JURNAL ANAK IJUP
25
BACKGROUND. Procalcitonin has been identified as a useful blood marker of serious bacterial infection in febrile infants. Many infants present with a febrile reaction after receiving immunizations. The effects of immunization on procalcitonin have not been investigated. METHODS.We performed a prospective observational cohort study at a large, urban pediatric emergency department. Infants _90 days of age with fever of _38°C were enrolled. Subjects were divided into 3 groups: infants with serious bacterial infection; subjects without serious bacterial infection who received recent (_48 hours) immunizations; and subjects without serious bacterial infection who did not recently receive immunizations. Procalcitonin was measured by using a quantitative immunometric assay. RESULTS. Over 13 months, procalcitonin was measured for 271 infants. There were 44 (16%) patients with serious bacterial infection, 35 in the recent-immunization group, and 192 in the no-recent-immunization group. The median procalcitonin level for serious bacterial infection was 0.53 ng/mL, for recent immunization was 0.29 ng/mL, and for no recent immunizations was 0.17 ng/mL. Procalcitonin values were elevated for patients with serious bacterial infection compared with patients both with and without recent immunizations. Compared with patients who had no recent immunizations, procalcitonin levels were elevated in patients with recent immunization. Using a cut point of 0.12 ng/mL, the sensitivity of procalcitonin for serious bacterial infection was 96%, specificity was 23%, and negative predictive value was 96%. Two patients with recent immunization who had serious bacterial infection were identified with this cut point.
Transcript of JURNAL ANAK IJUP

BACKGROUND. Procalcitonin has been identified as a useful blood marker of serious bacterial infection in febrile infants.Many infants present with a febrile reaction after receiving immunizations. The effects of immunization onprocalcitonin have not been investigated.
METHODS.We performed a prospective observational cohort study at a large, urban pediatric emergency department.Infants _90 days of age with fever of _38°C were enrolled. Subjects were divided into 3 groups: infants with seriousbacterial infection; subjects without serious bacterial infection who received recent (_48 hours) immunizations; andsubjects without serious bacterial infection who did not recently receive immunizations. Procalcitonin was measuredby using a quantitative immunometric assay.
RESULTS. Over 13 months, procalcitonin was measured for 271 infants. There were 44 (16%) patients with seriousbacterial infection, 35 in the recent-immunization group, and 192 in the no-recent-immunization group. The medianprocalcitonin level for serious bacterial infection was 0.53 ng/mL, for recent immunization was 0.29 ng/mL, and forno recent immunizations was 0.17 ng/mL. Procalcitonin values were elevated for patients with serious bacterialinfection compared with patients both with and without recent immunizations. Compared with patients who had norecent immunizations, procalcitonin levels were elevated in patients with recent immunization. Using a cut point of0.12 ng/mL, the sensitivity of procalcitonin for serious bacterial infection was 96%, specificity was 23%, and negativepredictive value was 96%. Two patients with recent immunization who had serious bacterial infection wereidentified with this cut point.CONCLUSIONS. Among febrile infants with recent immunization, procalcitonin levels are increased compared withpatients with fever and no identified bacterial infection. Despite this increase, procalcitonin can still reliablydiscriminate infants with serious bacterial infection. Pediatrics 2008;122:e1119–e1122FEVER WITHOUT AN identifiable source of infection isa common presenting complaint at primary careoffices and emergency departments. For infants _3months of age, fever may be the only sign of a seriousbacterial infection (SBI). In addition, infants routinelyreceive their first group of vaccinations between 6 and10 weeks of age. With the advent of the Pediarix(GlaxoSmithKline, Research Triangle Park, NC) vaccine,there have been reported rates of fever aftervaccination as high as 27.9%.1 There is no standardevaluation or management of fever in recently vaccinated

infants.Recent studies have identified procalcitonin as abiomarker of bacterial infections.2–6 We previously reportedthe procalcitonin values in a prospective cohortof infants _90 days old who presented to a pediatricemergency department with fever without source.7Procalcitonin was found to be a highly sensitivemarker of SBI in this cohort. The effect of immunizationon procalcitonin levels has not been well describedand theoretically might interfere with the useof procalcitonin as a diagnostic marker for SBI. Herein,we investigate the effect of recent immunization onthe diagnostic performance of procalcitonin in youngfebrile infants.METHODSThis study was part of a larger study investigating theperformance of procalcitonin as a discriminator of SBI inthis age group.7 The complete study methods are detailedin the original publication. We conducted a prospectivecohort study of infants _90 days of age who presented tothe emergency department with a documented temperatureof _38.0°C. Infants were excluded if they had anKey Words: fever, infant, immunization, vaccination, procalcitoninAbbreviations: SBI, serious bacterial infection; RI, recent immunization; NRI, no recentimmunization; CI, confidence interval; UTI, urinary tract infection; WBC, white bloodcell; NPV, negative predictive valuewww.pediatrics.org/cgi/doi/10.1542/peds.2008-1884doi:10.1542/peds.2008-1884Accepted for publication Jul 21, 2008Address correspondence to Andrew Dauber, MD, Children’s Hospital Boston, Division ofEndocrinology, LO-605, 300 Longwood Ave, Boston, MA 02115. E-mail: [email protected] (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2008 by theAmerican Academy of PediatricsPEDIATRICS Volume 122, Number 5, November 2008 e1119Downloaded from www.pediatrics.org. Provided by Indonesia:AAP Sponsored on December 12, 2010underlying chronic illness or antibiotic use within theprevious 48 hours.Patients were classified as having an SBI if they had ablood, urine, or cerebrospinal culture that grew a pathogenicorganism or had a chest radiograph that was interpretedby an attending radiologist who diagnosedpneumonia. Subjects were divided into 3 groups. Thefirst group included all patients with an SBI regardless of

