Dr. Mahmoud H. Taleb 1 Pharmacology II Lecture 3 Diuretics Dr. Mahmoud H. Taleb Assistant Professor...
31
Dr. Mahmoud H. Taleb Dr. Mahmoud H. Taleb 1 Pharmacology II Pharmacology II Lecture 3 Lecture 3 Diuretics Dr. Mahmoud H. Taleb Assistant Professor of Pharmacology and Toxicology Head of Department of Pharmacology and Medical Sciences, Faculty of Pharmacy- Al azhar University
-
Upload
miles-ellis -
Category
Documents
-
view
227 -
download
4
Transcript of Dr. Mahmoud H. Taleb 1 Pharmacology II Lecture 3 Diuretics Dr. Mahmoud H. Taleb Assistant Professor...

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 11
Pharmacology IIPharmacology II
Lecture 3Lecture 3
Diuretics
Dr. Mahmoud H. TalebAssistant Professor of Pharmacology and Toxicology
Head of Department of Pharmacology and Medical Sciences, Faculty of Pharmacy- Al azhar University

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 22
DiureticsDiureticsDiuretics are used to treat excessive water and Diuretics are used to treat excessive water and
sodium retention (edema states), hypertension, sodium retention (edema states), hypertension, and electrolyte disorders, e.g., hypokalemia. and electrolyte disorders, e.g., hypokalemia. These drugs are classified according to the These drugs are classified according to the renal tubular site of actionrenal tubular site of action. .
To understand the therapeutic and side effects of To understand the therapeutic and side effects of diuretics, it is important to review renal diuretics, it is important to review renal tubular function and the maintenance of tubular function and the maintenance of extracellular fluid and electrolyte homeostasis.extracellular fluid and electrolyte homeostasis.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 33
Normal Regulation of Fluid and Electrolytes by the Kidneys
Approximately 16 to 20 percent of the blood plasma entering the kidneys is filtered from the glomerular capillariesinto the Bowman's capsule. The filtrate, although normally free of proteins and blood cells, does contain mostlow-molecular-weight plasma components in approximately the same concentrations as are found in the plasma. These include glucose, sodium bicarbonate, amino acids, and other organic solutes as well as electrolytes, such asNa+, K+, and Cl-. The kidney regulates the ionic composition and volume of urine by the active reabsorption orsecretion of ions and/or the passive reabsorption of water at five functional zones along the nephron—namely, the proximal convoluted tubule, the descending loop of Henle, the ascending loop of Henle, the distal convoluted
tubule, and the collecting tubule and duct .
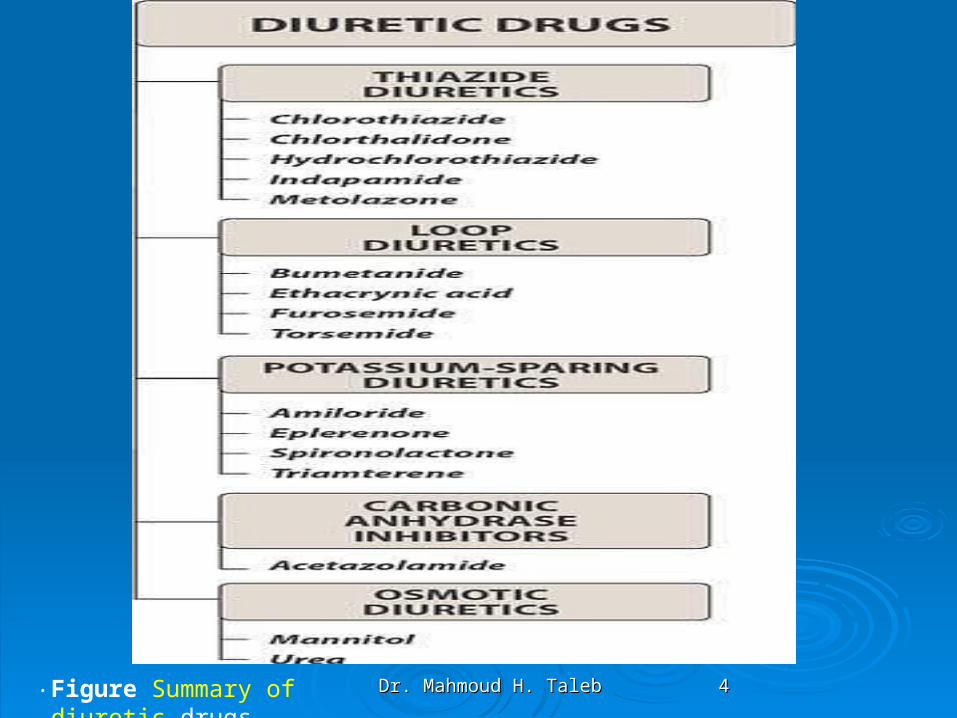
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 44.Figure Summary of diuretic drugs.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 55
REVIEW OF RENAL PHYSIOLOGYREVIEW OF RENAL PHYSIOLOGYThe kidney regulates sodium and water excretion to maintain The kidney regulates sodium and water excretion to maintain
extracellular fluid (ECF) volume within narrow limits despite extracellular fluid (ECF) volume within narrow limits despite an irregular and often excessive dietary intake of sodium. The an irregular and often excessive dietary intake of sodium. The filtered load of sodium first entering the nephron is equal to filtered load of sodium first entering the nephron is equal to the product of the glornerular filtration rate (GFR) and the the product of the glornerular filtration rate (GFR) and the plasma concentration of sodium. plasma concentration of sodium.
