GFR estimation - developments
95
Contemporary and Contemporary and recent advances in recent advances in renal function renal function assessment assessment Dr Manish Singla Dr Manish Singla 17-02-2012 17-02-2012
-
Upload
manish-singla -
Category
Health & Medicine
-
view
731 -
download
1
description
-Importance of GFR estimation -Formulas for GFR estimation (lately CKD-EPI equation ) -Radioisotope based methods (DTPA scan) -MRI as one stop shop
Transcript of GFR estimation - developments

Contemporary and recent Contemporary and recent advances in renal function advances in renal function
assessmentassessment
Dr Manish SinglaDr Manish Singla
17-02-201217-02-2012

Functions of the KidneyFunctions of the Kidney Homeostatic / Homeostatic /
waste removalwaste removal WaterWater Hydrogen ions (pH)Hydrogen ions (pH) SodiumSodium PotassiumPotassium CalciumCalcium PhosphatePhosphate MagnesiumMagnesium NitrogenNitrogen
EndocrineEndocrine 1,25-(OH)1,25-(OH)22 Vitamin D Vitamin D ErythropoietinErythropoietin ReninRenin
MetabolicMetabolic Glycogen storage Glycogen storage
(minor role)(minor role)
Drug removalDrug removal
The level of the glomerular filtration rate (GFR) is accepted as an overall index of excretory function.

Objectives Objectives
Renal function assessment methodsRenal function assessment methods Importance of GFR estimationImportance of GFR estimation Creatinine clearanceCreatinine clearance eGFR (formula based) eGFR (formula based) Cystatin CCystatin C Radionuclide scansRadionuclide scans CT / MRICT / MRI

26 yr male, 80 Kg, 26 yr male, 80 Kg, creatinine 1.3creatinine 1.3
eGFR ?eGFR ?
97 ml/min97 ml/min 75 yr female, 45 Kg, 75 yr female, 45 Kg, creatinine 1.3creatinine 1.3
eGFR ?eGFR ?
26 ml/min26 ml/min
How good is serum creatinine a marker How good is serum creatinine a marker for renal insufficiency?for renal insufficiency?


Wide range Wide range of GFR for a of GFR for a given serum given serum
creatininecreatinine
S.creatinine approx. = 1/GFR
GFR
Ser
um C
reat
inin
e (m
g/dL
)

What is GFR?What is GFR? GFR is a product of the average filtration rate GFR is a product of the average filtration rate
of each single nephron, multiplied by the of each single nephron, multiplied by the number of nephrons in both kidneys.number of nephrons in both kidneys.
GFR = N x SNGFRGFR = N x SNGFR Glomerular Filtration Rate is the volume of fluid Glomerular Filtration Rate is the volume of fluid
passing through the glomerulus in a given period passing through the glomerulus in a given period of time.of time.
Influenced by renal perfusion pressure, renal Influenced by renal perfusion pressure, renal vascular resistance, glomerular damage, post-vascular resistance, glomerular damage, post-glomerular resistance.glomerular resistance.

Physiologic Variability of the GFR & the Physiologic Variability of the GFR & the normal valuenormal value
““Normal Range” ~ 90 - 150 mL/minNormal Range” ~ 90 - 150 mL/min Approx 170 L per dayApprox 170 L per day
A larger healthy person has a higher GFRA larger healthy person has a higher GFR Can be reported as 90 - 150 mL/min/1.73mCan be reported as 90 - 150 mL/min/1.73m22
Varies according to Varies according to − Age - Physical activityAge - Physical activity− GenderGender - Diet - Diet − Body sizeBody size - Pharmacologic therapy - Pharmacologic therapy− PregnancyPregnancy

GFR -variablesGFR -variables
GFR ~ 8% higher in young men GFR ~ 8% higher in young men Declines with age ( mean rate of decline Declines with age ( mean rate of decline
0.75 ml/min/ year after the age of 40 yrs.)0.75 ml/min/ year after the age of 40 yrs.) Pregnancy : Pregnancy : ↑↑ ~ 50% in the 1 ~ 50% in the 1stst trimester. trimester. Diurnal variation – 10% ↓ at midnight than Diurnal variation – 10% ↓ at midnight than
afternoon.afternoon.

Need for estimating the GFRNeed for estimating the GFR
Monitoring progression of CKDMonitoring progression of CKD GFR estimates are used for drug dosing GFR estimates are used for drug dosing
decisionsdecisions Dosing of renally excreted drugsDosing of renally excreted drugs Avoiding nephrotoxic drugsAvoiding nephrotoxic drugs
Risk factor for cardiovascular disease Risk factor for cardiovascular disease mortalitymortality
Renal involvement in systemic diseases, Renal involvement in systemic diseases, such as diabetes mellitus or SLEsuch as diabetes mellitus or SLE

Measurement Of Glomerular Measurement Of Glomerular Filtration RateFiltration Rate
The glomerular filtration rate cannot be The glomerular filtration rate cannot be measured directly; it is estimated from the measured directly; it is estimated from the urinary urinary clearanceclearance of an ideal filtration of an ideal filtration marker. marker.

Concept of clearanceConcept of clearance
Clearance of a substance is defined as Clearance of a substance is defined as
the volume of plasma cleared of a marker the volume of plasma cleared of a marker
by excretion per unit of time.by excretion per unit of time.
Clearance does not represent an actual Clearance does not represent an actual
volume, but rather a virtual volume of volume, but rather a virtual volume of
plasma that is completely cleared of the plasma that is completely cleared of the
substance per unit of time.substance per unit of time.

Urinary ClearanceUrinary Clearance
C(x) = (Ux X V) / Px.C(x) = (Ux X V) / Px. Ux – Urinary concentration,Ux – Urinary concentration, V – Urinary flow rate,V – Urinary flow rate, The magnitude of urinary clearance The magnitude of urinary clearance
reflects the mechanism of excretion.reflects the mechanism of excretion. For substances that are filtered but are For substances that are filtered but are
neither secreted nor reabsorbed, the neither secreted nor reabsorbed, the urinary excretion equals the filter load, and urinary excretion equals the filter load, and urinary clearance equals GFR.urinary clearance equals GFR.