their recent immunization status (SBI group). The secondgroup included those patients without SBI who hadreceived immunizations within the previous 48 hours(RI group). The third group included those patientswithout SBI who had not received immunizations in theprevious 48 hours (NRI group).At the time of enrollment, the attending physician responsiblefor the care of the patient completed a questionnaireto assess the appearance of the infant on a 5-pointscale. Procalcitonin was measured on stored samples byusing an immunometric assay (Brahms [Hennigsdorf, Germany]procalcitonin-sensitive Kryptor kit).Statistical analysis was performed by using SPSS 14.0(SPSS Inc, Chicago, IL). For continuous variables, independent-samples t tests and the nonparametric Wilcoxonrank-sum test were used; for categorical data,Fisher’s exact test or _2 analysis was used. Analyses wereperformed between the SBI and RI groups, the SBI andNRI groups, and RI and NRI groups. The 95% confidenceintervals (CIs) for proportions were calculated by usingStata 6 (Stata Corp, College Station, TX).The study was approved by the Children’s HospitalBoston institutional review board and was compliantwith the Health Insurance Portability and AccountabilityAct of 1996.RESULTSDuring the study period, 874 infants _90 days old witha temperature of _38°C were evaluated in the emergencydepartment. Fifty-two patients met the exclusioncriteria. Of the remaining 822 patients, consent wasobtained for 501 (61%) of them. Of those patients, wewere able to measure the procalcitonin level from anavailable blood specimen in 271 patients (54% of consentedeligible patients).Of the 271 patients comprising the study group, therewere 44 (16%) patients in the SBI group, 35 (13%)patients in the RI group, and 192 (71%) patients in theNRI group. Of the 44 SBIs, 33 were urinary tract infections(UTIs), 2 were UTIs with bacteremia, 4 were bacteremia,and 5 were pneumonia. Demographics of theinfants in these 3 groups are presented in Table 1. Aspredicted by the timing of immunizations, the mean ageof patients in the RI group was significantly higher thanin the SBI and NRI groups. The patients were significantlymore well-appearing in the RI group in comparisonto those in the SBI group but not in comparison tothose in the NRI group.The white blood cell (WBC) and procalcitonin datafor the 3 groups are presented in Table 1. WBC valueswere significantly higher in the SBI and RI groups when

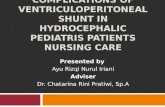
compared with the NRI group. There was no differencein the mean WBC count between the RI and SBI groups.Median procalcitonin levels were significantly higher inthe SBI group when compared with both the RI and NRIgroups. The procalcitonin levels in the RI group werealso higher than in the NRI group. Figure 1 depicts thedistribution of procalcitonin values in the SBI, RI andNRI groups.Two of 37 patients with recent immunization had anSBI. The first patient was a 77-day-old girl with a temperatureof 40.0°C who had received immunizations 2days before presentation. Her urine culture grew_100 000 colony-forming units/mL Escherichia coli. Herprocalcitonin level was 0.36 ng/mL. The second patientwas a 71-day-old boy who had received immunizationsearlier that day and presented with a temperature of38.4°C. His urine culture grew 30 000 colony-formingunits/mL E coli. His procalcitonin level was 0.211 ng/mL.Using our previously published cut point of 0.12 ng/mL, the sensitivity of procalcitonin for SBI in the entirecohort was 96% (95% CI: 83%–99%), the specificitywas 23% (95% CI: 18%–29%), and the negative predictivevalue (NPV) was 96% (95% CI: 86%–99%).Using the same cut point for the 37 patients who hadreceived immunizations in the past 48 hours (35 in theRI group and 2 with recent immunization in the SBIgroup), the sensitivity of procalcitonin for SBI was 100%(2 of 2), and the specificity for non-SBI was 8.6% (3 of35). This calculation was limited by the small sample sizeof 2 patients with SBI and recent immunizations.DISCUSSIONFever is the most frequently reported “serious” and“nonserious” adverse event after immunization accordingto the Vaccine Adverse Event Reporting System.8This presents a unique problem in those infants _3months of age who are at higher risk of having an SBI.TABLE 1 Comparison of the Study SubgroupsSBI Group(N_44)RI Group(N_35)NRI Group(N_192)PSBI vs RI SBI vs NRI RI vs NRIAge, mean (SD), d 45 (25) 63 (7) 51 (23) _.001 .133 .002Highest temperature, mean (SD), °C 38.9 (0.68) 38.7 (0.53) 38.6 (0.46) .207 .002 .32Overall appearance, median (IQR)a 4 (4–5) 5 (4–5) 4 (4–5) .019 .118 .112WBC, mean (SD), 103/_L 14.3 (7.8) 13.8 (4.7) 11.2 (4.2) .781 _.001 .001

Procalcitonin, median (IQR), ng/mL 0.53 (0.18–2.50) 0.29 (0.18–0.41) 0.17 (0.12–0.27) .017 _.001 .001IQR indicates interquartile range.a Appearance scale: 1, “moribund, toxic, ill appearing, unresponsive”; 5, “perfectly healthy, interactive infant.”e1120 DAUBER et alDownloaded from www.pediatrics.org. Provided by Indonesia:AAP Sponsored on December 12, 2010There is no consensus on whether to treat these patientsdifferently than those with fever and no recent history ofimmunization.The effect of vaccination on procalcitonin levels hasnot been well studied. A Medline database search revealedonly 1 article about procalcitonin levels aftervaccination: in a letter to the editor of the Pediatric InfectiousDisease Journal,9 Korczowski reported on a cohort of17 patients who presented to a pediatric emergencydepartment in Poland with vaccination-associated adverseevents. Sixteen of these patients had temperaturesof _38.5°C. The mean age of the infants was 20 weeks(range: 6–37 weeks). The mean serum procalcitoninlevel in these patients was 0.8 _ 0.9 ng/mL (range:0.1–3.6 ng/mL). There were no SBIs. Korczowski concludedthat procalcitonin levels can be modestly elevatedafter vaccination in the absence of infection.Ours was a prospective cohort study that included271 infants _90 days old with documented temperaturesof _38°C in a pediatric emergency department. Wepreviously reported the utility of procalcitonin level forpredicting SBI in those patients who had not receivedimmunizations in the previous 48 hours. In that cohort,a cut point of 0.12 ng/mL had a sensitivity of 95% (95%CI: 83%–99%), specificity of 26% (95% CI: 20%–32%),NPV of 96% (95% CI: 85%–99%), and negative likelihoodratio of 0.19 (95% CI: 0.05–0.74); all cases ofbacteremia were identified accurately with the cut-pointvalue.In the current study, we further subcategorized thepatients as those with SBI, those without SBI who hadrecently received immunizations, and those without SBIwho had not recently received immunizations. The medianprocalcitonin level was significantly higher in thegroup of infants who had received immunizations comparedwith those who had not, but it was significantlylower than in the SBI group. On the basis of this, it seemsthat immunization leads to an increase in serum procalcitoninvalues, but it can still be used to identify a groupat low risk for SBI regardless of immunization status. TheWBC count was also elevated in the RI group whencompared with non-SBI patients without recent immunization

