
Eurotransplant- Principles of Organ Allocation Dr. Axel Rahmel Medical Director Eurotransplant...
73
Eurotransplant Eurotransplant - - Principles of Organ Principles of Organ Allocation Allocation Dr. Axel Rahmel Dr. Axel Rahmel Medical Director Medical Director Eurotransplant International Foundation Eurotransplant International Foundation Meeting with Representatives from the Ministry of Meeting with Representatives from the Ministry of Health Health and the Republic Expert Commissions and the Republic Expert Commissions Belgrade, Serbia – 10.08.2009 Belgrade, Serbia – 10.08.2009
-
Upload
brett-leonard -
Category
Documents
-
view
233 -
download
2
Transcript of Eurotransplant- Principles of Organ Allocation Dr. Axel Rahmel Medical Director Eurotransplant...

EurotransplantEurotransplant--
Principles of Organ AllocationPrinciples of Organ Allocation
Dr. Axel RahmelDr. Axel RahmelMedical DirectorMedical Director
Eurotransplant International FoundationEurotransplant International Foundation
Meeting with Representatives from the Ministry of Health Meeting with Representatives from the Ministry of Health and the Republic Expert Commissionsand the Republic Expert Commissions
Belgrade, Serbia – 10.08.2009Belgrade, Serbia – 10.08.2009

The key problem in organ The key problem in organ transplantation in Europe is transplantation in Europe is
organ shortagorgan shortage…e…

Kidney waiting list and transplantsKidney waiting list and transplants Eurotransplant 1969 - 2007Eurotransplant 1969 - 2007
11308
3703
1032
Each day, Each day, 9 European citizens9 European citizens die whilst die whilst waiting for a suitable organ transplant*waiting for a suitable organ transplant*
*3.262 deaths on the waiting list in 2007, Council of Europe data 2008*3.262 deaths on the waiting list in 2007, Council of Europe data 2008
Grim facts…Grim facts…

......and organ donation rates are and organ donation rates are not equally distributed over not equally distributed over
EuropeEurope

> 20
15-20
10-15
< 10
Donors pmp
Council of Europe; Newsletter Transplant, Vol .13 No. 1, September 2008

15,6
20,2
24,8
14,412,3
18,6 17,8 17,8
1,30,0
5,0
10,0
15,0
20,0
25,0
30,0
ET A B G NL L SLO HR RS
PMPPMP
Organ donation – Eurotransplant andOrgan donation – Eurotransplant andRepublic of Serbia - 2008Republic of Serbia - 2008

WHO GUIDING PRINCIPLES ON WHO GUIDING PRINCIPLES ON HUMAN CELL, TISSUE HUMAN CELL, TISSUE AND ORGAN AND ORGAN
TRANSPLANTATIONTRANSPLANTATIONGuiding Principle 9Guiding Principle 9
• Where donation rates do not meet clinical Where donation rates do not meet clinical demand, demand, allocation criteria allocation criteria should be should be defined at national or subregional level by defined at national or subregional level by a committee that includes experts in the a committee that includes experts in the relevant medical specialties, bioethics and relevant medical specialties, bioethics and public health…public health…

WHO GUIDING PRINCIPLES ON WHO GUIDING PRINCIPLES ON HUMAN CELL, TISSUE HUMAN CELL, TISSUE AND ORGAN AND ORGAN
TRANSPLANTATIONTRANSPLANTATIONGuiding Principle 9Guiding Principle 9
• The allocation of organs, cells and tissues The allocation of organs, cells and tissues should be guided by clinical criteria and should be guided by clinical criteria and ethical norms, not financial or other ethical norms, not financial or other considerations. considerations.
• Allocation rules, defined by appropriately Allocation rules, defined by appropriately constituted committees, should be constituted committees, should be equitable, externally justified, and equitable, externally justified, and transparent.transparent.