Ideal MarkerIdeal Marker Constant productionConstant production SafeSafe ConvenientConvenient Readily diffusible in extracellular spaceReadily diffusible in extracellular space No protein binding and freely filterableNo protein binding and freely filterable No tubular reabsorptionNo tubular reabsorption No tubular secretionNo tubular secretion No extrarenal elimination or degradationNo extrarenal elimination or degradation Accurate and reproducible assayAccurate and reproducible assay No compounds interfere No compounds interfere InexpensiveInexpensive No influence on the GFRNo influence on the GFR

Filtration markersFiltration markers
EndogenousEndogenous UreaUrea CreatinineCreatinine Cystatin CCystatin C
ExogenousExogenous InulinInulin 125125I IothalamateI Iothalamate 99m99mTc DTPATc DTPA 5151Cr EDTACr EDTA Iohexol Iohexol IodixanolIodixanol

Inulin Inulin
5200-d uncharged polymer of fructose5200-d uncharged polymer of fructose It is freely filtered at glomerulus and It is freely filtered at glomerulus and
neither secreted nor reabsorbed by the neither secreted nor reabsorbed by the renal tubule.renal tubule.
The ideal protocol for inulin clearance The ideal protocol for inulin clearance requires a continuous intravenous requires a continuous intravenous infusioninfusion to achieve a steady state and to achieve a steady state and bladder catheterization with multiple timed bladder catheterization with multiple timed urine collections. urine collections.
Not used widely in clinical practice. Not used widely in clinical practice.
Urea Urea
The serum urea level has limited value as The serum urea level has limited value as an index of GFR, in view of widely variable an index of GFR, in view of widely variable urea generation and tubular reabsorption.urea generation and tubular reabsorption.
It is a 60-d end product of protein It is a 60-d end product of protein catabolism by the liver.catabolism by the liver.
It is freely filtered by the glomerulus and It is freely filtered by the glomerulus and then passively reabsorbed in both the then passively reabsorbed in both the proximal and distal nephrons.proximal and distal nephrons.

Owing to the tubular reabsorption, urinary Owing to the tubular reabsorption, urinary clearance of urea underestimates kidney clearance of urea underestimates kidney function.function.
At levels of GFR < 20 ml/min/1.73 m2, the At levels of GFR < 20 ml/min/1.73 m2, the overestimationoverestimation of GFR by creatinine of GFR by creatinine clearance due to creatinine secretion clearance due to creatinine secretion equalsequals to the to the underestimationunderestimation of GFR by of GFR by urea clearance due to urea reabsorption.urea clearance due to urea reabsorption.

Factors Affecting Serum Urea Nitrogen
American Journal of Kidney Diseases, Vol 47, No 1 (January), 2006: pp 174-183
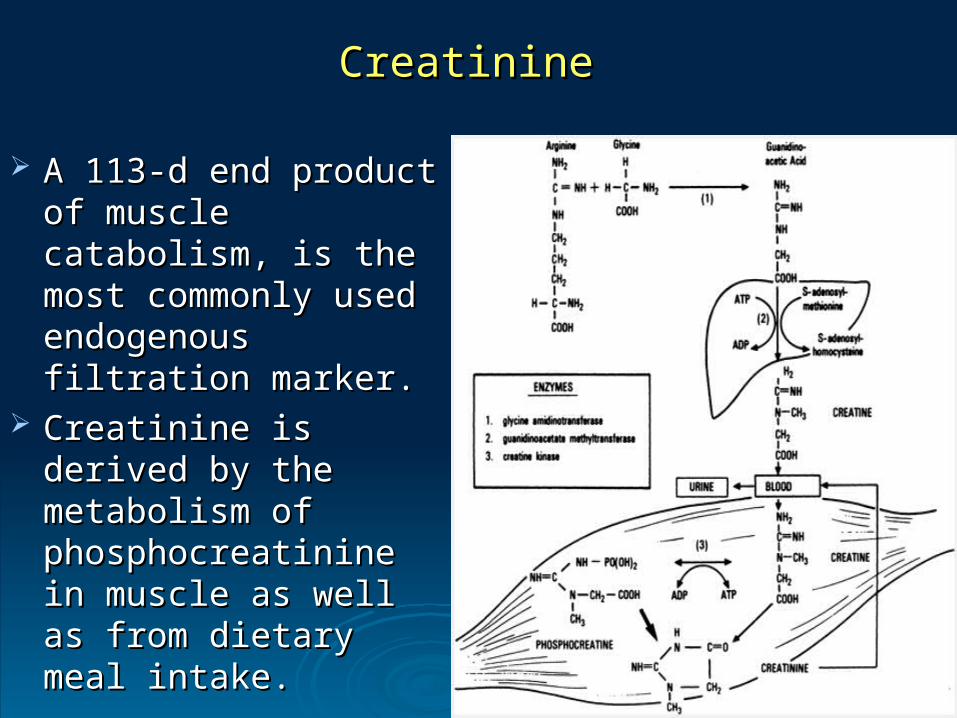
Creatinine Creatinine
A 113-d end product of A 113-d end product of muscle catabolism, is muscle catabolism, is the most commonly the most commonly used endogenous used endogenous filtration marker.filtration marker.
Creatinine is derived by Creatinine is derived by the metabolism of the metabolism of phosphocreatinine in phosphocreatinine in muscle as well as from muscle as well as from dietary meal intake.dietary meal intake.

CreatinineCreatinine
Not protein bound and freely filtered across the Not protein bound and freely filtered across the glomeruli.glomeruli.
Also secreted by the tubules, so creatinine Also secreted by the tubules, so creatinine clearance exceeds GFRclearance exceeds GFR
Several commonly used medications Several commonly used medications (cimetidine, trimethoprim) competitively inhibit (cimetidine, trimethoprim) competitively inhibit Creatinine secretion and reduce Creatinine Creatinine secretion and reduce Creatinine clearance.clearance.
Lead to rise in the serum Creatinine Lead to rise in the serum Creatinine concentration without effect on GFR.concentration without effect on GFR.