Sodium reabsorption occurs at four major sites along the Sodium reabsorption occurs at four major sites along the nephron: nephron: the proximal tubulethe proximal tubule, , the ascending limb of the loop the ascending limb of the loop of Henle,of Henle, the distal convoluted tubulethe distal convoluted tubule and and cortical collecting cortical collecting ductduct, and the medullary collecting duct . The first three , and the medullary collecting duct . The first three nephron segments each reabsorb at least two-thirds of the nephron segments each reabsorb at least two-thirds of the sodium chloride that is delivered to them. The bulk of sodium sodium chloride that is delivered to them. The bulk of sodium reabsorption occurs in the proximal tubule and loop of Henle, reabsorption occurs in the proximal tubule and loop of Henle, whereas the final amount of sodium excreted is dependent on whereas the final amount of sodium excreted is dependent on the fine-regulation at the distal sites.the fine-regulation at the distal sites.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 66
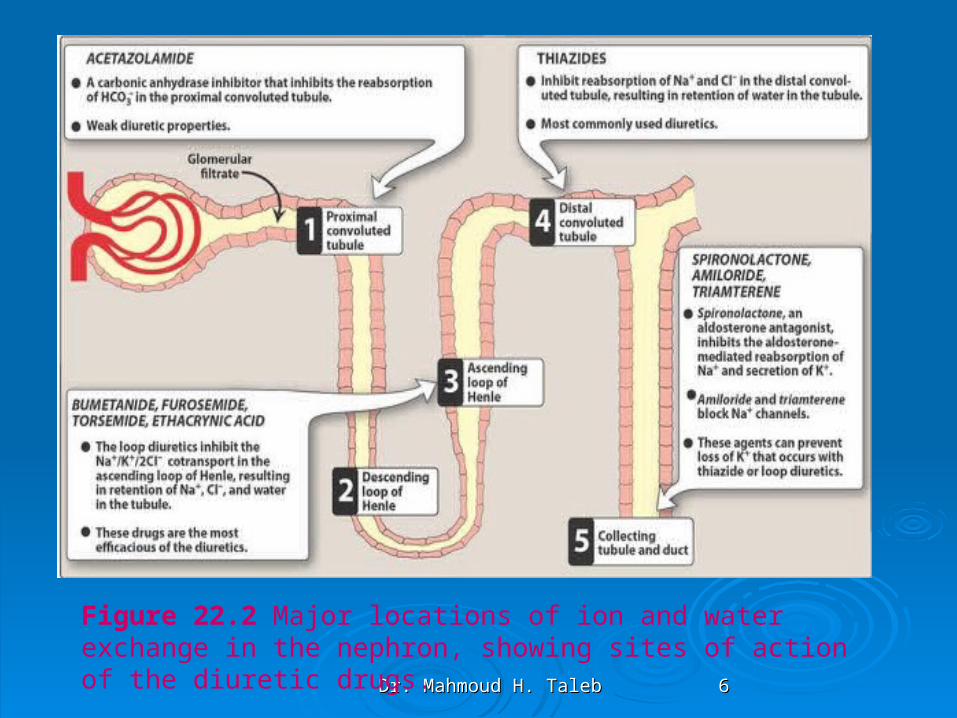
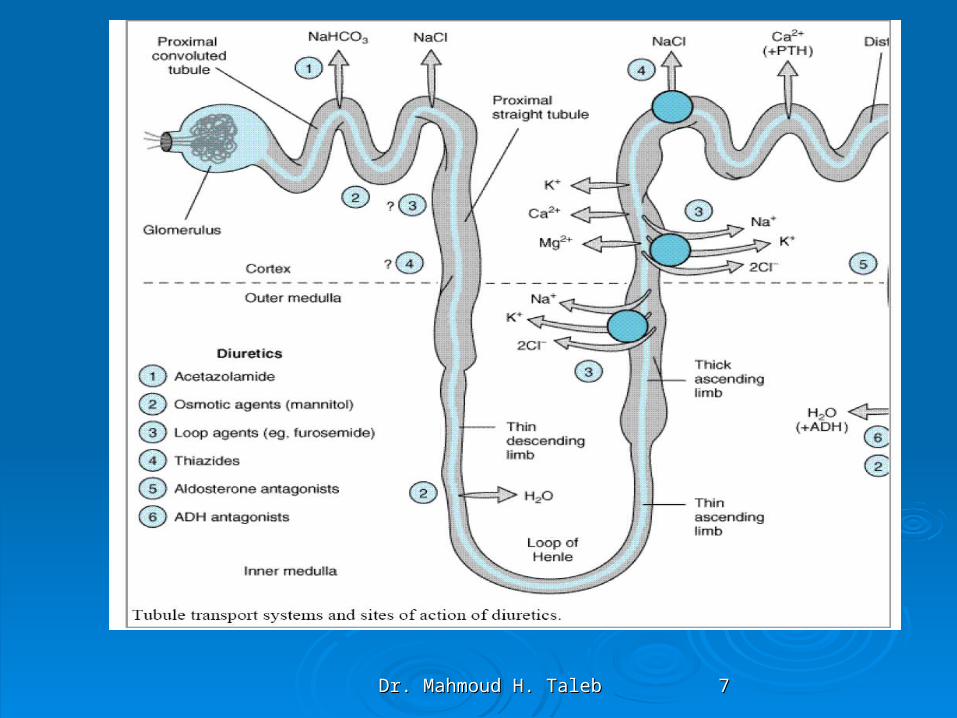
Figure 22.2 Major locations of ion and water exchange in the nephron, showing sites of action of the diuretic drugs.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 77
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 88
DIURETICSDIURETICS
Diuretics (saluretics) elicit increase production of urine (diuresis). In the strict sense, the term is applied to drugs with a direct renal action. The predominant action of such agents is to augment urine excretion by inhibiting the reabsorption of NaCl and water
Diuretic agents have been classified according to chemical Diuretic agents have been classified according to chemical structure and/or site of action. structure and/or site of action.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 99
11 - -Loop DiureticsLoop Diuretics
Mechanism and site of actionMechanism and site of actionThe loop diuretics directly inhibit the facilitated The loop diuretics directly inhibit the facilitated
chloride, sodium, potassium transport at the luminal chloride, sodium, potassium transport at the luminal membrane of the medullary segment of the thick membrane of the medullary segment of the thick ascending limb of Henle's loop.ascending limb of Henle's loop.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1010
PharmacokineticsPharmacokinetics
FurosemideFurosemide (Lasix, Furoside) is rapidly but incompletely absorbed from the (Lasix, Furoside) is rapidly but incompletely absorbed from the gastrointestinal tract. In the circulation, it is 93% protein-bound. Excretion gastrointestinal tract. In the circulation, it is 93% protein-bound. Excretion is primarily via proximal renal tubular secretion, at the organic-acid is primarily via proximal renal tubular secretion, at the organic-acid secretory site. As with most diuretics, renal tubular secretion of furosemide secretory site. As with most diuretics, renal tubular secretion of furosemide is necessary for pharmacological effect of the drug at the luminal is necessary for pharmacological effect of the drug at the luminal membrane.membrane.
Bumetanide Bumetanide (Burnex) is a sulfamoyl benzoic acid derivative like furosemide. (Burnex) is a sulfamoyl benzoic acid derivative like furosemide. It is almost completely absorbed from the gastrointestinal tract, reaching It is almost completely absorbed from the gastrointestinal tract, reaching peak blood concentrations within 30 minutes after an oral dose. In plasma, peak blood concentrations within 30 minutes after an oral dose. In plasma, it is 90% protein-bound. The drug is partially metabolized by the liver, but it is 90% protein-bound. The drug is partially metabolized by the liver, but more than 50% is excreted unchanged in the urine within 6 hours of more than 50% is excreted unchanged in the urine within 6 hours of administration.administration.
