Factors Influencing Compliance With Home Exercise Programs … · 2018-11-28 · Rosenstock, 1986)....
10
Factors Influencing Compliance With Home Exercise Programs Among Patients With Upper-Extremity Impairment Chiung-Ying Chen, Peggy Strecker Neufeld, Christine A. Feely, Celette Sugg Skinner Key Words: human activities and occupations ~ models, occupational therapy therapeutic exercise ~ volition Objective. Patient cooperation and satisfaction with home exerciseprograms are important for successfuloutcomes of intervention. This study investigatedfactors from three mod- els to predict increased compliance and satisfaction with home exercise programs: the Model of Human Occupation (MOHO), including the volition subsystem (interests), habituation subsystem (roles), and performance subsystem (reportedphysical capacity); the Health BeliefModel (HBM), including perceived barriers, benefits, self-efficacy, and severity; and the Health Locus of Control (HLOC). Method. Sixty-two outpatients at an orthopedic upper- extremity rehabilitation facility completed a battery of questionnaires and self- report instruments, including a health beliefsurvey to assessHBM factors, the Multidimensional Health Locus of Control Scale, the Modified Activity Profile to assessthe performance subsystem of the MOHO, a demo- graphic questionnaire (including roles), a report of home exercise, and a satisfaction scale of their therapist's treatment. Compliance was determined by comparing participants' report of exercises performed to exercisesspecified on their medical chart. Results. Stepwise regression identified two predictors of compliance: perceived self-efficacy and internal HLOC, R 2 = .16. Conclusion. Results supported the role of the MOHO's volition subsystem, but roles and physical capacity -- repre the habituation and performance subsystems of the MOHO--did not contribute significantly to the prediction of compliance. Chen, C.-Y.,Neufeld, E S., Feely, C. A., & Skinner,C. S. (1999). Factorsinfluencing compliance with home exercise programs among patientswith upper-extremity impairment. American Journal of Occupational Therapy, 53, 171-180. Chiung-Ying Chen, MS, OTR, is practicing in Taiwan. At the time of this study, she was Graduate Student, Program in Occupational Therapy, Washington University School of Medicine, St. Louis, Missouri. Peggy Strecker Neufeld, MA,OTR/L,is Instructor, Program in Occupational Therapy, Box 8505, Washington University School of Medicine, 4444 Forest Park Boulevard, St. Louis, Missouri 63108-2292. Christine A. Feely, PhD,was Assistant Professor, Occupational Therapy and Surgery, Program in Occupational Therapy, Washington University School of Medicine, St. Louis, Missouri, at the time of this study. Celette Sugg Skinner, PhD, is Assistant Professor, Duke University Medical Center, Durham, North Carolina. At the time of this study, she was Assistant Professor, Mallinckrodt Institute of Radiology,Washington University School of Medicine, St. Louis, Missouri. Thisarticle wasaccepted for publication July 7, 1998. T he extent to which a person follows medical or health recommendations, such as taking medica- tions or altering lifestyle (Blackwell, 1992), has tra- ditionally been termed compliance. Because following such recommendations is considered essential for good treat- ment outcomes (Codori, Nannis, & Pack, 1992; Jette, 1982), clinicians and researchers have investigated aspects of compliance and noncompliance, interventions to improve compliance, measures of compliance, and the rela- tionship between compliance and treatment outcomes. Types of compliance that have been studied extensively include keeping clinic appointments for the management of a chronic condition (Mirotznik, Ginzler, Zagon, & Baptiste, 1998), taking medications and treatment regimes (Crane, 1996; Sackett & Snow, 1979), following regimens for diabetes (Bashoff & Beaser, 1995; Kavanaugh, Gooley, & Wilson, 1993; Pham, Fortin, Thibaudeau, 1996), con- trolling hypertension (Kjellgren, Ahlner, & Saljo, 1995; Rudd, 1995), managing arthritis symptoms (Feinberg, Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930229/ on 11/28/2018 Terms of Use: http://AOTA.org/terms
Transcript of Factors Influencing Compliance With Home Exercise Programs … · 2018-11-28 · Rosenstock, 1986)....

Factors Influencing Compliance With Home Exercise Programs Among Patients With Upper-Extremity Impairment
Chiung-Ying Chen, Peggy Strecker Neufeld, Christine A. Feely, Celette Sugg Skinner
Key Words: human activities and occupations ~ models, occupational therapy �9 therapeutic exercise ~ volition
Objective. Patient cooperation and satisfaction with home exercise programs are important for successful outcomes of intervention. This study investigated factors from three mod- els to predict increased compliance and satisfaction with home exercise programs: the Model of Human Occupation (MOHO), including the volition subsystem (interests), habituation subsystem (roles), and performance subsystem (reported physical capacity); the Health Belief Model (HBM), including perceived barriers, benefits, self-efficacy, and severity; and the Health Locus of Control (HLOC).
Method. Sixty-two outpatients at an orthopedic upper- extremity rehabilitation facility completed a battery of questionnaires and self- report instruments, including a health belief survey to assess HBM factors, the Multidimensional Health Locus of Control Scale, the Modified Activity Profile to assess the performance subsystem of the MOHO, a demo- graphic questionnaire (including roles), a report of home exercise, and a satisfaction scale of their therapist's treatment. Compliance was determined by comparing participants' report of exercises performed to exercises specified on their medical chart.
Results. Stepwise regression identified two predictors of compliance: perceived self-efficacy and internal HLOC, R 2 = .16.
Conclusion. Results supported the role of the MOHO's volition subsystem, but roles and physical capacity -- r epre the habituation and performance subsystems of the MOHO--did not contribute significantly to the prediction of compliance.
Chen, C.-Y., Neufeld, E S., Feely, C. A., & Skinner, C. S. (1999). Factors influencing compliance with home exercise programs among patients with upper-extremity impairment. American Journal of Occupational Therapy, 53, 171-180.
Chiung-Ying Chen, MS, OTR, is practicing in Taiwan. At the time of this study, she was Graduate Student, Program in Occupational Therapy, Washington University School of Medicine, St. Louis, Missouri.