Creatinine assayCreatinine assay The most commonly used assay for measuring The most commonly used assay for measuring
serum Creatinine , the alkaline serum Creatinine , the alkaline picrate (Jaffe) picrate (Jaffe) assayassay, detects and quantifies the color reaction., detects and quantifies the color reaction.
Creatinine reacts directly with picrate ion under Creatinine reacts directly with picrate ion under alkaline conditions to form a red-orange complex alkaline conditions to form a red-orange complex that is easily detected and quantified that is easily detected and quantified
In normal subjects, upto 20% of the color In normal subjects, upto 20% of the color reaction is due to noncreatinine chromogensreaction is due to noncreatinine chromogens
Enzymatic assays Enzymatic assays do not detect non-creatinine do not detect non-creatinine chromogens and yield lower serum levels than chromogens and yield lower serum levels than the alkaline picrate assays. the alkaline picrate assays.

Factors Affecting SCr
American Journal of Kidney Diseases, Vol 47, No 1 (January), 2006: pp 174-183

Objectives Objectives
Renal function assessment methodsRenal function assessment methods Importance of GFR estimationImportance of GFR estimation Creatinine clearanceCreatinine clearance eGFR (formula based) eGFR (formula based) Cystatin CCystatin C Radionuclide scansRadionuclide scans CT / MRICT / MRI

Creatinine clearanceCreatinine clearance
Creatinine clearance is computed from the Creatinine clearance is computed from the creatinine excretion in a 24 hr urine creatinine excretion in a 24 hr urine collection and single measurement of collection and single measurement of serum Creatinine in the steady state.serum Creatinine in the steady state.

Drawbacks of Creatinine Drawbacks of Creatinine clearance clearance
Creatinine clearance overestimates GFR Creatinine clearance overestimates GFR due to tubular secretion. (magnified at due to tubular secretion. (magnified at lower levels of kidney function.)lower levels of kidney function.)
Challenges of achieving a complete urine Challenges of achieving a complete urine collection limit the accuracycollection limit the accuracy
Cumbersome and inconvenient for patientCumbersome and inconvenient for patient
Objectives Objectives
Renal function assessment methodsRenal function assessment methods Importance of GFR estimationImportance of GFR estimation Creatinine clearanceCreatinine clearance eGFR (formula based) eGFR (formula based) Cystatin CCystatin C Radionuclide scansRadionuclide scans CT / MRICT / MRI

Formula based estimation of Formula based estimation of GFRGFR
Based on plasma concentration Based on plasma concentration
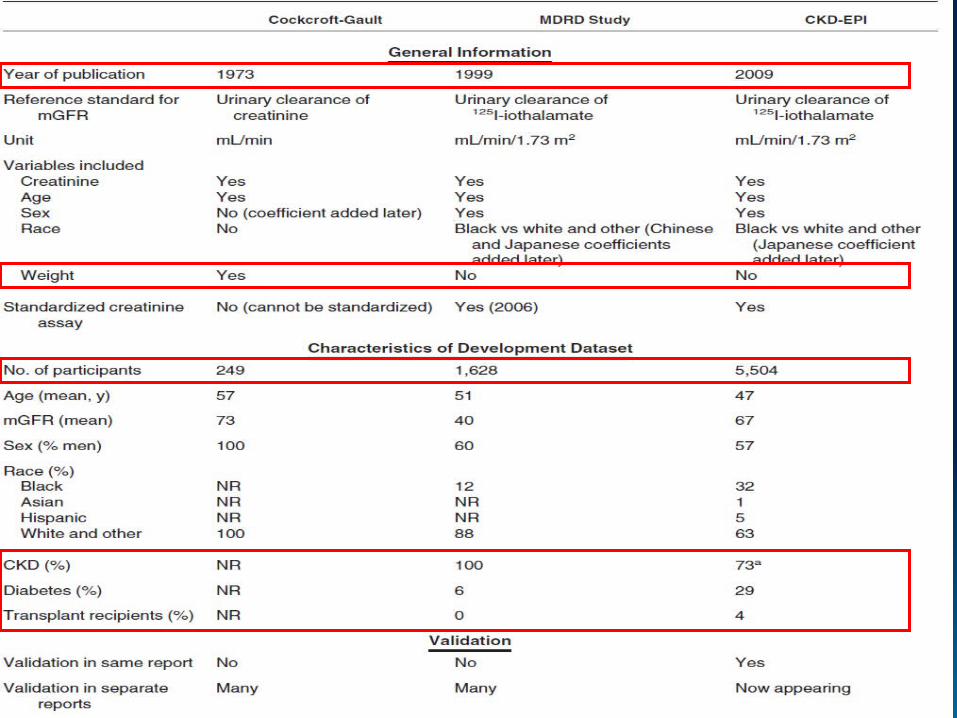
No need of urine sampleNo need of urine sample C G formulaC G formula MDRD equationMDRD equation CKD-EPICKD-EPI

Cockcroft-Gault FormulaCockcroft-Gault Formula
Ccr = Ccr = (140 – Age) X Weight(140 – Age) X Weight
72 X Pcr(mg/dl)72 X Pcr(mg/dl) Female : Ccr X 0.85Female : Ccr X 0.85

DrawbacksDrawbacks Does not take into account differences in Does not take into account differences in
creatinine production b/n individuals of the same creatinine production b/n individuals of the same age and sex or even in the same individual over age and sex or even in the same individual over time. time.
Overestimates GFR in individuals who are Overestimates GFR in individuals who are obese or edematous.obese or edematous.
Does not take into account extrarenal Does not take into account extrarenal elimination, tubular handling, or inaccuracies in elimination, tubular handling, or inaccuracies in the laboratory measurement of creatinine that the laboratory measurement of creatinine that can contribute to error in the serum creatinine can contribute to error in the serum creatinine estimate of GFR estimate of GFR

Modification of Diet in Renal Modification of Diet in Renal Disease Study EquationDisease Study Equation
OriginallyOriginally expressed as expressed as 6-variable6-variable equationequation using serum creatinine, urea, and albumin using serum creatinine, urea, and albumin concentrations in addition to demographic concentrations in addition to demographic variables to predict GFR.variables to predict GFR.
A revised 4 - variable equation has minimal bias A revised 4 - variable equation has minimal bias and precision and accuracy close to those of the and precision and accuracy close to those of the 6-variable equation.6-variable equation.
This equation has now been validated in African This equation has now been validated in African Americans, people with diabetic kidney disease, Americans, people with diabetic kidney disease, and kidney transplant recipients, three groups and kidney transplant recipients, three groups not included in large numbers in the original not included in large numbers in the original MDRD study.MDRD study.