Ethacrynic acid Ethacrynic acid (RX Edecrin)(RX Edecrin) is well absorbed from the gastrointestinal tract, is well absorbed from the gastrointestinal tract, and in the circulation it is 97% protein-bound. It undergoes partial hepatic and in the circulation it is 97% protein-bound. It undergoes partial hepatic metabolism. The major portion is secreted via the proximal renal tubular metabolism. The major portion is secreted via the proximal renal tubular organic-acid transport sites and can then be reabsorbed at more distal organic-acid transport sites and can then be reabsorbed at more distal nephron sites via pH-dependent nonionic diffusion.nephron sites via pH-dependent nonionic diffusion.
Torsemide Torsemide (RX Demadex),(RX Demadex), is very well absorbed from the gastrointestinal is very well absorbed from the gastrointestinal tract and reaches peak plasma concentrations within 30 minutes. It is tract and reaches peak plasma concentrations within 30 minutes. It is largely metabolized by the liver, only 20% being excreted unchanged in largely metabolized by the liver, only 20% being excreted unchanged in the urine, so it is less likely than the other drugs in this group to the urine, so it is less likely than the other drugs in this group to accumulate on repeated administration in patients with impaired renal accumulate on repeated administration in patients with impaired renal function. It also has a longer half-life than the other agents of this class, so function. It also has a longer half-life than the other agents of this class, so once-daily administration is sufficient.once-daily administration is sufficient.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1111
Pharmacological effectsPharmacological effectsLoop diuretics are highly efficacious natriuretic Loop diuretics are highly efficacious natriuretic
agents that have the capacity to inhibit agents that have the capacity to inhibit reabsorption of up to 20-25% of the filtered reabsorption of up to 20-25% of the filtered sodium load. This efficacy is related to the sodium load. This efficacy is related to the relatively large magnitude of sodium chloride relatively large magnitude of sodium chloride transport occurring in this nephron segment transport occurring in this nephron segment and to efficiency of the chloride transport and to efficiency of the chloride transport blockade.blockade.
The kaliuresis observed with loop diuretics is The kaliuresis observed with loop diuretics is proportional to the increased rate of urine flow proportional to the increased rate of urine flow caused by these agents.caused by these agents.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1212
Adverse effects and toxicityAdverse effects and toxicityOtotoxicity: Hearing can be affected adversely by the loop diuretics,
particularly when used in conjunction with the aminoglycoside antibiotics. Permanent damage may result with continued treatment. Ethacrynic acid is the most likely to cause deafness. Vestibular function is less likely to be disturbed, but it, too, may be affected by combined treatment with the antibiotic.
Hyperuricemia: Furosemide and ethacrynic acid compete with uric acid for the renal and biliary secretory systems, thus blocking its secretion and, thereby, causing or exacerbating gouty attacks..
