Malnutrition management- Key learnings at Northern Health
34
Malnutrition management- Key learnings at Northern Health Stephanie Yap, Grade 2 Dietitian
Transcript of Malnutrition management- Key learnings at Northern Health

Malnutrition management-Key learnings at Northern Health
Stephanie Yap, Grade 2 Dietitian

• Experience across general medical, oncology and renal inpatient wards
• Discharging patients to Northern Health subacute or outpatient services
Acute inpatients
• Worked across 2x GEM wards, 1x dementia ward
• Liaising with nursing nutrition champion in dementia ward
Subacute inpatients • Working in outpatient
rehab (SACS), CHSP and HACC PYP
• Majority of clients are seen via telehealth for malnutrition management
Outpatients/ Community
My experience at Northern Health
Malnutrition screening and weighing
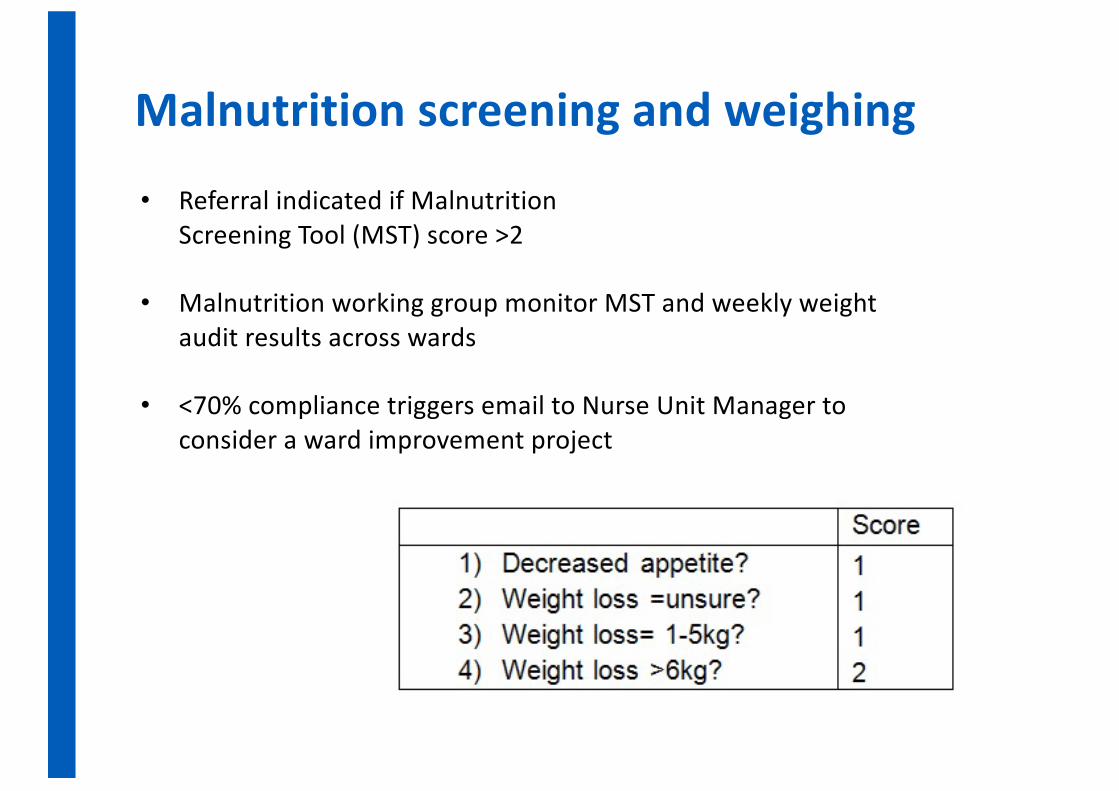
• Referral indicated if Malnutrition Screening Tool (MST) score >2
• Malnutrition working group monitor MST and weekly weight audit results across wards
• <70% compliance triggers email to Nurse Unit Manager to consider a ward improvement project

Malnutrition screening and weighing
0102030405060708090
Malnutritionscreening and
weight onadmission
Weekly rescreenand reweigh
Referral toDietitian
indicated andplaced
Average result (%) 84 61 71
CARE record nutrition and hydration audit results Jan -Jun 2021