Pros & ConsPros & Cons The equation appears to underestimate GFR in The equation appears to underestimate GFR in
populations with higher levels of GFRpopulations with higher levels of GFR It has not been validated in children, pregnant It has not been validated in children, pregnant
women, the elderly (age > 70 yrs), or other women, the elderly (age > 70 yrs), or other racial or ethnic subgroups.racial or ethnic subgroups.
MDRD study equation had greater precision and MDRD study equation had greater precision and greater overall accuracy than that of measured greater overall accuracy than that of measured creatinine clearance and of the Cockcroft-Gault creatinine clearance and of the Cockcroft-Gault FormulaFormula

The National Kidney Foundation's K/DOQI The National Kidney Foundation's K/DOQI guidelines consider the MDRD equation a guidelines consider the MDRD equation a reliable measure for GFR in adultsreliable measure for GFR in adults
The European Best Practice Guidelines The European Best Practice Guidelines Expert Group on Hemodialysis prefers it Expert Group on Hemodialysis prefers it over the Cockcroft-Gault equation for over the Cockcroft-Gault equation for individuals with advanced kidney failure individuals with advanced kidney failure

Neither equation is expected to work as Neither equation is expected to work as well in patients withwell in patients with
- extreme levels for creatinine - extreme levels for creatinine generation, such as generation, such as
• Amputees, Amputees, • Large or small individuals, Large or small individuals, • Patients with muscle wasting conditions, Patients with muscle wasting conditions, • People with high or low levels of dietary People with high or low levels of dietary
meat intake. meat intake.

Assumption of a steady state since the Assumption of a steady state since the serum creatinine level lags behind the serum creatinine level lags behind the change in GFR.change in GFR.
Thus, in a patient with rapidly declining Thus, in a patient with rapidly declining GFR (rising serum creatinine), GFR GFR (rising serum creatinine), GFR estimate will exceed the true GFR, and estimate will exceed the true GFR, and conversely, in a patient with rising GFR conversely, in a patient with rising GFR (declining serum creatinine), GFR (declining serum creatinine), GFR estimate will be lower than the true GFR.estimate will be lower than the true GFR.

CKD-EPI EquationCKD-EPI Equation
Based on the same four variables as the Based on the same four variables as the MDRD Study equation MDRD Study equation
A 2-slope “spline” to model the relationship A 2-slope “spline” to model the relationship between estimated GFR and serum between estimated GFR and serum creatinine, and a different relationship for creatinine, and a different relationship for age, sex and race. age, sex and race.

The CKD-EPI Equation for Estimating GFR

Pros Pros
Reported to perform better Reported to perform better Less bias than the MDRD Study equation, Less bias than the MDRD Study equation,
especially in patients with higher GFR. especially in patients with higher GFR. Reduced misclassification of CKD. Reduced misclassification of CKD.


Clinical situations in which estimating equations Clinical situations in which estimating equations for creatinine clearance or GFR measurements for creatinine clearance or GFR measurements may not be accurate and clearance may not be accurate and clearance measurements may be recommendedmeasurements may be recommended Extremes of age and body size Extremes of age and body size Severe malnutrition or obesity Severe malnutrition or obesity Diseases of skeletal muscle Diseases of skeletal muscle Paraplegia or quadriplegia Paraplegia or quadriplegia Vegetarian diet Vegetarian diet Rapidly changing kidney function Rapidly changing kidney function Pregnancy Pregnancy Prior to dosing drugs with significant toxicity that are Prior to dosing drugs with significant toxicity that are excreted by the kidneysexcreted by the kidneys

Objectives Objectives
Renal function assessment methodsRenal function assessment methods Importance of GFR estimationImportance of GFR estimation Creatinine clearanceCreatinine clearance eGFR (formula based) eGFR (formula based) Cystatin CCystatin C Radionuclide scansRadionuclide scans CT / MRICT / MRI
Cystatin CCystatin C A 13 kd protein that is unique in that it appears A 13 kd protein that is unique in that it appears
to be produced at a constant rate by all to be produced at a constant rate by all nucleated human cells.nucleated human cells.
Its low molecular mass and high isoelectric point Its low molecular mass and high isoelectric point allow it to be freely filtered by the glomerular allow it to be freely filtered by the glomerular membrane.membrane.
After filtration Cystatin C is reabsorbed and After filtration Cystatin C is reabsorbed and catabolized by tubular epithelial cells, with only catabolized by tubular epithelial cells, with only small amounts, excreted in the urine.small amounts, excreted in the urine.

Cystatin CCystatin C Thus, Cystatin C generation cannot be Thus, Cystatin C generation cannot be
quantitated by urinary excretion, nor can its quantitated by urinary excretion, nor can its urinary clearance be measured.urinary clearance be measured.
Cystatin C levels in surveys of normal adults Cystatin C levels in surveys of normal adults range from range from 0.54 to 1.550.54 to 1.55 mg/l with slight mg/l with slight variability depending on the assay used.variability depending on the assay used.

Cystatin CCystatin C Serum concentration of serum Cystatin C Serum concentration of serum Cystatin C
remains constant from ~ 1 to 50 yrs of ageremains constant from ~ 1 to 50 yrs of age Largely independent of height, gender, and Largely independent of height, gender, and
muscle mass.muscle mass. There is some suggestion that liver disease, There is some suggestion that liver disease,
thyroid disease, and large doses of thyroid disease, and large doses of corticosteroids may increase production of corticosteroids may increase production of Cystatin C.Cystatin C.

