
Issues in contraception
48
Issues in Contraception: Worth Talking About Dr Nurulhuda Samsudin
-
Upload
chaimingcheng -
Category
Documents
-
view
254 -
download
2
Transcript of Issues in contraception

Issues in
Contraception:
Worth Talking
AboutDr Nurulhuda Samsudin
What’s worth talking about?
• Everything.
What’s worth talking about in < 45 minutes?
The contraception “quick user manual”
• Getting started
- Making the right contraception choice.
• Troubleshooting
- Missed pills
- Delayed injectables
• Help
- Emergency contraceptions
Getting Started- What affect the couple’s
choice?
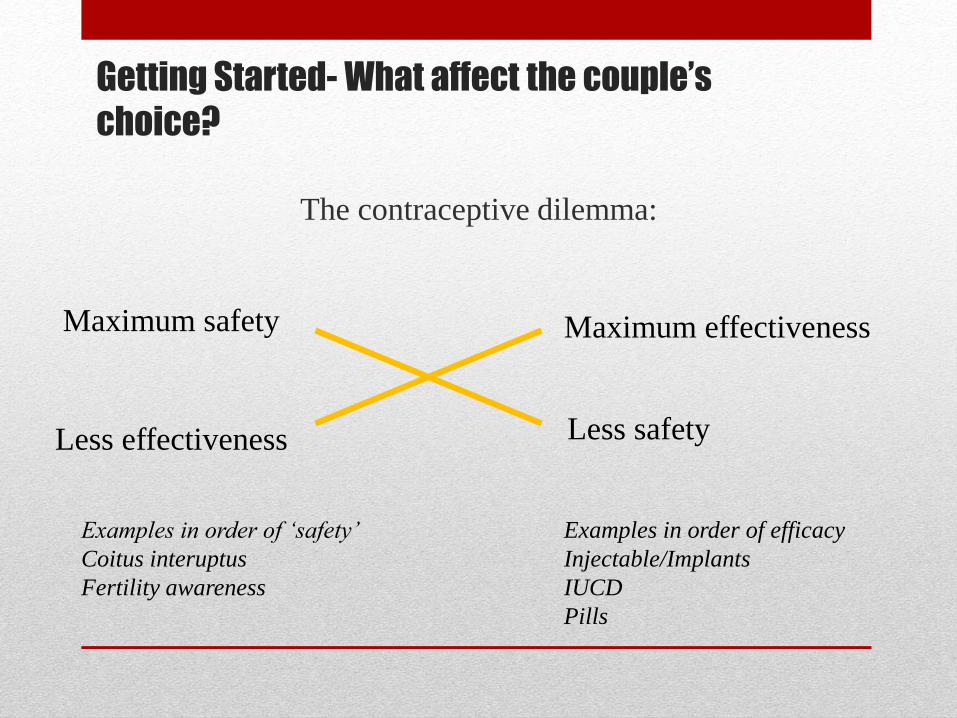
The contraceptive dilemma:
Maximum safety Maximum effectiveness
Less effectiveness Less safety
Examples in order of ‘safety’
Coitus interuptus
Fertility awareness
Examples in order of efficacy
Injectable/Implants
IUCD
Pills

Getting Started- Reproductive Decision- The Factor Wheel
Reproductive Decisions
Use of Contraception
Society
Culture
Religion
StatusAbortion laws
Personal attitude
Availability
Contraception methods
Service availability
Personnel
Children and their
valueIndividual
identity
Career
Self esteem
Unconscious factor
Couple relationship
Expectations
Family/Parents
Friends
Peer group
Class
Education
Knowledge
Beliefs
Myth

Getting Started- Knowing your patientThe 7 contraceptive ages
Age
0 Birth to puberty Sex and reproductive health education
1 Puberty to marriage(or equivalent) Pills, Injectables/Implants (WHO 2)
+ Condoms – protection against STD
* Emergency contraception
2 Marriage to equivalent to 1st child Any methods
Followed by fertility awareness
3 During breastfeeding LAM, POP, barrier
IUCD, Injectables, implants (LARC)– for
long spacing.
4 After breastfeeding Continue with ‘age 3’ method.
Shift to COCP or LARC
5 After the (probable) last child LARC, Pills, Barrier
6 Family complete IUCD/ male or female sterilisation
7 Perimenopausal (no sterilisation) IUCD

