
�� Diffusion weighted MRI (DWDiffusion weighted MRI (DW--MRI) MRI)
�� MR spectroscopic imaging (MR spectroscopic imaging (11HH--MRSI) MRSI)
�� Dynamic contrast enhanced MRI (DCEDynamic contrast enhanced MRI (DCE--MRI)MRI)
�� To demonstrate in practice how structured reporting using scorinTo demonstrate in practice how structured reporting using scoring g
schema can aid in communicating imaging findings back to schema can aid in communicating imaging findings back to
surgeons / oncologistssurgeons / oncologists
•Sciarra A, et al. Advances in magnetic resonance imaging: how they are changing the
management of prostate cancer. European Urology 2011; 59: 962-77
•Hoeks CM, et al. Prostate cancer: multiparametric MRI for detection, localization, and
staging. Radiology 2011; 261 – in press
•Padhani AR. Integrating multiparametric prostate MRI into clinical practice. Cancer Imaging
2011 - in press
IntroductionIntroduction
�� High field 3T MRI presents new exciting opportunities for promotHigh field 3T MRI presents new exciting opportunities for promoting ing
men's prostatic healthmen's prostatic health
�� Advanced MRI tools enable us to tackle new indications in the Advanced MRI tools enable us to tackle new indications in the
prostate cancer patients journeyprostate cancer patients journey
�� Raised PSA/PCa3 with negative TRUS biopsies Raised PSA/PCa3 with negative TRUS biopsies
�� Active surveillance patients Active surveillance patients –– enables appropriate patient selectionenables appropriate patient selection
�� Move into new areas of established disease Move into new areas of established disease
�� To identify poor prognosis tumours and guide focal therapies to To identify poor prognosis tumours and guide focal therapies to dominant dominant
intraprostatic lesionsintraprostatic lesions
�� Improved ability to tackle transition zone tumorsImproved ability to tackle transition zone tumors
�� Integration/ relative weighting/ communication of complex biologIntegration/ relative weighting/ communication of complex biological ical
information is a major bioinformatics challenge information is a major bioinformatics challenge

0++++++++++++0+++++++++++DCE-MRI
0+++++++++++++++++++++++DW-MRI
0++++++0+++++++++++MRSI
0++++++0000+0+MRI
biopsy
++++++++++++++++++++++++++++++++++Morphol
ogy
Contribution made by MRI techniques$
Define extent
of relapsed
disease and
complication
s (C)
Requirement
s for local
palliation (C)
Define
extent of
local
disease
and
absence
of
metastase
s (C)
Identify site
and volume
of recurrence
(C)
Detect active
disease in
absence of
significant
PSA rise (R)
Treatment
verification
(R)
Define
volume
and extent
of residual
disease (R)
Define
extent of
nodal &
distant
metastases
(C)
Requirement
s for local
palliation (C)
Confirm
confinement to
pelvis (C)
Nodal mapping
(C/R)
Define
dominant
lesion location
and size (C/R)
Detect
adverse
features (C)
Target pelvic
nodal
dissection (C)
Confirm
organ
confine
ment (C)
Docume
nt size
and
location(
C)
Depict
lesion
aggressi
veness
(C/R)
TNM
stage
(C)
Define
domina
nt
lesion
(C)
Define
lesion
aggressi
veness
(C/R)
Therapy
plannin
g (C)
Define
tumour
location and
size for
targeted
biopsy (C)
Clinical
(C) or
Research
(R)
require
ments
Disease is not
localised and
salvage is
impossible
Disease is
localised
and
salvage is
possible
Significant
rise in serum
PSA
Rare to use
imaging in
this role
(Serum PSA
surveillance)
Usually
after focal
therapies
Usually
hormonal
therapy ± RT
Usually
includes
neoadjuvant
hormonal
therapy
Organ confined
disease
No metastases
Organ
confinement
No tumour at
prostatic
apex
No
metastases
Small
volume
Low
aggressi
veness
Cancer
presenc
e
confirm
ed by
biopsy
Raised PSA
with negative
TRUS biopsy
or biopsies
Clinical
scenario
External beam
radiotherapy
to prostate ±
pelvic nodes
Ablative
therapies
(HIFU, PDT,
cryotherapy
brachytherapy)
Surgery
PalliativeLocal
salvage
PalliativeCurative intentInitial
observat
ion
(active
surveilla
nce)
→ Treatment of relapsed
disease
→
Suspect
relapse
→
Surveillance
of treated
disease
→
Monitoring
effectivene
ss of
therapy
→ Treatment of initial disease→
Stage
known
cancer
→ Suspect
cancer
Clinical
Journey
begins
here
Prostate cancer patient journey & contribution of MRI to careProstate cancer patient journey & contribution of MRI to care