Peggy Strecker Neufeld, MA, OTR/L, is Instructor, Program in Occupational Therapy, Box 8505, Washington University School of Medicine, 4444 Forest Park Boulevard, St. Louis, Missouri 63108-2292.
Christine A. Feely, PhD, was Assistant Professor, Occupational Therapy and Surgery, Program in Occupational Therapy, Washington University School of Medicine, St. Louis, Missouri, at the time of this study.
Celette Sugg Skinner, PhD, is Assistant Professor, Duke University Medical Center, Durham, North Carolina. At the time of this study, she was Assistant Professor, Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, Missouri.
This article was accepted for publication July 7, 1998.
T he extent to which a person follows medical or health recommendations, such as taking medica- tions or altering lifestyle (Blackwell, 1992), has tra-
ditionally been termed compliance. Because following such recommendations is considered essential for good treat- ment outcomes (Codori, Nannis, & Pack, 1992; Jette, 1982), clinicians and researchers have investigated aspects of compliance and noncompliance, interventions to improve compliance, measures of compliance, and the rela- tionship between compliance and treatment outcomes. Types of compliance that have been studied extensively include keeping clinic appointments for the management of a chronic condition (Mirotznik, Ginzler, Zagon, & Baptiste, 1998), taking medications and treatment regimes (Crane, 1996; Sackett & Snow, 1979), following regimens for diabetes (Bashoff & Beaser, 1995; Kavanaugh, Gooley, & Wilson, 1993; Pham, Fortin, Thibaudeau, 1996), con- trolling hypertension (Kjellgren, Ahlner, & Saljo, 1995; Rudd, 1995), managing arthritis symptoms (Feinberg,
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930229/ on 11/28/2018 Terms of Use: http://AOTA.org/terms

1988), and adhering to exercise programs (Dishman, 1982; Oldridge, 1992; Robison & Rogers, 1994).
Compliance with occupational therapy treatment reg- imens has not been the focus of many investigations, but compliance has been included as a variable in numerous studies. Patients who most closely follow their treatment recommendations have been observed to experience better treatment outcomes (Dovelle, Heeter, Fischer, & Chow, 1988; Groth, Wilder, & Young, 1994; Yuen, 1993). Although compliance with occupational therapy treatment recommendations is believed to be high (Codori et al., 1992, Feinberg, 1992), more research is needed to investi- gate a wide range of variables that may influence compli- ance and strategies that may facilitate compliance.
The term compliance has been criticized for its conno- tation that health care providers dictate what patients should do, and other terms have been suggested, such as adherence, patient cooperation, and maintenance. Groth and Wulf (1995) defined compliance in hand rehabilitation as, "an active engagement in the rehabilitation process" (p. 18). Their definition, which we have adopted here, denotes
that the therapist, physician, and patient are active agents in the rehabilitation process and that cooperation with agreed-upon specific recommendations is crucial to opti- mal patient outcomes.
Because compliance may be influenced by multiple factors, we adopted a holistic frame of reference as a con- conceptual basis for our research: the Model of Human Occupation (MOHO; Kielhofner & Burke, 1980), the Health Belief Model (HBM; Rosenstock, 1966), and the construct of Health Locus ofControl (HLOC; Wallston & Wallston, 1978). This study investigated how factors of the volition, habituation, and performance systems from the MOHO; perceived barriers, benefits, self-efficacy, and severity from the HBM; and the HLOC may influence compliance with home exercise programs for patients with upper-extremity impairment.
Literature Review Compliance in the Occupational Therapy Literature
In the occupational therapy literature, use of recommended items such as splints or other positioning devices, adaptive equipment, and wheelchairs are commonly considered as compliance behaviors (Bates, Spencer, Young, Rintala, 1993; Feinberg, 1992; Feinberg & Brandt, 1981; Furth, Holm, & James, 1994; Groth et al., 1994; Hannah & Cottrill, 1985; Krajnik & Bridle, 1992; Sharrott & Cooper-Fraps, 1986; Tyson & Strong, 1990), whereas fail- ure to keep appointments or perform specific exercises are considered noncompliance behaviors (Codori et al., 1992; Dovelle et al., 1988; Ekes & Marvin, 1985; Groth et al, 1994; Sharrott & Cooper-Fraps, 1986; Turton & Fraser, 1990; Wynn & Eckel, 1986). With few exceptions (Kielhofner & Nelson, 1983; Rust, Barris, & Hooper,
1987), studies of relationships between compliance and occupational therapy treatment outcomes or of compliance promotion interventions (Turton & Fraser, 1990; Yuen, 1993) have been a theoretical.
Models Pertaining to Compliance Several theories and explanatory models have been sug- gested to predict and explain compliance behaviors (Mullen, Hersey, & Iverson, 1987). The HBM, derived from Lewin's aspiration theory (Rosenstock, 1966; Strecher & Rosenstock, 1997), was developed to explain preventive health behaviors (Hochbaum, 1958). Janz and Becker (1984) summarized the model as consisting of the follow- ing dimensions:
�9 Perceived susceptibility--subjective perception of risk of contracting a condition.
�9 Perceived severity--evaluations of medical/clinical consequences (e.g., death, disability, pain) and possible social consequences (e.g., effects of the conditions on work, family life, and social relations).
�9 Perceived benefits--a "sufficiently-threatened" individual would not be expected to accept the recommended health action's effectiveness against perceptions that it may be expensive, dangerous (e.g., side effects, iatrogenic outcomes), unpleasant (e.g., painful, difficult, upsetting), inconvenient, time-consuming, and so forth. (p. 2)
The HBM has been studied extensively. Janz and Becker (1984) reviewed 46 studies and found perceived barriers to be the most powerful single predictor of health behavior across all studies, but the strength of predictors varied by type of behavior. Perceived risk (or susceptibility) was a stronger predictor of participation in preventive health behaviors, whereas perceived benefits was a stronger predictor of health actions recommended for persons who already had a medical condition (i.e., compliance with a treatment or rehabilitative regimen).
The HBM has been broadened to incorporate the role of self-efficacy in health-related behavior (Rosenstock, Strecher, & Becker, 1988). Self-efficacy beliefs concern one's perceived capability in performing a given behavior to produce desired outcomes (Bandura, 1977). Perceived self- efficacy may affect not only expectations for success, but also choices about where to attempt a task and how long or hard one works on it (Strecher, DeVellis, Becker, & Rosenstock, 1986).
