MODELING ANTIBIOTIC RESISTANCE EPIDEMICS IN HOSPITALS
34
MODELING ANTIBIOTIC RESISTANCE EPIDEMICS IN HOSPITALS Pierre Magal Pierre Magal Department of Mathematics Department of Mathematics Université du Havre Université du Havre 76058 Le Havre, FRANCE 76058 Le Havre, FRANCE Shigui Ruan Shigui Ruan Department of Department of Mathematics Mathematics University of Miami University of Miami Coral Gables, FL, USA Coral Gables, FL, USA Glenn Webb Glenn Webb Department of Department of Mathematics Mathematics Vanderbilt University Vanderbilt University Nashville, TN USA Nashville, TN USA Erika D’Agata, Erika D’Agata, Beth Israel Deaconess Medical Beth Israel Deaconess Medical Center Center Harvard Harvard University University Boston, MA, USA Boston, MA, USA Mary Ann Horn Mary Ann Horn Mathematical Sciences Division Mathematical Sciences Division National Science Foundation National Science Foundation Washington, DC, USA Washington, DC, USA Damien Olivier Damien Olivier Department of Computer Sciences Department of Computer Sciences Université du Havre Université du Havre 76058 Le Havre, FRANCE 76058 Le Havre, FRANCE
description
MODELING ANTIBIOTIC RESISTANCE EPIDEMICS IN HOSPITALS. Erika D’Agata, Beth Israel Deaconess Medical Center Harvard University Boston, MA, USA. Mary Ann Horn Mathematical Sciences Division National Science Foundation Washington, DC, USA. Pierre Magal Department of Mathematics - PowerPoint PPT Presentation
Transcript of MODELING ANTIBIOTIC RESISTANCE EPIDEMICS IN HOSPITALS

MODELING ANTIBIOTIC RESISTANCE
EPIDEMICS IN HOSPITALS
Pierre MagalPierre MagalDepartment of MathematicsDepartment of Mathematics
Université du HavreUniversité du Havre76058 Le Havre, FRANCE76058 Le Havre, FRANCE
Shigui RuanShigui RuanDepartment of MathematicsDepartment of Mathematics
University of MiamiUniversity of MiamiCoral Gables, FL, USACoral Gables, FL, USA
Glenn WebbGlenn WebbDepartment of MathematicsDepartment of Mathematics
Vanderbilt UniversityVanderbilt UniversityNashville, TN USANashville, TN USA
Erika D’Agata, Erika D’Agata, Beth Israel Deaconess Medical CenterBeth Israel Deaconess Medical Center
Harvard Harvard UniversityUniversityBoston, MA, USABoston, MA, USA
Mary Ann HornMary Ann HornMathematical Sciences DivisionMathematical Sciences Division
National Science FoundationNational Science FoundationWashington, DC, USAWashington, DC, USA
Damien OlivierDamien OlivierDepartment of Computer SciencesDepartment of Computer Sciences
Université du HavreUniversité du Havre76058 Le Havre, FRANCE76058 Le Havre, FRANCE

nos-o-co-mi-al nos-o-co-mi-al adj originating or occurring in a hospitaladj originating or occurring in a hospital
Nosocomial infections are infections which are a result
of treatment in a hospital or a healthcare service unit,
but secondary to the patient's original condition.
Infections are considered nosocomial if they first appear
48 hours or more after hospital admission or within 30
days after discharge.
WHAT IS A NOSOCOMIAL INFECTION?

• Hospitals house large numbers of people whose immune systems are often in a weakened state.
• Increased use of outpatient treatment means that people who are in the hospital are sicker on average.
• Medical staff move from patient to patient, providing a way for pathogens to spread.
• Many medical procedures bypass the body's natural protective barriers.
WHY ARE NOSOCOMIAL INFECTIONS COMMON?