Advanced MRI tools available for Advanced MRI tools available for
clinical practice clinical practice -- 20102010
Tool (abbreviation)Tool (abbreviation) Biological property depictedBiological property depicted
Diffusion MRI (DWI, Diffusion MRI (DWI,
DWDW--MRI)MRI)Extent of gland formation, cellular density, Extent of gland formation, cellular density,
necrosis and perfusionnecrosis and perfusion
Spectroscopy (MRSI)Spectroscopy (MRSI) Cell membrane turnover/energetics and Cell membrane turnover/energetics and
replacement of normal glandular tissuesreplacement of normal glandular tissues
Dynamic contrast Dynamic contrast
enhanced (DCEenhanced (DCE--MRI)MRI)Blood flow and vascular permeabilityBlood flow and vascular permeability

Prostate cancer Prostate cancer
localisation with dynamic localisation with dynamic
MRI and spectroscopy MRI and spectroscopy
Futterer, J. J. et al. Radiology 2006;
241:449-458
Peripheral zonePeripheral zone
Central GlandCentral Gland
MPKS = DCEMPKS = DCE--MRI scoreMRI score
T2W
MRSI
DCE-MRI
All

The multiparametric MRI challengeThe multiparametric MRI challenge
Pre RxPre Rx
Post antibioticsPost antibiotics
Post LHPost LH--RHaRHa
Post HIFUPost HIFU
T2WT2W b800b800 ADCADC DCEDCE--SubSub TumTum--MRSIMRSI PZPZ--MRSIMRSI Mean curveMean curve

