LCHS Community Assessment 2012 2013
50
2012-2013 Community Assessment Submitted to: Suzanne Miller, PhD Director On behalf of: Head Start of Lincoln County, Oregon (A Program of Community Services Consortium) Provided by: Joann Zimmer, MPAE
-
Upload
joannzimmer -
Category
Documents
-
view
1.025 -
download
1
description
Community Assessment report for Head Start of Lincoln County, Oregon.
Transcript of LCHS Community Assessment 2012 2013

2012-2013 Community Assessment
Submitted to:
Suzanne Miller, PhD
Director
On behalf of:
Head Start of Lincoln County, Oregon
(A Program of Community Services Consortium)
Provided by:
Joann Zimmer, MPAE

Community Assessment 2012-2013
i
TABLE OF CONTENTS
1.0 Summary .........................................................................................................................1
1.1 Executive ......................................................................................................................... 1
1.2 Data ................................................................................................................................. 2
1.2.1 Basic Needs Services ........................................................................................... 2
1.2.2 Employment ........................................................................................................ 2
1.2.3 Housing ............................................................................................................... 2
1.2.4 Childcare ............................................................................................................. 3
1.2.5 Transportation ..................................................................................................... 3
1.2.6 Health ................................................................................................................. 3
1.2.7 Education ............................................................................................................ 3
2.0 Community Assessment .................................................................................................4
2.1 Purpose and Scope of Project ........................................................................................... 4
2.2 Methodology.................................................................................................................... 4
3.0 Head Start .......................................................................................................................5
3.1 What is Head Start? ......................................................................................................... 5
3.1.1 Major Components .............................................................................................. 5
3.2 Grantee Description ......................................................................................................... 6
3.2.1 Lincoln County Need........................................................................................... 8
4.0 Geographic Area.............................................................................................................9
4.1 Oregon Poverty Overview ................................................................................................ 9
4.1.1 Basic Family Budget ........................................................................................... 9
4.1.2 Living Wage ...................................................................................................... 10
4.2 Lincoln County .............................................................................................................. 10
4.2.1. Population ......................................................................................................... 10
4.2.1.1 Race and Ethnicity .............................................................................. 11
4.2.2 Poverty .............................................................................................................. 12
4.2.3 Food .................................................................................................................. 13
4.2.4 Employment ...................................................................................................... 14
4.2.5 Children with Disabilities .................................................................................. 15
4.2.6 Housing ............................................................................................................. 17
4.2.7 Health Care ....................................................................................................... 18
4.2.7.1 Medical ............................................................................................... 20
4.2.7.2 Mental Health ...................................................................................... 23
4.2.7.3. Dental Care ......................................................................................... 24
4.2.8 Child Care ......................................................................................................... 25
4.2.8.1 Child Care Assistance .......................................................................... 25
4.2.8.2 Child Development Programs (in addition to CSCHS) ......................... 26
4.2.9 Domestic Violence ............................................................................................ 26

ii
4.2.10 Transportation ................................................................................................... 27
4.2.10.1 Local Options ...................................................................................... 27
4.2.10.2 Regional Options ................................................................................. 27
5.0 Conclusions and Recommendations............................................................................. 29
5.1 Discoveries .................................................................................................................... 29
5.2 Suggestions .................................................................................................................... 29
Appendix A .............................................................................................................................. 30
Successes and Partnerships ....................................................................................................... 30
Successes .................................................................................................................................. 30
Partnerships .............................................................................................................................. 31
Appendix B .............................................................................................................................. 32
Working Paper – Suggested Gaps/Needs in Child Development Programs in Lincoln County as
expressed by the Early Childhood Special Education Workgroup Notes .................................... 32
Appendix C .............................................................................................................................. 35
Suggestions for Improving Affordable Housing Availability in Lincoln County ........................ 35
Appendix D .............................................................................................................................. 36
Parent Survey and Comments.................................................................................................... 36
Parent Survey............................................................................................................................ 36
Parent Comments ...................................................................................................................... 38
Appendix E .............................................................................................................................. 39
Provider Interviews ................................................................................................................... 39
Input into what works, where improvement could be made ........................................................ 39
Positive ..................................................................................................................................... 39
Needs Improvement .................................................................................................................. 39
Appendix F .............................................................................................................................. 40
SWOT Analysis ........................................................................................................................ 40
Appendix G ............................................................................................................................. 41
Supported Affordable Housing in Lincoln County ..................................................................... 41
Appendix H ............................................................................................................................. 42
Glossary of Acronyms .............................................................................................................. 42
Information Citations ............................................................................................................. 43

iii
List of Figures
Figure 4-1. Basic Family Budget – 2010 vs. FPL ................................................................................. 9
Figure 4-2. Uninsurance Rate by Race ............................................................................................... 12
Figure 4-3. Child Care Funding ......................................................................................................... 25
List of Tables
Table 3-1. Early Head Start and Head Start Enrollment 2010 .............................................................. 5
Table 3-2. CSCHS 2012-2013 School Year Current Comprehensive Statistics .................................... 7
Table 3-3. CSCHS 2011-2012 School Year Current Comprehensive Statistics .................................... 7
Table 3-4. CSCHS 2012-2013 School Year Current Comprehensive Statistics .................................... 8
Table 3-5. CSCHS 2012-2013 School Year Current Comprehensive Statistics .................................... 8
Table 4-1. Lincoln County Poverty Information, 2010 ...................................................................... 11
Table 4-2. Population Changes 2000 to 2010 .................................................................................... 11
Table 4-3. Historical Median Household Income by Race – Lincoln County ..................................... 11
Table 4-4. Poverty by Age, Hispanic Origin, Race: 2011 Census – National ..................................... 12
Table 4-5. Household Poverty Rate by Family Type, 2006 - 2010..................................................... 12
Table 4-6. Change in Poverty Rate 2000 – 2010 Lincoln County ...................................................... 13
Table 4-7. Change in Childhood (0-17) Poverty Rate in Lincoln County 2000 - 2010 ....................... 13
Table 4-8. 2012 Lincoln County Hunger Facts.................................................................................. 14
Table 4-9. 2012 Lincoln County Youth Hunger Facts ....................................................................... 14
Table 4-10. Employment Data ............................................................................................................ 15
Table 4-11. Oregon Children with Disabilities – 2011 ........................................................................ 15
Table 4-12. EI/ESCE Report Card – 2010-2011 School Year .............................................................. 16
Table 4-13. Rental Costs in Lincoln County School District ............................................................... 17
Table 4-14. Housing Units without Plumbing, 2006 – 2010 ................................................................ 18
Table 4-15A. HRSA-Generated Data for HPSA .................................................................................... 18
Table 4-15B. HRSA-Generated Data for MUA/P .................................................................................. 19
Table 4-16. Pediatric and Family Medical Providers Accepting Medicaid ........................................... 21
Table 4-17. Institutional Medicare and Medicaid Providers, Second Quarter, 2011 ............................. 21
Table 4-18. Medical Information for CSCHS Enrolled Children 2011-2012 School Year .................... 22
Table 4-19. Medical Information for CSCHS Enrolled Children 2011-2012 School Year .................... 22
Table 4-20. Mental Health Information for CSCHS Children 2011-2012 ............................................ 24
Table 4-21. OHP Dental Providers in Lincoln County ........................................................................ 24

Community Assessment 2012-2013
1
1.0 SUMMARY
1.1 Executive
In alignment with the previous two years‟ brief Community Services Consortium‟s Head Start (CSCHS)
Community Assessment (CA) updates, there have been no significant demographic differences in Lincoln
County‟s basic data aside from the increase in poverty levels and continuing un-/under-employment
levels. While these on-going statistics can be somewhat attributed to the continuing recession, the County‟s service-based, lower-wage industry, and a lack of affordable housing, continue to be
problematic barriers to raising the standard of living and thus lowering poverty and unemployment levels.
There are, however, developments in play since the 2010 triennial assessment that are encouraging:
Oregon‟s federally supported pilot for health care reform (including Healthy Kids and potential for
influx of medical providers)
Coordinated Care Organizations (CCO), medical care homes, expanded Medicaid services/client base
Restructure of the Commissions on Children and Families into Early Learning Hubs (negative and/or positive effects on the Head Start program has yet to be realized)
After a highly competitive process, Lincoln County secured relocation of the west coast‟s National Oceanographic and Atmospheric Administration (NOAA) Marine Operations Center-Pacific on the
south shore of Yaquina Bay in Newport; this renowned research organization is expected to provide a
$20 million dollar per-year boost to the local economy.
In review of overall performance and perception of the CSCHS, it is noted that improvement of services
to its children and families coupled with its reputation as a model of partnership in early childhood
learning has increased significantly when compared to the 2010-2011 CA. Interviews and collaborative
meetings with community partners reflects the positive appreciation as do the increase in CLASS scores and creation of solid infrastructure, including comprehensive policies and procedures and an ongoing
monitoring tool. Staff pursuit of higher education and attainment of degrees and certifications continues,
and notably all program staff have developed educational plans.
Additionally, parent satisfaction remains high both with program and ancillary services, and staff have
high morale and demonstrate sustainable commitment to excellence as evidenced by discussion with the
CSCHS Director and various administrative and program staff. CSC itself is a continuing source of
program and family support through internal and partnered community-based referrals. It is also important to note that eight of twenty-five CSCHS staff members began as Head Start parents and should
be lauded both for importance to programmatic success and in reflecting positive and sustainable changes
this systemic program can engender to those in isolation and poverty.
The CSCHS Health Services Advisory Committee (HSAC) has proved itself as a vital component of the
resources in the Program‟s collaborative toolbox. The meetings occur quarterly and are substantive, and
the cross-section of involved disciplines reveals a strong community basis of support for the health and
well-being of the children and families engaged in CSCHS. The outcome measures and statistics reported monthly depict a well-monitored and developed system of assisting children and families in accessing
needed physical and dental health services. This aspect of the program is one of the strongest in spite of
difficulties operating a thriving program in a Health Professional Shortage Area (HPSA) as defined by the
Department of Health and Human Services‟ Health Resources and Services Administration (HRSA).
The monthly Eligibility, Recruitment, Selection, Enrollment and Attendance (ERSEA) reports I reviewed
show the Newport program site to contain the largest waitlist of the three CSCHS sites. While Toledo
historically has been considered as suffering the highest levels of poverty in the County, it is Newport that
now counts the highest level of poverty. The Newport site, according to the CSCHS Director, is showing increasing need for service expansion; Lincoln City continues to have the highest enrollment. Lastly,
South County (Waldport and Yachats) continues to show great interest in containing its own Head Start

2
site, and CSCHS has shared conversation with community members, electeds, and partners to talk about
the need and resources (human and capital) that would be required for such expansion. Currently there are no sustainable expansion funds available.
Finally, and perhaps most importantly, community information outlined in this report was of no surprise
to the CSCHS Director, and she continues to be responsive in addressing any specific concerns expressed
to her from program families and/or community at large. With a variety of changes anticipated at the State level, funding and/or broad organizational governance, there continues to be considerable opportunity
through forums and other public meetings in Lincoln County and elsewhere for partnership-building and
other collaborative efforts. The next years will be of critical significance to CSCHS‟ longevity and
structure (as well as other Oregon Head Start programs), and annual CA updates will track changes as they manifest.
1.2 Data
Based on information obtained through written survey; provider, Director, staff interviews; and available
statistical, historical and experiential data; the following areas have been identified as priority needs for low-income residents with pre-kindergarten children in Lincoln County, Oregon:
1.2.1 Basic Needs Services
Basic needs services continue to be a priority. Respondents reported concerns about food, shelter, utility,
and transportation. The level of these needs demonstrates the continued importance of mobilizing both
public and private entities to ensure that sufficient affordable housing, basic needs, and other community-based resources are available. Additionally, helping families to address basic needs is critical for
stabilization and prevention of episodic and/or long-term chronic homelessness. CSCHS staff, through
case management and advocacy, works directly with families to address any specific needs and concerns as they arise and provide referrals as appropriate.
1.2.2 Employment
Lincoln County residents continue to report employment and economic self-sufficiency as a significant
need. These reports are not surprising given the surge in the unemployment rate which reached 13% in Oregon generally and 9.5% in Lincoln County specifically in 2011 (was 8.5% in November 2012).
The economic stability needs of unemployed and underemployed Lincoln County residents can be
strengthened by helping link individuals to the many supports in the community including basic needs,
information about accessing state/other benefits, employment and training, and financial education supports. Life Skills education, including budgeting and household management assistance, are also
important steps that should be taken to enhance work toward self-sufficiency.
1.2.3 Housing
The Department of Housing and Urban Development (HUD) estimates that housing costs should reflect
30% of a family‟s income1. With affordable housing at a premium in Lincoln County, the ability of
families to afford a home is slipping further out of reach. The significant numbers of individuals reporting
a concern with housing issues clearly underscores the need for a concentrated effort to alleviate the strain
on families caused by the high cost of decent, safe housing2. The surge in unemployment and continuing
high foreclosure rates has placed additional strain on low-income individuals and families, which also
contributes to an increased risk in homelessness.
Workforce housing (including affordable housing for lower-income households) is increasingly in
demand and unavailable as any remaining available housing and land are being purchased and developed
1 www.hud.gov. 2 See Table 4-13 for cost of housing in Lincoln County.