Acute hypovolemia: Loop diuretics can cause a severe and rapid reduction in blood volume, with the possibility of hypotension, shock, and cardiac arrhythmias. Hypercalcemia may occur under these conditions.
Potassium depletion: The heavy load of Na+ presented to the collecting tubule results in increased exchange of tubular Na+ for K+, with the possibility of inducing hypokalemia. The loss of K+ from cells in exchange for H+ leads to hypokalemic alkalosis. Potassium depletion can be averted by use of potassium-sparing diuretics or dietary supplementation with K+.
Hypomagnesemia: A combination of chronic use of loop diuretics and low dietary intake of Mg2+ can lead to hypomagnesemia, particularly in the elderly. This can be corrected by oral supplementation.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1313
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1414
Drug interactionsDrug interactionsThree major groups of drug interactions are well recognized with loop Three major groups of drug interactions are well recognized with loop
diuretics. The most recently described, and likely the most common, diuretics. The most recently described, and likely the most common, is the blunting of the natriuretic effect of loop diuretics by most is the blunting of the natriuretic effect of loop diuretics by most nonsteroidal anti-inflammatory agents. Inhibition of intrarenal nonsteroidal anti-inflammatory agents. Inhibition of intrarenal prostaglandin synthesis by the latter is purported to be the prostaglandin synthesis by the latter is purported to be the mechanism of this interaction.mechanism of this interaction.
Less frequently, these diuretics potentiate the ototoxicity of Less frequently, these diuretics potentiate the ototoxicity of aminoglycoside antibiotics and the nephrotoxicity of first-generation aminoglycoside antibiotics and the nephrotoxicity of first-generation cephalosporins (cepha-loridine, cephalothin).cephalosporins (cepha-loridine, cephalothin).
Drug interactions with other organic acids have been described and are Drug interactions with other organic acids have been described and are due to competition between drugs for the secretory transport due to competition between drugs for the secretory transport system. For example, probenecid, a uricosuric agent, delays the system. For example, probenecid, a uricosuric agent, delays the renal tubular secretion of the loop diuretics, thereby retarding their renal tubular secretion of the loop diuretics, thereby retarding their diuretic effect. High doses of furosemide have been reported to diuretic effect. High doses of furosemide have been reported to delay the excretion of tubocurarine and prolong its action.delay the excretion of tubocurarine and prolong its action.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1515
22 - -Thiazide DiureticsThiazide DiureticsAll thiazides affectthe distal tubule, and all have equal maximum diuretic effects,
differing only in potency (expressed on a per milligram basis). [Note: They are sometimes called â€oeceiling diuretics,†because increasing the dose above normal does not promote a further diuretic response.] Like the actions of the loop diuretics, the thiazides partly depend on renal prostaglandin synthesis by a mechanism that is not yet understood.
Mechanism and site of actionMechanism and site of actionThiazideThiazide diuretics diuretics inhibit reabsorptioninhibit reabsorption of sodium from the lumen in the cortical of sodium from the lumen in the cortical
ascending (diluting) limb of Henle's loop and the distal convoluted tubule. The ascending (diluting) limb of Henle's loop and the distal convoluted tubule. The exact cellular mechanism of action is uncertain. Inhibition of glycolysis and exact cellular mechanism of action is uncertain. Inhibition of glycolysis and diminution of energy supplies (ATP) required for transport have been implicated.diminution of energy supplies (ATP) required for transport have been implicated.
PharmacokineticsPharmacokineticsThiazide diuretics are rapidly absorbed from the gastrointestinal tract. The more Thiazide diuretics are rapidly absorbed from the gastrointestinal tract. The more
substituted drugs (i.e., with hydrophobic side-chain) are more highly bound to substituted drugs (i.e., with hydrophobic side-chain) are more highly bound to plasma proteins. As well, they are more lipid-soluble and have a greater apparent plasma proteins. As well, they are more lipid-soluble and have a greater apparent volume of distribution. Protein binding decreases the rate of tubular secretion. volume of distribution. Protein binding decreases the rate of tubular secretion. Lipid solubility enhances reabsorption along the distal nephron. Most of these Lipid solubility enhances reabsorption along the distal nephron. Most of these agents are excreted unchanged in the urine. agents are excreted unchanged in the urine.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1616
Actions:Increased excretion of Na+ and Cl-: Chlorothiazide causes diuresis with increased Na+
and Cl- excretion which can result in the excretion of a very hyperosmolar urine. Loss of K+: Because thiazides increase the Na+ in the filtrate arriving at the distal tubule,
more K+ is also exchanged for Na+, resulting in a continual loss of K+ from the body with prolonged use of these drugs. Therefore, it is imperative to measure serum K+ often (more frequently at the beginning of therapy) to assure that hypokalemia does not develop
Therapeutic uses:a. Hypertension: Clinically, the thiazides have long been the mainstay of antihypertensive medication,
because they are inexpensive, convenient to administer, and well tolerated. They are effective in reducing systolic and diastolic blood pressure for extended periods in the majority of patients with mild to moderate
essential hypertension. After 3 to 7 days of treatment, the blood pressure stabilizes at a lower level and can be maintained indefinitely by a daily dosage level of the drug, which causes lower peripheral resistance without having a major diuretic effect.