A GROWING PROBLEM
• Approximately 10% of U.S. hospital patients (about 2 Approximately 10% of U.S. hospital patients (about 2
million every year) acquire a clinically significant million every year) acquire a clinically significant
nosocomial infectionnosocomial infection. .
• Nosocomial infections are responsible for about 100,000 Nosocomial infections are responsible for about 100,000
deaths per year in hospitalsdeaths per year in hospitals
• More than 70 percent of bacteria that cause hospital-More than 70 percent of bacteria that cause hospital-
acquired infections are resistant to at least one of the acquired infections are resistant to at least one of the
drugs most commonly used in treatmentdrugs most commonly used in treatment

Methicillin (oxacillin)-resistant Staphylococcus aureus (MRSA) Among ICU Patients, 1995-2004
0
10
20
30
40
50
60
70
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Year
Percent Resistance
Source: National Nosocomial Infections Surveillance (NNIS) System

Vancomycin-resistant Enterococi (VRE) Among ICU Patients,1995-2004
0
5
10
15
20
25
30
35
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Year
Percent Resistance
Source: National Nosocomial Infections Surveillance (NNIS) System

WHAT IS THE CONNECTION OF ANTIBIOTIC USE TO NOSOCOMIAL EPIDEMICS?
• High prevalence of resistant bacterial strains present in the High prevalence of resistant bacterial strains present in the hospitalhospital
• High capacity of bacteria to mutate to resistant strainsHigh capacity of bacteria to mutate to resistant strains
• Selective advantage of mutant strains during antibiotic therapySelective advantage of mutant strains during antibiotic therapy
• Misuse and overuse of antibioticsMisuse and overuse of antibiotics
• Medical practice focused on individual patients rather than the Medical practice focused on individual patients rather than the general hospital patient community general hospital patient community

TYPES OF MICROBIAL RESISTANCE TO ANTIBIOTICS
• Inherent - microorganisms may be resistant to antibiotics because of physical and biochemical differences.
• Acquired - bacteria can develop resistance to antibiotics driven by two genetic processes:
• (a) mutation and selection (vertical evolution)
• (b) exchange of genes (plasmids) between strains and species (horizontal evolution).

OBJECTIVES OF THE MODELING PROJECT
• Construct a model based on observable hospital
parameters, focusing on healthcare worker (HCW)
contamination by patients, patient infection by healthcare
workers, and infectiousness of patients undergoing
antibiotic therapy.
• Analyze the elements in the model and determine strategies
to mitigate nosocomial epidemics

THE TWO LEVELS OF A NOSOCOMIAL EPIDEMIC
• Bacteria population level in a single infected host:
(i) host infected with the nonresistant strain
(ii) host infected with the resistant strain
• Patient and healthcare worker level in the hospital:
(i) uninfected patients susceptible to infection
(ii) patients infected with the nonresistant strain
(iii) patients infected with the resistant strain
(iv) uncontaminated HCW
(v) contaminated HCW

AN ORDINARY DIFFERENTIAL EQUATIONS MODEL AT THE BACTERIA POPULATION LEVEL
A. Bacteria in a host infected only with the nonresistant strain
VF(a) = population of nonresistant bacteria at infection age a
F(a) = proliferation rate
F = carrying capacity parameter of the host
B. Bacteria in a host infected with both nonresistant and resistant strains
V(a) = population of nonresistant bacteria at infection age a
V(a) = population of resistant bacteria at infection age a
_(a)(a) = proliferation rates
= recombination rate, = reversion rate
A B F( )a _( )a +( )a VF(a)/ F V(a)/ F V(a)/ F
V (a)
V+(a)
VF(a)

MODEL OF PLASMID FREE BACTERIA IN A SINGLE INFECTED HOST INFECTED WITH ONLY PLASMID FREE BACTERIA
If F >0, then limaVF(a)=F; if F<0, then limaVF(a)=0.
€
dVF(a)
da= V
F(a) β
F−
VF(a)
κF
⎛
⎝ ⎜
⎞
⎠ ⎟,
F=12.0log(2) before treatment (doubling time = 2 hr), F=-2.0 after treatment, F=1010