Cystatin CCystatin C
With acute decline in GFR, one study With acute decline in GFR, one study demonstrated that the Cystatin C level increase demonstrated that the Cystatin C level increase before that of serum creatinine.before that of serum creatinine.
In comparative studies, serum cystatin C In comparative studies, serum cystatin C appears to be better filtration marker.appears to be better filtration marker.
Some studies show that elevations in Cystatin C Some studies show that elevations in Cystatin C level are a better predictor of the risk of level are a better predictor of the risk of cardiovascular disease and total mortality than cardiovascular disease and total mortality than an estimated GFR based on serum creatinine.an estimated GFR based on serum creatinine.

Cystatin C MeasurementCystatin C Measurement
Particle-enhanced turbidimetric Particle-enhanced turbidimetric immunoassay immunoassay (PETIA)(PETIA)
Particle-enhanced nephelometric Particle-enhanced nephelometric immunoassay immunoassay (PENIA)(PENIA) are the two are the two available versions of latex immunoassay. available versions of latex immunoassay.
On the basis of a On the basis of a 20022002 meta-analysis, meta-analysis, immunonephelometric (PENIA) immunonephelometric (PENIA) methods methods was declared to be was declared to be superior superior to other to other assaysassays
142 samples were run on the new PETIA and previous PENIA142 samples were run on the new PETIA and previous PENIA An unexpected observation was a consistent 23% bias across the An unexpected observation was a consistent 23% bias across the
measured range with the PETIA showing higher resultsmeasured range with the PETIA showing higher results Checked against international certified reference materialChecked against international certified reference material PETIA, but not the PENIA, yielded expected results for this PETIA, but not the PENIA, yielded expected results for this
international reference material.international reference material.
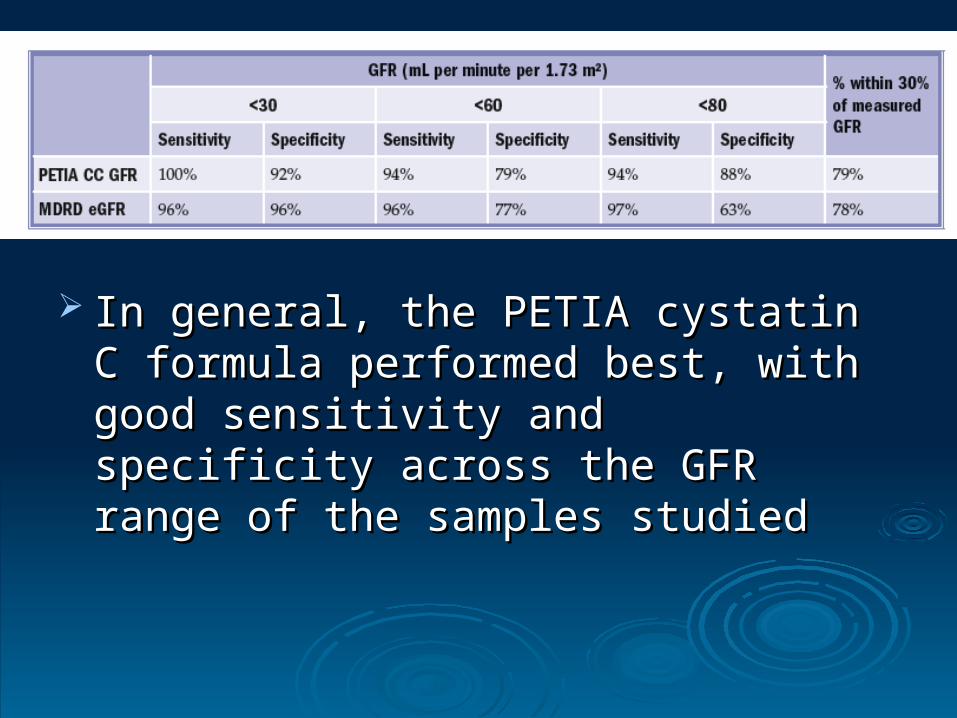
In general, the PETIA cystatin C formula In general, the PETIA cystatin C formula performed best, with good sensitivity and performed best, with good sensitivity and specificity across the GFR range of the specificity across the GFR range of the samples studiedsamples studied

GFR in ChildrenGFR in Children

GFR in children-Original Schwartz EquationGFR in children-Original Schwartz Equation
GFR GFR (mL/min/1.73 m(mL/min/1.73 m22)) = k (Height) / Serum creatinine = k (Height) / Serum creatinine k = Constant k = Constant
k = 0.33 in preemie infants k = 0.33 in preemie infants k = 0.45 in term infants to 1 year of age k = 0.45 in term infants to 1 year of age k = 0.55 in children to 13 years of age k = 0.55 in children to 13 years of age k = 0.70 in adolescent males (not females because of k = 0.70 in adolescent males (not females because of
the presumed increase in male muscle mass, the the presumed increase in male muscle mass, the constant remains .55 for females) constant remains .55 for females)
Height in cm Height in cm Serum creatinine in mg/dL Serum creatinine in mg/dL


Objectives Objectives
Renal function assessment methodsRenal function assessment methods Importance of GFR estimationImportance of GFR estimation Creatinine clearanceCreatinine clearance eGFR (formula based) eGFR (formula based) Cystatin CCystatin C Radionuclide scansRadionuclide scans CT / MRICT / MRI
Radionuclide scansRadionuclide scans The first attempt to asses the renal function with The first attempt to asses the renal function with
radionuclide applications was made in 1952 by radionuclide applications was made in 1952 by Oeser and Billion, who measured urine Oeser and Billion, who measured urine radioactivity after intravenous injection of 131 radioactivity after intravenous injection of 131 IiodoxylIiodoxyl
Orthoiodohippurate was labeled with 131I and Orthoiodohippurate was labeled with 131I and recommended for clinical estimation of the renal recommended for clinical estimation of the renal function in 1960function in 1960
Later, development many radioisotopes Later, development many radioisotopes transformed the field of renal nuclear medicinetransformed the field of renal nuclear medicine