• Kath Atkinson Ward at Northern Health recorded a compliance rate of 95% or higher last quarter
• KAW has a nursing nutrition champion- the first of her kind at Northern Health
• Nursing nutrition champion runs weekly in-services to promote nutrition screening/weighing, and maintains an ongoing communication channel between Nursing staff and Dietitians
Key learning- Consider ward nutrition nursing champion
Nursing nutrition champion

Discharge planning in the inpatient setting
Discharge planning• All pts assessed as at malnutrition risk are offered outpatient
follow up at Northern Health• Electronic referral to relevant Northern Health outpatient clinic• Providing dietary recommendations and brief education• Setting up patients with script for oral nutrition support
Key learning – Sending supplements immediately

Subacute Ambulatory Care Services (SACS) Phone clinic• Implemented in September 2019 (pre-COVID-19 in Victoria) • Aims to provide more robust outpatient follow up and utilise EFT in
outpatient rehab clinic
Types of patients to refer for a phone assessment:Patients at risk of malnutrition or malnourishedAble to weight themselves/ monitor weight at home Requiring assessment of oral nutrition supplement tolerance
Exclusion criteria:Dementia/delirium, communication barriers (e.g. aphasia, dysphasia) NESB * relaxed in COVID-19 situation

Phone outpatient clinic – key learnings so far
• Dramatically increased referral rates, contributing to increase in activity rates 18% in first 12 months
• Reduced waiting times from date of referral to initial assessment• Similar failure to attend (FTA) rates
• Clinical outcomes on discharge: -38% were weight stable -11% reported 5-10% weight gain -38% had unknown weight changes

Global Leadership Initiative on Malnutrition (GLIM)
• GLIM is an alternative malnutrition assessment tool that has global consensus to support its use
• Validated for use in adult inpatients, ICU, cancer patients, older adults*
• Used at Northern Health when a physical exam is not possible, or inadequate weight history details
GLIM Criteria for the Diagnosis of Malnutrition: A Consensus Report From the Global Clinical Nutrition Community JPEN. 2018; 0: 1-9

GLIM criteria
Phenotypic Criteria • Non-volitional weight loss• Low body mass index (BMI)• Reduced muscle mass (defined by validated body composition measuring
techniques such as bioelectrical impedance) Etiologic Criteria• Reduced food intake or assimilation• Disease burden/inflammation
1 phenotypic + 1 etiologic criterion should be present to diagnose malnutrition

At least 1 phenotypic criterion and 1 etiologic criterion should be present. Malnutrition severity
Phenotypic Criteria Etiologic Criteria Weight Loss (%)
Low Body Mass Index (kg/m2)
Reduced Food Intake or Assimilation
Inflammation
Moderate malnutrition
5-10% within 6/12, OR 10-20% > 6/12
<20 if < 70 years <22 if ≥ 70 years
≤ 50% of energy requirement >1 week OR Any reduction for > 2 weeks OR Any chronic GI condition that adversely impacts food assimilation** or absorption*
Acute disease/injury: major infection, burns, trauma, closed head injury OR Chronic disease-related: malignant disease, COPD, CCF, CKD, or any disease with chronic or recurrent inflammation # CRP may be used as a supportive biochemical measure
Severe malnutrition
>10% within the past 6 months OR >20% beyond 6 months
<18.5 if < 70 years <20 if ≥ 70 years
*Consider GI symptoms as supportive indicators that can impair food intake / absorption e.g. chronic dysphagia, nausea, vomiting, diarrhoea, constipation or abdominal pain
**Reduced assimilation is associated with SBS, pancreatic insufficiency, after bariatric surgery, oesophageal strictures, gastroparesis & intestinal pseudo-obstruction.
GLIM etiologic criteria

• Used as a secondary tool when unable to complete Subjective Global Assessment
• Useful for patients refusing physical exam, in isolation rooms and telehealth/phone assessments
• Reduced muscle mass is not assessed as body composition devices are not readily available in clinical setting
• Consider CRP in the wider clinical context when used as an indication of inflammation
GLIM –practical considerations