Many patients can be continued for years on the thiazides alone, although a small percentage of patients require additional medication, such as β-adrenergic blockers. [Note: Thehypotensive actions of angiotensin-converting enzyme inhibitors are enhanced when given in combination with the thiazides.]
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1717
b. Heart failure: Thiazides can be the diuretic of choice in reducing extracellular volume in mild to moderate
heart failure. If the thiazide fails, loop diuretics may be useful.
c. Hypercalciuria: The thiazides can be useful in treating idiopathic hypercalciuria, because they inhibit urinary Ca2+ excretion. This is particularly beneficial for patients with calcium oxalate stones in the urinary tract.
d.Diabetes insipidus: Thiazides have the unique ability to produce a hyperosmolar d. urine. Thiazides can substitute for antidiuretic hormone in the treatment of nephrogenic diabetes insipidus. The urine volume of
such individuals may drop from 11 L/day to about 3 L/day when treated with the drug.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1818
Adverse effectsMost of the adverse effects involve problems in fluid and electrolyte balance.Potassium depletion: Hypokalemia is the most frequent problem encountered
with the thiazide diuretics, and it can predispose patients who are taking digitalis to ventricular arrhythmias (Figure 22.5). Often, K+ can
be supplemented by diet alone, such as by increasing the intake of citrus fruits, bananas, and prunes. In some cases, K+ salt supplementation may be necessary. Activation of the renin-angiotensin-aldosterone
system by the decrease in intravascular volume contributes significantly to urinary K+ losses. Under these circumstances, the K+ deficiency can be overcome by spironolactone, which interferes with aldosterone
action, or by administering triamterene, which acts to retain K+. Low-sodium diets blunt the potassium depletion caused by thiazide diuretics.
HyponatremiaThis serious adverse effect may develop due to elevation of ADH as a result of
hypovolemia, as well as diminished diluting capacity of the kidney and increased thirst. Limiting water intake and lowering the dose of diuretic can prevent this condition.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 1919
Sustained hypercalcemia is very occasionally seen with thiazide diuretic use. This is Sustained hypercalcemia is very occasionally seen with thiazide diuretic use. This is partly due to the increased calcium reabsorption by the kidney. Its presence should partly due to the increased calcium reabsorption by the kidney. Its presence should alert the physician to pathological states that cause increased serum calcium alert the physician to pathological states that cause increased serum calcium (hyperparathyroidism, neoplastic disease.(hyperparathyroidism, neoplastic disease.
Volume depletion: This can cause orthostatic hypotension o d. r light-headedness.Hypercalcemia: The thiazides inhibit the secretion of Ca2+, sometimes leading to
elevated levels of Ca2+ inthe blood.e . Hyperglycemia: Patients with diabetes mellitus who are taking thiazides for
hypertension may become hyperglycemic and have difficulty in maintaining appropriate blood sugar levels. This is due to impaired release of insulin and tissue uptake of glucose.
f. Hyperlipidemia: The thiazides can cause a 5- to 15-percent increase in serum cholesterol as well as increased serum low-density lipoproteins. Lipid levels, however, may return to normal with long-term therapy.
g.. Hypersensitivity: Bone marrow suppression, dermatitis, necrotizing vasculitis, and interstitial nephritis are
Thiazide diuretics occasionally produce gastrointestinal intolerance (nausea and Thiazide diuretics occasionally produce gastrointestinal intolerance (nausea and vomiting), pancreatitis, and allergic manifestations (e.g., skin rashes). vomiting), pancreatitis, and allergic manifestations (e.g., skin rashes). Thrombocytopenia and agranulocytosis are rare toxic phenomena.Thrombocytopenia and agranulocytosis are rare toxic phenomena.