MODEL OF BACTERIA IN A SINGLE INFECTED HOST INFECTED
WITH PLASMID FREE AND PLASMID BEARING BACTERIA
€
dV − (a)
da= −
τV+(a)
V − (a)+V+(a)+ β
−−
V − (a)+V+(a)
κF
⎛
⎝ ⎜
⎞
⎠ ⎟V − (a)+γV+(a),
dV+(a)
da=
τV − (a)
V − (a)+V+(a)+ β
+−
V − (a)+V+(a)
κF
− γ ⎛
⎝ ⎜
⎞
⎠ ⎟V+(a),
⎧
⎨
⎪ ⎪
⎩
⎪ ⎪
Equilibria of the model: E0 = (0,0), EF = (F 0), and
€
E* =γκ
F
γ +σβ
−+σ −
τσ
γ +σ
⎛
⎝ ⎜
⎞
⎠ ⎟,σκ
F
γ +σβ
−+σ −
τσ
γ +σ
⎛
⎝ ⎜
⎞
⎠ ⎟
⎛
⎝ ⎜
⎞
⎠ ⎟
(i) If ,0<−+−=−+σ then 0Ei sunstabl eand FEi s stable
i.e., ,)(lim−−∞→=FaaV .0)(lim=+∞→aVa(ii)I f ,0>−+−=−+σ the ,n 0E(unstable), FEi (s unstable),and *E(stable),i.e.,,)(lim ⎟⎟⎠⎞⎜⎜⎝⎛+−++=−−∞→ σσσσFaaV .)(lim ⎟⎟⎠⎞⎜⎜⎝⎛+−++=−+∞→ σσσσσFaaV

-=8.0log(2), +=4.0log(2), =10 -5, = 10-3 , F=1010, σ0
-=8.0log(2), +=9.0log(2), =10 -5, = 10-3 , F=1010, σ00

AN INDIVIDUAL BASED MODEL (IBM) AT THE HOSPITAL POPULATION LEVEL
Three stochastic processes:
1) the admission and exit of patients
2) the infection of patients by HCW
3) the contamination of HCW by patients
These processes occur in the hospital over a period of months or years
as the epidemic evolves day by day. Each day is decomposed into 3 shifts
of 8 hours for the HCW. Each HCW begins a shift uncontaminated, but
may become contaminated during a shift. During the shift a time step t
delimits the stochastic processes. The bacterial load of infected patients
during antibiotic treatment is monitored in order to describe the
influence of treatment on the infectiousness of patients.

PATIENT AND HCW POPULATION LEVEL
QuickTime™ and aTIFF (LZW) decompressor
are needed to see this picture.
Top: Healthare workers are divided into four classes: uncontaminated (HU), contaminated only with non-resistant bacteria (HN), contaminated with both non-resistant and resistant bacteria (HNR), and contaminated only with resistant bacteria (HR)
Bottom: Patients are divided into five classes: uninfected patients (PU), patients infected only by the non-resistant strain (PN), and three classes of patients infected by resistant bacteria (PRS), (PNR), and (PRR). PRS consists of super-infected patients, that is, patients that were in class PN and later become infected with resistant bacteria. PRR consists of patients that were uninfected and then became infected by resistant bacteria. PNR consists of patients that were uninfected, and then become infected with both non-resistant and resistant bacteria.

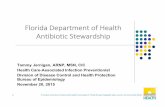
INFECTIOUSNESS OF INDIVIDUAL PATIENTSPatient PN Patient PRS
Patient PRR Patient PNR
Infectiousness periods when the antibiotic treatment starts on day 3 and stops on day 21 (inoculation occurs on day 0). The blue and red curves represent, respectively, the bacterial load of resistant and non-resistant bacteria during the period of infection. The green horizontal lines represent the threshold of infectiousness TH=1011. The green bars represent the treatment period. The yellow, red, and orange bars represent the periods of infectiousness for the non-resistant, resistant, and both non-resistant and resistant classes, respectively.

PARAMETERS OF THE MODEL AT THE HOSPITAL LEVEL
*Beth Israel Deaconess Medical Center, *Beth Israel Deaconess Medical Center, Harvard, BostonHarvard, Boston** Cook ** Cook County Hospital,County Hospital, Chicago Chicago
Number of patientsNumber of patients 400400**
Number of healthcare workersNumber of healthcare workers 100100**
Average length of stay for a patient not Average length of stay for a patient not infected with either straininfected with either strain
55 daysdays**
Average length of stay for a patient Average length of stay for a patient infected with the nonresistant straininfected with the nonresistant strain
14 days14 days**
Average length of stay for a patient Average length of stay for a patient infected with the resistant straininfected with the resistant strain
28 days28 days**
Average time between visits of HCW Average time between visits of HCW 90 min
Probability of contamination by a HCWProbability of contamination by a HCW 0.40.4****
Probability of infection by a patientProbability of infection by a patient 0.060.06****
Average time of contamination of HCWAverage time of contamination of HCW 60 min60 min****

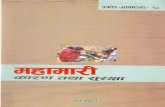
THE INFECTION AND CONTAMINATION PROCESSES
Patient-HCW contact diagram for 4 patients and 1 HCW during one shift. Patient status: uninfected (green), infected with the non-resistant strain (yellow), infected with the resistant strain (red). HCW status: uncontaminated (______ ), contaminated with the non-resistant strain (………), contaminated with the resistant strain (- - - - - ).