Few occupational therapy studies are based on the HBM. Kielhofner and Nelson (1983) attempted to apply its concepts to patient cooperation and participation with therapy, positing that the fit between patients' expectation for recovery and the goals of the therapy (i.e., recovery vs. adaptation to disability) predicted how much the patient valued therapy, which, in turn, predicted cooperation and participation. Perhaps, in part, because HBM aspects encompassed by the fit between patients' expectations and therapy goals were not clearly specified, these researchers found little support for the model. Groth and Wulf (1995) specified application of HBM concepts to hand rehabilita- tion. Perceived benefits would be "increased health and
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930229/ on 11/28/2018 Terms of Use: http://AOTA.org/terms

function, return to work, and re-engagement in activities of daily living" (p. 19), for example, "if a patient believes that wearing a protective splint following a flexor tendon repair will not prevent tendon rupture, he or she will be less likely to do so" (p. 19). This delineation of application of the HBM to a rehabilitation program set the stage for investi- gations testing elements of the model in an occupational therapy context.
The MOHO, which contains some of the same con- concepts as the HBM, may provide a more comprehensive framework for understanding compliance as a form of occupational behavior. The MOHO posits that three sub- systems--volition, habituation, and performance----deter- mine occupational behavior. These subsystems, and the ele- ments that comprise them, correspond to HBM variables as well as other variables investigated in the compliance litera- ture. For example, the MOHO's values and interests corre- spond to the HBM's perceived benefits. Findings from the few studies investigating the influence of interests on treat- ment compliance have been mixed. Fronczek (1985) reported that interests did not predict behavior change among patients in hand rehabilitation. Rust et al. (1987) likewise reported that an interests-specific and exercise-spe- cific measure did not contribute significantly to explaining exercise behavior. It may be that interests were too closely related to other predictors (exercise-specific personal causa- tion, exerciser role) to contribute independently. In con- contrast, Oldridge and Streiner (1990) reported that persons who dropped out of a cardiac rehabilitation program gen- erally did not participate in leisure activities, suggesting a relationship between interests and compliance. Interests as a predictor of compliance requires further investigation.
In the MOHO's habituation subsystem, patients' roles are expected to influence their occupational behavior. Al- though research findings support this claim (Carpenter & Davis, 1976; Jones, Jones, & Katz, 1987; Kiley, Lam, & Pollak, 1993), it is unclear whether compliance with treat- ment fits the daily routines of particular roles or whether some other aspects of roles are important (i.e., whether com- pliance allows for continuation of a role, such as worker). The influence of roles on compliance behavior, particularly in the context of the MOHO, deserves investigation.
In the MOHO's performance subsystem, it is postu- lated that skills influence occupational behavior. How skills specifically affect compliance behavior, however, is un- known. Very little research has examined patients' compli- ance and perceived physical capacity. Feinberg and Brandt (1981) reported that compliant patients with rheumatoid arthritis were more symptomatic and had greater impair- ment. On the basis of this result, patients with better per- ceived physical capacity may be less compliant.
HLOC refers to people's perceptions that their health is controlled by themselves, chance, or powerful others (Rotter, 1971; Wallston & Wallston, 1978). HLOC may
influence compliance behaviors (Fronczek, 1985). Patients with "internal" or "powerful others" HLOC have been found to be more likely to comply than patients believing that their health outcomes are controlled by chance (Fronczek, 1985; Kiley et al., 1993; Schlenk & Hart, 1984). Per- personal causation, another element of the MOHO's volition construct, is related to HLOC.
In the only study we found linking the MOHO to a behavior similar to compliance, Rust et al. (1987) investi- gated whether the model explained exercise behavior in women. Although exercise as a leisure form of occupational behavior differs from exercises prescribed in a rehabilitation program, both are types of occupational behavior and have longer-term health benefits than, for instance, activities such as cooking or doing laundry. Moreover, adherence to a prescribed exercise regimen for weight loss, diabetes con- trol, or cardiac rehabilitation can be characterized as com- pliance with medical recommendations (Bashoff & Beaser, 1995; Kavanaugh et al., 1993; Robertson & Keller, 1992). Rust et al. found that the following three variables explained 43% of the variability in exercise behavior: an exercise-specific measure of personal causation, the exer- ciser role, and values regarding leisure. Their findings pro- vided strong support for consideration of the elements of the MOHO as determinants of compliance with rehabili- tation programs.
In summary, we found support in the research literature that factors from MOHO's three subsystems can influence occupational behavior. In the volition subsystem, HLOC, health beliefs, and interests are factors that can influence occupational behavior as it pertains to compliance. In the habituation subsystem, roles (e.g., homemaker, worker, spouse) can favorably influence compliance with therapy. In the performance subsystem, skills can influence compliance.
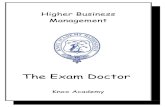
The purpose of our study was to assess the factors that predicted increased compliance of patients with upper- extremity orthopedic conditions with their home exercise programs. Our study integrated the MOHO, HBM, and HLOC to predict patient compliance. Figure 1 represents how the MOHO predicts compliance and incorporates the HBM and HLOC. Using the framework in Figure 1, we hypothesized that the following would predict greater com- pliance with home exercise programs:
�9 Greater perceived benefits of rehabilitation, greater perceived severity of the disease or injury, greater self-efficacy, and lower perceived barriers to carry- ing out the home exercise program
�9 Internal HLOC �9 Higher interest in the recommended home exercise
program activities.
Conversely, we hypothesized that perceived physical capa- bility should be negatively related to compliance and con- tribute significantly to predicting the level of compliance.
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930229/ on 11/28/2018 Terms of Use: http://AOTA.org/terms

The Model of Human Occupation
The Open System
Throughput
Feedback (change* In symptoms, overall improvement and other benefits) a
Output Compliance
Occupational
Behavior
Figure 1. The hypothesized relationship of compliance occu- pational behavior, the Model of Human Occupation, the Health Belief Model (HBM), and the Health Locus of Control (HLOC). The HBM includes perceived benefits, perceived barriers, perceived severity, perceived susceptibility, per- ceived self-efficacy, and cues to action. The HLOC includes internal locus of control and external locus of control (i.e., powerful others, chance).