Essential communication elementsEssential communication elements
�� Scoring systems that indicate likelihood of a Scoring systems that indicate likelihood of a
““significant cancersignificant cancer”” being presentbeing present
-- LikertLikert--like 5like 5--grade scoring systems*grade scoring systems*
» Score 1: clinically significant disease is highly unlikely to be present
» Score 2: clinically significant cancer is unlikely to be present
» Score 3: the presence of clinically significant cancer is equivocal
» Score 4: clinically significant cancer is likely to be present
» Score 5: clinically significant disease is highly likely to be present
�� Structured reporting using a graphical interfaceStructured reporting using a graphical interface
-- Matches prostate anatomyMatches prostate anatomy
*Dickinson L, et al. MRI for the detection, localisation, and characterisation of prostate cancer: recommendations from a European consensus meeting. Eur
Urol. 2011; 59:477-94
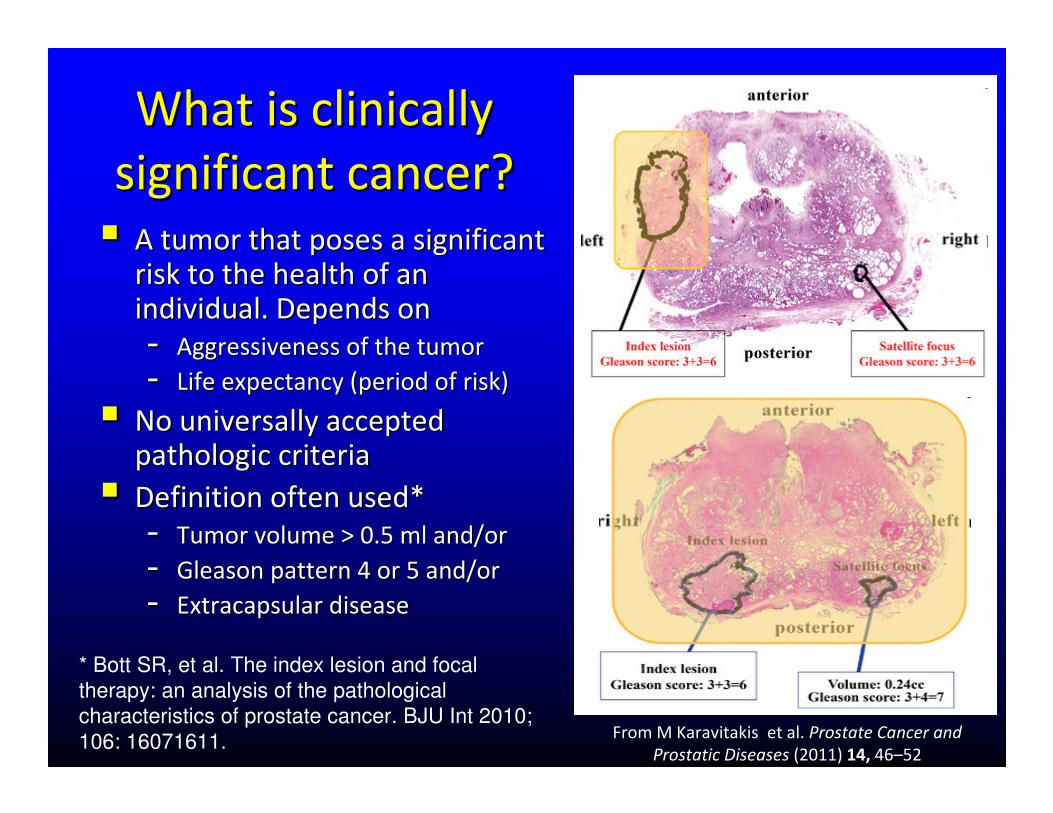
What is clinically What is clinically
significant cancer?significant cancer?
�� A tumor that poses a significant A tumor that poses a significant
risk to the health of an risk to the health of an
individual. Depends onindividual. Depends on
-- Aggressiveness of the tumorAggressiveness of the tumor
-- Life expectancy (period of risk)Life expectancy (period of risk)
�� No universally accepted No universally accepted pathologic criteriapathologic criteria
�� Definition often used* Definition often used*
-- Tumor volume > 0.5 ml and/or Tumor volume > 0.5 ml and/or
-- Gleason pattern 4 or 5 and/or Gleason pattern 4 or 5 and/or
-- ExtracapsularExtracapsular diseasedisease
* Bott SR, et al. The index lesion and focal
therapy: an analysis of the pathological
characteristics of prostate cancer. BJU Int 2010;
106: 16071611. From MFrom M KaravitakisKaravitakis et al. et al. Prostate Cancer and Prostate Cancer and
Prostatic DiseasesProstatic Diseases (2011) (2011) 14,14, 4646––5252
T2T2--weighted MRIweighted MRI
�� Excellent at depicting internal prostatic anatomyExcellent at depicting internal prostatic anatomy
�� Best for more advanced disease presentationsBest for more advanced disease presentations
�� Signal intensity of Signal intensity of tumorstumors appears to correlate with appears to correlate with
grade*grade*
�� Better at depicting dense cellular (dense) cancers Better at depicting dense cellular (dense) cancers
than sparse infiltrating disease**than sparse infiltrating disease**
* Wang L. et al. Radiology 2008; 246:168-176
** Langer DL, et al. Radiology 2008; 249:900-908

Score*Score* Peripheral zone appearancesPeripheral zone appearances illustrationsillustrations
1 1 -- clinically clinically
significant disease significant disease
is highly unlikely is highly unlikely
Normal PZ with uniform high signal intensityNormal PZ with uniform high signal intensity
2 2 –– clinically clinically
significant disease significant disease
is unlikely is unlikely
Linear, wedge shaped or geographic nonLinear, wedge shaped or geographic non--focal focal
areas of low SI, usually not well demarcatedareas of low SI, usually not well demarcated
3 3 -- indeterminate indeterminate Appearances not in categories 1/2 or 4/5Appearances not in categories 1/2 or 4/5
4 4 –– clinically clinically
significant disease significant disease
is likely is likely
Low signal (dark grayLow signal (dark gray--black) intensity focus/mass, black) intensity focus/mass,
well defined lesion confined to prostatewell defined lesion confined to prostate
5 5 –– clinically clinically
significant disease significant disease
is highly likely is highly likely
Low signal intensity mass, with invasive features Low signal intensity mass, with invasive features
including including extracapularextracapular or seminal vesicle invasion, or seminal vesicle invasion,
mass effect on capsule including bulgingmass effect on capsule including bulging
* Subtract 1 if significant haemorrhage in area of abnormality* Subtract 1 if significant haemorrhage in area of abnormality