Trouble Shooting
Barrier method
Coitus interruptus
Calendar method
IUCD
Emergency Contraception
Missed pills
Delayed injectables
Precautionary & corrective
steps
+/-Emergency
contraception

Missed Pill-
COCP/CHC

Missed Pills- COCP/CHC
• Getting to concept right- The Horse Shoe

The Pill Free Period

The Scientific Advice for Missed Pills- Shut the door and
keep it shut!
• 7 consecutive pills are enough to put the ovaries to sleep- Shutting the door.
• Thereafter, 8-21 pills are simply to maintain the ovaries in quiescence- keeping the door shut.
• More than 7 pills missed in total risks ovulation. Remember horse shoe.

2 Unresolved
Issues…even experts
disagree
• What constitute “missed pill”?
• COCP containing 30-35mcg EE versus Ultra Low Dose
COCP containing 20mcg EE.

What Constitute Missed Pills- The Debate
Continues
• Missed pills- trigger for
the pill taker to take
specific action other than
continue pill taking.
• 2 determining factors:
- Time of cycle.
- Number of pills.
The objective of the WHO was to
provide an evidence-based yet simple and
harmonized guide for missed pill taking.

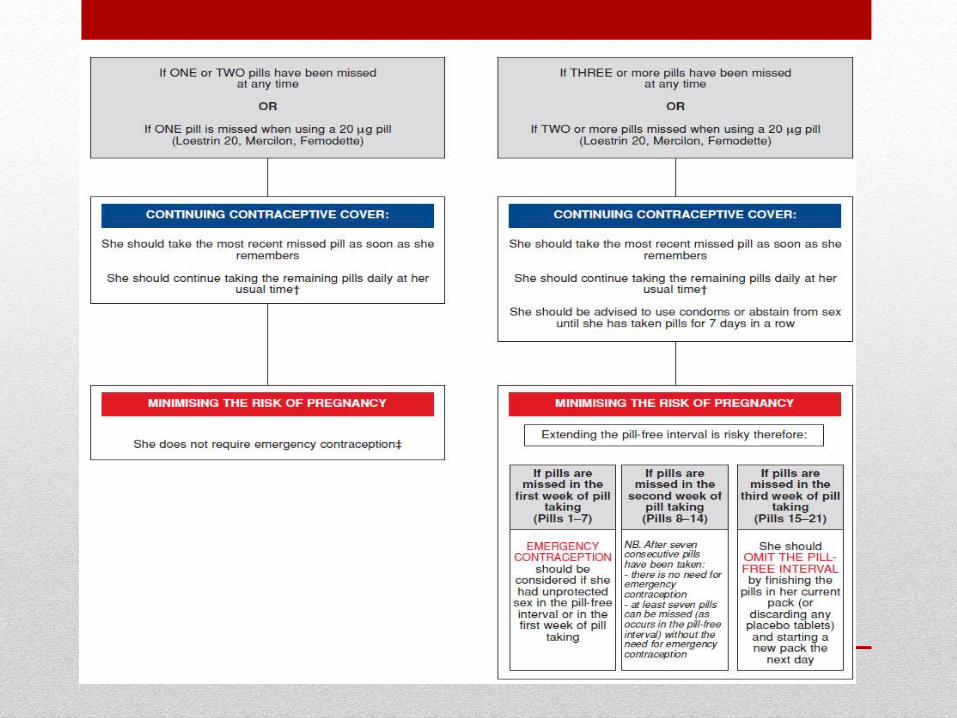
FFPRHC (2005) aides memoir for ‘missed pill rules’
• Just keep going.
• She should take a pill as soon as possible and then resume her usual pill-taking schedule.
• If the missed pills are in Week 3 she should omit the pill-free interval.
• A back-up method (usually condoms) or abstinence should be used for 7 days if the following numbers of pills are missed:
Two for twenty [i.e. if two or more 20 μg ethinylestradiol (EE) pills are missed]
Three for thirty (i.e. if three or more 30–35μg EE pills are missed]
Lightweight vs Featherweight
• COCP containing 30-35mcg EE versus Ultra Low Dose
COCP containing 20mcg EE.
• Evidence is limited on the pregnancy risk when missing
pills contain ≤20μg EE, but theoretically the pregnancy
risk may be higher.
• “Cautious approach is advised when missing these
COCs.”- FFPRHC Guidance (July 2006)

