Dyslpidemia Cme Com 25 May09
121
MANAGEMENT OF DYSLPIDEMIA IN FAMILY PRACTICE •
description
This presentation was presented by me in one of the CME programs, held in Comilla, Bangladesh on the 25th. May 2009.
Transcript of Dyslpidemia Cme Com 25 May09

MANAGEMENT OF DYSLPIDEMIAIN FAMILY PRACTICE
•

EARLY DETECTION
BY WHOM?

Family Physician
As a member of the patient’s family








KEY WORDS• NCEP ATPIII: National cholesterol
education program adult treatment panel III.
• ACC: American college of cardiology• AHA: American heart association• NHLBI: National heart lung blood institute• ADA: American diabetes association.• TLC: Therapeutic lifestyle change.

What is dyslipidemia?• Dyslipidemias are disorders of lipoprotein
metabolism including lipoprotein overproduction or deficiency.
• Most dyslipidemias are hyperlipoproteinemias may be manifested by high TC, high TG, high LDL-C & low HDL-C.
• Others dyslipidemias:• Hypolipoproteinemias• Miscellaneous lipid disorders.

Fats, Lipids & Lipoproteins
in
Clinical Lipidology

What is Lipid?• Lipids are broadly defined as any fat
soluble (lipophilic) naturally-occurring organic molecules:
• Fats, oils, waxes, cholesterols, sterols, fat soluble vitamins (A, D, E, K), FFA, monoglycerides, diglycerides, phospholipids and others.

DIETARY LIPID (major source of energy) COMPOSED OF
• MAINLY TRIGLYCERIDES (FAT) (95-99% of total lipid)
PLUS• MINOR AMOUNT OF OTHER LIPIDS 1. FATTY ACIDS 2. PHOSPHOLIPIDS 3. NON-GLYCERIDE COMPONENTS
(Carotinoids, vitamin A, D, E, K) 4. OTHERS (Sterols e.g. phytosterol &
cholesterol)

Dietary fat mainly composed of Triglyceride

DIETARY STEROLS
0.1-2% of total dietary fat.

LIPID METABOLISMTriglyceride
• Dietary lipid (TG) by the action of bile and pancreatic lipase form mono-glyceride and FFA, enter in to the enterocytes.
• In the enterocytes FFA again form triglycerides together with cholesterol, phospholipids & proteins form chylomicrons, go to blood stream via lymph.
• In the capillaries chylomicrons break down into FFA, go for fuel or storage in the adipose tissue.
• Remnants go to the liver.


LIPIDS-lipophilic
LIPOPROTEINS- Hydrophilic


Lipoprotein particle
• CORE: contains Triglyceride and esterified cholesterol.
• Outer shell: contains free cholesterol, phospholipids and apolipoproteins.

Four main types of lipoproteins
• Chylomicrons- carry triglyceride from intestine to liver, skeletal muscle and adipose tissue. Chylomicrons are triglyceride rich lipoproteins appear in the blood after fat containing meal.
• Very low density lipoproteins (VLDL) - carry synthesized triglycerides from liver to adipose tissue. VLDL is triglyceride rich lipoprotein contains 10-15% of total serum cholesterol.

Four main types of lipoproteins
• Low density lipoproteins (LDL) - carry cholesterol from liver to cells. It is referred to as the “bad cholesterol” lipoproteins. 60-70% of total serum cholesterol contains in LDL.
• High density lipoproteins (HDL) – collect cholesterol from the tissue back to the liver (RCT). It is referred to as the “good cholesterol” lipoproteins. HDL carry 20-30% of total serum cholesterol

Contents of lipoprotein particles

Patient Visit-1
• 58 year old man came to your chamber with only complaint FREQUENT TIREDNESS.
• He is hypertensive for 2 years but controlled with ACEI.
• No history of tobacco or alcohol.
• Medication: Ramipril 10mg/day, ASA 75mg/day.