Indications Indications
1)1) Renal function and perfusion(GFR or ERPF)Renal function and perfusion(GFR or ERPF)
2)2) Relative renal function by measurement split GFRRelative renal function by measurement split GFR
3)3) Obstruction (Lasix renal scan)Obstruction (Lasix renal scan)
4)4) Renovascular HTN (Captopril renal scan)Renovascular HTN (Captopril renal scan)
5)5) Infection (renal morphology scan)Infection (renal morphology scan)
6)6) Pre-surgical quantitation (nephrectomy) Pre-surgical quantitation (nephrectomy)
7)7) Renal transplantRenal transplant
8)8) Congenital anomalies, masses Congenital anomalies, masses (renal morphology scan)(renal morphology scan)

PrinciplesPrinciples
Blood flowBlood flow - 20% cardiac output to kidneys - 20% cardiac output to kidneys (1200 ml/min blood, 600 ml/min plasma)(1200 ml/min blood, 600 ml/min plasma)
FiltrationFiltration - 20% renal plasma flow filtered by - 20% renal plasma flow filtered by glomeruli glomeruli (120 ml/min, 170 L/d)(120 ml/min, 170 L/d)
Tubular secretionTubular secretion Tubular reabsorptionTubular reabsorption (1% ultrafiltrate – urine) (1% ultrafiltrate – urine)

PrinciplesPrinciples
Clearance is determined as amount of indicator Clearance is determined as amount of indicator injected divided by the integrated area of plasma injected divided by the integrated area of plasma concentration curve over time. concentration curve over time.
Assumed that volume of distribution and renal Assumed that volume of distribution and renal excretion are constant over time and there is no excretion are constant over time and there is no extra renal excretion extra renal excretion
Multiple blood samples taken Multiple blood samples taken

Newer Techniques not requiring Newer Techniques not requiring plasma samplingplasma sampling
Gamma Camera Positioned over kidney used to Gamma Camera Positioned over kidney used to measure Renal elimination of Radio active measure Renal elimination of Radio active indicator Tc DTPA.indicator Tc DTPA.

Radionuclide MarkersRadionuclide Markers
Plasma based 125125I-iothalamate I-iothalamate 5151Cr-EDTA Cr-EDTA
Gamma counter basedGamma counter based I-131 OIH Tc-99m DTPA Tc-99m DTPA Tc-99m MAG3 Tc-99m GHA Tc-99m DMSA

Renal RadiotracersRenal RadiotracersExcretion MechanismsExcretion Mechanisms
GF TS TFTc-99m DTPA >95%Tc-99m MAG3 <5% 95%I-131 OIH 20% 80%Tc-99m GHA 40%-60% 20%Tc-99m DMSA some 60%
Semin NM Apr.92

Renal RadiopharmaceuticalsRenal Radiopharmaceuticals
Extract. fraction Clearance
Tc-99m DTPA 20% 100-120 ml/min Tc-99m MAG3 40-50% ~ 300 ml/min I-131 OIH ~100% 500-600 ml/minDMSA 10%

Choosing Renal Choosing Renal RadiotracersRadiotracers
GFR quantitationGFR quantitation I-125 iothalamate, I-125 iothalamate,
Cr-51 EDTA, DTPACr-51 EDTA, DTPA
ERPF quantitationERPF quantitation MAG3, OIH, EdCMAG3, OIH, EdC
MorphologyMorphology DMSA, GHADMSA, GHA
Relative functionRelative function AllAll

Basic Renal ScintigraphyBasic Renal Scintigraphy
PatientPatient PreparationPreparation
Patient must be well hydratedPatient must be well hydrated Give 5-10 ml/kg water (2-4 cups) Give 5-10 ml/kg water (2-4 cups)
30-60 min. pre-injection30-60 min. pre-injection Can measure urine specific gravity Can measure urine specific gravity
(<1.015)(<1.015) Void before injectionVoid before injection Void @ end of studyVoid @ end of study
Int’l Consens. Comm.Int’l Consens. Comm.Semin NM ‘99:146-159Semin NM ‘99:146-159

Photograph of a dual headed Photograph of a dual headed SPECT-CT gamma cameraSPECT-CT gamma camera

Basic Renal Scintigraphy Basic Renal Scintigraphy
AcquisitionAcquisition
Supine position preferredSupine position preferred Flow (angiogram) : 2-3 sec / fr x 1 minFlow (angiogram) : 2-3 sec / fr x 1 min Dynamic: 15-30 sec / frame x 20-30 minDynamic: 15-30 sec / frame x 20-30 min Obtain post-void supine image of Obtain post-void supine image of
kidneys at end of studykidneys at end of study

Gates method used which employs Gates method used which employs images of renal uptake in the second and images of renal uptake in the second and third minutes after tracer administration. third minutes after tracer administration.
Regions of interest (ROIs) are drawn over Regions of interest (ROIs) are drawn over the kidneys and background activity the kidneys and background activity correction is applied.correction is applied.
Software calculates GFR based on ROI, Software calculates GFR based on ROI, transit time etc.transit time etc.

Relative uptakeRelative uptake
Contribution of each kidney to the total fctContribution of each kidney to the total fct
net cts in Lt ROInet cts in Lt ROI
% Lt kid% Lt kid = --------------------------------------- x 100% = --------------------------------------- x 100% net cts Lt + net cts Rt ROInet cts Lt + net cts Rt ROI
NormalNormal 50/50 - 56/4450/50 - 56/44 BorderlineBorderline 57/43 - 59/4157/43 - 59/41 AbnormalAbnormal > 60/40> 60/40
Taylor, SeminNM Apr 99

Renogram PhasesRenogram Phases
I.I. Vascular phase Vascular phase (flow study):(flow study):Ao-to-Kid ~ 3”Ao-to-Kid ~ 3”
II.II. Parenchymal phase Parenchymal phase (kidney-to-bkg): (kidney-to-bkg): TTpeakpeak < 5’ < 5’
III.III. Washout (excretory) phaseWashout (excretory) phase