3
as vacation homes. This housing type rents in off-seasons for greater amounts which, effectively, remove
any decent affordable housing from the market; what is left in affordability isn‟t always decent or safe.
1.2.4 Childcare
Affordable child care remains a significant need in Lincoln County, and greater numbers of working low-
income families indicate need for financial assistance with child care. Additionally, there is need for safe,
affordable, and flexible day care to aid a family‟s employment searches. Although employment-related
day care (ERDC) is available to low-income families through Oregon Department of Human Services, the legislatively approved caseload and funding opportunities don‟t adequately meet the need.
1.2.5 Transportation
Transportation continues to be an issue especially for lower-income residents. While the greater
percentage of CSCHS families report ownership of a running vehicle which can travel at least 50 miles, cost of gas and car repairs often bar use. CSCHS makes every effort to assist families with identified
transportation issues in connecting with other agencies and/or transportation services which might assist.
CSCHS families are encouraged to build carpool and other transportation-sharing options as well.
Ultimately, the need for reliable, flexible, and affordable public transportation presents as a contributing barrier to economic self-sufficiency and an improved quality of life.
1.2.6 Health
As previously written, the entirety of Lincoln County is considered a Health Professional Shortage Area
(HPSA) and additionally lists parts of the county as Medically Underserved Areas/Populations (MUA/P). This designation very much supports the reality that shortages exist in all aspects of health care in Lincoln
County, whether the need is in physical, mental, or dental health services. Most importantly, this medical
professional shortage is doubly concerning for children and families who are participants of Oregon‟s Medicaid program, Oregon Health Plan (OHP), as there are even fewer of the existing medical
professionals who accept this insurance option. Pediatric specialists who accept OHP are few, and in the
case of mental health professionals and dentists, there are none listed directly in Lincoln County in the
OHP provider network.
While there are regional transportation options available – free to obtain medical services in adjoining
counties through OHP – the reality is that a greater provider network locally is a severe need and deserves
– along with housing – greater community focus.
1.2.7 Education
With the fourth-lowest high school graduation rate as a state3 (National is 78%, Oregon is 66%, Lincoln
County is 65%), there clearly remains a solid need to address educational challenges. Survey respondents
report the need for enhanced education programs including improved literacy education, English as a
Second Language (ESL) support, and GED preparation, which clearly demonstrates the need to continue to develop and maintain comprehensive educational supports for children and adults alike. Through
improved educational outreach and programming, high school drop-out rates can be reduced and the
ability of residents to maintain longer-term economic self-sufficiency increased.
3 Ed.gov; “Regulatory Adjusted Cohort Graduation Rate, All Students: 2010-11”.

4
2.0 COMMUNITY ASSESSMENT
2.1 Purpose and Scope of Project
The purpose of this report is to present the results of a Community Assessment (CA) for CSCHS. A CA is
the collection and analysis of information on the needs and characteristics of Head Start (HS) eligible
children and families in a grantee‟s service area. Further, it identifies issues and trends that impact
families with young children and programs and community resources available to meet the family needs. A completed CA is used to guide program planning and evaluation decisions.
Every three years the National Head Start Program, through its Federal funder, Department of Health and
Human Services (HHS), requires all Head Start programs to conduct a full or extensive CA, and 2013 is
CSCHS‟s full report year (updates will be completed in each of the two years following the full CA). There are six content areas that must be included in a CA (labeled A1-A6):
1. A1: The estimated number, geographic location, and racial/ethnic composition of Head Start children 2. A2: Other child development programs that serve Head Start eligible children and the approximate
number served 3. A3: The estimated number of children four years old or younger with disabilities and services
provided to these children
4. A4: Data regarding the education, health, nutrition and social service needs of Head Start eligible
children and their families 5. A5: The education, health, nutrition and social service needs of Head Start eligible children and their
families as defined by families of Head Start families and by community institutions that serve young
children 6. A6: Community resources that could be used to address the needs of Head Start eligible children and
their families.
To most accurately and contextually present the requisite information, this report is organized into the
following sections:
Summary Geographic Area
Community Assessment Conclusions and Suggestions
Head Start Appendixes
2.2 Methodology
Information contained in this report was obtained from a variety of sources including written documents,
personal interviews, and the writer‟s own knowledge and understanding. Chief among the research
reports and tools accessed to determine specific demographics were: U.S. Census Bureau 2010 data and
American Community Survey; Children First for Oregon; Children‟s Defense Fund; Oregon Head Start‟s Program Information Report (PIR) summarized for Oregon HS programs/grantees; CSCHS internal
documents (e.g., 2011 PIR, newsletters, budget, and Governing Board presentation materials); and
information obtained through website review of various Lincoln County service providers and studies (e.g., Healthy Start, WIC, etc., 10-Year Plan to End Homelessness, Commission on Children and
Families‟ Assessment, etc.).
An informational survey was also designed by this writer and subsequently completed by 56% of the
current CSCHS parents of children participating at all three classroom sites. Further, person-to-person interviews were conducted and/or phone conversations were held with staff members from Lincoln
Commission on Children and Families; Olalla Center; Lincoln County Commissioners; Lincoln County
Health Department; Linn, Benton and Lincoln Education Service District; and Lincoln County school
district.

5
3.0 HEAD START
3.1 What is Head Start?
Head Start is a national program which provides comprehensive developmental services for America's
low-income, pre-school-aged children (three to five years) and social services and supports for their
families. Approximately 1,400 community-based non-profit organizations and school systems nationally
develop unique and innovative programs to meet specific needs.
Head Start began in 1965 in the Office of Economic Opportunity and is now administered by the
Administration for Children and Families. In FY2012, $7,9 billion4 was available for Head Start services
nationally and awarded to local public or private non-profit agencies; 20% of the total cost of a Head Start
program must be contributed by the community. Head Start programs operate in all 50 states, the District of Columbia, Puerto Rico, and the U.S. territories.
3.1.1 Major Components
Head Start provides diverse services to meet the goals of the following four components:
Education – Head Start's educational program is designed to meet the needs of each child, the community served, and its ethnic and cultural characteristics. Every child receives a variety of learning
experiences to foster school readiness by enhancing intellectual, social, and emotional growth.
Health – Head Start emphasizes the importance of early identification of health problems. Every child is involved in a comprehensive health program which includes immunizations, medical, dental, mental
health, and nutritional services.
Parent Involvement – An essential part of Head Start is the involvement of parents, as they are their
children‟s primary teachers and advocates. Parent engagement includes parent education, program planning, and operating activities. Many parents serve as members of policy councils and committees
and have a collaborative voice in administrative and managerial decisions. Participation in classes and
workshops on child development and staff visits to the home encourages parents to learn about the needs of their children and educational activities that can take place at home as well as information-
sharing with the teacher about their child‟s development.
Social Services – Specific services are geared to each family after needs are determined and could include community outreach; referrals; family need assessments; recruitment and enrollment of
children; and emergency assistance and/or crisis intervention.
Only 3% percent of eligible children are able to secure spots in Head Start due to limited funding (see Table 3-1 for enrollment information about Head Start Preschool)
5.
Table 3-1. Early Head Start and Head Start Enrollment 2010
4 http://www.acf.hhs.gov/programs/ohs/news/fy-2012-head-start-funding-increase-0 (HHS Administration for Children & Families); funding level represents an increase of approximately $409 million over the FY 2011 appropriation level. 5 National Women’s Law Center. 2011. “Head Start: Supporting Success for Children and Families”;
http://www.nwlc.org/sites/default/files/pdfs/head_start_fact_sheet_2011.pdf.

6
The annual cost of center-based pre-school for a four-year old is more than the annual in-state tuition at a
public four-year college in 26 states and the District of Columbia6, and 30% of children in poverty score
very low on early reading skills when compared to only 7% percent of children from moderate- or high-
income families7. Without high-quality early childhood intervention, an at-risk child is:
25% more likely to drop out of school
40% more likely to become a teen parent
50% more likely to be placed in special education
60% more likely never to attend college
70% more likely to be arrested for a violent crime8.
3.2 Grantee Description
Head Start is one of the nation‟s first child development programs to implement a two-generation approach, working with both children and their low-income parents as primary teachers of their own
children. Teachers are also „advocates‟ for the children and their families. In 2012-2013, CSCHS will provide federal- and state-funded preschool services to 160 Lincoln County children and their families
through classroom sites in Toledo, Newport, and Lincoln City, though the actual numbers served may
vary depending upon funding changes.
CSC began serving Head Start children and families of Lincoln County in August 1996. The program currently provides services to 160 three and four year old children from 155 families. The 160 children
are funded as follows: 102 are federal Head Start funded and 58 are Oregon Pre-Kindergarten funded. Children receive center-based services where they are offered 3.5 hours of classroom service four days a
week and four teacher conferences throughout the year, two of which are home visits. Center-based
classes are held in the cities of Lincoln City, Newport, and Toledo. The most recently opened location is Newport in May 2009. For program year 2011-2012, CSCHS‟s total budget was $1,436,585 and included
17.83 full-time equivalent staff.
CSCHS supports and understands that:
Low-income children who are hungry, have never been to the doctor, who have few or no books at home, who are more likely to view violence have different needs than their middle- or upper-income peers and
can benefit from the program. Eligible children benefit from intensive, targeted, community-based
services resulting in greater school and life success because of Head Start (see Table 3-2).
Research indicates9 that Head Start generates long-term improvements in important outcomes such as
schooling attainment, earnings, and crime reduction.
CSCHS‟s programming foundation is based on parent and service provider partnerships and, with the assistance of on-going and new community connections, meets its measureable outcomes through:
Supporting at-risk Lincoln County families in achieving successes and self-sufficiency with dignity
Providing experiences for enrolled pre-school children to grow socially, emotionally, physically, and
mentally
Providing every parent with opportunities to participate in program shared-decision-making
Connecting families to necessary community services and other opportunities geared toward stabilization.
6 “Double Jeopardy: How Third-Grade Reading Skills and Poverty Influence High School Graduation”; The Annie E, Casey
Foundation; Hernandez, Donald J.; April 2011. 7 Brookings Institution. 2012. “Starting School at a Disadvantage: The School Readiness of Poor Children.”
http://www.brookings.edu/~/media/research/files/papers/2012/3/19%20school%20disadvantage%20isaacs/0319_school_disadvantage_isaacs.pdf.
8 Center for American Progress. 2012. “Increasing the Effectiveness and Efficiency of Existing Public Investments in Early
Childhood Education: Recommendations to Boost Program Outcomes and Efficiency.” http://www.americanprogress.org/issues/2012/06/pdf/earlychildhood.pdf.
9 “Longer-Term Effects of Head Start” (NEBR Working Paper No. 8054); Eliana Garces, Duncan Thomas, and Janet Currie; 2001.