Method
Participants
The research was approved by Washington University School of Medicine's Human Studies Committee. A con- venience sample was recruited through occupational thera- pists and physical therapists at Barnes-Jewish Hospital's Orthopedic Center for Upper Extremity Rehabilitation. The treating therapist selected patients who met the study criteria and invited them to visit with the researcher imme- diately after treatment. Eligibility criteria were more than 21 years of age, upper-extremity impairment, recommen- dation of a home exercise program by an occupational ther- apist or physical therapist at least 1 week before the study, and a willingness to participate in this study as indicated by written consent. All home exercise programs required ac- tive participation or mobilization by the patient. Exclusion criteria were cognitive deficits or language barriers prevent- ing completion of the questionnaire, upper-extremity im- pairment secondary to upper motor neuron lesion, and no home exercise program involving the affected upper extremity. The consent form stated that the purpose of the research was to gain a better understanding of beliefs about health and treatment and to document how participants carried out their home exercise programs.
Instruments
Participants were invited to complete a 15-page battery of questionnaires and self-report instruments on site or at home and returned by mail. The following describes each
questionnaire and instrument contained in the battery. Demographic items. These items included age, gender,
marital status, date of injury or recent surgery, diagnosis, job description, educational background, and employment status.
Health Belief Model. The HBM is a 19-item health belief survey designed to assess perceived severity (7 items), benefits (2 items), barriers (8 items), and self-efficacy (2 items). Each item is measured on a 6-point Likert scale (1 = strongly disagree, 5 = strongly agree). The score for each dimension was the sum of the values for the items of that dimension.
Health Locus of Control The 18-item Multidimen- sional Health Locus of Control Scale (Form A) (Wallston & Wallston, 1978) measures perception of internal control (IHLC), the control of chance, or the control of powerful others. Each item is measured on a 6-point Likert scale (1= strongly disagree, 5 = strongly agree).
Interests and perceived physical capacity. The Modified Activity Profile, which is based on Baum's (1995) Activity Card Sort, was constructed for the purpose of this study to determine the perceived capacities and extent of enjoyability in activities by persons with upper-extremity orthopedic conditions. The Activity Card Sort had been developed to measure older persons' activities and determine activity patterns of persons with cognitive impairment. The Modified Activity Profile includes the original 78 activity items home management (21 items), leisure activities (47 items), and social activities (10 items)--but was modified in two respects. Participants were asked to rate their per- performance level for each item from 1 ("gave up due to injury") to 5 ("able to perform as prior to injury") and to rate each item for interest from 1 ("do not enjoy it at all") to 4 ("enjoy it very much"). We determined the self- reported physical capacity as the ratio of number of activi- ties currently performed to those activities performed before injury. Interest in activities was computed as the sum of the interest ratings divided by the total number of activities reported, indicating generally low (1, 2) or high (3, 4) ratings of interest.
Compliance rates. A home exercises self-report was designed to document each exercise, the number of repeti- tions per session, and the number of sessions per day that were recommended by the participants' therapists as well as which exercises, number of repetitions, and sessions per day were actually performed on a typical day during the previ- ous week. To determine compliance, we compared the par- participant's self-report of exercises performed to (a) his or her memory of therapist's recommendation and (b) the thera- pist's recommendation (determined from chart review). For both methods, a percentage of recommended exercises was calculated. For example, if the home exercise program involved three exercises performed four times each day for 10 repetitions each, the total possible would be 120. If par-
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930229/ on 11/28/2018 Terms of Use: http://AOTA.org/terms

16
14
12
1 0
6
1 5 9 13 17 21 25 29 33 37 41 45 49 to to to to to to to to to to to to to 4 8 12 16 20 24 28 32 36 40 44 48 52
N u m b e r o f weeks
_--> �9
53
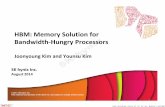
Figure 2. Frequency distribution of number of weeks since onset of injury or date of surgery.
participants performed 10 repetitions of all three exercises three times a day, their compliance would be 90/120 or 75%. In addition to the exact percentages, which were used in the correlation and regression analyses, participants were categorized as having low (0%0-33%), moderate (34%o-66%), or high (67%-100%) compliance.
Satisfaction. Participants rated their satisfaction with their therapist's treatment on a 6-point Likert scale (1 = very dissatisfied, 5 = very satisfied).
Data Analysis
Data management and analysis were performed with the Statistical Package for the Social Sciences (SPSS) for Windows 6.0 (Norusis, 1993). Spearman rank order cor- relation, t test, chi-square, and multiple linear regression analyses were performed. In the regression analysis, step- wise selection was used, combining backward and forward processes. SPSS first selects the independent variable that has the largest positive or negative association with the dependent variable. The correlation between independent and dependent variables must have a value of p < .05. Then, the selected variable is tested to see whether it should be removed on the basis of removal criteria (p< .10).
Results Of the 102 persons who agreed to participate in this study, 75 (74%) returned the questionnaires and self-report
instruments of which 13 were incomplete. Of the remain- ing 62 participants, 23 (37%) were men and 39 (63%) were women, ranging in age from 23 to 88 years (M= 47.8 years, SD = 13.8). Forty-one (66%) were married. Diagnoses included 24 (39%) nerve compression syn- dromes, 23 (37%) shoulder injuries, 9 (15%) fractures, and 6 (10%) other. Because there was no variation in satisfac- tion with treatment (61 participants rated themselves as satisfied or very satisfied), it was not examined in relation to compliance. Distribution of time since date of surgery or onset of injury is shown in Figure 2.
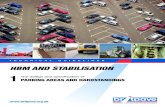
The two compliance measures compared participants' documentation of their actual exercise performance to (a) self-report and (b) chart documentation of the recom- mended home exercise program. On the basis of what they remembered their therapists' recommending, 74% were categorized as 100% compliant. In contrast, on the basis of chart documentation of the recommended regi- men, 35% were 100% compliant (see Figure 3). The cor- relation coefficient of these two compliance rates, although significant (p < .001), was .51. (In general, par- participants did not understand or forgot to mention about 12% of the home exercise program recommendations documented in their charts.) We considered the rates from chart review as more accurate and, thus, used them in sub- sequent analyses.