Visit-1 cont’d
• Office executive and physically inactive.
• Family history:• Mother had T2DM, HTN, CHD, died from
stroke at 72.• Father had T2DM and died from MI at 70.• Sister: 62 years old, Diabetic (T2DM)• Only daughter: 30 years old. Healthy.

Visit-1 cont’d(Physical examination)
• Height: 69 inches• Weight: 244 lbs.• Waist: 105 cm • BMI: 36kg/M2• BP: 119/78mmHg• Pulse rate: 89/m• Respiration: 19/m• No other abnormalities found.

Visit-1 cont’d
• Only complaint FREQUENT TIREDNESS with the above physical findings (F/H, HTN, high BMI) what is the most likely diagnosis?
• 1. Type 2 diabetes?
• 2. Dyslipidemia?
• 3. Metabolic syndrome (MS)?

Visit-1 cont’d
• Type 2 diabetes?
• This may be one of the correct answers.
• 2008 ADA guideline:
• Test an adult person for prediabetes or diabetes if he or she has BMI equal or >25, HTN and has T2DM in first degree relative.

Visit-1 cont’d
• Dyslipidemia?
• This is also one of the correct answers:
• Patient is obese and physically inactive.

Visit-1 cont’d
• Metabolic Syndrome (MSI)?• It may also a correct answer:
• NCEP ATPIII guideline: Waist plus any two of the following confirm Dx. Of MSI.
• Waist >102cm (for asian >90cm >80cm)• BP >130/>85mmHg or controlled with drug• TG>150mg/dl • HDL-C <40mg/dl(M),<50mg/dl(F)• FBG: >100mg/dl

Visit-1 cont’d
•WHAT ARE THE NEXT LABORATORY TESTS REQUIRED?

Visit-1 cont’d
• FBG: 120mg/dl (Pre-diabetes)• (FBG:100-125mg/dl=IFG, OGTT:140-
199mg/dl=IGT)• TC: 241mg/dl• HDL-C: 33mg/dl• LDL-C: 155mg/dl• TG: 243mg/dl• ECG, LFT, Renal functions are normal.

Visit-1 cont’d
• What is the diagnosis?
• T2DM?......NO• (He has prediabetes or IFG)• Metabolic syndrome (MSI)?...YES• (He has all 5 criteria for MS)• Dyslipidemia?....YES.• (Dyslipidemia :Lipid triad:High TG, high LDL-C
and low HDL-C called atherogenic dyslipidemia)

Visit-1 cont’d
• What other laboratory tests should be done for this patient to find additional risk factor for CVD?
• NHLBI/AHA identifies two aspects in patients with MSI to find risk factors for CVD.
• 1. Pro-inflammatory marker CRP• 2. Prothrombotic state: high fibrinogen and
plasminogen activator inhibitor1 (PAI-1)

Visit-1 cont’d
• Our patient has:• 1. Metabolic syndrome• 2. Atherogenic dyslipidemia• 3. Pre-diabetes.• What we have to do now?• -Start Thiazolidinedions (TZDs)?• -Calorie reduction and physical activity?• -Any other drug therapy?

Visit-1 cont’d
• Start thazolidinedions (TZDs)?• NO• WHY?
• TZDs are glucose lowering drug act by reducing insulin resistance. Although our patient needs to reduce insulin resistance at this moment but rosiglitazone found to increase CVD incidences. Pioglitazone leads to water retention, edema and increase in weight. So we should not start TZD.

Visit-1 cont’d
• Calorie reduction and physical activity?• YES:• Weight loss and physical activity are the
FIRST LINE treatment in patients with MSI. Moderate reduction in calorie intake (500-1000 calorie/day) and regular walking of 30 min/day with a goal of reducing body weight up to 10% in next 6 months.