Summary
• Consider ways to influence malnutrition management from within ward e.g. Nursing nutrition champion
• Key learnings in discharge planning-Supporting supplement compliance on discharge-Following up malnutrition risk patients via phone assessment clinic
• Importance of using alternative assessment tools to support malnutrition diagnosis in COVID-19 pandemic e.g. GLIM

Key Learning Areas
Introduction to the Community Care Program
Benefits of a multidisciplinary team in screening for malnutrition
Barriers to completing malnutrition assessments in the community
Impact of Covid on an outreach service

Community Care Program
Short-term outreach support
Complex health and psychosocial issues and are at risk of
hospital presentation.
Health Independence Program providing
individualised, client-centred care 1

Community Care Team
PhysiosOccupational
TherapistsSocial Workers
Pharmacists NursesRespiratory and Cardiac
Nurses
DoctorsAdvanced Care
Planning
Aboriginal Hospital
Liaison Officer
Dietitian
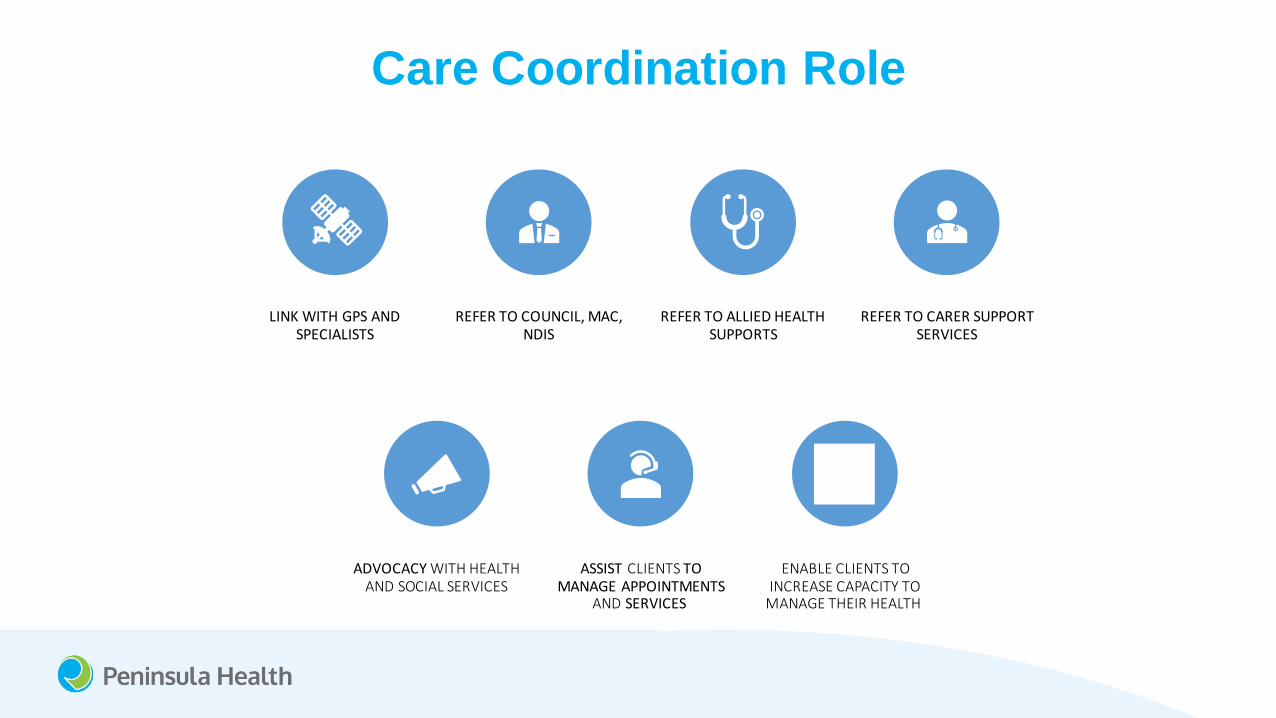
Care Coordination Role
LINK WITH GPS AND SPECIALISTS
REFER TO COUNCIL, MAC, NDIS
REFER TO ALLIED HEALTH SUPPORTS
REFER TO CARER SUPPORT SERVICES
ADVOCACY WITH HEALTH AND SOCIAL SERVICES
ASSIST CLIENTS TO MANAGE APPOINTMENTS
AND SERVICES
ENABLE CLIENTS TO INCREASE CAPACITY TO
MANAGE THEIR HEALTH