T tests examining differences in compliance on the basis of categorical, demographic variables yielded no
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930229/ on 11/28/2018 Terms of Use: http://AOTA.org/terms

50
45
40
10
0 to 11 21 31 41 51 61 71 81 91 10 to to to to to to to to to
20 30 40 50 60 70 80 90 100
Percentage compliance
[ ] patient's memory
[ ] chart review
Figure 3. Frequency distribution of compliance on the basis of participants' memory and chart review.
signficant differences by gender, marital status, or work status during rehabilitation. Participants who had child-care needs (76%) were more compliant than those without child-care needs (65%), but this difference did not achieve the criterion for significance of.05, t(60) = 11.64, p = .11.
Spearman rank order correlations among compliance, factors of the HBM and HLOC, and the demographic variables are shown in Table I. Only perceived self-efficacy was significantly correlated with compliance. Participants with higher perceived self-efficacy about the home exercises were more compliant and reported lower perceived barriers and higher perceived benefits associated with treatment. In the stepwise regression (see Table 2), only perceived self- efficacy and IHLC significantly contributed to compliance behavior (p < .01).
Individual health belief items were examined to deter- mine which were most salient. Table 3 shows the items with consistent agreement or disagreement. Items concern- ing spouse, significant others, and friends' expectations that the participant do the home exercises elicited strong agree- ment or disagreement among participants (6 to 10 of the participants left these items blank). Consequently, for all 62 participants, these items were not the most important. Finally, we attempted to examine associations between individual health belief items and a categorical measure of compliance behavior (low, moderate, high) using chi- square analyses, but the number of cells with only 2, 1, or 0 participants rendered the analysis unworkable.
Discussion This study partially supported our proposed conceptualiza- tion of how the MOHO, integrating aspects of the HBM and HLOC, explains compliance behavior with home exer- cise programs. Results particularly highlight the impor- tance of self-efficacy--the belief that one can perform par- particular behaviors, in this case home exercises. The construct of self-efficacy is an important component of the volition subsystem of the MOHO; that is, personal causation includes one's sense of efficacy in occupations. According to Kielhofner (1995), "Sense of efficacy is the perception of control over one's own behavior.., as well as a sense of control in achieving desired outcomes of behavior" (p. 43). Kielhofner and Burke (1985) stated that persons "possess an image of self-efficacy of skill, which is the belief that one's abilities are useful and relevant in one's life situation" (p. 16), and "this perceived match between one's capacity and the demands and resources of the environment leads one to make positive choices for encountering the environ- ment through occupational behavior" (p. 17). In our study, belief in ability to perform the exercises contributed to the participants' choice of occupational behaviors, that is, the actual performance.
The significant contribution of perceived self-efficacy supports findings of other studies (Becker, Drachman, & Kirscht, 1972; Strecher et al., 1986). Confidence in mak- ing successful change has been associated with cardiac reha- bilitation and alcoholism treatment compliance (Oldridge
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930229/ on 11/28/2018 Terms of Use: http://AOTA.org/terms

Table 1 Spearman Rank Order Correlation Analysis Among Compliance, Factors of the Health Belief Model and Health Locus of Control, and Demographic Variables Variable 1 2 3 4 5 6 7 8 9 10 11 12 13
1. Compliance 2. Barriers - . 11 - - 3. Benefits - .07 - .20 - - 4. Self-efficacy .30* -.36** .47*** - - 5. Severity - . 11 .06 - .08 -.26* - - 6. IHLC - .09 .02 .17 -.21 - .06 - - 7. C H L C .07 .50*** - .20 - .31" .13 - .19 - - 8. PHLC -.01 , .28* - .02 - .13 .15 .14 .47*** - - 9. Interest .08 -.01 .19 .25 - .10 .18 .02 .10 - -
10. Capacity .10 -.30* .27* .42** -.48*** .12 -.21 - .04 - .05 - - 11. Age .22 .08 - .02 - .03 - .14 - .19 .25 .25* .30* .18 - - 12. Weeks - .07 - .08 -.28* -.28* - .02 - .05 - .14 -.26* - .13 - .10 .02 - - 13. Education .13 - .02 - .08 .14 -.30* .01 - .09 - .07 - .07 .37** .03 .03 - -
Note. Barriers = perceived barriers; benefits = perceived benefits; self-efficacy = perceived self-efficacy; severity= perceived severity; IHLC = internal health locus of control; C H L C = chance health locus of control; PHLC = powerful others health locus of control; interest = interest in activities; weeks = weeks since onset. *p< .05. **p< .01. ***p< .001.
& Streiner, 1990; Rees, 1985). Therefore, encouraging patients to become actively involved in treatment and increasing their confidence in performing recommenda- tions seems to be crucial for treatment effectiveness (Blackwell & Gutmann, 1985). Our findings again con- firm that patients with higher expectations regarding out- come tend to be more actively engaged in treatment.
Perceived self-efficacy has been discussed recently in other contexts in the occupational therapy literature (Gage, Noh, Polatajko, & Kaspar, 1994; Gage & Polatajko, 1994). Gage et al. (1994) hypothesized that perceived self-efficacy may help explain "an alarming discrepancy between the occupational performance skills developed in the clinical setting and the degree to which the client willingly puts these skills to use outside the clinical environment" (p. 783). Although these researchers discussed perceived self- efficacy as it relates to general occupational therapy treat- ment, it also has value for understanding patients' imple- mentation of treatment as well as for understanding occupational performance in general.
Our finding that IHLC was inversely related to com- pliance was the opposite of findings reported by Fronczek (1985). On the one hand, this finding seems to contradict the finding that greater self-efficacy promotes compliance and appears not to support the MOHO. On the other hand, patients who have sustained injuries may be justified in feeling that they are not in control of their health and that their best possibility for recovery lies in the surgical and therapeutic procedures they are undergoing. For
Table 2 Summary of Stepwise Regression Analysis for Variables Predicting Compliance With Home Exercise Programs
Variable B (SE) 13
Step 1. Perceived self-efficacy 7.05 (2.60) .33 Step 2. Internal health locus of control -1 .46 (0.62) - .28
Note. R 2 = .08 for Step 1; Delta R 2 = .08 for Step 2 (ps < .05).
patients with lower IHLC, following recommendations from health providers with the encouragement of friends or family members would be consistent with their orientation and would lead to compliance (Schlenk & Hart, 1984). Therefore, this finding may not contradict the contribu- tion of perceived self-efficacy or the MOHO but may sug- gest that encouragement from the therapist, combined with a sense of self-efficacy with regard to performing the home exercise program (which can be enhanced by actual performance in the clinic), can significantly increase com- pliance with treatment.
The importance of perceived benefits from and barri- ers to therapeutic recommendations is consistent with find- ings from other studies and supports the MOHO (Becker, 1974; Becker et al., 1972; Newell, Price, Roberts, & Baumann, 1986; Yuen, 1993). Perceived barriers are con- nected to the habituation subsystem. If the home exercise program does not fit into the patient's routines, it is less likely to be performed. Therefore, therapists can help pa- tients understand benefits that will result from compliance and structure the home exercise program and the environ- ment to make compliance as convenient as possible.
Although only the volition subsystem of the MOHO contributed significantly to explaining compliance with home exercise programs, the habituation and performance subsystems still deserve attention. Our findings suggest that roles, a component of the habituation subsystem, influence compliance behavior. For example, participants with child-care needs were more compliant, and support from a significant other or spouse, family members, and friends for performing the exercises was important. The importance of social support for following therapeutic rec- ommendations confirms findings reported in previous research (Kirscht, Kirscht, & Rosenstock, 1981; Oakes, Ward, Gray, Klauber, & Moody, 1970; Rees, 1985; Schlenk & Hart, 1984). Therapists may find that helping family members and friends express confidence in the
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930229/ on 11/28/2018 Terms of Use: http://AOTA.org/terms

Table 3 Items From the Health Belief Survey That Have the Highest Percentage of Agreement or Disagreement Item % (Agree, Disagree)
I am not sure my therapist knows how to help me. I am afraid my home exercises will make my symptoms worse. I feel confident I can successfully do my home exercises. I think my exercises take too much time. My other family members expect or think I should do my exercises. I feel discouraged when I try to do my home exercises. My hand/arm injury/disease negatively affects my overall daily life. If I do my home exercises, my overall daily life will improve.
95 (Disagree) 92 (Disagree) 89 (Agree) 82 (Disagree) 81 (Agree) 81 (Agree) 81 (Agree) 77 (Agree)
Note. Agree = strongly agree + agree; disagree = strongly disagree + disagree.
patient's ability to make improvement by doing the exer- cises may be an especially effective strategy for enhancing compliance and, thus, promoting recovery. An important strategy therapists may use to enhance recovery would be to link patients and family members with relevant commu- nity resources, such as support groups for pain manage- ment or reflex sympathetic dystrophy or disability advocacy organizations.
With regard to the performance subsystem of the MOHO, our study did not support Feinberg and Brandt's (1981) finding that patients with higher physical capacity were less compliant. Greater perceived physical capacity was positively associated with perceived benefits and in- versely related to perceived barriers and severity. Perhaps patients with greater skill find it easier or more possible to perform their home exercise program and, thus, are more compliant. Whether this finding is generalizable beyond home exercise program regimens is still to be determined.
An examination of the items that showed consistent responses from the entire group of participants shows high confidence in the therapist and indicates that the exercises themselves are not a problem. However, the differences between perceived and actual compliance are noteworthy. The finding that about three quarters of participants thought that they were fully compliant but only one third actually were (as indicated by chart review) is consistent with Kortman's (1992) finding that patients recalled only 63% of 11 instructional statements for splint wearing and may partially explain why we found so few associations between health beliefs and compliance. Compliance may depend as much on correct understanding as on volition. Because most participants were not clear about what con- stituted the home exercise program, therapists may need to provide written instructions and periodically review their prescriptions with patients to identify and correct misun- derstanding.
This study has a number of limitations that may have affected the amount of variance explained by the predic- tors: a small sample size, large selection and response bias, instrumentation limitations, and much variation of time since injury. Selection bias was the major problem in this study. Convenience sampling may have resulted in thera- pists referring the most compliant patients on their case-
load. In addition, validity and reliability of the HBM and the Modified Activity Profile are unknown. The 15-page battery of questionnaires and self-report instruments may have been too long for most participants to complete, or they may have rushed to finish it without careful thinking (Rust et al., 1987). Finally, several methods of measuring compliance over a longer period would have yielded more accurate estimates of compliance than the one-time, one- method measure used in this study.
To address these limitations, future research should use a larger sample size, including randomly selected par- participants with similar medical conditions (e.g., all with carpal tunnel syndrome) and have a similar range of time since injury (e.g., acute, subacute, chronic). Variance may also be reduced if participants are examined on the basis of their time since the beginning of treatment instead of time since the onset of the orthopedic condition. Recommenda- tions to enhance reliability and validity of the instruments include designing a shorter survey and including an obser- vation assessment of the client's understanding of the home exercise program. Communicating more effectively with recruiting therapists to reduce selection bias is also important. Finally, a more accurate measure of the partici- pants' active engagement in the rehabilitation process would be a periodic assessment instead of using only a one- time measure.
Conclusion These findings partially supported the MOHO as a frame- work for predicting compliance behavior with occupa- tional therapy and physical therapy treatment. The volition subsystem made a greater contribution than the habitua- tion and performance subsystems, perhaps because persons are motivated by their beliefs and perceptions. Our find- ings that self-efficacy and IHLC are significant predictors of compliance with home exercise programs have implica- tions for practice. An enhanced IHLC with greater com- pliance or patient engagement might occur if therapists encouraged greater participation from patients in treat- ment planning, problem solving, and goal setting. Patients' sense of control may also be enhanced if therapists attempt to decrease the possible barriers to compliance, such as patient fears from lack of knowledge or the family member
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930229/ on 11/28/2018 Terms of Use: http://AOTA.org/terms

members' lack of understanding for the importance o f their sup- port. Strategies to improve patient self-efficacy for manage- ment o f a home exercise program may also further treat- ment outcomes, such as encouraging peer sharing for role modeling among patients in the rehabilitation experience and teaching patients to set realistic weekly goals to ensure success. In addition, therapists may encourage more accu- rate and consistent follow-through by giving patients the oppor tuni ty for further feedback and encouragement when requesting them to periodically demonstrate their home
exercise programs. H o m e programs and recommendat ions are important in achieving therapy outcomes, and occupa- tional therapists and physical therapists would benefit from further investigation o f the factors that influence patients' engagement in their treatment. �9
Acknowledgments We thank Duane Whitney, PhD, Carolyn Baum, PhD, OTR/C, FAOTA, the occupational therapists and physical therapists at the Orthopedic Center for Upper Extremity Rehabilitation, the Physical Therapy Department at Barnes-Jewish Hospital, and Ching-ying Shen for their valuable contributions to this research. This report is based on the first author's thesis submitted in partial fulfillment of the requirements for the degree of master of science.