7
Table 3-2. CSCHS 2012-2013 School Year Current Comprehensive Statistics Health
CSCHS promotes child school-readiness and family self-sufficiency through comprehensive and
intensive services including early childhood education, health and social services, nutritious meals, and
parent partnership and involvement. Through 11 primary domains of learning10
(aligned with the Head
Start Child Development and Early Learning Framework which is in the process of being adopted by the Oregon Department of Education as the early learning standards for children ages 3-5) and an overall
structure for school-readiness, children‟s progress is measured, adjusted, and reviewed with outcome
measurement tools including Galileo Pre-K Online assessment and Classroom Assessment Scoring System (CLASS).
Children are expected to make a 50-point gain in skills (from first assessment to final rating) over the
school year for each of the learning domains. CSCHS Developmental Level (DL) scores exceeded
expected gains in each domain; average point gain was 131 as evidenced by the following Table 3-3.
Table 3-3. CSCHS 2011-2012 School Year Current Comprehensive Statistics CSCHS Developmental Level (DL) scores
10 Physical Development & Health, Social & Emotional Development , Approaches to Learning , Language Development,
Literacy knowledge & Skills, Mathematics knowledge & Skills, Science knowledge & Skills, Creative Arts Expression, Logic
& Reasoning, Social Studies knowledge & Skills, English Language Development (for dual-language learners).
Statistics
Oct
2012
Nov
2012
Dec
2012
# of enrolled children with up-to-date/all possible immunizations to date 137 142 142
# of enrolled children on schedule of preventative/primary health care
(up-to-date physical exam) 105 120 123
# of enrolled children with ongoing source of continuous, accessible health care
(Medical Home) 152 156 155
# of enrolled children completing professional dental exams 89 102 108
# of enrolled children with continuous, accessible dental care provided by a dentist
(dental home) 151 152 151
Developmental Domain
Beginning of
Year End of Year
Point Gain
50 Expected
Percentage
Increase
Approaches to Learning 467 609 142 30%
Creative Arts 495 661 166 34%
Early Math 463 587 124 27%
English Language Acquisition 473 555 82 17%
Language 430 574 144 33%
Literacy 444 579 135 30%
Logic and Reasoning 508 630 122 24%
Nature and Science 438 586 148 34%
Physical Development & Health 449 576 127 28%
Social and Emotional Development 428 558 130 30%
Social Studies 477 597 120 25%

8
3.2.1 Lincoln County Need
CSCHS is a vital program that supports the enrolled children, families, and connected communities
within Lincoln County. In the 17 years the Program has been housed within CSCHS, the numbers served per year has increased from 97 to 160 through award of competitive grants both federal and state (see
Table 3-4). In 2011, the Program counted 86 eligible children/families on the waiting list (see Table 3-5).
The unfortunate truth is that:
Preschool children are the most likely age group to live in poverty Oregon is consistently included in national statistics as posting some of the highest unemployment and
food insecurity rates
Lincoln County has one of Oregon‟s highest domestic violence rates per capita and the second highest county child abuse rate (nearly twice the state‟s average)
Pre-school children need to have a safe space in which to learn developmentally appropriate
educational and social-emotional skills and receive support to ensure school readiness
Table 3-4. CSCHS 2012-2013 School Year Current Comprehensive Statistics Enrollment, Attendance, and Meal & Snack Report
Table 3-5. CSCHS 2012-2013 School Year Current Comprehensive Statistics Wait List Monthly Count
Poverty Income 130% Income Over Income Total Applications
Total Program Site T N LC T N LC T N LC T N LC
As of 10/25/2012 8 12 4 0 3 2 5 14 4 13 29 10 52
As of 11/5/2012 7 14 8 1 3 2 5 14 4 14 31 13 58
As of 12/5/2012 7 14 9 1 4 2 5 14 4 13 32 15 60
As of 1/4/2013 8 14 3 1 4 2 5 1 5 14 32 10 56
Month Enrollment Attendance Breakfast/Snack Lunch Total Meals
September 2012 160 91.22% 1,410 1,417 2,827
October 2012 160 87.08% 2,379 2,418 4,797
November 2012 160 82.57% 2,152 2,164 4,316
December 2012 160 86.69% 1,446 1,468 2,914
Totals 86.89% 7,387 7,467 14,854

9
4.0 GEOGRAPHIC AREA
4.1 Oregon Poverty Overview
The Federal Poverty Line (FPL) is based on a 1955 household survey and, though updated annually,
relies on out-of-date assumptions. It fails to address the impact of today‟s high housing, health, and child
care costs or even work-related expenses. The resulting “official” poverty rates seriously underestimate
the “real” poverty:
FPL for a family of four = $23,050 (2012)
Full time job at Oregon minimum wage = $18,304 (2012)
Full time job at Federal minimum wage = $15,080 (2012)
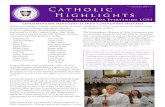
Basic Family Budget for a family of four in Oregon for 2012 = $50,304 (see graph below)
Though Oregon‟s minimum wage increased January 1, 2013, four-person households with two full-time
workers earning minimum wage (combined $37,232) is still less than 200% of the FPL. While many Oregonians did get the „boost‟ to help make ends meet, two incomes is a comfort few households have.
74% of households surveyed in a 2012 Oregon Food Bank project reported incomes below 100% of FPL.
4.1.1 Basic Family Budget
Using the Economic Policy Institute‟s (EPI) “basic family budget” calculator as a model, the family
budget illustrated above was fine-tuned using more localized sources for some of the figures. EPI‟s study was published in 2007 and adjusted for 2012 inflation using the Consumer Price Index calculator (see
Figure 4-1). The calculations by EPI, a non-profit, non-partisan think tank, also include such essentials as
housing, food, child care, and health insurance. For a typical Oregon family, a basic family budget ranges from 197% to 231% of the Federal poverty line
11. More than 1.4 million Oregonians, about one-third, try
to survive with incomes below 200% of the FPL ($46,100 for a family of four)12
.
Figure 4-1. Basic Family Budget – 2010 vs. FPL
11 Economic Policy Institute, Basic Family Budget Calculator, http://www.epi.org/budget_form.cfm?CFID=3447799&CFTOKEN=41949049. 12 U.S. Census, American Community Survey 2011; http://factfinder2.census.gov/faces/tableservices/jsf/pages/productview.xhtml? pid=ACS_11_1YR_S1701&prodType=table.

10
4.1.2 Living Wage
A living wage is one that allows families to meet their basic needs without resorting to public assistance
and one which provides some ability to deal with emergencies and plan ahead.
In 2010, the living wage for a single adult in Oregon was $15.20/ hour. Of all job openings in Oregon in
2010, 52% paid less than 15.20/hour; for job openings that pay at least $15.20 per hour, there are at least
14 seekers on average13
4.2 Lincoln County
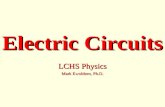
Lincoln County is primarily rural, and Newport serves as
the County seat. It has a total area of 1,194 square miles
about the size of Rhode Island. In terms of boundaries,
the county is bordered by the Pacific Ocean to the west, Tillamook County to the north, Polk County to the
northeast, Benton County to the southeast, and Lane
County to the south. Lincoln County has seven unique
incorporated communities: Depoe Bay, Lincoln City, Newport, Siletz, Toledo, Waldport, and Yachats.
The county's economy is based on services, tourism, trade, commercial fishing, food processing, paper
processing, and wood and lumber products. The economy is also supported by a large and increasing
number of retirees.
According to the 2010 US Census, Lincoln County families experience higher levels of poverty at 11.6%
as compared to the statewide rate of 11.0%.
Children are also greatly impacted by the recent poverty trends, counting approximately 39% of all
children in Oregon living in families with low incomes who cannot meet their basic needs for food and shelter. According to Patricia Post‟s report
14, some economists estimate that persistent childhood poverty
costs the United States roughly $500 billion a year by way of lost productivity, school drop-outs, crime,
and the growing numbers enrolled in nutrition and public assistance programs. Solving poverty is beyond the scope of this needs assessment, but it can point the way to a variety of near-term and longer-term
approaches to mitigate its most serious impacts. Every forward step taken as a co-productive community
will bring multiple benefits.
According to Jeffery Bartash of MarketWatch.com, even those traditionally living above the poverty level saw their earning power decline, with 2011 median income falling 2.9% from 2009, the second sharpest
decline on record. Some estimates indicate that more than 55 million people in the United States will need
assistance to meet their basic needs in the coming years.
The State of Oregon is 13th in the nation in economic recovery and, as we know, economic upheavals have a disproportionately negative impact on lower-income families as they enter the unemployment
lines, see a reduction in work hours and wages, and fight rising interest rates on credit debt, all of which
have the greatest impact on those who can afford it the least.
4.2.1. Population
2010 poverty estimates show a total of 7,734 persons living below the poverty rate in Lincoln County
with more than one in ten (17%) of all families living below the poverty line (FPL)15
(see Table 4-1).
13 2010 Job Gap Study http://nwfco.org/wp-content/uploads/2010/12/2010-1209_2010-Job-Gap.pdf. 14 “Hard to Reach: Rural Homelessness and Health Care,” http://www.nhchc.org/wp-
content/uploads/2012/02/October2001HealingHands.pdf. 15 U.S. Census Bureau, Small Area Income and Poverty Estimates (SAIPE), 2010.

11
Table 4-1. Lincoln County Poverty Information, 2010
Geographic Area
All Ages Age 0-17 Age 5-17
Number
of Persons
Poverty
Rate
Number of
Persons
Poverty
Rate
Number of
Persons
Poverty
Rate
Lincoln County, Oregon 7,734 17.0 2,325 30.1 1,538 28.3
Oregon 596,649 15.8 184,511 21.7 119,412 19.5
United States 46,215,956 15.3 15,749,129 21.6 10,484,513 19.8
Table 4-2 shows overall population changes in the United States, Oregon, and Lincoln County from 2000
to the 2010 census.
Table 4-2. Population Changes 2000 to 2010
4.2.1.1 Race and Ethnicity
Currently, the Hispanic16
population in Oregon is counted at 12%, while in Lincoln County this
population group is counted at 8.1%, an increase of 0.9% over the 7.2% listed in the 2010 community needs assessment report. The top needs identified for the Hispanic population via the CSHS Parent
Survey (see Appendix D) are employment, health care, legal assistance, ESL training, transportation (way
to obtain legal licenses), and affordable housing.
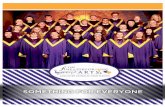
Table 4-3 shows median income of Lincoln County‟s Hispanic population, Table 4-4 shows childhood
poverty, and Figure 4-2 shows the lack of health insurance in Oregon by race. See the section on Health
Care (page 18) for information on Oregon‟s health care reform, coordinated care organizations and the
Healthy Kids initiative, all of which intends to increase the numbers of children covered by health insurance regardless of race.
CSCHS continues to respond to the needs of Spanish-speaking families by increasing interpreter hours,
making available bi-lingual forms, and hiring bi-lingual staff and engaging parent volunteers.
Table 4-3. Historical Median Household Income by Race – Lincoln County17
Race Lincoln County Oregon 10-Year
Average
U.S. 10-Year
Average 2006-2010 2005-2009 2000
Hispanic 30,097 36,167 33,500 35,294 38,718
White 40,189 38,315 32,956 47,177 51,407
16 For purposes of U.S. Census and American Community Survey data collection, the ethnic group Hispanic also includes any number of Latino populations. 17 American Community Survey 2000-2010
Geographic Area
Census 2000
Population
Census 2010
Population Population Change
%
Change
Lincoln County 44,479 46,034 1,555 3.50
Oregon 3,421,437 3,831,074 409,637 11.97
United States 281,424,602 312,471,327 31,046,725 11.03

12
Table 4-4. Poverty by Age, Hispanic Origin, Race: 2011 Census – National18
(Numbers in thousands)
Age and
Poverty
Status19
Total
Hispanic Origin and Race20
Hispanic
Non-Hispanic
Total White alone All other races
Number Percent Number Percent Number Percent Number Percent Number Percent
Under 18 years
74,494 100.0 17,435 100.0 57,059 100.0 40,494 100.0 16,565 100.0
Below poverty
16,401 22.0 6,110 35.0 10,291 18.0 5,002 12.4 5,289 31.9
At/above poverty
58,093 78.0 11,325 65.0 46,768 82.0 35,492 87.6 11,276 68.1
Figure 4-2. Uninsurance Rate by Race
Oregon Health Plan 20111
4.2.2 Poverty
Table 4-5 shows percentage of Lincoln County households in poverty by household type. In 2010, it is estimated that 11.67% of all households were living in poverty within the County compared to the
national average of 10.08%. Of the households in poverty, female headed households represented 40.66%
of all households in poverty compared to 8.15% and 51.20% of households headed by males and married couples, respectively.
Table 4-5. Household Poverty Rate by Family Type, 2006 - 2010
Geographic Area All Types Married Couples Male Householder Female Householder
Lincoln County 11.67 7.30 21.33 34.70
Oregon 9.60 4.81 16.49 30.27
United States 10.08 4.90 14.58 28.86
18 U.S. Census, American Community Survey 2011;
http://factfinder2.census.gov/faces/tableservices/jsf/pages/productview.xhtml? pid=ACS_11_1YR_S1701&prodType=table. 19 Poverty statistics exclude unrelated individuals under 15. 20 Hispanic refers to people whose origin is Mexican, Puerto Rican, Cuban, Spanish-speaking Central or South American countries, or other Hispanic/Latino, regardless of race.

