Benign Prostatic Hypertrophy, Prostatitis and Hematuria
24
Prostat itis Kishore SR Oman Medical College Chapter 14 & Hematuri
-
Upload
kishore-rajan -
Category
Health & Medicine
-
view
123 -
download
0
Transcript of Benign Prostatic Hypertrophy, Prostatitis and Hematuria

Prostatitis
Kishore SROman Medical CollegeChapter 14
& Hematuria

Contents
•Benign Prostatic Hypertrophy▫ Introduction▫Case Discussion▫ Investigation and Management▫Referral criteria's
•Acute and Chronic Prostatitis
•Hematuria▫D/Dx▫Management▫Referral Criteria's

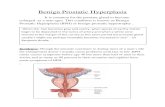
Benign Prostatic Hypertrophy (BPH)•Lower urinary tract symptoms consequent
upon bladder outlet obstruction due to benign prostatic hyperplasia (BPH), also known as benign prostatic enlargement (BPE). They are predominantly due to 2 components:
•a static component related to an increase in benign prostatic tissue narrowing the urethral lumen and
•a dynamic component related to an increase in prostatic smooth muscle tone mediated by alpha-adrenergic receptors.

•The prevalence of histological BPH does increase with age and affects approximately 42% of men between the ages of 51 and 60 years, and 82% of men between the ages of 71 and 80 years.
•BPH involves hyperplasia of both epithelial and stromal prostatic components. A key characteristic of BPH is increased stromal : epithelial ratio

Case History
•A 60-year-old man presents to his primary care physician with a 3-month history of increasing urinary frequency without burning and nocturia 3 times each evening. He has limited his fluid consumption and caffeine intake in the evening without much benefit. There is no personal or family history of prostate cancer.

Step-by-Step Diagnostic Approach
History•Patient can present with either Voiding
(obstructive) symptoms or with Storage (irritative) symptoms.
•Voiding symptoms include hesitancy, intermittency, weak stream, straining, incomplete emptying, and post-void dribbling.
•Storage symptoms include urinary frequency, nocturia, dysuria and urgency

•Fever, pain, and dysuria can suggest of alternative diagnosis such as prostatitis or UTI
•Hematuria increases the possibility of prostate or bladder cancer.
•Long-standing diabetes may suggest neurogenic bladder as a cause of lower urinary tract symptoms (LUTS)
•Medicines such as diuretics, anticholinergics, and adrenergic alpha-agonists may affect urinary flow rate or affect prostate bladder tone mimicking BPH
•Cardiovascular and renal disease may present with polyuria or nocturia

Physical examination•Abdominal examination – for distended
bladder, palpable kidneys. Examine the external genitalia
•Digital Rectal exam (DRE) – anal tone, estimate the size, shape and consistency of the prostate and to assess for prostate nodules or rectal masses.

Investigations
1. Urine analysis ▫ To rule out UTI. M, C and S
2. MSU▫ Dipstick for blood and glucose.
3. Serum Urea, creatinine and eGFR▫ Renal function assessment.
4. PSA▫ Increased PSA may suggest the presence of
underlying prostate cancer or prostatitis.5. IPSS6. Uroflowmetry▫ <15mL/s is abnormal
7. Ultrasound

The International Prostate Symptom Score (IPSS)•The IPSS, which is a self-administered
patient questionnaire with 8 questions (7 questions on symptoms and 1 question on quality of life) should be completed in the initial work-up.
•This is a reliable, accurate predictor of LUTS.
•Scores of 0 to 35 to define severity of symptoms.
0-7 mild 8-19 moderate 20-35 severe


Management •Watchful waiting: for those who have mild to
moderate symptoms at presentation with no complications of BPH and those not troubled severely by their symptoms. Self help can help.
•Drug Therapy:▫Alpha-adrenoceptor antagonists : Prazosin,
Doxazosin Watch for postural hypotension
▫5α-reductase inhibitors : Finasteride. For patients with bulky prostates. 6mo for effect.
Lowers the risk of urinary retention▫Combination therapy – reduces progression by
66%

Complications
•Recurrent UTI•Bladder stones•Hematuria•Acute retention of urine•Chronic retention•Overflow incontinence•Obstructive nephropathy

When to Refer?•Complicated BPH – Emergency admission
needed or Urgent•Nodular or Firm prostate – Urgent•High PSA - Urgent •Severe symptoms – Soon•Failure to respond to drug therapy after 3-
6 mo.. of prazosin or 6-12 mo.. of fenasteride - Routine

Acute Bacterial Prostatitis•The most frequent urological
diagnosis in men <50 years old.•Commonly caused by Escherichia
coli bacteria.•Consider in a patient with UTI•Features include; arthralgia,
myalgia, low back pain, perineal pain, penile pain, rectal pain
•Examination findings- DRE reveals Swollen, tender prostate

• Investigate using MSU
•Management – Ciprofloxacin 500mg bd or Ofloxacin 200mg bd
•Refer if not settling with treatment.
•Complications – Acute retention of urine, chronic bacterial prostatitis, prostate abscess.

Chronic Bacterial Prostatitis
•Chronic Pelvic pain Syndrome•Cause is unknown•Presents with >3 mo. history of ▫Urological pain – Low abd, pelvis/perineum,
Penis (especially tip w/t ejaculation), testis, rectum, low back
▫Irritative/Obstructive symptoms• Investigations – DRE, MSU, urine cytology, STI
screening, PSA, urodynamic study•T/t is difficult, provide info and support.•Try doxazosin 4mg od for 6 mo..

Hematuria•Macroscopic hematuria: ▫A substantial haemorrhage into the urinary tract
that will give the urine a red or brownish tinge•Microscopic hematuria : ▫>5 RBCs/hpf on two microscopic urinalyses
•Significant microscopic hematuria: ▫On microscopic examination of the urine, >5
RBCs /hpf in spun urine or >2 RBCs /hpf in unspun urine
• Investigate all cases • MSU, M,C & S and blood for U&E, creatinine, eGFR

Causes
•Kidney – Stones, Tumor, Infection, Glomerulonephritis
•Ureter – Stones, Tumor•Bladder – UTI, Stones,
Tumor, Chronic inflammation
•Prostate – Prostatitis, Tumor
•Urethral Inflammation

Management
Urgent Referral•Painless macroscopic hematuria•Age 40 or more with recurrent/persistent
UTI asst. with hematuria•Age 50 or more with unexplained
microscopic hematuria•Abdominal mass that is thought to be from
UT

Non- Urgent referral•Patients less than 50 with microscopic
hematuria.• If proteinuria, high serum creatinine or low
eGFR, refer to renal physician
In male patients with symptoms suggestive of UTI and macroscopic hematuria, diagnose and treat the infection first before referral.

Case Scenario A 75 year American old male comes to your office with a 6 month history of Nocturia, hesitancy, a slow flow of urine and terminal dribbling. No other significant medical illnesses except for diabetes
On examination, his abdomen is normal. He has an enlarged prostate gland which is smooth and firm with no nodules or irregularities.

Q. Before medical or surgical treatment of the patient, which of the following should be performed?A. Digital Rectal ExamB. CTC. ColonoscopyD. IPSSE. UltrasoundF. A and EG. A and D
Q. What are the risk factors in this patient?

Thank you

![Metastasis of Renal Cell Carcinoma to the Bladder · stump, bladder, and prostatic fossa [1,2]. Patients with RCC metastatic to the bladder typically present with gross hematuria.](https://static.fdocuments.in/doc/165x107/5e4ab3c0bb39856c894f36dc/metastasis-of-renal-cell-carcinoma-to-the-bladder-stump-bladder-and-prostatic.jpg)