Score*Score* Transition zone appearancesTransition zone appearances illustrationsillustrations
1 1 -- clinically clinically
significant disease is significant disease is
highly unlikely highly unlikely
TZ containing stromal & glandular TZ containing stromal & glandular
hyperplasia/adenoma with well defined margins. No hyperplasia/adenoma with well defined margins. No
low SI nodules or lenticular lesionslow SI nodules or lenticular lesions
2 2 –– clinically clinically
significant disease is significant disease is
unlikely unlikely
Round shaped low SI lesions with a smooth margins. Round shaped low SI lesions with a smooth margins.
Lenticular shaped, band like low SI in midline or around Lenticular shaped, band like low SI in midline or around
central adenomacentral adenoma
3 3 -- indeterminate indeterminate Appearances not in categories 1/2 or 4/5Appearances not in categories 1/2 or 4/5
4 4 –– clinically clinically
significant disease is significant disease is
likely likely
Lenticular shaped anterior low SI lesion without Lenticular shaped anterior low SI lesion without
capsule invasion.capsule invasion.
““charcoalcharcoal”” sign: homogeneous low SI lesion with loss sign: homogeneous low SI lesion with loss
of internal structure and unof internal structure and un--sharp marginssharp margins
5 5 –– clinically clinically
significant disease is significant disease is
highly likely highly likely
Lenticular or round mass with bulge / irregularity / Lenticular or round mass with bulge / irregularity /
retraction of the anterior prostate capsule.retraction of the anterior prostate capsule.
Irregular, infiltrating mass destroying TZ architecture, Irregular, infiltrating mass destroying TZ architecture,
invading adjacent PZ/SV/bladderinvading adjacent PZ/SV/bladder
* Subtract 1 if significant haemorrhage in area of abnormality* Subtract 1 if significant haemorrhage in area of abnormality

Limitations of T2Limitations of T2--weighted MRIweighted MRI
�� Tumour volume is underestimated and locations are not well Tumour volume is underestimated and locations are not well
depicteddepicted
–– Not all tumours are visibleNot all tumours are visible
–– Transition zone tumours not well seen (30% of cancers)Transition zone tumours not well seen (30% of cancers)
–– False positivesFalse positives: scars, BPH, prostatitis, hemorrhage & treatment : scars, BPH, prostatitis, hemorrhage & treatment
effectseffects
�� Restricted ability to distinguish localized (T2) from early T3 Restricted ability to distinguish localized (T2) from early T3
(advanced) disease(advanced) disease
→→ great staging variability (37great staging variability (37--96%)96%)
�� Important biologically characteristics are not well depictedImportant biologically characteristics are not well depicted
–– Tumour volume, location, histological grade, vascularisation, hyTumour volume, location, histological grade, vascularisation, hypoxia, poxia,
proliferation rate, proliferation rate, perineuralperineural invasion invasion

T2W b1000
ADC
T2W b1000
ADC
Park BK et al. Investigative Radiology
2007; 24:842-847
Qualitative assessmentQualitative assessment ––
hyperintensity in high bhyperintensity in high b--value imagesvalue images
Quantitative assessmentQuantitative assessment –– ADC valueADC value
DWDW--MRI pathological correlationsMRI pathological correlations
3T images

ADCs for tumors with different D’Amico clinical risk scores in the whole prostate
Turkbey B et al. Radiology 2011;258:488-495
©2011 by Radiological Society of North America
ADCs for tumors with different Gleason scores in the whole prostate

Distinguishing tumour from T2Distinguishing tumour from T2--shine throughshine through(look for hyperintensity on (look for hyperintensity on veryvery high bhigh b--value images)value images)
b0b0 b750tb750t
b900tb900t b1100tb1100t b1400tb1400t
ADC 0ADC 0--750t750t
For some moderate grade tumours it is necessary to have very higFor some moderate grade tumours it is necessary to have very high bh b--valuesvalues
Where is the tumour?Where is the tumour?