13
Poverty rate change in Lincoln County 2000 to 2010 is shown in Table 4-6. According to the U.S.
Census, the poverty rate for the County increased by 3.1%.
Table 4-6. Change in Poverty Rate 2000 – 2010 Lincoln County
Geographic
Area
Persons in
Poverty 2000
Poverty Rate
2000
Persons in
Poverty 2010
Poverty
Rate 2010
Change in Poverty
Rate
2000 – 2010
Lincoln County 6,070 13.9 7,734 17.0 3.1
Oregon 361,280 10.6 596,649 15.8 5.2
United States 31,581,086 11.3 46,215,956 15.3 4.0
The poverty rate change for all children in Lincoln County from 2000 to 2010 is shown in Table 4-7. In
this case, the childhood poverty rate for the County increased by 7.5% compared to an Oregon increase of
6.6% and a national increase of 5.4%.
Table 4-7. Change in Childhood (0-17) Poverty Rate in Lincoln County 2000 - 2010
4.2.3 Food
According to 2012 Oregon Food Bank report21
, Oregon has higher-than-national-average rates for hunger
and food insecurity (currently 17.5% in Lincoln County). More than half (61%) of Lincoln County
students (k-12) qualify for free or reduced lunch, and more than 400 students in the school district are considered homeless (defined as living with relatives or friends, awaiting foster care, or living in an
emergency shelter, motel, campground, car or park).
Oregon Food Bank VOICES 2009 reported that families are making food choices based on cost or quality
when knowing that choosing healthy foods may mean not having enough food to last the month. On a state level, roughly one in six Oregonians receive food stamps (see Table 4-8). This number is the highest
in the history of the state program and well above the national average. The average food stamp benefit is
$176 a month or $1.96/meal, less than the $2.50/child Head Start is reimbursed. Food stamps are tied to match inflation, but in 2008 the drastic spike in prices kept the annual increase from keeping pace with
prices. Sixty-seven percent (67%) of food stamp recipients report that benefits last less than two weeks.
Access to food is difficult in pockets through the County. Residents in Eddyville, for example, must drive
more than 25 miles leaving those without transportation or mobility vulnerable22
. Rural grocery stores have become more or less convenience stores, offering little in the way of fresh produce or really
nutritious food. This is alarming considering many rural residents depend on these stores.
21 “Profiles of Hunger and Poverty in Oregon, 2012 Hunger Factors Assessment”; Oregon Food Bank. 22 A person is considered „food insecure‟ if she/he lives more than 10 miles or more from a grocery store.
Geographic
Area
Children in
Poverty 2000
Poverty Rate
2000
Children in
Poverty 2010
Poverty Rate
2010
Change in Poverty
Rate 2000 – 2010
Lincoln County 2,064 22.6 2,325 30.1 7.5
Oregon 127,544 15.1 184,511 21.7 6.6
United States 11,587,118 16.2 15,749,129 21.6 5.4

14
Each month, too many Lincoln County residents rely on emergency food assistance as a necessity to
make ends meet. Children are particularly vulnerable with before- and after-school program cuts, as these opportunities are often their most consistent source of food. Programs – such as the Backpack for Kids
program23
– rely on a precarious structure of volunteers and community donations. The East County
Backpack program serves 56 students in Toledo and Siletz with 30 to 40 more kids in need but no funding
for them to participate. Fortunately Lincoln City and Newport sites have backpack programs for their high need families and it is anticipated that Toledo will also have one in 2013 (see Table 4-9 for youth hunger
facts).
Poverty and low wages are the underlying causes for food insecurity in the region. High
underemployment and unemployment can be blamed to a degree, but living costs for basic monthly expenses including high rent, child care costs, and gas (currently hovering near $3.80/gallon) make even
those who work full-time at minimum wage food insecure.
Table 4-8. 2012 Lincoln County Hunger Facts
Table 4-9. 2012 Lincoln County Youth Hunger Facts
4.2.4 Employment
Labor force, employment, and unemployment data for Lincoln County is provided in Table 4-10. In
November 2011, the non-adjusted unemployment rate was 9.5%. October 2012 saw the rate drop to 8.6%,
and November 2012‟s rate was lower again at 8.8%. Nearly one third (29%) of the Lincoln County work
force is employed in the leisure and hospitality industry, the most common employment for non-skilled labor in the county. The average hourly wage for this industry is minimum wage, $8.80/hour
24, or roughly
$18,304 annually25
if the employee works full time.
23 See collaborative partner successes in Appendix A. 24 Oregon minimum wage rose to $8.95/hour January 1, 2013. 25 Oregon employment Department Covered Employment and Wages, Q3 2012.
Food Insecurity 17.5%
SNAP Users 18.9%
SNAP $ into the County $13 Million
SNAP Participation Rate 71%
Food Boxes 13,580
Minimum Wage Hours for a 1 Bdrm Apartment 56 hours/week
Cost per Meal $2,84
County Health Outcomes 27th
Free/Reduced-Meal Eligibility 67.4%
Free/Reduced-Meal Participation Rate 62.6%
Summer Meals (served 2010) 15.144
Backpack Programs 3
Homeless Students 471
Childhood Obesity 28.9%

15
Table 4-10. Employment Data
According to WorkSource Oregon‟s Labor Force and Unemployment estimates26
– November 2012 – the
county labor force consisted of 22,342 people. Employment levels tend to fluctuate throughout the year
due to dependence on seasonal employment activities like tourism, food processing, and fishing, and the underemployment level includes the unemployed and also people who work part time but would like to
work full time. Rather than hiring new employees when the economy improves, companies probably will
move these employees to full time, meaning an unchanged jobless rate. Therefore, unfortunately, there is
a direct correlation between unemployment and poverty; as unemployment increases so does poverty. All this serves as important context information when examining HS eligible children and families in Lincoln
County.
It is evident that economic hardship exists in all areas of the County and that job losses continue through all industries. However, it is interesting to note that health care and government job losses are new trends,
with 11.8% and 2.3% labor decreases, respectively. Additionally, the population is slow to grow with the
baby-boom generation aging into retirement and the Latino population is the 2nd
highest impoverished
population group. Ultimately, the CSCHS wait list demographics is an indicator of where services are needed and confirms current service locations are appropriately placed throughout the County.
4.2.5 Children with Disabilities
Partnership with Early Childhood Special Education (ECSE) is a very successful collaboration in Lincoln
County (see Appendix E for Provider Interviews). By December of 2012, 20 CSCHS children, or 13% of total enrollment, had been identified with special needs and appropriately referred to ECSE for further
evaluation and services. The partnership is important as it serves a vulnerable and high-need population,
and addresses the necessity of preparing these children for mainstream school readiness. According to
Oregon Department of Human Services27
, 108 children in Lincoln County received on-going case management services in 2011.
Table 4-11 shows numbers of Oregon children with disabilities divided by urban and rural locations.
Table 4-11. Oregon Children with Disabilities – 2011
The Oregon Department of Education contracts with nine Education Service Districts (ESDs) across the state to provide early intervention/early childhood special education (EI/ECSE) services in 33 local
programs. This system includes Part C early intervention (EI) for children birth to age three and Part B
26 Oregon Labor Market Information System; http://www.qualityinfo.org/olmisj/DoQuery?itemid=00004804. 27 DHS Developmental Disabilities Data Book – 2011.

16
early childhood special education (ECSE) for children age three to kindergarten age, which is age five in
Oregon. Children who are age five by September 1 are eligible for public school with special education services provided by the local school district.
In Lincoln County, the Linn-Benton-Lincoln ESD in Albany administers this opportunity, and the Lincoln
County School district provides an in-house administrator who reviews referred children against these
disability eligibility criteria and disorders: communications; autism spectrum; hearing, visual, orthopedic and other impairments; specific learning disability; emotional disturbance; intellectual disability;
deafness; blindness; traumatic brain injury; early intervention. Table 4-12 demonstrates the effectiveness
of specific EI/ECSE measures in preparing children for school-readiness in Lincoln County28
. The full
Report Card and additional measures can be accessed via the web link in Footnote 34.
Table 4-12. EI/ESCE Report Card – 2010-2011 School Year
Improved Outcomes in Positive
Social-Emotional Skills Program
State
Target
Infants and toddlers who entered or exited early intervention below age
expectations and substantially increased their rate of growth by
age 3 or when they exited the program
92.3% 80.9%
Infants and toddlers who were functioning within age expectations by age 3 or
when they exited the program
71.4% 59.1%
Preschool children who entered the preschool program below age expectations
and substantially increased their rate of growth by
age 6 or when they exited the program
86.4% 74.3%
Preschool children who were functioning within age expectations by age 6 or
when they exited the program
26.9% 32.5%
Improved Acquisition and Use of
Knowledge and Skills Program
State
Target
Infants and toddlers who entered or exited early intervention below age
expectations and substantially increased their rate of growth by
age 3 or when they exited the program
85.7% 63.7%
Infants and toddlers who were functioning within age expectations by age 3 or
when they exited the program
<5.0% 7.3%
Preschool children who entered the preschool program below age expectations and substantially increased their rate of growth by
age 6 or when they exited the program
61.9% 60.5%
Preschool children who were functioning within age expectations by age 6 or
when they exited the program
19.2% 23.6%
Improved Use of Appropriate
Behaviors to Meet Needs Program
State
Target
Infants and toddlers who entered or exited early intervention below age
expectations and substantially increased their rate of growth by
age 3 or when they exited the program
76.9% 64.4%
Infants and toddlers who were functioning within age expectations by age 3 or
when they exited the program
7.1% 18.1%
Preschool children who entered the preschool program below age expectations
and substantially increased their rate of growth by
age 6 or when they exited the program
57.1% 44.8%
Preschool children who were functioning within age expectations by age 6 or
when they exited the program
23.1% 31.7%
28 Oregon Department of Education; http://www.ode.state.or.us/data/reportcard/sped/SPEDpdfs/12/12-SpEdReportCard-Conf-
EC21.pdf.

17
4.2.6 Housing
The combination of high demand, a limited base of buildable land, and low wages have worked in concert
to create a workforce housing crisis in Lincoln County beyond the continuing and growing need for clean, safe, and affordable low-income housing. Even the burst of the housing bubble that helped precipitate the
recession did not reverse the fact that in a span of two decades, housing prices grew twice as fast as
wages29
(see Table 4-13). The fair market rent of a 2 bedroom unit in Lincoln County is $659/month30
, and the estimated average hourly wage for a Lincoln County renter is $8.80. The affordable rent, typically
no more than 30% of gross monthly income31
would be $441. This means that the average renter in
Lincoln County would need to work ten hours a day, seven days a week to afford the fair market value of
a 2-bedroom unit32
. A list of supported affordable housing in Lincoln County is available in Appendix G.
The Lincoln County Workforce Housing Needs Assessment completed in 2011 found that rental rates in
the county are high. Much of the rental units available, both apartments and homes, are older, often not in
good repair (See Table 4-14), and lack many of the amenities renters require. Lacking affordable housing brings unintended consequences such as difficulty in attracting and retaining qualified workers, and many
workers are often forced to commute long distances (into Benton County, for example) from their homes
as they find themselves (doctors, teachers, service workers in leisure and hospitality employment) priced
out of the rental market. Many workers even double-bunk with friends and/or family or „rough‟ sleep in campers and cars just to maintain even part-time employment.
Table 4-13. Rental Costs in Lincoln County School District33
Additionally, the practice by property owners and funders alike34
to require individuals to have no felony
convictions may exclude the majority of individuals in early recovery and those whose life history
includes criminal activity. For some CSCHS families, this may create another barrier to housing that is
insurmountable especially given limited affordable housing options and employment suitable for ex-offenders.
29 Lincoln County Workforce Housing Needs Assessment 2011. 30 HUD Data Sets, http://www.huduser.org/portal/datasets/fmr.html. 31 The U.S. Census Bureau considers a family to be cost-burdened if it is paying more than 30 percent of its gross income for
housing and severely cost burdened if it is paying more than 50 percent of its gross income for housing. In Lincoln County,
more than half (56.8 percent) of all households are paying 30 percent or more of their monthly income for housing. 32 National Low Income Housing Coalition – Out of Reach 2012. 33 USA.com Lincoln County Oregon School District; based on 2006-2010 data. 34 http://www.rurdev.usda.gov/SupportDocuments/3560-2chapter06.pdf.
Monthly Rental Lincoln County School District % Oregon U.S.
Occupied Units Paying Rent 6,408 100% 519,755 35,969,315
$199 or Less 229 3.57% 1.89% 2.25%
$200 to $299 348 5.43% 2.35% 3.41%
$300 to $499 849 13.25% 8.10% 9.80%
$500 to $699 1,866 29.12% 23.34% 19.41%
$700 to $999 1,974 30.81% 37.56% 29.88%
$1,000 to $1,499 927 14.47% 20.25% 23.51%
$1,500 to $1,999 144 2.25% 4.52% 7.56%
$2,000 or More 71 1.11% 2.00% 4.16%
Median $692 - $795 $841

18
The number and percentage of occupied housing units without plumbing in Lincoln County are shown in
Table 4-14. U.S. Census data shows 128 housing units were without plumbing in 2000 while a decreased 74 housing units without plumbing were reported in 2010. While lack of plumbing is a tremendous issue,
it is not uncommon to find lower-income housing rife with holes in floors, roofs, and walls; heating
systems that don‟t work (rental and owner-occupied), electrical issues that are dangerous for children, etc.
Unfortunately, these types of units are often the only ones available for a population with low-income, bad credit, and any number of other personal issues. Additionally, housing inspections which are required
of rental assistance programs and Section 8 housing vouchers will „fail‟ such housing in disrepair and
thus effectively „remove‟ additional available housing from the low-income renter.
Table 4-14. Housing Units without Plumbing, 2006 – 2010
Geographic
Area
Occupied
Housing
Units, 2000
Housing
Units
without
Plumbing,
2000
Percent
without
Plumbing,
2000
Occupied
Housing
Units, 2006-
2010
Housing
Units
without
Plumbing,
2006-2010
Percent
without
Plumbing,
2006-2010
Lincoln County,
Oregon
19,296 128 0.48 20,652 74 0.36
Report Area 19,296 128 0.66 20,652 74 0.36
Oregon 1,333,723 7,025 0.48 1,499,267 9,729 0.65
United States 106,741,426 736,626 0.69 114,235,996 602,324 0.53
4.2.7 Health Care
According to the Department of Health and Human Services‟ Health Resources and Services
Administration (HRSA), the entirety of Lincoln County is considered a Health Professional Shortage
Area (HPSA) and additional lists parts of the county as Medically Underserved Areas/Populations (MUA/P).
HPSAs are designated by HRSA as having shortages of primary medical care, dental, and/or mental
health providers and may be geographic (a county or service area), demographic (low-income population)
or institutional (comprehensive health center, federally qualified health center or other public facility). MUA/Ps are areas or populations designated by HRSA as having too few primary care providers, high
infant mortality, high poverty and/or high elderly population. Tables 4-15A and 4-15B provide HRSA
data specific to Lincoln County.
Table 4-15A. HRSA-Generated Data for HPSA35
Criteria:
State: Oregon County: Lincoln County ID: All
Date of Last Update: All Dates
Discipline: Primary Medical Care, Dental, Mental Health Metro: All Status: Designated Type: All
35 Of particular interest are the columns marked „FTE‟ and „# Short.‟ People attempting to be served in the County are well aware of the shortages in providers.