but was similar to those with SBI. Therefore,WBC count, a commonly used marker for SBI, is lessuseful for patients who have recently received vaccinations.When using our previously published cut point of0.12 ng/mL, the sensitivity of procalcitonin for SBI in theentire cohort was 96% (95% CI: 83%–99%), specificitywas 23% (95% CI: 18%–29%), and NPV was 96% (95%CI: 86%–99%). Overall, the addition of vaccinated infantsinto the analysis of the entire cohort led to a similarsensitivity and NPV but decreased the specificity of procalcitoninlevel as a marker of SBI. This change is becauseof the vast majority of immunized patients havinga procalcitonin value that was greater than our cut pointof 0.12 ng/mL. However, procalcitonin levels can continueto be used to identify patients at low risk for SBI,and by using the same cut point, both patients in ourcohort with SBIs who had recently received immunizationswere identified.Our study has several limitations. The study was conductedat an academic pediatric emergency departmentand, therefore, may not represent the larger populationof patients after immunization. In addition, even amongthose febrile infants who were recently vaccinated andpresented with fever, there may be a bias of who hadany laboratory evaluation. Furthermore, we did not collectinformation on the type of vaccinations receivedand, thus, cannot provide further details on the specificeffects of individual vaccines on procalcitonin values.SBI RI NRIStudy subgroup543210Procalcitonin, ng/mLFIGURE 1Comparison of the study subgroups. The boxes representthe limits of the 25th and 75th percentiles and are dividedwith a line at the median. The whiskers represent 1.5 timesthe IQR.PEDIATRICS Volume 122, Number 5, November 2008 e1121Downloaded from www.pediatrics.org. Provided by Indonesia:AAP Sponsored on December 12, 2010Finally, our definitions of SBI were intended to be conservativeto include all possible SBIs, because we werehoping to identify a low-risk group for SBI. We acknowledgethat some of the patients with low-colony-countUTIs and radiographic pneumonia may not have represented

true bacterial infections. Our initial study providesfurther analysis on definite and possible SBIs toaccount for this difficulty in definitions.CONCLUSIONSAmong young febrile infants with recent immunization,procalcitonin levels are increased compared with patientswith fever and no identified bacterial infection.Despite this increase, procalcitonin levels can still reliablydiscriminate infants with SBI.ACKNOWLEDGMENTSWe thank the physician colleagues in the emergencydepartment who facilitated enrollment for the study,and we gratefully acknowledge the help and expertise ofRichard Snider, PhD, and Robyn Neches, BS, for workon the procalcitonin assays.We are thankful for the financial support of the FrederickH. Lovejoy, Jr, MD, Resident Research Fund andthe American Academy of Pediatrics Resident ResearchGrant. In addition, we acknowledge technical supportrelated to specimen processing by the General ClinicalResearch Center at Children’s Hospital Boston (NationalCenter for Research Resources, General Clinical ResearchCenters Program, National Institutes of Healthgrant M01RR02172). The funding organizations had norole in the design, data analysis, or manuscript preparation.The Children’s Hospital Boston General ClinicalResearch Center was involved in sample processing
terjemahan.
LATAR BELAKANG. Procalcitonin telah diidentifikasi sebagai penanda darah yang berguna infeksi bakteri serius pada bayi demam.Banyak bayi hadir dengan reaksi demam setelah menerima imunisasi. Efek dari imunisasi padaprocalcitonin belum diselidiki.
METHODS.We melakukan studi kohort prospektif observasional di sebuah departemen, darurat kota besar pediatrik.Bayi usia _90 hari dengan demam _38 ° C yang terdaftar. Subyek dibagi menjadi 3 kelompok: bayi dengan seriusinfeksi bakteri; subyek tanpa infeksi bakteri serius yang menerima terakhir (_48 jam) imunisasi, dansubyek tanpa infeksi bakteri serius yang tidak baru-baru menerima imunisasi. Procalcitonin diukurdengan menggunakan uji immunometric kuantitatif.
HASIL. Selama 13 bulan, procalcitonin diukur untuk 271 bayi. Ada 44 (16%) pasien dengan serius