SUMMARY OF THE IBM MODEL ASSUMPTIONS
(i) each HCW begins the first visit of the shift uncontaminated and subsequent patient visits are randomly chosen among patients without a HCW;
(ii) at the end of a visit a HCW becomes contaminated from an infectious patient with probability PC and a patient becomes infected from a contaminated HCW with probability PI;
(iii) the bacterial load of an infected patient is dependent on treatment scheduling and infected patients are infectious to a HCW when their bacterial load is above a threshold TH;
(iv) each time step t a contaminated HCW exits contamination with probability 1 - exp(-t/AC) and exits a visit with probability 1 - exp(-t/AV);
(v) (v) each time step t a patient of type L exits the hospital with probability 1 - exp(-t/AL), where L = U,N,R.
(vi) The number of patients in the hospital is assumed constant, so that a patient leaving the hospital is immediately replace by a new patient in class (U).

SIMULATIONS OF THE IBM
Beginning of treatment day 3 End of treatment day 21
Beginning of treatment day 1End of treatment day 8
From the two IBM simulations we see that when treatment starts earlier and has a shorter period, both non-resistant and resistant strains are eliminated. Earlier initiation of treatment reduces the non-resistant bacterial load and shorter treatment intervals reduce the time that patients infected by the resistant strain are infectious for this strain.

A COMPLEMENTARY DIFFERENTIAL EQUATIONS MODEL (DEM)
The DEM corresponds to the average behavior of the IBM over a large number of simulations. Denote by PU(t), PN(t), PR(t) the fraction of patients in the class (U), (N), (R) respectively.
To describe the infectiousness status of patients, we use the age of infection a, which represents the time already spent in the class of infected patients (N), (RS), (RR), or (NR). For K=N, RS, RR, NR, we denote by pK(t,a) the density of the fraction of patients with infection status (K) and infection-age a at time t. For K=N, RS, RR, NR
€
PK ( t) = pK (t,a)da0
+∞
∫ .

STATE VARIABLES OF THE (DEM)
Symbol Interpretation
€
HU(t) fraction of HCW workers uncontaminated
€
HN(t) fraction of HCW contaminated only by non-resistant strain
€
HNR(t) fraction of HCW contaminated by both resistant and non-resistant strains
€
HR(t) fraction of HCW contaminated only by resistant strain
€
PU(t) fraction of patients uninfected
€
PN(t) fraction of patients infected only by non-resistant strain
€
PRS(t) fraction of patients infected first by non-resistant strain and then by resistant strain
€
PNR(t) fraction of patients infected first by both resistant and non-resistant strain
€
PRR(t) fraction of patients infected only by resistant strain
€
pK(t,a) infection age density of the fraction of infected patients of class K=N,RS,RR,NR
€
PKI(t) fraction of patients infectious with the strain K=N,NR,R
Note: Infected patients may or may not be infectious, depending on stage of infection and use of antibiotics.

PARAMETERS OF THE (DEM)
Symbol Interpretation
€
V=NBH/NBP probability for a patient to be visited by a healthcare
worker
€
νV=1/AV rate at which a healthcare worker exits a visit
€
νC=1/AC rate at which a healthcare worker becomes
uncontaminated
€
νN=1/AN rate at which a class N patient exits the hospital
€
νR=1/AR rate at which a class R patient exits the hospital