Renogram curvesRenogram curves

Basic Renal ScintigraphyBasic Renal Scintigraphy ProcessingProcessing
Time to peakTime to peak Best from cortical ROIBest from cortical ROI Normal < 5 minNormal < 5 min
Residual Cortical Activity (RCAResidual Cortical Activity (RCA20 or 3020 or 30)) RatioRatio of cts @ 20 or 30 min / peak cts of cts @ 20 or 30 min / peak cts
Normal RCANormal RCA2020 for MAG3 < 0.3 for MAG3 < 0.3

TT1/2:1/2: Time required for 50% tracer to leave the dilated unit Time required for 50% tracer to leave the dilated unit
i.e. time required for activity to fall to 50% of peaki.e. time required for activity to fall to 50% of peak
Normal Normal < 10 min< 10 min Obstructed Obstructed > 20 min> 20 min Indeterminate Indeterminate 10 - 20 min10 - 20 min
Interpret whole study (Visual dynamic images, Washout curve shape Interpret whole study (Visual dynamic images, Washout curve shape
and Tand T1/21/2) and not T) and not T1/2 1/2 alone alone
Basic Renal ScintigraphyBasic Renal Scintigraphy ProcessingProcessing


DTPA normalDTPA normal
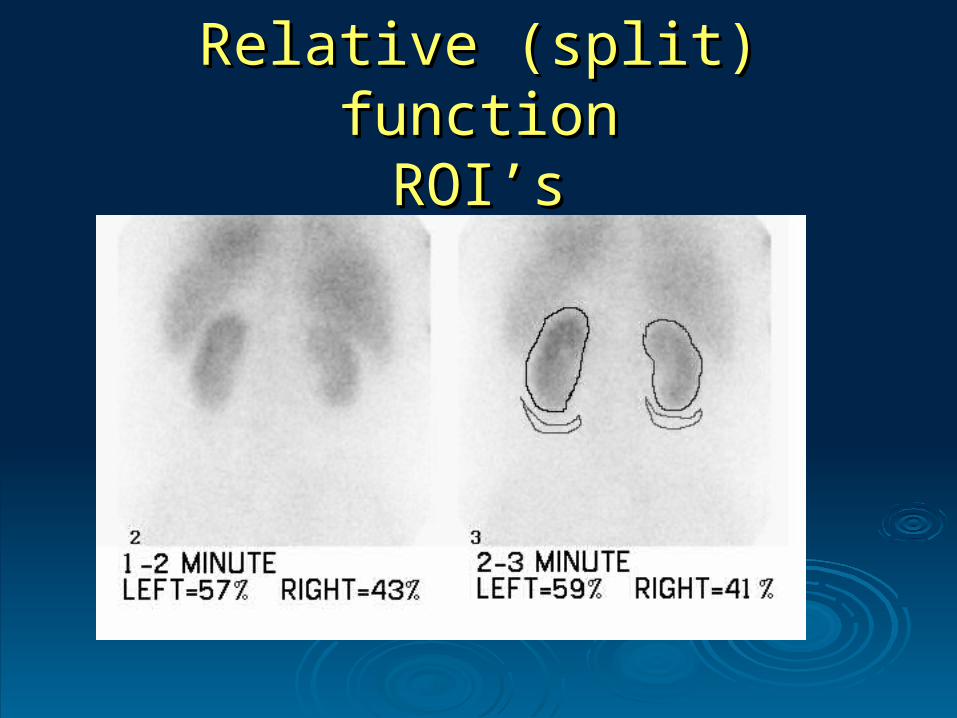
Relative (split) functionRelative (split) functionROI’sROI’s

99mTc-DTPA 99mTc-DTPA
dynamic dynamic scintigraphy of a scintigraphy of a patients with patients with chronic chronic pyelonephritis of pyelonephritis of the left kidney.the left kidney.

99m Tc-DTPA 99m Tc-DTPA dynamic dynamic scintigraphy of a scintigraphy of a patient with patient with hydronephrosis hydronephrosis of the left of the left kidney.kidney.
Pitfalls on RadionuclidePitfalls on Radionuclide
Unlike contrast media, which are presented as Unlike contrast media, which are presented as an ampule of sterile fluid, radiopharmaceuticals an ampule of sterile fluid, radiopharmaceuticals need to be prepared on the day of use, with full need to be prepared on the day of use, with full aseptic precautions and dispencing.aseptic precautions and dispencing.
Protein binding of Tc-DTPA significant source of Protein binding of Tc-DTPA significant source of errorerror
Radio isotopes in children and pregnant women Radio isotopes in children and pregnant women carry increased risk of exposure to radiation, it is carry increased risk of exposure to radiation, it is contraindicated.contraindicated.
Expense, time and labour needed to carry out Expense, time and labour needed to carry out the assay.the assay.

Objectives Objectives
Renal function assessment methodsRenal function assessment methods Importance of GFR estimationImportance of GFR estimation Creatinine clearanceCreatinine clearance eGFR (formula based) eGFR (formula based) Cystatin CCystatin C Radionuclide scansRadionuclide scans CT / MRICT / MRI

CT/MRICT/MRI
Applying similar principals and Applying similar principals and compartment model, radiocontrast and compartment model, radiocontrast and paramagnetic molecules, can be used for paramagnetic molecules, can be used for functional renal evaluation in CT and MRI functional renal evaluation in CT and MRI respectivelyrespectively

Radiocontrast markers Radiocontrast markers Iothalamate sodium (conray)Iothalamate sodium (conray) Diatrizoate meglumine (hypaque)Diatrizoate meglumine (hypaque) Iohexol (Omnipaque)Iohexol (Omnipaque) Iodixanol (Visipaque)Iodixanol (Visipaque)Paramagnetic moleculesParamagnetic molecules GadoliniumGadolinium Gd - DTPAGd - DTPA
Radionuclide and Radio contrastRadionuclide and Radio contrast