infeksi bakteri, 35 dalam kelompok terakhir-imunisasi, dan 192 pada kelompok tidak-terakhir-imunisasi. Mediantingkat procalcitonin untuk infeksi bakteri yang serius adalah 0,53 ng / mL, untuk imunisasi terakhir adalah 0,29 ng / mL, dan untuktidak ada imunisasi terakhir adalah 0,17 ng / mL. Nilai Procalcitonin terangkat untuk pasien dengan bakteri yang seriusinfeksi dibandingkan dengan pasien baik dengan dan tanpa imunisasi terakhir. Dibandingkan dengan pasien yang tidak memilikiimunisasi terakhir, tingkat procalcitonin meningkat pada pasien dengan imunisasi terakhir. Menggunakan titik potong dari0,12 ng / mL, kepekaan procalcitonin untuk infeksi bakteri yang serius adalah 96%, spesifisitas adalah 23%, dan negatifnilai prediksi adalah 96%. Dua pasien dengan imunisasi terakhir yang mengalami infeksi bakteri seriusdiidentifikasi dengan titik potong.KESIMPULAN. Di antara bayi demam dengan imunisasi terakhir, tingkat procalcitonin meningkat dibandingkan denganpasien dengan demam dan tidak ada infeksi bakteri diidentifikasi. Meskipun peningkatan ini, procalcitonin masih bisa dipercayadiskriminasi bayi dengan infeksi bakteri serius. Pediatri 2008; 122: e1119-e1122TANPA DEMAM AN diidentifikasi sumber infeksimenyajikan keluhan umum di perawatan primerkantor dan departemen darurat. Untuk bayi _3bulan usia, demam bisa jadi hanya tanda yang seriusinfeksi bakteri (SBI). Selain itu, bayi secara rutinKelompok pertama menerima mereka vaksinasi antara 6 dan10 minggu usia. Dengan munculnya Pediarix yang(GlaxoSmithKline, Research Triangle Park, NC) vaksin,ada telah dilaporkan tingkat demam setelahvaksinasi setinggi 27,9% .1 Tidak ada standarevaluasi atau manajemen demam pada baru-baru divaksinasibayi.Penelitian terbaru telah mengidentifikasi procalcitonin sebagaibiomarker bakteri infections.2-6 Kami sebelumnya dilaporkannilai-nilai procalcitonin dalam kohort prospektifbayi _90 hari tua yang disajikan kepada anak-anakgawat darurat dengan demam tanpa source.7Procalcitonin ditemukan untuk menjadi sangat sensitifpenanda SBI pada kohort ini. Efek dari imunisasipada tingkat procalcitonin belum dijelaskan dengan baikdan secara teoritis dapat mengganggu penggunaandari procalcitonin sebagai penanda diagnostik untuk SBI. Di sini,kami menyelidiki efek dari imunisasi baru padakinerja diagnostik procalcitonin di mudademam bayi.METODEPenelitian ini merupakan bagian dari penelitian yang lebih besar menyelidikikinerja procalcitonin sebagai diskriminator SBI diusia ini group.7 Metode studi lengkap yang rincidalam publikasi asli. Kami melakukan prospektif

kohort studi _90 hari bayi usia yang disampaikan kepadadepartemen darurat dengan suhu didokumentasikandari _38.0 ° C. Bayi dikeluarkan jika mereka memilikiKata Kunci: demam, bayi, imunisasi, vaksinasi, procalcitoninSingkatan: SBI, infeksi bakteri yang serius; RI, imunisasi terakhir; NRI, tidak baru-baru iniimunisasi; CI, interval kepercayaan, ISK, infeksi saluran kemih, WBC, darah putihsel, NPV, nilai prediksi negatifwww.pediatrics.org/cgi/doi/10.1542/peds.2008-1884doi: 10.1542/peds.2008-1884Diterima untuk publikasi, 21 Juli 2008Alamat korespondensi untuk Andrew pengoles, MD, Rumah Sakit Anak Boston, DivisiEndokrinologi, LO-605, 300 Longwood Ave, Boston, MA 02115. E-mail: andrew.dauber @ anak-anak.harvard.eduPediatrics (ISSN Nomor: Cetak, 0031-4005; Online, 1098-4275). Hak Cipta © 2008 olehAmerican Academy of PediatricsPediatri Volume 122, Nomor 5, November 2008 e1119Download dari www.pediatrics.org. Diberikan oleh Indonesia: AAP sponsor pada 12 Desember 2010kronis yang mendasari penyakit atau penggunaan antibiotik dalamsebelumnya 48 jam.Pasien diklasifikasikan sebagai memiliki SBI jika mereka memilikidarah, urin, atau budaya serebrospinal yang tumbuh patogen yangorganisme atau memiliki radiograf dada yang ditafsirkanoleh seorang ahli radiologi menghadiri yang didiagnosispneumonia. Subyek dibagi menjadi 3 kelompok. ParaKelompok pertama termasuk semua pasien dengan SBI terlepas darimereka terakhir imunisasi status (SBI kelompok). Yang keduatermasuk kelompok pasien tanpa SBI yang telahmenerima imunisasi dalam waktu 48 jam sebelumnya(Kelompok RI). Kelompok ketiga termasuk pasientanpa SBI yang belum menerima imunisasi disebelumnya 48 jam (NRI kelompok).Pada saat pendaftaran, dokter yang hadir bertanggung jawabuntuk perawatan pasien menyelesaikan kuesioneruntuk menilai penampilan bayi pada titik 5-skala. Procalcitonin diukur pada sampel yang disimpan olehmenggunakan uji immunometric (Brahms [Hennigsdorf, Jerman]procalcitonin-sensitif kit Kryptor).Analisis statistik dilakukan dengan menggunakan SPSS 14.0(SPSS Inc, Chicago, IL). Untuk variabel kontinyu, mandiri-sampel t tes dan Wilcoxon nonparametrikrank-sum test digunakan; untuk data kategori,Uji eksak Fisher atau _2 analisis digunakan. Analisisdilakukan antara SBI dan kelompok RI, SBI danKelompok NRI, dan RI dan kelompok NRI. Kepercayaan 95%interval (CI) untuk proporsi dihitung dengan menggunakan