19
HPSA Score (lower limit): 0
Results: 21 records found. (Satellite sites of Comprehensive Health Centers automatically assume the HPSA score of the affiliated grantee. They are not listed separately.)
HPSA Name ID Type FTE # Short Score
041 - Lincoln County
Lincoln 741041 Single County 1 1 18
Lincoln County Health and Human Services 141999412M Comprehensive Health Center
0 2
Coastal Health Practitioners 141999412Q Rural Health Clinic
0 16
Lincoln City Medical Center 141999412R Rural Health Clinic
0 16
Siletz Community Health Clinic 141999413R Native American Tribal
Population 0 13
Delake/Depoe Bay 141999413X Geographical Area 5 1 8
Depoe Bay CCD
Minor Civil Division
Lincoln City CCD
Minor Civil Division
Low Income - North Dunes/Siuslaw 141999419S Population Group 0 2 15
C.T. 9517.00
Census Tract
Lincoln County Health and Human Services 6419994173 Comprehensive Health Center
11
Low Income - Lincoln County 6419994174 Population Group 1 4 18
Lincoln
Single County
Siletz Community Health Clinic 64199941A4 Native American Tribal
Population 12
Bayshore Family Medicine 64199941AF Rural Health Clinic 0
6
Lincoln City Medical Center 64199941AH Rural Health Clinic 0
23
Coastal Health Practitioners 64199941AI Rural Health Clinic 0
23
Lincoln County Health and Human Services 7419994149 Comprehensive Health Center
12
Siletz Community Health Clinic 7419994158 Native American Tribal
Population 13
Lincoln City Medical Center 741999416D Rural Health Clinic 0
22
Coastal Health Practitioners 741999416E Rural Health Clinic 0
22
Table 4-15B. HRSA-Generated Data for MUA/P
Criteria:
State: Oregon County: Lincoln County ID #: All
Results: 8 records found.
Name ID# Type Score Designation Date Update Date
Lincoln County
Yachats Service Area 07080 MUA 49.80 2001/09/13
CT 9517.00
Low Inc - North Lincoln 07327 MUP 61.40 2003/04/11
MCD (90884) Depoe Bay CCD
MCD (?) Unknown
Low Inc - Toledo 07378 MUP 60.80 2003/10/16
MCD (91020) Eddyville CCD
MCD (93230) Toledo CCD
In Lincoln County, three of Samaritan Health Services' hospitals are officially designated as rural
facilities, and they partnered with the Federal Office of Rural Health to form special collaborations to
address the particular needs of rural residents. The partnership, known as a Community Health
Improvement Partnership (CHIP), has been active in Lincoln County (Samaritan North Lincoln and Samaritan Pacific Communities hospitals) since 2002.

20
In Lincoln County, the identified CHIP priorities are:
Children's health School-based health clinics
Chronic disease management
Affordable health insurance
Healthy communities promotion Access/referral to health services.
At one time, the four school-based health clinics in Lincoln County had lost state funding and were in
danger of closing their doors. By using data from the original health care gap assessment, the CHIP
partners were able to leverage initial CHIP seed money for bridge funding and other grants and all four centers continue to operate. Additionally, the Lincoln County CHIP sponsors a children's health fair that
provides free immunizations and was selected to be one of Oregon's pilot-site counties for the Healthy
Community initiative and is working with the Kellogg Foundation to look at school-based clinics.
Additional Lincoln County projects include:
Working with high school media departments to produce theater-related activities encouraging self-
esteem and good decision-making among local teens.
Working with the Parish Nurse Program to set up classes to help parents initiate parent-teen talks. This was a result of hearing parents express a need for tools to help them talk to their children about sex and
other teen behavioral concerns.
Working with Medical Teams International to provide needed dental services.
4.2.7.1 Medical
When it comes to covering kids with health insurance, Oregon is a step ahead of national health care
reform36
. Healthy Kids provides health coverage to all uninsured Oregon children, and no family earns
too much to qualify37
. Healthy Kids covers all necessary care: doctor visits, dental care, vision,
prescription medicines, mental and behavioral health care, and more, with no hidden deductibles or high co-pays. Even kids with current health conditions can enroll, and national healthcare reform protects the
Healthy Kids program for years to come.
CSCHS reports that 96% of enrolled children are covered by OHP, Oregon‟s traditional Medicaid
program. Healthy Kids is an alternate insurance coverage available to Oregon children. Table 4-16 shows the OHP-accepting pediatricians and family medicine doctors in Lincoln County.
For children covered through private insurance, national health reform is making important
improvements:
Health care reform eliminated pre-existing coverage exclusions for children. Pre-existing-condition clauses had been a barrier to health care coverage for children. This meant that children with serious
medical problems couldn‟t get the health coverage they needed.
Children‟s dental and vision needs will be covered beginning in 2014. Healthy Kids covers dental and vision care but many private plans don‟t. National reform requires coverage of not only basic pediatric
services under all new health plans, but also dental and vision needs.
The insurance exchange, a key component of national health reform, will provide a central
marketplace for health insurance, which puts families in charge of their child‟s health care and provides options. The exchange will provide one-stop shopping for individuals and small businesses to
compare rates, benefits and quality among plans. The exchange will also administer the new federal
health insurance tax credits for those who qualify and make it easier to enroll in health insurance.
36 at www.oregonhealthykids.gov. 37 A family of four earning as much as $66,000 a year qualifies for subsidized, low-cost coverage.

21
Oregon‟s insurance exchange will complement the Healthy Kids program by providing more health
insurance choices to families without job-based coverage and providing tax credits to those who can‟t afford it. This program ensures that children have access to affordable child-only health insurance
policies, regardless of whether their parents change jobs, leave a job, move, or get sick. Health care
reform will improve the quality of care children receive.
Table 4-16. Pediatric and Family Medical Providers Accepting Medicaid
Table 4-17 shows the total institutional Medicare and Medicaid providers, including hospitals, nursing
facilities, federally qualified health centers, rural health clinics and community mental health centers
currently available in Lincoln County38
.
Table 4-17. Institutional Medicare and Medicaid Providers, Second Quarter, 2011
Geographic
Area
Total
Institutional
Providers Hospitals
Nursing
Facilities
Federally
Qualified Health
Centers
Rural
Health
Clinics
Community
Mental
Health
Centers
Lincoln County 21 2 2 8 4 0
Oregon 672 68 138 104 64 12
United States 75,166 7,195 15,714 4,923 3,899 633
38 U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services, Provider of Services File, Second Quarter, 2011.
Pediatric and Family Medicine Providers Lincoln County
Sean Rash Pediatric Physician Coastal Pediatric Associates Newport Accepts OHP and new patients
Stephen Burns Pediatric Physician Coastal Pediatric Associates Newport Accepts OHP and new patients
Linell Wood Pediatric Physician Coastal Pediatric Associates Newport Does not accept OHP but takes new patients
David Bice Family Medicine Newport Accepts OHP and new patients
Robert Kay Family Medicine Lincoln City Accepts OHP and new patients
Bayshore Family Medicine Lincoln City Accepts OHP
Jennifer Wrazen Pediatric Physician Samaritan Waldport Clinic Waldport Accepts OHP and new patients
D. Orton Family and Emergency Medicine Lincoln City Accepts OHP and new patients
Jerry Flamming Family Medicine Depoe Bay Accepts OHP and new patients
TBA Family Medicine Depoe Bay Accepts OHP and new patients
Marlene Nelson, Meg Portwood Coastal Health Practitioners Lincoln City
Lincoln City Medical Center Lincoln City Accepts OHP
Samaritan Waldport Clinic Waldport
Samaritan Toledo Clinic Toledo
John Leher Family Medical Clinic Newport
Theresa Curran, PA Samaritan Coastal Clinic
Lincoln City

22
Table 4-18 shows 2011-2012 CSCHS data for enrolled children with respect to health insurance and
medical home.
Table 4-18. Medical Information for CSCHS Enrolled Children 2011-2012 School Year
Table 4-19 shows 2011-2012 CSCHS data for enrolled children with respect to medical services
provided.
Table 4-19. Medical Information for CSCHS Enrolled Children 2011-2012 School Year

23
4.2.7.2 Mental Health
According to available data39
, currently practicing in Lincoln County there are counted six counselors,
seven clinical social workers/therapists, 1 marriage/family therapist, 1 substance abuse counselor, and 1 certified and registered psychologist, all of which list children as an aspect of their practice. It is unclear,
however, how many (if any) of those professionals accept OHP40
. When the search is expanded to include
neighboring county opportunities, the number of available mental health professionals greatly increases.
The American Mental Health Alliance regularly updates and makes available to practitioners and libraries
printed directories of therapists throughout of the Portland area and Oregon41
.
Locally, low- and no-cost mental health services can be accessed through Lincoln Community Health
Center (locations in Newport, Lincoln City, and South Beach), which is supported through Lincoln County Health and Human Services Department, Federal HRSA grant, Oregon Department of Human
Services, Lincoln County, and funds through donation, foundations, and patient fees. Additionally, there
is a toll-free telephone number available for mental health emergencies, and the Children‟s Advocacy
Center in Newport is also listed as available for working with child mental health concerns.
In 2011, the last period for which data is available, only 7% of children statewide receive needed mental
health services, with the last two quarters of that year seeing a 10% drop in that 7% served. Conversely,
enrollment in OHP increased overall by 4% in the same timeframe. It would be positive to think that
fewer children need mental health services, but in areas such as Lincoln County, the downturn in mental health service provision is more likely due to lack of available local providers.
Currently, for Lincoln County residents on OHP, the primary mental health provider is Accountable
Behavior Health Alliance (ABHA) which is located in Benton County, Corvallis specifically. Though
there are contracted ABHA providers who specialize in children, none are located in Lincoln County, so families must travel substantial distance (40 miles or greater) for this vital service. Table 4-20 shows
2011-2012 CSCHS data for enrolled children.
39 American Mental Health Alliance, Psychology Today. 40 http://www.oregon.gov/oha/amh/child-mh-soc-in-plan-grp/docs/brs-provider-list-county.pdf - no providers listed in Lincoln County who serve children and accept OHP. 41 http://or.americanmentalhealth.com/freeprintdirectory.trust?cart=13597328832166374.

24
Table 4-20. Mental Health Information for CSCHS Children 2011-2012
4.2.7.3. Dental Care
Dental care for OHP participants in Lincoln County is limited similarly as medical and mental health provision and also contains no local pediatric specialists. Though potential transportation options are
available deliver patients to professional offices outside the local area, scheduling and timing continue to
present difficulties for low-income families. Table 4-21 shows the dental provider options available to
OHP recipients and, contained within that group, are four local options: two in Lincoln City, one in Newport, and one in Toledo (again, none of whom serve young children).
Table 4-21. OHP Dental Providers in Lincoln County

25
4.2.8 Child Care
Lack of child care in Lincoln County especially
for working parents continues to be a significant need, and for every 100 children who need
childcare, there are approximately only 19 slots
available with licensed facilities. Of course there are opportunities for child care in unlicensed
private and family homes, but these facilities are
not eligible for State subsidy if any is available.
According to OSU‟s Childcare Research Project, childcare costs about $35 a day per
child, and public subsidies for childcare have
been significantly reduced in recent years. Figure 4-3 shows who pays for childcare in
Oregon.
4.2.8.1 Child Care Assistance
The Employment Related Day Care program (ERDC) helps eligible low-income working
families pay for child care which assists lower-
income parent obtain and maintain employment
as their children are cared-for in stable child care arrangements. ERDC helps approximately 20,000 Oregon families every year pay for child care for
approximately 35,000 children each year and works with providers and other childcare partners across the
state to help families find and keep good childcare, improve the availability of quality childcare in Oregon, and to develop resources for parents and childcare providers.
If a parent qualifies for assistance, DHS will pay a portion of their child care bill, the amount of which is
based on the family‟s income, type of child care, and how many hours of child care are needed. Most
parents are required to pay part of the cost, and DHS pays its portion to the family‟s child care provider directly. Providers must apply and pass a background check to participate.
The number of families served is based on the program‟s budget, and the program budget and caseload
maximums are set by the Oregon State Legislature. The caseload maximums started July 1, 2011:
July 2011 through December 2011: 9,000 cases; January 2012 through December 2012: 9,500 cases; and,
January 2013 through June 2013: 10,000.
When the caseload maximum is reached, a reservation list will be created. As there are openings, families
on the waiting list will be randomly selected and invited to apply – within 30 days – for the subsidy.
Additional, non-subsidized childcare resources might be available through the Oregon Child
Care Resource and Referral Network42
and/or the Family Care Connection which is operated through the
Oregon State University Extension Service43
.
42 http://www.oregonchildcare.org. 43 http://extension.oregonstate.edu/lincoln/family_care.
Figure 4-3. Child Care Funding

26
4.2.8.2 Child Development Programs (in addition to CSCHS)
Newport Montessori - Preschool
1428 Northeast Yaquina Heights Drive, Newport, OR (541) 265-3572
Mouse Factory Co-Op - Preschool 227 Northeast 12th Street, Newport, OR
(541) 265-5527
Nye Beach Montessori School - Preschool
144 Southwest Coast Street, Newport, OR
(541) 265-3027
ABC Preschool Kindergarten
208 Northwest 6th Street, Newport, OR
(541) 265-2654
4.2.9 Domestic Violence
The annual survey conducted by the National Network to End Domestic Violence (NNEDV) provides
insight into domestic violence services in the United States. On September 15, 2011 – one 24-hour period
– domestic violence victim advocates served more than 67,000 victims and answered more than 22,000 emergency hotline calls. This annual snapshot shows that shelters and programs continue to find a way to
help almost the same number of victims in one day as in past years – a staggering 67,399 adults and
children. However across the United States there were 1,040 more unmet requests than in September 2011.
In Oregon44
, though 1,692 victims were served that day, there were also 423 unmet requests for services;
70% were people looking for emergency shelter and transitional housing. Across the nation, the unmet
requests are 16% of the number of people served. In Oregon, the unmet requests total 25% of the number of people served. Programs reported they were unable to provide services for many reasons:
42% not enough funding for needed programs and services
40% not enough staff 38% not enough specialized services
31% no available beds or funding for hotels
9% limited funding for translators, bilingual staff, or accessible equipment
My Sisters‟ Place (MSP) in Lincoln County is a private non-profit program, incorporated in 1980, which provides supportive services to victims of domestic violence, sexual assault, and dating abuse. Services
include crisis intervention, emergency shelter, 24-hour crisis line, safety planning, advocacy, court
information and support, agency referral, education and outreach activities.
44http://nnedv.org/docs/Census/DVCounts2011/DVCounts11_StateSummary_OR.pdf.

27
In 2012, MSP counted the following:
24-Hour Shelter and Services Emergency Shelter - 69 Women, 45 children
Total Bed Nights - 4,077
Meals Served - 12,231
24-Hour Crisis Line Domestic Violence Calls - 1,979
Sexual Assault Calls – 667
Stalking - 95 Homeless and Other Issues - 146
Victim Services
People Served - 822 Information & Referral Services - 6,733
Peer Counseling - 9,386
Court Advocacy - 1,367
Agency Advocacy - 1,191 Protective Order Services - 272
Safety Planning - 1,917
Total volunteer Hours - 7,794
4.2.10 Transportation
Oregon is a largely rural state, and this is problematic for public transit, whether through fixed route or
demand-response service (Dial-a-Ride, etc.). People living in rural areas who lack cars and access to
public transportation are at a strong disadvantage and may be relegated to relying on friends, family, or
co-workers for travel. Independence is severely limited, and older adults and people with disabilities, in particular, often experience more restrictions on ability to travel and must rely more heavily on informal
networks or formal supportive services to meet their needs. Rural public transit also plays a vital role for
agricultural workers45
.
4.2.10.1 Local Options
In Lincoln County, the following low- and no-cost transportation options are available:
Dial- A-Ride (Curb-to-curb transportation service); $1.00 per ride Lincoln County Transit Service
46 (three bus routes originating from Siletz, Yachats, and Lincoln City
to Newport); $1.00 per zone (seniors 90 and over and children five and under are free)
Bay to Beach Shuttle Service (May – September); free.
4.2.10.2 Regional Options
Cascades West Ride Line coordinates transportation for OHP clients traveling to and from covered non-
emergency medical services who have no other way to get to their appointments. Transportation is
arranged through locally – and limited – contracted transportation providers, so it is important that rides are scheduled in advance. There is no cost to eligible clients for OHP/Medicaid transportation services,
which is especially important given that a considerable number of medical, dental, and mental health
services for children are located outside Lincoln County in neighboring Linn and Benton counties.
45 David Evans and Associates, 2012. 46 http://www.co.lincoln.or.us/transit/pdfs/TriCounty.pdf.

28
Linn, Benton, and Lincoln Counties are working together to provide consistent and sustainable
transportation services across county lines and currently includes the following options: Coast to Valley Express from Newport to Corvallis (service for seniors, people with disabilities, and
low-income patrons)
Cascades West Ride Share/Valley VanPool which is a carpool and vanpool matching service for
commuters with connections to major cities including Salem and Eugene. Additional options might be found through Oregon Department of Transportation‟s TripChecks
website.
Additionally, Oregon Cascades West Council of Governments facilitates a regional transportation
workgroup, the Cascades West Area Commission on Transportation (CWACT)47
, which provides a forum for local governments to communicate and collaborate on local, regional, and state transportation issues.
The CWACT is chartered by the Oregon Transportation Commission (OTC) as an advisory body and
provides input, advice and recommendations to the OTC and ODOT.
An important role of the CWACT is to solicitation public input on transportation needs and to provide
recommendations to ODOT and the OTC on project priorities for the Statewide Transportation
Improvement Program (STIP). The CWACT provides input on state transportation plans, policies and
programs and maintains an inventory of transportation system improvement needs.
47 http://www.ocwcog.org/ccbindex.asp?ccbid=101.

29
5.0 CONCLUSIONS AND RECOMMENDATIONS
5.1 Discoveries
Community Services Consortium‟s Lincoln County Head Start (CSCHS) provides an excellent program
for children, as evidenced by continually improved and documented outcomes, as well as solid infrastructure and ongoing monitoring systems. Interviewed partners and providers noted that CSCHS
is a program of excellence in their service to, and support of, parents and children
CSCHS has a comprehensive, reporting system for their program. CSCHS annual Pre-Service trainings are comprehensive; with identified program improvement trainings throughout the year
Staff qualifications for the eight CSCHS teacher/advocates: three teachers, one with advanced degree and two with baccalaureate degrees, currently meet Head Start requirement as of September 30, 2013
that 50% of teachers nationwide possess an advanced or baccalaureate degree in early childhood
education or a related field. One teacher possesses current Child Development Associate (CDA) credential and is working on her associate degree in early childhood education. Remaining three
teachers possess current Head Start teaching staff requirements and are taking courses online each term
to earn their baccalaureate degrees. Of the six CSCHS teaching assistants, two hold current CDA credentials and four are in process of attaining their CDA credentials. All meet Head Start requirements
as of September 30, 2013
All CSCHS sites operate at capacity, drawing from waiting lists as openings occur
Enrolled program children represent the community‟s ethnicities and races very well
Program staff accommodates Spanish-speaking families well by incorporating bilingual abilities into
classroom instruction, family services, training, and through employment of bi-lingual staff and on-call parents/volunteers. Written information is provided in both English and Spanish
Training and professional development are on-going goals. Annual training opportunities extend to
Lincoln County Board of Commissioners (Shared Governance) and the CSCHS Policy Council and parents
The program already does an excellent job of referral to crisis programs and intends to continue this work.
5.2 Suggestions
Since there is constant change in types of programs and resources available to families in the community, CSCHS needs to maintain diligence in keeping the community resource list updated
With the uncertainty of funding, CSCHS should continue to research new funding streams
Continued advocacy support to families with transportation issues that arise throughout the year
Greater demand for mental health support for families and children surpasses availability of local providers to meet the current community needs. CSCHS, in partnership with the Olalla Center for
Children and Families, continues to help in early identification of pre-school children. More mental health professions are needed
Because single and married fathers/brothers caring for children have unique needs, it is suggested CSCHS provide/collaborate with partners to provide special father events
Continue encouraging parents to apply for employment with CSCHS as openings occur (including training opportunities whenever presented). Currently this strategy has resulted in regular full-time
employment at CSCHS for eight former CSCHS parents.

30
APPENDIX A
Successes and Partnerships
The core purpose to ensure that our youngest children have a solid foundation for life is a CSCHS
fundamental reason for being. These core values are demonstrated through respect for the uniqueness of
every individual served; developing family partnerships; and providing quality, comprehensive services
with demonstrated results and collaboration among staff and community partners. CSCHS is committed to providing a learning environment for staff, parents and community partners and values the partnerships
formed, recognizing these partnerships as essential to ensuring accessibility and availability of needed
services.
Successes
While there are daily successes counted within each of the CSCHS program sites, included among those
most notable are:
Maintenance of full enrollment with 160 children with a solid wait list of 86
CLASS observations and coaching have resulted in ongoing significant quantifiable improvements
Receipt of pro bono services of a community partner to assist in family counseling, support, and referrals as well as counsel for the teachers; results in a services savings of thousands of dollars and an
increased value of the program
Provision supplemental food for the children over weekends through the „Backpacks for Kids‟ program
through support of Friends of Head Start and Businesses for Excellence in Youth
Partnership through the Olalla Center via contract to continue providing observation, consultation, and
training to staff and parents regarding children‟s mental health concerns
Trainings for staff in both Positive Behavior Intervention Support and Zoo Phonics (reading focus)
Continued partnership with Lincoln County School District‟s Early Childhood Special Education office to assess children with potential developmental challenges to ensure inclusion in appropriate learning
environments
Award of funds to purchase special „Hatch‟ computers for enhanced learning, hardware for teachers,
and play/movement learning equipment (Spirit Mountain Community Fund and federal programs)
Partnered with the Rotary of Newport to hold a „Literacy Night‟ where 60 families attended and
received the gift of a book; each child was also registered for a free library card. The Rotary plans a second year Literacy Night for 2013.
Continued the hiring and utilization of current and former Head Start parents in provision of programs
and services (eight former HS parents are now staff, and three current parents are on-call staff)
WIC and Head Start programs serve many of the same families. By teaming up, the programs are
maximizing resources through the coordination of services. One tangible way to do this is through data-sharing agreements that allow WIC to provide participant data directly to local Head Start programs.
This includes height, weight, hemoglobin, and nutrition risks. Benefits to this kind of collaboration
include: o Minimizes duplicative efforts for families and staff
o Provides more opportunities for WIC and Head Start to benefit from each other‟s strengths, expertise
and best practices o Offers more ways to make a positive impact on good health and nutrition for children and families