References Bandura, A. (1977). Self-efficacy: Toward a unifying theory of
behavioral change. Psychological Review, 84, 191-215. Bashoff, E. C., & Beaser, R. S. (1995). Insulin therapy and the
reluctant patient. Postgraduate Medicine, 97, 86-96. Bates, E S., Spencer, J. C., Young, M. E., & Rintala, D. H. (1993).
Assistive technology and the newly disabled adult: Adaptation to wheel- chair use. American Journal of Occupational Therapy, 47, 1014-1021.
Baum, C. M. (1995). The contribution of occupation to function in persons with Alzheimer's disease. Journal of Occupational Science (Australia), 2(2), 59-67.
Becker, M. H. (1974). The Health Belief Model and sick role behavior. Health Education Monographs, 2, 409-414.
Becket, M. H., Drachman, R. H., & Kirscht, J. P. (1972). Predicting mothers' compliance with pediatric medical regimens. Journal of Pediatrics, 81, 843-853.
Blackwell, B. (1992). Compliance. Psychotherapy and Psycho- somatics, 58, 161-169.
Blackwell, B., & Gutmann, M. C. (1985). Compliance. In C. J. Bulpitt (Ed.), Handbook of hypertension: Epidemiology of hypertensive (pp. 453-472). New York. Elsevier.
Carpenter, J. O., & Davis, L.J. (1976). Medical recommendations followed or ignored: Factors influencing compliance in arthritis. Archives of Physical Medicine and Rehabilitation, 57, 241-245.
Codori, A. M., Nannis, E. D., & Pack, A. (1992). The develop- ment of a clinical measure of compliance with hand rehabilitation. Journal of Hand Therapy, 5, 29-33.
Crane, L. A. (1996). Social support and adherence behavior among women with abnormal Pap smears. Journal of Cancer Education, 11(3), 16/t-173.
Dishman, tLK. (1982). Compliance/adherence in health-related exercise. Health Psychology, 1, 237-267.
Dovelle, S., Heeter, P. K., Fischer, D. R., & Chow, J. A. (1988). Case Report--Early controlled motion following flexor tendon graft. American Journal of Occupational Therapy, 42, 457-463.
Ekes, A., & Marvin, J. A. (1985). Burn patient cooperation in phy- sical and occupational therapy. Journal of Burn Care and Rehabilitation, 6, 246-249.
Feinberg, J. (1988). The effect of patient-practitioner interaction on compliance: A review of the literature and application in rheumatoid arthritis. Patient Education and Counseling, 11, 171-187.
Feinberg, J. (1992). Effect of the arthritis health professional on compliance with use of resting hand splints by patients with rheumatoid arthritis. Arthritis Care and Research, 5, 17-23.
Feinberg, J., & Brandt, K. D. (1981). Use of resting splints by patients with rheumatoid arthritis. American Journal of Occupational Therapy, 35, 173-178.
Fronczek, Y. R. (1985). A study of the compliance and roles, locus of control, and interests of the acute hand injured patient. Unpublished master's thesis, Virginia Commonwealth University, Richmond.
Furth, H. J., Holm, M. B., &James, A. (1994). Reinjury preven- tion follow-through for clients with cumulative trauma disorders. American Journal of Occupational Therapy, 48, 890-898.
Gage, M., Noh, S., Polatajko, H. J., & Kaspar, V. (1994). Measuring perceived self-efficacy in occupational therapy. American Journal of Occupational Therapy, 48, 783-790.
Gage, M. N., & Polatajko, H. (1994). Enhancing occupational performance through an understanding of perceived self-efficacy. American Journal of Occupational Therapy, 48, 452-461.
Groth, G. N., Wilder, D., & Young, V. L. (1994). The impact of compliance on rehabilitation of mallet finger injuries. Journal of Hand Therapy, 7, 21-24.
Groth, G. N., & Wulf, M. B. (1995). Compliance with hand reha- bilitation: Health beliefs and strategies. Journal of Hand Therapy, 8, 18-22.
Hannah, R. E., & Cottrill, S. D. (1985). The Canadian collar: A new cervical spine orthosis. American Journal of Occupational Therapy, 39, 171-177.
Hochbaum, G. M. (1958). Public participation in medical screening program: A sociopsychological study (PHS Publication no. 572). Washington, DC: U.S. Government Printing Office.
Janz, N. K., & Becker, M. H. (1984). The Health Belief Model: A decade later. Health Education Quarterly, 11, 1-47.
Jette, A. M. (1982). Improving patient cooperation with arthritis treatment regimens. Arthritis and Rheumatism, 25, 447-453.
Jones, P. K., Jones, S. L., & Katz, L. (1987). Improving compliance for asthmatic patients visiting the emergency department: Using a Health Belief Model intervention. Journal of Asthma, 24, 199-206.
Kavanangh, D. J., Gooley, S., & Wilson, P. H. (1993). Prediction of adherence and control in diabetes. Journal of Behavioral Medicine, 16, 509-522.
Kielhofner, G. (1995). A model of human occupation:, Theory and application (2nd ed.). Baltimore: Williams & Wilkins.
Kielhofner, G., & Burke, J. P. (1980). A model of human occupa- tion, part 1. Conceptual framework and content. American Journal of Occupational Therapy, 34, 572-581.
Kielhofner, G., & Burke, J. P. (1985). Components and determi- nants of human occupation. In G. Kielhofner (Ed.), A model of human occupation: Theory and application (pp. 12-36). Baltimore: Williams & Wilkins.
Kielhofner, G., & Nelson, C. (1983). A study of patient motiva- tion and cooperation/participation in occupational therapy. Occu- pational Therapy Journal of Research, 3, 35-46.
Kiley, D.J., Lam, C. S., & Pollak, R. (1993). A study of treatment compliance following kidney transplantation. Transplantation, 55(1), 51-56.
Kirscht, J. P., Kirscht, J. L., & Rosenstock, I. M. (1981). A test of interventions to increase adherence to hypertensive medical regimens. Health Education Quarterly, 8, 261-272.
Kjellgren, K. I., Ahlner, J., & Saljo, R. (1995). Taking antihyper- tensive medication: Controlling or co-operating with patients. International Journal of Cardiology, 47, 257-268.
Kortman, B. (1992). Patient recall and understanding of instruc- tions concerning splints following a Zone 2 flexor tendon repair.
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930229/ on 11/28/2018 Terms of Use: http://AOTA.org/terms

Australian Occupational Therapy JournaL 39, 5-11. Krajnik, S. R., & Bridle, M. J. (1992). Hand splinting in quadri-
plegia: Current practice. American Journal of Occupational Therapy, 46, 149-156.
Mirotznik, J., Ginzler, E., Zagon, G., & Baptiste, A. (1998). Using the Health Belief Model to explain clinic appointment-keeping for the management of a chronic disease condition. Community Health, 23, 195-210.
Mullen, P. D., Hersey, J. C., & Iverson, D. C. (1987). Health behavior models compared. Social Science Medicine, 24, 973-981.
Newell, S. M., Price, J. H., Roberts, S. T., & Baumann, R. R. (1986). Utility of the modified Health Belief Model in predicting com- pliance with treatment by adult patients with advanced cancer. Psychological Report, 59, 783-791.
Norusis, M. J. (1993). SPSS for Windows: Base system user's guide (Release 6.0). Chicago: SPSS Inc.
Oakes, T. W., Ward, J. R. Gray, R. M., Klauber, M. R., & Moody, P. M. (1970). Family expectations and arthritis patient compliance to a hand resting splint regimen. Journal of Chronic Disease, 22, 757-764.
Oldridge, N. B. (1992). Compliance bias as a factor in longitudi- nal exercise research: Osteoporosis. Sports Medicine, 13(2), 78-85.
Oldridge, N. B., & Streiner, D. L. (1990). The Health Belief Model: Predicting compliance and dropout in cardiac rehabilitation. Medicine and Science in Sports and Exercise, 22, 678-683.
Pham, D. T., Fortin, E, & Thibaudeau, M. E (1996). The role of the Health Belief Model in amputees' self-evaluation of adherence to diabetes self-care behaviors. Diabetes Education, 22, 126-132.
Rees, D. W. (1985). Health beliefs and compliance with alco- holism treatment. Journal of Studies on Alcohol, 46, 517-524.
Robertson, D., & Keller, C. (1992). Relationships among health beliefs, self-efficacy and exercise adherence in patients with coronary artery disease. Heart and Lung, 21(1), 56-63.
Robison, J. I., & Rogers, M. A. (1994). Adherence to exercise pro- grammes. Sports Medicine, 17(1), 39-52.
Rosenstock, I. M. (1966). Why people use health services. Milbank Memorial Fund Quarterly, 44(3, Suppl.), 94-127.
Rosenstock, I. M., Strecher, V. J., & Becker, M. H. (1988). Social learning theory and the Health Belief Model. Health Education Quarter/v, 15, 175-183.
Rotter, J. B. (1971). External control and internal control. Pscyhology Today, 5, 37-42.
Rudd, P. (1995). Clinicians and patients with hypertension: Unsettled issues about compliance. American Heart Journal 130, 572-579.
Rust, K. M., Barris, R., & Hooper, E H. (1987). Use of the Model of Human Occupation to predict women's exercise behavior. Occupational Therapy Journal of Research, 7, 23-35.
Sackett, D. L., & Snow, J. C. (1979). The magnitude of compli- ance and noncompliance. In R. B. Haynes, D. W. Taylor, & D. L. Sackett (Eds.), Compliance in health care (pp. 11-22). Baltimore: Johns Hopkins University Press.
Schlenk, E. A., & Hart, L. K. (1984). Relationship between health locus of control, health value, and social support and compliance of persons with diabetes mellitus. Diabetes Care, 7, 566-574.
Sharrott, G. W., & Cooper-Fraps, C. (1986). Theories of motiva- tion in occupational therapy; An overview. American Journal of Occupational Therapy, 40, 249-257.
Strecher, V. J., DeVellis, B. M., Becker, M. H, & Rosenstock, I. M. (1986). The role of self-efficacy in achieving health behavior change. Health Education Quarterly, 13, 73-91.
Strecher, V. J., & Rosenstock, I. M. (1997). The Health Belief Model. In K. Glanz, E Lewis, & B. K. Rimer (Eds.), Health behavior and health education (2nd ed., pp. 41-59). San Francisco: Jossey-Bass.
Turton, A., & Fraser, C. (1990). The use of home therapy pro- grammes for improving recovery of the upper limb following stroke. British Journal of Occupational Therapy, 53, 457-463.
Tyson, R., & Strong, J. (1990). Adaptive equipment: Its effective- hesS for people with chronic lower back pain. Occupational Therapy Journal of Research, 10, 111-121.
Wallston, K. A., & Wallston, B. S. (1978). Development of the Multidimensional Health Locus of Control (MHLC) Scales. Health Education Monographs, 6, 160-170.
Wynn, K. S., & Eckel, E. M. (1986). Juvenile rheumatoid arthri- tis and home physical therapy program compliance. Physical and Occupational Therapy in Pediatrics, 6(1), 55-63.
Yuen, H. K. (1993). Increasing medication compliance in a woman with anoxic brain damage and partial epilepsy. American Journal of Occupational Therapy, 47, 30-33.
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930229/ on 11/28/2018 Terms of Use: http://AOTA.org/terms