EQUATIONS FOR THE HEALTHCARE WORKERS
€
0 = −νV PC PNI (t)+ PNR
I ( t)+ PRI (t)[ ]HU( t)+ν C H N ( t)+ H NR( t)+ H R(t)[ ],
0 = νV PC PNI ( t)HU( t)− νV PC PNR
I ( t)+ PRI (t)[ ]H N ( t)− ν C H N ( t),
0 = νV PC PNRI ( t)+ PR
I (t)[ ]H N ( t)+νV PC PNRI (t)HU(t)+νV PC PN
I (t)+ PNRI ( t)[ ]H R(t)− ν C H NR( t),
0 = −νV PC PNI (t)+ PNR
I ( t)[ ]H R(t)+νV PC PRI (t)HU(t)− ν C H R(t),
⎧
⎨
⎪ ⎪ ⎪
⎩
⎪ ⎪ ⎪
The equations for the HCW are motivated by a singular perturbation technique. The idea is that the time scale of the HCW is much smaller than the time scale for the evolution of the epidemic at the patient level. These equations are solved for the HCW fractions.
€
HU( t)+ H N (t)+ H NR( t)+ H R(t) = 1.

EQUATIONS FOR THE FRACTIONS OF PATIENTS INFECTIOUS FOR THE BACTERIAL STRAINS
€
PNI (t) = γ N
N
0
+∞
∫ (a) pN (t,a) + γ NRS (a) pRS (t,a) + γ N
RR (a) pRR (t,a) + γ NNR (a) pNR (t,a)da,
PRI (t) = γ R
N
0
+∞
∫ (a) pN (t,a) + γ RRS (a) pRS (t,a) + γ R
RR (a) pRR (t,a) + γ RNR (a) pNR (t,a)da,
PNRI (t) = γ NR
N
0
+∞
∫ (a)pN (t,a) + γ NRRS (a)pRS (t,a) + γ NR
RR (a)pRR (t,a) + γ NRNR (a) pNR (t,a)da.
⎧
⎨
⎪ ⎪ ⎪
⎩
⎪ ⎪ ⎪
€
The infectious functions γ NN(a), γ N
RS(a), γ NRR(a), and γ N
NR(a) are defined
by the solutions of the bacterial load levels obtained from the bacteria
population model for patients undergoing antibiotic therapy.
€
KL (a) =
1 if a patient of class L is infectious with bacteria of type
K at age of infection a
0 otherwise.
⎧
⎨ ⎪
⎩ ⎪

INFECTIOUSNESS OF INDIVIDUAL PATIENTSPatient PN Patient PRS
Patient PRR Patient PNR
Infectiousness periods when the antibiotic treatment starts on day 3 and stops on day 21 (inoculation occurs on day 0). The blue and red curves represent, respectively, the bacterial load of resistant and non-resistant bacteria during the period of infection. The green horizontal lines represent the threshold of infectiousness TH=1011. The green bars represent the treatment period. The yellow, red, and orange bars represent the periods of infectiousness for the non-resistant, resistant, and both non-resistant and resistant classes, respectively .

EQUATIONS FOR THE DEM
€
dPU (t)
dt= (ν N PN (t) + ν R PR (t)) −ν V βV PI HN (t) + HNR (t) + HR (t)( )P
U (t),
∂
∂tpN +
∂
∂apN ⎛
⎝ ⎜
⎞
⎠ ⎟(t,a) = − ν N + ν V βV PI HR (t) + HNR (t)( )( )pN (t,a),
pN (t,0) = ν V βV PI HN t( )PU (t),
∂
∂tpRS +
∂
∂apRS ⎛
⎝ ⎜
⎞
⎠ ⎟(t,a) = −ν R pRS (t,a),
pRS (t,0) = ν V βV PI HR (t) + HNR (t)( )PN (t),
∂
∂tpRR +
∂
∂apRR ⎛
⎝ ⎜
⎞
⎠ ⎟(t,a) = −ν R pRR (t,a),
pRR (t,0) = ν V βV PI HR (t)PU (t),
∂
∂tpNR +
∂
∂apNR ⎛
⎝ ⎜
⎞
⎠ ⎟(t,a) = −ν R pNR (t,a),
pNR (t,0) = ν V βV PI HNR (t)PU (t),
⎧
⎨
⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪
⎩
⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪

COMPARISON OF THE IBM AND THE DEM
Beginning of treatment day 3 End of treatment day 21
Beginning of treatment day 1End of treatment day 8