Community Care Dietitian Role
ASSESSMENT AND EDUCATION ON A RANGE OF DIETARY CONDITIONS
HOME VISITS ATTEND RELEVANT APPOINTMENTS WITH
CLIENTS
LIAISE WITH COMMUNITY CARE TEAM OR
COMMUNITY SERVICES
PROVIDE EVIDENCEBASED EDUCATION BASED ON
CLIENT GOALS
FACILITATE REFERRAL TO ONGOING SERVICES

Prevalence of malnutrition in the community
• Can be difficult to determine.
• Some studies indicate rate of malnutrition in the community setting range between 5-15%.2,3
• The degree of clients screened to be at moderate to high risk of malnutrition also varied widely. 2,3
• The variability may be related to the use of different screening tools.

Impact of malnutrition on community
clients
• Increased risk of hospitalization and poorer outcome.
• Increased risk of pressure sores and poor wound healing.
• Increased risk of falls and harm from falls.
• Reduced independence.
• Increased risk of needing increased services or placement in aged care facility.
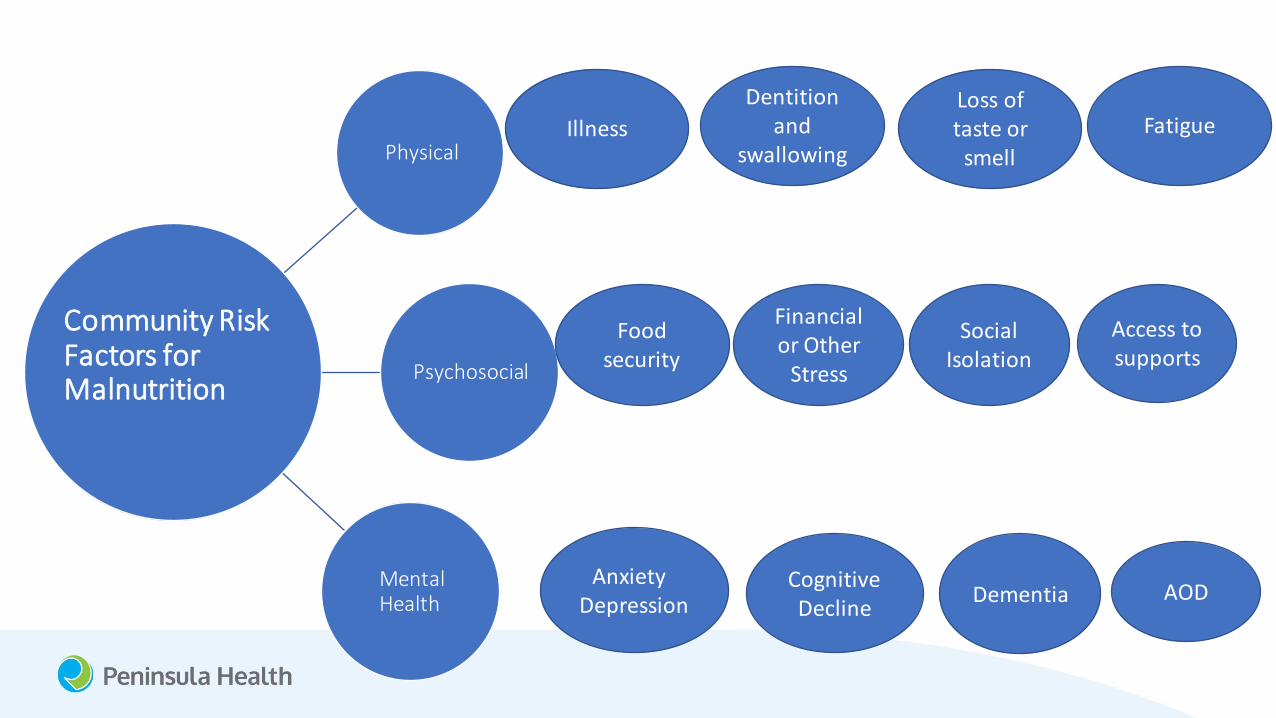
Community Risk Factors for Malnutrition
Physical
Psychosocial
Mental Health
Cognitive Decline
AnxietyDepression Dementia AOD
IllnessLoss of taste or
smell
Dentition and
swallowingFatigue
Food security
Financial or Other
Stress
Social Isolation
Access to supports
Community Risk Factors for Malnutrition