MRI for the evaluation of renal MRI for the evaluation of renal functionfunction
In recent years, progress has been made in the use of In recent years, progress has been made in the use of MRI for the evaluation of renal functionMRI for the evaluation of renal function
Renal scintigraphy provides information about the Renal scintigraphy provides information about the function of each kidney, but this test lacks anatomic function of each kidney, but this test lacks anatomic detail. detail.
CT has the disadvantage of ionizing radiation and the CT has the disadvantage of ionizing radiation and the use of potentially nephrotoxic contrast, which may use of potentially nephrotoxic contrast, which may cause deterioration of renal function in diseased cause deterioration of renal function in diseased kidneys.kidneys.
MRI has the potential to combine the functional and MRI has the potential to combine the functional and anatomic information about each kidney individuallyanatomic information about each kidney individually


Ninety patients underwent simultaneous Ninety patients underwent simultaneous determinations of GFR using 1 mCi of Tc-DTPA and determinations of GFR using 1 mCi of Tc-DTPA and 0.05 mmol/kg Gd-DTPA 0.05 mmol/kg Gd-DTPA
The Gd-DTPA derived GFR closely approximated The Gd-DTPA derived GFR closely approximated the the 99m99mTc-DTPA derived GFR which ranged from 15 Tc-DTPA derived GFR which ranged from 15 to 147 ml/min. to 147 ml/min.
Gd-DTPA is a safe, non-radioactive indicator of GFR Gd-DTPA is a safe, non-radioactive indicator of GFR that may provide an alternative renal clearance that may provide an alternative renal clearance method for clinical studies of progressive renal method for clinical studies of progressive renal disease and nephrotoxicity.disease and nephrotoxicity.

For the measurement of the GFR by MRI, several For the measurement of the GFR by MRI, several techniques have been investigated:- techniques have been investigated:-
The The first technique first technique used MR spectroscopy to used MR spectroscopy to measure the T1 relaxation times of urine and measure the T1 relaxation times of urine and serum samples taken at serial intervals serum samples taken at serial intervals
GFR calculation was based on the linear GFR calculation was based on the linear relationship of 1/T1 to the serial dilution relationship of 1/T1 to the serial dilution measurements of these samplesmeasurements of these samples
Disadvantage of measuring the GFR of both Disadvantage of measuring the GFR of both kidneys togetherkidneys together

Second technique Second technique assessing each individual assessing each individual kidney was developed by calculating the kidney was developed by calculating the extraction fraction (EF) of Gd-DTPA, which is the extraction fraction (EF) of Gd-DTPA, which is the difference between renal arterial and renal difference between renal arterial and renal venous Gd-DTPA concentration, normalized to venous Gd-DTPA concentration, normalized to the arterial Gd-DTPA concentration: the arterial Gd-DTPA concentration:

ThirdThird technique to measure GFR is based on a technique to measure GFR is based on a the time-dependent concentrations of Gd-DTPA the time-dependent concentrations of Gd-DTPA in the cortex and the medulla—a two in the cortex and the medulla—a two compartment modelcompartment model
The different techniques to measure GFR still The different techniques to measure GFR still need to be validated, and their role in clinical need to be validated, and their role in clinical practice needs to be establishedpractice needs to be established

MRA & MRU correctly MRA & MRU correctly identified renal vessels and identified renal vessels and urinary system respectively. urinary system respectively.
MAG3-GFR of each kidney MAG3-GFR of each kidney correlated strongly with MR-correlated strongly with MR-GFR (GFR (rr = 0.54; = 0.54; PP <0.01), and <0.01), and mean MAG3 and MR mean MAG3 and MR clearance values were similar clearance values were similar for right and left kidneys.for right and left kidneys.

The high spatial resolution provided by these The high spatial resolution provided by these modalities, coupled with dynamic imaging of modalities, coupled with dynamic imaging of contrast agents or radioactive tracers, potentially contrast agents or radioactive tracers, potentially could allow detailed clinical evaluation of regional could allow detailed clinical evaluation of regional renal function and blood flowrenal function and blood flow
Furthure, MR imaging is the only single Furthure, MR imaging is the only single noninvasive test that provides a complete picture noninvasive test that provides a complete picture of renal status with minimal risk to the patient, of renal status with minimal risk to the patient, simultaneously improving diagnosis while lowering simultaneously improving diagnosis while lowering medical costs by virtue of its being a single testmedical costs by virtue of its being a single test

Although advances in both the technical and Although advances in both the technical and clinical aspects of functional renal MR imaging clinical aspects of functional renal MR imaging have been made, much remains to be done.have been made, much remains to be done.
The preliminary results reported in the many The preliminary results reported in the many studies reviewed are exciting, but these studies reviewed are exciting, but these techniques need to be validated against techniques need to be validated against accepted standards where such standards exist. accepted standards where such standards exist.
In addition, and perhaps more important, the In addition, and perhaps more important, the effects of these new diagnostic methods on effects of these new diagnostic methods on patient outcomes must be studied.patient outcomes must be studied.

Conclusions Conclusions

Conclusions Conclusions
Serum creatinine is the most widely used indirect Serum creatinine is the most widely used indirect measure of GFR, its popularity attributable to measure of GFR, its popularity attributable to convenience and low cost convenience and low cost
But it is very insensitive to substantial decline. GFR But it is very insensitive to substantial decline. GFR may be reduced 50% before serum creatinine may be reduced 50% before serum creatinine becomes elevated becomes elevated
Assessing renal functions by directly looking at Assessing renal functions by directly looking at urea or creatinie value can be grossly errounousurea or creatinie value can be grossly errounous
eGFR is simple and quick methodeGFR is simple and quick method

Cystatin C is a novel marker, independent of Cystatin C is a novel marker, independent of age, gender,sex but issues like thyroid disease, age, gender,sex but issues like thyroid disease, smoking etcsmoking etc
Radionuclide scans are the gold standards for Radionuclide scans are the gold standards for renal function assessment esp split GFR renal function assessment esp split GFR
BUT practical issues like availability, cost & BUT practical issues like availability, cost & radiation exposureradiation exposure
MRI has the potential to combine the functional MRI has the potential to combine the functional and anatomic information about each kidney and anatomic information about each kidney individually with ease and low risk to patientindividually with ease and low risk to patient
But need further development and validationBut need further development and validation
Conclusions Conclusions

Thank you Thank you