WHOSPR & FFPRHC (2005) Guidelines-The Critism
• Many women are unsure of the dose of ethinylestradiol in their pill, having two rules, one for 30–35mcg pills and one for 20mcg pills, would lead to confusion. “One rule for all” would be better.
• There is no universally accepted definition of a “missed pill.” There is no definition in the recommendations.
? Extending the dose regimen to more than 36 h (taking a contraceptive pill more than 12 h late from the designated daily time).
? Being 2 days late starting the contraceptive pill after a pill-free interval might mean between 49 h and 71 h late.
Extra hormone-free hour matters.
• There is no strong evidence that it is safe to miss up to three 30–35mg pills at the start of a new pack without using back-up contraception or EC.
Ovulation after deliberate extension of the pill-free interval has been documented and is linked to the type and dose of steroids used, the administration regimen, users' adherence, and the individual responsiveness of women taking the combined oral contraceptive pill
The small studies done to detect ovulation after deliberate extension of the HFI were not powered to detect wide inter-individual variability.
Mansour & Fraser;The Lancet, Volume 365, Issue 9472, Pages
1670 - 1671, 14 May 2005

Similiarly….
• “ In my view it is very unfortunate that the latest
(2005)WHOSPR – on which Faculty (UKMEC) and fpa
leaflet advice is based- issued instruction ( against my advice)
which differ according to the estrogen dose in particular pill.
I argue this is illogical, given that individual variation in blood
levels and response to contraceptive hormones is so great.
Even with the 30-53mcg brands, ovulation has been
demonstrated occasionally if the PFI is lengthened to only 8
or 9 days”
[Guillebaud J 2005 Journal of Family Planning and Reproductive Health Care
31:252]
The Response..
• The scientific evidence base of WHOSPR has not changed significantly since 2005.
• Anecdotal evidence suggests that women and health professionals found the 2005 rules complicated and difficult to use.
• The rules were not universally adopted and the pharmaceutical industry continued to give patient information advising the original missed pill rules in patient information leaflets, which suggested reduced efficacy after a pill was 12 hours late.
• The UK Medicines and Healthcare products Regulatory Agency (MHRA) identified a need for clearer, more consistent rules and issued new missed pill guidance in 2011, which has been approved by the FSRH.

FSRH Guidance (October 2011)
Combined Hormonal Contraception

Missed Pills- POP

Understanding POP
• All POP alter cervical mucus to
prevent sperm penetration.
• Traditional POP prevents
ovulation but the effect are
variables.
• Desogestrel only pill
(Cerazette) results in
anovulatory cycles in 97% of
users.
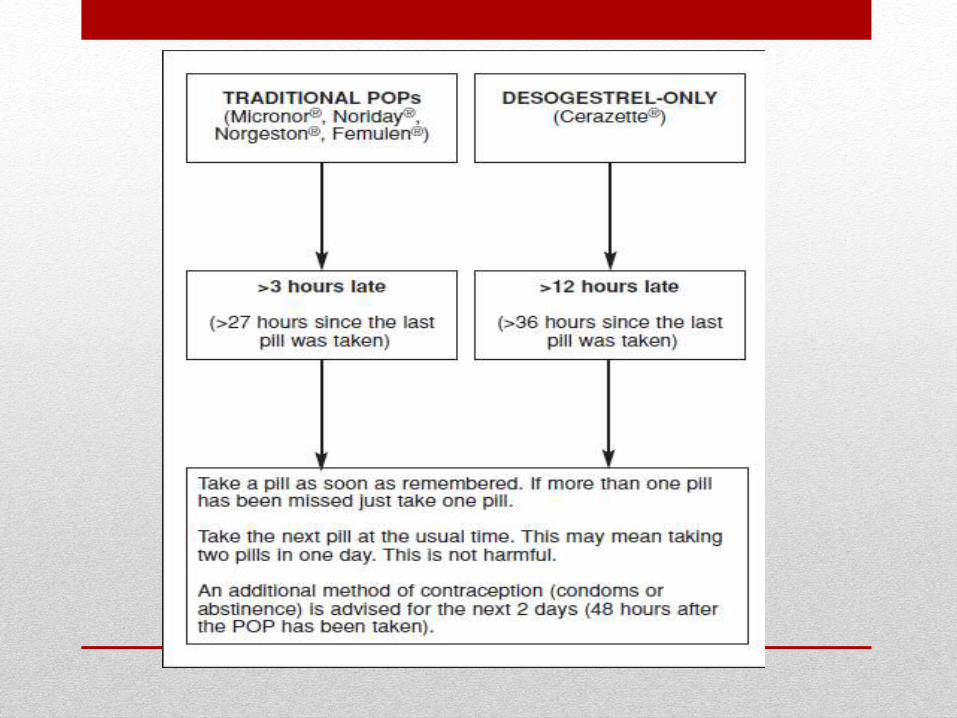
Missed POP- Indication for EC
• This decision should be based on the mucus effect.
• Emergency contraception (EC) should be offered for any unprotected intercourse that occurred:
After the 3-h delay (more than 27 h since the last pill) which might lead to loss of the mucus effect, but before two pills have been taken to restore it.
• A minimum 2 days of extra precautions should then follow.
• For Cerazette, if unprotected sex occurs more than 36 h since the last pill, EC should be offered, followed by 2 days of extra precautions.

Progesterone Only Injectables- Delayed
Injections and The Controversies
• What is the time frame for delayed injection for minimal risk of ovulation?
• Using anovulants models, the risk of conception is low up to 7 days delayed injection.
• Most international guidelines e.g FSRH, CDC gives 2 weeks leeway.
• “DMPA can be given up to 4 weeks late without requiring additional contraceptive protection. For NET-EN, the repeat injection can be given up to 2 weeks late without requiring additional contraceptive protection.”
WHO SPPR 2008

Response to the WHOSPR recommendation by CDC 2013
• A systematic review identified 12 studies evaluating time to pregnancy or ovulation after the last injection of DMPA.
Pregnancy rates were low during the 2-week interval following the reinjection date.
For 4 weeks following the reinjection date, data were sparse and one study included a large proportion of breastfeeding women.
Paulen ME, Curtis KM. When can a woman have repeat progestogen-only injectables—depot medroxyprogesterone acetate or norethisterone enantate? Contraception 2009;80:391–408
• Studies also indicated a wide variation in time to ovulation after the last DMPA injection, with the majority ranging from 15 to 49 weeks from the last injection.

Delayed Injectables
FSRH guidelines 2008

Emergency Contraception- The important
role in reducing unintended pregnancies
• Emergency contraception can reduce the risk of unintended pregnancies.
• The number of unintended pregnancy is increasing.
Teenage pregnancies.
Poor contraception prevalance rate among older/married couple in Malaysia.
Rising rape cases.
The number of rape cases has risen from 1 760 in 2004 to 3 262 in 2009.4
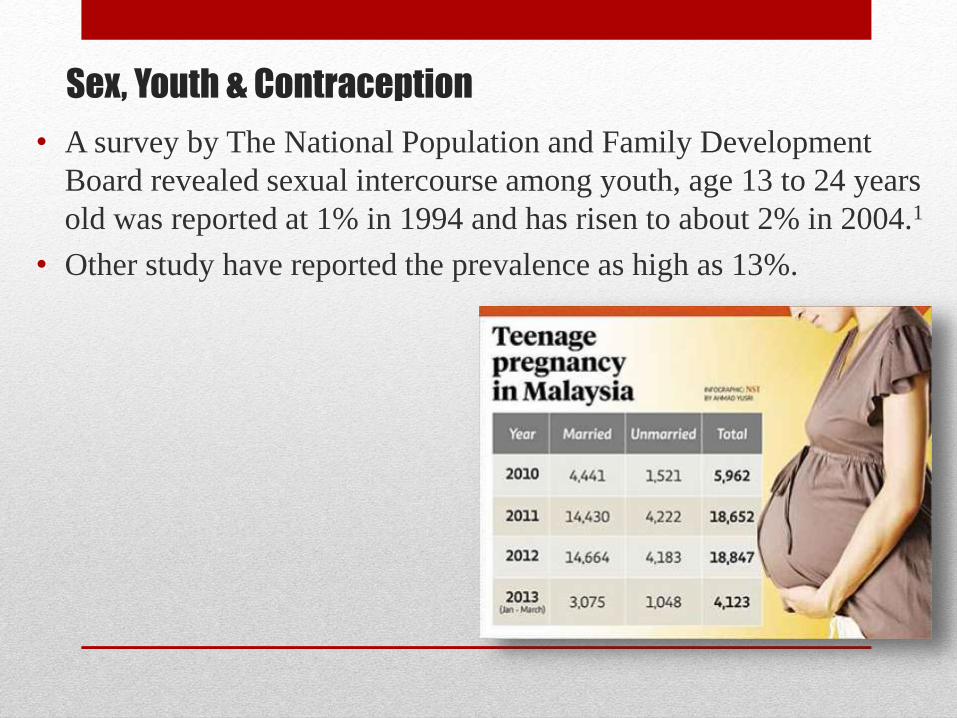
Sex, Youth & Contraception
• A survey by The National Population and Family Development
Board revealed sexual intercourse among youth, age 13 to 24 years
old was reported at 1% in 1994 and has risen to about 2% in 2004.1
• Other study have reported the prevalence as high as 13%.
Sex, Youth &
Contraception- Serious
unmet need for
contraception

Contraception Prevalance Rate Among
Married Couple
• In Malaysia there is an increasing trend in the CPR between 1966 to 1994, then it plateau at about 50%.
• The recent figure in 2004 showed that only 51.7% of married Malaysian women are practicing family planning.
• The main reasons given:
Plan to conceive (39%),
Concerned of side effects (27%) and
Not permitted by the husbands (13%).
Prevention of Unintended Pregnancies-
Why it Matters
• Unwanted effects of teenage pregnancies:
High risk pregnancy.
Social problem e.g dropping out from school,unemployment etc.
Illegal abortion.
Baby dumping.
• Report on the Confidential Enquiries into Maternal Death (CEMD) Malaysia 2001 – 2005 which revealed that up to 70% of the maternal deaths never practiced any form of family planning.

Emergency Contraceptions
• Copper-bearing intrauterine device (Cu-IUD)
• Yuzpe regime
• Levonorgestrel (LNG)
• Ulipristal acetate (UPA)
Copper-bearing intrauterine device (Cu-IUD)
• Copper is toxic to the ovum and sperm.
• (Cu-IUD) is effective immediately after insertion and works primarily by inhibiting fertilisation.
• It has both pre & post fertilisation effect.
• Highly efficacious, failure rate < 1%
• There is also an anti-implantation effect.
A potential arbotificient.
Medico legal and ethical implication.
Thus, it should be inserted before implantation.
Mean time from ovulation to implantation is 9 (range 6–18) days
Should be fitted within the first 5 days (120 hours) following first UPSI in a cycle or within 5 days from the earliest estimated date of ovulation.
Case Illustration
• Regina v. Dhingra 24 January 1991, Mr Justice Wright
did not convict a GP accused of illegal abortion by
inserting IUCD 11 days after intercourse.
“ I further hold, in accordance with the uncontroverted
evidence that I have heard, that a pregnancy cannot come
into existence until the fertilized ovum has become
implanted in the womb, and that stage is not reached
until, at the earliest, the 20th day of a 28-day cycle and in
all probability, until the next period is missed.”
LNG – MECHANISM OF ACTION
• Levonorgestrel (LNG) works primarily by inhibition of ovulation.
• LNG taken prior to the luteinising hormone surge has been shown to result in ovulatory dysfunction in the subsequent 5 days.
• LNG can thus inhibit ovulation for 5–7 days, by which time any sperm in the reproductive tract will have become non-viable.
LNG 1.5mg LNG 0.75mg per tablet
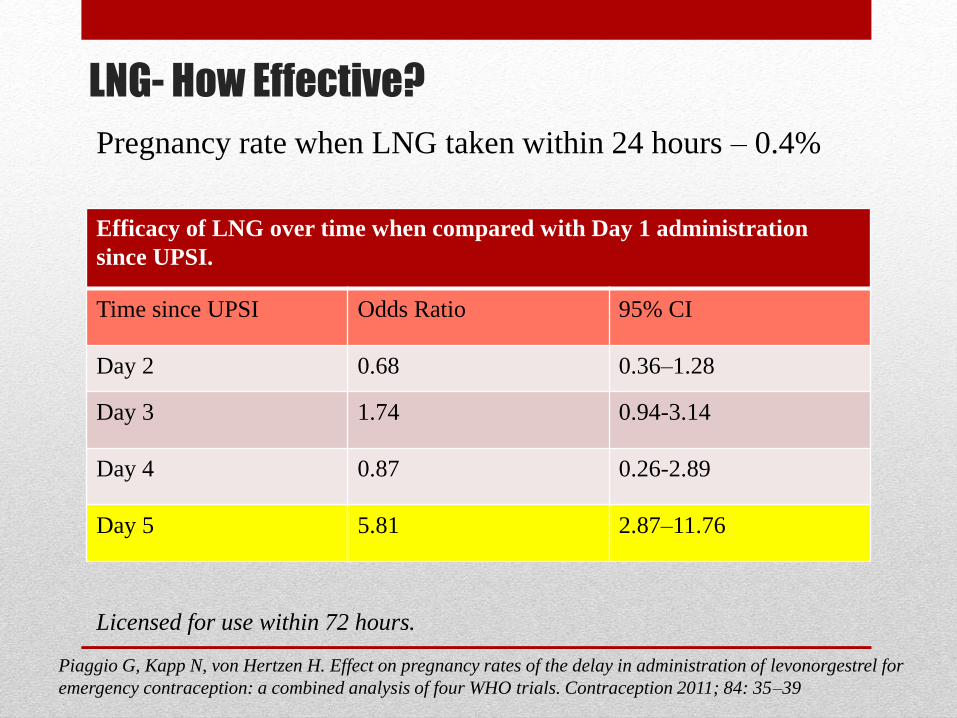
LNG- How Effective?
Efficacy of LNG over time when compared with Day 1 administration
since UPSI.
Time since UPSI Odds Ratio 95% CI
Day 2 0.68 0.36–1.28
Day 3 1.74 0.94-3.14
Day 4 0.87 0.26-2.89
Day 5 5.81 2.87–11.76
Pregnancy rate when LNG taken within 24 hours – 0.4%
Licensed for use within 72 hours.
Piaggio G, Kapp N, von Hertzen H. Effect on pregnancy rates of the delay in administration of levonorgestrel for
emergency contraception: a combined analysis of four WHO trials. Contraception 2011; 84: 35–39

LNG- Side effects & Interactions
• Headache, nausea and altered bleeding patterns.
• If a woman vomits within 2 hours of taking LNG she should take a further dose as soon as possible or offer IUCD.
• If in doubt about whether menstruation has occurred, a pregnancy test should be performed ≥3 weeks after UPSI has occurred.
• Women on liver enzyme-inducing drugs or who have stopped using them (≤28 days ago) should be offered a Cu-IUD.

Yuzpe Regimen
Dr Al Yuzpe MD, FRCS
Yuzpe Method
• Devised in the mid 1970s.
• The original method consist of 2 tablet of COCP containing 250mcg LNG with 50mcg EE taken 12 hours apart.
• This has been supplanted by progesterone only EC.
• Also, the high dose COCP has been largely replaced by low dose COCP.
• Modified Yuzpe method;
e.g Micrgynon (30mcg EE, 15mcg LNG) 4 tablets taken 12 hours apart.
• Started within 72 hours of UPSI.
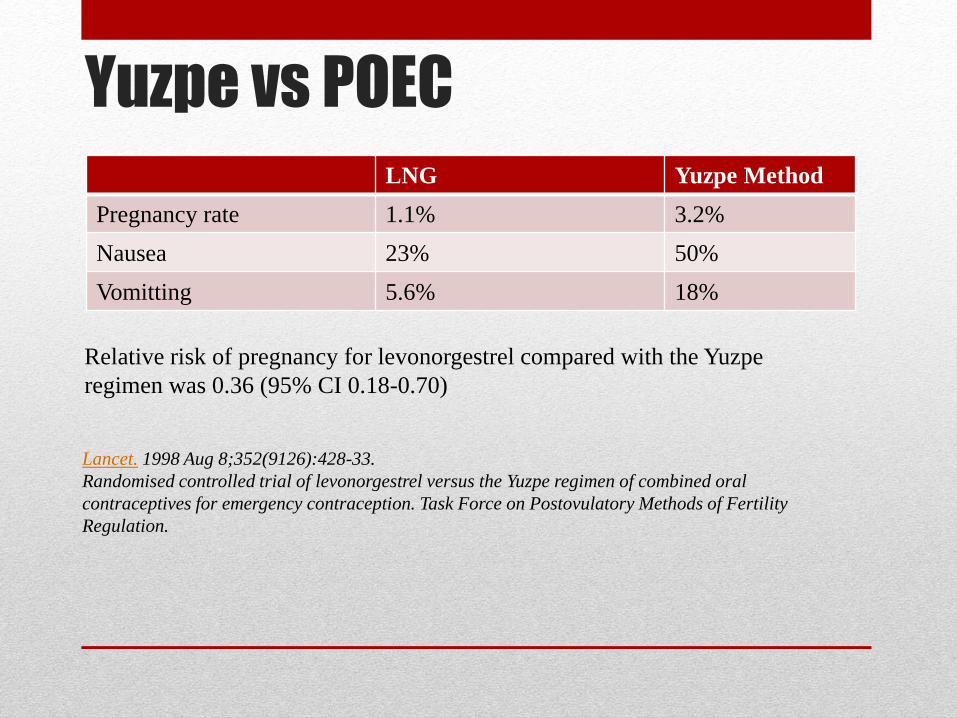
Yuzpe vs POEC
Relative risk of pregnancy for levonorgestrel compared with the Yuzpe
regimen was 0.36 (95% CI 0.18-0.70)
Lancet. 1998 Aug 8;352(9126):428-33.
Randomised controlled trial of levonorgestrel versus the Yuzpe regimen of combined oral
contraceptives for emergency contraception. Task Force on Postovulatory Methods of Fertility
Regulation.
LNG Yuzpe Method
Pregnancy rate 1.1% 3.2%
Nausea 23% 50%
Vomitting 5.6% 18%

Ulipristal Acetate
• A progesterorne receptor modulator.
• Work by inhibition or delay of ovulation.
• Administered within 120 hours.
• No apparent decline in efficacy within that time period.
Fine P, Mathe H, Ginde S, Cullins V, Morfesis J, Gainer E. Ulipristal acetate taken 48–120 hours after
intercourse for emergency contraception. Obstet Gynecol 2010; 115: 257–263
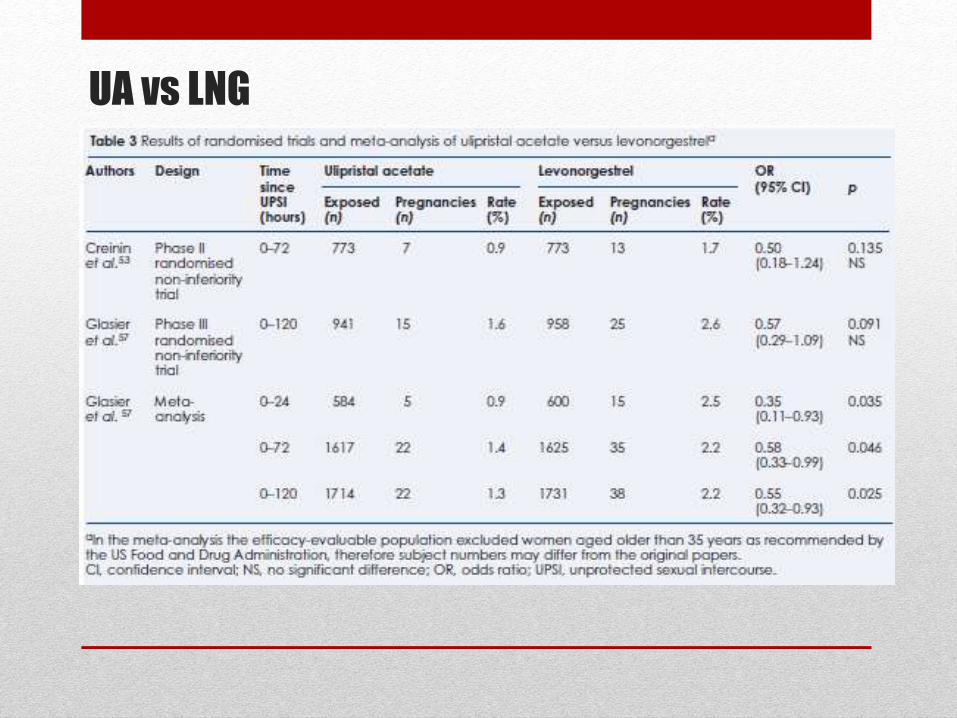
UA vs LNG

Assessment• Determine UPSI has taken within the time frame when EC is
effective.
• Determine risk of pre-existing pregnancy.
• Discuss broader issues:
STD
Sexual assault
• Determine contraindications.
• Explained side effects.

Followup
• Pregnancy test if normal menses does not resume 21 days after EC.
• Long term contraception.
Start after normal menses vs ‘Quick Start’
Quick Start
Ethico-legal issues
Outside term of product license.
Illegal to insert IUCD in a pregnant woman.
Because pregnancy cannot be excluded it is recommended when:
- The woman is likely to continue to be at risk of pregnancy.
- The woman has expressed a preference to begin contraception as soon as possible.
- POP, COCP, Implants, IUCD.
• Treatment of STI.

Checklist for Quick Start after EC
If risk of pregnancy cannot be reasonably excluded, the contraceptive provider should ensure that the woman is:
• Likely to continue to be at risk of pregnancy or that she has expressed a preference to begin contraception immediately.
• Aware that there is a possibility of pregnancy.
• Informed that there is a theoretical risk from fetal exposure to contraceptive hormones but most evidence indicates no harm.
• Aware that pregnancy cannot be excluded until she has had a pregnancy test no sooner than 3 weeks after the last episode of unprotected sexual intercourse.
• Provided with a pregnancy testing kit or informed of alternative options for pregnancy testing, including local providers of free testing.
• Given advice on additional contraceptive precautions.
• Offered a supply of condoms or informed of local providers of condoms.
• Advised to return if there are any concerns or problems with her contraception
CLEAR DETAILED DOCUMENTATION IS ESSENTIAL

Conclusion
• Get to know your patient.
• Conceptualize the various methods of contraception and
its mechanism of action.
• EC is not a substitute to appropriate contraception.
However due to the serious unmet need for contraception,
EC has played a bigger role in preventing unplanned
pregnancies.

Thank you


