Scoring system for DWScoring system for DW--MRI (PZ)MRI (PZ)
TZ criteria to be decidedTZ criteria to be decided
ClassClass DescriptionDescription b1000b1000 ADCADC
1 1 -- clinically clinically
significant disease significant disease
is highly unlikely is highly unlikely
No reduction in ADC compared to normal
glandular tissue / no increase in signal on
high b-value images (≥b1000)
2 2 –– clinically clinically
significant disease significant disease
is unlikely is unlikely
Diffuse, hyperintensity on ≥b1000 image with
low ADC; No focal features - linear, triangular
or geographical features allowed
3 3 -- indeterminate indeterminate Diffuse unilateral hyperintensity on
≥b1000 image with diffuse low ADC (no
focal features)
4 4 –– clinically clinically
significant disease significant disease
is likely is likely
Focal area(s) of reduced ADC but
isointense SI on high b-value images
(≥b1000)
5 5 –– clinically clinically
significant disease significant disease
is highly likely is highly likely
Focal area/mass of hyperintensity on the
high b-value images (≥b1000) with
reduced ADC

CaCaCaCa
CaCa
CaCa
CaCa
CaCa
PINPIN
PINPIN
PINPIN
PINPIN
ROC curves show Az values for DCE-MRI (MPKS)
and MRS for localization of prostate tumors with
volumes of >0.5 cm3
Futterer JJ, et al. Radiology 2006;241:449-458
washout
kep – rate constant
Ktrans – transfer constant
ve – leakage space
Bloch BN, et al.Bloch BN, et al.
Radiology. 2007; Radiology. 2007;
245(1):176245(1):176--85.85.
N = 32
Validating DCEValidating DCE--MRI for prostate cancer MRI for prostate cancer
localisation and staginglocalisation and staging
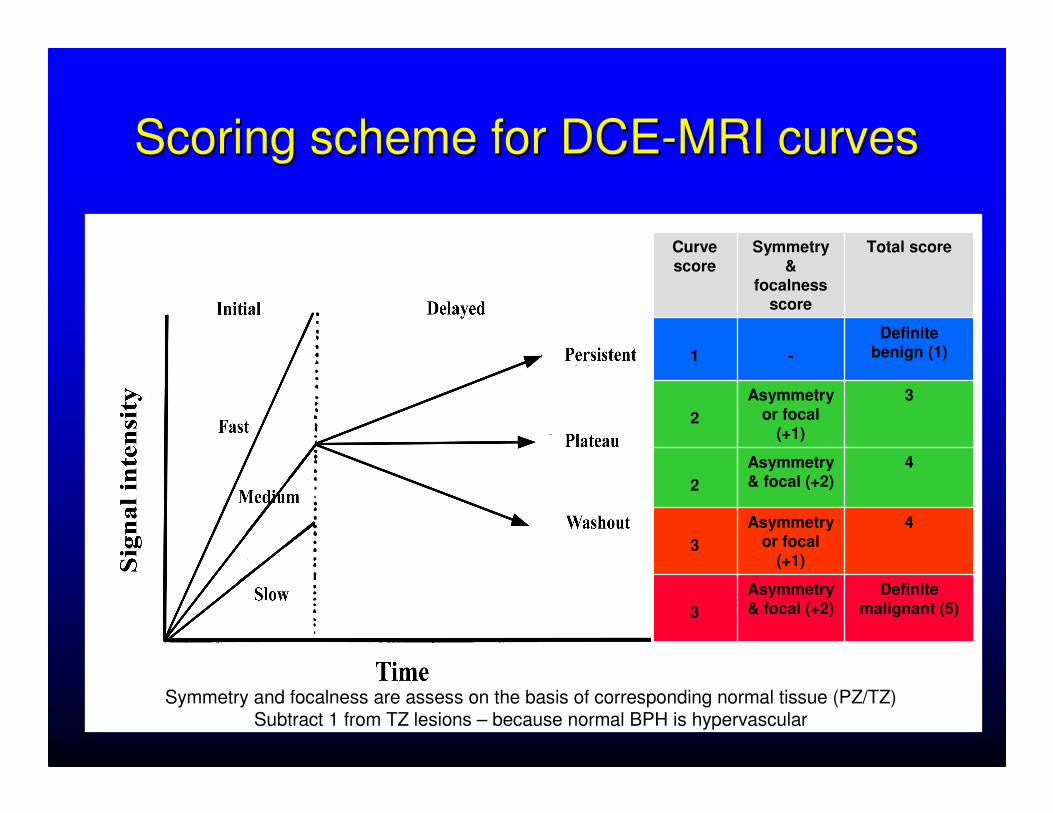
Scoring scheme for DCEScoring scheme for DCE--MRI curvesMRI curves
Symmetry and focalness are assess on the basis of corresponding normal tissue (PZ/TZ)Subtract 1 from TZ lesions – because normal BPH is hypervascular
Curve score
Symmetry &
focalnessscore
Total score
1 -
Definite benign (1)
2
Asymmetry or focal
(+1)
3
2
Asymmetry & focal (+2)
4
3
Asymmetry or focal
(+1)
4
3
Asymmetry & focal (+2)
Definite malignant (5)