Visit-1 cont’d
• Any other drug therapy?• NO.• The AHA/NHLBI/ADA guidelines recommend
that lifestyle modifications focusing on weight loss, smoking cessation, dietary patterns that reduce intake of saturated fat, trans-fat, cholesterol, and simple sugars, while increasing intake of fruits, vegetables, and whole grains, and increasing physical activity are first-line therapies to improve the lipid profile in patients with the metabolic syndrome.

DYSLIPIDEMIA RISK ASSESSMENT
• Major risk factors:• Smoking, • Physical inactivity, • Atherogenic diet, • HTN, • Low HDL-C, • established CHD, Family history of premature CHD,
cerebrovascular disease, or PAD. CKD, • DM, • Age ( men >45, women >55) • HDL >60 is a negative risk factor and its presence
removes one risk factor from the count.)

Framingham Risk Score
• Include the following factors:• Age• Gender• Total Cholesterol• HDL-C• Smoker• Systolic blood pressure• Any anti-hypertensive medications

To estimate
10 year risk of death from CAD or non-fatal Myocardial infarction

Risk categories:
• Very high risk: with 2 or more major risk factors, in whom the 10 year risk of death (Framingham risk score) from CAD or non fatal myocardial infarction is 20% or higher.
• Patients with CVD+ACS with DM with MSI with high BP and smokers.

Risk categories:• High Risk: ( 10 years risk, 20% or higher)• Patients with CVD or DM or CVD equivalent.
• Moderate or intermediate high risk: • with a 10 year risk is greater than 10% but less than 20%.
• Moderate risk:• With a 10 years risk < 10%
• Low risk:• Those with zero or 1 risk factor

What is the risk of our patient?
• Framingham Risk score table shows that his 10 years risk for CHD is 13%.
• So, our patient now is in moderately high risk.

Visit-1 cont’d
• Therapeutic lifestyle change advised:
• Diet restriction.• Daily physical activity e.g.
walking 30 min each day of the week.
• (ADA recommend 150min walking/week)

Visit-2(after 3 months)
• At visit-1
• TC: 241mg/dl• HDL-C:
33mg/dl• LDL-C:
155mg/dl• TG: 243mg/dl
After 6 weeks of TLC
• TC: 237mg/dl• HDL-C:
35mg/dl• LDL-C:
150mg/dl• TG: 259mg/dl

Visit-2 cont’d
We need drug treatment now.
•How to treat dyslipidemia in our patient?

Visit-2 cont’d
• After Therapeutic Lifestyle change (TLC) according to NCEP ATPIII guideline which of the lipid parameters should be targeted first to reduce risk of CVD?
• 1. Total Cholesterol?
• 2. LDL-C?
• 3. TG and HDL-C?

Visit-2 cont’d
• Total cholesterol?...NO
• TG and HDL-C?....NO
• LDL-C?...YES

Visit-2 cont’d(explanation)
• According to NCEP ATPIII primary target of lipid lowering therapy is LDL-C.
• Once LDL-C target met, secondary target is non-HDL-C if TG equal or >200mg/dl.
• Non-HDL-C goal is 30mg/dl above LDL-C.
• Non-HDL-C= TC-HDL-C (LDL-C+VLDL).
• Our patient’s LDL-C target is <130mg/dl with optional target <100mg/dl.


DO REMEMBER!
•IRRESPECTIVE OF RISK CATEGORIES LDL-C >100mg/dl IS ALWAYS ATHEROGENIC!

Drugs used in lipid lowering therapy
• Five classes of lipid lowering drugs are available:
• 1. STATINS (mainly reduce LDL-C upto 55%))
• 2. BILE ACID SEQUESTRANTS: (reduce LDL-C up to 25%)
• 3. FIBRIC ACIDS (reduce TG up to 50%)• 4. NICOTINIC ACID (raises HDL-C up to
35% )• 5. CHOLEASTEROL ABSORPTION
INHIBITORS

Visit-2 cont’d
• What is the next step for our patient to improve his lipid profile?
• 1. Prescribe a statin?
• 2. Prescribe a fibrate?
• 3. Prescribe Nicotinic acid?

Visit-2 cont’d
• 1. Prescribe a statin?.......YES
• 2. Prescribe a fibrate?....NO
• 3. Prescribe Nicotinic acid?...NO

Visit-2 cont’d(prescribe a statin-explanation)
• Statin reduces LDL-C up to 55%. Fibrate or nicotinic acid lower LDL-C up to 20%.
• LDL-C 150mg/dl. So our primary target to reduce LDL-C and statin is the best option.
• He has TG: 259mg/dl and HDL-C: 35mg/dl.• Atorvastatin 20mg/day prescribed and next
follow up after 3 months.• If TLC and statin do not improve his lipid
parameters, along with statin fibrate or nicotinic acid is recommended.

Visit-2 cont’d
•Any other advices to patient?

Do not forget about statin side effects!
• TWO MAJOR ADVERSE EFFECTS OF STATINS:
• MYOTOXICITY
• HEPATOTOXICITY

Do not forget about statin side effects!
• Before statin prescription, physician should have the baseline level of the following laboratory tests:
• 1. CPK• 2. SGPT and SGOT both.• Patient should be advised to report any muscle pain.
If follow up shows CPK >10 times of the upper limit of normal, statin should be discontinued.
• For any GI complaint if transaminases >3 times of the upper limit of the normal, statin should be discontinued.

Visit-3 (after 6 months)
• 3 months back
• TC: 237mg/dl• HDL-C: 35mg/dl• LDL-C: 150mg/dl• TG: 259mg/dl• FBG: 120mg/dl
• Waist: 106cm. BMI increased to 37kg/m2.
• FBG: 128mg/dl• Lipid Profile:• TC: 171mg/dl• HDL-C: 37mg/dl• LDL-C: 90mg/dl• TG: 220mg/dl• Non-HDL-C: 134mg/dl• Our patient is already
diabetic.

Visit-3 cont’d
• Although LDL-C target met but high TG and low HDL-C are also risk factors for CVD.
• ADA: TG: <150mg/dl• HDL-C: >40mg/dl for male and >50mg/dl for
female.• NCEP ATPIII: If TG 200-499mg/dl, secondary
target is non-HDL-C with goal <130mg/dl. • Our patients value 134mg/dl.• WHAT TO DO NEXT?

Visit-3 Cont’d
• Add Metformin?
• Increase statin dose?
• Add fibrate or Nicotinic acid?

Visit-3 Cont’d
• 1. Add metformin?..............YES.• (ADA: at the time of Dx. of T2DM, metformin is
the best option along with TLC)• 2. Increase statin dose?.........NO.• (Increased statin dose will not work on TG and
HDL-C)• 3. Add fibrate or nicotinic acid?.........YES.• (Very good option)

Visit-3 cont’d(Fibrate or nicotinic acid)
• ADA/NCEP ATPIII: Combination with statin and fibrate or nicotinic acid is the best option in reducing TG and increasing HDL-C.
• Avoid gemfibrozil. Both statin (Atorvastatin, simvastatin & lovastatin) and gemfibrozil are metabolized through P450 (CYP3A4) and may increase side effects of statins.

Visit-3 con’d
• Prescribed:
• 1. Metformin 850mg twice daily
• 2. Atorvastatin 20mg daily
• 3. Nicotinic acid ER 500mg at bed time and increased dose up to 1g after 1 month.

Why nicotinic acid?+ Statin as mono-therapy reduces CVD events by 30% but along
with nicotinic acid, reduction of CVD is approx. 75%.
• + Nicotinic acid slows the progression of atherosclerosis in patients with CAD by reducing TG, Lp(a) and increasing HDL-C (21%)
• Confirmed by CIMT.
• Ref: ARBITER (Arterial Biology for the Investigation of the Treatment effects of Reducing Cholesterol) 2 and HATS (HDL-Atherosclerosis Treatment Study) trials.

Visit-4After 9 months
• FBG: 91mg/dl
• TC: 148mg/dl
• HDL-C: 45mg/dl
• LDL-C: 77mg/dl
• TG: 141mg/dl
• Non-HDL-C: 103mg/dl.

Hyperlipidemia (Secondary causes)
• Physical Inactivity• Atherogenic diet
• Diabetes, • Hypothyroidism, • Obesity, • Smoking, • Nephrotic syndrome, • Obstructive liver disease, • Alcoholism, • Menopause, • Puberty (in male), • Use of drugs like anabolic steroids, progestins, estrogens.

Dyslipidemia(Genetic causes)
• Fredrickson Classification
• Type I: Familial hyperchylomicronemia expressed as elevated chylomicrons.
• Type IIa: Familial hypercholesterolemia characterized by elevated LDL-C only.
• Type IIb: Familial combined hyperlipidemia characterized by elevated VLDL, LDL and triglycerides.
• Type III: Familial dysbetalipoproteinemia expressed as increased IDL.
• Type IV: Endogenous hyperlipemia characterized by increased VLDL
• Type V: Familial hypertriglyceridemia characterized by increased VLDL and chylomicrons

Visit-1
• Male, 45 years of age came to your office for medical check up.
• No complaint.• Smoker-half a pack/day.• Physically inactive.• Father died from MI at 49.• Physical examination: BP: 140/90mmHg• BMI: 31kg/m2

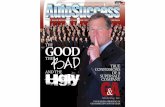
Skin: Yellow patches under his eyes (Xanthoma)

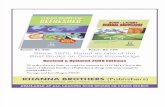
Skin: Yellow patches on the palmar surface of hands (Xanthoma)

What is the most likely Dx?
• 1. Isolated hypertriglyceridemia ?
• 2. Familial hypercholesterolemia ?

Isolated hypertriglyceridemia?NO
• Isolated hypertriglyceridemia does not lead to such lipid deposits.
• Severe hypertriglyceridemia leads to another type of xanthoma called eruptive xanthomas - papular lesions.


Most likely diagnosis is Familial Hypercholesterolemia.
• 1. Family history of premature coronary artery disease .
2. Xanthomas below eyes.
3. Yellow patches (xanthomas) in the palmar creases.

What is the initial screening test required for this patient?
• 1. Lipoprotein electrophoresis.• (Lipoprotein Electrophoresis is more authentic
but this procedure is not widely available and more costly.)
• 2. Fasting lipid profile which includes total cholesterol, HDL, LDL and triglyceride.
• (NCEP/ATP III: the best initial screening test to evaluate for the presence of dyslipidemia is a fasting lipid profile for all individuals of age 20 or older.)

Our patient’s fasting lipid profile
• Total Cholesterol: 355mg/dl
• HDL: 40mg/dl
• Triglyceride: 100mg/dl

Calculate LDL level by
Friedewald Equation

Friedewald Equation
• In mg/dl: LDL-C = Total cholesterol – HDL-C -(0.20XTriglyceride)
• In mmol/L: LDL-C = Total cholesterol – HDL-C- (0.45XTriglyceride)
• Conditions:
• Fasting for 12-14 hours.
• Triglyceride must be <400mg/dl

For this patient
355 – 40 – (0.20X100)= 295
LDL-C = 295mg/dl

According to Fredrickson Classification
Which type of dyslipidemia is it?

Familial hypercholesterolemia
• Expressed as very high LDL-C and low TG
• It is a genetic disorder due to deficiency of LDL receptors.

What is our next step?
• NCEP ATPIII: Patients without known heart disease and LDL-C >190mg/dl should be treated with high dose of statin or combination of lipid lowering drugs along with TLC.
• Framingham risk score found 17%
• What should be LDL-C target?...<100mg/dl

Patient was started atorvastatin 40mg/day.
• After 1 months his LDL-C came down to 131mg/dl.
What is our next step?1. Start fibrate?2. Start nicotinic acid?3. Start ezetimibe?4. Do nothing?

He is not in his target with high dose of statin.
• Target: <100mg/dl
• Ezetimibe works by inhibition of cholesterol absorption in the gut and has an excellent safety profile in combination with a statin.
• Ezetimibe 10mg/day started with statin.

After 6 months
• Patient informed you about his severe myalgia and and also informed that he has stopped statin and ezetimibe 15 days back after which his pain has relieved considerably.
• You went for his CPK and transaminases.• CPK found 11 times higher than upper limit of
the normal.• His TC: 320mg/dl, LDL-C: 200mg/dl.• ECG: Ischemic changes. ETT: positive.

What is our next step?
? ? ? ?

LIPID APHERESIS***

What is lipid apheresis?
• This is the process by which portion of the patient’s blood is taken out of the body, plasma is separated from the whole blood, selectively removed Apo B containing lipoproteins [LDL, Lp(a), & VLDL] then plasma and blood are recombined and returned back to the body.
• This process is indicated to the following high risk patients with:
• LDL-C equal or >300mg/dl or• LDL-C equal or >200mg/dl and documented coronary heart
disease (CHD)
• In case when TLC is ineffective and maximum drug therapy is either ineffective or not tolerated.

Ref: AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Vol. 122 No. 1 July 2008, pp. 198-208
(doi:10.1542/peds.2008-1349)

Cholesterol screening in the form of LIPID PROFILE is recommended for:
• -All children at the age of 2 years but not later than 10 years with family history of high cholesterol or heart disease.
• -All children whose family history is unknown.
• -All children with Obesity, HTN, DM.

If values are normal, testing should be repeated in 3-5 years.
• If children are over weight or obese, with high TG, low HDL-C and/or high LDL-C:
• RECOMMENDATION:
• change in diet and physical activity.

For the children of 8 years of age or above with high LDL-C:
• PHARMACOLOGICAL INTERVENTION INDICATED IF:
• LDL-C >190mg/dl OR• -LDL-C >160mg/dl with family history of
heart disease. OR• -LDL-C >130mg/dl if the child is Diabetic.
OR• -Children with Familial
hypercholesterolemia.

Pharmacological intervention with primary goal
<160mg/dl and gradually up to <110mg/dl

LIPID LOWERING DRUGS FOR CHILDREN
• Cholesterol absorption inhibitor (Ezetimibe), first line of treatment.
• Bile acid sequestrant.
• 4 statins are approved by FDA for children: pravastatin, atorvastatin, Lovastatin & simvastatin.

LDL-C OR LDL-P?
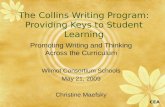
Risk of atherosclerosis is increased by the number of lipoprotein particles, not by the cholesterol they contain.



20+ years of studies:Patients with smaller LDL size have greater
CHD risk at any given level of LDL-C.
20+ years of studies:Patients with smaller LDL size have greater
CHD risk at any given level of LDL-C.
LDLCholesterol
Balance
130 mg/dL 130 mg/dL
Large LDL(Pattern A)
Small LDL(Pattern B)
Higher riskLower risk

20+ years of studies:Patients with smaller LDL size have greater
CHD risk at any given level of LDL-C.
20+ years of studies:Patients with smaller LDL size have greater
CHD risk at any given level of LDL-C.
LDLCholesterol
Balance
130 mg/dL 130 mg/dL
Large LDL(Pattern A)
Small LDL(Pattern B)
Higher riskLower risk
But they also have more particles!

Particle Uptake by Macrophage
Cholesterol Deposition;
Increased Plaque Burden
Particle Uptake by Macrophage
Cholesterol Deposition;
Increased Plaque Burden
Particle Movement into Intima
– Gradient driven
Particle Movement into Intima
– Gradient driven
Particle Oxidation Particle Oxidation
Adhesionmolecules MCP-1
Colony-stimulatingfactors
TissuefactorPAI-1
Endothelial cellscells
MonocyteMonocyte
Particle Retention
– Lipoprotein particle binding to proteoglycans
Particle Retention
– Lipoprotein particle binding to proteoglycans
Mildly modified LDL
Extensively modified LDL
“The rate of passive diffusion is increased when the circulating levels of LDL are elevated.” 1
“The rate of passive diffusion is increased when the circulating levels of LDL are elevated.” 1
Enhanced Endothelial Dysfunction
Enhanced Endothelial Dysfunction
1 Weissberg PL, Rudd JH. Textbook of Cardiovascular Medicine. 2002. p. 6.
LDL Particles Promote Atherogenesis
Lumen
Intima

NOT LDL-CBUT
LDL-P

Each of the atherogenic particles
• LDL, VLDL, IDL & Lp(a) contain one molecule of apolipoprotein B and the total Apo B concentration and/or non-fasting ApoB:ApoA-1 more specifically ApoB100:ApoA-1ratio is the better marker of any vascular event than LDL-C. (Ref: INTERHEART study, Lancet 2008 Jul 19; 372:224

NMR LipoProfile
• This test is done by NMR
LipoProfile via Nuclear Magnetic Resonance Spectroscopy.

DIABETIC DYSLIPIDEMIA
•The involvement of multiple risk factors (micro and macro vascular complications) in diabetes underlines the fact that it is a vascular disease along with metabolic.

DIABETIC DYSLIPIDEMIA
• Diabetic patients are tend to have
higher proportion of sd-LDL-P and this
is the reason why diabetic patients are
more prone to coronary events.

DIABETIC DYSLIPIDEMIA
•FOR THIS REASON:•Almost all adults with diabetes should be taking statins even if they have normal cholesterol levels and no evidences of heart diseases.
• Ref:BMJ 2004;328:1095 (8 May), doi:10.1136/bmj.328.7448.1095-a.

PRACTICE TIPS
• 1. Test for lipid profile after 9-12 hours of fasting.
• 2. Identify presence of atherosclerotic diseases:
• Clinical CHD• Symptomatic carotid artery disease,• PAD• Abdominal aortic aneurism• Diabetes mellitus.

PRACTICE TIPS
• 3. Determine the presence of risk factors.• 4. Assess risk category according to
Framingham risk table and establish LDL goal, need for TLC, determine the level of drug consideration.
• 4.Initiate TLC if LDL above goal.• Diet: Saturated fat <7% of calories,
cholesterol <200 mg/day.• Fiber 10-25g and plant stenol 2g per day.• Increase physical activity.

PRACTICE TIPS
• 5. Consider drug (statin) simultaneously with TLC for CHD and CHD equivalents.
• 6. Consider adding drug to TLC after 3 months for other risk categories.
• LDL is the primary target. Non-HDL is the secondary target
• 7. Identify metabolic syndrome and treat, if present.

PRACTICE TIPS
• 8. Treat elevated triglyceride:
• A. If TG 150-199mg/day, TLC.
• B. If 200-499mg/dl, intensify therapy with LDL-lowering drug, or add nicotinic acid or fibrate.
• C. If >500 treat it first to reduce risk of pancreatitis.

Lipid Profile analysis in risky patients
• LDL-C > 100mg/dl always atherogenic.
• TG:HDL-C >3.8 indicates presence of sd-LDL-P.
• LDL <70mg/dl (lower is better)• Non-HDL-C <100mg/dl• TC:HDL-C < 4 for women & < 5 for
men• LDL-C:HDL-C <2.5• TG:HDL-C <3.8

SOCRATES (469 BC - 399 BC)
• “Thou shouldst eat to live; not live to eat.”
• (You should eat to live; not live to eat)
• MODERN ERA
(You should live to eat; not eat to live)
• “