Allocation principlesAllocation principles

Organ allocation principlesOrgan allocation principles
• Equity: every patient the same chanceEquity: every patient the same chance
• Queuing: longest waiting firstQueuing: longest waiting first
• Utility: best post-Tx outcome firstUtility: best post-Tx outcome first
• Need: sickest patient firstNeed: sickest patient first
• Net benefit: balancing urgency and Net benefit: balancing urgency and
outcomeoutcome

Organ allocation principlesOrgan allocation principles
• Equity: every patient the same chanceEquity: every patient the same chance• Sense of fairness or impartialitySense of fairness or impartiality• Lack of bias or discriminationLack of bias or discrimination
• Queuing: longest waiting firstQueuing: longest waiting first
• Need/urgency: sickest patient firstNeed/urgency: sickest patient first
• Utility: best post-Tx outcome firstUtility: best post-Tx outcome first
• Net benefit: balancing urgency and Net benefit: balancing urgency and
outcomeoutcomeLotteryLottery
Equal/similar patientshave to be treated
equal/similar

• Equity: every patient the same chanceEquity: every patient the same chance
• Queuing: longest waiting firstQueuing: longest waiting first• Waiting time is easy to understandWaiting time is easy to understand• ““first come first served” is a fair way to do first come first served” is a fair way to do
thingsthings
• Need/urgency: sickest patient firstNeed/urgency: sickest patient first
• Utility: best post-Tx outcome firstUtility: best post-Tx outcome first
• Net benefit: balancing urgency and Net benefit: balancing urgency and outcomeoutcome
Organ allocation principlesOrgan allocation principles

Important factors in allocationImportant factors in allocationPublic opinionPublic opinion
No priorityNo priority
• Gender (95%)Gender (95%)
• Income (97%)Income (97%)
• Employment status Employment status (95%)(95%)
• Profession (92%)Profession (92%)
High priorityHigh priority
• Waiting time (87%)Waiting time (87%)
• Post-tx outcome Post-tx outcome (79%)(79%)
• Young age (66%)Young age (66%)
• Parental status (56%)Parental status (56%)
Social Science and Medicine 2001; 52:853-861

Queuing: longest waiting firstQueuing: longest waiting firstEmergency departmentEmergency department
?

Urgency vs. outcome in allocationUrgency vs. outcome in allocationThe „net-benefit“-conceptThe „net-benefit“-concept
• Need/urgency: sickest patient firstNeed/urgency: sickest patient first• Direct organs to those most in need, i.e. most at risk
of death without a transplant (medical urgency)
• Utility: patient with best outcome firstUtility: patient with best outcome first• Transplanting patients who will not survive is a waste Transplanting patients who will not survive is a waste
of a limited resourceof a limited resource
• Net benefit-concept: Balancing urgency and Net benefit-concept: Balancing urgency and outcome in allocationoutcome in allocation
UrgencyUrgency OutcomeOutcome

Balancing urgency and outcomeBalancing urgency and outcome“Transplant window“-concept“Transplant window“-concept
-> Increasing organ failure ->
Mortality
Med. TherapyTransplantation
benefit
“too early”
“too late”
“Transplantation window”

Organ exchange between the Organ exchange between the European Organ Exchange European Organ Exchange
Organizations (EOEO)Organizations (EOEO)

ScandiatransplantScandiatransplant
UK TransplantUK Transplant
AdB, FranceAdB, France
Swiss TransplantSwiss Transplant
LusotransplanteLusotransplante
ONT, SpainONT, Spain
EurotransplantEurotransplant
BalttransplantBalttransplant
PoltransplantPoltransplant
CzechtransplantCzechtransplant
HungarotransplantHungarotransplant
CNT, ItalyCNT, Italy
HNTO, GreeceHNTO, Greece
European organ exchange European organ exchange organizations (EOEO)organizations (EOEO)
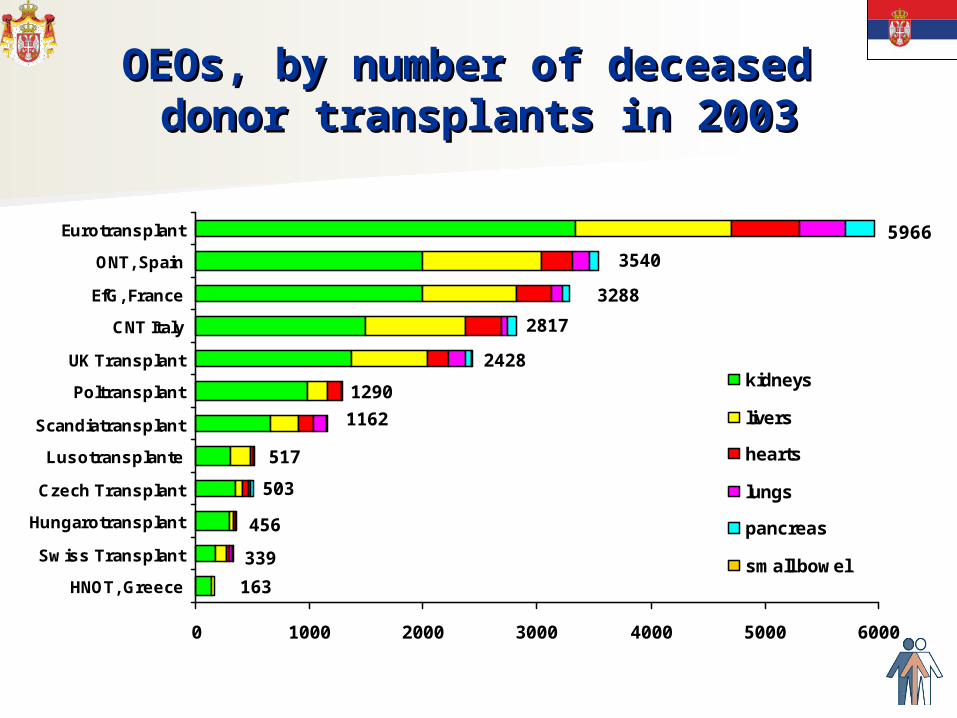
163
339
456
503
517
1162
1290
2428
2817
3288
3540
0 1000 2000 3000 4000 5000 6000
HNOT, Greece
Swiss Transplant
Hungarotransplant
Czech Transplant
Lusotransplante
Scandiatransplant
Poltransplant
UK Transplant
CNT Italy
EfG, France
ONT, Spain
Eurotransplant
kidneys
livers
hearts
lungs
pancreas
small bowel
5966
OEOs, by number of deceased OEOs, by number of deceased donor transplants in 2003donor transplants in 2003

Organ allocationOrgan allocation
Offering to other Organ Exchange Organizations
Allocation within the own country /
Organ Exchange Organization
No suitable recipient within
own country/OEO

Origin of donor organs transplanted in ETOrigin of donor organs transplanted in ET01.01.2001 – 31.12.200501.01.2001 – 31.12.2005

Organ offers from other OEO‘s to ETOrgan offers from other OEO‘s to ETKidney transplantation 2001-2005Kidney transplantation 2001-2005
(n = 207)(n = 207)
HCV pos39%
HBSAg pos16%
< 8 years21%
> 65 years12%
BG AB6%
Other6%

Principles of organ exchange Principles of organ exchange between EOEOsbetween EOEOs
• Organ exchange between European OEO‘s is Organ exchange between European OEO‘s is mainly „mainly „donor-drivendonor-driven“: “:
• Donor organ exchange only if no suitable Donor organ exchange only if no suitable recipient for this donor is available in donor recipient for this donor is available in donor countrycountry• Difficult to allocate donorDifficult to allocate donor
• Extended criteria donor (ECD)Extended criteria donor (ECD)• Rare blood group, size or ageRare blood group, size or age
• -> Reduction of loss of donor organs-> Reduction of loss of donor organs• -> No balancing of exchanged donor organs-> No balancing of exchanged donor organs
• Main benefit for countries/EOEOs with Main benefit for countries/EOEOs with • Large waiting listLarge waiting list• Liberal organ acceptance policyLiberal organ acceptance policy

Principles of organ exchange within ETPrinciples of organ exchange within ET
• Organ exchange within the Eurotransplant Organ exchange within the Eurotransplant area is also area is also „recipient driven“:„recipient driven“:
• DonorDonor organ exchange for special patient organ exchange for special patient groups and medical reasonsgroups and medical reasons• High urgent patientsHigh urgent patients• Immunized patientsImmunized patients• Pediatric patients etc.Pediatric patients etc.
• -> Supports special patient groups / -> Supports special patient groups / improves outcomeimproves outcome
• -> Optimization of donor organ usage-> Optimization of donor organ usage

Origin of donor organs transplanted in ETOrigin of donor organs transplanted in ET01.01.2001 – 31.12.200501.01.2001 – 31.12.2005

Principles of organ exchange within ETPrinciples of organ exchange within ET
• Solidarity principle between Eurotransplant Solidarity principle between Eurotransplant member countriesmember countries
• Exchange when medically indicatedExchange when medically indicated• National, regional or local allocation when National, regional or local allocation when
possible and/or medically indicated (short possible and/or medically indicated (short ischemic time)ischemic time)• ET Senior programET Senior program• Extended criteria donor organsExtended criteria donor organs
• National balancing mechanisms National balancing mechanisms

Kidney allocationKidney allocation

Kidney waiting list and transplantsKidney waiting list and transplants Eurotransplant 1969 - 2007Eurotransplant 1969 - 2007
11308
3703
1032

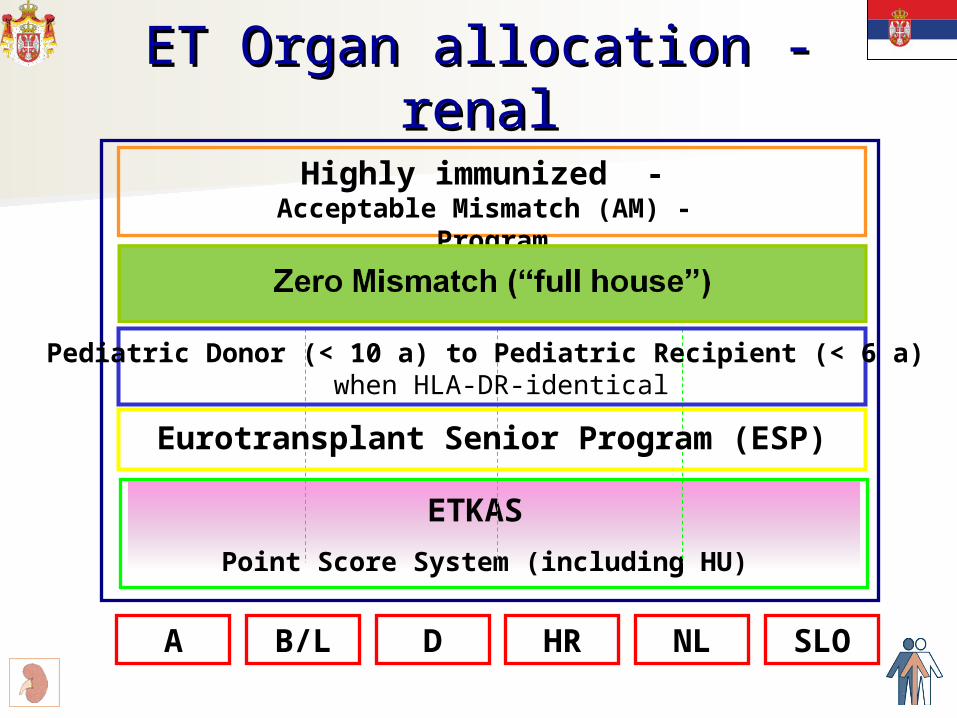
ET Organ allocation - renalET Organ allocation - renal
Highly immunized - Acceptable Mismatch (AM) - Program
Zero Mismatch (“full house”)
ETKAS Point Score System (including HU)
A
Pediatric Donor (< 10 a) to Pediatric Recipient (< 6 a) when HLA-DR-identical
Eurotransplant Senior Program (ESP)
B/L D HR NL SLO

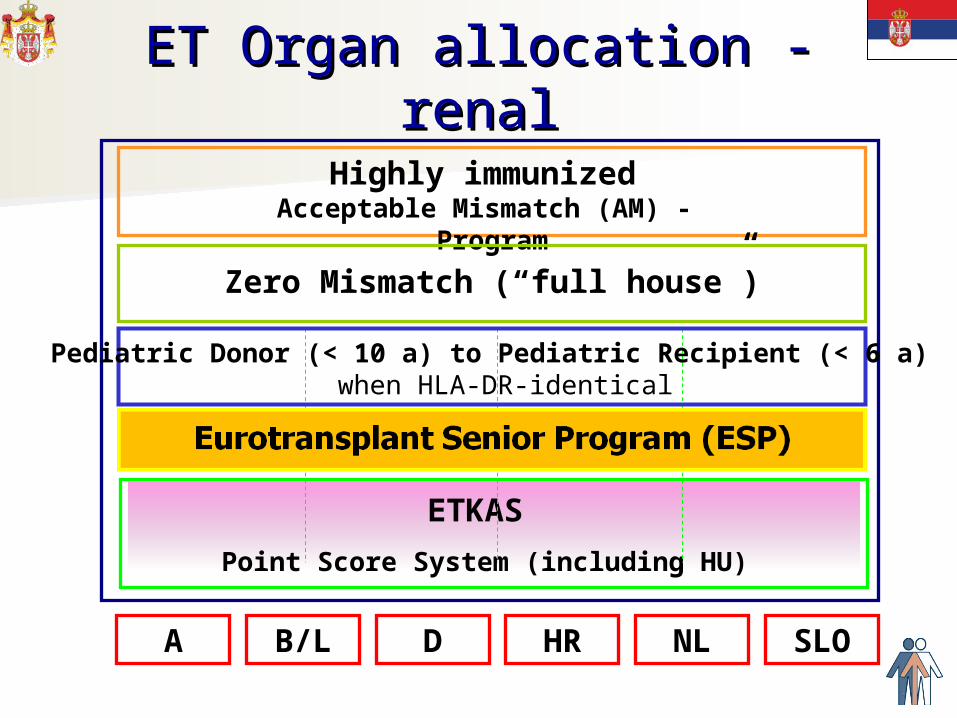
ET Organ allocation - renalET Organ allocation - renal
Zero Mismatch (“full house”)
ETKAS
Point Score System (including HU)
A
Pediatric Donor (< 10 a) to Pediatric Recipient (< 6 a) when HLA-DR-identical
Eurotransplant Senior Program (ESP)
B/L D HR NL SLO

Chance of every Chance of every newnew highly sensitized patient to receive a highly sensitized patient to receive a suitable crossmatch negative organ within 12 months suitable crossmatch negative organ within 12 months
(real life data)(real life data)
11
43
0
20
40
60Offer[%]
Standard allocation
AM

Claas et al. Transplantation, 2004
ET Organ allocation - renalET Organ allocation - renal
Highly immunized - Acceptable Mismatch (AM) - Program
ETKAS
Point Score System (including HU)
A
Pediatric Donor (< 10 a) to Pediatric Recipient (< 6 a) when HLA-DR-identical
Eurotransplant Senior Program (ESP)
B/L D HR NL SLO

Role of HLA-matching for graft survivalRole of HLA-matching for graft survivalafter kidney transplantationafter kidney transplantation
CTS Newsletter 2004:1CTS Newsletter 2004:1
6.2 yrs.difference

Influence of HLA-A,B,DR matching Influence of HLA-A,B,DR matching for primary transplant on subsequent for primary transplant on subsequent
sensitization (CDC)sensitization (CDC)
0
20
40
60
80
100
Before 0 MM 1 MM 2 MM 3 MM 4 MM 5 MM 6 MM
T [<6% PRA] I [6-84 % PRA] HS [>84% PRA]
%

100%100%1007310073totaltotal0,4%0,4%4444662,4 %2,4 %2442445510,5 %10,5 %105510554430,2%30,2%304330433326,6 %26,6 %2679267922
83283211
2176217600
PercentagPercentagee
No. of No. of transplantationtransplantation
ss
No. of No. of mismatchesmismatches
HLA-matching in kidney transplantationHLA-matching in kidney transplantationET 2000-2004, non-ESP patientsET 2000-2004, non-ESP patients
8,3 %8,3 %
21,6 %21,6 %

ET Organ allocation - renalET Organ allocation - renal
Highly immunized - Acceptable Mismatch (AM) - Program
Zero Mismatch (“full house”)
ETKAS
Point Score System (including HU)
A
Eurotransplant Senior Program (ESP)
B/L D HR NL SLO

High Urgency : 500 points extra
Pediatric Patients : double points for sharing of the HLA-antigens with the donor
0 - 5 years : 1095 extra waiting days i.e. 99 points
6 - 10 years : 365 extra waiting days i.e. 33 points
11 - 16 years : 730 extra waiting days i.e. 66 points
ETKAS - Pediatric allocation factorsETKAS - Pediatric allocation factors

Probability of receiving a kidney transplantProbability of receiving a kidney transplantET, Registration WL 01.01.1999 – 31.12.2000ET, Registration WL 01.01.1999 – 31.12.2000
0
20
40
60
80
100
0 1 2 3 4 5
%
<6 a (N=134)
6-10 a (N=108)
11-16 a (N=192)
16-64 a (N=10829)
>65 a (N=1054)
Waiting time (yrs)
Recipient age

Mortality on the kidney waiting listMortality on the kidney waiting listET, Registration WL 01.01.1999 – 31.12.2000ET, Registration WL 01.01.1999 – 31.12.2000
0
5
10
15
20
25
0 1 2 3 4 5
Waiting time (years)
%
<6 a (N=134)
6-10 a (N=108)
11-16 a (N=192)
16-64 a (N=10829)
>65 a (N=1054)
Recipient age
ET Organ allocation - renalET Organ allocation - renal
Highly immunized Acceptable Mismatch (AM) - Program
Zero Mismatch (“full house”)
ETKAS
Point Score System (including HU)
A
Pediatric Donor (< 10 a) to Pediatric Recipient (< 6 a) when HLA-DR-identical
B/L D HR NL SLO

Development in organ donation for different donor age groups
Reported kidney donors, Eurotransplant, 2000-2006
0
50
100
150
200
250
2000 2001 2002 2003 2004 2005 2006
Year
0-15
16-54
55-64
65 and up
Donor agegroups
Nu
mb
er
of
don
ors
(in
rela
tion
to 2
00
0)

Eurotransplant Senior Program (ESP)Eurotransplant Senior Program (ESP)RationaleRationale
• HLA-matching probably less important in HLA-matching probably less important in older recipients older recipients • Reduced risk of repeated re-transplantationReduced risk of repeated re-transplantation• Older patients might be less prone to rejection Older patients might be less prone to rejection
after transplantationafter transplantation
• Short ischemic time might reduce risk of Short ischemic time might reduce risk of graft loss from older donorsgraft loss from older donors
• For older recipients shorter waiting time For older recipients shorter waiting time might be especially importantmight be especially important

Eurotransplant Senior Program (ESP)Eurotransplant Senior Program (ESP)Practical implementationPractical implementation
• Priority allocation for kidneys Priority allocation for kidneys from donors over age 65 years from donors over age 65 years to recipients over age 65 years to recipients over age 65 years -> -> “old for old” program“old for old” program
• First transplantFirst transplant
• No HLA-matchingNo HLA-matching
• Regional allocationRegional allocation• Short ischemic timeShort ischemic time

Kidney discard rate by donor age:Kidney discard rate by donor age:US vs. Eurotransplant US vs. Eurotransplant
0102030405060
3 9 18 50 55 60 6566+Donor Age
Perc
en
t D
iscard
ed
EurotransplantUS

Patient survival for ESP patients vs. controlPatient survival for ESP patients vs. controlEurotransplant, 1999-2004Eurotransplant, 1999-2004
Frei et al.. AJT 2007; 7:1-8
= ETKAS 60-64 y

ET organ allocation - renalET organ allocation - renal
Highly immunized - Acceptable Mismatch (AM) - Program
Zero Mismatch (“full house”)
ETKAS
Point Score System (including HU)
A
Pediatric Donor (< 10 a) to Pediatric Recipient (< 6 a) when HLA-DR-identical
Eurotransplant Senior Program (ESP)
B/L D HR NL SLO

ETKAS allocation factorsETKAS allocation factors
Min Max
HLA-A, B, DR Mismatch 0 400
Mismatch Probability 0 100
Waiting time
Distance Donor / Transplant Center
National Import / Export Balance 0
balance dependent
0.09 points per day = 33 points per year
0 - 100 - 200 - 300

International organ exchange in International organ exchange in kidney transplantationkidney transplantation
Impact for selected patient groupsImpact for selected patient groupsEurotransplant 01.01.2002 -31.12.2006 Eurotransplant 01.01.2002 -31.12.2006
0%
20%
40%
60%
80%
100%
Outside ET 0 1 0 0 44
Other ET country 121 1022 141 87 1422
Recipient country 60 1420 336 271 9106
Highly immunized
000- HLA MM
PaediatricHigh
UrgencyOther

Impact of kidney organ exchange on Impact of kidney organ exchange on special patient groupsspecial patient groupsBelgiumBelgium, 01.01.2001 - 31.12.2005, 01.01.2001 - 31.12.2005
0%
20%
40%
60%
80%
100%
outside ET 0 1 0 0 5
other ET country 11 129 5 37 418
own country 3 64 3 22 1176
Highly Immunized
000- HLA MM
High Urgency
Children other

Non-renal organsNon-renal organs

Organ allocationOrgan allocation
International HU
(Accepted) Combined Organs
Elective
Elective
Elective
Elective
Elective
Other Organ Exchange Organizations
National HU National HU National HU National HU
Eu
rotr
an
sp
lan
t

Liver allocationLiver allocation

Liver waiting list and transplantsLiver waiting list and transplantsEurotransplant 1995 – 2008Eurotransplant 1995 – 2008
2442

ET Organ allocation – LiverET Organ allocation – Liver
International HU
Accepted combined organs (ACO)
Elective (labMELD)
A, Sl G, Cr NLB
Elective
center-oriented
allocation
Elective
MatchMELD
(labMELDSE, NSE)
Elective
MatchMELD
(labMELDSE, (NSE))
Elective
MatchMELD
(labMELDSE, NSE)PediatricMELD

n=201 (16%) n=1053 (84%)
Waiting time HU liver-transplantWaiting time HU liver-transplantFirst HU liver-tx [n=1254]First HU liver-tx [n=1254]
Pediatric (<16 yrs) Adult (16+ yrs)
Median waiting time: 2 d (both groups)
819
39
191
4
0-2 d 3-4 d
5-8 d 9-16 d
128
4
3
27
39
0-2 d 3-4 d 5-8 d
9-16 d 16+ d

Probability of dying on the liver waiting list Probability of dying on the liver waiting list
or removal due to clinical deterioration or removal due to clinical deterioration Elective liver-tx candidates, ET Jan 2002 – Jun 2009 Elective liver-tx candidates, ET Jan 2002 – Jun 2009

Thoracic organ allocationThoracic organ allocation

Heart waiting list and transplantsHeart waiting list and transplantsEurotransplant 1995 - 2007Eurotransplant 1995 - 2007
732 759 782 759 702623 596 580 570 542 555 577
553
0
300
600
900
1200
Active waiting list Heart transplants
959

Lung waiting list and transplantsLung waiting list and transplantsEurotransplant 1995 - 2007Eurotransplant 1995 - 2007
465 506
228
451
154 155242 258 272
125
358 378419
0100200300400500600700800900
Active waiting list Lung (s+d) transplants
856

Thoracic allocation rulesThoracic allocation rulesEurotransplantEurotransplant
• Three active urgency groupsThree active urgency groups• High urgentHigh urgent• UrgentUrgent• Transplantable = electiveTransplantable = elective
• Uniform „international“ HU-rulesUniform „international“ HU-rules+ separate national HU-rules+ separate national HU-rules
• Organ exchange with national balancing Organ exchange with national balancing within different urgency tierswithin different urgency tiers

New member countriesNew member countries--
PrerequisitesPrerequisites

Legal prerequisites for new Legal prerequisites for new ET member countriesET member countries
• Non-commercialization of organ donation Non-commercialization of organ donation • Brain death definition and diagnostic procedures Brain death definition and diagnostic procedures • Accreditation of transplant centersAccreditation of transplant centers• Data safety and protection principles / legislationData safety and protection principles / legislation
• Collection and delivery of transplant follow-up data to Collection and delivery of transplant follow-up data to improve organ allocation improve organ allocation
• Legislation allowing organ exchange with ET Legislation allowing organ exchange with ET partner countries based on commonly agreed ET partner countries based on commonly agreed ET allocation principlesallocation principles
• Adherence to EU standards on organ Adherence to EU standards on organ transplantation (EU directive)transplantation (EU directive)
Logistical prerequisites for new Logistical prerequisites for new ET member countriesET member countries
• 24/7 duty for organ procurement, organ 24/7 duty for organ procurement, organ offering and HLA-typing and cross-matchingoffering and HLA-typing and cross-matching
• Clearly defined contact persons for ETClearly defined contact persons for ET• Official language inside ET is EnglishOfficial language inside ET is English
• Reporting of all donors to EurotransplantReporting of all donors to Eurotransplant• Standardized transport logisticsStandardized transport logistics
• Donor organsDonor organs• HLA seraHLA sera
• Defined responsibilities and contact Defined responsibilities and contact institutions for financial settlementsinstitutions for financial settlements• Registration and procurement costsRegistration and procurement costs

Medical prerequisites for new Medical prerequisites for new ET member countriesET member countries
• Standardized and qualified Standardized and qualified • Brain death definition and diagnostic Brain death definition and diagnostic
procedures procedures • Donor evaluation and pretreatmentDonor evaluation and pretreatment• Donor organ explantation by experienced Donor organ explantation by experienced
teamsteams• Donor organ packing and transportationDonor organ packing and transportation
• Accreditation of HLA-laboratory by Accreditation of HLA-laboratory by European Foundation for Immunogenetics European Foundation for Immunogenetics (EFI)(EFI)

15,6
20,2
24,8
14,412,3
18,6 17,8 17,8
1,30,0
5,0
10,0
15,0
20,0
25,0
30,0
ET A B G NL L SLO HR RS
PMPPMP
Organ donation – Eurotransplant andOrgan donation – Eurotransplant andRepublic of Serbia - 2008Republic of Serbia - 2008
Reducing the gap

Integration of Croatia into Integration of Croatia into EurotransplantEurotransplant

Cooperation ET – CroatiaCooperation ET – CroatiaStepwise ApproachStepwise Approach
• Partial membership for one yearPartial membership for one year
• Cooperation in the field of special patient Cooperation in the field of special patient groups (HU, AM, pediatrics)groups (HU, AM, pediatrics)
• Zero-national balanceZero-national balance
• All donors reportedAll donors reported
• Participation in the Organ Advisory Participation in the Organ Advisory CommitteesCommittees
• Aiming at full membership after one yearAiming at full membership after one year

Cooperation ET – CroatiaCooperation ET – CroatiaStepwise Approach IIStepwise Approach II
• HU liver program HU liver program
• Kidney acceptable mismatch programKidney acceptable mismatch program• Consecutive listing of all eligable highly Consecutive listing of all eligable highly
immunized patientsimmunized patients
• HU heart and HU kidneyHU heart and HU kidney
• Elective pediatric heart and liver Elective pediatric heart and liver transplantationtransplantation
• Full membershipFull membership

Organ Exchange with CroatiaOrgan Exchange with CroatiaKidney Transplantation 2007Kidney Transplantation 2007
Net-Import to Croatia:16 Kidneys

SummarySummary
• Collaboration offers mutual benefits to Collaboration offers mutual benefits to participating centers and countries, e.g.participating centers and countries, e.g.• Improved allocationImproved allocation
• Transparent patient oriented allocation Transparent patient oriented allocation • Zero mismatch 20%, high urgency patients…Zero mismatch 20%, high urgency patients…• Scientifically based evolution of allocation rules Scientifically based evolution of allocation rules
• Reduced loss of donor organsReduced loss of donor organs• Multinational scientific cooperationMultinational scientific cooperation
• Data registry accessible to participantsData registry accessible to participants

Thank you for your attention


