Rising PSA Rising PSA ––negative biopsy x 2negative biopsy x 2
�� 56 56 yoyo raised serum PSA level raised serum PSA level and 2 negative TRUSand 2 negative TRUS�� 1/12 ICU following TRUS1/12 ICU following TRUS
�� 8 mm nodule in the left PZ with 8 mm nodule in the left PZ with washwash--out curve out curve
�� Low ADC values within the Low ADC values within the nodule. The lesion is not seen nodule. The lesion is not seen on the b900 image because of on the b900 image because of persistent high signal intensity persistent high signal intensity of the peripheral zone. of the peripheral zone.
�� ADC map does not depict all ADC map does not depict all intraprostatic lesions intraprostatic lesions –– misses misses the small, Gleason 6 tumour focithe small, Gleason 6 tumour foci
June
08
4/54/5
4/5
2/5
5/55/5
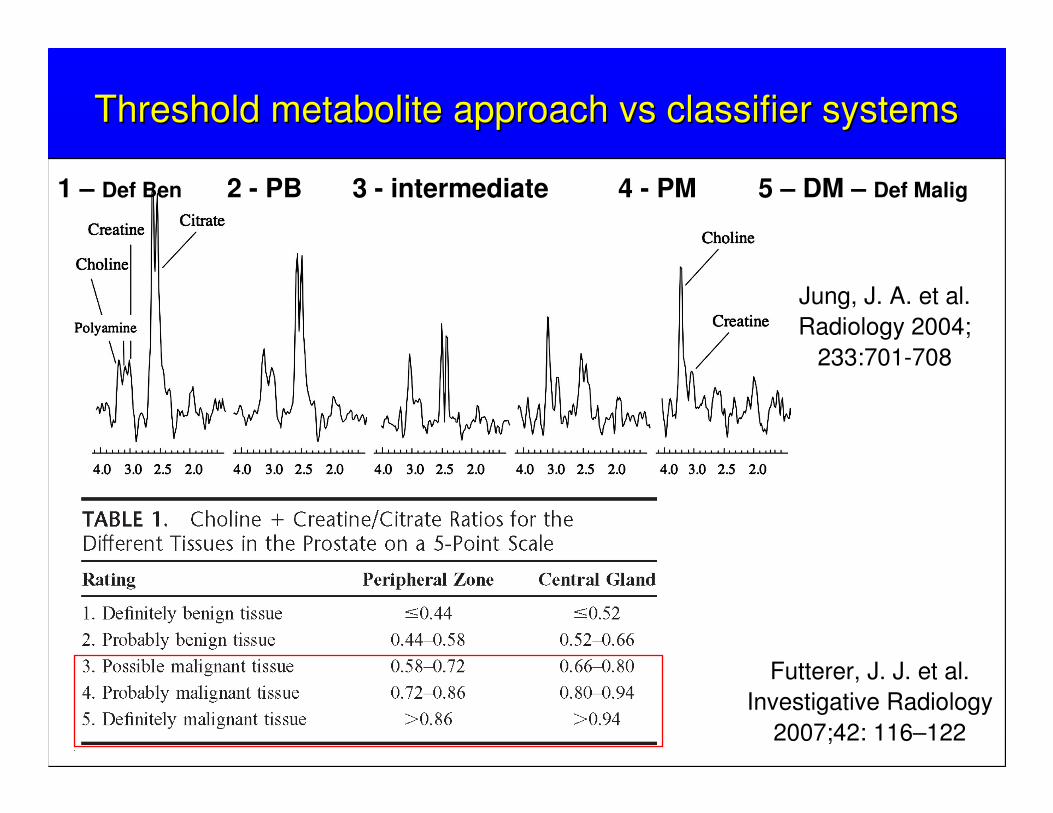
Threshold metabolite approach Threshold metabolite approach vsvs classifier systems classifier systems
Jung, J. A. et al. Jung, J. A. et al.
Radiology 2004; Radiology 2004;
233:701233:701--708708
Futterer, J. J. et al.
Investigative Radiology
2007;42: 116–122
1 – Def Ben 2 - PB 3 - intermediate 4 - PM 5 – DM – Def Malig
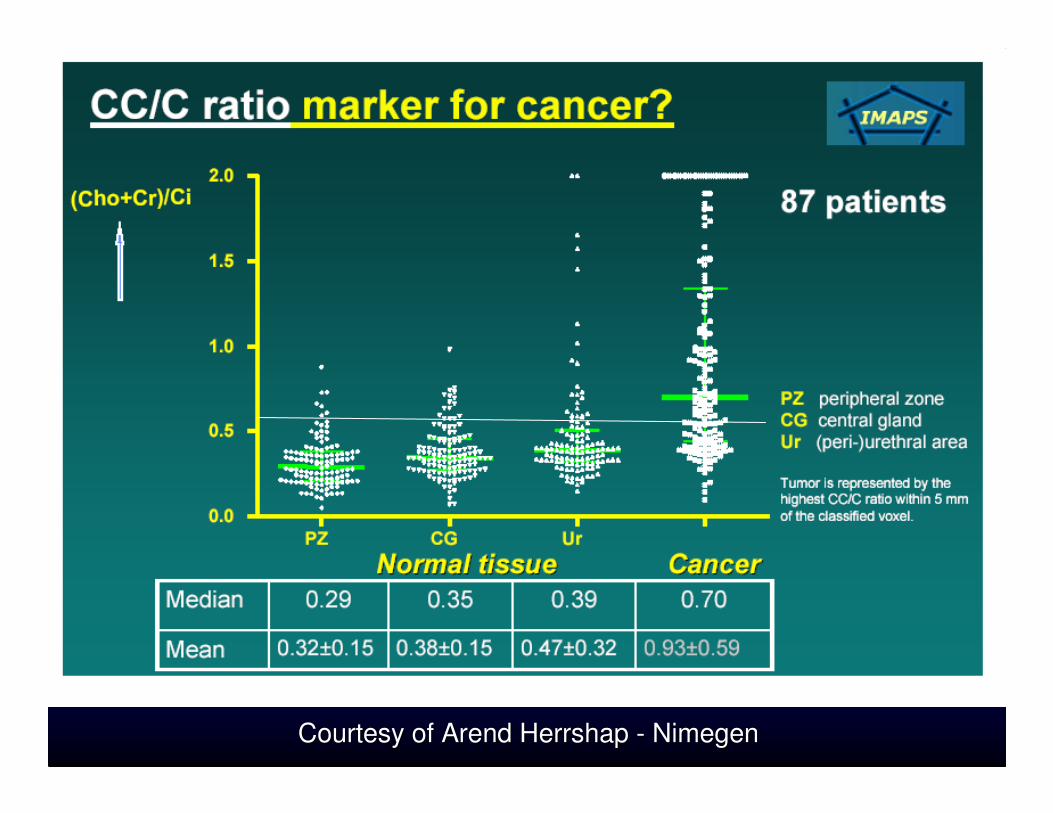
Overlap of Overlap of choline:citratecholine:citrate ratios ratios
between malignant and between malignant and
benign/normal tissuesbenign/normal tissues
IMAPS data IMAPS data –– ask ask ArendArend HershapHershap
Courtesy of Courtesy of ArendArend HerrshapHerrshap -- NimegenNimegen