Stata 6 (Stata Corp, College Station, TX).Penelitian ini disetujui oleh Rumah Sakit AnakBoston papan review kelembagaan dan sesuaidengan Asuransi Kesehatan Portabilitas dan AkuntabilitasAct of 1996.HASILSelama masa penelitian, 874 bayi _90 hari tua dengansuhu _38 ° C dievaluasi dalam keadaan daruratdepartemen. Lima puluh dua pasien bertemu pengecualiankriteria. Dari 822 pasien yang tersisa, persetujuan itudiperoleh untuk 501 (61%) dari mereka. Dari pasien, kitamampu mengukur tingkat procalcitonin daridarah yang tersedia spesimen dalam 271 pasien (54% dari persetujuanpasien yang memenuhi kriteria).Dari 271 pasien yang terdiri dari kelompok studi, adaadalah 44 (16%) pasien dalam kelompok SBI, 35 (13%)pasien dalam kelompok RI, dan 192 (71%) pasien dalamNRI kelompok. Dari 44 SBI, 33 adalah infeksi saluran kemih(UTI), 2 adalah UTI dengan bakteremia, 4 adalah bakteremia,dan 5 pneumonia. Demografi daribayi dalam 3 kelompok disajikan pada Tabel 1. Sebagaidiprediksi oleh waktu imunisasi, usia rata-ratadari pasien dalam kelompok RI secara signifikan lebih tinggi daridalam kelompok SBI dan NRI. Para pasien secara signifikanlebih baik muncul pada kelompok RI dibandingkankepada mereka dalam kelompok SBI tetapi tidak dibandingkan denganpada kelompok NRI.Sel darah putih (WBC) dan data procalcitoninuntuk 3 kelompok disajikan pada Tabel 1. WBC nilaisecara signifikan lebih tinggi di SBI dan kelompok RI saatdibandingkan dengan kelompok NRI. Tidak ada perbedaandalam hitungan WBC rata-rata antara RI dan kelompok SBI.Tingkat procalcitonin median secara signifikan lebih tinggi padaSBI kelompok bila dibandingkan dengan kedua RI dan NRIkelompok. Tingkat procalcitonin dalam kelompok RI yangjuga lebih tinggi dari pada kelompok NRI. Gambar 1 menggambarkandistribusi nilai procalcitonin di SBI, RI danNRI kelompok.Dua dari 37 pasien dengan imunisasi terakhir memilikiSBI. Pasien pertama adalah seorang gadis 77-hari-tua dengan suhudari 40,0 ° C yang telah menerima imunisasi 2hari sebelum presentasi. Kultur urin nya tumbuh_100 000 unit pembentuk koloni / mL Escherichia coli. Nyatingkat procalcitonin adalah 0,36 ng / mL. Pasien keduaadalah seorang anak 71-hari-tua yang telah menerima imunisasisebelumnya hari itu dan disajikan dengan suhu38,4 ° C. Kultur urin nya tumbuh 30 000 pembentuk koloniunit / mL E coli. Tingkat procalcitonin Nya adalah 0,211 ng / mL.Menggunakan dipotong diterbitkan sebelumnya kami titik 0,12 ng /mL, kepekaan procalcitonin untuk SBI di seluruh

kohort adalah 96% (95% CI: 83% -99%), spesifisitasadalah 23% (95% CI: 18% -29%), dan prediksi negatifnilai (NPV) adalah 96% (95% CI: 86% -99%).Menggunakan titik potong yang sama untuk 37 pasien yang telahmenerima imunisasi dalam 48 jam terakhir (35 padaRI kelompok dan 2 dengan imunisasi terakhir di SBIkelompok), kepekaan procalcitonin untuk SBI adalah 100%(2 dari 2), dan spesifisitas untuk non-SBI adalah 8,6% (3 dari35). Perhitungan ini dibatasi oleh ukuran sampel yang kecildari 2 pasien dengan SBI dan imunisasi terakhir.PEMBAHASANDemam adalah yang paling sering dilaporkan "serius" dan"Nonserious" peristiwa buruk setelah imunisasi menurutuntuk Event Vaksin Merugikan Pelaporan System.8Hal ini menimbulkan masalah unik dalam mereka bayi _3bulan usia yang berisiko lebih tinggi memiliki SBI.Tabel 1 Perbandingan Subkelompok StudiKelompok SBI(N_44)Kelompok RI(N_35)NRI Kelompok(N_192)PSBI SBI vs vs RI NRI RI vs NRIUmur, rata-rata (SD), d 45 (25) 63 (7) 51 (23) 0,133 0,002 _.001Suhu tertinggi, rata-rata (SD), ° C 38,9 (0,68) 38,7 (0,53) 38,6 (0,46) .207 .002 .32Secara keseluruhan penampilan, median (IQR) dengan 4 (4-5) 5 (4-5) 4 (4-5) .019 .118 .112WBC, rata-rata (SD), 103/_L 14,3 (7,8) 13,8 (4,7) 11,2 (4,2) .781 .001 _.001Procalcitonin, median (IQR), ng / mL 0,53 (0,18-2,50) 0,29 (0,18-0,41) 0,17 (0,12-0,27) 0,017 0,001 _.001IQR menunjukkan kisaran interkuartil.skala Penampilan: 1, "sekarat, beracun, sakit muncul, tidak responsif", 5, "yang sehat bayi, interaktif."pengoles E1120 dkkDownload dari www.pediatrics.org. Diberikan oleh Indonesia: AAP sponsor pada 12 Desember 2010Tidak ada konsensus pada apakah untuk mengobati pasienberbeda dibandingkan dengan demam dan tidak ada sejarah baru-baruimunisasi.Pengaruh vaksinasi pada tingkat procalcitonin telahbelum diteliti dengan baik. Sebuah pencarian database Medline mengungkapkanhanya 1 artikel tentang tingkat procalcitonin setelahvaksinasi: dalam sebuah surat kepada editor dari Pediatric InfectiousPenyakit Journal, 9 Korczowski melaporkan pada kohort17 pasien yang disajikan untuk keadaan darurat pediatrikdepartemen di Polandia dengan vaksinasi terkait merugikanperistiwa. Enam belas pasien memiliki suhudari _38.5 ° C. Usia rata-rata bayi adalah 20 minggu