31
Partnership
Katey Townsend Lincoln County School District
Homeless Outreach Program
Coordinator
Yaquina View
351 SE Harney St Newport, OR 97365
(541) 265-4506
Lila Kuykendall LBL ESD: Early Intervention
Health Services Advisory Committee
Yaquina View
351 SE Harney St Newport, OR 97365
(541) 574-2240 ext 105
http://www/lblesd.k12.or.us
Ray Burleigh Olalla Center for Children &
Families
805 NE Reservoir Ln. Toledo,
OR 97391
(541) 336-2254
Jill Luther
LBL ESD: Early Intervention
Yaquina View
351 SE Harney St Newport, OR 97365
(541)-574-2240 ext 117
FAX: 541-265-6490
Bill Hall
Lincoln County Commissioner
225 W Olive St. Room 110
Newport, OR 97365
(541)-265-4100
Doug Hunt
Lincoln County Commissioner
225 W Olive St. Room 100
Newport, OR 97365
(541)-265-4100
Cynthia Breves
Coastal Families Together
351 SW Harney St Newport, OR 97365
(541) 574-4485
www.coastalfamiliestogether.com
Megan Sherwood
Child Forensic Interviewer
Lincoln County Children’s Advocacy Center
PO Box 707
Newport, Or 97365
(541)-574-0841
Theresa Curran
Samaritan Health Services
Physician Assistant 825 NW Hwy 101
Lincoln City, OR 97367
(541)-996-7480
Joell Archibald
Public Health Division
Director LCHHS
36 SW Nye St
Newport, OR 97365
(541)-265-0605
Jan Ostby
OSU Extension Lincoln County
Nutrition Education Instructor
29 SE 2nd St
Newport, OR 97365
(541)-574-2240 ext 105
Signe Miller
Oregon Family Support Network
(541)-563-8697
(541)-961-6646 cell
Cristina Simpson
CSC
Healthy Kids Coordinator
120 NE Avery St.
Newport, OR 97365 (541)-921-8185
Linda Mann
Capitol Dental Group
Dental Hygienist
3000 Market St. Suite 228 Salem, OR
97301 (503)-545-8114
Talitha Dale
Elks Children’s Clinic, OHSU
Preschool Vision Screening
Program
3181 S.W. Sam Jackson Park Rd.
Portland, Oregon 97239-3098
Stacie Johnson
Contract Registered
Dietician/Nutritionist
Food Service Director LCSD
353 NE Burgess Rd.
Toledo, OR 97391-2294
(541)-336-2156
(541)-270-2146 cell
Linda Miller
Sam Case Elementary School
Kindergarten Teacher
School Readiness Contact for LCSD
459 NE 12th St.
Newport, Or 97365
(541)-265-8598

32
APPENDIX B
Working Paper – Suggested Gaps/Needs in Child Development Programs in Lincoln County as expressed by Early Childhood Special Education Workgroup Notes
0-8 Agencies/Types
of Services Services Children
Need/Gaps?
Capacity of Proposed
Providers? Next Steps
Commission on Children and Families
Healthy Start – (53 families) Home Visitation
CFT Parent Education (62 parents).
HELP/LIFT (90) kids/families
Services for 2nd
time parents.
# Of Families in need of Home Visitation Services/waitlisted?
Expand classes to include School Readiness format.
Lincoln County should be courted to partner with.
Ask counties “why” we should partner with them…
Which agencies in Lincoln County could act as fiscal agent for a multicounty region/HUB?
Strength of fiscal agents in possible Hub counties?
1. Continue ECCC Monthly Planning Work Groups as part of monthly ECCC meetings on second Thursday of each month. Build Early Learning Collaborative/Partnerships within Lincoln County and Strengthen Partnerships. Discuss capacity. Begin Hub discussions with Tillamook and Polk Counties.
2. System Mapping /Develop Matrix of Early Childhood System in LC. Include Family Support Worker Survey.
3. Create Tool Analysis of client data, screening tools, assessment tools, coordination.
4. Develop Outcomes Matrix of Maternal and child health, child language and literacy, parent and family support, cognitive development, social emotional develop.
Head Start
(Head Start cont.)
(160) 3-5yrs/33% Hispanic
No Early Head Start 0-3/(56) families on waitlist, Spanish Parenting Classes & Staff Training
5. Develop a Framework with these components:
Early Identification,
Referrals to Services,
Early Learning Services, Outcomes/Results

33
0-8 Agencies/Types
of Services Services Children
Need/Gaps?
Capacity of Proposed
Providers? Next Steps
YYFAP – Preschool/(30)
3-4 & 4-5 yr olds.
Afterschool program (15) 6-12 yr olds. Early childhood and parent literacy programs including literacy nights and preschool
Need to offer more slots for preschool.
Curriculum needs/training for staff.
6. Develop an integrated system that includes the 5 essential service components (SAMHSA) :
Home Visitation, Developmental Screening and Referral, Integration of Behavioral Health in primary care, Mental Health Consultation and Family Strengthening.
SELC – (62) Early Childcare Center 6 weeks (infants) – 8 yrs old (SELC)
Need for infant care, but too costly & w/o enough space.
CCCD Center (58) 0-12 yr olds w/ 12 infants
More spots for infant care…
Home -Based Childcare, Infant Care, Early Care Communication with Schools, Training for Staff
EI/ECED
0-2yr olds Home Visits & 3-5yr olds in Groups
Therapeutic Classrooms, Specialists/Therapy, Home Visits/Assessment
Mental Health
Ages 0-18/21(250 families)
(30) 0-8yr olds in Intensive Services
(2) In home trainers
Need additional trained Mental Health Therapists and In Home trainers. Training for preschool teachers/childcare workers on Explosive Child Curriculum.

34
0-8 Agencies/Types
of Services Services Children
Need/Gaps?
Capacity of Proposed
Providers? Next Steps
LCSD/Sam Case Primary School – SIOP and TRIBES (RTI/PBIS) Trained Staff at Sam Case
Communication with preschools/day
cares. Low language kids and ELL needs. Whole child assessment/intervention strategies on entering K’s from preschools. Evidence based curriculum taught in preschools/day
care settings. School Readiness classes for parents and children in preparation for kindergarten.
Resource and Referral
Reduction in Home Based Child Care, Infant Care. Evidence based curriculum/training for home based providers.
DHS SSP Help Parents find work/skill building/self sufficiency, enrolled in parenting classes & school readiness classes.
Health Care/Dental Services
Access to health care needs and dental services. Oral health screenings for expecting Moms and children ages 2-5.

35
APPENDIX C
Suggestions for Improving Affordable Housing Availability in Lincoln County48
There is a need for multifamily rental units for the working poor; those earning 50% of median family income down to 17% of median family income (persons on Social Security Supplemental Income).
Over 40% of Lincoln County renters pay more than 30 % of their income for housing.
Real wages have actually declined in Lincoln County since the late 1970s, while the cost of housing has
continued to increase.
There are approximately 900 units of subsidized multifamily housing in Lincoln County. This is about
12% of all rental units.
There are 400 federal Section 8 vouchers in Lincoln County, with a waiting list of up to two years. Over
1,300 low income households are currently waiting for housing.
The average annual income of households currently receiving housing assistance is $12,179.
Resident services provided to tenants of affordable multifamily housing are aimed at facilitating family self-sufficiency.
Availability of affordable buildable land is a major hurdle to building affordable housing. Housing development organizations should solicit donations of land.
The land use process should be streamlined and zoning rules examined to make it easier to site affordable housing (mixed use, parking, setbacks, and density). This will require action at both the state
and local levels.
System development charges could be amortized rather than due up front.
There is a need to explore the availability of federal and state funding programs for the elderly, mentally ill and other populations.
There must be more networking between landlords with available housing and the Housing Authority of Lincoln County.
Combine several small tax credit projects along the coast in order to address the high overhead costs.
48 “At Home in Lincoln County 2.0”: The updated 10-year housing plan for Lincoln County; December 2012.

36
APPENDIX D
Parent Survey and Comments
Parent Survey

37

38
Parent Comments
Lower rent for houses so kids can have back yards
Physical activities for child
Legal assistance going through divorce
Landlord will not return deposit so we can move to lower income housing
I have a need for computer for college and work search
I feel that I am pretty well set up right now and that things are running smoothly.
Childcare for weekends/evenings
Counseling services for kids with behavior issues
A place for my child and myself
Behavior issues – 5 year old
Help paying off debt as well as help paying power bill
Transportation for my child to Head Start
We are fine for the moment
When the races are equal we can work together
Everyone needs public transportation, but if we have our own car it‟s better for us.
Not possible to get a license without a social security number in Oregon, which makes transportation
hard for us.
We would like transportation to Head Start because some of our family does not have transportation.

39
APPENDIX E Provider Interviews
Input into what works, where improvement could be made
Positive
Overall health assessment (dental, mental, physical)
Works with children at risk/most at risk
School district partnership in case management especially for kids with special education needs, early
intervention services, of great benefit in school readiness
CSCHS does a great job at partnering with the school district to prepare kids for school
„Marveling‟ about the good work CSCHS does with at-risk children and families
Greatest impact is the skills-building the CSCHS teachers and children work on together
Really appreciate CSCHS‟s director and staff willingness to work with school district homeless liaisons
Continue family literacy programs; builds family relationships and encourages learning as a unit
CSCHS provides referrals to community programs and follow up to access health centers, hygiene, clothes, and guides families toward other community resources
Health Services Advisory Committee is an excellent partnership and brings a wealth of information to the community and families that otherwise wouldn‟t be known
CSCHS program quality, services, and expertise have increased in the last few years and it is amazing; some of the best currently in preschool. Suzanne Miller and Andrea Daniels management have resulted
in teachers showing that the increased training, CLASS, have increased capacity and resulted in higher
levels of confidence
Good critical program that make differences in people‟s lives.
Needs Improvement
Affordable housing – amount rent assistance can cover (fair market rent) too high
County economics (housing, goods unaffordable to middle-/low-income workers)
Only 55% of eligible kids are currently served
Transportation organization by families in South County to get kids to existing programs/classrooms (though many interviewed commented that transportation isn‟t prohibitive to class attendance
generally-speaking)
Mental health services for young children is a great and growing need, especially for children who
don‟t meet the test for special education/developmental disability but who manifest difficult social, emotional, behavioral issues
Enhanced collaboration between school district and Head Start in transitioning kids from early learning to kindergarten; Head Start does a great job but the partnership could be improved with new tools for
measuring children‟s levels of learning upon entry to K-12.
Services for kids outside of school year – Boys and Girls Club, for example; kids with no food resources on the weekends, special summer programs, etc.
Family literacy, ESL classes, basic needs supports for families; collaborative parent training (with school district, health providers, etc.)
No educational programs for children 0-3 years of age; opportunity for collaborative efforts to design and find funding for Early Head Start

40
APPENDIX F
SWOT Analysis
Analysis Goal: To Frame Vitality of CSCHS in the Lincoln County Community
Strengths
History of excellence in service provision via
monitoring and performance analysis
Variety of and expansion of collaborating
agencies/organizations
Specific timelines for grants, performance standards,
etc. (achievable goals)
Potential for planning/building a quality early
childhood system in Lincoln County
Participation of families and parents Dedicated/experienced/dependable/educated staff
Systematic alignment of goals and objectives
Increased awareness of Lincoln County needs for pre-
school readiness
Effective communication – staff, partners, parents
Open to new/enhanced partnerships
Existing relationships with school district partners
Strong and competent consultants
Technology and support
Good and growing community feedback loop
Creative and innovative staff
Community Action Agency, CSC, offers a variety of
supports to families and program Comprehensive Policies and Procedures/Ongoing
Monitoring Protocols
CLASS observation and coaching – continual teaching
improvement
Solid family/parent involvement in systems/program
planning
Weaknesses
Lack of sustainable funds for expansion to south county
Transportation issues in rural area
Funding limits and challenges
Lack of current capital to fund projects, maintenance
and/or enhancement of buildings, etc.
Limited resources in local communities to assist with program operation/enhancement
No clear, consistent pathways for children/family
support beyond Head Start experience beyond
comprehensive transition planning and
implementation.
Opportunities
Common vision for „equal access‟ pre-school readiness programs/services beyond income eligibility
Information-, training-sharing opportunities
Building/enhancing partnerships with similar
outcomes to pool/share/seek resources – to plan and
build early childhood learning system
Information-sharing, networking
Enhance school readiness opportunities, training, resources for parents and children through partnership
and shared resources
Identifying and applying for non-Head Start private,
state, and federal funds to create/enhance similar
programs outside of eligibility factors
Threats
Funding cuts, especially with little notice (federal, state, partner, etc.)
Difficulty to meet all parent/children needs even with
solid community partnerships
Program and staff costs (wages, benefits) outgrowing program funding; e.g., PERS increases, health care
Teaching salaries are not competitive with licensed
teachers despite increased requirements in education

41
APPENDIX G
Supported Affordable Housing in Lincoln County
Project Name Address City Management Company Phone
Agate Heights 150 NE 60th St Newport Lincoln Co HA 541-265-5326
Beacon Crest Apts. 2897 NE 47th Street Lincoln City Legacy Senior Living LLC 425-423-0304
Big Creek Point Apts. 2725 NE Crestview Dr Newport Legacy Senior Living LLC 425-423-0304
Fisterra Gardens Apartments 101 Diversity Drive Yachats Lincoln Co HA 541-265-5326
Jetty Apts. 426 SE Jetty Ave Lincoln City Guardian Mgmt 503-802-3600
Lincoln Village 2530 NE 31st Lincoln City Guardian Mgmt 503-802-3600
Mariner Heights 230 NW First St Newport HA of Lincoln Co 541-265-5326
Newport Apts. 114-125 NW 60th St; 444-448 SW Surf St
Newport Neel Mgmt Team 541-895-8801
Pelican Place 320 NW 3rd St Newport Dolphin RE 541-265-6638
Ridge Apts. 3340 SE Harbor Dr Lincoln City Cascade Mgmt 503-682-7788
Salmon Run 7035 NE Echo Ct Newport HA of Lincoln Co 541-265-5326
Tern House 655 SW 9th Street Newport Clay Martin 541-758-2615
Vandehaven By The Bay 385 Grant Street Waldport HA of Lincoln Co 541-265-5326
West Devil's Lake Apts. 3109 NE 26th St Lincoln City NW RE Capital Corp 208-947-8593
Yaquina Breeze 5927 N Coast Hwy Newport Assurance Real Estate Services 541-270-9945