Integration, reporting and Integration, reporting and
communicationcommunication�� Structured reporting method via graphical interface to match Structured reporting method via graphical interface to match
prostate anatomyprostate anatomy
�� AnteriorAnterior--posterior border 1.7cm from the rectal wall (average length posterior border 1.7cm from the rectal wall (average length
of core biopsy needle)of core biopsy needle)
�� Use sUse scoring system that indicates the likelihood of a coring system that indicates the likelihood of a
““significant cancersignificant cancer”” being presentbeing present
�� Assign scores per prostate/ sector/ lesion (max 5 lesions)Assign scores per prostate/ sector/ lesion (max 5 lesions)
�� Dominant cancer focus makes up to 90% of the cancer volume and Dominant cancer focus makes up to 90% of the cancer volume and
80% of small foci have tumour volumes < 0.5 ml80% of small foci have tumour volumes < 0.5 ml
�� Give a putative TNM stageGive a putative TNM stage
�� Take account of patient history and symptoms, serum PSA, Take account of patient history and symptoms, serum PSA,
DRE findings, concomitant medications (particularly antiDRE findings, concomitant medications (particularly anti--
androgens) and time since TRUS biopsyandrogens) and time since TRUS biopsy

Active surveillanceActive surveillance –– baseline (Dec 2008)baseline (Dec 2008)
PSA 5.3ng/ml; TRUS PSA 5.3ng/ml; TRUS -- small foci of Gleason 3+3 plus prostatitis in PZ; TRUS missed asmall foci of Gleason 3+3 plus prostatitis in PZ; TRUS missed anterior gland tumor (ADC 835 nterior gland tumor (ADC 835 µµmm22/s)/s)
TRUS biopsy only = Gleason 3+3 on left side with prostatitisTRUS biopsy only = Gleason 3+3 on left side with prostatitis
PZ: T2W =3/5; DWI =2/5
DCE = 3/5; MRSI =1/5
Ant TZT2W =2/5; DWI =4/5
DCE =5/5; MRSI =1/5

Active surveillance Active surveillance –– post antibiotics (Dec 2009)post antibiotics (Dec 2009)
PSA 5.8ng/ml; enlarging anterior gland tumor (ADC 835PSA 5.8ng/ml; enlarging anterior gland tumor (ADC 835→ 583 583 µµmm22/s) with decreased flow in PZ /s) with decreased flow in PZ
PZ: T2W =3/5; DWI =2/5
DCE = 2/5; MRSI =1/5
Ant TZT2W =4/5; DWI =4/5
DCE =5/5; MRSI =1/5


PostPost--androgens, preandrogens, pre--HIFU (Oct 2010)HIFU (Oct 2010)
Smaller anterior gland tumor (ADC 1355 Smaller anterior gland tumor (ADC 1355 µµmm22/s) with decreased flow & marked metabolic atrophy/s) with decreased flow & marked metabolic atrophy
PZ: T2W =3/5; DWI =2/5
DCE = 1/5; MRSI =ND
Ant TZT2W =3/5; DWI =3/5
DCE =4/5; MRSI =ND

ChallangesChallanges
�� Ability to display, coAbility to display, co--register, segment, fuse, and register, segment, fuse, and
analyse every tool in an integrated single workspace analyse every tool in an integrated single workspace
would be ideal would be ideal
�� Methods for dealing with missing functional datasets Methods for dealing with missing functional datasets
(not obtained, corruption, artefacts) are needed(not obtained, corruption, artefacts) are needed
�� Relative weighting of individual tests requires further Relative weighting of individual tests requires further
researchresearch
�� LocalizationLocalization: : DWDW--MRI MRI >> T2W T2W = = DCEDCE--MRI MRI >> MRSI ???MRSI ???
�� Aggressiveness:Aggressiveness: DWDW--MRI MRI == MRSI MRSI >> T2W T2W >> DCEDCE--MRI ???MRI ???


