Screening for malnutrition in the
community
• Other Peninsula Health Community Programs including Community Health and Community Rehabilitation Program.
• All dietetic referrals are screened at ACCESS level with MST to prioritise referrals.
• All participants in group programs are also screened with MST at ACCESS level with a score of 2 prompting an offer of referral to a dietitian for follow up.

Screening for malnutrition in the
community• Community Care
• Each Initial Assessment and discipline assessments ask questions on:
• Unintentional weight changes
• Dentition and swallowing issues
• Falls
• Any concerns the patient has regarding their nutrition
This would prompt a referral to be made for Dietitian review.

Benefits of multi and trans disciplinary
screening for malnutrition
• Allows for repeated opportunity to identify concerns throughout the client's episode of care
• Patient is viewed holistically and through varied lenses
• May increase acceptance of referral and interventions when encouraged by multiple clinicians

Difficulties in completing Malnutrition
Assessments in the community
• Discussions between community health and acute about a standardized assessment of malnutrition across all areas of dietetics within Peninsula Health (SGA).
• However, after some trials, there was consensus between Community Care and Community Health that the SGA may not be appropriate for community- based clients.
• In Community Care the principles of SGA are used where possible to comment on degree of muscle wastage and subcutaneous fat loss to validate diagnosis of malnutrition.

Management of malnutrition in the
community• Education on high energy, high protein meal and snack ideas.
• Food first approach.
• Provide education on benefit of nutritional supplements if requirements cannot be met with food.
• Provide samples and education on online ordering platforms to support the easy provision of nutritional solutions to patients at home.
• Home visits allow for further observation of environment and identify potential barriers to adhering to recommendations.

Links between acute and community
services
• Community Health is integrated within the greater Peninsula Health Service.
• All records are electronic and available between acute, sub-acute and community settings.
• Community Care sits in between acute/sub-acute and Community Health programs.
• Enables timely communication and handover of clients as well as clinical support and education.
• Enables to clients to pass through various services with limited disruption.

Referral to ongoing dietitian services
Community Care
Community Health
Community Rehab Program
Private or NDIS

Impact of Covid
SIGNIFICANT IMPACT ON THE FUNCTION OF COMMUNITY CARE
HOME VISITS BECAME VERY LIMITED UNLESS ESSENTIAL
PHONE BASED CONSULTS POSSIBLE REDUCED CONNECTION BETWEEN CLIENTS AND CLINICIANS
POSSIBLE DELAY IN IDENTIFYING
DETERIORATION OR NEED FOR SUPPORT
INCREASED ISOLATION FROM SUPPORTS
INCLUDING MEDICAL AND SOCIAL SERVICES
REDEPLOYMENTINTO COVID WORKFORCE
Summary
Community Care is a short term care coordination program that aims to increase clients capacity to engage in their health care.
A diverse multi-disciplinary team enables clients to be screened for risk of malnutrition holistically.
It can be difficult to determine rates of malnutrition in the community.
Covid significantly impacted the traditional work of Community Care but clinicians were able to adapt to ensure patients were supported.
References
• 1. Victorian Department of Health. 2020. Care Coordination. <https://www2.health.vic.gov.au/hospitals-and-health-services/patient-care/rehabilitation-complex-care/health-independence-program/care-coordination>
• 2. Tasmanian Department of Health. June 2020. Malnutrition.< https://www.dhhs.tas.gov.au/__data/assets/pdf_file/0004/343372/Malnutrition_background.pdf>
• 3. Dietitians Assocation of Australia. 2019. Malnutrition in older Australians. <https://agedcare.royalcommission.gov.au/system/files/2020-06/DAA.0001.0001.0079.pdf>

Thank you