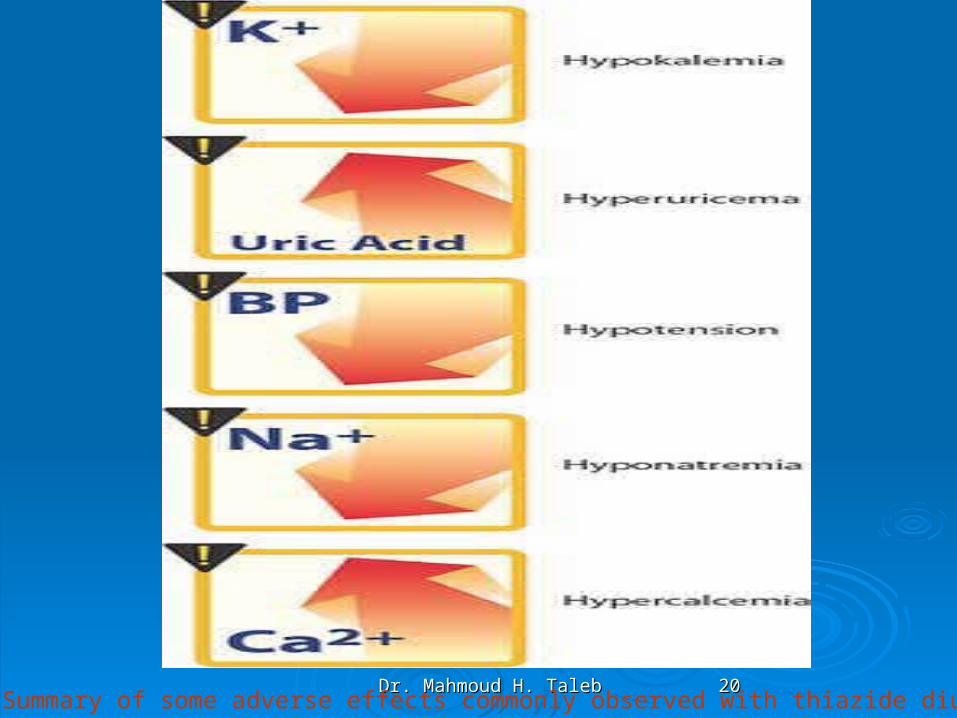
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2020Figure Summary of some adverse effects commonly observed with thiazide diuretics.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2121
33 - -Carbonic Anhydrase Carbonic Anhydrase Inhibitors: AcetazolamideInhibitors: Acetazolamide
Mechanism and site of actionMechanism and site of actionAcetazolamide inhibits proximal renal tubular and luminal brush-border carbonic Acetazolamide inhibits proximal renal tubular and luminal brush-border carbonic
anhydrase. Normally carbonic anhydrase catalyzes the reaction:anhydrase. Normally carbonic anhydrase catalyzes the reaction:Inhibition of carbonic anhydrase results in delayed conversion of intraluminal Inhibition of carbonic anhydrase results in delayed conversion of intraluminal
carbonic acid (H2CO3) to CO2 and H2O. The rise in luminal H+ carbonic acid (H2CO3) to CO2 and H2O. The rise in luminal H+ concentration provides a gradient against H+ secre tion from the tubular cell. concentration provides a gradient against H+ secre tion from the tubular cell. The intracellular hydration of CO2 to H2CO3 and subsequent production of The intracellular hydration of CO2 to H2CO3 and subsequent production of H+ and HCO3– is retarded. Therefore, intracellular H+ available for H+ and HCO3– is retarded. Therefore, intracellular H+ available for secretion into the tubular lumen is also decreased. Proximal tubular secretion into the tubular lumen is also decreased. Proximal tubular reclamation of filtered bicarbonate (HCO3–) occurs indirectly by combina reclamation of filtered bicarbonate (HCO3–) occurs indirectly by combina tion of secreted H+ with filtered HCO3– to ultimately form CO2 and H2O, tion of secreted H+ with filtered HCO3– to ultimately form CO2 and H2O, which are immediately reabsorbed. Carbonic anhydrase inhibition causes which are immediately reabsorbed. Carbonic anhydrase inhibition causes HCO3– to remain in the tubular fluid. Furthermore, since sodium is the HCO3– to remain in the tubular fluid. Furthermore, since sodium is the cation that accompanies the entry of HCO3– into the peritubular circulation, cation that accompanies the entry of HCO3– into the peritubular circulation, carbonic anhydrase inhibition results in some natriuresis. This natriuresis is carbonic anhydrase inhibition results in some natriuresis. This natriuresis is mild, partly because proximal sodium reabsorption is proportionately larger mild, partly because proximal sodium reabsorption is proportionately larger with other sol utes, and because of sodium uptake at more distal sites.with other sol utes, and because of sodium uptake at more distal sites.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2222
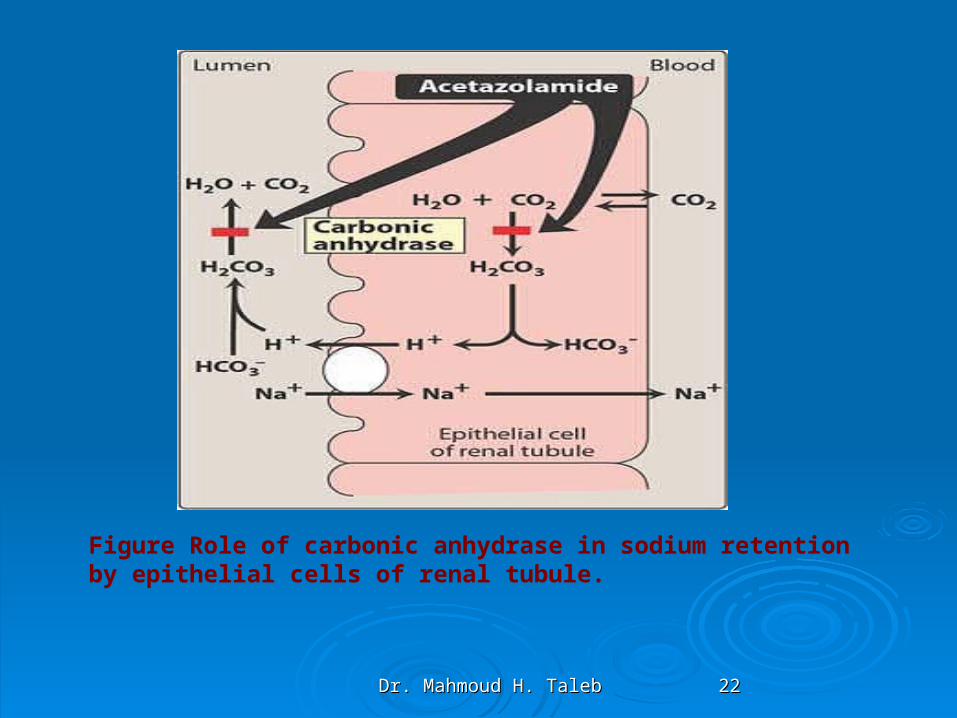
Figure Role of carbonic anhydrase in sodium retention by epithelial cells of renal tubule.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2323
PharmacokineticsPharmacokinetics Carbonic anhydrase inhibitors, like Carbonic anhydrase inhibitors, like
thiazide diuretics, are well absorbed from thiazide diuretics, are well absorbed from the gastrointestinal tract and excreted via the gastrointestinal tract and excreted via proximal renal tubular secretion within 24 proximal renal tubular secretion within 24 hours.hours.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2424
Therapeutic usesTreatment of glaucoma: The most common use of acetazolamide is
to reduce the elevated intraocular pressure of open-angle glaucoma. Acetazolamide decreases the production of aqueous humor, probably by blocking carbonic anhydrase in the ciliary
body of the eye. It is useful in the chronic treatment of glaucoma but should not be used for an acute attack; pilocarpine is preferred for an acute attack because of its immediate action. Topical carbonic anhydrase inhibitors, such as dorzolamide and brinzolamide, have the advantage of not causing any systemic effects.