ANALYSIS OF THE PARAMETRIC INPUT - R0
A major advantage of the DEM is that the parametric input can be analyzed through the basic reproductive numbers R0 , which predict the expected number of secondary cases per primary case. When R0 <1, then the epidemic extinguishes and when R0 >1, then the epidemic becomes endemic.
R0N for patients infected only by the non-resistant strain is
€
R0N =
νV( )2βV PI PC
ν C
γ NN (a)exp(−ν N a)da
0
+∞
∫ .
If R0N<1, then R0
R for patients infected only by the resistant strain is
€
R0R =
νV( )2βV PI PC
ν C
r(A),
where r(A) is the largest eigenvalue of the matrix
€
A =γ R
RR(a)exp(−ν Ra)da0
+∞
∫ γ RNR(a)exp(−ν Ra)da
0
+∞
∫
γ NRRR(a)exp(−ν Ra)da
0
+∞
∫ γ NRNR(a)exp(−ν Ra)da
0
+∞
∫
⎛
⎝
⎜ ⎜ ⎜ ⎜
⎞
⎠
⎟ ⎟ ⎟ ⎟
.

EFFECTS OF CHANGING THE DAY TREATMENT BEGINS AND HOW LONG IT LASTS
R0
N<1 always, but R0R<1 or R0
R>1 depending on the starting day and the duration of treatment. Both R0
N and R0R are increasing when the starting day of treatment increases,
because the bacterial loads of both strains are higher if treatment is delayed and thus more likely to reach threshold Further, R0
N decreases and R0R increases as the length of treatment
duration increases, because the resistant strain prevails during treatment.

EFFECTS OF CHANGING THE LENGTH OF VISITS AND THE LENGTH OF CONTAMINATION OF HCW
Both R0N and R0
R decrease as the length of visits AC increases and increase as the length of contamination AV increases, but the dependence is linear in AC and quadratic in 1/AV. The reason is AC is specific to HCW, but AV is specific to both HCW and patients.

CONCLUSIONS OF THE MODEL
•Start treatment as soon as possible after infection is diagnosed and minimize its duration. Recent clinical trials suggest that the duration of antimicrobial therapy can be decreased substantially in the treatment of certain community- and hospital-acquired infections with equivocal patient outcomes.
•Because R0N and R0
N depend linearly on AC and quadratically on 1/AV, extending the average length of visits (which is correlated to the allocation of HCW resources) may have less benefit than reducing the average length of the contamination (which is correlated to improvement in hygienic measures).
•The care of individual patients and the general patient population welfare must be balanced.
•Mathematical models provide a framework to analyze the dynamic elements in antibiotic resistance epidemics and quantify their impact in specific hospital environments.

REFERENCES
D.J. Austin, K.G. Kristinsson, and R.M. Anderson, The relationship between the volume of antimicrobial consumption in human communities and the frequency of resistance, Proc. Natl., Acad. Sci., Vol. 96 (1999), 1152-1156.
C.R. Bergstrom, M. Lipsitch, and B.R. Levin, Natural selection, infectious transfer and the existence conditions for bacterial plasmids, Genetics, Vol. 155 (2000), 1505-1519.
E. D’Agata, M.A. Horn, and G.F. Webb, The impact of persistent gastrointestinal colonization on the transmission dynamics of vancomycin-resistant enterococci, J. Infect. Dis. ,Vol. 185 (2002), 766-773.
E. D’Agata, M.A. Horn, and G.F. Webb, A mathematical model quantifying the impact of antibiotic exposure and other interventions on the endemic prevalence of vancomycin-resistant enterococci, J. Infect. Dis., Vol. 192 (2005), 2004-2011.
E. D’Agata, P. Magal, S. Ruan, and G.F. Webb, A model of antibiotic resistant bacterial epidemics in hospitals, Proc. Nat. Acad. Sci. Vol. 102, No. 37, (2005), 13343-13348.
E. D'Agata, P. Magal, S. Ruan, and G.F. Webb, Modeling antibiotic resistance in hospitals: The impact of minimizing treatment duration, J. Theoret. Biol., Available online Aug. 27 (2007).
I. Pelupessy, M. C. M. Bonten and O. Diekmann, How to assess the relative importance of different colonization routes of pathogens within hospital settings, Proc. Natl., Acad. Sci. 99 (2002), 5601-5605.