(Rentang: 6-37 minggu). Para procalcitonin serum rata-ratatingkat pada pasien ini adalah 0,8 _ 0,9 ng / mL (kisaran:0,1-3,6 ng / mL). Tidak ada SBI. Korczowski menyimpulkanbahwa tingkat sederhana procalcitonin dapat meningkatsetelah vaksinasi dengan tidak adanya infeksi.Kita adalah sebuah studi kohort prospektif yang mencakup_90 271 hari tua dengan suhu didokumentasikan bayidari _38 ° C dalam departemen darurat pediatrik. Kamidilaporkan sebelumnya utilitas tingkat procalcitonin untukmemprediksi SBI pada pasien yang tidak menerimaimunisasi dalam 48 jam sebelumnya. Dalam kohort itu,titik potong dari 0,12 ng / mL memiliki sensitivitas 95% (95%CI: 83% -99%), spesifisitas 26% (95% CI: 20% -32%),NPV dari 96% (95% CI: 85% -99%), dan kemungkinan negatifrasio 0,19 (95% CI: 0,05-0,74), semua kasusbakteremia diidentifikasi secara akurat dengan titik cut-nilai.Dalam studi saat ini, kami lebih lanjut subcategorized yangpasien yang dengan SBI, mereka tanpa SBI yang telahbaru-baru menerima imunisasi, dan mereka tanpa SBIyang tidak baru saja menerima imunisasi. Mediantingkat procalcitonin secara signifikan lebih tinggi dalamkelompok bayi yang telah menerima imunisasi dibandingkandengan mereka yang tidak, tetapi secara signifikanlebih rendah dibandingkan pada kelompok SBI. Atas dasar ini, tampaknyabahwa imunisasi menyebabkan peningkatan serum procalcitoninnilai-nilai, tetapi masih dapat digunakan untuk mengidentifikasi kelompokberisiko rendah untuk SBI tanpa memandang status imunisasi. ParaWBC count juga meningkat pada kelompok RI saatdibandingkan dengan non-SBI pasien tanpa imunisasi terakhirtetapi mirip dengan mereka dengan SBI. Oleh karena itu,WBC count, penanda umum digunakan untuk SBI, kurangberguna untuk pasien yang baru menerima vaksinasi.Bila menggunakan memotong diterbitkan sebelumnya kami titik0,12 ng / mL, kepekaan procalcitonin untuk SBI dalamseluruh kelompok adalah 96% (95% CI: 83% -99%), spesifisitasadalah 23% (95% CI: 18% -29%), dan NPV adalah 96% (95%CI: 86% -99%). Secara keseluruhan, penambahan divaksinasi bayike dalam analisis kohort seluruh menyebabkan serupasensitivitas dan NPV tetapi menurun kekhususan dari procalcitonintingkat sebagai penanda SBI. Perubahan ini karenadari sebagian besar pasien diimunisasi memilikiprocalcitonin nilai yang lebih besar dari titik potong kamidari 0,12 ng / mL. Namun, tingkat procalcitonin dapat melanjutkanyang akan digunakan untuk mengidentifikasi pasien yang beresiko rendah untuk SBI,dan dengan menggunakan titik potong yang sama, kedua pasien di kamikohort dengan SBI yang baru menerima imunisasidiidentifikasi.Penelitian kami memiliki beberapa keterbatasan. Penelitian dilakukanpada departemen darurat akademis pediatrik

dan, karenanya, tidak dapat mewakili populasi yang lebih besarpasien setelah imunisasi. Selain itu, bahkan di antaraorang demam bayi yang baru-baru divaksinasi dandisajikan dengan demam, mungkin ada bias yang telahsetiap evaluasi laboratorium. Selain itu, kami tidak mengumpulkaninformasi tentang jenis vaksinasi yang diterimadan, dengan demikian, tidak dapat memberikan rincian lebih lanjut tentang spesifikefek dari vaksin individu pada nilai-nilai procalcitonin.SBI RI NRIStudi subkelompok543210Procalcitonin, ng / mLGAMBAR 1Perbandingan dari subkelompok studi. Kotak mewakilibatas dari persentil 25 dan 75 dan dibagidengan garis di median. Kumis mewakili 1,5 kaliIQR tersebut.Pediatri Volume 122, Nomor 5, November 2008 e1121Download dari www.pediatrics.org. Diberikan oleh Indonesia: AAP sponsor pada 12 Desember 2010Akhirnya, definisi kami SBI yang dimaksudkan untuk menjadi konservatifuntuk mencakup semua SBI mungkin, karena kamiberharap untuk mengidentifikasi kelompok berisiko rendah untuk SBI. Kami mengakuibahwa beberapa pasien dengan rendah-koloni-hitunganUTI dan pneumonia radiografi mungkin tidak terwakilibenar bakteri infeksi. Studi awal kami menyediakanlanjut analisis terhadap SBI yang pasti dan mungkin untukaccount ini kesulitan dalam definisi.KESIMPULANDi antara bayi demam muda dengan imunisasi terakhir,tingkat procalcitonin meningkat dibandingkan dengan pasiendengan demam dan tidak ada infeksi bakteri diidentifikasi.Meskipun peningkatan ini, tingkat procalcitonin masih bisa dipercayadiskriminasi bayi dengan SBI.UCAPAN TERIMA KASIHKami berterima kasih kepada rekan-rekan dokter di daruratdepartemen yang memfasilitasi pendaftaran untuk penelitian,dan kami mengucapkan terima kasih atas bantuan dan keahlianRichard Snider, PhD, dan Robyn Neches, BS, untuk bekerjapada tes procalcitonin.Kami berterima kasih atas dukungan keuangan FrederickH. Lovejoy, Jr, MD, Residen Research Fund danAmerican Academy of Pediatrics Residen PenelitianGrant. Selain itu, kita mengakui dukungan teknis

terkait dengan pemrosesan spesimen oleh Klinis UmumResearch Center di Rumah Sakit Anak Boston (NasionalPusat Penelitian Sumber Daya, Penelitian Klinis UmumPusat Program, Institut Kesehatan Nasionalhibah M01RR02172). Organisasi pendanaan tidakperan dalam desain, analisis data, atau persiapan naskah.Anak-Anak Rumah Sakit Umum Boston KlinisPusat Penelitian terlibat dalam pengolahan sampel.
PROCALCITONIN
Procalcitonin (PCT) is a peptide precursor of the hormone calcitonin, the latter being involved with calcium homeostasis. It is composed of 116 amino acids and is produced by parafollicular cells (C cells) of the thyroid and by the neuroendocrine cells of the lung and the intestine.
The level of procalcitonin in the blood stream of healthy individuals is below the limit of detection (10 pg/mL) of clinical assays.[1] The level of procalcitonin raises in a response to a proinflammatory stimulus, especially of bacterial origin. In this case, it is produced mainly by the cells of the lung and the intestine. It does not raise significantly with viral or non-infectious inflammations. With the derangements that a severe infection with an associated systemic response brings, the blood levels of procalcitonin may rise to 100 ng/ml. In serum, procalcitonin has a half-life of 25 to 30 hours. Remarkably the high procalcitonin levels produced during infections are not followed by a parallel increase in calcitonin or serum calcium levels.
Contents [hide]
1 Uses o 1.1 Diagnosis and prognosis of sepsis o 1.2 Diagnosis of bacteremia o 1.3 Prognosis of pneumonia
2 References
3 External links
[edit] Uses
[edit] Diagnosis and prognosis of sepsis
Measurement of procalcitonin can be used as a marker of severe sepsis and generally grades well with the degree of sepsis,[2] although levels of procalcitonin in the blood are very low. PCT has the greatest sensitivity (85%) and specificity (91%) for differentiating patients with SIRS from those with sepsis, when compared with IL-2, IL-6, IL-8, CRP and TNF-alpha.[3] Evidence is emerging that procalcitonin levels can reduce unnecessary antibiotic prescribing to people with lower respiratory tract

infections.[4] Currently, procalcitonin assays are widely used in the clinical environment.[5]
[edit] Diagnosis of bacteremia
A meta-analysis reported a sensitivity of 76% and specificity of 70%.[6]
[edit] Prognosis of pneumonia
A cluster randomized trial found that the procalcitonin level can help guide antibiotic therapy. In this trial, "on the basis of serum procalcitonin concentrations, use of antibiotics was more or less discouraged (<0.1 mcg/L or <0.25 mcg/L) or encouraged (> or =0.5 mcg/L or > or =0.25 mcg/L), respectively".[7] However, an earlier nonrandomized, observational study reported "limited, prognostic value" of procalcitonin measurement.[8]
Procalcitonin levels may be useful to distinguish bacterial infections from nonbacterial infections. Trials from 2008 and 2009 have shown that they may help guide therapy and reduce antibiotic use, which can help save on cost of antibiotic prescriptions and drug resistance.
Procalcitonin May Help Guide Antibiotic Use in Intensive Care Units
January 27, 2010 — A procalcitonin-guided strategy to treat suspected bacterial infections in nonsurgical patients in intensive care units (ICUs) may safely reduce antibiotic exposure and selective pressure, according to the results of a multicenter, prospective, parallel-group, open-label trial reported online January 23 in The Lancet.
Procalcitonin is a calcitonin precursor hormone thought to be a fairly specific marker for severe bacterial infection in patients with suspected sepsis. Use of blood procalcitonin concentration to guide antibiotic use has been associated with markedly less antibiotic prescriptions in patients seen in the emergency department or hospitalized for lower respiratory tract infections.
"Reduced duration of antibiotic treatment might contain the emergence of multidrug-resistant bacteria in intensive care units," write Lila Bouadma, MD, from Université Paris 7–Denis-Diderot, Hôpital Bichat–Claude-Bernard, Assistance Publique-Hôpitaux de Paris in Paris, France, and colleagues from the PRORATA trial group. "We aimed to establish the effectiveness of an algorithm based on the biomarker procalcitonin to reduce antibiotic exposure in this setting."
Inclusion criteria were expected length of ICU stay of more than 3 days, suspected bacterial infection, and age 18 years or older. Patients were randomly assigned in a 1:1 ratio to receive procalcitonin (n = 311) or to a control group (n = 319) with use of an independent, computer-generated randomization sequence. The investigators were blinded to assignment before randomization but not subsequently.