42
APPENDIX H
Glossary of Acronyms
ABHA
Accountable Behavior Health Alliance
CA
Community Assessment
CCO
Coordinated Care Organization
CHIP
Community Health Improvement Partnership
CLASS
Classroom Assessment Scoring System
CSCHS
Community Services Consortium Head Start
CWACT
Cascades West Area Commission on Transportation
DL
Developmental Level
ECSE
Early Childhood Special Education
EI
Early Intervention
EI/ECSE
Early Intervention/Early Childhood Special Education
EPI
Economic Policy Institute
ERDC
Employment-Related Day Care
ERSEA
Eligibility, Recruitment, Selection, Enrollment and Attendance
ESD
Education Service Districts
ESL
English as a Second Language
FPL
Federal Poverty Line
HHS
Department of Health and Human Services
HPSA
Health Professional Shortage Area
HRSA
Health Resources and Services Administration
HSAC
Health Services Advisory Committee
HUD
Department of Housing and Urban Development
MSP
My Sisters‟ Place
MUA/P
Medically Underserved Areas/Populations
NNEDV
National Network to End Domestic Violence
NOAA
National Oceanographic and Atmospheric Administration
OHP
Oregon Health Plan
OTC
Oregon Transportation Commission
PIR
Program Information Report
STIP
Statewide Transportation Improvement Program

43
INFORMATION CITATIONS
„At Home in Lincoln County 2.0‟; The Updated Ten Year Housing Plan for Lincoln County;
http://homelessinlincolncounty.files.wordpress.com/2012/01/at-home-in-lincoln-county-2-0.pdf . December 2012.
American Mental Health Alliance: Therapist Locator, Lincoln County Oregon;
http://therapists.americanmentalhealth.com/therapistlocator.trust?chapter=therapists&buttonName=Thera
pist+Locator&F_sortBy=name&action=search&F_NAME=&F_CHAPTER=OR&F_FOCUS=ANY&F_
ZIP=97365&F_theString. 2012.
Children‟s Defense Fund, „The State of America's Children® 2012 Handbook‟;
http://www.childrensdefense.org/child-research-data-publications/data/soac-2012-handbook.html.
Children‟s Trust of Lincoln County; http://childrenstrustoflincolncounty.org/ct_info.html.
Community Services Consortium, „Head Start Annual Report‟;
http://www.csc.gen.or.us/documents/HeadStart/HSAnnualReport2011_2012.pdf.
Community Services Consortium; Lincoln County Head Start 2012-2013 Stats for Governing Board
Review.
Community Services Consortium; Lincoln County Head Start Oregon Pre-Kindergarten Monthly Reports;
2011-2012 and 2012-2013.
Community Services Consortium; Lincoln County Head Start Performance Information Report; 2011-
2012 and Final Addendum.
Economic Policy Institute: „What we need to get by: A basic standard of living costs $48,778, and nearly
a third of families fall short‟; James Lin and Jared Bernstein, Briefing Paper #224; http://www.epi.org/page/-/old/briefingpapers/224/bp224.pdf; October 2088.
Find the Data: Health Care Quality and Research; http://www.findthedata.org/category/Health. Accessed
2012.
Healthgrades Physician Search; Oregon, Lincoln County; http://www.healthgrades.com/provider-search-
directory/search?q=Pediatrics&prof.type=provider&search.type=provider&loc=Lincoln+City%2C+Orego
n&pt=&locIsSolrCity=false.
Indexmundi: „Oregon Hispanic or Latino Origin Population Percentage by County‟;
http://www.indexmundi.com/facts/united-states/quick-facts/oregon/hispanic-or-latino-population-percentage#table. 2010.
Lincoln County Oregon; „Public and Special Needs Transportation Guide‟; http://www.co.lincoln.or.us/transit/pdfs/TriCounty.pdf. 2011.
My Sister‟s Place, Domestic Violence Shelter, Lincoln County, Oregon; http://www.mysistersplace.us/.

44
National Alliance on Mental Illness: „Grading the States 2009 – Oregon‟;
http://www.nami.org/gtstemplate09.cfm?section=grading_the_states&Template=/contentmanagement/contentDisplay.cfm&ContentID=74714. Accessed 2012.
National Health File; „Medical Doctors, Non-Federal, Pediatrics, General, Research Health Data for Lincoln County, Oregon‟; http://oregon.nationalhealthfile.org/Lincoln/Details/Medical-Doctors,-Non--
Federal,-Pediatrics,-General,-Research. Accessed 2012.
National Network to End Domestic Violence; „2011 Domestic Violence Counts: a 24-hour Census of
Domestic Violence Shelters and Services‟; Oregon Summary;
http://nnedv.org/docs/Census/DVCounts2011/DVCounts11_StateSummary_OR.pdf. 2011.
Oregon Dental Association Dentists Search; Oregon, Lincoln County; Pediatric;
http://www.oregondental.org/custom/directory/membership.cfm.
Oregon Department of Education: Students Eligible for Free or Reduced Lunch 2011-2012;
http://www.ode.state.or.us/sfda/reports/r0061Select.asp. 2012.
Oregon Department of Education; Special Education Report Cards; „Special Education Report Cards for School Districts and Early Intervention/Early Childhood Special Education Programs‟;
http://www.ode.state.or.us/data/reportcard/sped/default.aspx?RptYr=20102011&Type=P&Language=E.
2010-2011.
Oregon Department of Human Services Child Welfare Programs; „Striving to Meet the Need: Summary
of Services Provided by Sexual and Domestic Violence Programs in Oregon‟;
http://www.oregon.gov/dhs/abuse/domestic/docs/dv_sa_11summary.pdf. April 2012.
Oregon Department of Human Services, Office of Business Intelligence; „2011 Child Welfare Data Book‟; http://www.oregon.gov/dhs/abuse/publications/children/2011-cw-data-book.pdf. October 2012.
Oregon Department of Human Services; „News Flash: July 2012 SNAP and TANF Caseload Information‟; http://www.oregon.gov/dhs/news/2012news/2012-0829caseload-release.pdf. 2012.
Oregon Food Bank; „Community Food Assessment: Lincoln County‟; http://www.oregonfoodbank.org/Our-Work/Building-Food-Security/Community-
Programs/~/media/Files/Community-Food-Systems/Lincoln%20County%20CFA1pdf. 2010.
Oregon Food Bank; „Voices: Real Stories are Different from the Myths‟;
http://www.oregonfoodbank.org/About-Us/~/media/CAB05CAD908D47368157106E22EE4F86.pdf.
2012.
Oregon Health Authority Office for Oregon Health Policy and Research; „Health Insurance Coverage in
Oregon: 2011 Oregon Health Insurance Statewide Survey Results‟; http://www.2011_ohis_statewide_uninsurance_estimates_nov21.pdf. 2012.
Oregon Health Authority Oregon Health Plan (Medicaid) Provider Lists; http://www.oregon.gov/oha/amh/child-mh-soc-in-plan-grp/docs/. 2012.

45
Oregon Health Authority Oregon Health Plan (Medicaid); „Children‟s Mental Health Dashboard‟;
http://www.oregon.gov/oha/amh/child-mh-soc-in-plan-grp/docs/dash4q10-4q11.pdf. September 12, 2012.
Oregon Health Sciences University Office of Rural Health; „Oregon Federally Certified Rural Health
Clinics‟; http://www.ohsu.edu/xd/outreach/oregon-rural-health/clinics/upload/2011-RHC-Report-for-the-Web.pdf. 2011.
Oregon Housing and Community Services; „Low-Cost Housing by County‟; http://www.oregon.gov/ohcs/hd/pdfs/oregon_low_cost_affordable_housing_by_county.pdf. December
12, 2012.
Oregon Labor Market Information System: WorkSource Oregon Information; „Key Workforce
Challenges: More Severe in Oregon's Rural Areas‟; Nick Beleiciks and Gail Krumenauer;
http://www.qualityinfo.org/olmisj/ArticleReader?itemid=00008442; November 19, 2012.
Oregon Labor Market Information System: WorkSource Oregon Information; „Multiple-Job Holders: A
Small but Important Bellwether‟; Charles Johnson; http://www.qualityinfo.org/olmisj/ArticleReader?itemid=00008398; October 18, 2012.
Oregon Labor Market Information System: „Labor Force Data, Unemployment Rate Monthly Data 2012‟;
http://www.qualityinfo.org/olmisj/labforce?stat=unemprate&periodtype=03&year=2012&month=00&yso
rt=asc&msort=asc&key=Continue.
Oregon Labor Market Information System; WorkSource Wages and Income;
http://www.qualityinfo.org/olmisj/OlmisZine?zineid=00000012.
Pew Research: Hispanic Data Center: Demographic information on Latino Eligible Voters in Oregon;
http://www.pewhispanic.org/2012/10/01/latinos-in-the-2012-election-oregon/. 2012.
Psychology Today: „The Therapy Directory: Child or Adolescent Therapists in Lincoln County Oregon‟;
http://therapists.psychologytoday.com/rms/prof_results.php?sid=1359732507.2884_7760&county=Lincoln&state=OR&spec=5. 2012.
State of Oregon: „Report from Kindergarten Readiness Assessment Workgroup to the Early Learning Council‟; http://www.oregon.gov/gov/docs/OEIB/aKRAReport.pdf. July 12, 2012.
The Annie E. Casey Foundation, KIDS COUNT Data Center, „Data by State‟; http://datacenter.kidscount.org/data/bystate/stateprofile.aspx?state=OR&group=Grantee&loc=5363&dt=1
%2c3%2c2%2c4; Oregon, Lincoln County Data. 2011.
The Children‟s Defense Fund, „Children in the States Fact Sheets‟;
http://www.childrensdefense.org/child-research-data-publications/data/state-data-
repository/cits/2011/children-in-the-states-factsheets.html; January 31, 2011.
The Health Care for the Homeless Clinicians Network; „Hard to Reach: Rural Homelessness & Health
Care‟; Vol. 5, No. 5; http://www.nhchc.org/wp-content/uploads/2012/02/October2001HealingHands.pdf. October 2001.

46
The Oregonian; „Your Schools: 2012 Oregon High School Graduation Rates‟;
http://schools.oregonlive.com/grads/. 2012.
U.S. Census Bureau; „Model-based Small Area Income & Poverty Estimates (SAIPE) for School
Districts, Counties, and States‟; http://www.census.gov/did/www/saipe/index.html. December 2012.
U.S. Department of Health and Human Services Health Resources and Services Administration Health
Professionals Data Warehouse and Reporting Tools; http://datawarehouse.hrsa.gov/customizereports.aspx. Accessed 2012.
U.S. Department of Health and Human Services Health Resources and Services Administration Health
Professionals; Find Health Shortage Areas; http://hpsafind.hrsa.gov/HPSASearch.aspx. 2012.
U.S. Department of Health and Human Services Health Resources and Services Administration Health
Professionals; „Designated Mental Health Care Health Professional Shortage Areas‟;
http://bhpr.hrsa.gov/shortage/hpsas/updates/09012011mentalhpsas.html#Oregon. 2012.
U.S. Department of Health and Human Services Health Resources and Services Administration Health
Professionals; „Designated Mental Health Care Health Professionals Shortage Areas‟; http://bhpr.hrsa.gov/shortage/hpsas/updates/09012011mentalhpsas.html#Oregon. September 1, 2011.
U.S. Department of Health and Human Services Health Resources and Services Administration Health Professionals; „Find Shortage Areas: MUA/P by State and County‟; http://muafind.hrsa.gov/index.aspx.
2012.
U.S. Department of Health and Human Services Health Resources and Services Administration Health
Professionals; Find a Health Center; http://www.hrsa.gov/index.html. 2012.
USA Today Newspaper, „Oregon growth rate slows; its Hispanic population booms‟; Christopher Hagan
(Salem, Ore.) Statesman Journal; http://usatoday30.usatoday.com/news/nation/census/profile/OR;
February 24, 2011.
USA.com; Lincoln County School District Housing Information; http://www.usa.com/school-district-
4107500-housing.htm. 2006-2010 data.