Mountain sickness: Less commonly, acetazolamide can be used in the prophylaxis of acute mountain sickness among healthy, physically active individuals who rapidly ascend above 10,000 feet. Acetazolamide given nightly for 5 days before the ascent prevents the weakness, breathlessness, dizziness, nausea, and
cerebral as well as pulmonary edema characteristic of the syndrome.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2525
Ad verse effectsAd verse effectsThe most frequent adverse effects seen with carbonic anhydrase The most frequent adverse effects seen with carbonic anhydrase
inhibitors are hypokalemia and systemic metabolic acidosis.inhibitors are hypokalemia and systemic metabolic acidosis.Allergic and toxic effects are similar to those of other thiazide diuretics. Allergic and toxic effects are similar to those of other thiazide diuretics.
Acute renal failure caused by nephrolithiasis (acetazolamide may Acute renal failure caused by nephrolithiasis (acetazolamide may crystallize in acidic urine) has been described during chronic acet crystallize in acidic urine) has been described during chronic acet azolamide use in the treatment of glaucoma. A more recent azolamide use in the treatment of glaucoma. A more recent congener, methazolamide (Neptazane), has not caused this side congener, methazolamide (Neptazane), has not caused this side effect.effect.
Drug interactionsDrug interactionsNo recognizable adverse drug interactions have been described for No recognizable adverse drug interactions have been described for
these agents. When carbonic anhydrase inhibitors are combined these agents. When carbonic anhydrase inhibitors are combined with thiazide and loop di uretics, the natriuretic and kaliuretic effects with thiazide and loop di uretics, the natriuretic and kaliuretic effects of the drugs can be augmented.of the drugs can be augmented.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2626
4- Potassium-Sparing Diuretics4- Potassium-Sparing DiureticsAldosterone antagonists: spironolactoneAldosterone antagonists: spironolactone
Mechanism and site of actionMechanism and site of action::Normally, aldosterone acts on nephron segments beyond the distal convoluted Normally, aldosterone acts on nephron segments beyond the distal convoluted
tubule, stimulating sodium reabsorption in exchange for potassium and tubule, stimulating sodium reabsorption in exchange for potassium and hydrogen ions. Spironolactone and its major metabolite, canrenone, inhibit hydrogen ions. Spironolactone and its major metabolite, canrenone, inhibit the effect of aldosterone on the kidney. Both bind competitively to the effect of aldosterone on the kidney. Both bind competitively to cytosolic receptor sites for aldosterone prior to translocation into the cytosolic receptor sites for aldosterone prior to translocation into the nucleus.nucleus.
Pharmacokinetics:Pharmacokinetics:Spironolactone is well absorbed from the gastrointestinal tract and rapidly Spironolactone is well absorbed from the gastrointestinal tract and rapidly
undergoes hepatic biotransformation to canrenone, the major metabolite. undergoes hepatic biotransformation to canrenone, the major metabolite. Canrenone is highly protein-bound and has an elimination half-life of Canrenone is highly protein-bound and has an elimination half-life of approximately 18 hours, so it contributes to the total dura tion of action of approximately 18 hours, so it contributes to the total dura tion of action of spironolactone. Excretion occurs via the kidneys and the gastrointestinal spironolactone. Excretion occurs via the kidneys and the gastrointestinal tract.tract.
Pharmacological effects:Pharmacological effects:Aldosterone-stimulated sodium reabsorption in exchange for potassium and Aldosterone-stimulated sodium reabsorption in exchange for potassium and
hydrogen ion, in the distal, collecting tubules and ducts, accounts for only hydrogen ion, in the distal, collecting tubules and ducts, accounts for only 2-3% of total sodium reabsorption. Spironolactone therefore causes only a 2-3% of total sodium reabsorption. Spironolactone therefore causes only a mild natriuresis.mild natriuresis.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2727
Adverse effectsAdverse effects:: The most potentially dangerous adverse effect of The most potentially dangerous adverse effect of
spironolactone is hyperkalemia. This occurs frequently spironolactone is hyperkalemia. This occurs frequently because of inadvertent admin istration of spironolactone because of inadvertent admin istration of spironolactone together with potassium supplementation, or because of together with potassium supplementation, or because of administration to patients with moderate-to-severe renal administration to patients with moderate-to-severe renal insufficiency.insufficiency.