On the basis of predefined cutoff ranges of procalcitonin concentrations, antibiotics were started or stopped for patients in the procalcitonin group. In the control group, antibiotics were prescribed according to current guidelines. The treating physician controlled drug selection and the final decision to start or stop antibiotics. The main study outcomes were mortality at days 28 and 60 (noninferiority analysis) and number of days without antibiotics by day 28 (superiority analysis). Analyses were by intent-to-treat, with use of a 10% margin of noninferiority.
After exclusion of 9 patients, analyses included 307 patients in the procalcitonin group and 314 in the control group. Compared with the control group, the procalcitonin group had apparently noninferior mortality at day 28 (21.2% [65/307] vs 20.4% [64/314]; absolute difference, 0.8%; 90% confidence interval [CI], –4.6 to 6.2) and day 60 (30.0% [92/307] vs 26.1% [82/314]; absolute difference, 3.8%, 95% CI –2.1 to 9.7).
Compared with the control group, the procalcitonin group also had significantly more days without antibiotics (14.3 ± 9.1 days vs 11.6 ± 8.2 days; absolute difference, 2.7 days; 95% CI, 1.4 - 4.1; P < .0001).
"A procalcitonin-guided strategy to treat suspected bacterial infections in non-surgical patients in intensive care units could reduce antibiotic exposure and selective pressure with no apparent adverse outcomes," the study authors write. "The diverse clinical characteristics and reasons for admissions to the intensive care unit for patients enrolled in this study suggest that our conclusions could be applicable to most non-surgical patients in the intensive care unit, including those who are immunocompromised."
Limitations of this study include open design, inability to extrapolate the findings to surgical patients, lack of algorithm-guided treatment in more than half of patients randomly assigned to the procalcitonin group, and definitions of relapse and superinfection based on microbiological criteria.
"We stress that infection is the tip of the iceberg compared with digestive colonisation," the study authors conclude. "Rectal, nasal, and axillary swab screening was not routinely done and might more accurately show antibiotic selective pressure. Moreover, a 3-day reduction of antibiotic use for only a small subset of admitted patients might not be sufficient to record a decreased resistance-emergence rate, especially for some intensive care units with high cross-transmission rates."
In an accompanying comment, Marin H. Kollef, MD, FACP, from Washington University School of Medicine in St. Louis, Missouri, discusses treatment bias and other potential limitations of this study.
"Experience so far suggests that unnecessary antibiotic use can be curtailed in the hospital setting, particularly within intensive care units," Dr. Kollef writes. "Whether the ideal strategy involves the use of a serum marker such as procalcitonin or a locally applied practice protocol remains to be established."
Assistance Publique-Hôpitaux de Paris, France, and Brahms, Germany supported this study. Some of the study authors have disclosed various financial relationships

with Brahms, Merck Sharp & Dohme-Chibret, AstraZeneca, Lilly, Pfizer, Wyeth, Johnson & Johnson, Nektar-Bayer, Arpida, Janssen-Cilag, Gilead, and/or AstraZeneca. Dr. Kollef has disclosed no relevant financial relationships.
Lancet. Published online January 23, 2010.
http://www.medscape.com/viewarticle/716014
Sepsis is systemic inflammation due to infection. It is the most common cause of death in intensive care units (1), with a mortality rate up to 50% depending on severity. Sepsis can be considered in individuals with systemic inflammatory response syndrome (SIRS) manifested by alterations in at least two of temperature, heart rate, respiratory rate, and/or white blood cell count. These SIRS criteria are non-specific for sepsis and may be present in alternative pathophysiologic states, both medical and surgical (1). The earlier sepsis is identified and treated the better the prognosis (1). Currently diagnosis involves documentation of infection (by culture) in patients with SIRS. Cultures take at least 24 hours and > 50% may be false negative and 30% false positive. A biomarker that could identify sepsis early in a population of patients with overlapping clinical symptoms, i.e. patient’s with non-infectious SIRS would improve patient care. Many suggest that Procalcitonin (PCT) is an ideal sepsis biomarker. PCT is the pro-hormone form of calcitonin and is produced by extra-thyroidal immune cells within 2-4 hours of a bacterial insult and/or inflammatory response. Elevated PCT is seen in septic patients and concentrations correlate with severity of disease. Increasing PCT over time is associated with poor prognosis, while decreasing concentrations correlate to good prognosis and/or response to antibiotic therapy. Thus, proponents suggest that the clinical utilities of PCT are: to differentiate patients with sepsis from those with non-infectious SIRS; to guide antibiotic therapy; and to predict prognosis of critically ill patients (2). Procalcitonin: an early predictor of sepsis? Thousands of studies have investigated the clinical utility of almost 200 biomarkers of sepsis (3). Among these, PCT and CRP are most often referenced. In comprehensive reviews comparing their diagnostic accuracies, PCT consistently performs better, but sensitivity and specificities to predict sepsis are <90% for both markers. Two meta-analyses recommend routine use of PCT for diagnosis of sepsis while two others discourage its use (3-6). Why the discrepancy? Lack of a gold standard for sepsis diagnosis. Diverse patient populations--PCT is elevated postsurgery, trauma, or in other instances of systemic inflammation limiting its diagnostic accuracy. Different PCT cut-offs are used. Sepsis is diagnosed retrospectively with knowledge of bacterial cultures and a full clinical picture in most studies. To date, few studies have addressed the utility of PCT to predict sepsis in “real time”. Until, large real time studies with well defined patient populations are completed, the utility of PCT to predict sepsis will remain controversial. Does PCT have a role in tailoring antibiotic therapy?Overuse of antibiotics in ICU settings has contributed to the increase in antibiotic resistant bacteria. Most randomized control trials demonstrate that using serial

PCT based algorithms to guide continuation/cessation of antibiotic therapy reduces the number of days patients are on antibiotics without adverse effects. None has demonstrated a reduction in multidrug resistant (MDR) bacterial infections (7). In practice, there is limited utility for PCT to guide initiation of antimicrobial therapy because most ICU patients are taking antibiotics at admission. Further, these algorithms are not effective in patients with recent trauma, surgery or other global inflammation. Thus, PCT based algorithms for guiding antibiotic therapy are limited to guiding secession/continuation of therapy in non-surgical/trauma ICU patients. And even in these populations, serial PCT measurements may be cost prohibitive if no reduction in MDR infections is observed. Can procalcitonin be used to predict prognosis?Increasing PCT concentrations correlate with increasing severity of sepsis and poor outcome, while decreasing or low PCT predicts a good prognosis for ICU patients. Most studies exclude patients with a recent trauma, surgery or other inflammatory event (6). Given the complicated pathobiology of sepsis and significant overlap in clinical symptoms with SIRS patients, it may be that no one biomarker works for sepsis. Studies looking at multi-biomarker panels have shown promise in the prediction and monitoring of sepsis in ICU and ED patients (3). http://www.aacc.org/members/nacb/NACBBlog/lists/posts/post.aspx?ID=16