Improving Quality in Practice. Approaching Improvement in a Complex System SPICE and Service...
31
Improving Quality in Practice. Approaching Improvement in a Complex System SPICE and Service Improvement Methodology Jonathon Gray Director Healthcare Improvement Wales Centre for Health
-
Upload
annice-mckenzie -
Category
Documents
-
view
218 -
download
1
Transcript of Improving Quality in Practice. Approaching Improvement in a Complex System SPICE and Service...

Improving Quality in Practice. Approaching Improvement in a
Complex System
SPICE and Service Improvement Methodology
Jonathon GrayDirector Healthcare Improvement Wales Centre for Health
PARISIN THE
THE SPRING


PARISIN THE
THE SPRING

How many legs does this elephant have?

The First Law Of Healthcare Improvement
“Every system is perfectly designed to achieve exactly the results it gets”
Therefore, Although Not All Change Is Improvement, All Improvement Is Change
Source: Don Berwick, IHI (Boston)
Welsh Policy Context
2003 Wales: A Better Country
• Where are we going?
2005 Designed for Life
• What do we need?
2005 Healthcare Standards for Wales
• What do we do?
2006 The Healthcare Quality Improvement Plan: Designed to Deliver
• How will we get there?

Aims for Improvement
“By 2015, Wales will have minimized avoidable deaths, pain, delays, helplessness, and waste.”
Designed for Life
SafetyEffectivenessPatient ExperienceTimelinessEfficiency

“The needs of the patient come first…..”
No needless deathsNo needless pain or suffering
No unwanted waitingNo helplessness
No waste……For anyone

What do we need to measure and why?
IHI Model for Improvement

CAUTION!
Gathering data can bring new and surprising knowledge to those who dare to seek it!

How Hazardous Is Health Care?
1
10
100
1,000
10,000
100,000
1 10 100 1,000 10,000 100,000 1,000,000 10,000,000
Number of encounters for each fatality
Tota
l lives lost per
year
REGULATEDDANGEROUS(>1/1000)
ULTRA-SAFE(<1/100K)
HealthCare
Mountain Climbing
Bungee Jumping
Driving
Chemical Manufacturing
Chartered Flights
Scheduled Airlines
European Railroads
Nuclear Power

Hospital Death Rate (Standardized for Age, Sex, Race, Payer, Admission Source & Type)
vs Charge per Admission (Standardized for Age and Diagnosis) -- AHRQ 1997 Data
020406080
100120140160180
0 5,000 10,000 15,000 20,000 25,000
Standardized Charge ($ per Admission)
Stan
dard
ized
Dea
th R
ate
Organisation with a Memory
15,000 to 70,000 adverse events each year in the Wales NHS hospital sector (10 - 40% of admissions)
£100 million direct cost in additional hospital days alone
Clinical negligence cost - £85m (2004-05)
Half might be avoidable.
Source: Organisation with a memory - CMO England)

Essential Elements for Large-Scale Change
•Will•Ideas•Execution
We will explore new ways of working, recognising that there may now
be better and different methods


The Knowledge Base for Continual Improvement
Knowledge for Improvement Systems Variation Psychology PDSA
Subject andDiscipline Knowledge
Continual Improvement
+

The Project Method: The Model for Improvement (Nolan, et al.)
Act Plan
Study Do
What are we trying to accomplish?
How will we know that a change is an improvement?
What changes can we make that will result in an improvement?
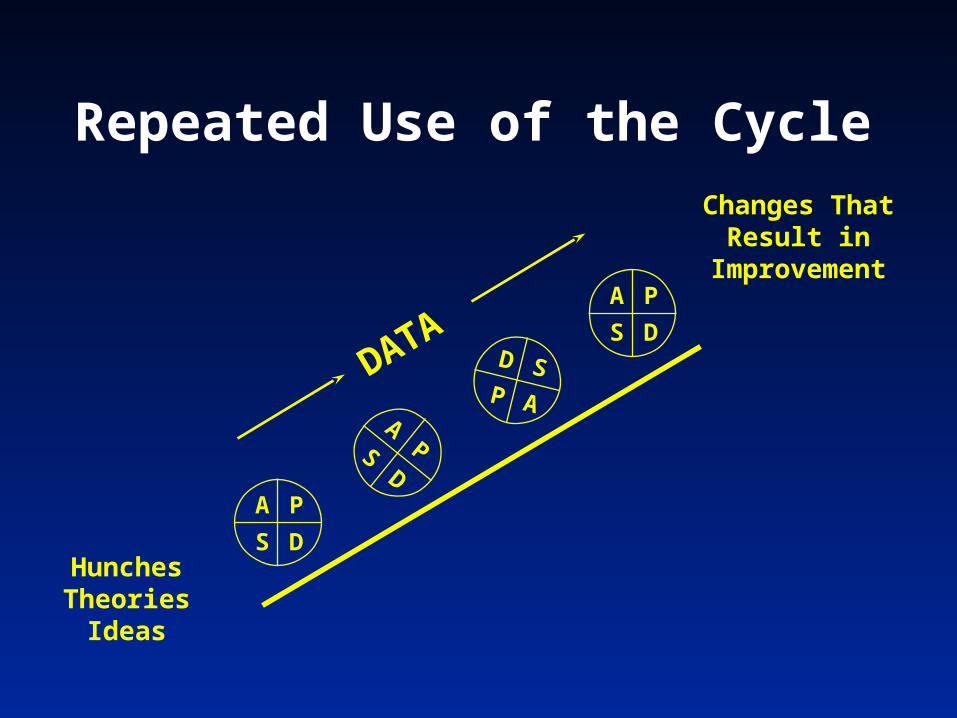
Repeated Use of the Cycle
Hunches Theories
Ideas
Changes That Result in
Improvement
A P
S D
APS
D
A P
S DD S
P ADATA

Set-up-Target population -Adopter audiences -Successful sites -Key partners-Initial spread strategy
Social System-Key messengers -Communities -Technical support-Transition issues
Communication Strategies (awareness & technical)
Knowledge Management
Measurement and Feedback
Leadership-Topic is a key strategic initiative
-Goals and incentives aligned-Executive sponsor assigned
-Day-to-day managers identified
Better Ideas-Develop the case -Describe the ideas
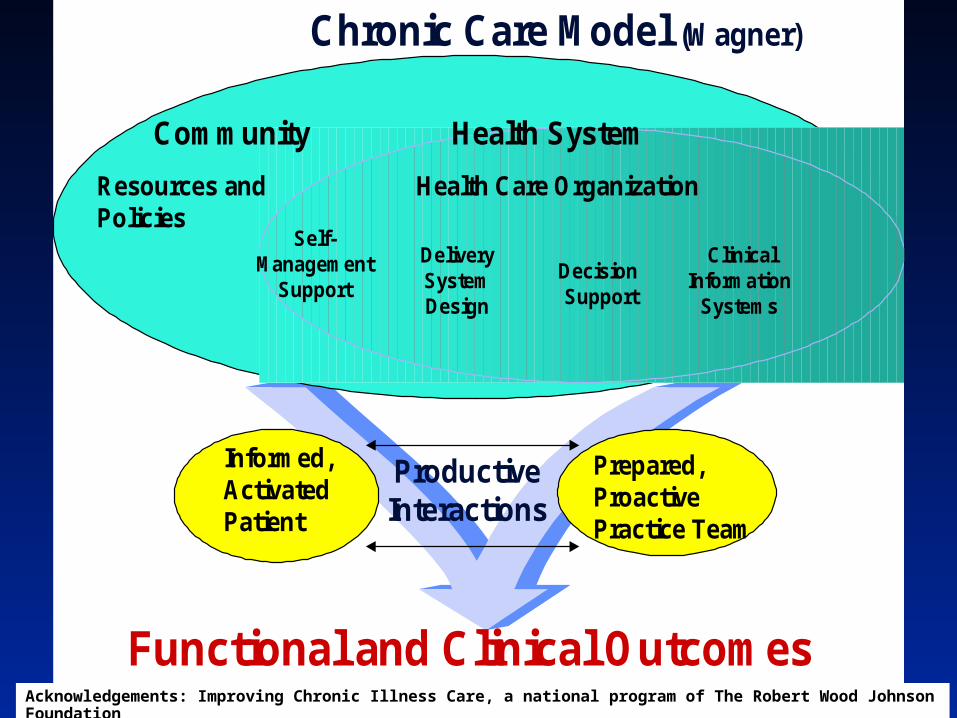
Informed,ActivatedPatient
ProductiveInteractions
Prepared,ProactivePractice Team
Functional and Clinical Outcomes
DeliverySystemDesign
DecisionSupport
ClinicalInformation
Systems
Self-Management
Support
Health System
Resources and Policies
Community
Health Care Organization
Chronic Care Model (Wagner)
Acknowledgements: Improving Chronic Illness Care, a national program of The Robert Wood Johnson Foundation
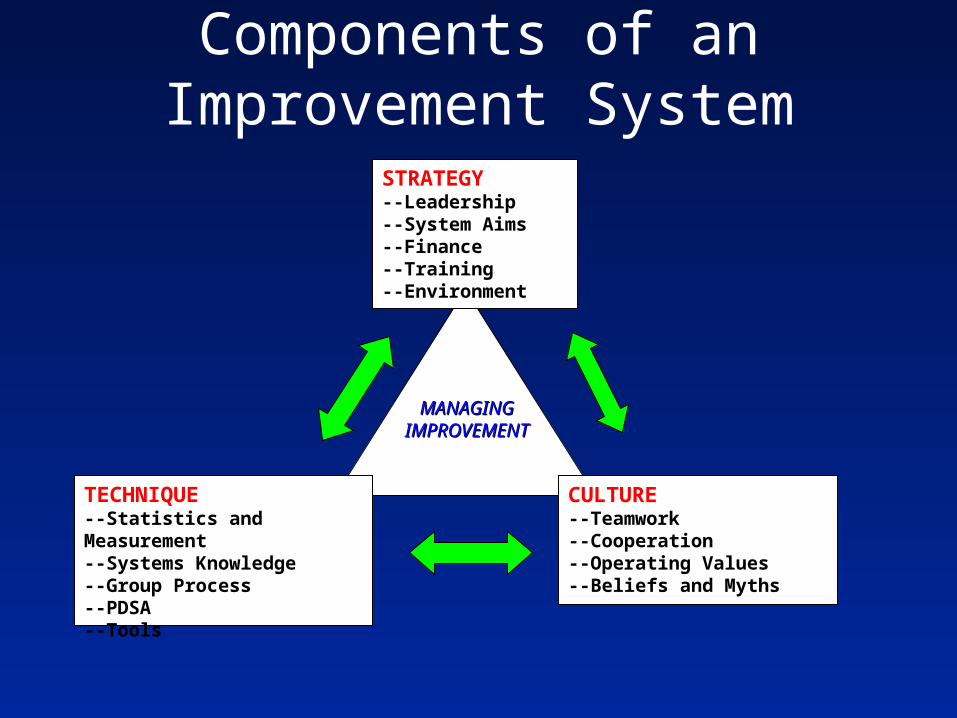
Components of an Improvement SystemSTRATEGY--Leadership--System Aims--Finance--Training--Environment
TECHNIQUE--Statistics and Measurement--Systems Knowledge--Group Process--PDSA--Tools
CULTURE--Teamwork--Cooperation--Operating Values--Beliefs and Myths
MANAGING MANAGING IMPROVEMENTIMPROVEMENT
Justin

Justin Micalizzi (by Dale Ann Micalizzi)
• “On January 15th, 2001, Justin, a healthy 11-year old boy, was taken into surgery to incise and drain a swollen ankle. He was dead by 7:55 a.m. the next morning, leaving behind two grieving and bewildered parents who desperately wanted to know why their son had died. But medical care was to fail them twice- first their son died and then no one would explain to them why.”
Justin Micalizzi (by Dale Ann Micalizzi)
• I know the chaos, the nursing shortages, overtime, the financial obligations, the insurance company guidelines and the arrogance that interferes with the quality of care. I have worked in healthcare and education for over 20 years. I also know, when it came time for my son’s surgery, you remove the chaos. You develop a team effort to review all information and establish a plan. You openly communicate between specialists, remove arrogance and intimidation and have a common goal to heal. It is your obligation to complete checklists, check and double check medications and dosages, assign a nursing team and treat every case as a possible emergency with the patient as your ONLY focus. Look at the child; listen to the parents and use common sense and professional judgment when making all decisions. Slow down! You are holding my child’s life in your hands. Justin WAS important and should have been important to his healthcare providers also. I trusted you.
Justin Micalizzi (by Dale Ann Micalizzi)
• The hospital failed us, the nurses who were his advocates failed us, and the technicians who didn’t draw pre-op labs failed us. And, most importantly, the surgeon who gave the case to the resident and was NOT even in the OR at the time of surgery failed us. The health department failed us by accepting the medical personnel’s information as truthful. The hospital CEO failed us by not providing us with any information or support. Error upon accepted error killed my son and my faith in a medical system that was meant to comfort and heal. We will not let this happen to another family. The pain is unbearable.
Justin Micalizzi (by Dale Ann Micalizzi)
“….. when it came time for my son’s surgery, you remove
the chaos……”
The Simple, Wrong Answer
Blame Somebody
The First Law of Improvement
“Every System Is Perfectly Designed to Achieve Exactly the
Results It Gets”
(Therefore, Although Not All Change Is Improvement, All Improvement Is Change)