Other frequent side effects of spironolactone in clude an Other frequent side effects of spironolactone in clude an unpleasant peppermint aftertaste and nau sea/vomiting. unpleasant peppermint aftertaste and nau sea/vomiting. Its steroid molecular structure has been implicated in Its steroid molecular structure has been implicated in painful gynecomastia, frequently noted in men. Other painful gynecomastia, frequently noted in men. Other side effects related to the steroid structure include loss of side effects related to the steroid structure include loss of libido, impotence, and men strual irregularities. libido, impotence, and men strual irregularities.

Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2828
Other potassium-sparing diuretics: triamterene and Other potassium-sparing diuretics: triamterene and amiIoride:amiIoride:
Mechanism and site of actionMechanism and site of action::Triamterene and amiloride inhibit sodium transport in nephron segments beyond the Triamterene and amiloride inhibit sodium transport in nephron segments beyond the
distal convoluted tubule. They do not interact with aldosterone receptors. The specific distal convoluted tubule. They do not interact with aldosterone receptors. The specific mechanism of action of triamterene is still unknown. Amiloride directly inhibits the mechanism of action of triamterene is still unknown. Amiloride directly inhibits the luminal sodium channel. Since sodium uptake enhances potassium secretion in the luminal sodium channel. Since sodium uptake enhances potassium secretion in the collecting duct, inhibition of sodium uptake reduces potassium loss.collecting duct, inhibition of sodium uptake reduces potassium loss.
PharmacokineticsPharmacokinetics::Triamterene undergoes fast and essentially complete gastrointestinal absorption, Triamterene undergoes fast and essentially complete gastrointestinal absorption,
whereas only 50% of amiloride is absorbed. Onset of diuretic effect is similar for the whereas only 50% of amiloride is absorbed. Onset of diuretic effect is similar for the two drugs, occurring some 2 hours after ingestion. Duration of effect for triamterene is two drugs, occurring some 2 hours after ingestion. Duration of effect for triamterene is 7-9 hours and up to 24 hours for amiloride.7-9 hours and up to 24 hours for amiloride.
Pharmacological effectsPharmacological effects::Since sodium uptake by the collecting tubules and ducts accounts for only 2-3% of total Since sodium uptake by the collecting tubules and ducts accounts for only 2-3% of total
sodium reabsorption, only a mild natriuresis will occur with these potassium-sparing sodium reabsorption, only a mild natriuresis will occur with these potassium-sparing diuretics. The natriuresis is coupled with decreased potassium excretion.diuretics. The natriuresis is coupled with decreased potassium excretion.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 2929
Adverse effectsAdverse effects::The major adverse effect is hyperkalemia, which frequently The major adverse effect is hyperkalemia, which frequently
occurs because of inadvertent concurrent potassium occurs because of inadvertent concurrent potassium supplementation, coadministration of ACE inhibitors, or supplementation, coadministration of ACE inhibitors, or because of moderate to severe renal insufficiency. because of moderate to severe renal insufficiency. Another fre quent adverse effect is gastrointestinal Another fre quent adverse effect is gastrointestinal intolerance.intolerance.
Drug interactions:Drug interactions:Although not extensively studied, nonsteroidal anti-Although not extensively studied, nonsteroidal anti-
inflammatory agents op pose the natriuretic effect of inflammatory agents op pose the natriuretic effect of triamterene. Further more, use of indomethacin together triamterene. Further more, use of indomethacin together with triamterene has been reported to cause reversible with triamterene has been reported to cause reversible renal insuffi ciency.renal insuffi ciency.
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3030
5- Osmotic Diuretics:5- Osmotic Diuretics:Mannitol Mannitol and and urea urea have been utilized as osmotic diuretics. For this have been utilized as osmotic diuretics. For this
purpose these agents are adminis tered intravenously; they are purpose these agents are adminis tered intravenously; they are rapidly and freely filtered by the glomerulus. The hyperosmolality rapidly and freely filtered by the glomerulus. The hyperosmolality caused by the high intratubular concentration of these solutes caused by the high intratubular concentration of these solutes prevents sodium reabsorption by effectively diluting the intraluminal prevents sodium reabsorption by effectively diluting the intraluminal sodium concentration and by markedly increasing the tubular fluid sodium concentration and by markedly increasing the tubular fluid flow rate. The overall effect is increased sodium and water flow rate. The overall effect is increased sodium and water excretion.excretion.
The adverse effects encountered with osmotic diuretics include The adverse effects encountered with osmotic diuretics include hypokalemia and acute intravascular volume overload. The latter hypokalemia and acute intravascular volume overload. The latter effect occurs because the osmotic agent increases the transfer of effect occurs because the osmotic agent increases the transfer of fluid to the intravascular compartment from interstitial sites. The fluid to the intravascular compartment from interstitial sites. The principal indications for the use of mannitol are to reduce brain principal indications for the use of mannitol are to reduce brain edema (e.g., head trauma) and to acutely expand the intravascular edema (e.g., head trauma) and to acutely expand the intravascular volume (e.g., during cardiovascular surgery).volume (e.g., during cardiovascular surgery).
Dr. Mahmoud H. TalebDr. Mahmoud H. Taleb 3131
THERAPEUTIC APPLICATIOnTHERAPEUTIC APPLICATIOnEdemaEdemaPulmonary edema:Pulmonary edema:Congestive cardiac failure:Congestive cardiac failure:Cirrhosis with ascites:Cirrhosis with ascites:Renal diseasesRenal diseasesHypertensionHypertensionHyperparathyroidism:Hyperparathyroidism: